hiv prevention, treatment and care among people who inject drugs fabienne hariga, md, mph senior hiv...
TRANSCRIPT

HIV Prevention, treatment and care amongpeople who inject drugs
Fabienne Hariga, MD, MPHSenior HIV Adviser, UNODC Vienna

Co-sponsor
HIV among People who Use Drugs
HIV in Prison
Settings
CONVENING AGENCY

Prevalence of HIV among people who inject drugs12.7 million PWID (0.27 % )
1.7 million PWID living with HIV (13.1% of PWID)52% with hepatitis C
Source: World Drug report 2014

HIV AND PEOPLE WHO INJECT DRUGS IN PRISONS

JOINT UN RECOMMENDED INTERVENTIONSComprehensive Package of interventions for HIV prevention,
treatment and care among people who inject drugs
1. Needle and syringe programmes (NSPs)2. Opioid substitution therapy (OST) and other evidence-based drug
dependence treatment3. HIV testing and counselling (HTC)4. Antiretroviral therapy (ART)5. Prevention and treatment of sexually transmitted infections (STIs)6. Condom programmes for people who inject drugs and their sexual
partners7. Targeted information, education and communication (IEC) for
people who inject drugs and their sexual partners8. Prevention, vaccination, diagnosis and treatment for viral hepatitis9. Prevention, diagnosis and treatment of tuberculosis (TB).

Effectiveness of NSP Reduction in the rate of HIV transmission (and
HCV) Frequency of unsafe injection (risk HIV and HCV)
No initiation of injecting among people who have not injected previously
No increase in the duration or frequency of illicit drug use or drug injection
Allow for IEC Allow for referral to OST, HTC or ARV and TB
Reduce number of used syringes discarded in public areas
Bleach is not an effective alternative especially for Hepatitis C
HIV (and hepatitis C or B) is transmitted among people who inject drugs through sharing
injection equipment

Opioid use Frequency of injection & unsafe injection (risk HIV and
HCV) Risk of overdoses Risk of abortion/miscarriage of pregnant opiate dependent
women
Increase retention in drug dependence treatment Adherence to treatment (ARV , TB, Hepatitis C) Improve health status and wellbeing Social functioning Work and productivity and economic status
Criminal behaviour Recidivism Violence, drug seeking in prison
Reduction in the rate of HIV transmission (and HCV)
Effectiveness of OST

Why a comprehensive approach?
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
2021
2022
2023
2024
2025
2026
2027
2028
2029
2030
0
200000
400000
600000
800000
1000000
1200000
baseline substitution (only)
needle exhange only comprehensive harm reductions
Pe
op
le li
vin
g w
ith H
IV (
mill
ion
s)
Source: Sarkar et al, 2008
Universal Access
• Physically accessible – geographically distributed – Hard to reach location
• Affordable – patients should not have to pay for their treatment
• Equitable and non-discriminatory – no exclusion criteria except medical ones, e.g. – OST should not be limited to only those IDUs who are HIV infected or who
have failed on other drug dependence treatment– No compulsory treatment
• Non-rationed – supply should be determined by need: – e.g. needle and syringe programmes with strict limits on the number of
syringes provided to each client are less successful than those that do not impose such restrictions
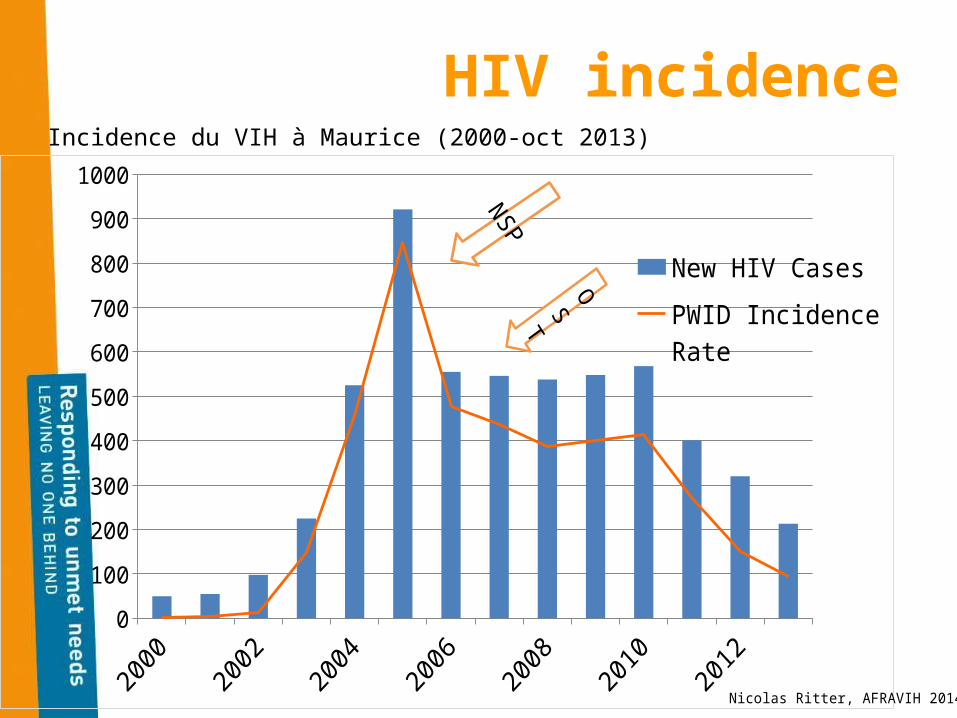
HIV incidence
0
100
200
300
400
500
600
700
800
900
1000
New HIV Cases
PWID Incidence Rate
Nicolas Ritter, AFRAVIH 2014
Incidence du VIH à Maurice (2000-oct 2013)
NSP

PRINCIPLES
Prison health is public health Linkages with public health and
community programmes
Human rights based and gender sensitive Principle of equivalence Medical ethics No segregation of PLWH;
Criminal justice reforms to reduce the prison population Alternatives to imprisonment Reduce pre-trial incarceration End compulsory detention of drug users
and sex workers for “rehabilitation” Prison reforms
Ensure safe prison conditions Prevent violence Proper classification Conjugal visiting rooms

12
Harm reduction in prisons
New HIV Infections in Lithuanian prisons
Intervention Availability
NSP No
OST No
HIV Testing Yes
ARV Therapy 18%
Harm Reduction Education
5 pilot projects
Source: UNODC S. Rotberga, Tallinn, 2011
New HIV Infections in Spanish prisons
Intervention Availability
NSP Yes, 30 Prisons
OST10.2% of inmates (6,429 in 2010)
HIV Testing 76.10%
ARV Therapy64.6%
(2,668 in 2010)
Peer Health Education
100%
Increase of HIV in Lithuanian prisons in the absence of prevention services
Decrease of HIV in Spanish prisons in the presence of prevention services
Source: Enrique Acín García, M.D., Head of Public Health Department. General Secretariat of Penitentiary Institutions. Ministry of Interior. Spain.
3 1
10
28
0
5
10
15
20
25
30
2006 2007 2008 2009 2010 2011
Ne
w H
IV I
nfe
cti
on
s i
n P
ris
on
s (
#)
0.60%
0.70%
0.14%
0.15% 0.17%0.15%
0.06%
0.16%
0.09%
0.08%0%
in 20100.0%
0.1%
0.2%
0.3%
0.4%
0.5%
0.6%
0.7%
0.8%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
HIV
Pre
va
len
ce
in
Sp
an
ish
Pri
so
ns
(%
)

Stigma
Bottlenecks

Critical enablers
• Supportive legal and policy framework
• Supportive law enforcement practices
• Empowerment of people who use drugs
• Alternatives to imprisonment including decriminalisation of drug use
Appropriate funding

New publications:
• Police, HIV and PWID: a training manual
• Policy brief on HIV and women who inject drugs
• Handbook on needle and syringe programmes in prisons

…Unfortunately, many national drug control systems rely on sanctions and imprisonment, rather than evidence-based health care in full compliance with human rights standards …
… These are major barriers to HIV and to harm reduction services, including in prisons and other closed settings…
UNAIDS Programme Coordinating Board,1
July 2014
