how can we personalize rt as part of breast-conserving...
TRANSCRIPT
How can we Personalize RT
as part of
Breast-Conserving Therapy?
Jay R. Harris
Dana-Farber Cancer Institute (DFCI)
Brigham and Women’s Hospital (BWH)
Harvard Medical School

Disclosures
I have no COI disclosures

Current Results with BCT
• Our results from DF/BWCC and MGH
are illustrative of the current
excellent results seen with BCT
• Our initial results* were also the first
to illustrate the importance of
biologic subtypes in BCT
* Nguyen P et al JCO 2008
Nguyen P et al JCO 2008
• Approximated biologic subtype
using standard markers was the
only variable in the final model
• No other variables, including
margins, dose, grade, stage and
age were in the final model

Our Updated Experience
• 1434 BCT patients
• T1 80%, pN0 67%
• Margins: Negative 89%, close 8%
• ST used in 91% (No Herceptin)
• Median FU = 85 months (7.1 years)
• 5-year rate of LR = 2.1%!
Ref: Arvold N et al JCO 2011 29:3885
New Definitions of Subtypes
• Luminal A = HR+, HER2-, Gr 1-2 (905)
• Luminal B = HR+, HER2-, Gr 3 (198)
• Luminal-HER = HR+, HER2+ (105)
• HER2 = HR-, HER2+ (55)
• Triple Negative = HR-, HER2- (171)
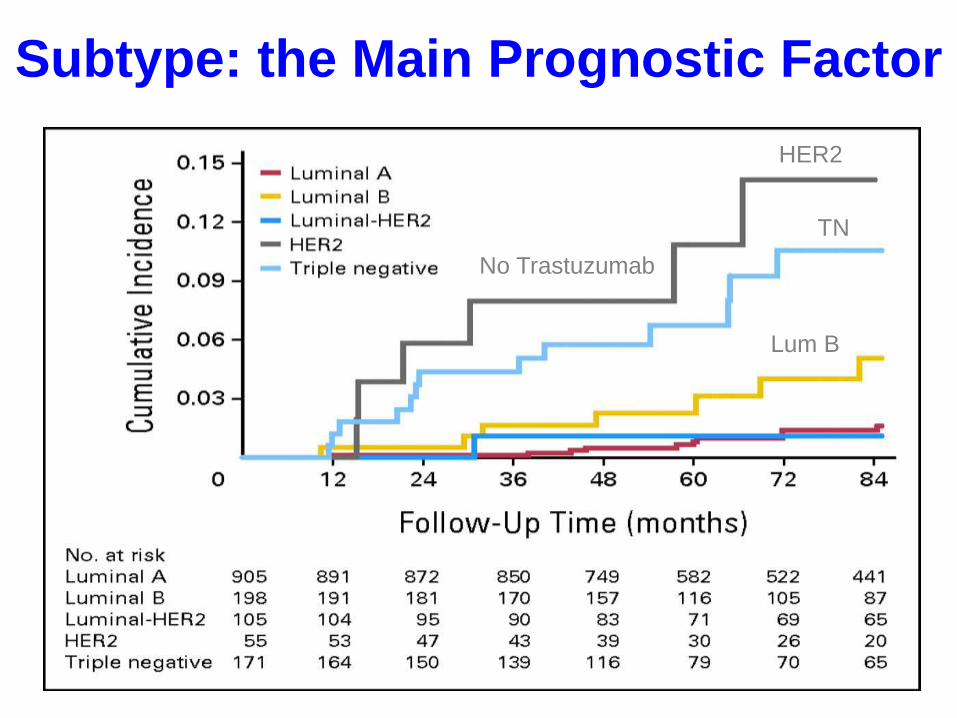
Subtype: the Main Prognostic Factor
HER2 (No Herceptin)
Triple -
Lum B
Lum A
Lum-HER2
No Trastuzumab
HER2
TN
Lum B

Age is also Prognostic (note scale)
< 47
47- 55
56 - 64
> 64
Age 23-46
Age 47-54
Conclusions
• New definition of subtype is useful
• Both subtype and to a lesser extent
age are prognostic for LR
• LR rates are much lower than in the
past
Reasons for Excellent Outcomes
• Better imaging with mammography
(not MRI); use of MRI controversial
• Better evaluation of the resected
breast specimens, especially margins
• Use of systemic therapy (ST), which
greatly improves results of RT

10-Year LR in NSABP Trials (Ref: Anderson SJ et al. JCO 2005, 27: 2466)
Trial ER
Status
10-Year
LR (%)
B-13 No Chemo - 13.3
B-13 Chemo - 3.5
B-14 No Tamoxifen + 11.0
B-14 Tamoxifen + 3.6
B-19 Chemo - 6.5
B-20 Tam +/- Chemo + 4.7
B-23 Chemo - 4.3
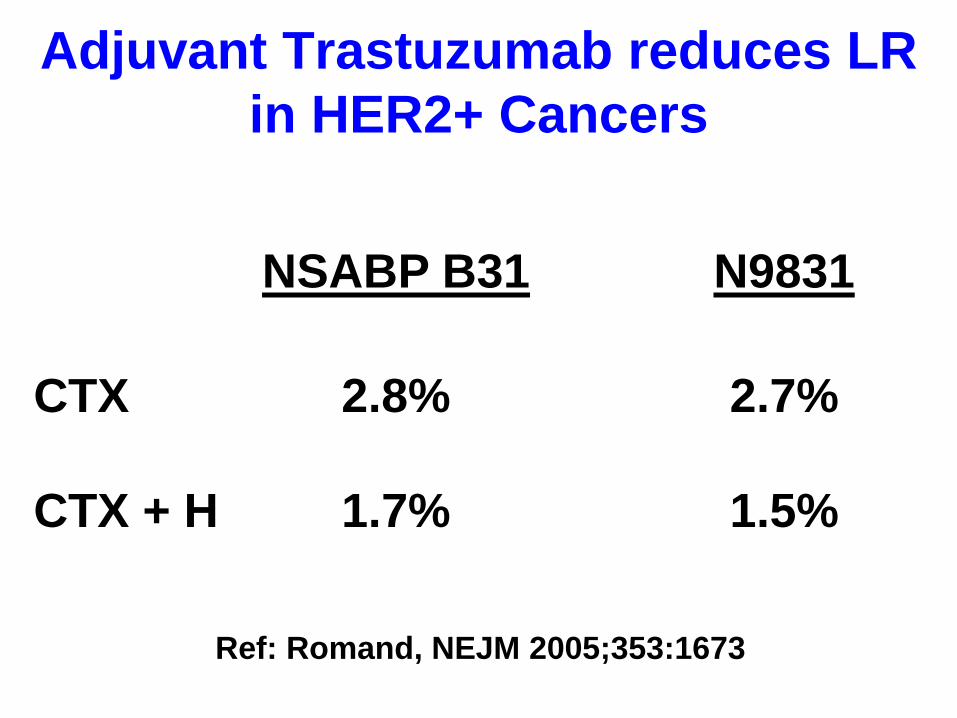
Adjuvant Trastuzumab reduces LR
in HER2+ Cancers
Ref: Romand, NEJM 2005;353:1673
NSABP B31 N9831
CTX
CTX + H
2.8%
1.7%
2.7%
1.5%
Is Bigger Surgery Better for
Triple Negative Breast Cancer?
• Studies from Canada, MSKCC and MD Anderson have shown that if anything LR is lower with BCT than with mastectomy
• Abdulkarim B, JCO 2011;29:2852
Ho A et al, Cancer 2012;118:4944
Adkins F et al, Ann Surg Oncol 2011;18:3164

Conventional Fractionation
• 45-50 Gy WB with boost to 60 Gy
• With long-term FU, shown to be safe
and effective
• However, there is growing interest in
hypofractionated breast RT
Rationale for Hypofractionation
• Convenience and Cost
• Major improvements in RT delivery
with higher energies, 3-D dose
calculation and beam modulation ->
much greater 3-D dose homogeneity
• More refined radiobiologic estimate
of dose equivalence

Major 1st Generation Trials
Canadian Start A UK* Start B UK
# Pts 1234 2236 2215
Med
FU
12 yrs 9.3 yrs 9.9 yrs
Arms
(Gy x
# Fx)
2 x 25 in 5
wks
2.66 x 16 in
3+ wks
2 x 25 in 5 wks
3 x 13 in 5 wks
3.2 x 13 in 5
wks
2 x 25 in 5
wks
2.66 x 15 in 3
wks
* Trial performed to determine α/β Ratio

Major 1st Generation Trials
Canadian Start B UK
# Pts 1234 2215
Arms
(Gy x # Fx)
2 x 25 in 5 wks
2.66 x 16 in 3+
wks
2 x 25 in 5 wks
2.66 x 15 in 3 wks
Use of a
Boost
Not Allowed Allowed
(Used in half)
Major 1st Generation Trials
• The Canadian Trial with 12 years of
FU was practice-changing in the US
• Updated results of the START trials
were published in Lancet Oncol in 2013
• Together, they provide justification
for increased use of hypofractionation
Refs: Whelan T et al NEJM 362:513, 2010
Haviland J et al Lancet Oncol 14: 1086, 2013
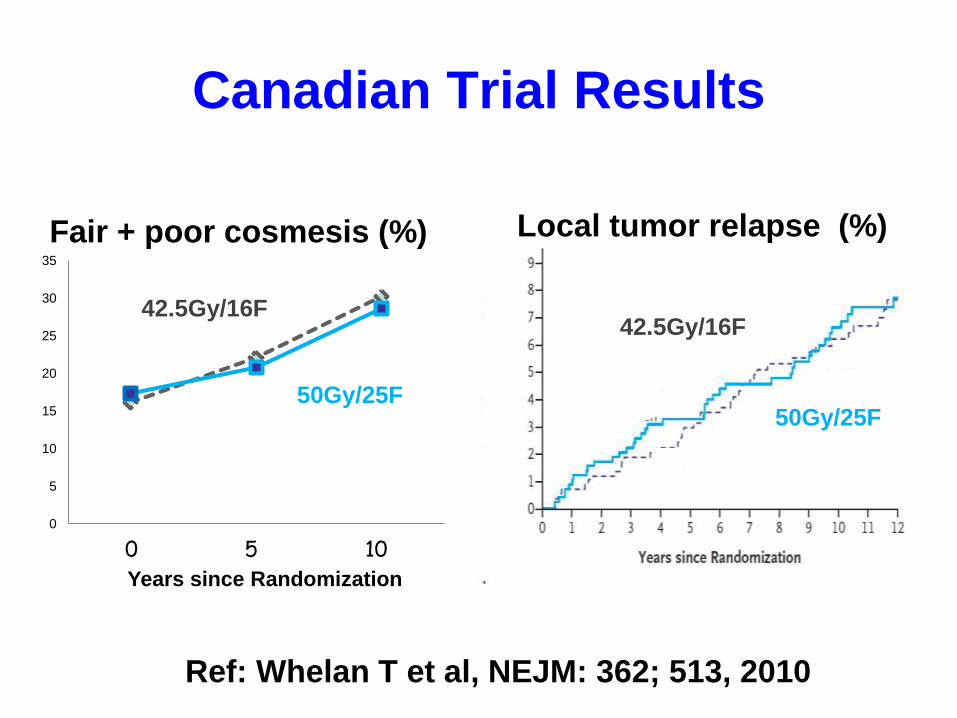
Ref: Whelan T et al, NEJM: 362; 513, 2010
0
5
10
15
20
25
30
35
1 2 3
15F 25F 0 5 10 Years since Randomization
42.5Gy/16F
Fair + poor cosmesis (%)
50Gy/25F
42.5Gy/16F
Local tumor relapse (%)
Canadian Trial Results
50Gy/25F
Time from randomization (years)
Rate of local tumor relapse
0
0.01
0.02
0.03
0.04
0.05
0.06
0.07
0.08
0.09
0.1
0 1 2 3 4 5 6 7 8 9 10
50 Gy
40 Gy
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10
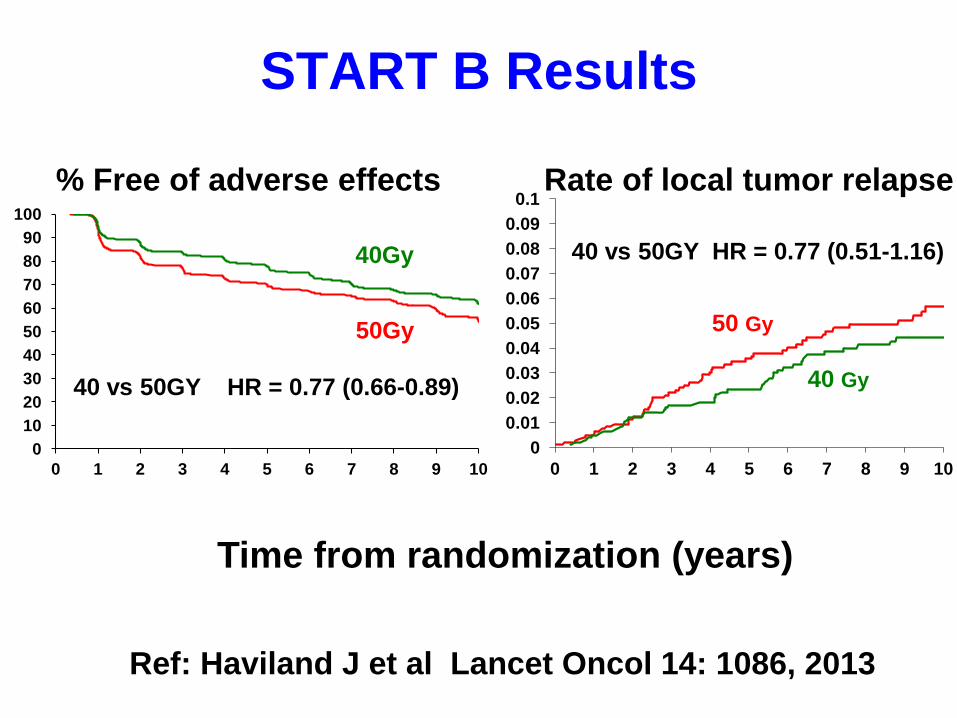
% Free of adverse effects
40Gy
50Gy
START B Results
40 vs 50GY HR = 0.77 (0.66-0.89)
40 vs 50GY HR = 0.77 (0.51-1.16)
Ref: Haviland J et al Lancet Oncol 14: 1086, 2013
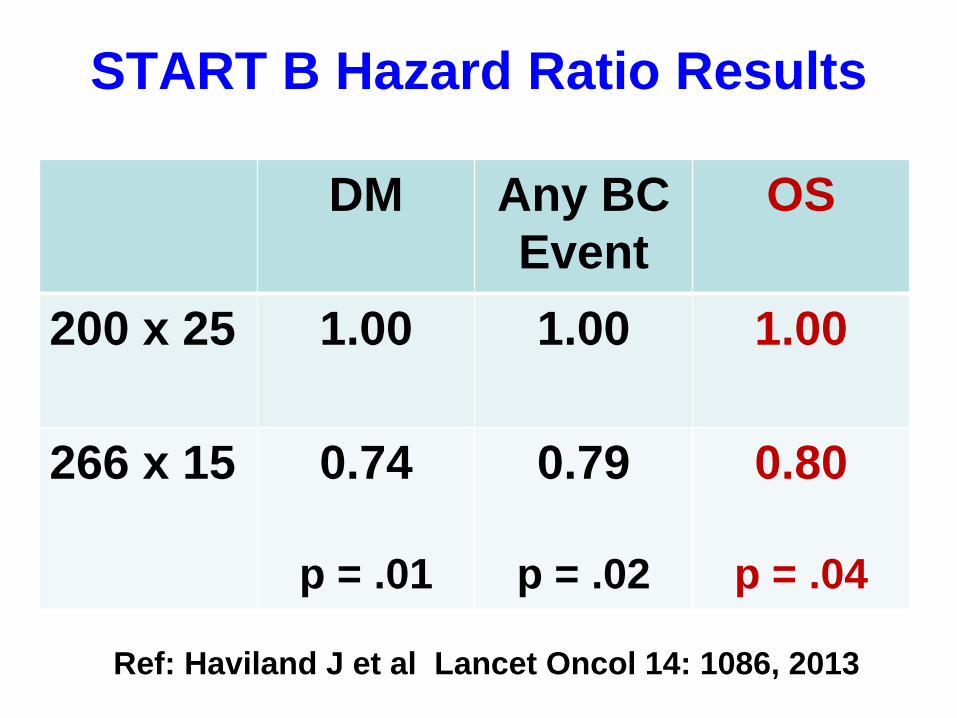
START B Hazard Ratio Results
Ref: Haviland J et al Lancet Oncol 14: 1086, 2013
DM Any BC
Event
OS
200 x 25 1.00 1.00 1.00
266 x 15 0.74
p = .01
0.79
p = .02
0.80
p = .04
Concerns/Uncertainties
• Potential effects on late-responding
normal tissue (late toxicity) -> need
long-term follow up
• ? Interaction with systemic
therapies, especially chemotherapy
• Patient selection – which patients?
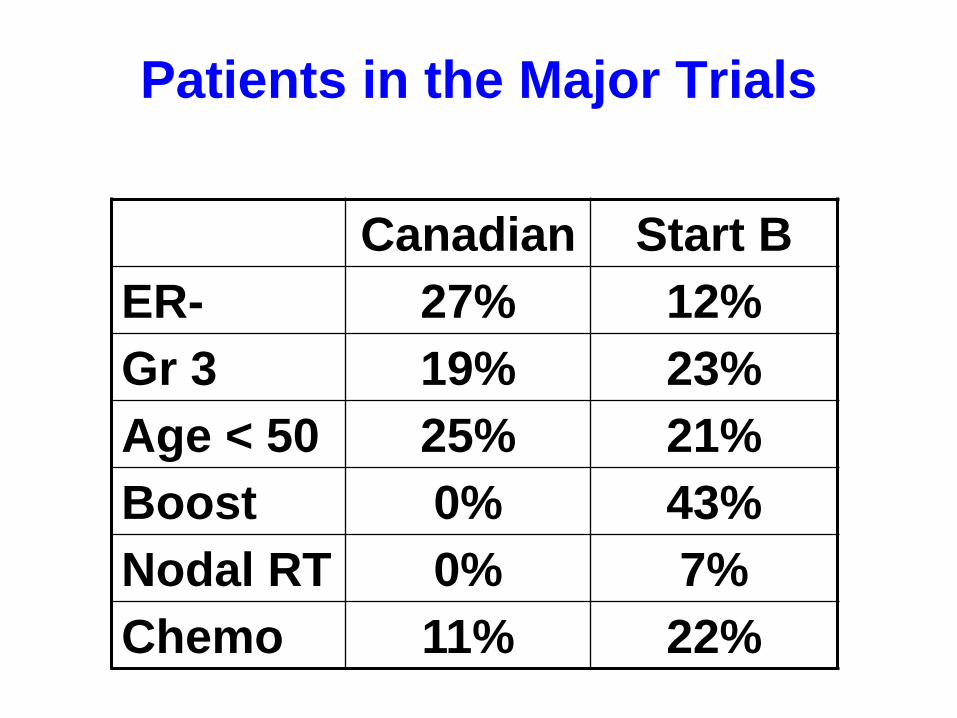
Patients in the Major Trials
Canadian Start B
ER- 27% 12%
Gr 3 19% 23%
Age < 50 25% 21%
Boost 0% 43%
Nodal RT 0% 7%
Chemo 11% 22%
Generalizability of these Results
• Patients in the these trials were older
with favorable cancers
• Chemotherapy and boost not routine
• However, in START B, cosmetic
results were the same with and
without chemotherapy
Case: Need for Long FU
• 1981 BK presents with T1N0 cancer
treated with BCT including nodal RT
• 2001 (20 yrs later) She develops
numbness of right hand; no evident
recurrence -> Dx brachial plexopathy
• 2001-> present Progressive loss of
motor function to ‘useless’ arm
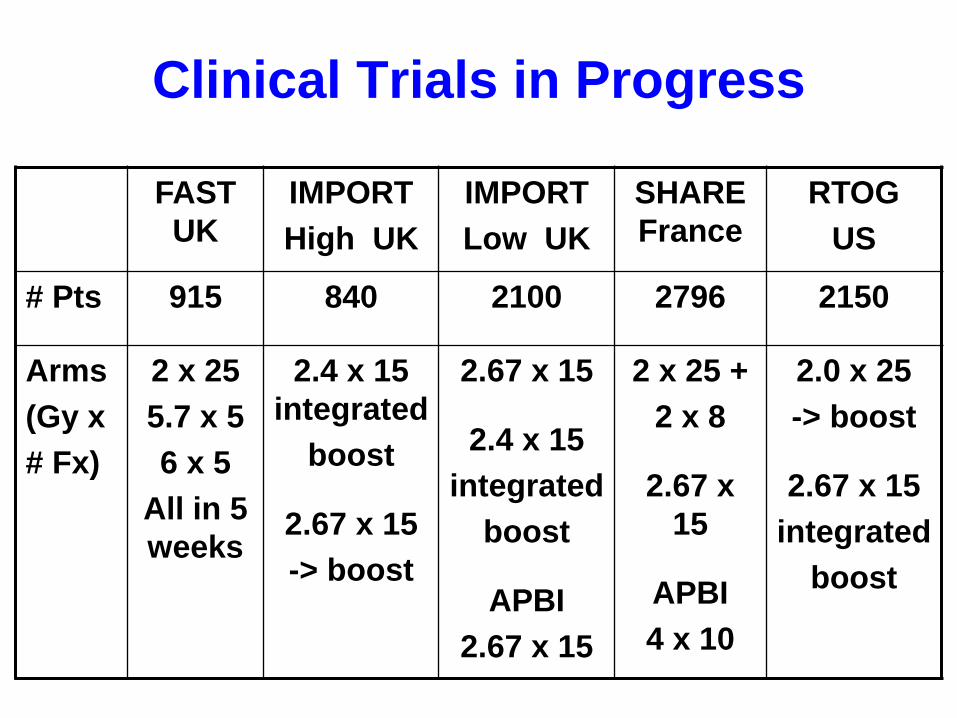
Clinical Trials in Progress
FAST
UK
IMPORT
High UK
IMPORT
Low UK
SHARE
France
RTOG
US
# Pts 915 840 2100 2796 2150
Arms
(Gy x
# Fx)
2 x 25
5.7 x 5
6 x 5
All in 5
weeks
2.4 x 15
integrated
boost
2.67 x 15
-> boost
2.67 x 15
2.4 x 15
integrated
boost
APBI
2.67 x 15
2 x 25 +
2 x 8
2.67 x
15
APBI
4 x 10
2.0 x 25
-> boost
2.67 x 15
integrated
boost

ASTRO Guidelines (2011)
Age/Stage > 50 yrs, T1,2 N-
Surgery BCS
Chemotherapy None
Fractionation 266 cGy x 16
Heart in Field 0
Boost No Agreement
Dose Homogeneity < 7%
Ref: Smith B et al IJROBP 2011 81: 59
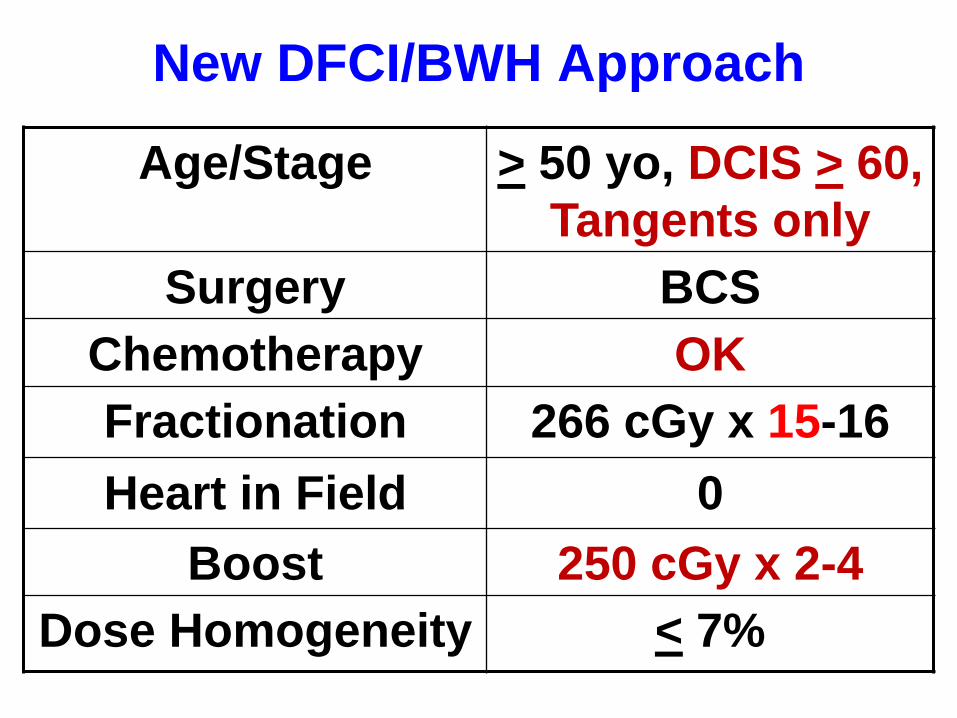
New DFCI/BWH Approach
Age/Stage > 50 yo, DCIS > 60,
Tangents only
Surgery BCS
Chemotherapy OK
Fractionation 266 cGy x 15-16
Heart in Field 0
Boost 250 cGy x 2-4
Dose Homogeneity < 7%
Hypofractionation
• The available RCTs, particularly the
Canadian and START B Trials, provide
increased support for hypofractionation
• This approach is clearly indicated in
many patients and will likely be
increasingly used

‘Personalized’ BCT based on
Subtype, Age (DFCI/BWH)
• Luminals > 60: 266 x 16, no boost
• Luminals 50-60: 266 x 15, 250 x 2
• HER2+ > 50: 266 x 15, 250 x 4
< 50: 200 x 22 + 200 x 8 = 60 Gy
• TN: Conventional + concurrent
platinum on protocol