hlc008-01-820 hc2020 volume to value revolution volume to value revolution ... pub lic information...
TRANSCRIPT

© 2011 OLIVER WYMANHEALTH AND LIFE SCIENCES
Thomas J. MainPartner and US Market Leader
THE VOLUME TO VALUE REVOLUTION HEALTHCARE 2020
Scripps Green Hospital Grand RoundsWednesday, December 14, 2011

1© 2011 OLIVER WYMAN | HLC008-01-820
Report qualifications/assumptions and limiting conditions
December 12, 2011
This report is for the exclusive use of the Oliver Wyman client named herein. This report is not intended for general circulation or publication, nor is it to be reproduced, quoted or distributed for any purpose without the prior written permission of Oliver Wyman. There are no third party beneficiaries with respect to this report, and Oliver Wyman does not accept any liability to any third party.
Information furnished by others, upon which all or portions of this report are based, is believed to be reliable but has not been independently verified, unless otherwise expressly indicated. Public information and industry and statistical data are from sources we deem to be reliable; however, we make no representation as to the accuracy or completeness of such information. The findings contained in this report may contain predictions based on current data and historical trends. Any such predictions are subject to inherent risks and uncertainties. Oliver Wyman accepts no responsibility for actual results or future events.
The opinions expressed in this report are valid only for the purpose stated herein and as of the date of this report. No obligation is assumed to revise this report to reflect changes, events or conditions, which occur subsequent to the date hereof.
All decisions in connection with the implementation or use of advice or recommendations contained in this report are the soleresponsibility of the client. This report does not represent investment advice nor does it provide an opinion regarding the fairness of any transaction to any and all parties.

2© 2011 OLIVER WYMAN | HLC008-01-820
Four mega forces reshaping healthcare – the volume to value revolution
Information, integration and actionable insights
Science, genomics and personalization
Healthcare affordability
and value
Retail market, consumerism and social media
Healthcare 2020 Market Convergence
The move to a value-based retail healthcare marketplace
December 12, 2011

3© 2011 OLIVER WYMAN | HLC008-01-820
The new rule of innovation and value – .95p + 1.2v + 2t
Job’s Law 75% of last year’s price and 3 times
the value Every 3 years
Bezos’s Law 50% of last year’s price and 3 times
the value Every 2 years
Healthcare Law 108% of last year’s price and 90% of
the value Every year
Price (P) Value (V) Time (T)
December 12, 2011

4© 2011 OLIVER WYMAN | HLC008-01-820
Old school or new school – the market is desperate to reward value
• Benefit design
• Financial engineering
• Integrated reward systems
• Employer culture of health with promotion programs
• On-site clinics
• Consumer engagement
• Health advocacy and coaching
• Health management
• Network contracting
• Population segmentation (15/55)
• Patient registries
• Predictive modeling
• Personalized health itinerary
• Health engagement (integrated consumer experience)
• Connected practices – inclusion of clinical data
• Real time clinical and biometric triggers (home monitoring)
• Value based care models (VBP) – IOCP– PCMH– e-health – ACOs– Retail clinics
• Health information enablement (EBM at point of care, virtual MDTs, etc.)
• Social media
• Behavioral/social/clinical science
The Race
to Value.95p + 1.2v every 2t
• Demand or supply management – how do you unlock the value (30/70)?
• Value chain integration and convergence – can you get there in disconnected silos?
• Virtual integration and cloud computing – will it offset massive fragmentation and capital andskill barriers?
Old school New school
December 12, 2011

5© 2011 OLIVER WYMAN | HLC008-01-820
Accelerating the shift to a value-based market – the diffusion cycle is broken
December 12, 2011
Innovation Adoption Mastery Monetization
• Market fragmentation• FFS economics• Wholesale buyers• Lack of consumer
buying power• Capital rotation
• Basis of competition• Craft skills• Liability• Information gaps• Culture• Leadership
Diffusion barriers
6© 2011 OLIVER WYMAN | HLC008-01-820
Table of contents
• Section 1: The consumer driven industry transformation
• Section 2: Health management company implications
• Section 3: The volume of value revolution
• Section 4: The race to value
December 12, 2011

7© 2011 OLIVER WYMAN | HLC008-01-820 December 12, 2011
THE CONSUMER DRIVEN INDUSTRY TRANSFORMATION
Section 1
8© 2011 OLIVER WYMAN | HLC008-01-820
Consumers buying patterns will shatter the traditional wholesale buying model and reshape the healthcare marketplace
As consumers make real tradeoff decisions between benefits, health management programs, personal accountability, physician relationships and financial exposure (risk and cost)…
…they will make different choices than their employers made for them and drive industry transformation.
December 12, 2011
9© 2011 OLIVER WYMAN | HLC008-01-820
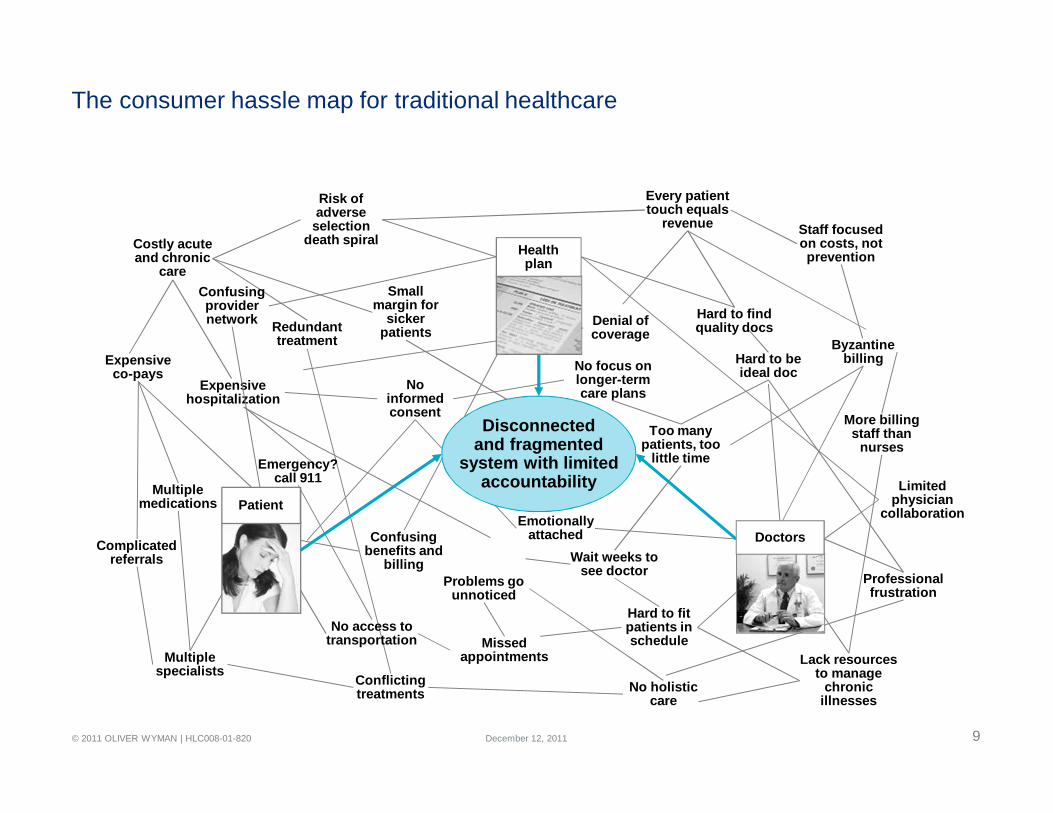
The consumer hassle map for traditional healthcare
Hard to fit patients in schedule
Lack resources to manage
chronic illnesses
Wait weeks to see doctor
Too many patients, too
little time
No focus on longer-term care plans
Emotionally attached
Byzantine billing
More billing staff than
nurses
Hard to be ideal doc
Professional frustration
Missed appointments
Problems go unnoticed
Complicated referrals
Multiple medications
Expensive hospitalization
Multiple specialists Conflicting
treatments No holistic care
Expensive co-pays
No informed consent
Redundant treatment
Hard to find quality docs
Costly acute and chronic
care
Risk of adverse
selection death spiral
Every patient touch equals
revenue Staff focused on costs, not prevention
Small margin for
sicker patients
Confusing benefits and
billing
Confusing provider network
Limited physician
collaboration
Disconnectedand fragmented
system with limitedaccountability
Emergency? call 911
Denial of coverage
No access to transportation
Healthplan
Doctors
Patient
December 12, 2011

10© 2011 OLIVER WYMAN | HLC008-01-820
Traditionalists
Percentage of Buyers 29% 26% 11% 25% 9%
Attitudes
• View insurance as a commodity, want basic coverage
• Not looking for help, advice or a relationship with their health plan
• Very willing to engage with insurers in health management activities
• Want help making healthcare decisions
• Experienced with the healthcare system and trust their doctor
• Price is most important• Willing to compromise
convenience and access to save $
• Willing to stay healthy to save on premiums
• No desire to engagewith insurers
• Like status quo• See greater engagement
as an unnecessary inconvenience
• Want easy, convenient access to healthcare
• Value technology, willing to try new things
• Willing to spend $for value
Demographics
• Less educated (~40% only finished high school), less employed, struggling to makeends meet
• Mix of singles and small families
• Largely middle-class• 30-40-somethings• Mix of single and families
• Lower middle class• 30-40-somethings• Mix of single and families
• Aging baby boomer• Employed or homemaker• Financially stable• Many empty nesters,
some dependents
• Younger, dualincome families
• Well-educated, majority have at least a college degree
Health Status and Lifestyle
• >75% currently uninsured
• Healthy, but riskier lifestyles
• ~50% currently uninsured
• At-Risk/Chronic, but attempting to get better with positive lifestyles
• ~50% insured (Indiv)• Healthy with good
lifestyles
• ~70% insured (SG)• At-Risk/Chronic• Avoid smoking or
drinking, but don’t exercise
• ~80% insured (SG/Indiv)• Healthy & At-Risk• Protect health with
exercise
Busy FamiliesWant to Be Healthier
Engaged to Save
Struggling & Unengaged
Source: Oliver Wyman Consumer Survey and Analysis. Health Status based on self-reported health conditions.
“I work 2 jobs to pay for food and a place to live, I’m not sick, so I just want basic insurance to cover me in case”
“I’ll do whatever it takes to get a better price on health insurance. I don’t need a lot”
“I want to be healthier, but its not easy. I’d like less expensive insurance, but am not willing to limit my options, I like my doctor.”
“The health insurance I already have works well for me, why fix something that isn’t broken?”
“I’m too harried to spend much time thinking about health insurance for me and my family, but I want care when I need it”
Oliver Wyman consumer segments – five distinct markets with unmet needs
December 12, 2011

11© 2011 OLIVER WYMAN | HLC008-01-820
Consumers will buy differently than employers bought for them – and their $500 BN in buying power will reshape the marketplace
• Lower cost through benefit buy downs and cost shifting to employees; facilitated through brokers and consultants
• Reduce employee noise through a broad access one-size-fits-all provider network
• Limited offering of opt-in health management programs focused on reducing medical cost
• Transactional service and administrative efficiency to lower cost and minimize employee feedback
1
2
3
4
• Buy an affordable product by balancing benefits, personalized engagement, and physician/health system choices with cost and exposure
• Select a personalized set of physicians and health systems to meet your needs and your budget
• Consumer-focused engagement programs to improve health and reduce consumer costs
• Personalized, integrated, simple and effective service focused on the consumer’s needs
NETWORK
PRODUCT
HEALTHMANAGEMENT
SERVICE
Employer-driven wholesale model Consumer-driven retail model
December 12, 2011
12© 2011 OLIVER WYMAN | HLC008-01-820 December 12, 2011
HEALTH MANAGEMENT COMPANY IMPLICATIONS
Section 2

13© 2011 OLIVER WYMAN | HLC008-01-820
Leading the volume to value revolution
Traditionalhealthcare
organizations
Value-basedhealthcarecompanies
• CEO and Board driven vision
• CEO-driven change agenda
• CEO actions to address barriers
• Physician-led disease-focused businesses
• Commercializing value-based care
• Rebuilding the business model
• Shifting organizational culture
Transforming the healthcare system requires a redesign of how healthcare is managed and delivered and the underlying economics
Healthcare CEO perspectives
December 12, 2011
14© 2011 OLIVER WYMAN | HLC008-01-820
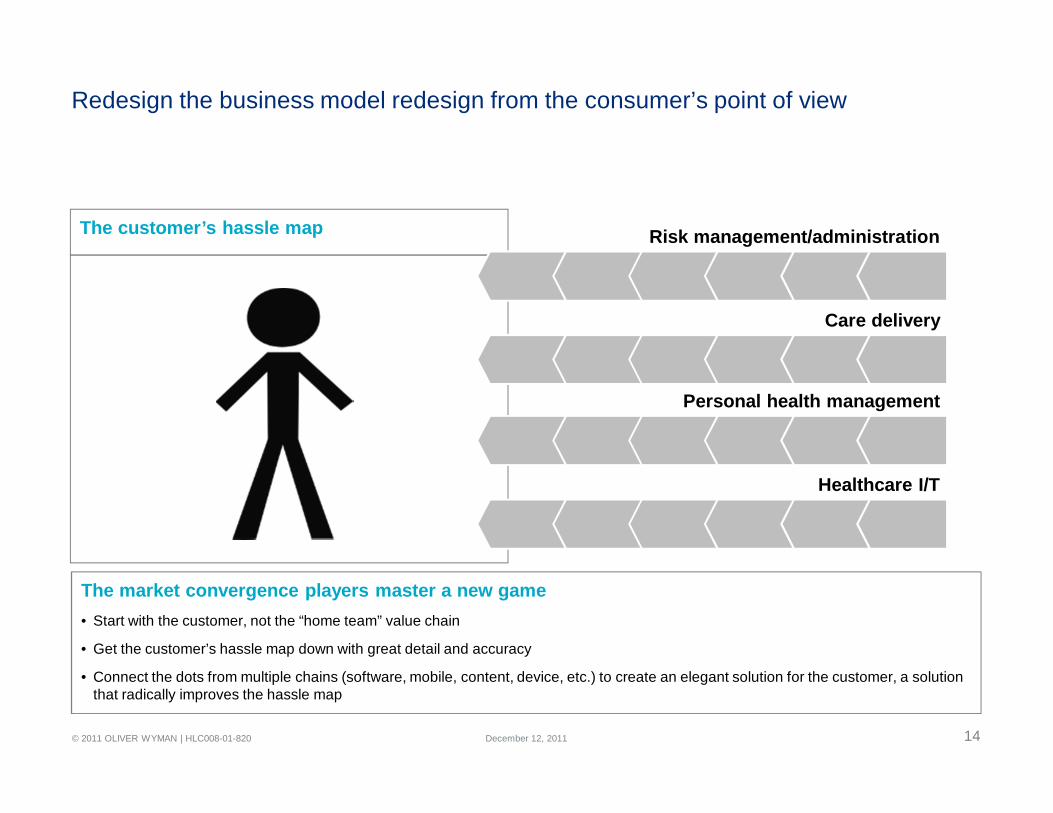
The Customer’s Hassle Map
The customer’s hassle map
Redesign the business model redesign from the consumer’s point of view
Risk management/administration
Care delivery
Healthcare I/T
Personal health management
The market convergence players master a new game• Start with the customer, not the “home team” value chain
• Get the customer’s hassle map down with great detail and accuracy
• Connect the dots from multiple chains (software, mobile, content, device, etc.) to create an elegant solution for the customer, a solution that radically improves the hassle map
December 12, 2011
15© 2011 OLIVER WYMAN | HLC008-01-820
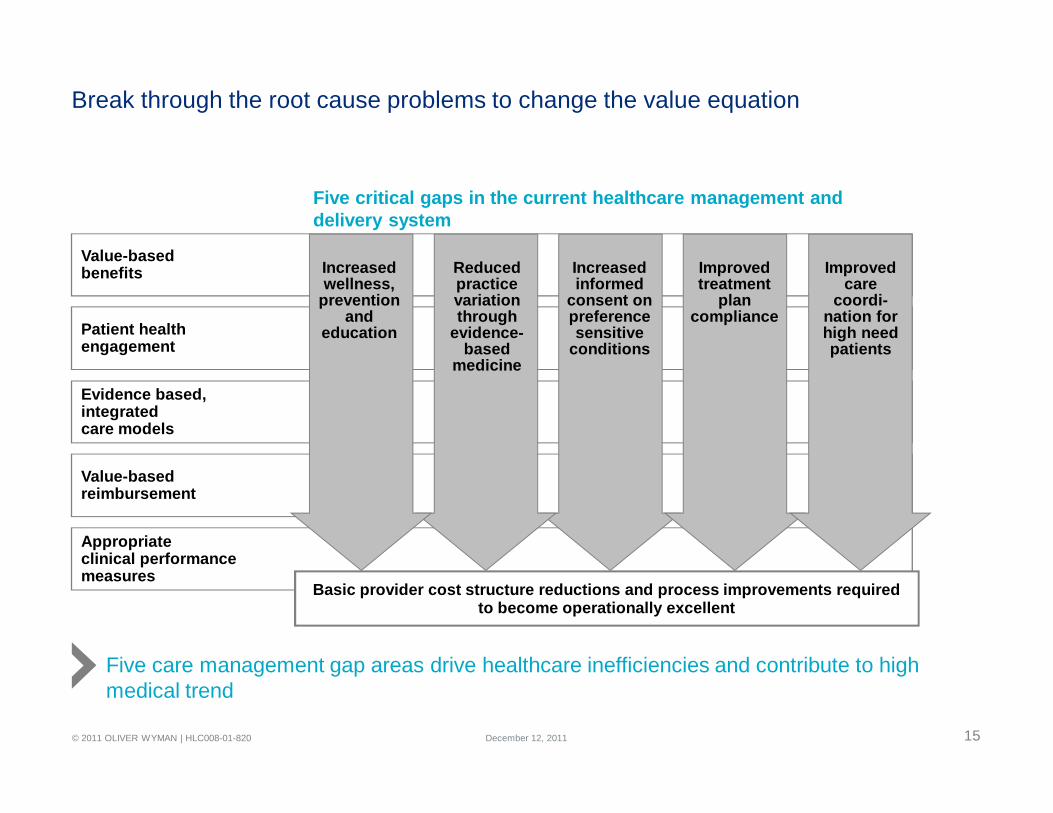
Break through the root cause problems to change the value equation
Evidence based, integratedcare models
Patient health engagement
Value-based benefits
Value-based reimbursement
Appropriate clinical performancemeasures
Improved care
coordi-nation for high need patients
Improved treatment
plan compliance
Reduced practice variation through
evidence-based
medicine
Increased informed
consent on preference sensitive
conditions
Increased wellness,
prevention and
education
Basic provider cost structure reductions and process improvements required to become operationally excellent
Five critical gaps in the current healthcare management and delivery system
Five care management gap areas drive healthcare inefficiencies and contribute to high medical trend
December 12, 2011

16© 2011 OLIVER WYMAN | HLC008-01-820
Develop a clinical strategy based on population health needs – reinvent the care models accordingly
TransactionalEfficiency (FFS)
Episodic Care Models(payment model driven)
Condition Based Care Models(care model driven)
Population Based Care Models(integrated whole person)
Simple service based models that can continue to deliver highly efficient care in aFFS environment
Complex service based models that can deliver efficient care through high levels of specialization and low operational variability
Specialized care delivery model that is organized along specific condition and/or disease etiologies
High value-based delivery model that manages the clinical risk of targeted or whole patient populations
• Stand-alone ERs• Urgent care facilities• Dermatologists• Ophthalmologists• Dentists• Walk-in-clinics
• Orthopedics (Hips and knees)
• CV surgery• General/
specialty surgery
Definition
Example Model Types
• Cardiology• Cancer• Diabetes • Pulmonary• Kidney
• Partial Pop. Managers• Frail elder• High risk• Poly-chronic• Full Pop Managers• ACOs• Globally capitated models
December 12, 2011
17© 2011 OLIVER WYMAN | HLC008-01-820
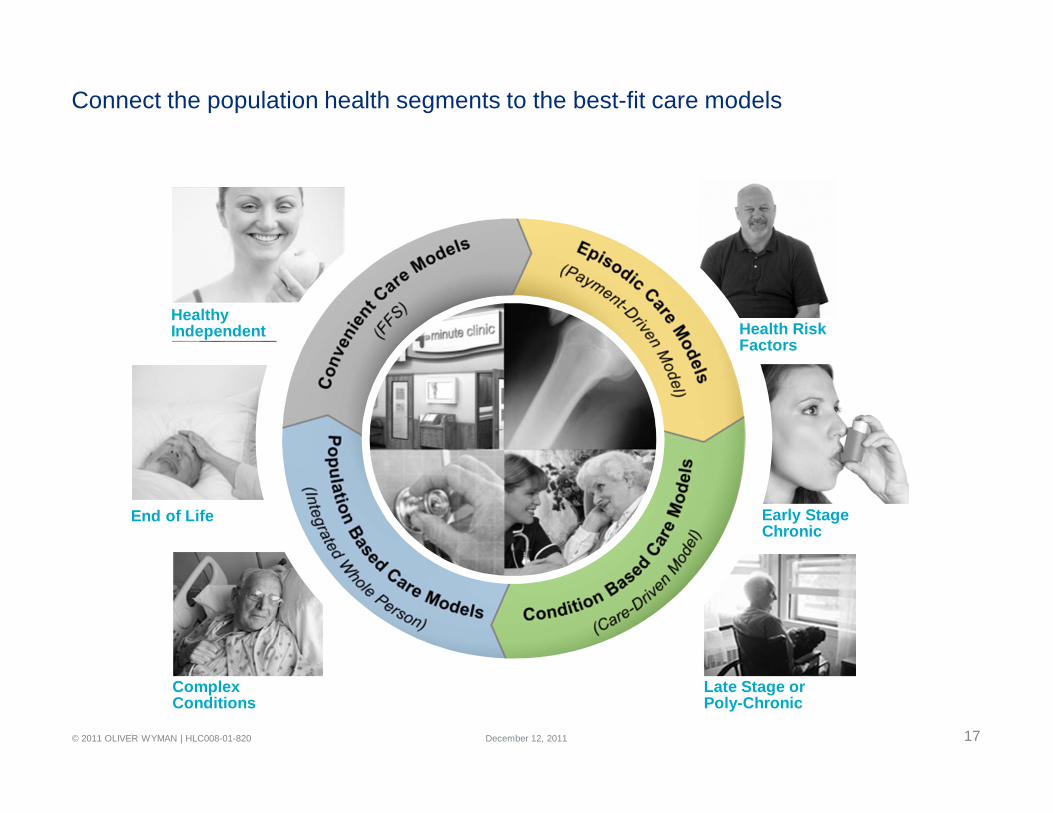
Connect the population health segments to the best-fit care models
End of Life
ComplexConditions
HealthyIndependent Health Risk
Factors
Late Stage orPoly-Chronic
Early StageChronic
December 12, 2011

18© 2011 OLIVER WYMAN | HLC008-01-820
Bring the missing capabilities to market – they are required for long-term success
INFRASTRUCTURE
Electronic Health Record (Integrated EHR)
Clinical Data Repository (CDR)
HEALTH MANAGEMENT ENABLEMENT
Clinical Performance Management
Patient Care Programs Clinical Risk Management andPayer Contracting
Clinical Model Redesign
Population Management, Patient Registriesand Personalized MedicineTreatment Management and
Multidisciplinary Teams
ACO or IDN CommercializationProvider and Service Network Development
Evidenced Based Guidelines andClinical Trial Programs
Clinical Strategy andLeadership Model
Care model redesign
Performance management
Commercial-ization
December 12, 2011

19© 2011 OLIVER WYMAN | HLC008-01-820
Replace fee for service networks with value based care models over time
Intensive OP Care Programs(80% of improvement opportunity)
Proactive Prevention(17%)
Routine Care (3%)
% Members 20% 24% 56%
% Costs 58% 17% 25%
IOCP
Prevention & Chronic Care Management
Routine Care
Intensive active management of the sickest individuals within the population
Proactive engagement for early chronic and at-risk individuals
Efficient routine and urgent care services for everyone
Complex/Poly-chronic Early Stage Chronic/At Risk HealthyPopulation
Model Description
Integrated Community Care Model
Source: Sample claims data, OW Analysis
PCMH (3 in 1 model)
UrgentCare
HomeCare
Social Services
Transport
Nutrition& Meals
Drug & Alcohol
Programs
CommunityPrograms
Fitness
3 in 1 PCMH and IOCP model improves cost and value for the complex poly chronic patients
December 12, 2011

20© 2011 OLIVER WYMAN | HLC008-01-820
Replace fee for service networks with value based care models over time
Offices Services
Offices Services
Diagnostic Imaging Diagnostic
Imaging
Pre-Hab Services Pre-Hab
Services
Surgical Center
Surgical Center
Anesthesia
Anesthesia
Implant or Device
Implant or Device
Pharmacy
Pharmacy
Rehab Services
Rehab Services
FFS Revenue Management FFV Integrated Cost and QualityManagement
TODAY100%
FUTURE85%
ILLUSTRATIVE
• Pain management effectiveness
• Functional improvement services
• Return to work
• Patient satisfaction
The shift
to value
Integrated orthopedic care model lowers costs by 15% Performance outcome measures
December 12, 2011

21© 2011 OLIVER WYMAN | HLC008-01-820
Total Care
Treat the tumor Treat the patientCoordinated Oncology Care
Patient
Interventional Radiology
Histopathology
Molecular Profiling
Research
Surgical Oncology
Medical Oncology
Radiation Oncology
Imaging/Radiology
Evidenced-based Pathways
Focal Therapy
Psychological Support
Nutrition
Financial Guidance/Support
Hospice
Hair and Beauty
Complimentary Therapy
Palliative Care
Information
Fitness/Rehabilitation
Survivorship
Multi-Disciplinary Team/ Treatment
Planning
Patient Navigation
PCP/Cancer Physician Alignment
Replace fee for service networks with value based care models over time
Integrated oncology model lowers cost by 25% while improving the patient experience
December 12, 2011
22© 2011 OLIVER WYMAN | HLC008-01-820 December 12, 2011
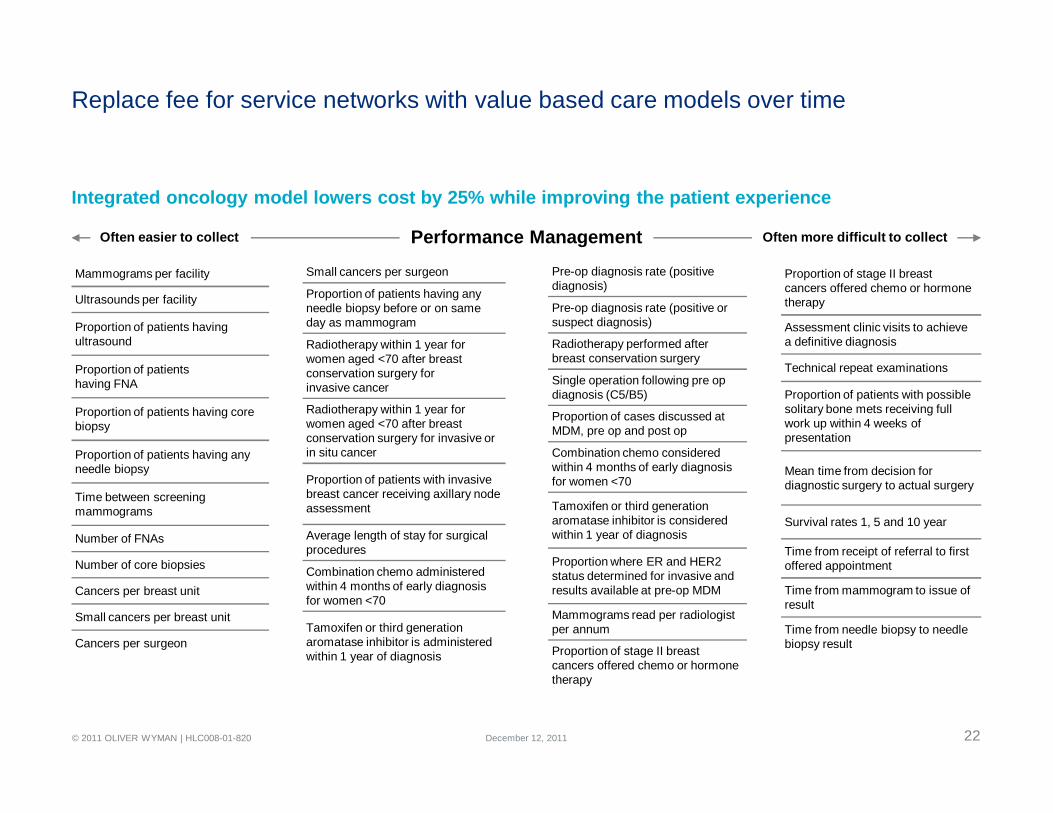
Mammograms per facility
Ultrasounds per facility
Proportion of patients having ultrasound
Proportion of patientshaving FNA
Proportion of patients having core biopsy
Proportion of patients having any needle biopsy
Time between screening mammograms
Number of FNAs
Number of core biopsies
Cancers per breast unit
Small cancers per breast unit
Cancers per surgeon
Small cancers per surgeon
Proportion of patients having any needle biopsy before or on same day as mammogram
Radiotherapy within 1 year for women aged <70 after breast conservation surgery forinvasive cancer
Radiotherapy within 1 year for women aged <70 after breast conservation surgery for invasive or in situ cancer
Proportion of patients with invasive breast cancer receiving axillary node assessment
Average length of stay for surgical procedures
Combination chemo administered within 4 months of early diagnosis for women <70
Tamoxifen or third generation aromatase inhibitor is administered within 1 year of diagnosis
Pre-op diagnosis rate (positive diagnosis)
Pre-op diagnosis rate (positive or suspect diagnosis)
Radiotherapy performed after breast conservation surgery
Single operation following pre op diagnosis (C5/B5)
Proportion of cases discussed at MDM, pre op and post op
Combination chemo considered within 4 months of early diagnosis for women <70
Tamoxifen or third generation aromatase inhibitor is considered within 1 year of diagnosis
Proportion where ER and HER2 status determined for invasive and results available at pre-op MDM
Mammograms read per radiologist per annum
Proportion of stage II breast cancers offered chemo or hormone therapy
Proportion of stage II breast cancers offered chemo or hormone therapy
Assessment clinic visits to achieve a definitive diagnosis
Technical repeat examinations
Proportion of patients with possible solitary bone mets receiving full work up within 4 weeks of presentation
Mean time from decision for diagnostic surgery to actual surgery
Survival rates 1, 5 and 10 year
Time from receipt of referral to first offered appointment
Time from mammogram to issue of result
Time from needle biopsy to needle biopsy result
Replace fee for service networks with value based care models over time
Integrated oncology model lowers cost by 25% while improving the patient experience
Often easier to collect Often more difficult to collectPerformance Management

23© 2011 OLIVER WYMAN | HLC008-01-820
Replace fee for service networks with value based care models over time
Health care goes retail
Closed ACO with patient-directed care
Closed ACO withpatient navigator
ACO with patient-centered medical home
• $500 per month premium• $150 monthly contribution
after subsidy • No co-pay• Silver benefits
• $425 per month premium• $75 monthly contribution
after subsidy • No co-pay • Silver benefits
• $400 per month premium• $50 monthly contribution after subsidy • No co-pay• Gold benefits
• Good community brand• Reputable physician panel
• Good community brand• Affiliation with an academic• Reputable physician panel• Patient navigator• 24-hour telephonic triage
• Good community brand• Reputable physician panel• 24-hour telephonic triage • Wellness program with
integrated fitness• Health coach
ACOs become exchange eligible community products and complete on value
December 12, 2011

24© 2011 OLIVER WYMAN | HLC008-01-820
Replace fee for service networks with value based care models over time
Health care goes retail
Healthy independentconsumer network
Lower income working classfamily network
Poly-chronic consumer network?
• Retailer walk-in clinic (Walgreens)• e-health primary care access
(American Well or Google +)• Social media community • Local community health system• Center of excellence (Mayo)
• Walmart exclusive for pharmacy and walk-in clinic
• Designated patient centered medical home with integrated AICU
• Community ACO with a value specialist network
• Meets key needs• Saves money• Offers Value-adds (fitness center,
life insurance, etc.)
• Meets critical family healthcare needs• Affordable• Better patient care
Consumer needs driven network models
December 12, 2011
25© 2011 OLIVER WYMAN | HLC008-01-820
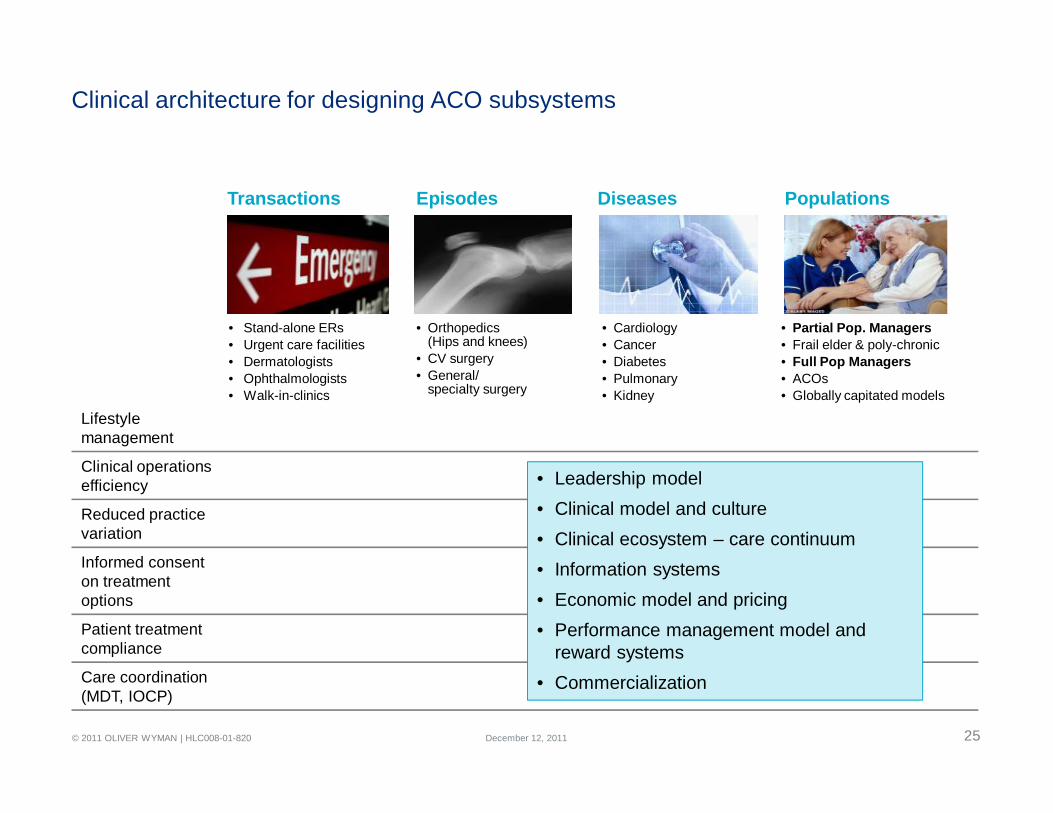
Clinical architecture for designing ACO subsystems
Transactions Episodes Diseases Populations
• Stand-alone ERs• Urgent care facilities• Dermatologists• Ophthalmologists• Walk-in-clinics
• Orthopedics (Hips and knees)
• CV surgery• General/
specialty surgery
• Cardiology• Cancer• Diabetes • Pulmonary• Kidney
• Partial Pop. Managers• Frail elder & poly-chronic• Full Pop Managers• ACOs• Globally capitated models
Lifestylemanagement
Clinical operations efficiency
Reduced practice variation
Informed consent on treatment options
Patient treatment compliance
Care coordination (MDT, IOCP)
• Leadership model• Clinical model and culture• Clinical ecosystem – care continuum• Information systems• Economic model and pricing• Performance management model and
reward systems• Commercialization
December 12, 2011
26© 2011 OLIVER WYMAN | HLC008-01-820
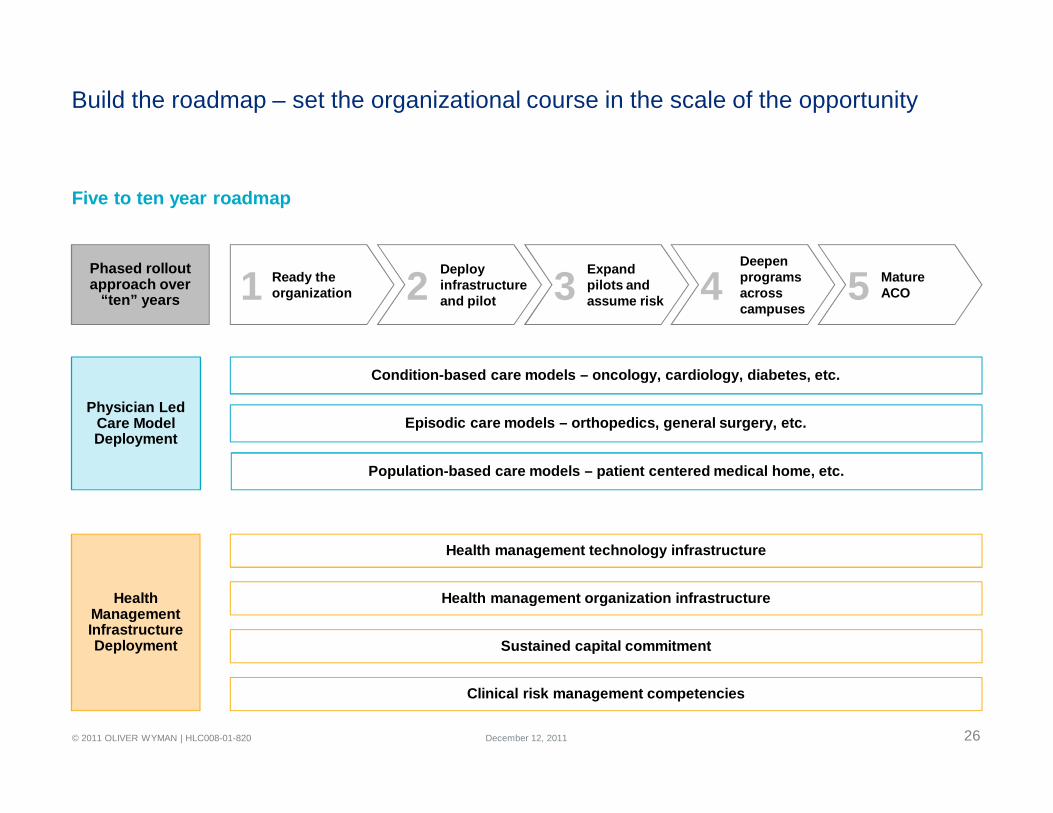
Build the roadmap – set the organizational course in the scale of the opportunity
Condition-based care models – oncology, cardiology, diabetes, etc.
Episodic care models – orthopedics, general surgery, etc.
Population-based care models – patient centered medical home, etc.
Health management technology infrastructure
Health management organization infrastructure
Sustained capital commitment
Clinical risk management competencies
Phased rollout approach over
“ten” years
Physician Led Care Model Deployment
Health Management Infrastructure Deployment
Mature ACO
Deepen programs across campuses
Expandpilots andassume risk
Deployinfrastructureand pilot
Ready the organization1 2 3 4 5
Five to ten year roadmap
December 12, 2011
27© 2011 OLIVER WYMAN | HLC008-01-820
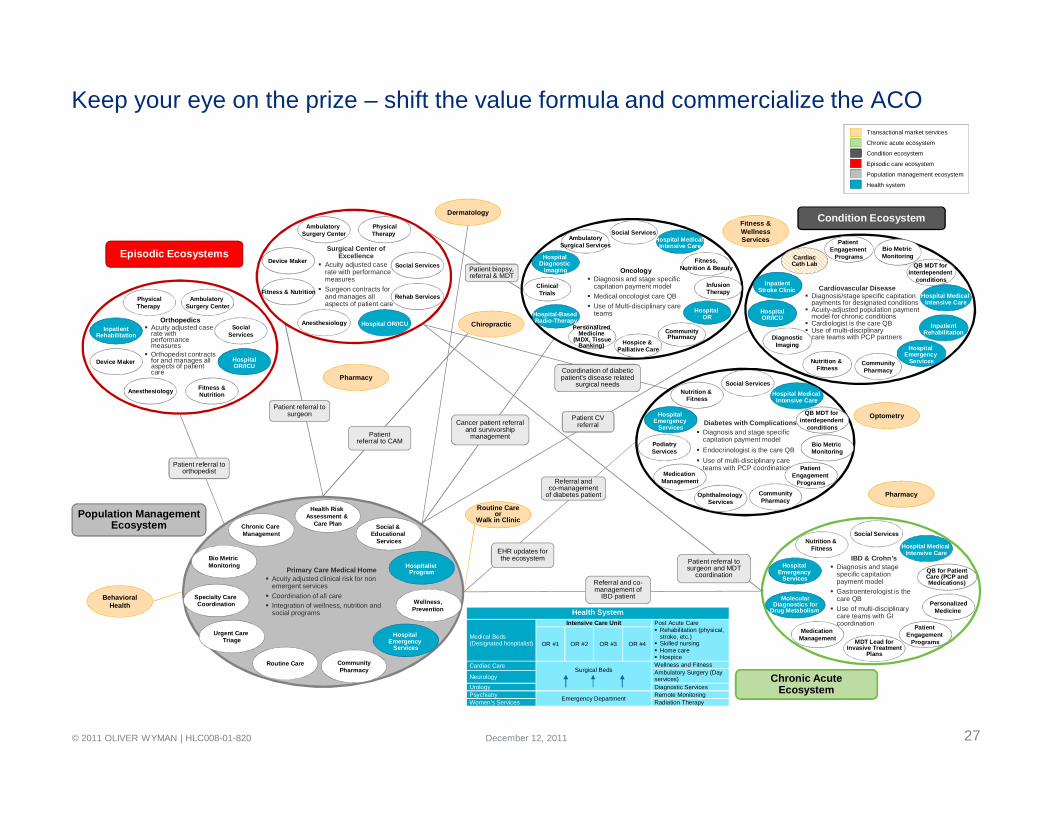
Keep your eye on the prize – shift the value formula and commercialize the ACO
Health System
Medical Beds(Designated hospitalist)
Intensive Care Unit Post Acute Care Rehabilitation (physical,
stroke, etc.) Skilled nursing Home care Hospice
OR #1 OR #2 OR #3 OR #4
Cardiac CareSurgical Beds
Wellness and FitnessAmbulatory Surgery (Day services)Neurology
Urology Diagnostic Services Psychiatry Emergency Department Remote MonitoringWomen’s Services Radiation Therapy
IBD & Crohn’s Diagnosis and stage
specific capitation payment model
Gastroenterologist is the care QB
Use of multi-disciplinary care teams with GI coordination
MolecularDiagnostics for
Drug Metabolism
Orthopedics Acuity adjusted case
rate with performance measures
Orthopedist contracts for and manages all aspects of patient care
Ambulatory Surgery Center
PhysicalTherapy
Device Maker
Anesthesiology
SocialServices
Fitness &Nutrition
HospitalOR/ICU
Surgical Center of Excellence
Acuity adjusted caserate with performance measures
Surgeon contracts for and manages allaspects of patient care
Ambulatory Surgery Center
PhysicalTherapy
Device Maker
Anesthesiology
Social Services
Fitness & Nutrition
Hospital OR/ICU
Episodic Ecosystems
Rehab Services
Condition Ecosystem
Patient biopsy, referral & MDT
Patient referral to surgeon
Coordination of diabetic patient’s disease related
surgical needs
Routine Care or
Walk in Clinic
Dermatology
Chiropractic
Cancer patient referraland survivorship
management
Hospital Emergency
Services
Nutrition & Fitness
Patient Engagement
Programs
Social Services
QB for PatientCare (PCP andMedications)
Hospital Medical Intensive Care
MDT Lead forInvasive Treatment
Plans
Medication Management
PersonalizedMedicine
Chronic AcuteEcosystem
Patient referral to orthopedist
Population Management Ecosystem
Patient CV referral
Patientreferral to CAM
Patient referral to surgeon and MDT
coordination
Optometry
Oncology Diagnosis and stage specific
capitation payment model Medical oncologist care QB Use of Multi-disciplinary care
teams
Hospital Diagnostic
Imaging
AmbulatorySurgical Services
Hospice & Palliative Care
ClinicalTrials
Social Services
Fitness,Nutrition & Beauty
Hospital-Based Radio-Therapy
Hospital Medical Intensive Care
Hospital OR
Personalized Medicine
(MDX, TissueBanking)
InfusionTherapy
Fitness & Wellness Services
Primary Care Medical Home Acuity adjusted clinical risk for non
emergent services Coordination of all care Integration of wellness, nutrition and
social programs
Bio Metric Monitoring
Chronic Care Management
Hospital Emergency
Services
Specialty Care Coordination
Health Risk Assessment &
Care Plan
Hospitalist Program
Social & Educational
Services
Routine Care
Urgent Care Triage
Wellness, Prevention
Referral andco-management
of diabetes patient
Behavioral Health
Diabetes with Complications Diagnosis and stage specific
capitation payment model Endocrinologist is the care QB Use of multi-disciplinary care
teams with PCP coordination
Hospital Emergency
Services
Nutrition & Fitness
Patient Engagement
Programs
PodiatryServices
Social Services
QB MDT for interdependent
conditions
Ophthalmology Services
Medication Management
Bio Metric Monitoring
Hospital Medical Intensive Care
InpatientRehabilitation
Diagnosis/stage specific capitation payments for designated conditions
Acuity-adjusted population paymentmodel for chronic conditions
Cardiologist is the care QB Use of multi-disciplinary
care teams with PCP partners
Nutrition & Fitness
Hospital Emergency
Services
Hospital Medical Intensive Care
QB MDT for interdependent
conditions
Bio Metric Monitoring
Patient Engagement
Programs
DiagnosticImaging
HospitalOR/ICU
CardiacCath Lab
InpatientRehabilitation
InpatientStroke Clinic Cardiovascular Disease
EHR updates for the ecosystem
Referral and co-management of
IBD patient
Pharmacy
Pharmacy
Population management ecosystem
Episodic care ecosystem
Condition ecosystem
Transactional market services
Health system
Chronic acute ecosystem
CommunityPharmacy
CommunityPharmacy
CommunityPharmacy
CommunityPharmacy
December 12, 2011

28© 2011 OLIVER WYMAN | HLC008-01-820 December 12, 2011
THE VOLUME TO VALUE REVOLUTIONSection 3

29© 2011 OLIVER WYMAN | HLC008-01-820
Healthcare 2020 drivers
• The current system will be bankrupt without change – CMS, Medicaid, employers and individuals
• $3 TN market with 5% growth and unhappy customers will stimulate investment and disruptive innovation
• Consumer demand will reshape the basis of competition
• CMS-led value based payment models will drive health systems to organize around value
• Cloud computing – digitization and integration (EHR, PHR, EBM) will enable vastly improved healthcare organizations
• Personalized medicine and genomics will drive “market of one” thinking
• Healthcare will be much more virtual and global – even service delivery
• Social media, gaming and communities will reshape consumer expectations and accelerate change
• Industry convergence (four chain) will create new world healthcare organizations – health, media, finance, lifestyle, IT
Reshaping healthcare for the next generationThree quarters of the cost, one and half times the value with a radically improved patient experience
December 12, 2011

30© 2011 OLIVER WYMAN | HLC008-01-820
The Customer’s Hassle Map
The customer’s hassle map
Business model redesign starts with the customer hassle map
Risk Management/Administration
Care Delivery
Healthcare I/T
Personal Health Management
The market convergence players master a new game
• Start with the customer, not the “home team” value chain
• Get the customer’s hassle map down with great detail and accuracy
• Connect the dots from multiple chains (software, mobile, content, device, etc.) to create an elegant solution for the customer, a solution that radically improves the hassle map
December 12, 2011
31© 2011 OLIVER WYMAN | HLC008-01-820
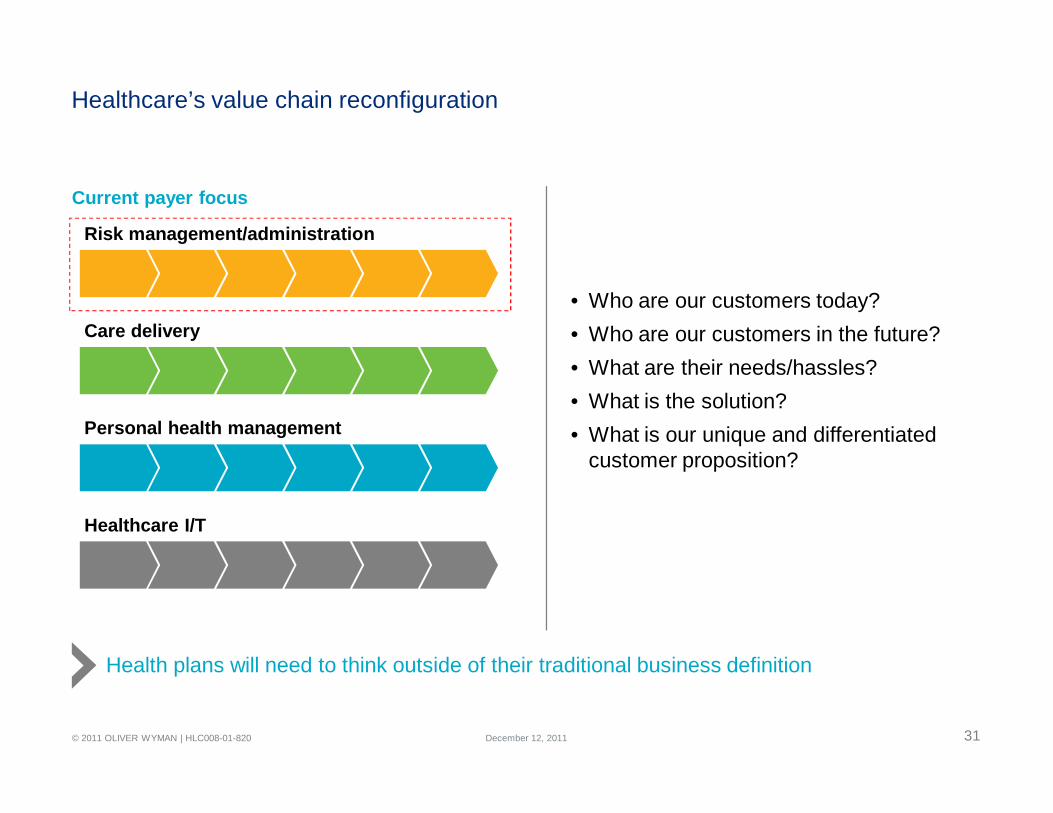
Current payer focus
Healthcare’s value chain reconfiguration
• Who are our customers today? • Who are our customers in the future?• What are their needs/hassles?• What is the solution?• What is our unique and differentiated
customer proposition?
Risk management/administration
Personal health management
Care delivery
Healthcare I/T
Health plans will need to think outside of their traditional business definition
December 12, 2011
32© 2011 OLIVER WYMAN | HLC008-01-820
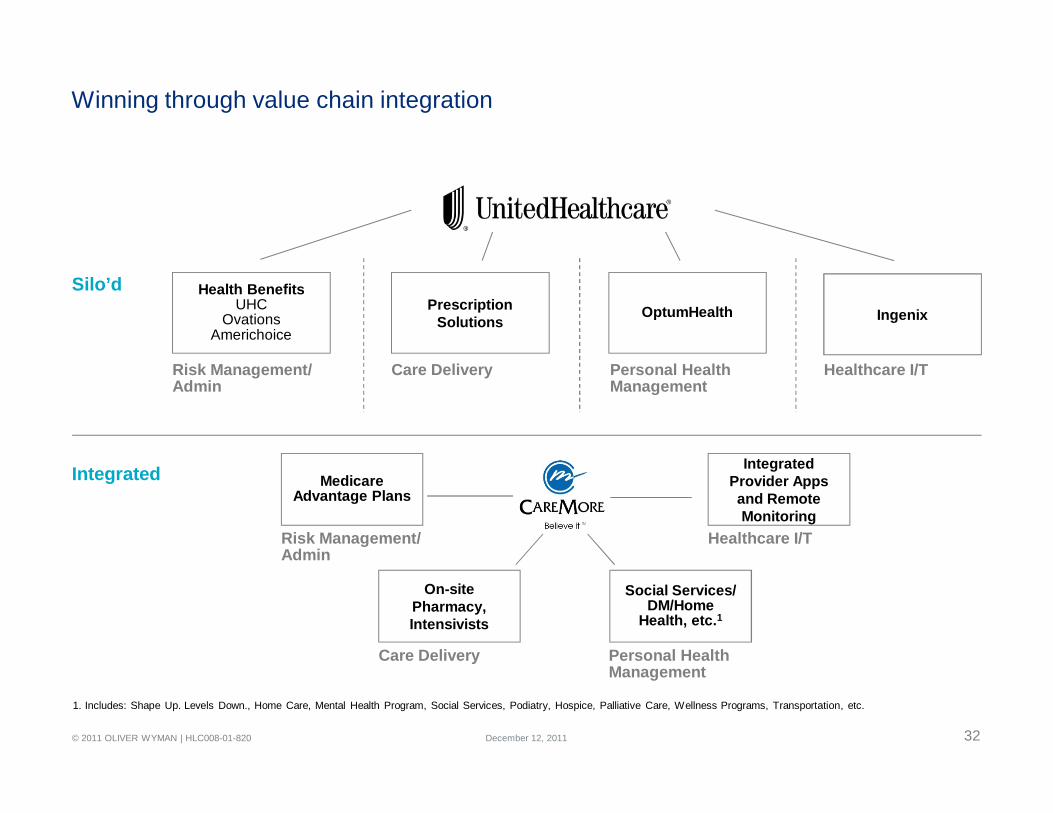
Winning through value chain integration
Health BenefitsUHC
OvationsAmerichoice
OptumHealth
Risk Management/ Admin
Ingenix
Healthcare I/TPersonal Health Management
PrescriptionSolutions
Care Delivery
Medicare Advantage Plans
On-site Pharmacy, Intensivists
Social Services/DM/Home
Health, etc.1
Integrated Provider Apps and Remote Monitoring
Healthcare I/T
Care Delivery
Risk Management/ Admin
Personal Health Management
Silo’d
Integrated
1. Includes: Shape Up. Levels Down., Home Care, Mental Health Program, Social Services, Podiatry, Hospice, Palliative Care, Wellness Programs, Transportation, etc.
December 12, 2011
33© 2011 OLIVER WYMAN | HLC008-01-820
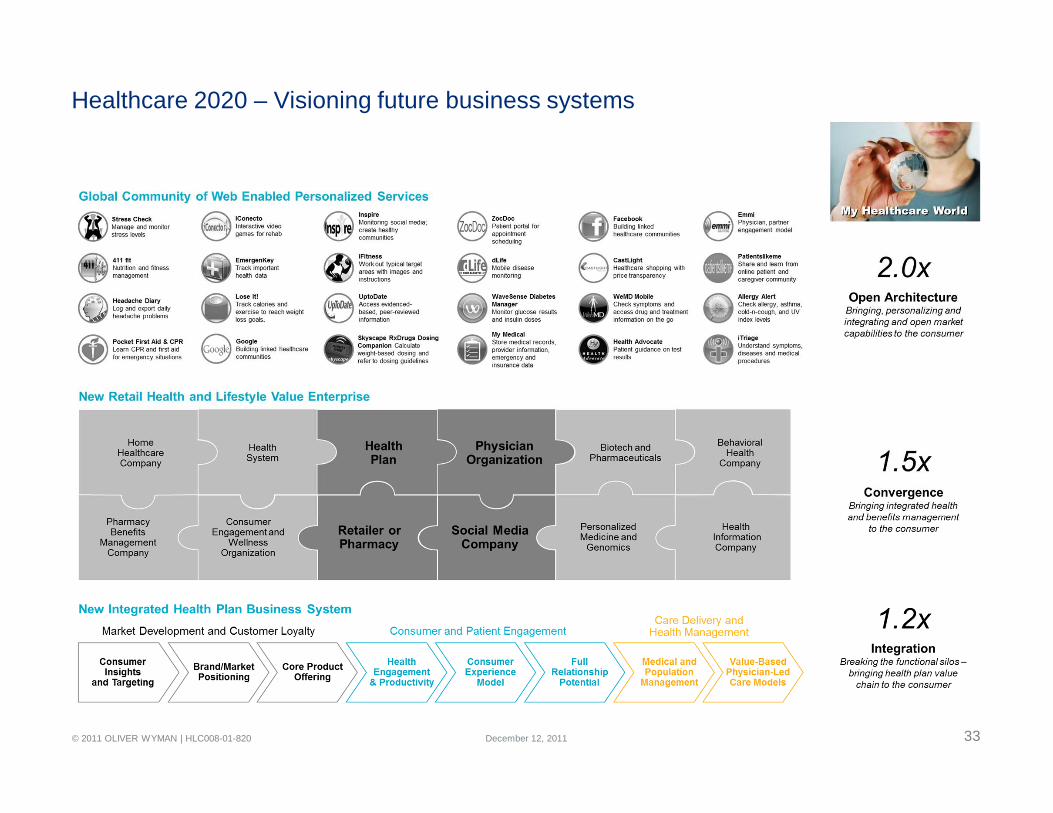
Healthcare 2020 – Visioning future business systems
December 12, 2011

34© 2011 OLIVER WYMAN | HLC008-01-820
Early signs of convergence
+
+ + +
+ ++ +
Health Plan and Health System
National Plan and HIT
Retail Pharmacy and Clinic
+
+
+ + +
+
+
+Powered by:
December 12, 2011
35© 2011 OLIVER WYMAN | HLC008-01-820 December 12, 2011
THE RACE TO VALUESection 4

36© 2011 OLIVER WYMAN | HLC008-01-820
Consumer demand redefines competition – web 2.0 expectations meet healthcare
• Personalized networks• Value based benefit plans • Integrated product and service lifestyle
packages • Health coaches – with connected homes• Web based healthcare shopping services
with performance transparency• e-pharmacist access models• Social communities with expert advisors• Personalized integrated mobile applications • Gaming and personalized avatar applications• 24 hour e-health triage services
• Personalized hassle free easy-to-use healthcare services
• Personalized solutions leading to greater engagement
• Personalized provider networks • Integrated solutions – meeting health,
lifestyle and financial needs• Value based benefits creating aligned
incentives to motivate behavioral changes• Personalized coaching and lifestyle/health
itinerariesLose It!
Track calories and exercise.
iFitnessWork out typical target areas with images and
instructions.
Natural CuresTreat conditions with natural and prescription therapies.
WaveSense Diabetes Manager
Monitor glucose results and insulin doses.
iTriageUnderstand diseases and medical procedures.
My MedicalStore medical records,
provider information, and insurance data.
WebMD Mobile Check symptomson the go.
Allergy Alert
Patientslikeme Online patient and caregiver community.
Stress Check Manage and monitor stress levels
Health Cloud Access Google Health records.
Headache Diary
Consumer engagementTransforming the consumer experience – a bridge to better health
Improving healthcare quality while bending the trend through active consumer engagement
Staying on top of your healthcare needs
December 12, 2011

37© 2011 OLIVER WYMAN | HLC008-01-820
Empowered point-of-care with personalized actionable insights – the last mile
• Meaningful use – $44 BN
• Electronic health record adoption
• Embedded order sets
• Patient history
• Embedded pharmacy formulary
• Lifestyle factors
• Patient itinerary
• Patient portals
• Mobile applications
• More complete health evaluation
• Improved patient engagement
• Improved treatment compliance
• Preventative focus where there arerisk factors
• Reduction of unwarranted practice variation
• Improved quality – drug interaction, care alerts, screening, etc.
Electronic health record Transforming the point-of-care
Improving healthcare quality whilebending the trend
Perfecting thepoint of care
December 12, 2011
38© 2011 OLIVER WYMAN | HLC008-01-820
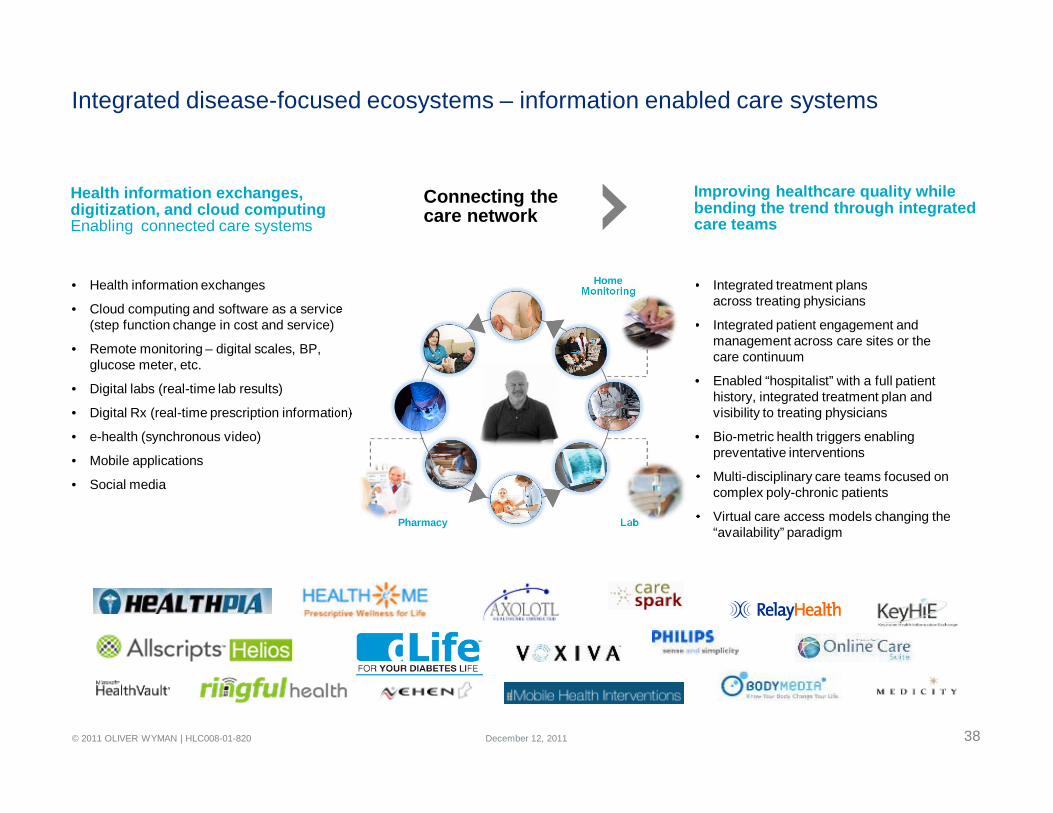
Integrated disease-focused ecosystems – information enabled care systems
• Health information exchanges
• Cloud computing and software as a service (step function change in cost and service)
• Remote monitoring – digital scales, BP, glucose meter, etc.
• Digital labs (real-time lab results)
• Digital Rx (real-time prescription information)
• e-health (synchronous video)
• Mobile applications
• Social media
• Integrated treatment plans across treating physicians
• Integrated patient engagement and management across care sites or the care continuum
• Enabled “hospitalist” with a full patient history, integrated treatment plan and visibility to treating physicians
• Bio-metric health triggers enabling preventative interventions
• Multi-disciplinary care teams focused on complex poly-chronic patients
• Virtual care access models changing the “availability” paradigm
Health information exchanges, digitization, and cloud computing Enabling connected care systems
Improving healthcare quality while bending the trend through integrated care teams
Home Monitoring
LabPharmacy
Connecting thecare network
December 12, 2011

39© 2011 OLIVER WYMAN | HLC008-01-820
New cloud enabled ACOs – from information to actionable insights
• Patient registries or databases
• Comprehensive patient or consumer profiles – health history, health status, lifestyle, behaviors
• Genomic profiles and tissue banking
• Evidence based guidelines – integrated health literature, clinical trial results, published studies
• Physician and health system databases with related attributes – treatment, cost and outcomes
• Clinical population segment information –treatment, costs and outcomes
• Disease and condition information –treatment, costs and outcomes
• Consumer stratification and clinical segmentation by health need – 15%/55% rule
• Patient-panel stratification for physician practices to shift to population management
• Real-time EBM guidelines with clinical economics at point of care
• Virtual shared treatment plans enabling MDTs – reducing practice variation and duplicate services
• Poly chronic patient care guidelines –addressing high cost clinical segments
• Social media with leader boards and information transparency – accelerating positive change
Health informatics and cloud computingTransforming the system though personalized actionable insights
Improving healthcare quality while bending the trend through actionable insights
Home Monitoring
LabPharmacy
Labfeeds
ResearchStudies
Clinical Trials
GenomicsCMSData
ProviderDB
PersonalizedActionable
Insights
HealthyIndependent
Health RiskFactors
Complex/Polychronic
Connected carenetwork
PatientDB
VBEBM
Powering the system thru the health cloud
December 12, 2011
40© 2011 OLIVER WYMAN | HLC008-01-820
New care models that shift the value equation (95% of the price with 20% more value)
• Retail clinics, PCMH, IOCP, and triage models
• Health coaches – with connected homes• e-health (synchronous interactive video)
consults• e-health for primary care and
specialists consults • Global center of excellence network• Social communities with expert advisors
for selected health populations• Global labor sourcing and 24 hour
e-health services• Social media (gaming) and personalized
avatar applications
• Healthy routine care models meet consumer needs and improve value
• Specialized care models for poly chronic patients (15/55)
• Integrated episodic care models with outcomes measures for procedural medicine i.e. surgery, knee replacement, etc.
• 24 hour triage services to eliminate most unnecessary emergency department visits
• Retail pharmacist – led medication management programs with 24 hour e-health wrap around
• Integrated condition management programs with patient navigators
Glucose Buddy
Symptom Navigator
Aetna Mobile
Care model innovation
Integrated orthopedic center of excellence
Intensivist care model for poly chronic
patientsRetail pharmacist and medication manager
Health coach with an integrated social,
behavioral, clinical engagement model
e-health 24 hour urgent care triage Routine care clinic
Value-based healthcare designed around the patientHealthcare “your way” – personalizing the system while transforming access and service
Improving healthcare quality while bending the trend through care model innovation
Designing around the patient’s needs
December 12, 2011
41© 2011 OLIVER WYMAN | HLC008-01-820
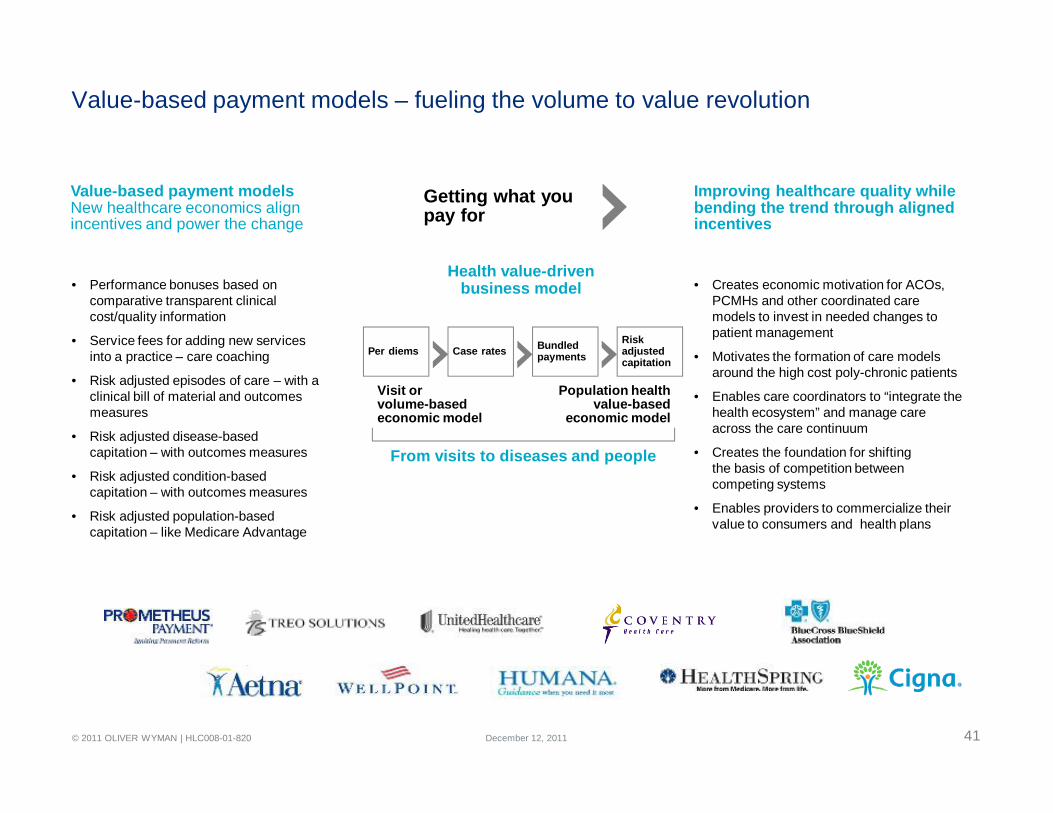
Value-based payment models – fueling the volume to value revolution
Health value-driven business model• Performance bonuses based on
comparative transparent clinical cost/quality information
• Service fees for adding new services into a practice – care coaching
• Risk adjusted episodes of care – with a clinical bill of material and outcomes measures
• Risk adjusted disease-basedcapitation – with outcomes measures
• Risk adjusted condition-based capitation – with outcomes measures
• Risk adjusted population-based capitation – like Medicare Advantage
• Creates economic motivation for ACOs, PCMHs and other coordinated care models to invest in needed changes to patient management
• Motivates the formation of care models around the high cost poly-chronic patients
• Enables care coordinators to “integrate the health ecosystem” and manage care across the care continuum
• Creates the foundation for shiftingthe basis of competition between competing systems
• Enables providers to commercialize their value to consumers and health plans
Value-based payment modelsNew healthcare economics align incentives and power the change
Improving healthcare quality while bending the trend through aligned incentives
Per diems Case rates Bundled payments
Risk adjusted capitation
Visit orvolume-based economic model
Population healthvalue-based
economic model
From visits to diseases and people
Getting what you pay for
December 12, 2011

42© 2011 OLIVER WYMAN | HLC008-01-820
Commercializing value-based solutions – public and private exchanges
Finding theperfect healthcare
Consumer segment specific products
Value based competitionwith lots of choice
• 76% of the 51 MM uninsured expressed intent to buy on the public exchanges –39 MM new insureds
• Small group and self funded employers will send another 46 MM shopping
• Consumers will be shopping for “best value” health benefits – measured by expected out-of-pocket costs and value
• Exchanges will provider consumers with tools to easily compare health plan offerings
• Web application players will bring personalized decision engines and advisors to guide consumer decision making
• Private exchanges will embrace a wide variety of health and lifestyle services
• Federalized bronze/silver product standards motivates new entrants
• Health plans differentiate on value – mostly through new network strategies
• Consumers shop for healthcare through the exchange – net costs drives decisions
• Web applications enable consumer shopping• Social media creates a “dialog” about what
to buy – transparent rating systems• Private exchanges for non-Federally
subsidized consumers offer a broad menu of services
• e-brokers bring personalization and shopping advice
• Mobile web applications help consumer predict future health needs
Shopping exchangesConsumers will make very different decisions than their employers made for them
85 MM consumers with $500 BN of purchasing power will change healthcare forever
December 12, 2011
43© 2011 OLIVER WYMAN | HLC008-01-820
Unlocking value?
December 12, 2011