his initiative update qi and performance initiative update pihoa board meeting, march, 2015 a mark...
TRANSCRIPT

HIS Initiative UpdateQI and Performance Initiative Update
PIHOA Board Meeting, March, 2015
A Mark Durand
PIHOA Performance & Health Information Coordinator
HIS Extension Services-
EHR- (Pohnpei)Organizational readiness assessment, System requirements,Project scope of work, Network upgrade proposal and a PD recruitment of a manager for this project.
Assistance with of cause-specific, age-adjusted NCD mortality from vital stats (Pohnpei)
NCD Core Surveillance Profiles (Pohnpei, RMI, Palau)
Data consultation for Million Hearts project (Palau)

HIS Highlights past 6 months
• Recruitment of Drs Cash & Hancock to work with PIHOA in the region
• Submission of a full DDM-FETP curriculum and delivery strategy proposal to FNU
• Pilot testing of DDM3 with multiple completed dataset analyses
• Partnerships
• Delivery of 3-day Ebola Preparedness & Infection Control Workshop(RMI, FSM, Palau)
• Development of 1-day Ebola Preparedness & Infection Control Workshop Curriculum


DDM1) Outbreak surveillance and response
DDM2) Basic applied epidemiology and data analysis
DDM3) Intermediate applied epidemiology and data analysis
DDM4) Public health surveillance
DDM5) Special project
DDM Courses:

DDM3 Intermediate Epi & Data Analysis- Oct, 2014• Incidence/Prevalence of Hepatitis in Guam• Alcohol Prevention Messages in FSM (NOM Survey)• Obesity in School Children in Kosrae• Breast and Cervical Cancer Screening in Palau• Current Drinking, Binge Drinking in Guam• Oral Health Survey- Palau• STEPs survey- Pohnpei• Mortality in RMI• Environmental Health Inspections in Palau









0 5 10 15 20 25 300%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
DDM3 Course Scores (Exam + Poster presentation) Guam October 2014
Exam+presCutoff
Students
Exam
+ P
oste
r pre
sent
ation
per
cent
age

Next DDM Activities- Guam, May 4-15
• DDM3 Intensive review and exam retake• DDM4 Pilot • DDM5 Project Kick-off• Partners’ Retreat
For Individual Board Member Consideration:o Nomination of participants
> Previous DDM participants> New DDM candidates who have some epi/stats background

Proposed USAPI Regional Epi Capacity Building Unit (REU): Building blocks
Workforce:• Cohort of Epi Technicians at each health dept (DDM1-DDM5) • At least 1 fully qualified, non-expat applied epidemiologist at each health
dept (SHIP)Systems: • Routine weekly communicable disease reports• High quality SitReps during outbreaks• NCD surveillance plan• Annual NCD surveillance profile• Annual Regional NCD and CD surveillance profile• HIS capable of measuring preventive services coverage accurately

Proposed REU: Formal agreements Health Dept REU
• New system elements to install
• Nominations of Epi Technician candidates
• Expectations of candidates
• Support to be provided by Director/Minister/Secretary

Proposed REU:Terms of engagement for REU staff
• Monitoring & Mentoring: REU staff Epi Tech in-country work• Sharing correspondence within REU• Annual regional products: • Evaluations of CD and NCD surveillance systems in each USAPI• Regional profile of CD and NCDs- Progress and capacities
• Formal letters of notification through PIHOA ED for site visits of REU members
For Board Consideration: o Consider endorsement of REU, communique to CDC and partners
For Individual Board Member Consideration:o Nomination of Epi Technician candidates for your agencyo Development of REU agreement

NCD Surveillance & Response
???

NCD
Pol
icy
Tool
kit
Other Good Frameworks:
•CDC Healthy People 2020•WHO NCD Global Monitoring Framework• Framework Convention for Tobacco Control•WHO “Best Buys” for NCDs•WHO Pacific Roadmap for NCDs

Advantages of USAPI NCD “Products”1) Commissioned by you2) Developed by your Technical Working Groups3) Pacific appropriate4) Emergency-level intensity (Comprehensive)5) Designed to fit with both CDC and WHO approaches6) Gives you a place on the global stage

Out of 144 measurements: 14=improved, 15=worse, 33=no change, 82=not enough data
USAPINCD Core SurveillanceIndicators
Tobacco Alcohol
↑BMI Diseases(adult)
Deaths(30-69 years)
Cigs- youth
Cigs- adult
Chew- Youth
Chew- adult
Youth
Adult
Youth
Adult
HTN
DM
↑Cholesterol
All Cause
Cardiovascular
Cancer
Diabetes
Chronic Lung
Jurisdiction A ↓ N ↓ ↑ N N N N N
Jurisdiction B ↓ N ↓ N ↓ N ↑ ↑ ↑ N ↓
Jurisdiction C
Jurisdiction D
Jurisdiction E
Jurisdiction F N N N N N ↓ N ↓ N
Jurisdiction G ↓ ↓ ↑ N ↓ N N N N N N ↑ N ↑ ↑ ↑
Jurisdiction H ↑ N ↓ N ↓ N N N ↑ ↑ ↑ N N
Jurisdiction I ↑ ↓ ↑ ↓ N
POPU
LATI
ON

1) Update USAPI NCD Core Surveillance Framework:• Change in age group for NCD STEPs• CHL program monitoring of early child BMI• Harmonize with Global Monitoring Framework
2) Update PIHOA “Progress in the Fight against NCDs in the USAPI” Evidence Brief
Work Needed for NCD Core Surveillance
For Board Consideration:o Guidance on re-convening the USAPI Technical Working Group to review and
update the USAPI NCD Monitoring and Surveillance Framework
For Individual Board Member Consideration:o Delegate a counterpart to update of NCD surveillance & policy profile

Environment & Social
Youth Risks- Tobacco- Alcohol- Obesity
Adult Risks- Tobacco- Alcohol- Obesity
Diseases:CVDCancer
DiabetesCOPD(HTN)(Lipids)
Deaths- COPD- Heart+Stroke- Cancer- Diabetes
Medical Care
(policy commitment
Package)
Community & Policy
Health Promotion &
Education

Preventive Services Delivery
???



Clinic-based interventions (eg. PEN- CCM) Community Screening & Outreach
Other clinicsNCD Clinic Not attending clinics
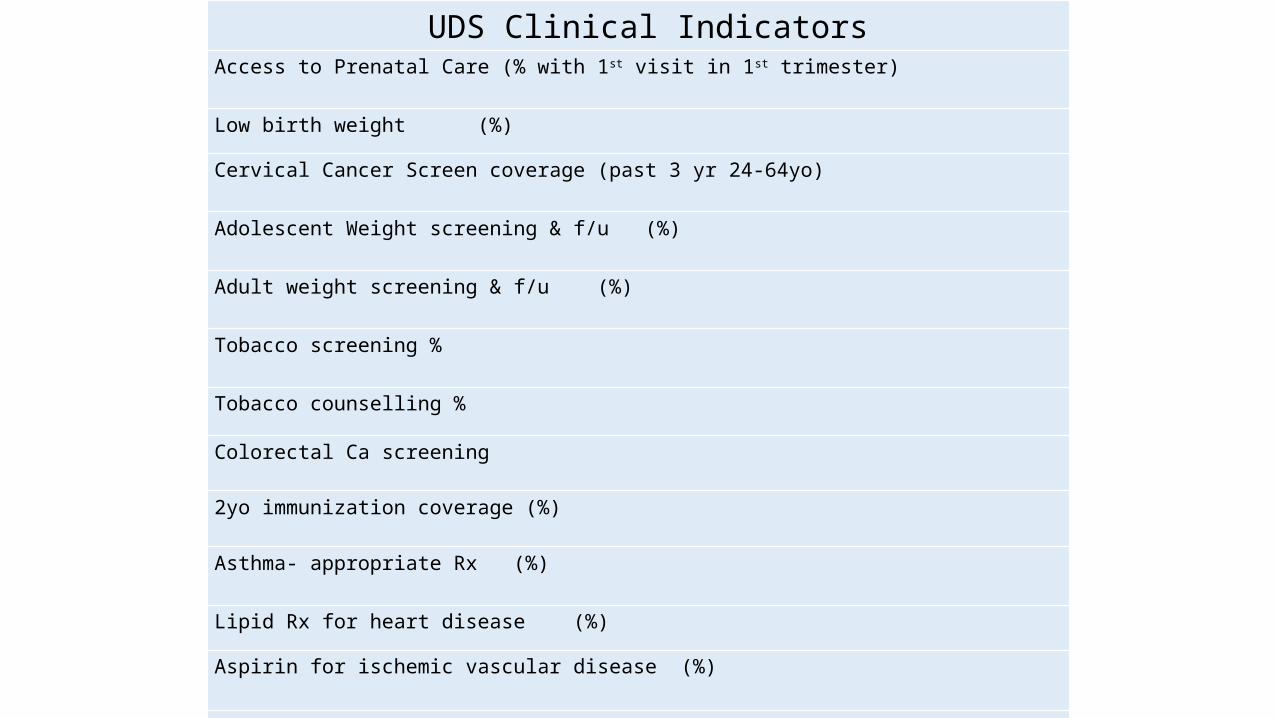
UDS Clinical IndicatorsAccess to Prenatal Care (% with 1st visit in 1st trimester)
Low birth weight (%)
Cervical Cancer Screen coverage (past 3 yr 24-64yo)
Adolescent Weight screening & f/u (%)
Adult weight screening & f/u (%)
Tobacco screening %
Tobacco counselling %
Colorectal Ca screening
2yo immunization coverage (%)
Asthma- appropriate Rx (%)
Lipid Rx for heart disease (%)
Aspirin for ischemic vascular disease (%)
BP control (% under control)
Diabetes control (% with A1C test less than 9)

84 measurements: 23=better, 10=worse, 45=No change, 5=not enough data
CHC Preventive Services Indicators
Early PNT Care
% Low birth weight
Cervical Ca Screeng
Youth weight
Adult weight
Tobacco use screen
Tobacco counsel
2 YO Immunization
Colon Ca screening
Asthma Rx
Lipid Rx for Ht Disease
Aspirin for vascular disease
High BP Control
Diabetes Control
CHC- A W N B W N B B W N N N B B
CHC- B N N W N B B N N N W N N B
CHC- C N W N B N N N N B N N N N N
CHC- D B N B N W N W N N N N N B N
CHC- E B N N N B B B N N N B B W N
CHC- F N B B N N B B W N N
CHC- G
Range (%) 7-69 4-23 4-93 0-100 0-53 9-90 7-83 0-89 0-36 0-100 0-94 9-100 29-84 28-53
B= BetterW= WorseN= No change
Hea
lth S
ervi
ces

CHC Preventive Services Indicators
Early PNT Care
% Low birth weight
Cervical Ca Screeng
Youth weight
Adult weight
Tobacco use screen
Tobacco counsel
2 YO Immunization
Colon Ca screening
Asthma Rx
Lipid Rx for Ht Disease
Aspirin for vascular disease
High BP Control
Diabetes Control
Heavy work burden 4/7 3/7 6/7 6/7 6/7 6/7 5/6 5/7 3/7 6/7 6/7 5/6 5/6 4/6
Perceived accuracy 7/7 5/7 2/7 2/7 3/7 2/7 1/6 3/7 3/7 2/7 2/7 2/7 2/6 4/6
74%
16 %
Heavy Work Burden (%)
YesNo 42%
58%
Accuracy (%)
YesNo

Take Home Messages
Population Level:• Many gaps in surveillance picture• Some progress, especially tobacco and alcohol• Lots of room for more progress
Health services level:• Must “ramp up” preventive services delivery move beyond pilot projects in NCD clinics• Information systems are a key element
Both levels: • Dis-coordination among technical assistance agencies is a big handicap• NCD surveillance plans at jurisdiction level need reinforcement

Hopes for next 6 months
• Update the USAPI NCD Surveillance Framework
• Update USAPI NCD Progress Profile, and policy uptake mapping
• Bring at least some DDM participants through entire DDM series to Epi Technician certification
• Accelerate data and epi systems development across the USAPI with the assistance of Drs Cash and Hancock
• Identify stable, core funding for DDM-SHIP to allow wider dissemination of EpiTech

Board guidance requestedo On Concept Brief for a Regional Epi Capacity Building Unit & Framework (with
possible endorsement and communique)o On re-convening the USAPI Technical Working Group to review and update the
USAPI NCD Monitoring and Surveillance Framework o Whether USAPI NCD “products” are still relevant (if yes, how to promote them
with TA partners)
For Individual Board Member Consideration in your Jurisdiction• Nominees to upcoming DDM4• Nominate a cohort of Epi Technician candidates in your jurisdiction• Formal Data & Surveillance Capacity Agreements with REU• Delegate a staff member to update of NCD surveillance & policy profile

QI and Performance Management
???


QI-PM Extension Services-
• Pharmacy procurement & inventory improvement (Pohnpei)
• Quality Improvement policies and procedures development (Pohnpei, Palau CHCs)
• Management strengthening consultation (RMI)
• UDS QI workshop held with USAPI CHC managers at PIPCA meeting

International Council of Nurses Leadership for Change Program
Summary, Outcomes, Lessons learned and Next Steps
Pacific Island Health Officers AssociationRepublic of Palau
March 9, 2015Kristine Qureshi, PhD, RN, CEN, APHN-BC
Technical consultant, PHIOA

ICN-LFC RecapTraining program designed to build leadership
capacity among mid/senior level manages17 participants from USAPI (9 PIHOA funded,
8 jurisdiction support)Three 5 day sessions in HNLAll selected a change project that was
approved by their supervisor

ICN LFC Projects Decubitus ulcer reduction X2 OPD waiting time reduction Organizational leadership capacity X2 Midwifery career ladder Organizational leadership capacity Access to IUD technology Expansion of HIV / STI services Development of a strategic plan Strategic plan for management & leadership Cervical Ca. screening follow up Standardize pt. referral across MOH Move administration of daily insulin from ED to the community
(home) setting

Outcomes (see handout)
All projects initiatedMost at initial implementation phase
Examples of successful QI change projects: ◦ Ebeye team: Of 82 pts. receiving 2 X day daily
insulin from ED, moved 62 to home administration, goal to address remaining 20.
◦ AS team: Three yr. gradual increase in readmission rate. Revised discharge planning process. Now 89% (from 23%) discharge planning initiated on admission, developed a medication reconciliation policy, started caregivers classes.

Factors that influenced project success
Topic deemed very relevant to senior leadership in the organization
Strong support and engagement from senior leadership
Management skills of participant

Lessons learned (relative to this project)
Organizational change requires support from the very top
Leadership is not the same as management, and management skills need to be cultivated
Managers need to be “supervised, managed & supported”… stay on target & on task, have barriers addressed along the way
Most managers know the principles and mechanics of QI, but some are not formally supervised and or lack the organizational support to really effect improvement change

Lessons learned (continued)Managers should be focusing efforts on the
priority areas of senior management– that are linked to the strategic plan
Sustainability requires abilities to hand off projects and assure accountability

Next steps……Dissemination: Invitation letter from
nursing management journal for publication – needs to be written up
Projects have been initiated, but not yet completed– ongoing management support and supervision of progress
Ongoing PIHOA technical support requires jurisdiction level will and support (example: Kosrae has budgeted funds for roll out across their management workforce)
DISCUSSION, what are your thoughts ???
