how to do primary pci the basics and adjunctive pharmacology dr andrew sutton ma md frcp fesc...
TRANSCRIPT
How to do Primary PCI
The basics and adjunctive pharmacology
Dr Andrew Sutton MA MD FRCP FESCConsultant Cardiologist
The James Cook University Hospital
NO CONFLICT OF INTEREST TO DECLARE

Before the cath lab..
• Discussion, formulation and agreement of a clear regional protocol is key
• Essential stakeholders: ambulance services, regional cardiologists, General Practitioners; walk-in centres; A&E staff
Before the cath lab..
• Aim for one pre-hospital patient pathway for each geographical region – irrespective of the day of the week, time of day, start/end of shifts.
• Familiarity with and repetition of a single pathway breed slickness and efficiency
• Continuous review, audit and feedback essential

Monthly median door to balloon times (minutes) JCUH October 2006 to October 2008
50
5754
49
5350
40 41 40
34.5
30.53234
48.5
39
44.544
35
4744
52
49
69
60.5
63
0
10
20
30
40
50
60
70
80
Oct
06
Nov
06
Dec
06
Jan
07
Feb
07
Mar
07
Apr
07
May
07
Jun
07
Jul
07
Aug
07
Sep
07
Oct
07
Nov
07
Dec
07
Jan
08
Feb
08
Mar
08
Apr
08
May
08
Jun
08
Jul
08
Aug
08
Sep
08
Oct
08
Oct 06 to Oct 07=52.3 minutes
Nov 07 to Jun 08=42.4 minutes
Jun 08 to Oct 08 32.8 minutes
mean
ucl
Influence of PPCI pathway policy changes on median door to balloon times The James Cook University Hospital October 2006 to October 2008

Monthly median door to balloon times (minutes) JCUH October 2006 to October 2008
50
5754
49
5350
40 41 40
34.5
30.53234
48.5
39
44.544
35
4744
52
49
69
60.5
63
0
10
20
30
40
50
60
70
80
Oct
06
Nov
06
Dec
06
Jan
07
Feb
07
Mar
07
Apr
07
May
07
Jun
07
Jul
07
Aug
07
Sep
07
Oct
07
Nov
07
Dec
07
Jan
08
Feb
08
Mar
08
Apr
08
May
08
Jun
08
Jul
08
Aug
08
Sep
08
Oct
08
Oct 06 to Oct 07=52.3 minutes
Nov 07 to Jun 08=42.4 minutes
Jun 08 to Oct 08 32.8 minutes
mean
ucl
Influence of PPCI pathway policy changes on median door to balloon times The James Cook University Hospital October 2006 to October 2008
CCU coordinator receives call from paramedic crew and copy of initial ECG

Monthly median door to balloon times (minutes) JCUH October 2006 to October 2008
50
5754
49
5350
40 41 40
34.5
30.53234
48.5
39
44.544
35
4744
52
49
69
60.5
63
0
10
20
30
40
50
60
70
80
Oct
06
Nov
06
Dec
06
Jan
07
Feb
07
Mar
07
Apr
07
May
07
Jun
07
Jul
07
Aug
07
Sep
07
Oct
07
Nov
07
Dec
07
Jan
08
Feb
08
Mar
08
Apr
08
May
08
Jun
08
Jul
08
Aug
08
Sep
08
Oct
08
Oct 06 to Oct 07=52.3 minutes
Nov 07 to Jun 08=42.4 minutes
Jun 08 to Oct 08 32.8 minutes
mean
ucl
Influence of PPCI pathway policy changes on median door to balloon times The James Cook University Hospital October 2006 to October 2008
CCU coordinator receives call from paramedic crew and copy of initial ECG
Patient admitted directly to cath lab

Monthly median door to balloon times (minutes) JCUH October 2006 to October 2008
50
5754
49
5350
40 41 40
34.5
30.53234
48.5
39
44.544
35
4744
52
49
69
60.5
63
0
10
20
30
40
50
60
70
80
Oct
06
Nov
06
Dec
06
Jan
07
Feb
07
Mar
07
Apr
07
May
07
Jun
07
Jul
07
Aug
07
Sep
07
Oct
07
Nov
07
Dec
07
Jan
08
Feb
08
Mar
08
Apr
08
May
08
Jun
08
Jul
08
Aug
08
Sep
08
Oct
08
Oct 06 to Oct 07=52.3 minutes
Nov 07 to Jun 08=42.4 minutes
Jun 08 to Oct 08 32.8 minutes
mean
ucl
Influence of PPCI pathway policy changes on median door to balloon times The James Cook University Hospital October 2006 to October 2008
CCU coordinator receives call from paramedic crew and copy of initial ECG
Patient admitted directly to cath lab
Cath lab opened byresident member of staff
Aways room for improvement..

Help your out of area ambulance colleagues...


DTB direct Q3 2009 2010
Door to Balloon (direct) October 2009 to December 2009
46
43
40
39
38
36
0
50
100
150
200
250
300
350
400
450
Oct09 Oct09 Oct09 Nov09 Nov09 Nov09 Nov09 Nov09 Dec09 Dec09 Dec09 Dec09 Dec09 Dec09
DTB median 33.5 ucl 93

In the cath lab..• Brief assessment (history, ECG , examination)• Exclude aortic dissection, PE• Look for acute MR, VSD; determine access• Previous angio available?• Determine history of allergy• Record usual medication (esp. anticoagulants)
and medication already administered (aspirin, opiate analgesia)
• Obtain witnessed verbal consent

In the cath lab..• Slick patient preparation (iv access; ECG
monitoring; remote pads for defibrillation; monitoring of O2; removal of jewellery)
• Access – “normal” route is radial (82% radial last 1000 sequential cases in JCUH)
• Preferable to have easy access to femoral artery, even if not used

In the cath lab..• Common practice to administer a
“radial cocktail” (GNT/verapamil +/- UFH) after sheath insertion
• Advisable to avoid verapamil for STEMI• Diagnostic angio followed by choice of
guide catheter or whole procedure with Kiemeneij guide catheter

In the cath lab..• Do the case• Use of a thrombus extraction device is normal
practice• Clarify any pending non cardiac surgery prior
to choice of stent• Ask yourself if the stent big enough• TR band for radial access (increasingly use of
a closure device for femoral access)• Do the next case

In the cath lab – particular considerations
• Inferior STEMI– Bezold-Jarisch reaction: liberal use of iv fluids,
atropine; may require phenylephrine
• Culprit vessel or MV PCI?– Our default strategy is culprit vessel PCI (MV
PCI performed in context of cardiogenic shock and lack of haemodynamic response to culprit vessel PCI)

“A word of advice, Durk: it’s the Mesolithic, we’ve domesticated the dog, we’re using stone tools and no one’s naked anymore.”
JCUH drugs
Aspirin loading 300mg (paramedic).
Weight adjusted UFH (60U per kg) assuming patient will also receive ReoPro (89% of last 1000 sequential cases).
ReoPro is only administered in the cath lab.
“A word of advice, Durk: it’s the Mesolithic, we’ve domesticated the dog, we’re using stone tools and no one’s naked anymore.”
JCUH drugs
Clopidogrel loading 600mg
(not by paramedics)
For self-presenters to local or regional A&E, load with aspirin 300mg and clopidogrel 600mg prior to urgent transfer

“A word of advice, Durk: it’s the Mesolithic, we’ve domesticated the dog, we’re using stone tools and no one’s naked anymore.”
JCUH drugs
Prasugrel is used instead of clopidogrel on a patient by patient basis at operator discretion.
“A word of advice, Durk: it’s the Mesolithic, we’ve domesticated the dog, we’re using stone tools and no one’s naked anymore.”
Alternatively…
Aspirin loading 300mg (paramedic).
Prasugrel 60mg loading dose as routine (well recognised exceptions); potential for administration by ambulance crew.
Bivalirudin + bail out GpIIb/IIIa inhibitor.

In the cath lab.. escalation of care
• Not all PPCI is simple

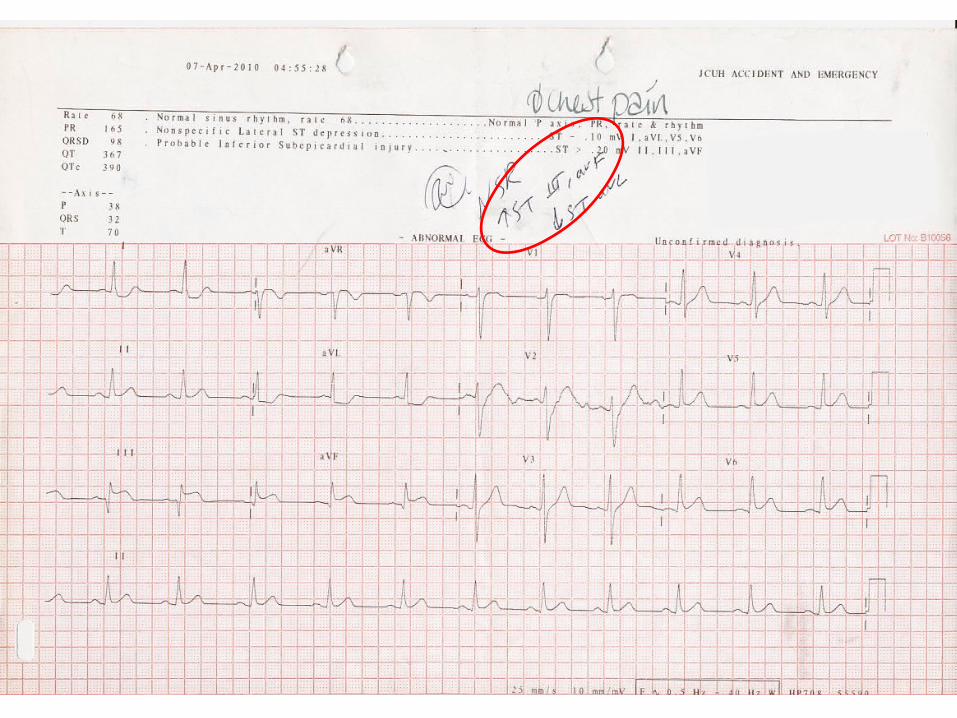
83F
Inferior STEMI
TIMI 2 flow
Critical prox RCA

Lesion uncrossablewith whole range of CTO balloons

Lesion successfully crossed with 2.1F Tornus device

Subsequent rotablation and stenting
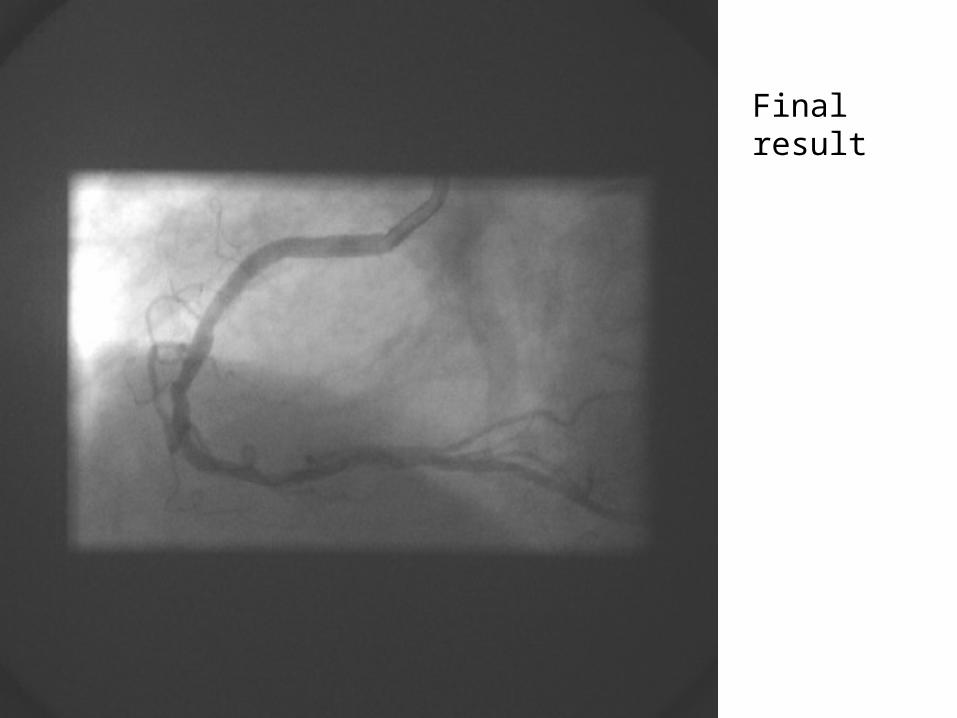
Final result
In the cath lab.. escalation of care
• Not all PPCI is simple
• Not all MI (or PPCI) is without complication

62M
Posterolateral STEMI
Severe pulmonary oedema requiring NIV and anaesthetic support
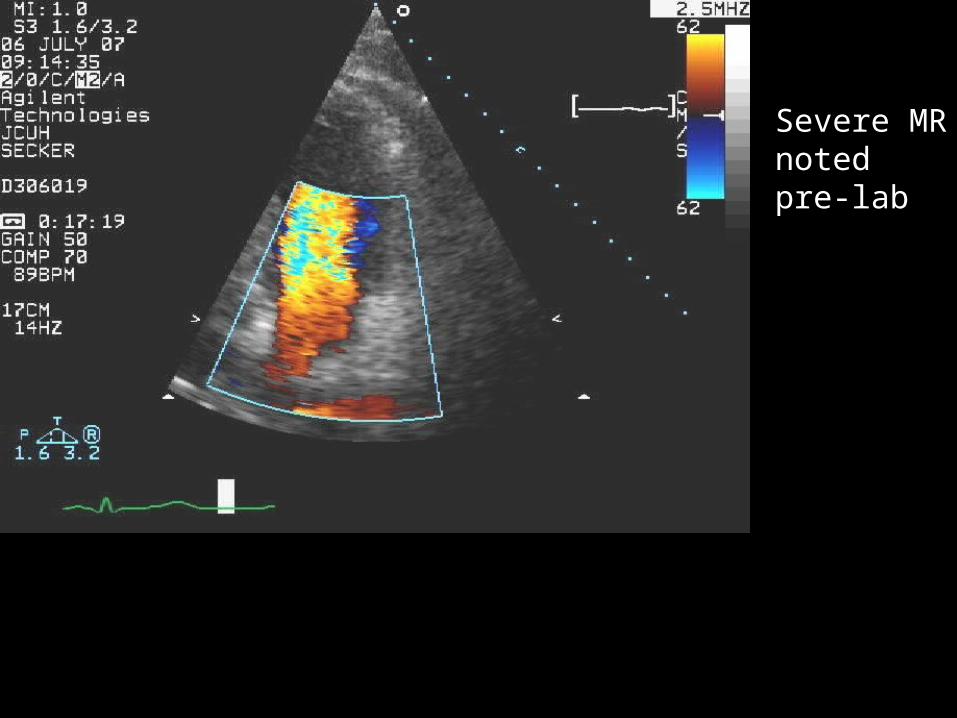
Severe MR noted pre-lab

Sub-total occlusion of Cx

Cx ballooned for ongoing pain
IABP

Urgent mechanical mitral valve replacement 90 minutes later
Complete recovery

77F
Inferior STEMI with CHB
Ostial LMS disease and calcified, severe LAD and Cx disease

Occluded RCA in calcified vessel

Vessel opened
Serial balloon inflations
TIMI 3 flow
Delivery of kit very difficult
No stent; planned urgent CABG
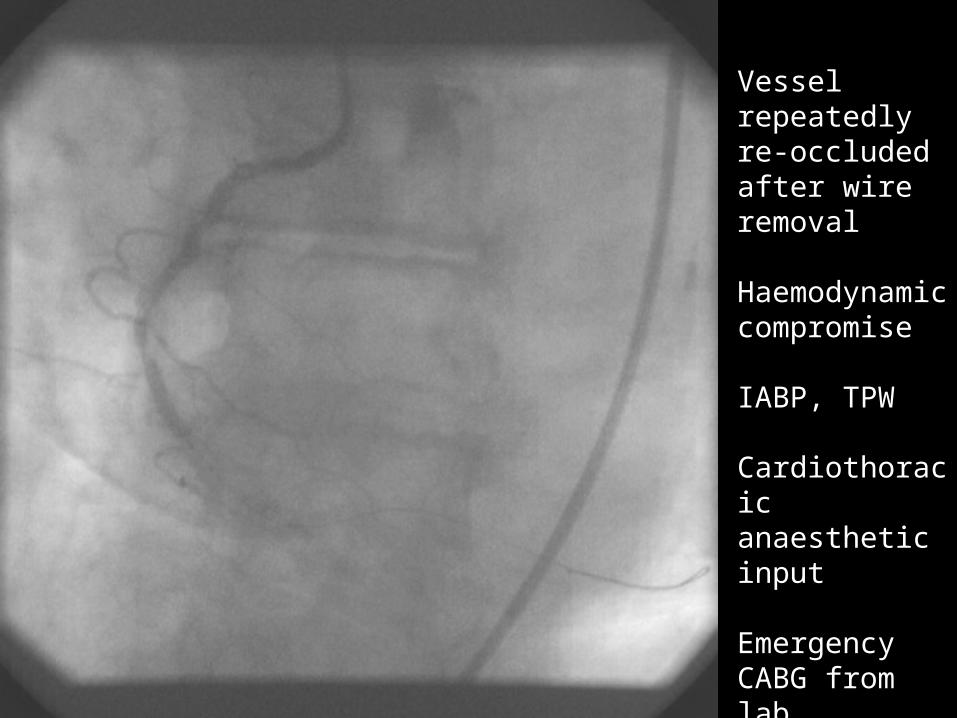
Vessel repeatedly re-occluded after wire removal
Haemodynamic compromise
IABP, TPW
Cardiothoracic anaesthetic input
Emergency CABG from lab

In the cath lab.. escalation of care
• Not all PPCI is simple
• Not all MI (or PPCI) is without complication
• ...which means you get some very sick patients

In the cath lab.. escalation of care• Infrastructure for the sickest group
must be in place

In the cath lab.. escalation of care• Infrastructure for the sickest group
must be in place– Input from experienced cardiothoracic
anaesthetists vital for some
In the cath lab.. escalation of care• Infrastructure for the sickest group
must be in place– Input from experienced cardiothoracic
anaesthetists vital for some– Provision for invasive ventilation– Provision for IABP
General ITU do not take these patients

In the cath lab.. escalation of care• Infrastructure for the sickest group
must be in place– Input from experienced cardiothoracic
anaesthetists vital for some– Provision for invasive ventilation– Provision for IABP– Provision for cooling
General ITU do not take these patients

In the cath lab.. escalation of care• Infrastructure for the sickest group
must be in place– Input from experienced cardiothoracic
anaesthetists vital for some– Provision for invasive ventilation– Provision for IABP– Provision for cooling– Provision for cardiothoracic surgical input
General ITU do not take these patients

The basics.... conclusion
Agreed regional protocol for delivery of PPCI
Mechanism in place for wherever the patient presents
Mechanism of continuous monitoring, audit and feedback
The basics.... conclusion
Agreed regional protocol on drugsStrategy for the PPCI which is not
simpleInfrastructure for those patients
requiring urgent anaesthetic and surgical input
