hiv exposure does not worsen outcome in stage iii necrotizing enterocolitis with current treatment...
TRANSCRIPT
www.elsevier.com/locate/jpedsurg
Journal of Pediatric Surgery (2012) 47, 665–672
HIV exposure does not worsen outcome in stage IIInecrotizing enterocolitis with current treatment protocolsMarion Arnold, Samuel W. Moore⁎
Division of Paediatric Surgery University of Stellenbosch, Cape Town, South Africa
Received 13 June 2011; revised 16 November 2011; accepted 16 November 2011
MS
0d
Key words:Necrotizing enterocolitis(NEC);
Human immunodeficiencyvirus (HIV);
Risk factors;Surgery;Prematurity;Neonates
AbstractBackground/Purpose: The heavy burden of maternal HIV infection in developing countries such asSouth Africa has resulted in a high prevalence of premature birth and necrotizing enterocolitis (NEC).Uninfected infants born to HIV-infected mothers also demonstrate immune deficiencies. It is, therefore,essential to have a better understanding of how to mitigate HIV as an independent risk factor forsurgically treated NEC and to evaluate the relevant contributing factors in the presence of an aggressivestrategy of pasteurized breast milk feeding and antiretroviral prophylaxis.Methods: Infants with stage IIIb NEC presenting over a 4-year period were retrospectively reviewed.HIV-exposed infants were compared with non–HIV-exposed infants. Contributing factors wereevaluated and studied by systematic statistical methods to evaluate risk.Results: Twenty percent (17/87) infants were HIV-exposed, and 80% (70/87), unexposed, whereas afurther 10 (total, n = 97) had unknown HIV exposure status. Demographics and other perinatal riskfactors between the 2 groups were not significantly different other than that HIV-exposed infantsreceived pasteurized breast milk and nonexposed infants received unpasteurized breast milk. There wereno statistically significant differences between the groups with respect to disease presentation orseverity, surgical findings or type of surgery, postoperative complications, survival, or timing of death.Trends toward higher antenatal steroid exposure and increased postoperative sepsis in the HIV-exposedgroup (P = .03) were noted but were not related. All HIV-exposed infants received antiretrovirals; therewere no significant differences on subanalysis between different antiretroviral regimens.Conclusions: HIV-exposed infants do not have a more severe disease course nor more adverse outcomesin stage IIIb NEC than unexposed infants. Significant factors were antenatal steroids and post-NECinfective episodes.© 2012 Elsevier Inc. All rights reserved.
1. Background
⁎ Corresponding author. Division of Paediatric Surgery, Faculty ofedicine, University of Stellenbosch, PO Box 19063, Tygerberg 7505,outh Africa. Tel.: +27 21 9389280; fax: +27 21 9337999.E-mail address: [email protected] (S.W. Moore).
022-3468/$ – see front matter © 2012 Elsevier Inc. All rights reserved.oi:10.1016/j.jpedsurg.2011.11.047
Maternal HIV infection has been identified as anindependent risk factor for neonatal necrotizing enterocolitis(NEC) [1] and is associated with a high incidence of pretermlabor and premature birth [2]; thus, the burden of NEC in theHIV-exposed newborn population is significant. Importantly,maternal HIV infection has previously been linked with a

666 M. Arnold, S.W. Moore
doubling of mortality in infants with NEC requiring surgicalintervention [3]. The impact of maternal HIV in these infantsin the current era of prophylactic antiretroviral therapy anddonor/pasteurized breast milk feeds is unknown.
HIV infection with AIDS is well known to be associatedwith a worse outcome in surgical patients [4-7]. However,the role of HIV infection in postoperative recovery may beless significant than the nature of the surgery per se and age-related factors in young children [8]. HIV-uninfected infantsborn to infected mothers may also demonstrate immunedeficiencies [9-15], which could influence their outcome,particularly in advanced NEC.
Premature infants with NEC requiring surgical interven-tion are severely ill and have a high overall mortality (30%-50%). The outcome of surgically treated neonates with NECis good in some, but these patients may often developdevastating long-term complications, including poor neuro-developmental outcomes and increased infectious morbidityand mortality [16,17]. All of these could possibly beadversely affected by HIV exposure [18], but HIV exposureas a risk factor cannot be looked at in isolation because of themultiple factors, which put infants at risk for NEC.
In the light of the overall paucity of data on the outcomeof HIV-exposed uninfected infants, identification andmitigation of the multiple risk factors for NEC in the NEC-HIV setting are essential to limit the incidence and impact ofthe disease in the vulnerable HIV-exposed population. Theimpact of impaired immunity in this subgroup in theperioperative period also requires further investigation.
1.1. Aim
The aim of this study is to evaluate the diseasepresentation, progression, and outcome in stage III NECamong HIV-exposed compared with unexposed infants.
2. Method
Infants with stage III NEC presenting to the pediatricsurgery department at Tygerberg Children's Hospital over a4-year period, who were considered to have full-thicknessgut necrosis based on clinical and radiologic criteria(including pneumoperitoneum, fixed dilated intestinal loopor increasing ascites in association with persistent metabolicdeterioration, abdominal wall erythema, tender abdominalmass, worsening metabolic acidosis not responding toresuscitative measures), were retrospectively reviewed.HIV-exposed infants were compared with non–HIV-ex-posed infants with respect to the following:
(A) Demographics (gestational age, birth weight, sex);(B) Other known risk factors for NEC or bowel perforation
(formula feeding and lack of breast milk exposure [19];maternal syphilis [20]; weight below third centile for
gestational age [21]; cardiac anomalies [22]; nonste-roidal anti-inflammatory (Nurofen) received for patentductus arteriosus closure [23,24]; blood transfusion inprevious 48 hours [25]; umbilical line placement andpolycythemia [26]; multiple birth; no antenatal steroidexposure [27,28]; hypoxic events causing impairedbowel blood flow [29] including hypoxic ischemicencephalopathy; inotrope exposure preceding NECdevelopment; maternal cocaine or methamphetamineabuse [29,30]; maternal preeclampsia/hypertension,elevated liver enzymes, low platelets; and hypogyly-cemic insults [31] as well as neonatal and maternalperinatal sepsis [32]);
(C) Disease presentation and surrogate markers fordisease severity (bacteremia detected on bloodculture); radiologic markers of severe NEC, SNAPPEII, and CRIB II scores [33-36]; metabolic parameters(pH, base excess, lactate, serum sodium, hyperglyce-mia), hematologic (white cell, polymorph, plateletcount, international normalized ratio [INR], C-reac-tive protein levels [37-39]) and hemodynamic param-eters (inotrope requirements [40]); and fulminantpresentation (gangrenous bowel within 24 hours ofpresentation) [41];
(D) Surgical findings (total gut necrosis, isolatedperforation as opposed to multiple perforations[42,43]) and type of surgery done (peritoneal drains[44], primary anastomosis [45], stoma [46]).Surgery was performed either by or under thesupervision of experienced pediatric surgeons accord-ing to a departmental protocol.
(E) Outcomes (death, timing of death in relation tosurgery, post-NEC sepsis, survival to stoma closure,survival to discharge home).
Antiretroviral exposure in the HIV-exposed group was alsoevaluated for the above parameters, comparing infants whoreceived antiretroviral prophylaxis for 1 week vs 1 month,which were given according to the South African nationalguidelines for the prevention of mother-to-child transmissionof HIV at the time [47,48]. Maternal CD4 counts [13] andinfant HIV–polymerase chain reaction (PCR) serology werecollated. HIV-PCR was repeated at or after 6 weeks of age inall HIV-exposed survivors.
2.1. Statistics
HIV-exposed and nonexposed groups were compared foreach variable using the Pearson χ2 test and Fisher's Exact test.Continuous variable parameters were assessed using the F testand Mann-Whitney U test after testing for homogeneity ofvariances. P b .05 was considered significant. P values were notcalculatedwhere sample sizewas too small to be significant. The1-tailed t test was used where clinically important for powercalculations where P values were insignificant but ≤.3 tomeasure the effect of the small sample size.

667HIV exposure does not worsen outcome in stage III NEC
3. Results
Eighty-seven of the NEC cohort had a known HIV status.Twenty percent (17/87) of these were exposed to maternalHIV virus, whereas 80% (70/87) were not. In a further 10(10.3%) of the 97, the HIV exposure status was unknown.Demographics were very similar between the exposed andunexposed groups, with a mean gestation of 30.64 (SD, ±3.12) in the HIV-exposed compared with 30.44 (SD, ±3.20)(P = .67) in the unexposed group and mean birth weights of1364 ± 432 g vs 1343 ± 504 g, respectively (P = .66). Male-female ratio was 1.43 in the exposed compared with 1.26 inthe unexposed group.
Table 1 reflects other potential perinatal risk factorsbetween the 2 groups. There was no significant differencebetween those HIV-exposed infants who received pas-teurized breast milk and unexposed infants receivingunpasteurized breast milk (power, 0. 48). More specifi-cally, there was no statistically significant differencebetween the groups with respect to disease presentation orseverity (Table 2), surgical findings or type of surgery(Table 3), postoperative complications, survival, or timingof death (Table 4).
Table 1 Comparison of incidence of perinatal risk factors for NEC ainfants with stage III NEC
Risk factors: NEC/bowel perforation
TOTAL (n=97; HIV status unknown in 10)Maternal & antenatal VDRL positive
Antenatal steroidsMaternal cocaine/metamphetamineMaternal PET/HELLP syndromeMaternal sepsis
Congenital Multiple birthBirth weight b3rd centile for gestationMajor congenital anomaly (not cardiac)Cardiac anomaly (incl. PDA)
Post-natal Nurofen to close PDANumber doses Nurofen (Mean)Umbilical linePolycythaemiaMultiple seizuresInotropes (before NEC episode)Neonatal sepsisHypoxic ischaemic encephalopathyHypoglycaemiaBlood transfusion b48 h before NEC
Feeding Exclusively breastmilkPasteurized EBMUnpasteurized EBMDonor EBMMixed (EBM & formula)Formula only
PET indicates preeclampsia; HELLP, hypertension, elevated liver enzymes, low⁎ Too small to calculate.
There was higher antenatal steroid exposure, andincreased postoperative sepsis in the HIV-exposed group(P = .03) was noted (Tables 1 and 4), and there was nocorrelation between antenatal steroid exposure and postop-erative sepsis (P = .73 for whole group; P = 1.0 for HIV-exposed subgroup). A trend toward earlier NEC presentationin the HIV-exposed group (mean, 9.5 compared with 13 daysof age) was not statistically significant owing to large overlapbetween the 2 groups (power, 0.43) and had no relationshipwith antenatal steroid use (P = .96). There was norelationship between antenatal steroid therapy and isolated(focal) NEC perforation (P = .78). Isolated single perforationat surgery was found in 18% of exposed compared with 9%of unexposed infants (P = .3; power, 0.34).
All HIV-exposed survivors were HIV-PCR negative atdischarge. There were no significant differences on sub-analysis between different antiretroviral regimens for any ofthe variables listed above (perinatal risk factors [P = .27-1.0],surgical findings and procedure performed [P = .27-.77],death or time of death [P = .85-1.0], postoperative sepsis[P = .3-.51], and survival to discharge home [P = .6-.84]).
Seven (44%) received a single dose of nevirapine (NVP),followed by 7 days of zidovudine (AZT), which was given
nd bowel perforation between HIV-exposed and HIV-unexposed
HIV exposed HIV non-exposed P
Total n % Total n %
87 17 20% 87 70 80%12 0 0% 69 4 6%16 8 50% 70 15 21% .0316 0 0% 70 2 3% ⁎
16 2 13% 70 17 24% .2816 2 13% 70 5 7% .5016 2 13% 70 5 7% .5017 2 12% 70 6 9% .6916 1 6% 70 2 3% ⁎
16 6 38% 70 22 31% .6416 4 25% 70 16 23% .8616 (0.31 ± 0.60) 70 (0.44 ± 0.91) .9816 0 0% 70 3 4% .2616 0 0% 70 3 4% .2616 1 6% 70 2 3% ⁎
16 0 0% 70 2 3% ⁎
16 3 19% 70 19 27% .4816 0 0% 70 1 1% ⁎
16 0 0% 70 3 4% ⁎
16 0 0% 70 4 6%12 6 50% 43 32 74% .1212 10 83% 43 1 2% .0012 0 0% 43 37 86% .0012 1 8% 44 4 9% .9312 4 33% 43 10 23% .4912 2 17% 44 3 7% .32
platelets; PDA, patent ductus arteriosus. P b .01 is considered significant.

Table 2 Comparison of disease presentation in HIV-exposed and HIV-unexposed infants with stage III NEC
Disease presentation HIV exposed HIV nonexposed P
Total n % Mean SD Total n % Mean SD
Age (d) at NEC presentation 17 8.8 4.9 70 13.2 12.0 .27Fulminant NEC 17 6 35% 70 25 36% .97Positive blood culture ≤5 d of presentation 17 5 29% 70 27 39% .48Radiologic Pneumoperitoneum 15 10 67% 66 38 58% .51
Portal venous gas 14 4 29% 65 10 15% .26Pneumatosis intestinalis in3-4 quadrants
14 8 57% 62 25 40% .25
Physiologic SNAPPE II score 15 18.9 15.9 54 25.9 23.3 .44CRIB II score 12 8.2 2.7 46 8.2 3.0 .84Modified CRIB II score a 16 6.8 3.5 66 6.9 3.6 .92
Worst preoperative values pH 15 7.1 0.2 68 7.2 0.2 .57Base excess 15 −12.3 6.5 67 −11.5 7.2 .61Blood lactate 11 7.5 4.7 59 6.6 4.6 .50Serum sodium 17 130 7 68 129 6 .48White cell count 15 6.0 7.4 64 6.5 4.6 .24Neutrophil count 13 3.8 7.0 48 4.4 4.7 .20Platelet count 16 142 147 70 112 111 .67C-reactive protein 14 71.6 51.7 69 83.3 65.9 .72INR 15 2.49 2.10 64 1.95 1.28 .22
Inotropic support Required 16 9 56% 65 38 58% .87High doses b 16 5 31% 64 14 22% .44
a CRIB II score also calculated (using same scoring system as for 32 weeks gestation) for neonates with gestation more than 32 weeks.b More than 1 drug, odds ratio greater than 15 μg/kg per minute.
668 M. Arnold, S.W. Moore
orally in 4 patients, with mode of administration notconsistently found in the documentation of the other 3because of the retrospective nature of the study. Eight (50%)of the HIV-exposed infants received a single dose of NVP,followed by 1 month of AZT, of which one received IVAZT only, 4 received oral treatment only (before thedevelopment of NEC), and mode of administration wasunclear in the remaining 3. Only 1 patient (6%) receivedNVP only in accordance with new prevention of mother-to-child transmission guidelines [48]. Maternal Highly ActiveAntiretroviral Therapy (HAART) treatment was given in 2of the “7-day prophylaxis” group and 1 of the “1-monthprophylaxis” group. Mean (and median) maternal CD4
Table 3 Comparison of surgical findings and surgery performed betw
Surgical findings and procedure
TotalPeritoneal drainsLaparotomySurgery findings Full thickness gut necrosis present
Open and close: total or near-total gut necrosisIsolated single perforation
Procedure done Primary anastomosis doneDistal Hartmann pouchDistal mucous fistulaRepeat laparotomy (eg, relook surgery)
counts were 542 (524) in the “7-day” group, 409 (431) in the“1-month” group, and 520 in the NVP-only patient.
4. Discussion
The 19.5% HIV prevalence in our study of severe (Bellstage III/ necrotic bowel) NEC concords with our 18.5%provincial HIV prevalence [49] (somewhat lower than theSouth African national maternal HIV prevalence of 29%[50]). Maternal HIV poses numerous indirect risk factors forNEC development and poor outcome in NEC. Firstly, itincreases the risk of premature labor [51,52], and the risk ofNEC is inversely proportional to gestational age [30].
een HIV-exposed and HIV-unexposed infants with stage III NEC
HIV exposed HIV nonexposed P
Total n % Total n %
87 17 18% 87 70 72%17 6 35% 70 26 37% .8917 13 76% 70 51 73% .7617 11 65% 70 49 70% .6717 1 6% 70 5 7% .8517 3 18% 70 6 9% .3017 3 18% 70 8 11% .5017 5 29% 70 21 30% .9617 2 12% 70 11 16% .6717 3 18% 70 3 4%
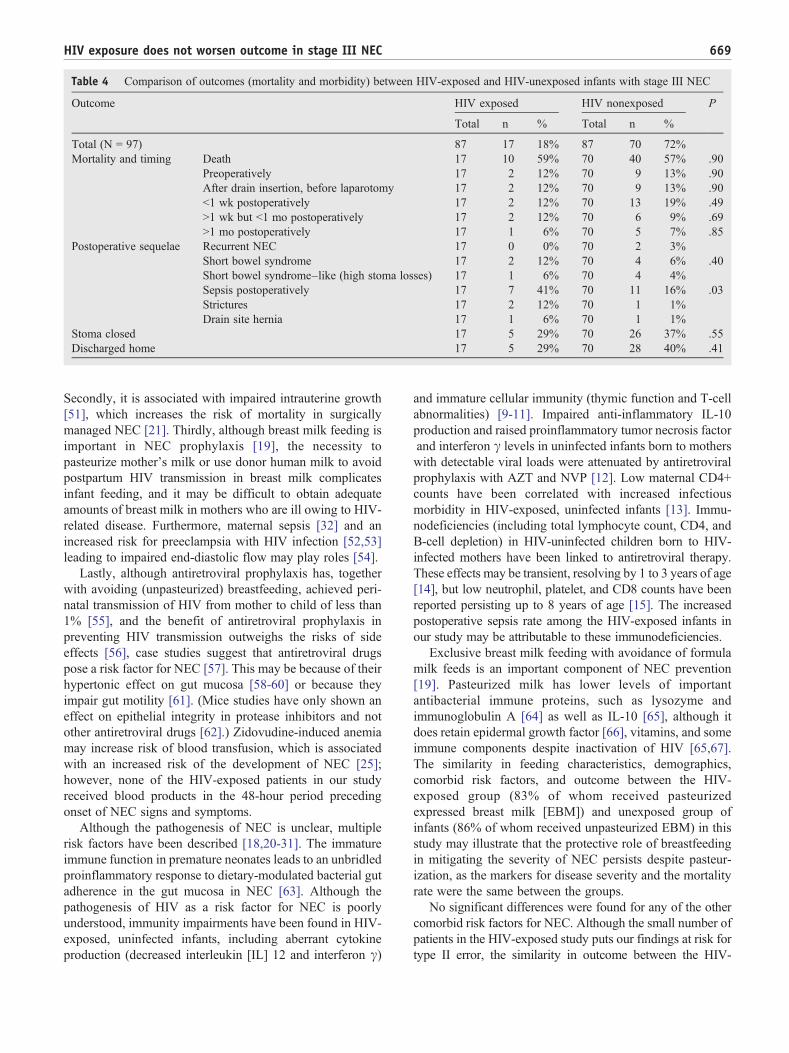
Table 4 Comparison of outcomes (mortality and morbidity) between HIV-exposed and HIV-unexposed infants with stage III NEC
Outcome HIV exposed HIV nonexposed P
Total n % Total n %
Total (N = 97) 87 17 18% 87 70 72%Mortality and timing Death 17 10 59% 70 40 57% .90
Preoperatively 17 2 12% 70 9 13% .90After drain insertion, before laparotomy 17 2 12% 70 9 13% .90b1 wk postoperatively 17 2 12% 70 13 19% .49N1 wk but b1 mo postoperatively 17 2 12% 70 6 9% .69N1 mo postoperatively 17 1 6% 70 5 7% .85
Postoperative sequelae Recurrent NEC 17 0 0% 70 2 3%Short bowel syndrome 17 2 12% 70 4 6% .40Short bowel syndrome–like (high stoma losses) 17 1 6% 70 4 4%Sepsis postoperatively 17 7 41% 70 11 16% .03Strictures 17 2 12% 70 1 1%Drain site hernia 17 1 6% 70 1 1%
Stoma closed 17 5 29% 70 26 37% .55Discharged home 17 5 29% 70 28 40% .41
669HIV exposure does not worsen outcome in stage III NEC
Secondly, it is associated with impaired intrauterine growth[51], which increases the risk of mortality in surgicallymanaged NEC [21]. Thirdly, although breast milk feeding isimportant in NEC prophylaxis [19], the necessity topasteurize mother's milk or use donor human milk to avoidpostpartum HIV transmission in breast milk complicatesinfant feeding, and it may be difficult to obtain adequateamounts of breast milk in mothers who are ill owing to HIV-related disease. Furthermore, maternal sepsis [32] and anincreased risk for preeclampsia with HIV infection [52,53]leading to impaired end-diastolic flow may play roles [54].
Lastly, although antiretroviral prophylaxis has, togetherwith avoiding (unpasteurized) breastfeeding, achieved peri-natal transmission of HIV from mother to child of less than1% [55], and the benefit of antiretroviral prophylaxis inpreventing HIV transmission outweighs the risks of sideeffects [56], case studies suggest that antiretroviral drugspose a risk factor for NEC [57]. This may be because of theirhypertonic effect on gut mucosa [58-60] or because theyimpair gut motility [61]. (Mice studies have only shown aneffect on epithelial integrity in protease inhibitors and notother antiretroviral drugs [62].) Zidovudine-induced anemiamay increase risk of blood transfusion, which is associatedwith an increased risk of the development of NEC [25];however, none of the HIV-exposed patients in our studyreceived blood products in the 48-hour period precedingonset of NEC signs and symptoms.
Although the pathogenesis of NEC is unclear, multiplerisk factors have been described [18,20-31]. The immatureimmune function in premature neonates leads to an unbridledproinflammatory response to dietary-modulated bacterial gutadherence in the gut mucosa in NEC [63]. Although thepathogenesis of HIV as a risk factor for NEC is poorlyunderstood, immunity impairments have been found in HIV-exposed, uninfected infants, including aberrant cytokineproduction (decreased interleukin [IL] 12 and interferon γ)
and immature cellular immunity (thymic function and T-cellabnormalities) [9-11]. Impaired anti-inflammatory IL-10production and raised proinflammatory tumor necrosis factorand interferon γ levels in uninfected infants born to motherswith detectable viral loads were attenuated by antiretroviralprophylaxis with AZT and NVP [12]. Low maternal CD4+counts have been correlated with increased infectiousmorbidity in HIV-exposed, uninfected infants [13]. Immu-nodeficiencies (including total lymphocyte count, CD4, andB-cell depletion) in HIV-uninfected children born to HIV-infected mothers have been linked to antiretroviral therapy.These effects may be transient, resolving by 1 to 3 years of age[14], but low neutrophil, platelet, and CD8 counts have beenreported persisting up to 8 years of age [15]. The increasedpostoperative sepsis rate among the HIV-exposed infants inour study may be attributable to these immunodeficiencies.
Exclusive breast milk feeding with avoidance of formulamilk feeds is an important component of NEC prevention[19]. Pasteurized milk has lower levels of importantantibacterial immune proteins, such as lysozyme andimmunoglobulin A [64] as well as IL-10 [65], although itdoes retain epidermal growth factor [66], vitamins, and someimmune components despite inactivation of HIV [65,67].The similarity in feeding characteristics, demographics,comorbid risk factors, and outcome between the HIV-exposed group (83% of whom received pasteurizedexpressed breast milk [EBM]) and unexposed group ofinfants (86% of whom received unpasteurized EBM) in thisstudy may illustrate that the protective role of breastfeedingin mitigating the severity of NEC persists despite pasteur-ization, as the markers for disease severity and the mortalityrate were the same between the groups.
No significant differences were found for any of the othercomorbid risk factors for NEC. Although the small number ofpatients in the HIV-exposed study puts our findings at risk fortype II error, the similarity in outcome between the HIV-

670 M. Arnold, S.W. Moore
exposed and HIV-unexposed groups is at odds with previousfindings of higher mortality in HIV-exposed infants with NECrequiring surgery, and further research in larger numbers isplanned to confirm our findings and assess the impact of HIV-exposure in all stages of NEC.
An interesting observation from this study is that there is ahigher rate (50% vs 20%) of antenatal steroid therapy in theHIV-exposed group. Antenatal corticosteroid therapy given toimprove lung maturity in premature labor reduces theincidence and severity of NEC [27,68]. It may be possiblethat the higher rate of antenatal steroid therapy in the HIV-exposed group confounded the apparent similarity in severitybetween the HIV-exposed and HIV-unexposed groups in ourstudy and that the HIV-exposed group would have done worsewithout this protective benefit. Nevirapine and AZT are notassociated with altered steroid metabolism, unlike proteaseinhibitors, nor with increased intestinal epithelial apoptosis (ina study on mice) [62]. Studies have shown that antenatalsteroids are not associated with an increased risk ofspontaneous intestinal perforation [69]. However, althoughthe increased incidence of isolated single perforations in theHIV-exposed group was not statistically significant, this maybe because of small sample size (type II error) as suggested bythe low value of the power calculation. Antenatal steroidsgiven more frequently in the HIV-positive group may reflect aheightened awareness among obstetricians of the increased rateof premature labor that is associated with untreated maternalHIV aswell asmaternal antiretroviral therapy [2,51]. Antenatalsteroids were not associated with increased risk of neonatalsepsis in a systematic review of randomized controlled trials[27], and there was no correlation between antenatal steroidexposure and increased postoperative sepsis in our study,although there was a trend toward more postoperative sepsis inthe HIV-exposed group. Potential beneficial effects ofantenatal steroid administration in this population requirefurther assessment.
Where antiretroviral prophylaxis is given and using currentprotocols of exclusive breastmilk feeding,with pasteurization incase of HIV exposure, HIV exposure does not appear to increasethe severity of stage III NEC or worsen the outcome, anddifferent treatment or worse prognostication is not justified as inthe previous era. However, HIV-exposed infants may be atincreased risk for postoperative sepsis compared with unex-posed infants with surgically managed NEC; a larger study isrequired to confirm this. The impact of the HIV epidemic on theoverall prevalence of all stages of NEC remains to be elucidated,ideally in a large, multicenter prospective study. More researchinto the impact on postsurgical recovery of HIV exposure inuninfected infants is also recommended.
References
[1] Desfrere L, de Oliveira I, Goffinet F, et al. Increased incidence ofnecrotizing enterocolitis in premature infants born to HIV-positivemothers. AIDS 2005;19:1487-93.
[2] Schulte J, Dominguez K, Sukalac T, et al. Declines in low birth weightand preterm birth among infants who were born to HIV-infectedwomen during an era of increased use of maternal antiretroviral drugs:pediatric spectrum of HIV disease, 1989-2004. Pediatrics 2007;119:e900-6.
[3] Karpelowsky JS, van Mil S, Numanoglu A, et al. Effect of maternalhuman immunodeficiency virus status on the outcome of neonates withnecrotizing enterocolitis. J Pediatr Surg 2010;45:315-8 [discussion 8].
[4] Deneve JL, Shantha JG, Page AJ, et al. CD4 count is predictive ofoutcome in HIV-positive patients undergoing abdominal operations.Am J Surg 2010;200:694-9 [discussion 9-700].
[5] Patel MS, Malinoski DJ, Nguyen XM, et al. The impact of selectchronic diseases on outcomes after trauma: a study from the NationalTrauma Data Bank. J Am Coll Surg 2011;212:96-104.
[6] Karpelowsky JS, Leva E, Kelley B, et al. Outcomes of humanimmunodeficiency virus–infected and –exposed children undergoingsurgery—a prospective study. J Pediatr Surg 2009;44:681-7.
[7] Bowley DM, Rogers TN, Meyers T, et al. Surgeons are failing torecognize children with HIV infection. J Pediatr Surg 2007;42:431-4.
[8] Karpelowsky JS, Zar HJ, van Bogerijen G, et al. Predictors ofpostoperative complications in HIV-infected children undergoingsurgery. J Pediatr Surg 2011;46:674-8.
[9] Clerici M, Saresella M, Colombo F, et al. T-lymphocyte maturationabnormalities in uninfected newborns and children with verticalexposure to HIV. Blood 2000;96:3866-71.
[10] Nielsen SD, Jeppesen DL, Kolte L, et al. Impaired progenitor cellfunction in HIV-negative infants of HIV-positive mothers results indecreased thymic output and low CD4 counts. Blood 2001;98:398-404.
[11] Chougnet C, Kovacs A, Baker R, et al. Influence of humanimmunodeficiency virus–infected maternal environment on develop-ment of infant interleukin-12 production. J Infect Dis 2000;181:1590-7.
[12] Hygino J, Lima PG, Filho RG, et al. Altered immunological reactivityin HIV-1–exposed uninfected neonates. Clin Immunol 2008;127:340-7.
[13] Mussi-Pinhata MM, Freimanis L, Yamamoto AY, et al. Infectiousdisease morbidity among young HIV-1–exposed but uninfectedinfants in Latin American and Caribbean countries: the NationalInstitute of Child Health and Human Development International SiteDevelopment Initiative Perinatal Study. Pediatrics 2007;119:e694-704.
[14] Slogrove AL, Cotton MF, Esser MM. Severe infections in HIV-exposed uninfected infants: clinical evidence of immunodeficiency. JTrop Pediatr 2010;56:75-81.
[15] Bunders M, Thorne C, Newell ML. Maternal and infant factors andlymphocyte, CD4 and CD8 cell counts in uninfected children of HIV-1–infected mothers. AIDS 2005;19:1071-9.
[16] Arnold M, Moore SW, Sidler D, et al. Long-term outcome ofsurgically managed necrotizing enterocolitis in a developing country.Pediatr Surg Int 2010;26:355-60.
[17] Schulzke SM, Deshpande GC, Patole SK. Neurodevelopmentaloutcomes of very low-birth-weight infants with necrotizing enteroco-litis: a systematic review of observational studies. Arch PediatrAdolesc Med 2007;161:583-90.
[18] Filteau S. The HIV-exposed, uninfected African child. Trop Med IntHealth 2009;14:276-87.
[19] Dvorak B, Halpern MD, Holubec H, et al. Maternal milk reducesseverity of necrotizing enterocolitis and increases intestinal IL-10 in aneonatal rat model. Pediatr Res 2003;53:426-33.
[20] Siplovich L, Davies MR, Kaschula RO, et al. Intestinal obstructionin the newborn with congenital syphilis. J Pediatr Surg 1988;23:810-3.
[21] de Souza JC, da Motta UI, Ketzer CR. Prognostic factors of mortalityin newborns with necrotizing enterocolitis submitted to exploratorylaparotomy. J Pediatr Surg 2001;36:482-6.
671HIV exposure does not worsen outcome in stage III NEC
[22] Giannone PJ, Luce WA, Nankervis CA, et al. Necrotizingenterocolitis in neonates with congenital heart disease. Life Sci2008;82:341-7.
[23] Koehne PS, Bein G, Alexi-Meskhishvili V, et al. Patent ductusarteriosus in very low birthweight infants: complications ofpharmacological and surgical treatment. J Perinat Med 2001;29:327-34.
[24] Ohlsson A, Walia R, Shah S. Ibuprofen for the treatment of patentductus arteriosus in preterm and/or low birth weight infants. CochraneDatabase Syst Rev 2008:CD003481.
[25] Christensen RD, Wiedmeier SE, Baer VL, et al. Antecedents of Bellstage III necrotizing enterocolitis. J Perinatol 2010;30:54-7.
[26] Uslu S, Ozdemir H, Bulbul A, et al. The evaluation of polycythemicnewborns: efficacy of partial exchange transfusion. J Matern FetalNeonatal Med 2011.
[27] Roberts D, Dalziel S. Antenatal corticosteroids for accelerating fetallung maturation for women at risk of preterm birth. Cochrane DatabaseSyst Rev 2006;3:CD004454.
[28] Bortolin L, Boer M, Christiansen S, et al. Effects of prenatal steroids inthe development of necrotizing enterocolitis in wistar rat neonates.Arch Argent Pediatr 2011;109:24-9.
[29] Obladen M. Necrotizing enterocolitis—150 years of fruitless searchfor the cause. Neonatology 2009;96:203-10.
[30] Lin PW, Nasr TR, Stoll BJ. Necrotizing enterocolitis: recent scientificadvances in pathophysiology and prevention. Semin Perinatol 2008;32:70-82.
[31] Unachukwu CN, Uchenna DI, Young EE. Endocrine and metabolicdisorders associated with human immune deficiency virus infection.West Afr J Med 2009;28:3-9.
[32] Carter BM, Holditch-Davis D. Risk factors for necrotizing enteroco-litis in preterm infants: how race, gender, and health status contribute.Adv Neonatal Care 2008;8:285-90.
[33] Bonnard A, Zamakhshary M, Ein S, et al. The use of the score forneonatal acute physiology-perinatal extension (SNAPPE II) inperforated necrotizing enterocolitis: could it guide therapy in newbornsless than 1500 g? J Pediatr Surg 2008;43:1170-4.
[34] Gagliardi L, Cavazza A, Brunelli A, et al. Assessing mortality riskin very low birthweight infants: a comparison of CRIB, CRIB-II,and SNAPPE-II. Arch Dis Child Fetal Neonatal Ed 2004;89:F419-22.
[35] Richardson DK, Corcoran JD, Escobar GJ, et al. SNAP-II andSNAPPE-II: simplified newborn illness severity and mortality riskscores. J Pediatr 2001;138:92-100.
[36] Couselo Jerez M, Ibanez Pradas V, Marijuan Sahuquillo V, et al.Evaluation of the SNAPPE-II and Metabolic Disorder Index aspredictors of mortality in necrotizing enterocolitis. Cir Pediatr2010;23:99-102.
[37] Schober PH, Nassiri J. Risk factors and severity indices in necrotizingenterocolitis. Acta Paediatr Suppl 1994;396:49-52.
[38] Kenton AB, O'Donovan D, Cass DL, et al. Severe thrombocytopeniapredicts outcome in neonates with necrotizing enterocolitis. J Perinatol2005;25:14-20.
[39] Ververidis M, Kiely EM, Spitz L, et al. The clinical significance ofthrombocytopenia in neonates with necrotizing enterocolitis. J PediatrSurg 2001;36:799-803.
[40] Milner ME, de la Monte SM, Moore GW, et al. Risk factors fordeveloping and dying from necrotizing enterocolitis. J PediatrGastroenterol Nutr 1986;5:359-64.
[41] Voss M, Moore SW, van der Merwe I, et al. Fulminanting necrotisingenterocolitis: outcome and prognostic factors. Pediatr Surg Int1998;13:576-80.
[42] Roy A, Tayeb M, Khogeer SS, et al. Predictors of gangrenousnecrotizing enterocolitis and extent of disease. Early laparotomy versusperitoneal drainage. Saudi Med J 2005;26:447-52.
[43] Wang YH, Su BH, Wu SF, et al. Clinical analysis of necrotizingenterocolitis with intestinal perforation in premature infants. ActaPaediatr Taiwan 2002;43:199-203.
[44] Sola JE, Tepas 3rd JJ, Koniaris LG. Peritoneal drainage versuslaparotomy for necrotizing enterocolitis and intestinal perforation: ameta-analysis. J Surg Res 2010;161:95-100.
[45] Hall NJ, Curry J, Drake DP, et al. Resection and primaryanastomosis is a valid surgical option for infants with necrotizingenterocolitis who weigh less than 1000 g. Arch Surg 2005;140:1149-51.
[46] Ta BD, Roze E, van Braeckel KN, et al. Long-term neurodevelop-mental impairment in neonates surgically treated for necrotizingenterocolitis: enterostomy associated with a worse outcome. Eur JPediatr Surg 2011;21:58-64.
[47] Policy and guidelines for the implementation of the PMTCT pro-gramme. Pretoria, Republic of South Africa: South African Departmentof Health; 2008. p. 43.
[48] Clinical Guidelines: PMTCT (Prevention of Mother-to-Child Trans-mission). Pretoria, Republic of South Africa: South African Depart-ment of Health; 2010.
[49] Shisana O, Simbayi L, Nelson Mandela/HSRC study ofHIV/AIDS. In: Shisana O, Rehle T, Simbayi L, editors. SouthAfrican National HIV prevalence, HIV incidence, behaviour andcommunication survey, 2005. Cape Town: South African MedicalResearch Council. Human Sciences Research Council Press; 2008.p. 156. (ISBN 13 978-07969-2325-7).
[50] National Department of Health, South Africa; South African NationalAIDS Council. 2010 Clinical Guidelines: PMTCT (Prevention ofMother-to-Child Transmission); National Department of Health, SouthAfrica.2010; Pretoria, Republic of South Africa. p. 11-13.
[51] Grosch-Woerner I, Puch K, Maier RF, et al. Increased rate ofprematurity associated with antenatal antiretroviral therapy in aGerman/Austrian cohort of HIV-1–infected women. HIV Med2008;9:6-13.
[52] Aebi-Popp K, Lapaire O, Glass TR, et al. Pregnancy and deliveryoutcomes of HIV infected women in Switzerland 2003-2008. J PerinatMed 2010;38:353-8.
[53] Kilewo C, Natchu UC, Young A, et al. Hypertension in pregnancyamong HIV-infected women in sub-Saharan Africa: prevalence andinfant outcomes. Afr J Reprod Health 2009;13:25-36.
[54] Musemeche CA, Kosloske AM, Bartow SA, et al. Comparative effectsof ischemia, bacteria, and substrate on the pathogenesis of intestinalnecrosis. J Pediatr Surg 1986;21:536-8.
[55] Volmink J, Siegfried NL, van der Merwe L, et al. Antiretrovirals forreducing the risk of mother-to-child transmission of HIV infection.Cochrane Database Syst Rev 2007:CD003510.
[56] Thorne C, Newell ML. Safety of agents used to prevent mother-to-child transmission of HIV: is there any cause for concern? Drug Saf2007;30:203-13.
[57] De Carolis MP, Lacerenza S, De Luca D, et al. Is neonatalantiretroviral therapy a risk factor for NEC occurrence? Turk J Pediatr2010;52:108-10.
[58] Thorne C, Newell ML. The safety of antiretroviral drugs in pregnancy.Expert Opin Drug Saf 2005;4:323-35.
[59] van der Meulen EF, Bergman KA, Kamps AW. Necrotisingenterocolitis in a term neonate with trisomy 21 exposed tomaternal HIV and antiretroviral medication. Eur J Pediatr2009;168:113-4.
[60] Mutz AE, Obladen MW. Hyperosmolar oral medication andnecrotizing enterocolitis. Pediatrics 1985;75:371-2.
[61] Brindley NM. Antiretroviral agents mimicking functional neonatalbowel obstruction: a case report. Eur J Pediatr Surg 2006;16:276-8.
[62] Braga Neto MB, Aguiar CV, Maciel JG, et al. Evaluation of HIVprotease and nucleoside reverse transcriptase inhibitors on prolifera-tion, necrosis, apoptosis in intestinal epithelial cells and electrolyte andwater transport and epithelial barrier function in mice. BMCGastroenterol 2010;10:90.
[63] Kosloske AM. Epidemiology of necrotizing enterocolitis. ActaPaediatr Suppl 1994;396:2-7.

672 M. Arnold, S.W. Moore
[64] Akinbi H, Meinzen-Derr J, Auer C, et al. Alterations in the hostdefense properties of human milk following prolonged storage orpasteurization. J Pediatr Gastroenterol Nutr 2010;51:347-52.
[65] Untalan PB, Keeney SE, Palkowetz KH, et al. Heat susceptibility ofinterleukin-10 and other cytokines in donor human milk. BreastfeedMed 2009;4:137-44.
[66] Yagi H, Suzuki S, Noji T, et al. Epidermal growth factor in cow's milkand milk formulas. Acta Paediatr Scand 1986;75:233-5.
[67] Israel-Ballard K, Chantry C, Dewey K, et al. Viral, nutritional, andbacterial safety of flash-heated and pretoria-pasteurized breast milk to
prevent mother-to-child transmission of HIV in resource-poorcountries: a pilot study. J Acquir Immune Defic Syndr 2005;40:175-81.
[68] Halac E, Halac J, Begue EF, et al. Prenatal and postnatal corticosteroidtherapy to prevent neonatal necrotizing enterocolitis: a controlled trial.J Pediatr 1990;117:132-8.
[69] Attridge JT, Clark R, Gordon PV. New insights into spontaneousintestinal perforation using a national data set (3): antenatal steroidshave no adverse association with spontaneous intestinal perforation. JPerinatol 2006;26:667-70.