hormonal causes of secondary osteoporosis
TRANSCRIPT
HORMONAL CAUSES OF SECONDARY OSTEOPOROSIS
Iris Thiele Isip Tan MD, MSc Professor 3, UP College of Medicine Chief, UP Medical Informatics Unit
?? SECONDARY osteoporosis
HORMONAL causes
TREATMENT
?? SECONDARY osteoporosis
HORMONAL causes
TREATMENT
SECONDARY OSTEOPOROSISLow bone mineral density or increased risk of fragility fracture
caused by any factor other than aging or postmenopausal status
Miller PD. Endocrinol Metab Clin N Am 2012;41:613-628
OSTEOPOROSISReduction in the strength of bone that
leads to an increased risk of fractures
Fractures of the spine or hip that occur in the absence of major trauma would be sufficient to diagnose
OSTEOPOROSISregardless of BMD
CC-BY-SA-3.0 (http://creativecommons.org/licenses/by-sa/3.0/)], via Wikimedia Commons
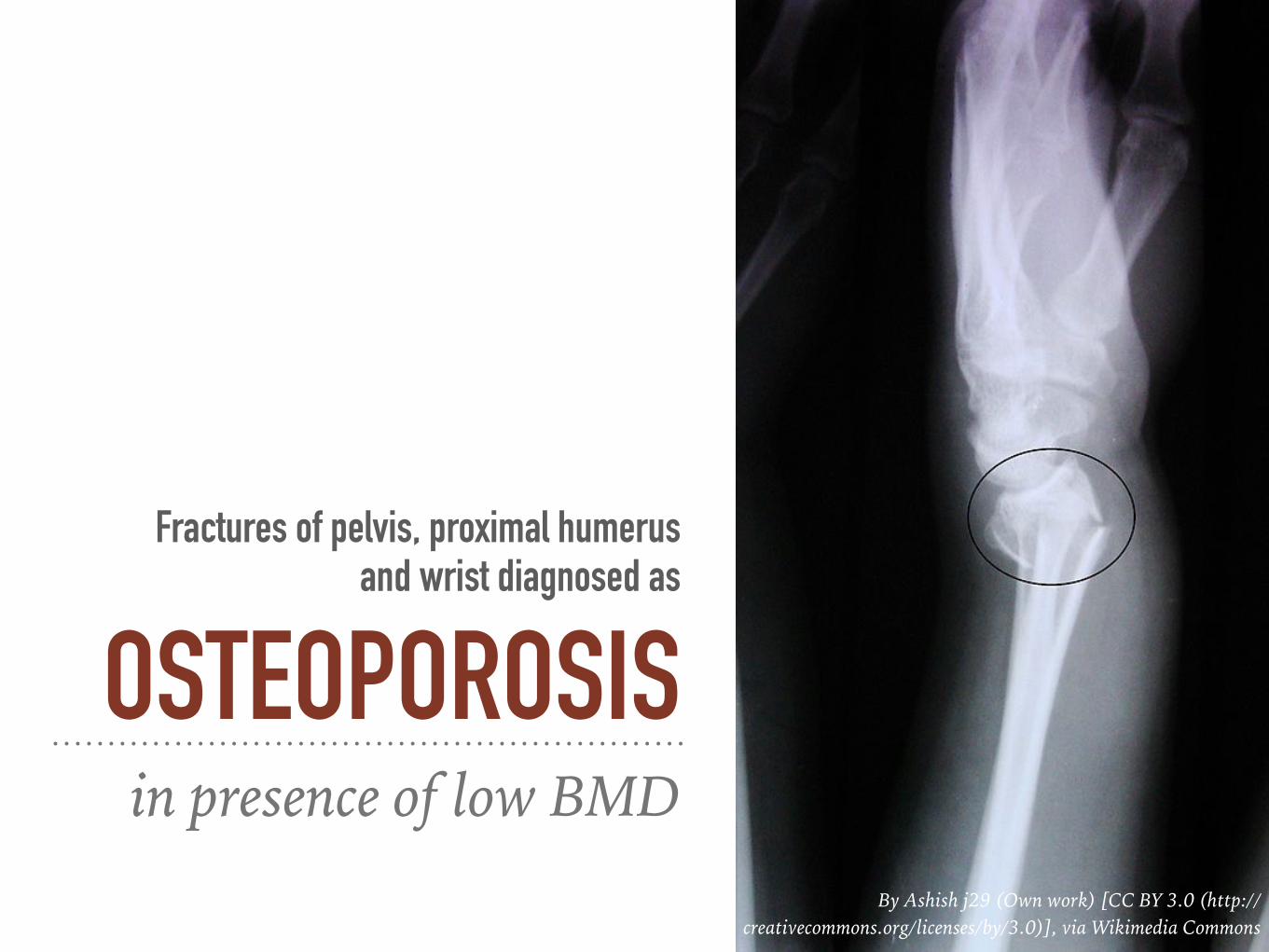
Fractures of pelvis, proximal humerus and wrist diagnosed as
OSTEOPOROSISin presence of low BMD
By Ashish j29 (Own work) [CC BY 3.0 (http://creativecommons.org/licenses/by/3.0)], via Wikimedia Commons
~50% of pre- and perimenopausal women with osteoporosis have an associated underlying cause
SECONDARY OSTEOPOROSIS
UNKNOWN number of postmenopausal women with
osteoporosis from a secondary cause
Sweet et al Am Fam Physician 2009; 79(3):193-200

WORK UP FOR SECONDARY
OSTEOPOROSIS Men 65 y or younger 50-65% of cases
Soriano et al Best Pract Res Clin Endoc Metab 2014; 28:885-894
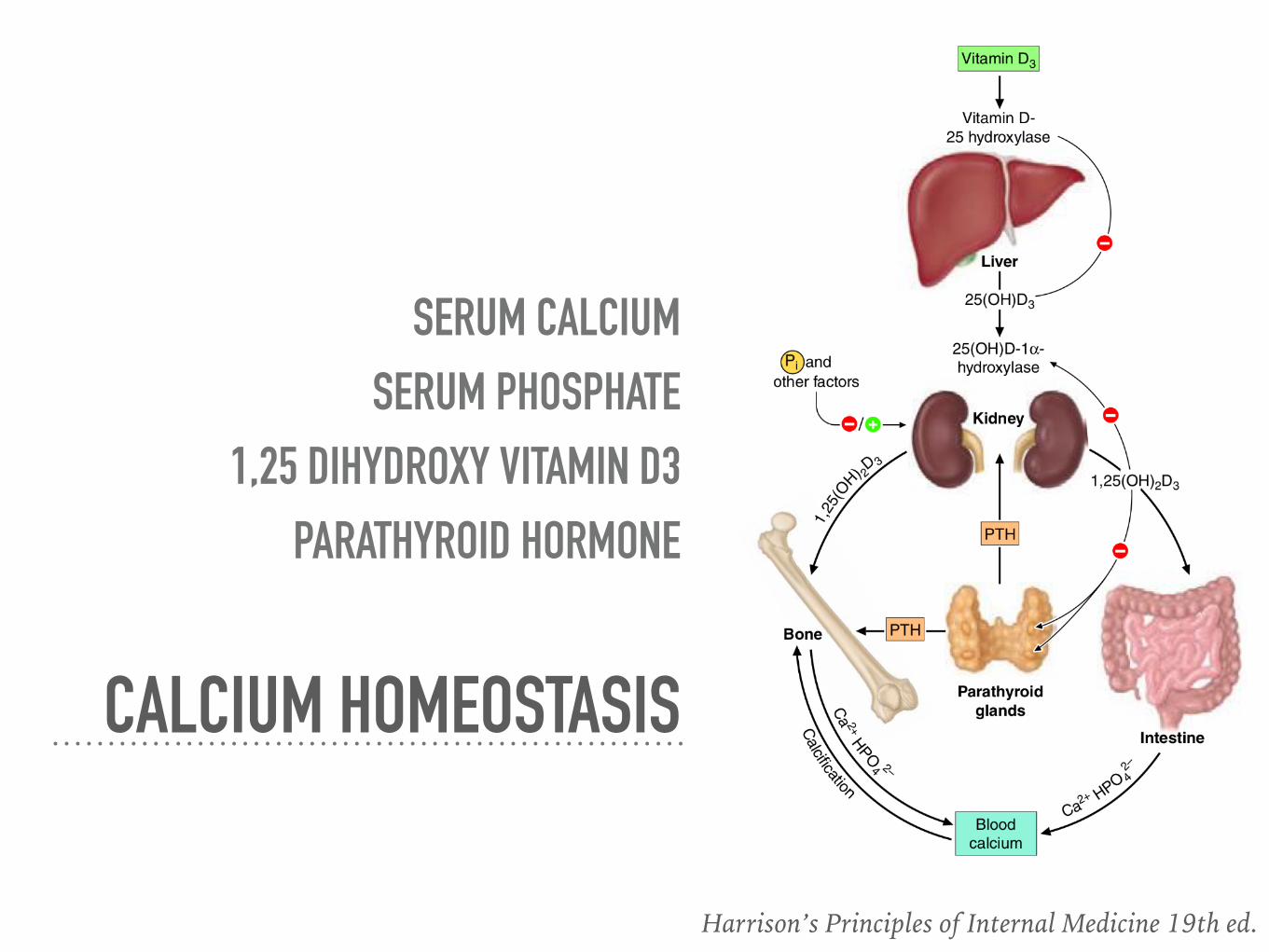
SERUM CALCIUM SERUM PHOSPHATE
1,25 DIHYDROXY VITAMIN D3 PARATHYROID HORMONE
CALCIUM HOMEOSTASIS
Harrison’s Principles of Internal Medicine 19th ed.

CONDITIONS, DISEASES & MEDICATIONS THAT
CONTRIBUTE TO OSTEOPOROSIS &
FRACTURESHistory and PE!
Harrison’s Principles of Internal Medicine 19th ed.
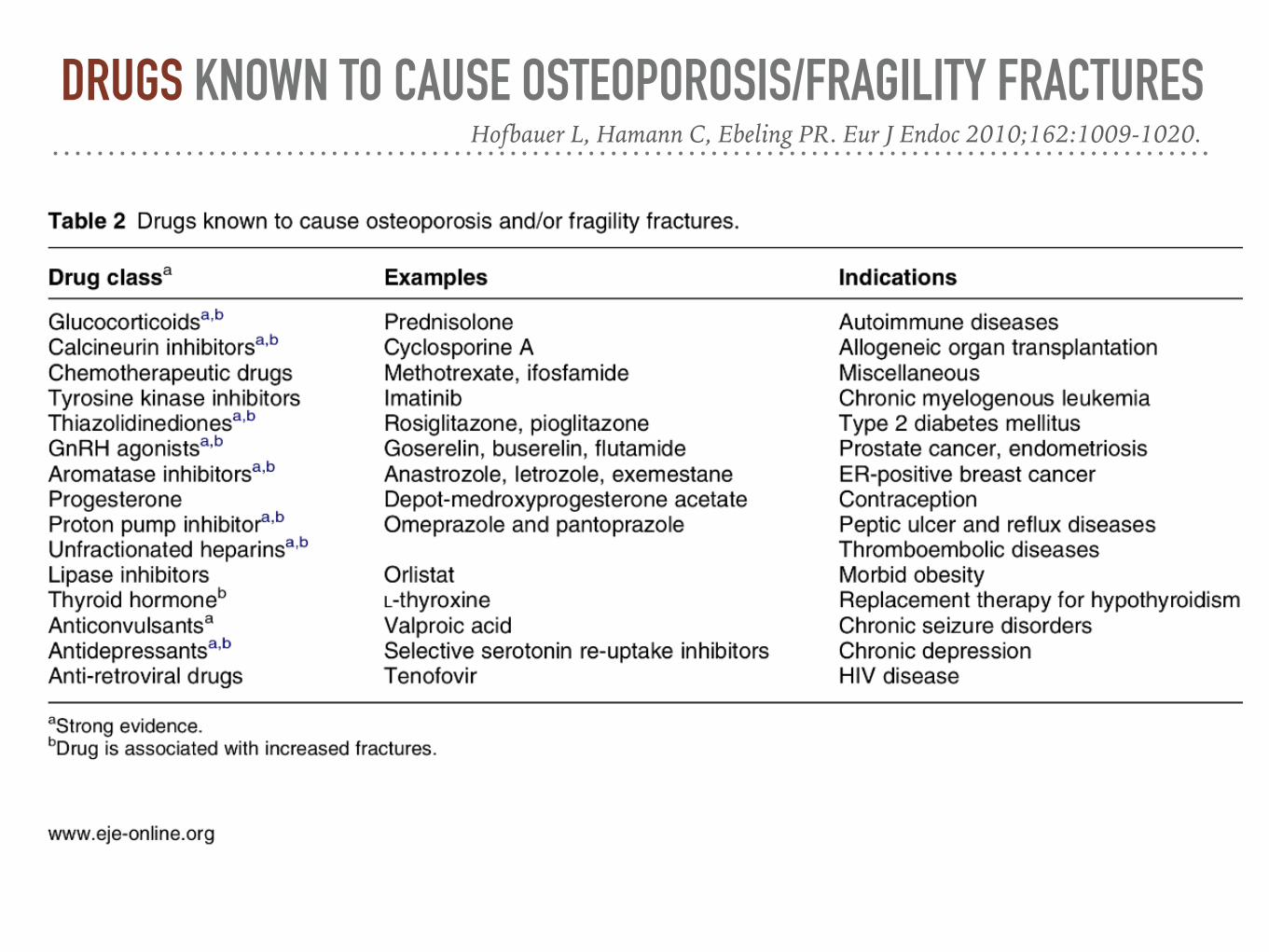
DRUGS KNOWN TO CAUSE OSTEOPOROSIS/FRAGILITY FRACTURESHofbauer L, Hamann C, Ebeling PR. Eur J Endoc 2010;162:1009-1020.
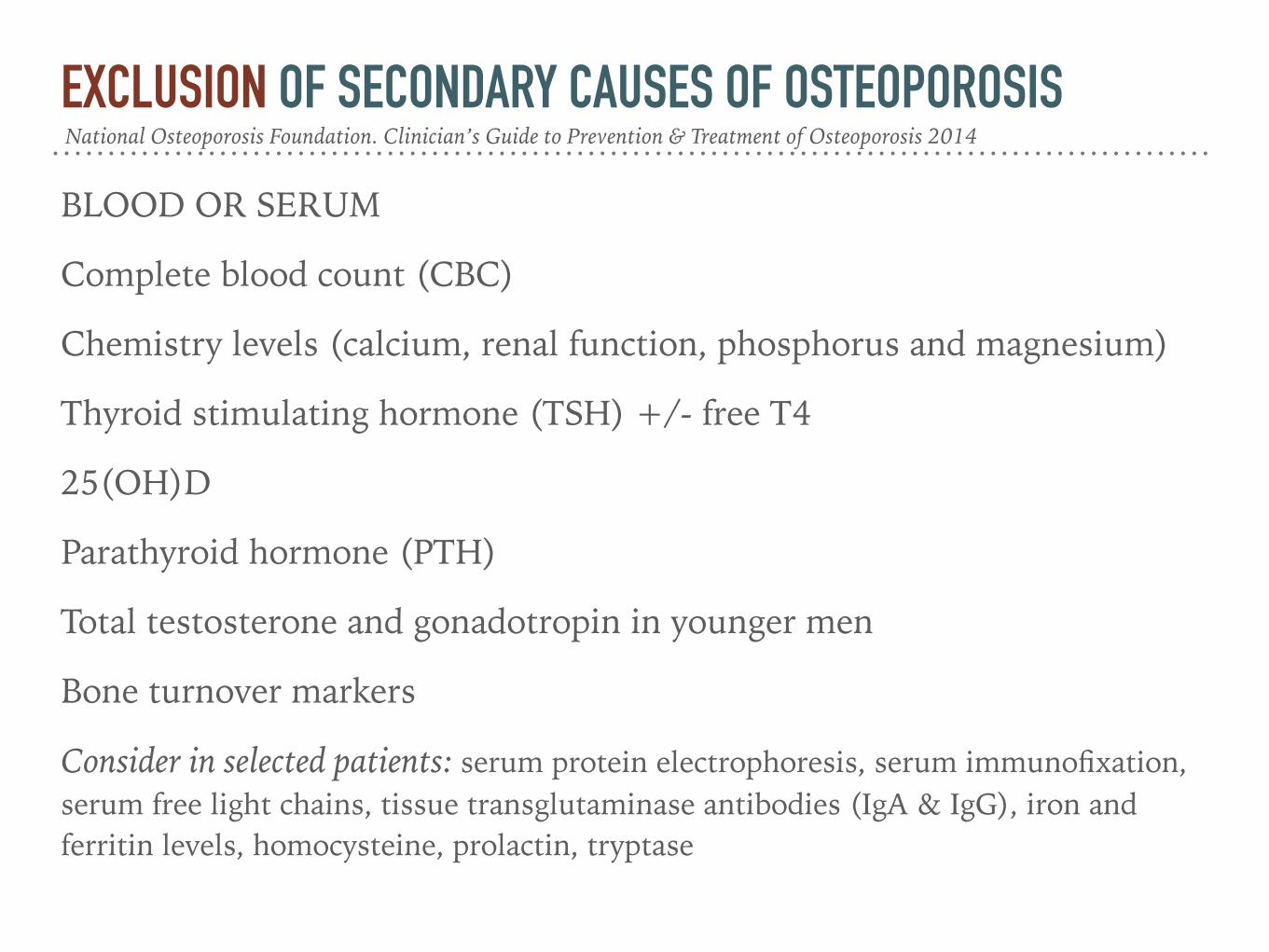
EXCLUSION OF SECONDARY CAUSES OF OSTEOPOROSIS
BLOOD OR SERUM
Complete blood count (CBC)
Chemistry levels (calcium, renal function, phosphorus and magnesium)
Thyroid stimulating hormone (TSH) +/- free T4
25(OH)D
Parathyroid hormone (PTH)
Total testosterone and gonadotropin in younger men
Bone turnover markers
Consider in selected patients: serum protein electrophoresis, serum immunofixation, serum free light chains, tissue transglutaminase antibodies (IgA & IgG), iron and ferritin levels, homocysteine, prolactin, tryptase
National Osteoporosis Foundation. Clinician’s Guide to Prevention & Treatment of Osteoporosis 2014

EXCLUSION OF SECONDARY CAUSES OF OSTEOPOROSIS
URINE
24-h urinary calcium
Consider in selected patients: protein electrophoresis (UPEP), urinary free cortisol level, urinary histamine
National Osteoporosis Foundation. Clinician’s Guide to Prevention & Treatment of Osteoporosis 2014

?? SECONDARY osteoporosis
HORMONAL causes
TREATMENT
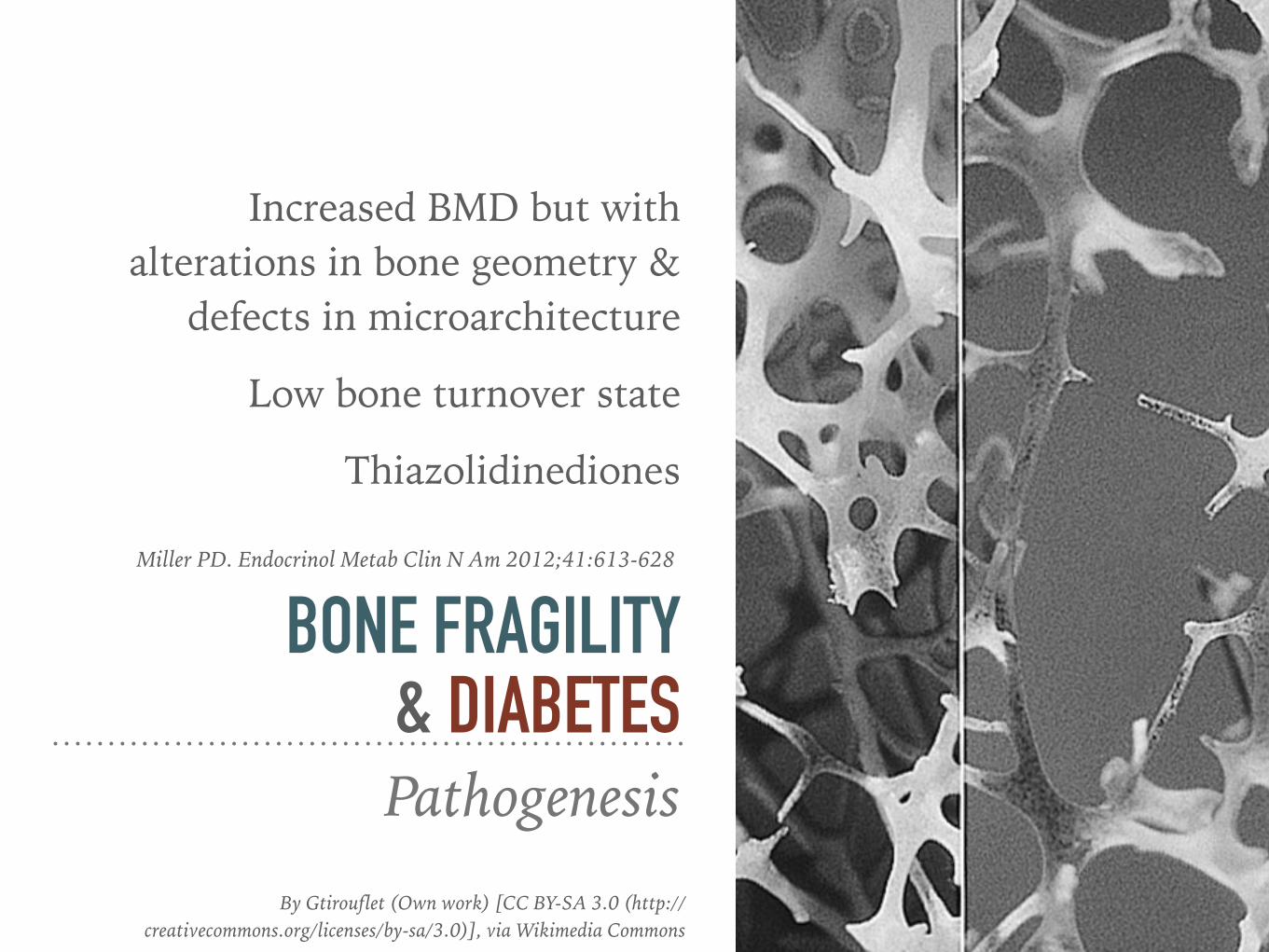
Increased BMD but with alterations in bone geometry &
defects in microarchitecture
Low bone turnover state
Thiazolidinediones
BONE FRAGILITY & DIABETESPathogenesis
Miller PD. Endocrinol Metab Clin N Am 2012;41:613-628
By Gtirouflet (Own work) [CC BY-SA 3.0 (http://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons
Type 1 diabetes: 12-fold increased risk
Longer duration of diabetes
Insulin use
Increased risk of falls
RISK FACTORS FOR FRACTURES IN DIABETES
Miller PD. Endocrinol Metab Clin N Am 2012;41:613-628
CC-BY-SA-3.0 (http://creativecommons.org/licenses/by-sa/3.0/)], via Wikimedia Commons
30-50% of patients on chronic glucocorticoid therapy will
experience a fracture
Most common iatrogenic cause of osteoporosis
GLUCOCORTICOID EXCESS & OSTEOPOROSIS
By Gtirouflet (Own work) [CC BY-SA 3.0 (http://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons
Emkey GR & Epstein S. Best Prac Res Clin Endoc Metab 2014;28:911-935
Glucocorticoids decrease osteoblast precursors
Increased apoptosis of mature osteoblasts
GLUCOCORTICOID EXCESS & OSTEOPOROSIS
Emkey GR & Epstein S. Best Prac Res Clin Endoc Metab 2014;28:911-935
PathogenesisBy Gtirouflet (Own work) [CC BY-SA 3.0 (http://
creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons
Rapid decrease in bone strength with early fracture
risk even at prednisone as low as 2.5-7.5 mg/day
GLUCOCORTICOID EXCESS & OSTEOPOROSIS
CC-BY-SA-3.0 (http://creativecommons.org/licenses/by-sa/3.0/)], via Wikimedia Commons
Soriano et al Best Pract Res Clin Endoc Metab 2014; 28:885-894
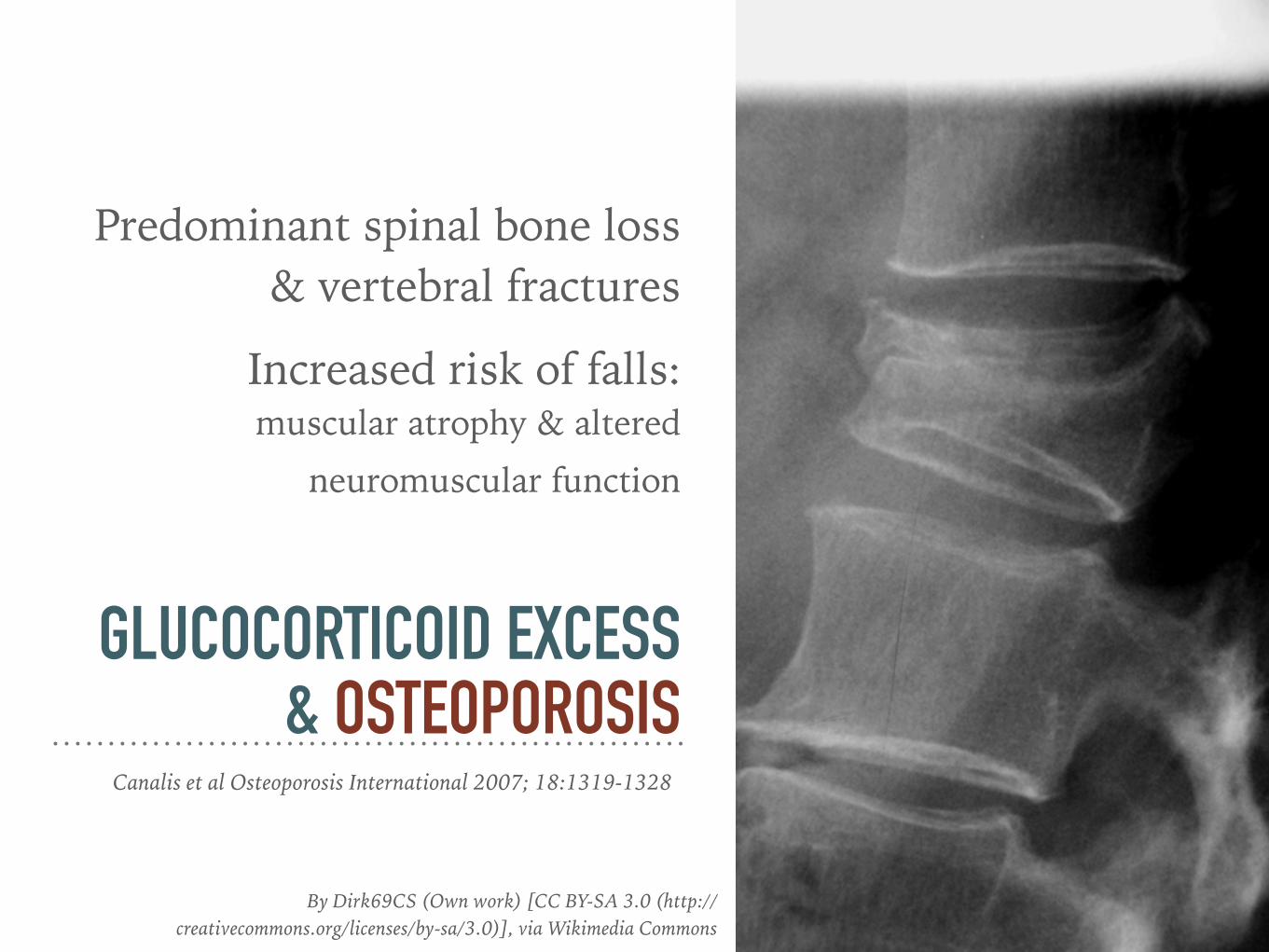
Predominant spinal bone loss & vertebral fractures
Increased risk of falls: muscular atrophy & altered
neuromuscular function
GLUCOCORTICOID EXCESS & OSTEOPOROSIS
Canalis et al Osteoporosis International 2007; 18:1319-1328
By Dirk69CS (Own work) [CC BY-SA 3.0 (http://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons
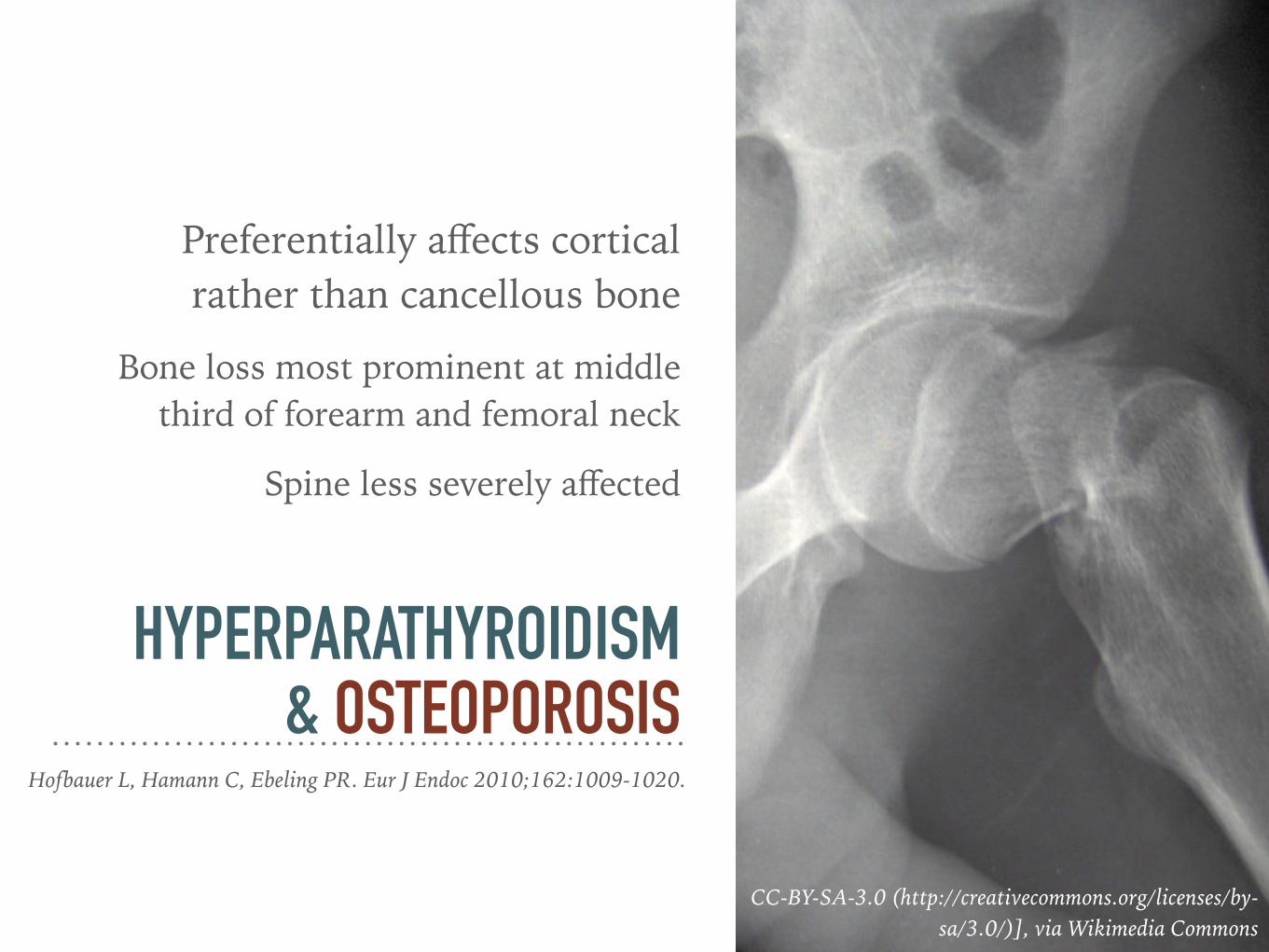
Preferentially affects cortical rather than cancellous bone
Bone loss most prominent at middle third of forearm and femoral neck
Spine less severely affected
HYPERPARATHYROIDISM & OSTEOPOROSIS
CC-BY-SA-3.0 (http://creativecommons.org/licenses/by-sa/3.0/)], via Wikimedia Commons
Hofbauer L, Hamann C, Ebeling PR. Eur J Endoc 2010;162:1009-1020.
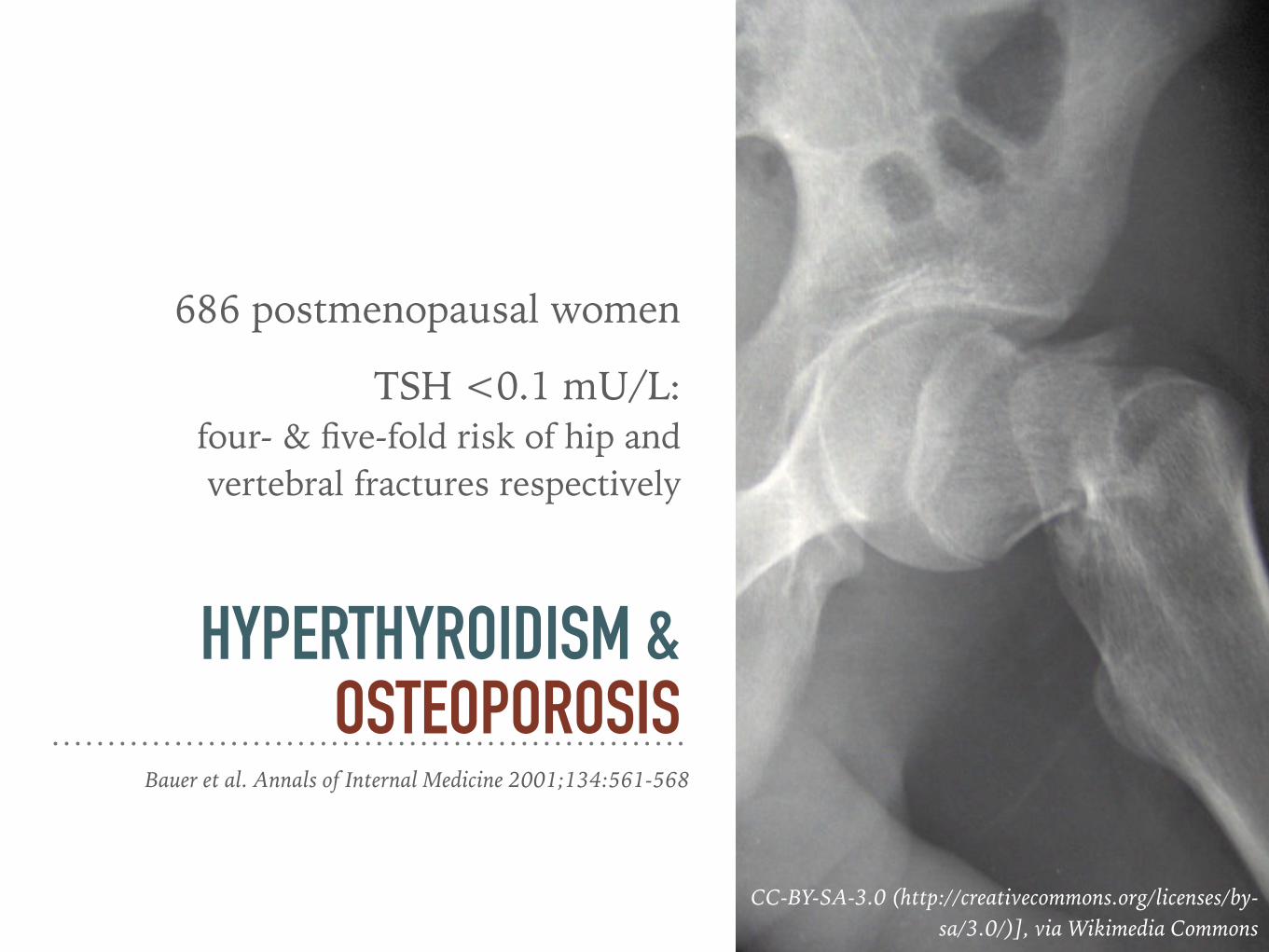
686 postmenopausal women
TSH <0.1 mU/L: four- & five-fold risk of hip and vertebral fractures respectively
HYPERTHYROIDISM & OSTEOPOROSIS
CC-BY-SA-3.0 (http://creativecommons.org/licenses/by-sa/3.0/)], via Wikimedia Commons
Bauer et al. Annals of Internal Medicine 2001;134:561-568
Meta-analysis of 21 studies: Thyroid hormone therapy for TSH
suppression in thyroid cancer
Associated with osteoporosis in postmenopausal women
HYPERTHYROIDISM & OSTEOPOROSIS
Heemstra et al. Thyroid 2006;16:583-591
?? SECONDARY osteoporosis
HORMONAL causes
TREATMENT

Treat underlying disease, if known
Treat osteoporosis and prevent further fractures
MANAGEMENT Secondary Osteoporosis

SAME OSTEOPOROSIS TREATMENT OPTIONS FOR DIABETES
Diabetic nephropathy may limit use of bisphosphonates
Kurra S, Fink DA, Siris ES. Endocrinol Metab Clin N Am 2014;43L233-243
DEFICIENT OSTEOBLASTIC FUNCTION IN DIABETES: USE ANABOLIC DRUGS?
By Gtirouflet (Own work) [CC BY-SA 3.0 (http://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons
Garcia et al. Clinical Practice Guidelines for evaluation and treatment of osteoporosis associated to endocrine and nutritional conditions. Endocrinol Nutr 2012; 59:174-196
MEASUREMENT OF BMD HAS LIMITED PREDICTIVE VALUE IN DETERMINING FRACTURE RISKin the context of glucocorticoid therapy
Henneicke et al. Trends Endocrinol Metab 2014;25(4):197-211

RECOMMENDED FOR PREVENTION & TREATMENT OF GIO
Intervention DoseEvidence
Grade (BMD)
Evidence Grade
(Fracture)Calcium Oral: 1000-1500 mg daily A -Vitamin D Oral: 800-1000 IU daily A -Alendronate Oral: 70 mg once/week A BRisedronate Oral: 35 mg once/week A AZoledronic acid IV: 5 mg once/year A -Teriparetide SC: 20 mg once/day A A
Etidronate Oral: 400 mg daily for 2 weeks every 3 months A A
Henneicke et al. Trends Endocrinol Metab 2014;25(4):197-211
Indication for parathyroid surgery in otherwise asymptomatic patient
Osteoporotic fractures
T score of <-2.5
HYPERPARATHYROIDISM & OSTEOPOROSIS
Hofbauer L, Hamann C, Ebeling PR. Eur J Endoc 2010;162:1009-1020.
8% increase in lumbar spine BMD & 6% increase in femoral neck 1 year after resection
BMD RECOVERS AFTER PARATHYROIDECTOMY10 yr data: 12% and 14% increase in BMD for spine and femur respectively
Soriano et al Best Pract Res Clin Endoc Metab 2014; 28:885-894
Men age 50-70: 1000 mg/day Women age >51 y and men age >71 y: 1200 mg/day
CALCIUM INTAKEIntakes in excess of 1200-1500 mg/day may increase risk of kidney stones, CVD and stroke.
National Osteoporosis Foundation. Clinician’s Guide to Prevention & Treatment of Osteoporosis 2014
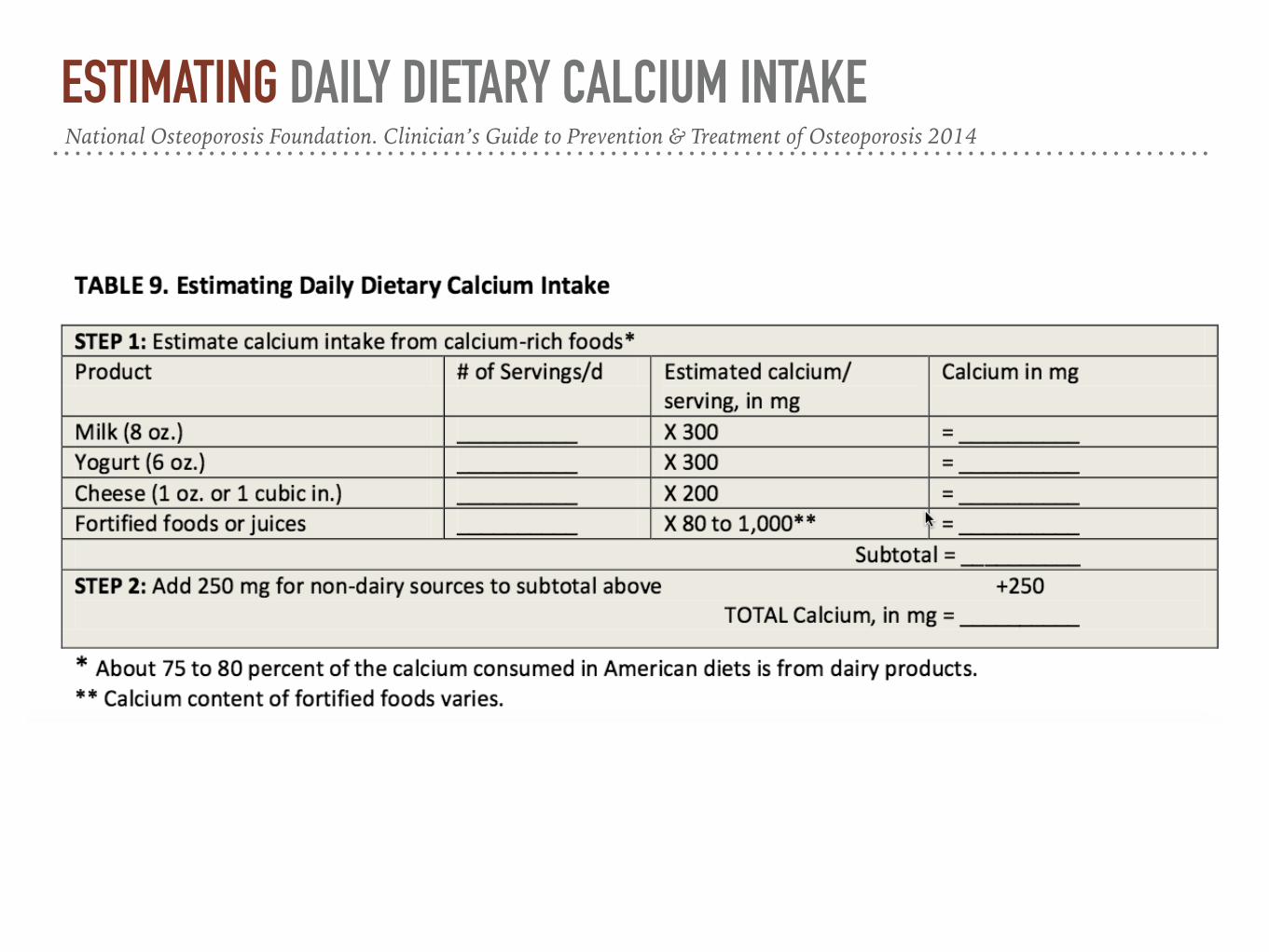
ESTIMATING DAILY DIETARY CALCIUM INTAKENational Osteoporosis Foundation. Clinician’s Guide to Prevention & Treatment of Osteoporosis 2014
800 to 1,000 IU per day for adults >50 y
VITAMIN DIOM Dietary Reference Intakes for vitamin D 600 IU/day
until age 70 y and 800 IU/day for older adults National Osteoporosis Foundation. Clinician’s Guide to Prevention & Treatment of Osteoporosis 2014
?? SECONDARY osteoporosis
HORMONAL causes
TREATMENT
