how to get maximum value from your emr dr. alan brookstone south island division of family practice...
TRANSCRIPT

How to Get Maximum Value from your EMR
Dr. Alan BrookstoneSouth Island Division of Family PracticeJanuary 30, 2012

Keys to Success
• Goals• Expectations• Leadership• Foundational computer skills• Practice, Practice, Practice• Collaboration• There are some things you cannot change, right
now…
Focus of Today’s Presentation
1. Adoption & Current State2. Data Quality3. Change and Workflow4. Training5. Maximizing EMR Use6. Sharing Knowledge & Skills

1. Adoption & Current State
• International• US vs. Canada• South Island
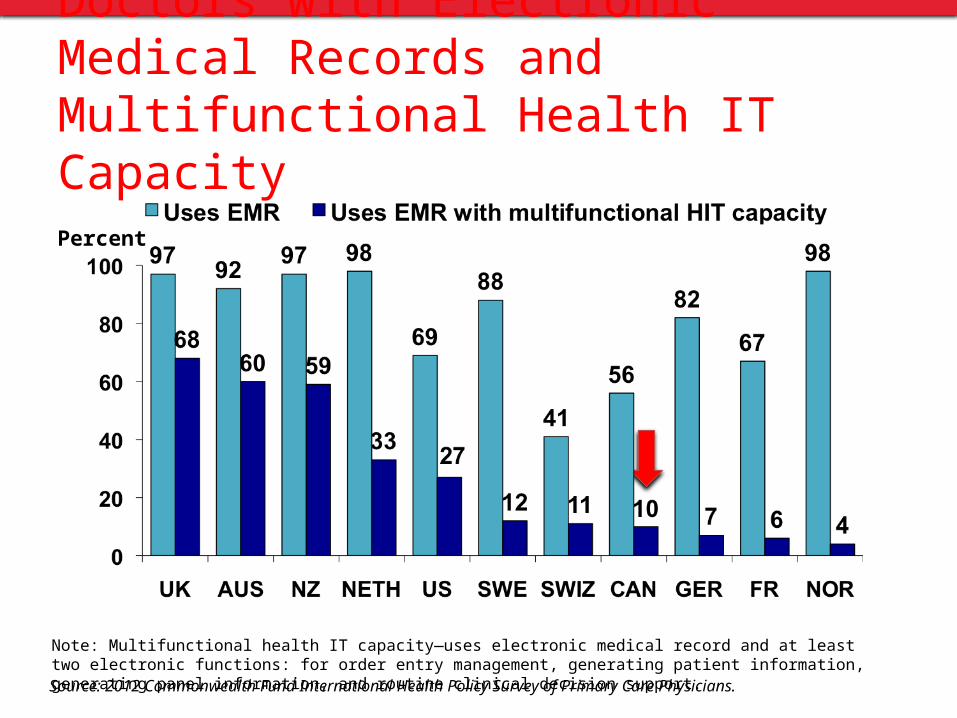
Note: Multifunctional health IT capacity—uses electronic medical record and at least two electronic functions: for order entry management, generating patient information, generating panel information, and routine clinical decision support.
Percent
Source: 2012 Commonwealth Fund International Health Policy Survey of Primary Care Physicians.
Doctors with Electronic Medical Records and Multifunctional Health IT Capacity

US – Regional Extension Center Program
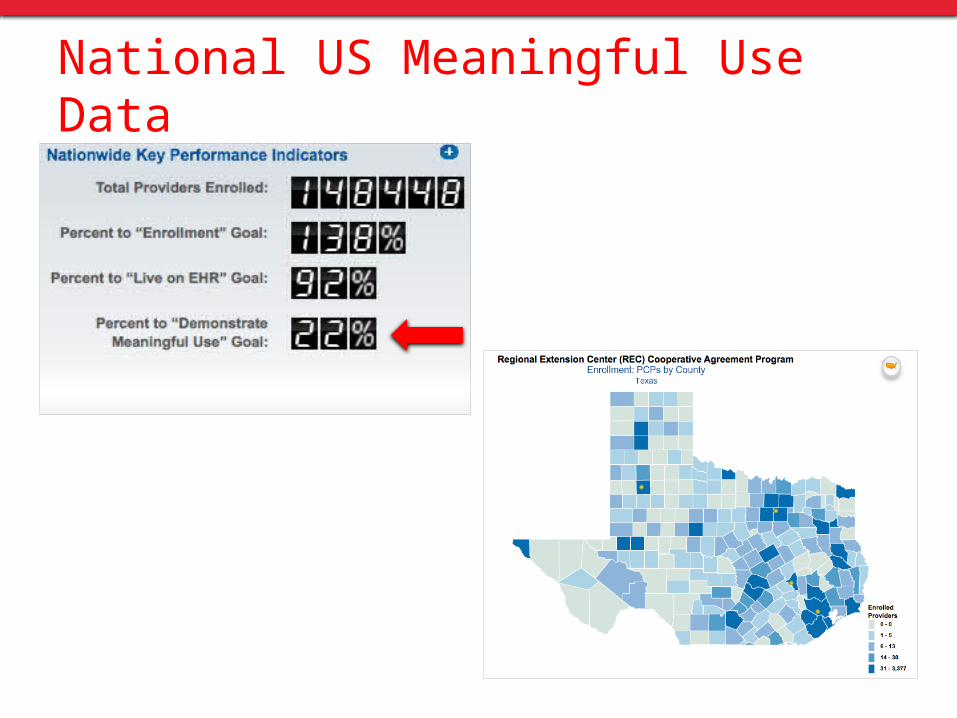
National US Meaningful Use Data
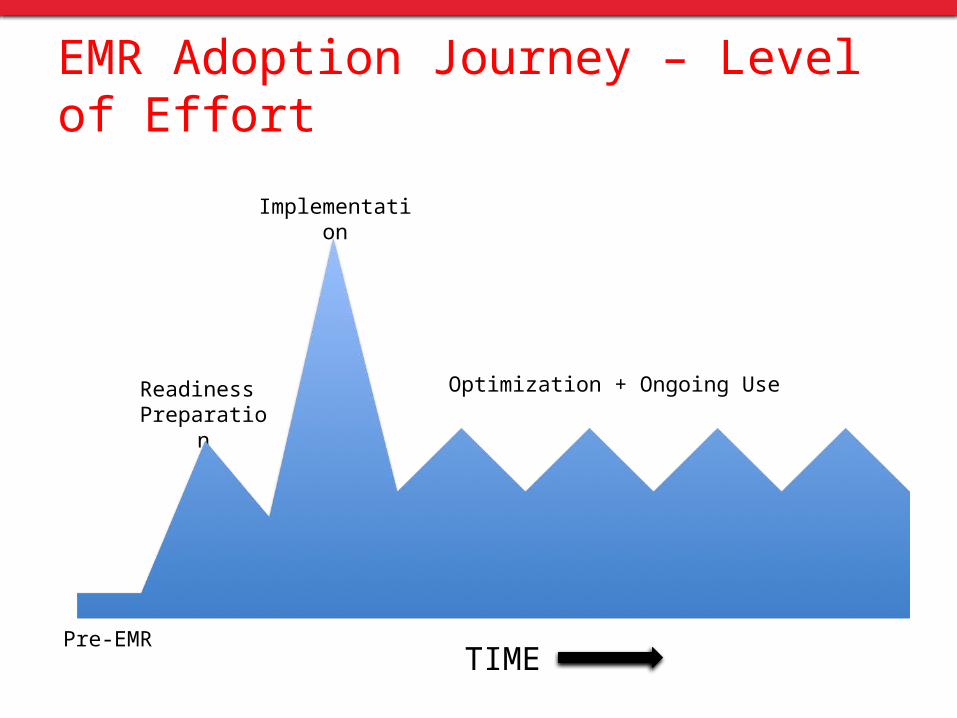
EMR Adoption Journey – Level of Effort
TIME
Readiness Preparation
Implementation
Optimization + Ongoing Use
Pre-EMR
Data Discipline
• Example - If you cannot identify your patients with bowel disease, how can you do colon cancer screening?
• Standardize– Coding– Diagnoses, Medications, Labs, History
• Clean– Coverage – all patients are in the system– Consistency – all data tells the same story– Completeness – all data is in the system– Correctness – right patients in, wrong patients out– Coded – all relevant data is coded or in a single format
• System thinking– Templates, reminders and searches work together
Dr. Karim Keshavjee – Physician & Consultant – Mississauga, Ontario

Adoption ≠ Effective Use of EMR
• 16.1% of physicians report using Electronic Medical Records instead of paper charts. This compares to 9.8% in 2007
• 34.1% of physicians used combination of paper charts and EMR in 2010 vs. 26.1% in 2007.
2010 National Physician Survey - http://www.nationalphysiciansurvey.ca/nps/home-e.asp
3. Change & Workflow
• Change is disruptive• No disruption = Not sustainable• How to manage the manage
– Set clear direction, goals and objectives– Communicate regularly– Invite and acknowledge contributions and concerns– Address resistance by asking for input– Reward initiative– Build commitment
Workflow
• Workflow describes how a process takes place. The process is evaluated and improved to ‘flow’ more smoothly
• Optimizing workflow– Improve efficiency– Reduce redundancy (waste/duplication)– Identify gaps or areas of instability
• Plan on paper first– Office Visits– Chart Conversions– Allergy/Therapeutic injections

Chart is placed at vitals station
Ht, Wt, BP Taken & recorded
Patient is called to vitals station
Patient is taken to exam room
Chart is placed in sleeve on exam door
Paper trigger
Paper trigger
Template needed
How many vitals stations?
How often do we see patient in room without vitals?
Are cuffs and scales available in all rooms?
How many BP’s do we miss?
Ann Lefebvre MSW, CPHQ, Executive Director, NC Regional Extension Center
Workflow – Vitals Collection

Workflow – Chart Conversion
• Stop Light System– Charts pulled for the next day and a GREEN dot is
applied. The paper chart is for read only – everything is documented in the EMR
– Additional information has been pre-loaded e.g. Meds, Allergies, Problem list, Recent vitals etc.
– Physicians flag additional information in the chart they wanted preloaded or scanned
– The next time the patient is seen, the chart gets a YELLOW dot, and a RED dot on the third visit
– 4th visit – chart is not pulled because of RED dot– Goal: Everything in chart that is needed by 3rd visit
Pearls
• Expect and manage disruption• EMR implementation is just the beginning, not the
destination• Change is never complete – processes can always be
improved

4. Training
• Training not just for implementation and upgrades • Should be ongoing and comprehensive - includes
new learning and advanced functions • As users get comfortable with a system, they learn
new and faster ways to work using the EMR• More complex features require more training

17
5. Maximizing EMR Use
• Clinical decision support• HIMSS Definition
– Clinical Decision Support is a process for enhancing health-related decisions and actions with pertinent, organized clinical knowledge and patient information to improve health and healthcare delivery
– Made up of:• Clinical elements e.g. reference information• Administrative elements e.g. alerts or reminders
Types of Clinical Decision Support
• Drug-Drug Interactions • Drug-Allergy interactions • Dose Range Checking • Pick lists• Standardized evidence based
order sets e.g. for CDM • Rules (core measures,
antibiotic usage, INR management)
• Links to knowledge references (in the EMR or Web-based)
• Alerts• Templates • Relevant data displays • Point of care reference
information• Diagnostic decision
support tools

19
Evaluation Criteria – Data & Tools
• Relevance• Efficiency• Sensitivity• Currency• Usability
20
Relevance
• General vs. specialty focused– Alerts, reminders, templates
• Is the tool primary care/internal medicine focused?– Chronic disease management
• How does it relate to your practice?– EMRs have their strengths and weaknesses

• Does the tool slow you down or improve efficiency?– Speed of use (number of mouse-clicks)
• Does the benefit outweigh the cost in terms of the time it takes to use it?– Financial & time cost vs. clinical benefit
21
Efficiency

• Does the tool provide the right amount of information to make the decision?– Too much or too little?– Who controls sensitivity settings?
• Individual user vs. practice level
• Need to ensure the right sensitivity settings – Alert sensitivity too high or low won’t provide the right
information at the right time
22
Sensitivity
• How timely is the information? Is it up-to-date?– Drug data– Clinical reference data– Out of date information loses relevance
23
Currency

• How does the tool fit into your workflow?– If distracting or poorly designed, can increase risk of error
• What is the general satisfaction of users?– Speak with colleagues– Importance of user groups
24
Usability & Human Factors

Where Can CDS Add Value?
• Improved quality– By guiding users to best practices
• Increased safety– By verifying an action was the intended one
• Reduced cost– By identifying duplicate or unnecessary orders
• Improved documentation– Using templates or order sets for specific conditions
• Improved communication– Among clinicians regarding patient status– Between clinicians and patients
Source: HIMSS
5. Tips to Maximize EMR Use
• Set goals, personally, at the practice level• Get complete buy-in from physicians and staff• First, optimize your internal practice environment• Hold regular practice meetings• Make your data comparable and reproducible. Standardize on lists, codes,
medications, order sets and templates• Avoid short cuts in documentation. It may be tempting to enter certain data in
narrative format – time pressured. To make data reproducible, it needs to be in a standard format
• Trust your gut. The EMR is a tool. Use clinical judgment when making decisions. Your EMR vendor is not infallible and needs your support and feedback
• Keep an open mind. What can your EMR do for you that you were never able to do before?
• Effective EMR Adoption and Use is about collaboration and the community in which you practice

Sharing Knowledge & Skills
• The skills and knowledge to be successful are right here in this room
• Mechanisms to support one another– Based upon common interests– Sustainable value
• Community level Goals– Improve health of CDM patients (e.g. recalls, alerts)– Information sharing – referrals & consultations (e.g. standardized
South Island referral form, improve format of consultation reports
• User Groups– EMR based - share knowledge, develop super users