how to use information from implantable sensors
TRANSCRIPT

How to use Information from
Implantable Sensors
Jag Singh MD DPhil FHRS
Massachusetts General Hospital
Harvard Medical School
Boston
Session: Follow up of CRT patients

Presenter Disclosure Information
FINANCIAL DISCLOSURE:
Research Grants: Boston Scientific, Biotronik,
Medtronic, St. Jude Medical
Steering Committee, DSMB Boston Scientific, CardioInsight,
Consulting: Medtronic, St. Jude Medical
Sorin Group, Biosense Webster,
theheart.org, Respicardia Inc.
Educational Symposia: Boston Scientific, Biotronik,
St. Jude Medical, Sorin Group
Stock Options: None
Salary Support: None
Speaker Bureau: None
Overview
• The Paradigm Shift in CRT Patient Care
• Sensors: • What and Why?
• Types
• Levels of Monitoring
• Role of Sensors • Clinical situations
• Risk Stratification
• Sensors in the Pipeline
• Tying it all together

CRT Patient: Need for a Multi-factorial Approach
TRIGGERS
ACUTE HF
CHRONIC HF
CO-MORBIDITIES
CRT
Patient

Chronic renal failure
Percent of Comorbid Diseases in CHF Patients
Depression
Thyroid
Lower respiratory
Osteoarthritis
Peripheral vascular
Dyslipidemia
Valve
Ocular
COPD
Diabetes
Arrythmias
CAD
HTN
Braunstein JB. J Am Coll. Cardiol. 2003 Oct 1;42(7):1226-33.

The Goal: Stabilize Disease Progression
• Cumulative effect of
recurrent acute heart
failure events leads to
progressive decline in
cardiac function
• Sensor strategies and
timely intervention may
help
Gheorghiade M, et al, AJC 2005

What is a Sensor?
• In a closed system, the sensor is an element
connected to the device that detects change
and signals the ‘effector’ to initiate a
response
• The effector could be:
– The Patient
– The Healthcare Provider
– The Device

Device Based Monitoring & Intervention
• Simple Sensors
• Heart rate and derivatives
• Accelerometers
• Impedance-based
• Sophisticated Sensors
• Pressure: left atrial pressure, pulmonary artery pressure,
RV dP/dt, etc.
• Heart Sounds: PEA
• Cardiac Output: Doppler
• Chemicals: PO2, PCO2, pH, electrolytes and glucose
• Biomarkers: TNF, BNP, etc.
Merchant, Dec and Singh JP. Circulation EP, 2010:3: 357

Heart Rate Trend and Hospitalization
Hospital stay
Ellery et al. Clin Res Cardiol 2006

Respiration Sensor : Progressive increase in Minute
Ventilation prior to HF event
Respiration Rate
Tid
al V
olu
me

Heart Rate Variability (SDANN) and Clinical
Course
Days from the Implant Visit
Sur
viva
l Pro
babi
lity
0 60 150 240 330 420
0.70
0.75
0.80
0.85
0.90
0.95
1.00
Quartiles of SDANN Two weeks
Days from the Three Month Visit
Sur
viva
l Pro
babi
lity
0 60 150 240 330 420
0.70
0.75
0.80
0.85
0.90
0.95
1.00
Quartiles of SDANN Three Months
Days from the Six Month Visit
Sur
viva
l Pro
babi
lity
0 60 150 240 330 420
0.70
0.75
0.80
0.85
0.90
0.95
1.00
Quartiles of SDANN Six Months
Days from the Implant Visit
Sur
viva
l Pro
babi
lity
0 60 150 240 330 420
0.70
0.75
0.80
0.85
0.90
0.95
1.00
Quartiles of Footprint Two weeks
IV (highest)IIIIII (low est)
Days from the Three Month Visit
Sur
viva
l Pro
babi
lity
0 60 150 240 330 420
0.70
0.75
0.80
0.85
0.90
0.95
1.00
Quartiles of Footprint Three Months
Days from the Six Month Visit
Sur
viva
l Pro
babi
lity
0 60 150 240 330 420
0.70
0.75
0.80
0.85
0.90
0.95
1.00
Quartiles of Footprint Six Months
Fantoni et al, JACC 2005:10;1875-82 Gilliam, FR, Singh JP et al, J Electrocardiol, 2007
HRV-HF Registry

Accelerometers & Physical Activity
Kadhiresan et al, AJC 2002:89;1435-7

Integrating the
Information
• Chicken & Egg
Situation
• Was the HF episode
precipitated by AF or
vice-versa?
• Non-responsiveness
worsened by atrial
arrhythmia
Merchant, Dec and Singh JP. Circulation
EP; 2010:3: 357

Risk Stratifying Prospectively: Using Device-based Signals

Simple Sensors and Outcome
• Clinical risk score
– Contak-Renewal Study
– Variables extracted from
device were dichotomized with
score of 1 for:
– SDANN <43
– mean HR >74
– Footprint < 29
– Physical activity % <5.
– Total score= sum of
dichotomized variables
– Low (1)
– Moderate: 2-3
– High: 4
Singh JP et al Europace 2010
N=838
18 % Mortality
4 % Mortality

PARTNERS-HF: Prognosticating Heart Failure Hospitalizations
• 694 CRT patients followed up for 1 year
• 141 HF hospitalizations
• Device diagnostic criteria when positive, were associated with a 5.5
fold increased risk for HF hospitalization
Whellan DJ et al, JACC 2010: 55: 1803

DOT-HF Study: Proactive intervention with
Audible Impedance Alerts
• 335 patients randomized to OptiVol information with audible alerts
• Heart Failure hospitalizations near 2-fold higher in the Access arm versus control arm
• 3-fold increase in outpatient visits
• Role of Impedance measures questionable?
Van Veldhuisen et al. Circulation 2011: 124

Sophisticated Sensors
Early Recognition & Intervention
for ADHF

Multivector Impedance
INTRA-CARDIAC VECTORS
• LV ring – RV ring
• LV ring – RA ring
INTRA-THORACIC VECTORS
• RV ring – Can
• LV ring – Can
• RA ring – can
• RV coil – Can
Khoury DS. J Am Coll Cardiol. 2009 Mar 24;53(12):1075-81
- Multiple vectors
- The LV ring–Can vector resulted in the fastest and largest change
in impedance and highly reflective of LV end diastolic volume and
LA pressure.

SV
SZ
Positive Correlation of
SZ and SV
LVEDV
ED
Z
Inverse Correlation of EDZ
and LVEDV
Impedance-based Sensor for Hemodynamics A Measure of LV volume changes
Ejection phase Filling phase
Impedance Impedance
R = 0.86
P < 0.001
R = -0.86
P < 0.001
Maier et al., Clin Res Cardiol 2007, 96 (Suppl 1):V1027

Proactive vs. Reactive Intervention Impedance vs. Hemodynamic sensors
Merchant F, Dec GW and Singh JP. Circulation EP, 2010:3: 357
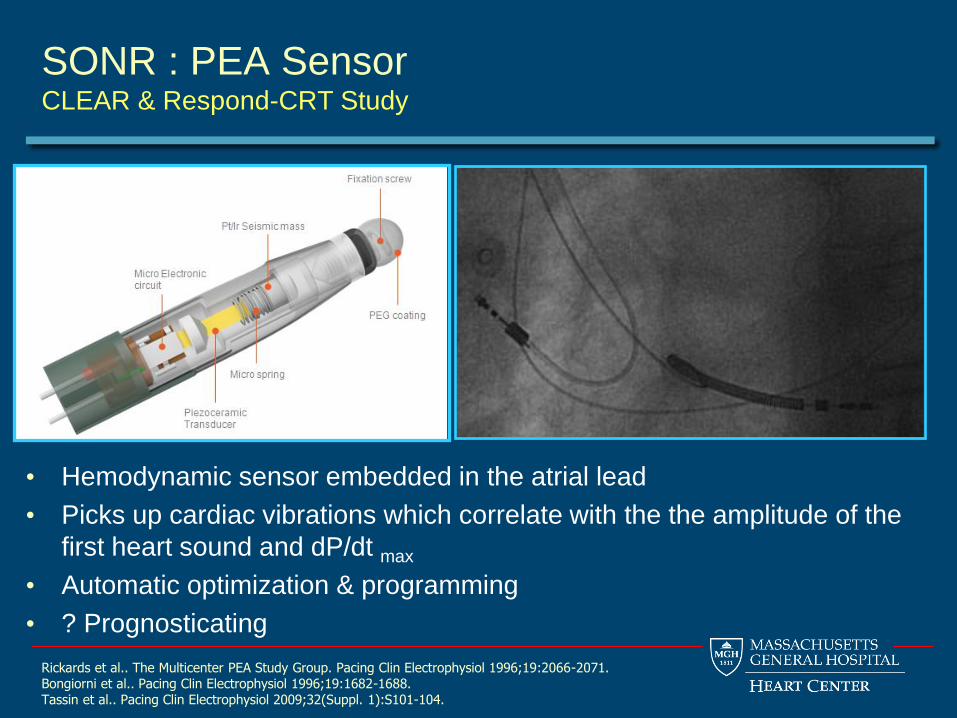
SONR : PEA Sensor CLEAR & Respond-CRT Study
• Hemodynamic sensor embedded in the atrial lead
• Picks up cardiac vibrations which correlate with the the amplitude of the
first heart sound and dP/dt max
• Automatic optimization & programming
• ? Prognosticating
Rickards et al.. The Multicenter PEA Study Group. Pacing Clin Electrophysiol 1996;19:2066-2071. Bongiorni et al.. Pacing Clin Electrophysiol 1996;19:1682-1688. Tassin et al.. Pacing Clin Electrophysiol 2009;32(Suppl. 1):S101-104.

Left Atrial Pressure Sensor Device
Merchant, Dec and Singh JP. Circulation EP, 2010:3: 357
Proximal Anchor
Distal
Anchor Sensor
Diaphragm ~ 3
mm
Implantable
Sensor Lead
(ISL)

• 40 patient study
• Prospective, observational and first-in-human
• After initiation of LAP-guided therapy – frequency of elevated readings (>25 mmHg) was reduced by 67%
– Mean daily LAP fell (from 17.6 mmHg to 14.8 mmHg)
– Doses of ACEI, ARB’s and BB were up-titrated by 37% and 40%, respectively, where as doses of loop diuretics fell by 27%
– Reduced compliance and LAP> 25 associated with HF
Ritzema J et al. Circulation 2010; 121: 1086
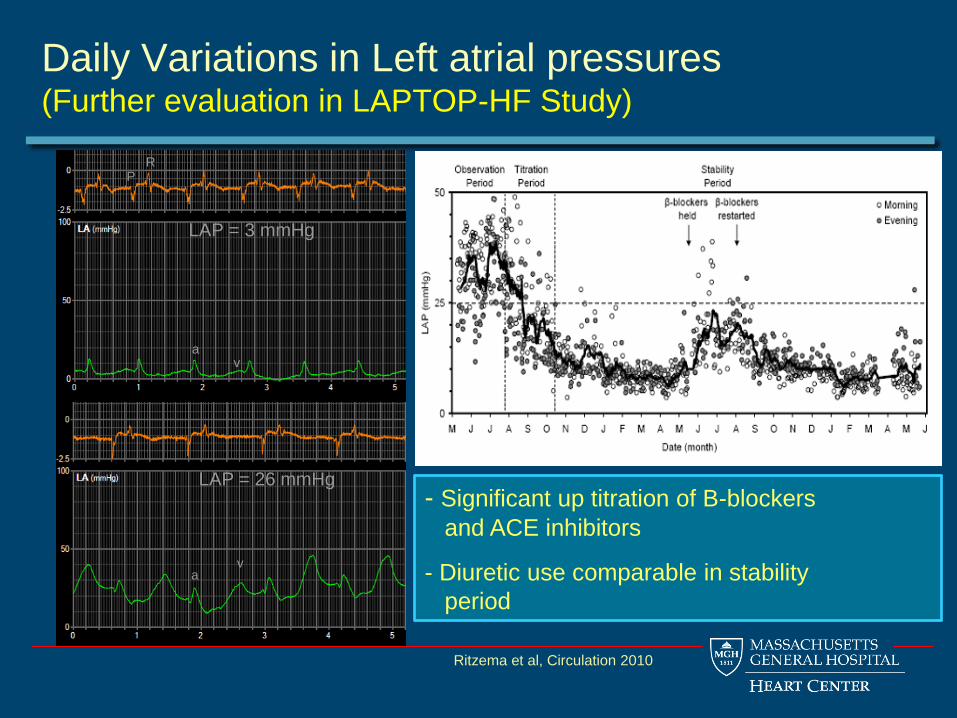
LAP = 3 mmHg
LAP = 26 mmHg
a v
a v
P R
Daily Variations in Left atrial pressures (Further evaluation in LAPTOP-HF Study)
- Significant up titration of B-blockers
and ACE inhibitors
- Diuretic use comparable in stability
period
Ritzema et al, Circulation 2010

Pulmonary Artery Pressure Monitoring
*CardioMEMS Inc., Atlanta, Georgia, USA; Caution: Investigational Device
Champion Study, Lancet 2010
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
0 90 180 270 360 450 540 630
HR = 0.71 (0.55-0.92), p = 0.009
No. at RiskTreatment270 226 202 169 130 104 84 62Control 280 223 186 146 113 80 57 39
TreatmentControl
Su
rviv
al o
r F
ree
do
m fro
m
First
HF
Ho
sp
ita
liza
tio
n
- Catheter-based delivery system
- Implanted PA branch diameter 7-15 mm
- Target range (mmHg):
– PA systolic: 15-35
– PA diastolic: 8-20
– PA mean: 10-25
29% relative risk reduction
550 NYHA III patients from 63 centers

Next Generation Hemodynamic Detection
• Bio-degradable material
• Miniaturization allowing implantations with minimally invasive techniques
• Locations: Endovascular & Epivascular
• Integrating the information for HF treatment
• Clinical testing and validation
EAP technology Bio-MEMs Sensor Technology (NASA)

Raisin System Links Therapy, Behavior and Physiology (Proteus Heart Study)
Self administration of Furosemide
Orthopnea / disrupted sleep Restful sleep

Putting it all together: Sensing & Intervening
Chronic HF
- Neurohormonal
status
- Compliance
- Myocardial risk
Heart Failure
Hospitalization
Triggers
- Ischemia
- Electrolytes
- Endothelial
function
• Arrhythmias
Co-Morbid - Diabetes
- HT
- COPD
- AF
EARLY DETERMINANTS
- Hemodynamic Instability
- LAP
- PADP
- RV dp/dt
- PEA
- Impedance-based
- Neurohormones
- Inflammatory markers
- CRP
- IL-6
- BNP, etc
- Acute vascular changes
- MR
- Venous drainage
LATE
DETERMINANTS
- Physical Activity
- Heart Rate
-HRV
-SDANN
-Footprint
- OptiVol
- Impedance-based
measures

Summary
• Where are we now? – Risk stratification for mortality
– Predicting heart failure exacerbations
– But still no concrete strategy and limited adoption
• Where do we need to be? – Sensors coupled with remote monitoring integrated into clinical
practice, facilitating personalized medicine
• The Future : – Multiple Sensors
– Automated prediction and prevention of heart failure
– Provide for care beyond heart failure
– Personalized medicine, with self-management strategies is here to stay


The Integrated Futuristic Device
Courtesy: David Hayes

Some important points
• Cardiomems – Intensive PAD monitoring
works
– Goal PAD 8-20
– Needs physician intervention
regularly
– Simpler implant
• LAP – Puts patient in control
– Computer algorithm incorporated
– Takes any intrinsic pre-capillary
PH out of the equation
– Direct access to LA and
waveforms
– More involved procedure
- Problem with both is that they leave the RV and RA out of the picture
- That’s why physical exam is important to understand patients physiology
- 24 hour averages maybe preferable than 2-points in time

Summary: Sensor Strategies
Current Generation:
• Surrogate measure
• Stand-alone
• Provider-dependent
• Intervention-independent
Next Generation:
• Primary measure
• Networked
• Provider-independent
• Intervention-dependent
Modified from Cleland, JACC 2009

Case example: LAP pre- and post Diuretics 60 year old man with ischemic CM (LVEF 25%)
a
v
a v
P R
= 40 = 13 LAP (mmHg) = 40 P LAP (mmHg) = 13
0900 hrs, Dynamic Therapy LAP-Guidance: Furosemide 80 mg 1300 hrs
Ritzema J, et al. Circulation 2010;121:1086-1095.