how to diagnose gdm - tau · how to diagnose gdm ? hadar eran, md helen schneider hospital for...
TRANSCRIPT
How to Diagnose GDM ?
Hadar Eran, MD
Helen Schneider Hospital for WomenRabin Medical Center & the Sackler Faculty of Medicine

Many Names & Organizations
Multiple Tests & Cutoffs
No Consensus
O’sullivan
Mahan
Screening
NDDG
Carpenter & Coustan
ACOG
ADA
NIH
IADPSG
OGTT GCT
Two Step
Screening
Diagnosis
Selective
Universal
Workshops
50g
75g
100g
HAPO
WHO
2

What is the Definition of GDM ?
• ADA 2006:
“Carbohydrate intolerance first diagnosed during pregnancy”
• ADA 2011:
“Carbohydrate intolerance first diagnosed during pregnancy, that is not overt diabetes”
3

4
The Evolution of the OGTT Cut-offs

O’sullivan & Mahan
• The foundation for GDM diagnosis (1964):• 100g OGTT was the routine diagnostic procedure for diabetes
• 2 SDs above fasting and challenged glucose for 752 pregnant women
• Compared to data of 1013 gestational and post partum OGTTs
• Abnormal OGTT outcome was post partum DM
• GDM Prevalence 1.99%
• Post Partum Diabetes 22.6%, within 8 years
O’Sullivan & Mahan. Criteria for oral glucose tolerance test in pregnancy. Diabetes 19645

6
O’sullivan & Mahan

O’sullivan & Mahan
Pre DiabetesT2DMFollow UPnReference
4%3%4-8w103Catalano 1991
--14%1-4m1636Shafer-Graf 2002
50%10%1-6m122Buchanan 1998
16%15%3-6m788Pallardo 1999
9%14%1-5y70Dalfra 2001
8%11%1-12y477Gran 1986
--29%4y395Kwak 2013
--50%5y671Kjos 1995
7

The Workshops
• Guidelines for GDM screening & diagnosis were presented at series of 5 workshops
• The basis is the O'sullivan & Mahan criteria with modifications
Carpenter & Coustan
NDDG
8Summary and recommendations of the 4th International Workshop-Conference on Gestational Diabetes Mellitus. Diabetes Care 1998Summary and recommendations of the 5th International Workshop-Conference on Gestational Diabetes Mellitus. Diabetes Care 2007

National Diabetes Data Group(NDDG,1979)
• O'sullivan & Mahan’s measurements:• Preformed in venous whole blood
• Analyzed by Somogyi-Nelson technique
• NDDG is a conversion to plasma or serum measurements
• Rounded O’Sullivan values Increased by ~15%
National Diabetes Data Group. Classification and diagnosis of diabetes mellitus and categories of glucose intolerance. Diabetes 1979 9

National Diabetes Data Group(NDDG,1979)
10

Carpenter & Coustan(C&C, 1982)
• Second set of thresholds derived from O’Sullivan and Mahan
• Universal change in laboratory methods:Somogyi-Nelson Enzymatic method (Glucose Oxidase)
• -5mg/dL decrease from O'sullivan to C&C values
• +14% increase for the change from whole blood to plasma
Carpenter & Coustan: Criteria for screening tests for gestational diabetes. AJOG 198211

Carpenter & Coustan(C&C, 1982)
Carpenter & Coustan: Criteria for screening tests for gestational diabetes. AJOG 198212

The Organizations: ACOG, ADA
• Endorse suggested diagnostic criteria & establish diagnostic procedures & cutoffs.
• Recommendations for: Risk Assessment
Selective/Universal screening
75 / 100g Glucose load
ADA2009
ACOG2001
Gestational Diabetes. ACOG practice bulletin No.30. Obstet Gynecol 2001American Diabetes Association. Diagnosis and classification of diabetes mellitus (Position Statement). Diabetes Care 2009
13

The Organizations: WHO
• WHO endorsed a different set of criteria (1999)
• Based on classification of impaired glucose tolerance innon-pregnant population
• 75g OGTT: Fasting and 2h glucose
World Health Organization: Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications. 1999 14
mmol/Lmg/dl75g OGTT
6.1-6.9110-125Fasting
7.8-11140-1992 Hour

What are the “Current” Guidelines ?
15

Risk Assessment, Screening, Diagnosis
• GDM risk assessment at 1st prenatal visit
• Screening for GDM:• None
• Selective: Depending upon risk factors
• Universal: For all pregnant women
• The Screening tool is a 50g glucose challenge test (GCT):• One hour, No Fasting, Plasma Glucose
• The diagnostic tool is an oral glucose tolerance test (OGTT):• 75/100g load and various cutoffs
16

Risk Assessment
• Every year > 25 4% increase in the risk for GDM:• Age <20 years: <1%
• Age 20–30 years: 2%
• Age >30 years: 8–14%
• 25% of women with GDM Positive family history
• BMI >30 Vs. <20kg/m2 3-fold increase in GDM incidence
• Ethnicity (Vs. Caucasians):• Asians 5-fold
• Hispanic , African-American 2-2.5 fold
17
Hanna et al. Screening for gestational diabetes. Diabet Med 2002Rodriguez et al. Prevalence of GDM among James Bay Cree women. CMAJ 1999
Dooley et al. GDM disease prevalence and perinatal outcome. Diabetes 1991

Screening & Diagnosis: Low Risk
18
Blood glucose testing not required if all is true:
HispanicAfricanNative AmericanAsianPacific Island
Not from a high prevalence ethnicity
No known diabetes in first-degree relatives
Age < 25 years
Normal Pre-Pregnancy Weight
Normal Weight at Birth
No history of abnormal glucose metabolism
IUFD, MacrosomiaNo history of poor obstetric outcome

• Only 10% of the population are low risk
• About 3% of the GDMs will not be diagnosed
Danilenko & Dixon. Universal versus selective gestational diabetes screening. AJOG 1997
Screening & Diagnosis: Low Risk

Screening & Diagnosis: Average Risk
20
Perform blood glucose testing at 24–28 weeks:
50g GCT ScreeningIf positive 100g OGTT
Two-step
100g OGTT on all subjectsOne-step

Screening & Diagnosis: High Risk
21
Blood glucose testing as soon as feasible (1 or 2 steps)
BMI > 35Kg/m2Severe obesity
Family history of T2DM
GDMImpaired glucose metabolismGlucosuria
Previous history of:
If GDM is not diagnosed Repeat testing at 24–28w
or if suggestive signs and symptoms occur

How to choose the GCT cutoff ?
GDM / T2DM Prevalence
High
Low
Low Cutoff Sensitivity ↑
High Cutoff Cost / Effect ↑
22

What is the cutoff for the GCT ?Screen Positive Rate
• The cut-off for a positive screening test:• 130mg/dl 23-25% screen positive
• 140mg/dl 15% screen positive
23
Screen PositiveCut Off
23-25%130mg/dl
15%140 mg/dl
O’Sullivan et al. Screening criteria for high risk gestational diabetic patients. AJOG 1973Coustan et al. Maternal age and screening for gestational diabetes. Obstet Gynecol 1989
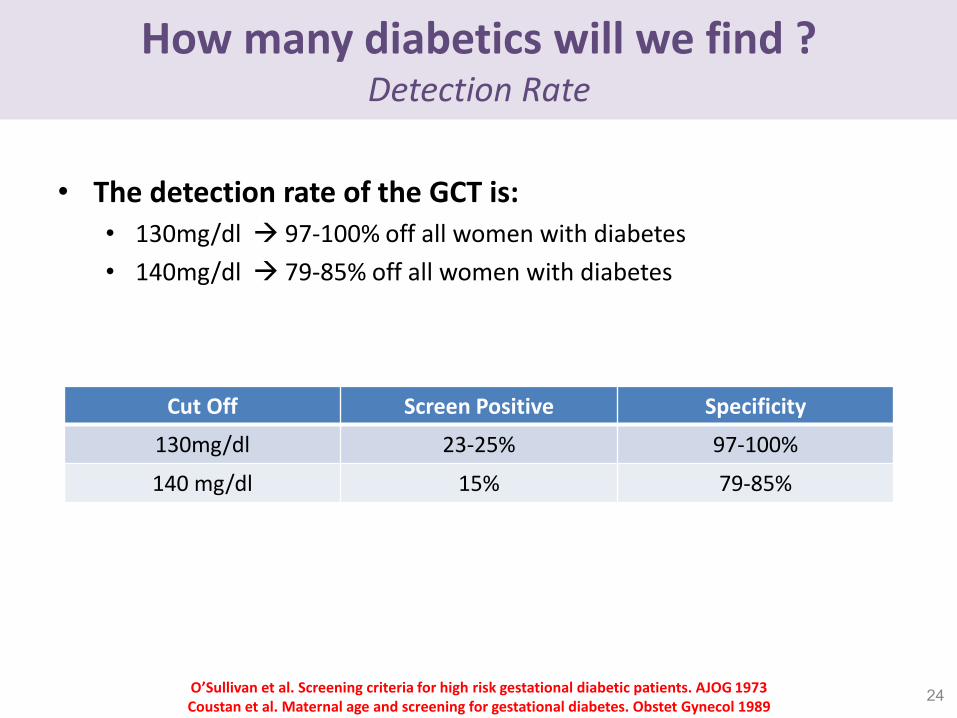
How many diabetics will we find ?Detection Rate
• The detection rate of the GCT is:• 130mg/dl 97-100% off all women with diabetes
• 140mg/dl 79-85% off all women with diabetes
24O’Sullivan et al. Screening criteria for high risk gestational diabetic patients. AJOG 1973Coustan et al. Maternal age and screening for gestational diabetes. Obstet Gynecol 1989
SpecificityScreen PositiveCut Off
97-100%23-25%130mg/dl
79-85%15%140 mg/dl
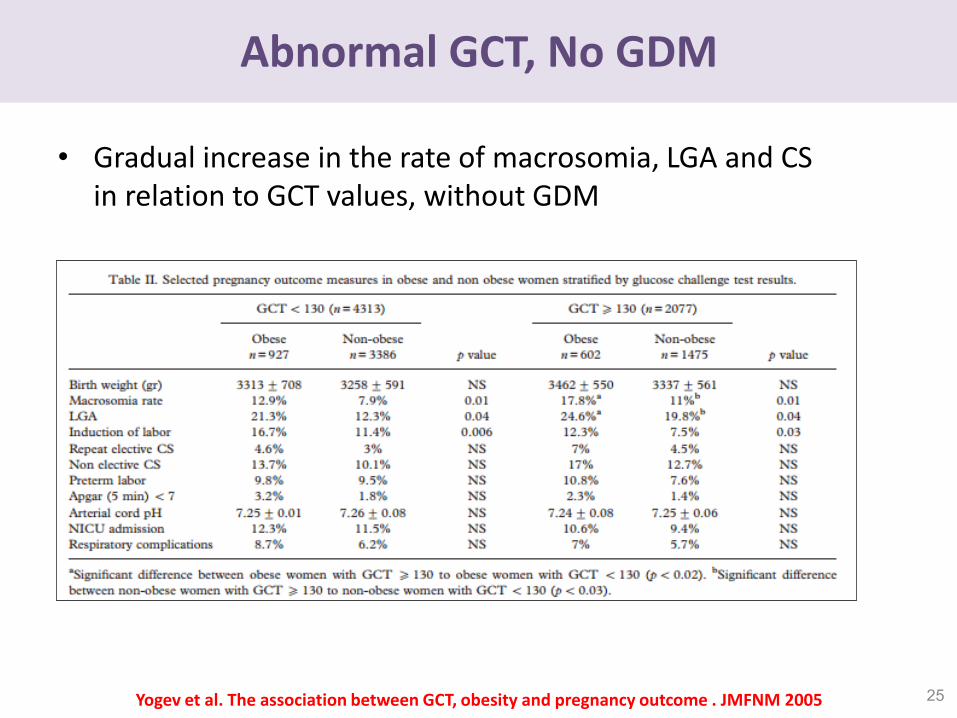
Abnormal GCT, No GDM
• Gradual increase in the rate of macrosomia, LGA and CSin relation to GCT values, without GDM
25Yogev et al. The association between GCT, obesity and pregnancy outcome . JMFNM 2005

How to Perform an OGTT ?
• 3 days of unrestricted diet of at least 150g/d Carbohydrate+ physical activity
• Overnight fasting (8-14hr), No smoking, Seating
• If 2/4 OGTT values abnormal GDM• Carpenter & Coustan criteria
• National diabetes data group criteria
• Alternatively….many more criteria:• WHO criteria (1/2 abnormal values of a 75g OGTT)
• ADA Criteria (2/3 abnormal values of a 75g OGTT)
• UK, Canada, Australia, Germany….
26

OGTT Cutoffs
27
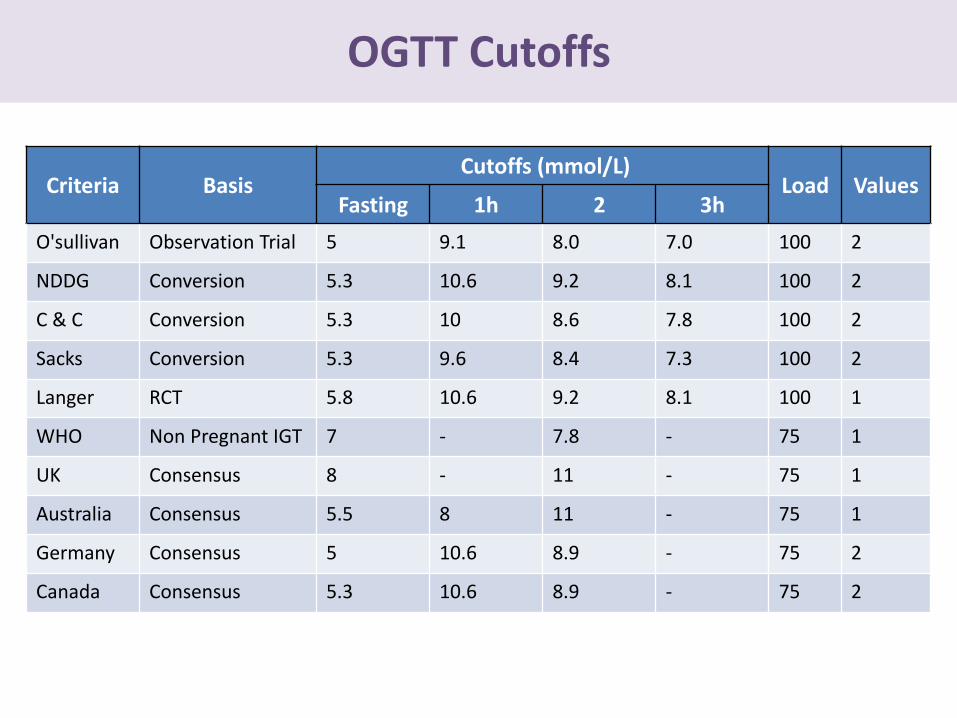
OGTT Cutoffs
Criteria BasisCutoffs (mmol/L)
Load ValuesFasting 1h 2 3h
O'sullivan Observation Trial 5 9.1 8.0 7.0 100 2
NDDG Conversion 5.3 10.6 9.2 8.1 100 2
C & C Conversion 5.3 10 8.6 7.8 100 2
Sacks Conversion 5.3 9.6 8.4 7.3 100 2
Langer RCT 5.8 10.6 9.2 8.1 100 1
WHO Non Pregnant IGT 7 - 7.8 - 75 1
UK Consensus 8 - 11 - 75 1
Australia Consensus 5.5 8 11 - 75 1
Germany Consensus 5 10.6 8.9 - 75 2
Canada Consensus 5.3 10.6 8.9 - 75 2

What about a single Abnormal OGTT?
• The use of one abnormal value OGTT is controversial
• Supported by Pathophysiology and some Evidence:• Glucose is a continuous measure
• Mild hyperglycemia is associated with adverse outcome
• Glucose intolerance related to:Macrosomia, CS, PET, NICU
29
Sermer et al. The Toronto Tri-Hospital GDM Project. AJOG 1995Jensen et al. Clinical impact of mild carbohydrate intolerance in pregnancy. AJOG 2001
Leikin et al. Abnormal glucose screening tests in pregnancy. OG 1987Mello et al. Risk factors for fetal macrosomia. Eur J Endocrinol 1997
Tallarigo et al. Relation of glucose tolerance to complications of pregnancy. NEJM 1986.

What about a single Abnormal OGTT?
• Fasting insulin, insulin resistance , glucose profiles: Similar in patients with one abnormal OGTT vs. GDM
• Patients with one abnormal OGTT, if retested 4 week later 34% found with ≥ 2 abnormal values
• Neonatal morbidity(Obesity, Hyperinsulinemia, Hypoglycemia, Hyperbilirubinemia, Polycythemia)
Associated to one abnormal OGTT
• Adverse Pregnancy Outcome(LGA, Macrosomia, PET, CS)
Associated to one abnormal
30
Ergin et al. IIsulin secretion in patients with one abnormal OGTT. AJOG 2002
Schaefer-Graf et al. Infants born to women with one abnormal OGTT value. J Perinat Med 1988
Lindsay et al. The relationship of one abnormal OGTT and pregnancy complications. OG 1989.
Gorest et al. OGTT: The significance of one abnormal value. Clin Biochem 1994
Forest et al. Glucose tolerance test during pregnancy. Clin Biochem 1994

What about a single Abnormal OGTT?
• Untreated (One Abnormal) Vs. Treated and Non-GDM Higher rate of adverse outcome in the Untreated
31Langer et al. Significance of one abnormal OGTT on adverse outcome in pregnancy. AJOG 1987
0
5
10
15
20
25
30
35
Macrosmia LGA Ponderal Index MetabolicComplications
RespiratoryComplications
Shoulder Dystocia CS Rate
One Abnormal OGTT (425)
Treated (850)
Non-GDM (850)
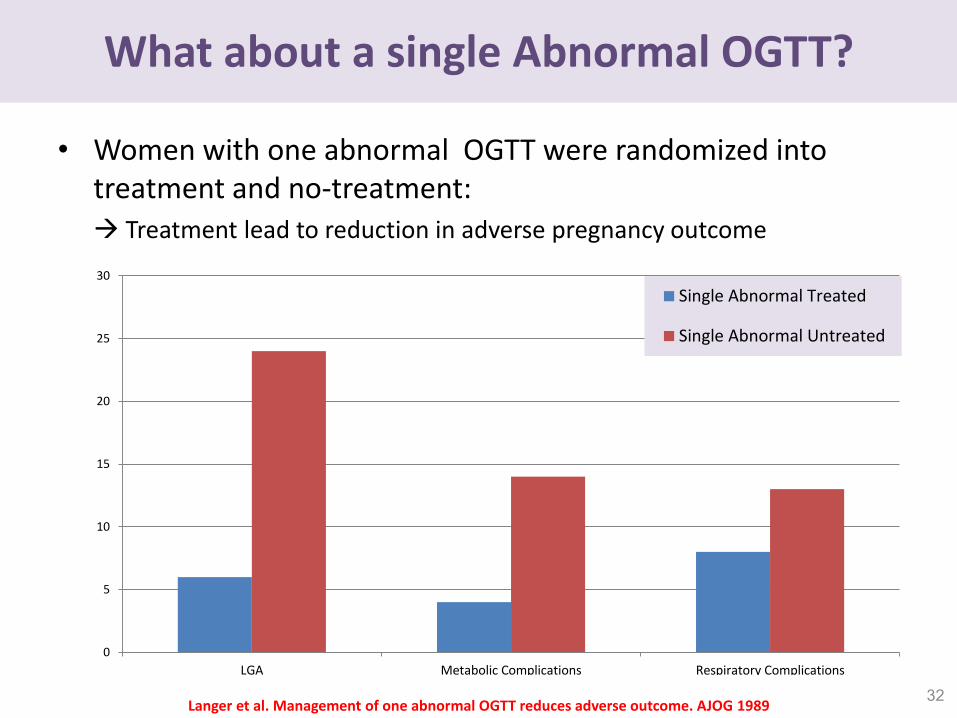
What about a single Abnormal OGTT?
• Women with one abnormal OGTT were randomized into treatment and no-treatment: Treatment lead to reduction in adverse pregnancy outcome
32Langer et al. Management of one abnormal OGTT reduces adverse outcome. AJOG 1989
0
5
10
15
20
25
30
LGA Metabolic Complications Respiratory Complications
Single Abnormal Treated
Single Abnormal Untreated

Can we diagnose Overt Diabetes during pregnancy ?
• Remember the definition:• 2006: “Carbohydrate intolerance first diagnosed during pregnancy” • 2011: “Carbohydrate intolerance first diagnosed during pregnancy,
that is not overt diabetes”
• Women with fasting hyperglycemia <24w had pregnancy outcomes similar to those for women with overt diabetes
(Shuffield 1999, Bartha 2000, Most 2009)
• Early fasting hyperglycemia is almost invariably overt diabetes
33

The HAPO Study
HAPO Study Cooperative Research Group: Hyperglycemia and adverse pregnancy outcomes. N Engl J Med. 200834

HAPO Study
• Prospective, observational, multinational, blinded study:• 2-hour 75g OGTT during 24-28 weeks of gestation
• Caregivers and participants blinded to the results
• Unblinded if hypoglycemia or overt diabetes detected
• ~25,000 women
• 7 Years, 15 Centers, 9 Countries
35

HAPO Study
• A linear association between increasing levels of fasting, 1 and 2 hour plasma glucose post a 75g OGTT to all outcomes:
• Primary: Birth weight > 90th percentile
Cord blood C-peptide > 90th percentile
Primary cesarean delivery
Clinical neonatal hypoglycemia
• Secondary: Premature delivery
Preeclampsia
Shoulder dystocia or birth injury
NICU admission
Hyperbilirubinemia36

HAPO Study
37

38IADPSG recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010

IADPSG: 1st Prenatal visit
• At the first prenatal visit, all (universal) or only high-risk (selective) women should be tested for:• Fasting plasma glucose (FPG)
• Glycosylated hemoglobin (HbA1C)
• Random plasma glucose (RPG)
High RiskLow Risk
Pre-pregnancy obesityNo diabetes in 1st degree relatives
Family history of T2DMAge <25 years
GDM in a prior pregnancyNormal pre-pregnancy weight
Known carbohydrate intolerance or glucosuria
No history of poor carbohydratemetabolism
No history of adverse pregnancy outcome
39

IADPSG: 1st Prenatal visit
40
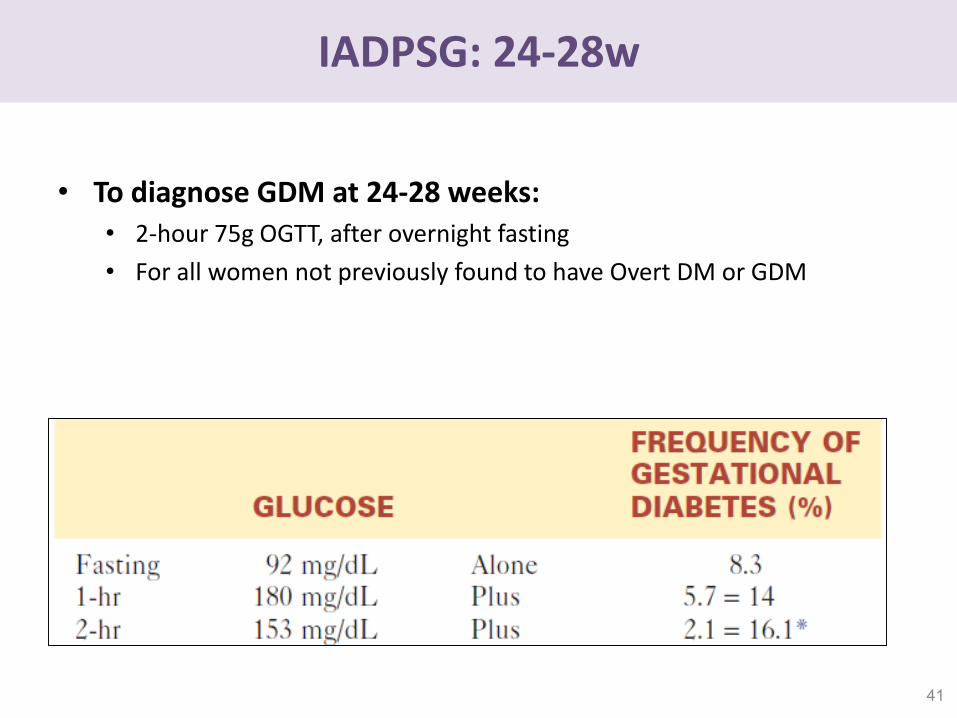
IADPSG: 24-28w
• To diagnose GDM at 24-28 weeks:• 2-hour 75g OGTT, after overnight fasting
• For all women not previously found to have Overt DM or GDM
41

IADPSG: 24-28w
42

Early GDM and Overt Diabetes During 1st trimester
• Women with overt diabetes, were undiagnosed prior to IADPSG criteria
• IADPSG allows for the diagnosis of early GDM and overt diabetes
• However:• This is expert opinion
• No data to support that treatment of early GDM, improves outcome
• Both universal and selective testing are optional
• Timing for testing: “during the first prenatal visit”
43
How to choose the outcome?
• Linear association without a cutoff:
Until now: post partum T2DM
What? Birth weight > 90th percentile (LGA)Cord C-peptide > 90th percentileBody fat percentage above 90th percentile
Why? Strongest association to glucoseFactors of the diabetic fetopathy
44

How to choose the outcome?Yes for LGA
• LGA and Macrosomia are correlated to gestational hyperglycemia
• HAPO LGA babies are at an increased risk for:CS & neonatal hypoglycemia
• LGA independently associated with other adverse outcome:• Neonatal adiposity
• Fetal hyperinsulinemia
• Birth trauma
45
Coustan. JAMA 1996Langer et al. AJOG 2005iss et al. BJOG 2000Zhang AJOG 2008Yang et al. Diabetes Care 2002Jang et al. Diabetes Care 1997Boulet et al. AJOG 2003Esakoff TF et al. AJOG 2009Carpenter et al. AJOG 1982

How to choose the outcome?No for LGA
• It is questionable whether LGA is a clinically relevant endpoint
• Does LGA has a long term metabolic effect ? Only a long term follow up of the HAPO population will answer this
• Is there proof that treatment of will result in benefits ? No
• Why not choosing other endpoints ?Modest risk ratio, non discriminatory between healthy to GDM
46

How the set the odds ratio?
• 1.75 odds ratio was chosen :“The glucose values at which odds for selected outcomes reached 1.75
times the estimated odds of these outcomes at mean glucose values”
47
Threshold Values for diagnosis of GDM at OR=1.75
Glucose Measure Glucose Threshold
Mmol/L mg/dl
Fasting Plasma Glucose 5.1 92
1 Hour Post 75g OGTT 10.0 180
2 Hour Post 75g OGTT 8.5 153

How the set the odds ratio? Why not 2
48Ryan et al. Diagnosing gestational diabetes. Diabetologia 2011
OR=1.75 OR=2.0
GDM (n) 4150 2448
GDM Rate 16.1% 8.8%
LGA 140
Shoulder Dystocia 21
Birth Injury 16

How it will impact prevalence ?
• Implementing the IADPSG criteria on the HAPO population:• Average GDM prevalence: 18% (Range 10 - 25%)
• Other populations: 12 - 37%
• Is it “the criteria” or the“anticipated increase” in theprevalence of T2DM?
49

Is there a benefit for the newly diagnosed?Yes
50
Landon 2009 Crowther 2005
Criteria For TX FPG < 95 IGT
PET
LGA
Shoulder Dystocia -
CS Rate 27 34% 31 32%
Serious Complications NS NNT=34

Is there a benefit for all the newly diagnosed?No
51Bodmer-Roy et al. Pregnancy Outcomes in Women With and Without GDM according to IADPSG Criteria. Obstet Gyncol 2012
IADPSG+ Non-GDM

52
Where do we stand ?

ADA, WHO,FIGO: For the IADPSG Criteria
53

FIGO Initiative
54

ACOG: Against
55

Israel MOH
56
ללא , להיריון28-24לכלל אוכלוסיית הנשים ההרות בשבועות ( GCT)גלוקוז גרם 50להציע בדיקת סקר של העמסת יש •
.לבדיקהצורך בהנחיות צום או בדיאטה מיוחדת קודם
.בפלזמהגרם גלוקוז תימדד רמת הגלוקוז 50לאחר שתיית שעה •
(OGTT)האבחנתית יחייב לבצע בהקדם האפשרי את הבדיקה ( ל"ד/ג"מ)מיליגרם לדציליטר 140-של מעל לערך •
לאחר -שעתיים ושלוש שעות , שעות יימדדו ערכי הגלוקוז בפלזמה בצום ושעה14-8צום של לאחר , OGTTבבדיקת •
. ההעמסה
.בהתאמהל"ד/ג"מ140-ו155, 180, 95הגלוקוז יוגדרו כפתולוגיים מעל ערכי •
.בבדיקהסוכרת הריונית תיעשה במידה ושני ערכים יימצאו פתולוגיים אבחנת •
סוכרת בהיריון קודם או לידה בעבר , גיל מבוגר, השמנת יתר)של ערך אחד פתולוגי וגורמי סיכון נוספים במקרים •
.גבוהיש לשקול הפנייה למרפאה להיריון בסיכון ( גרם4000מעל
גרם 4500עם סוכרת הריונית בהריונות קודמים ובנשים עם לידה בעבר של יילוד מעל בנשים , (BMI>30)שמנות בנשים •
. ללא בדיקת סקר( OGTT)יש להמליץ על ביצוע הבדיקה האבחנתית -
ל"ד/ג"מ200או בדיקת גלוקוז אקראית של , ל"ד/ג"מ125גלוקוז בצום מעל , GCT-בל"ד/ג"מ200של מעל תוצאה •
.האבחנהואין צורך לבצע בדיקות נוספות לאישור , סוכרת הריוניתמגדירות , ומעלה
אלא רק בבדיקת רמות גלוקוז , (גלוקומטר)בדיקות הסקר והאבחנה אין להשתמש במכשירי ניטור גלוקוז ביתיים לצורך •
. בפלזמה