hirsutism
TRANSCRIPT

HIRSUTISM
Hirsutism
DURU SHAH1,2,3,4 & SUKHPREET PATEL5
1Gynaecworld Assisted Fertility Unit, 2Breach Candy Hospital, 3Jaslok Hospital and Research Centre, 4Sir HN Hospital and
Research Centre, Mumbai, India and 5Gynaecworld, Mumbai, India
(Received 11 July 2008; accepted 16 July 2008)
AbstractHirsutism is a distressing and relatively common problem, affecting 5 to 10% of women in the reproductive age group. It isusually a sign of androgen excess, the commonest cause being the polycystic ovarian syndrome (PCOS). Diagnosis dependsmainly on assessment of the clinical symptoms and laboratory values of various hormones. Antiandrogens combined withvarious cosmetic therapies form the mainstay of treatment.
Keywords: Hirsutism, polycystic ovarian syndrome, adrenal, antiandrogens
‘The hair is the richest ornament of women’ – Martin
Luther
Introduction
The richest ornament, when inappropriately placed,
can be a cause of terrible distress for a woman.
Hirsutism is a distressing and relatively common
problem, affecting 5–10% of women in the repro-
ductive age group [1]. It is defined as excess terminal
hair growth in a female in a typically male distribution. It
may be the result of either androgen excess or
increased sensitivity of the hair follicles to normal
levels of androgens. The current review deals with
the various aspects of hirsutism such as its causes,
diagnosis and management.
Physiology of hair growth
Besides the soles, palms and lips, the entire skin
surface of the human body is covered with hair. The
number of hair follicles that humans are born with
remains more or less constant throughout life, and
depends greatly on racial and constitutional factors.
As defined earlier, hirsutism is the presence of excess
terminal hair growth in a female in a typically male
distribution. To understand this definition, it is
essential to understand the normal physiology of hair
growth.
Hair can be classified in two different ways.
1. Structurally, hair may be of three different types,
namely, lanugo, vellus and terminal hair. Lanugo is
the soft downy hair that covers the fetus at birth,
and is usually shed in the few months that follow.
Vellus hairs are the small, straight, fair and non-
pigmented hair that cover the apparently hairless
areas of the body. Terminal hairs are the larger,
curlier and darker, hence more visible hairs.
Although they are normally present on the scalp,
eyebrows, eyelashes, axillae and pubic area in
both sexes, they are also seen on the face, back
and abdomen in males.
2. Depending on its sensitivity to sex steroids, hairs
may also be classified into sexual and non-sexual.
Hair which responds to the sex hormones is
termed sexual hair. Sexual hair grows on the
face, lower abdomen, anterior thighs, the chest,
breasts, pubic area, and in the axillae.
Phases of hair growth
Hair undergoes three distinct phases of growth,
namely, anagen, catagen and telogen. Hair appears to
Correspondence: Duru Shah, Kwality House, Above Chinese Room Restaurant, Kemps Corner, Mumbai 400 026, India. E-mail: [email protected]
Gynecological Endocrinology, March 2009; 25(3): 140–148
ISSN 0951-3590 print/ISSN 1473-0766 online ª 2009 Informa Healthcare USA, Inc.
DOI: 10.1080/09513590802531567
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 11
/02/
14Fo
r pe
rson
al u
se o
nly.
be growing continuously in humans due to the lack of
synchrony between the phases of different hair
follicles. Therefore, although some of the follicles
grow actively in the anagen phase, the others may be
in the telogen or resting phase. The ratio of the
duration of the anagen to telogen phase is different for
hair belonging to different areas of the body. Although
the anagen phase for hair on the scalp may last a few
years, it may only last a few months for body hair. The
sex hormones have an effect on the duration of the
various phases of hair growth (Table I).
Effect of sex hormones on hair
Amongst the sex steroids, androgens are of utmost
importance for regulating the distribution pattern
and characteristic of hair. At puberty, with the
increase in the amount of circulating androgens,
there is stimulation of sexual hair. Although this gives
rise to axillary and pubic hair in both sexes, it also
stimulates sexual hair on other sites in the male, such
as the face, chest, etc. Thus, the soft vellus hair is
converted to the dark, coarse, pigmented terminal
hair. In the presence of an excess of androgens or an
increase in the sensitivity of hair follicles to circulat-
ing androgens, stimulation of sexual hair may
similarly manifest as hirsutism in females.
Androgens have a paradoxical effect on scalp hair,
leading to balding. This is due to a reduction of the
anagen phase and regression of scalp hair to vellus
hair [1,2]. Therefore, associated balding may be
observed in hirsute women.
Androgens in women
Androgens in women can arise from three different
sources
1. Ovary
2. Adrenal
3. Peripheral conversion
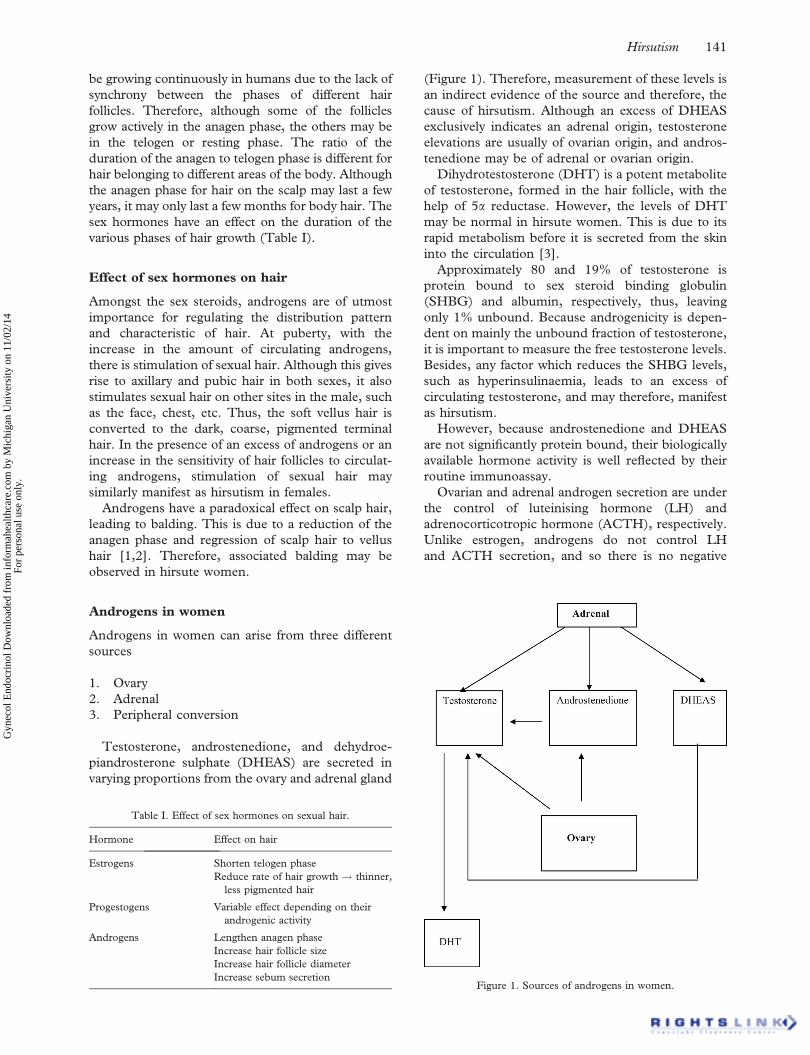
Testosterone, androstenedione, and dehydroe-
piandrosterone sulphate (DHEAS) are secreted in
varying proportions from the ovary and adrenal gland
(Figure 1). Therefore, measurement of these levels is
an indirect evidence of the source and therefore, the
cause of hirsutism. Although an excess of DHEAS
exclusively indicates an adrenal origin, testosterone
elevations are usually of ovarian origin, and andros-
tenedione may be of adrenal or ovarian origin.
Dihydrotestosterone (DHT) is a potent metabolite
of testosterone, formed in the hair follicle, with the
help of 5a reductase. However, the levels of DHT
may be normal in hirsute women. This is due to its
rapid metabolism before it is secreted from the skin
into the circulation [3].
Approximately 80 and 19% of testosterone is
protein bound to sex steroid binding globulin
(SHBG) and albumin, respectively, thus, leaving
only 1% unbound. Because androgenicity is depen-
dent on mainly the unbound fraction of testosterone,
it is important to measure the free testosterone levels.
Besides, any factor which reduces the SHBG levels,
such as hyperinsulinaemia, leads to an excess of
circulating testosterone, and may therefore, manifest
as hirsutism.
However, because androstenedione and DHEAS
are not significantly protein bound, their biologically
available hormone activity is well reflected by their
routine immunoassay.
Ovarian and adrenal androgen secretion are under
the control of luteinising hormone (LH) and
adrenocorticotropic hormone (ACTH), respectively.
Unlike estrogen, androgens do not control LH
and ACTH secretion, and so there is no negative
Table I. Effect of sex hormones on sexual hair.
Hormone Effect on hair
Estrogens Shorten telogen phase
Reduce rate of hair growth ! thinner,
less pigmented hair
Progestogens Variable effect depending on their
androgenic activity
Androgens Lengthen anagen phase
Increase hair follicle size
Increase hair follicle diameter
Increase sebum secretionFigure 1. Sources of androgens in women.
Hirsutism 141
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 11
/02/
14Fo
r pe
rson
al u
se o
nly.

feedback mechanism. Therefore, excess ovarian and
adrenal production can readily occur.
Causes of hirsutism
The causes of hirsutism can be classified into
Ovarian, adrenal, iatrogenic and idiopathic (Figure 2).
Hirsutism: the ovarian component
Polycystic ovarian syndrome
Polycystic ovarian syndrome (PCOS) is responsible
for the majority of women presenting with hirsutism
[2].
It is usually slow progressing, starts around
puberty, and gradually worsens with time, if not
treated. Hirsutism due to PCOS may be accompa-
nied by acne, weight gain, cycle irregularity, inferti-
lity and hair loss from the scalp. Hyperpigmentation
or acanthosis nigricans may also be observed in 5%
of obese women with insulin resistance.
In our personal series of over 500 PCOS patients,
46% presented to us with the complaint of hirsutism.
Only 38% of these demonstrated an elevated free
testosterone levels.
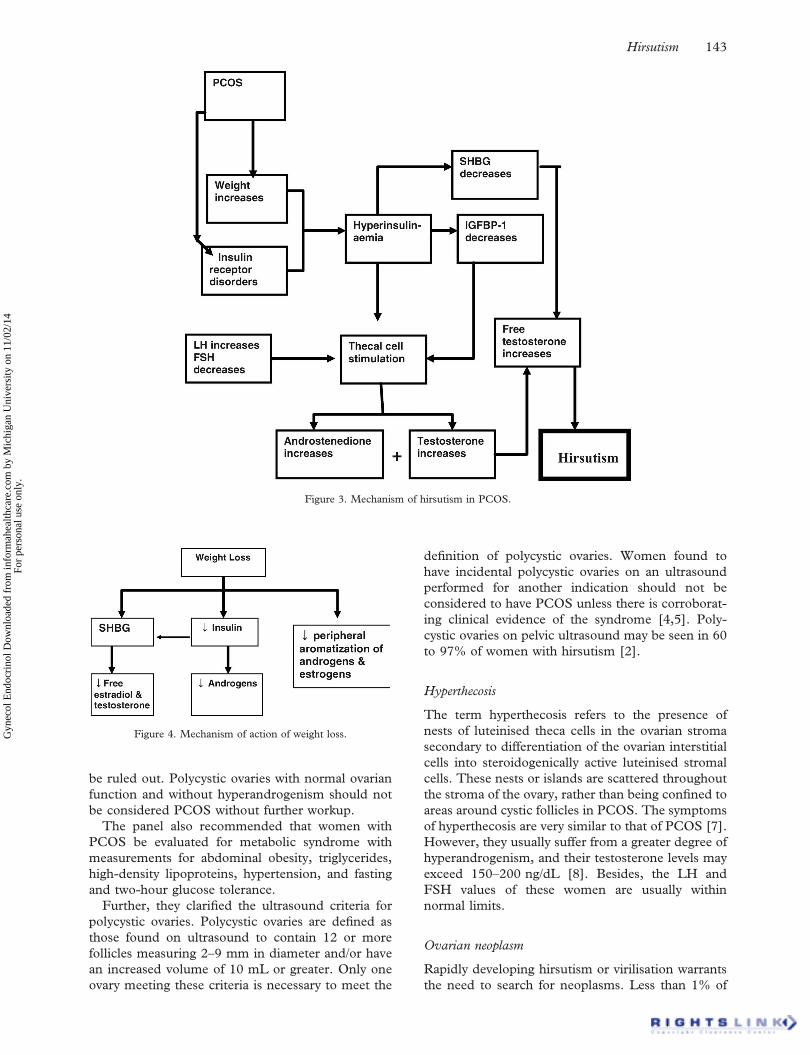
The ovary is usually the source of androgen excess
in women with PCOS. Hyperinsulinaemia further
exacerbates the problem by stimulating the thecal
cells and reducing the SHBG (Figure 3). Insulin
resistance can occur in up to 50% of patients with
PCOS [4,5].
Increase in weight also results in a reduction in the
SHBG, thereby increasing the free testosterone.
Therefore, weight loss is an extremely important
measure in treatment of hirsutism for women with
PCOS (Figure 4).
Laboratory investigations may reveal elevated
LH and insulin values. Further, an increase in
testosterone, androstenedione and DHEAS may also
be observed [6]. The best measures of objectively
measuring hyperandrogenism are free testosterone
levels or the free testosterone index. However, not
all patients with PCOS have elevated circulating
androgen levels, and not all circulating andro-
gens will be accounted for with these tests. In our
personal series of over 500 PCOS patients, 46%
presented to us with the complaint of hirsutism.
Only 38% of these demonstrated an elevated
free testosterone levels. Testosterone values do
not usually exceed 200 ng/dL in women with
PCOS.
Diagnosing PCOS can sometimes pose a dilemma
to the physician. During the last 20–30 years many
definitions for PCOS have been presented, as it
became clear that the description of Stein and
Leventhal represented only one end of the spectrum.
On 28 January 2004, the European Society for
Human Reproduction and Embryology and the
American Society for Reproductive Medicine co-
sponsored the Rotterdam PCOS consensus work-
shop group to revise the guidelines for diagnosis and
management that the National Institutes of Health
released in 1990 [4,5]. The revised guidelines have
been briefly mentioned.
The Rotterdam panel concluded that PCOS
encompasses a broader variety of manifestations of
ovarian dysfunction than those included in the
original diagnostic criteria defined by the National
Institutes of Health in 1990. Although the cardinal
features are hyperandrogenism and polycystic ovary
morphology, no single criterion is sufficient for
clinical diagnosis.
To be diagnosed with PCOS by the Rotterdam
criteria, a woman must have two of the following
three manifestations: irregular or absent ovulation,
elevated levels of androgenic hormones, and/or
enlarged ovaries containing at least 12 follicles each.
Other conditions with similar signs, such as andro-
gen-secreting tumors or Cushing’s syndrome, must
Figure 2. Causes of Hirsutism.
142 D. Shah & S. Patel
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 11
/02/
14Fo
r pe
rson
al u
se o
nly.
be ruled out. Polycystic ovaries with normal ovarian
function and without hyperandrogenism should not
be considered PCOS without further workup.
The panel also recommended that women with
PCOS be evaluated for metabolic syndrome with
measurements for abdominal obesity, triglycerides,
high-density lipoproteins, hypertension, and fasting
and two-hour glucose tolerance.
Further, they clarified the ultrasound criteria for
polycystic ovaries. Polycystic ovaries are defined as
those found on ultrasound to contain 12 or more
follicles measuring 2–9 mm in diameter and/or have
an increased volume of 10 mL or greater. Only one
ovary meeting these criteria is necessary to meet the
definition of polycystic ovaries. Women found to
have incidental polycystic ovaries on an ultrasound
performed for another indication should not be
considered to have PCOS unless there is corroborat-
ing clinical evidence of the syndrome [4,5]. Poly-
cystic ovaries on pelvic ultrasound may be seen in 60
to 97% of women with hirsutism [2].
Hyperthecosis
The term hyperthecosis refers to the presence of
nests of luteinised theca cells in the ovarian stroma
secondary to differentiation of the ovarian interstitial
cells into steroidogenically active luteinised stromal
cells. These nests or islands are scattered throughout
the stroma of the ovary, rather than being confined to
areas around cystic follicles in PCOS. The symptoms
of hyperthecosis are very similar to that of PCOS [7].
However, they usually suffer from a greater degree of
hyperandrogenism, and their testosterone levels may
exceed 150–200 ng/dL [8]. Besides, the LH and
FSH values of these women are usually within
normal limits.
Ovarian neoplasm
Rapidly developing hirsutism or virilisation warrants
the need to search for neoplasms. Less than 1% of
Figure 3. Mechanism of hirsutism in PCOS.
Figure 4. Mechanism of action of weight loss.
Hirsutism 143
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 11
/02/
14Fo
r pe
rson
al u
se o
nly.
ovarian neoplasms secrete androgens. Ovarian neo-
plasms such as sex cord stromal tumors are rare and
usually responsible for rapidly developing hirsutism
with total testosterone values exceeding 200 ng/dL.
Sex cord Stromal tumors may be of various types,
namely, Granulosa cell tumors, Leydig cell tumors,
Sertoli–Leydig cell tumors and thecomas. Of these,
the Sertoli–Leydig and Leydig tumors are most
common. Although the Sertoli–Leydig cell tumours
are seen during the reproductive years, the Leydig
cell tumors generally present at or after menopause.
They are both usually unilateral and benign. Occa-
sionally, some primary ovarian epithelial tumors can
also secrete excess androgen. Thecomas are rarely
responsible for hirsutism in pregnant women. Eva-
luation with the help of transvaginal ultrasound,
computed tomography and MRI may help in
diagnosing ovarian neoplasms.
Hirsutism: the adrenal component
Cushing’s syndrome
Hypercortisolism secondary to excessive ACTH
production can be either from the pituitary gland
(Cushing’s disease), or from ectopic ACTH secre-
tion by a non-pituitary tumor (Cushing’ syndrome).
Even though it is an uncommon cause for hirsutism,
the morbidity and mortality related with it if
untreated warrants attention and treatment. Endo-
crine and radiological evaluation is essential to make
a diagnosis of Cushing’s disease or syndrome.
Endocrine evaluation includes ACTH levels, basal
and post corticotrophin releasing hormone (CRH)
injection, and the low and high dexamethasone
suppression test. Although ACTH levels may be
normal or high in pituitary or ectopic ACTH
secretion disorders, they are usually low in adrenal
neoplasms. Computed tomography and magnetic
resonance imaging are also useful modalities in
diagnosing a pituitary adenoma.
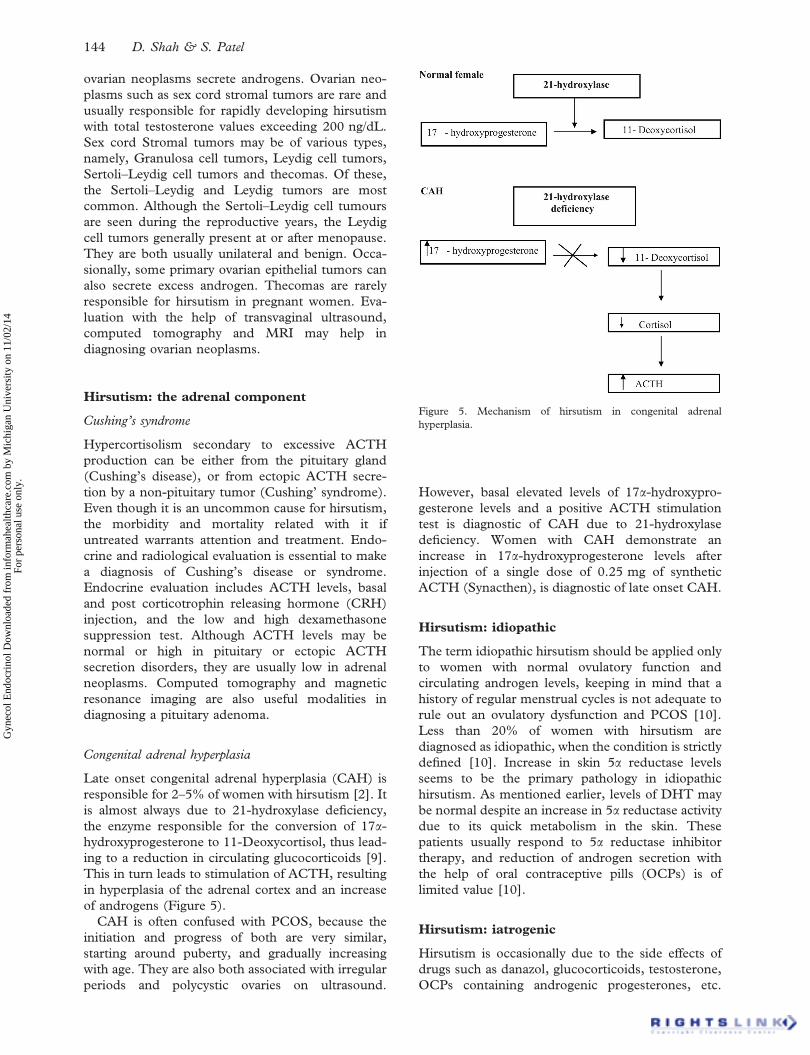
Congenital adrenal hyperplasia
Late onset congenital adrenal hyperplasia (CAH) is
responsible for 2–5% of women with hirsutism [2]. It
is almost always due to 21-hydroxylase deficiency,
the enzyme responsible for the conversion of 17a-
hydroxyprogesterone to 11-Deoxycortisol, thus lead-
ing to a reduction in circulating glucocorticoids [9].
This in turn leads to stimulation of ACTH, resulting
in hyperplasia of the adrenal cortex and an increase
of androgens (Figure 5).
CAH is often confused with PCOS, because the
initiation and progress of both are very similar,
starting around puberty, and gradually increasing
with age. They are also both associated with irregular
periods and polycystic ovaries on ultrasound.
However, basal elevated levels of 17a-hydroxypro-
gesterone levels and a positive ACTH stimulation
test is diagnostic of CAH due to 21-hydroxylase
deficiency. Women with CAH demonstrate an
increase in 17a-hydroxyprogesterone levels after
injection of a single dose of 0.25 mg of synthetic
ACTH (Synacthen), is diagnostic of late onset CAH.
Hirsutism: idiopathic
The term idiopathic hirsutism should be applied only
to women with normal ovulatory function and
circulating androgen levels, keeping in mind that a
history of regular menstrual cycles is not adequate to
rule out an ovulatory dysfunction and PCOS [10].
Less than 20% of women with hirsutism are
diagnosed as idiopathic, when the condition is strictly
defined [10]. Increase in skin 5a reductase levels
seems to be the primary pathology in idiopathic
hirsutism. As mentioned earlier, levels of DHT may
be normal despite an increase in 5a reductase activity
due to its quick metabolism in the skin. These
patients usually respond to 5a reductase inhibitor
therapy, and reduction of androgen secretion with
the help of oral contraceptive pills (OCPs) is of
limited value [10].
Hirsutism: iatrogenic
Hirsutism is occasionally due to the side effects of
drugs such as danazol, glucocorticoids, testosterone,
OCPs containing androgenic progesterones, etc.
Figure 5. Mechanism of hirsutism in congenital adrenal
hyperplasia.
144 D. Shah & S. Patel
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 11
/02/
14Fo
r pe
rson
al u
se o
nly.

Therefore, history of drug use is important and
alternative medication should be offered to the
patient.
Diagnosis
Diagnosis of the cause of hirsutism is essential in
order to offer appropriate management to the patient.
Hirsutism should be differentiated from hypertricho-
sis and virilisation. Hypertrichosis is the excessive
growth of androgen independent vellus hair in non-
sexual areas. It is commonly familial, and can also be
seen in conditions such as hypothyroidism, anorexia
nervosa and malnutrition.
Virilisation is a condition in which in addition to
hirsutism, other symptoms of androgen excess such
as clitoromegaly, deepening of voice, increase in
muscle mass and libido, and breast atrophy are also
present.
The diagnosis of hirsutism can be simplified by
proceeding in an organised manner; starting
from history, physical examination and finally
investigations.
History
The history should reveal the onset and progression
of the problem. Although PCOS and late CAH start
at puberty and progress gradually, conditions such
as Cushing’s and androgen secreting tumors occur
at any age and are rapidly progressing. The most
common causes of hirsutism are PCOS and idio-
pathic hirsutism [11]. History of use of drugs
mentioned earlier, may reveal the cause of hirsut-
ism. The presence of menstrual irregularity, acne,
hair loss, clitoromegaly, hoarseness of voice, ab-
dominal weight gain, are the other symptoms of
androgen excess which should be enquired about.
Since thyroid disorders and hyperprolactinaemia
may rarely lead to hirsutism, symptoms regarding
thyroid disorders and galactorrhoea must be
looked into.
Physical examination
Basic physical examination should include height,
weight and calculation of BMI. The degree of
hirsutism can be assessed using the Ferriman–
Gallwey scoring system. This involves grading nine
body areas from zero to four, from no hirsutism to
the presence of severe hirsutism [12]. A score of eight
or more is suggestive of hirsutism. Signs of virilisa-
tion and galactorrhoea should be looked for during
the examination. Pelvic examination may rarely
reveal a palpable ovarian mass.
Moon face, striae, buffalo hump and supraclavi-
cular fat may suggest the diagnosis of Cushing’s
syndrome.
Investigations
Measurement of levels of the various androgenic
hormones may help in diagnosing the source of
androgen production. Serum testosterone levels
poorly correlate with severity of symptoms. However,
it is a useful indicator of serious pathology, and levels
more than 200 ng/dL should warrant further inves-
tigation for neoplasms. Low levels of SHBG are
observed in women with PCOS and are inversely
related to free testosterone levels. Patients with
polycystic ovaries may also exhibit high levels of LH.
Though DHEAS elevations are usually observed in
adrenal pathology, mildly elevated values may be
observed in PCOS. In the presence of DHEAS levels
of more that 700 mg/dL, with or without testosterone
elevation, an androgen producing adrenal tumor
should be strongly suspected [13].
Measurement of basal elevated levels of 17a-
hydroxyprogesterone levels, and an increase in its
level after injection of synthetic ACTH, is diagnostic
of late onset CAH.
Cushing’s syndrome can be evaluated with the
help of ACTH levels, basal and post CRH injection,
and the low and high dexamethasone suppression
test. Although ACTH levels may be normal or high
in pituitary or ectopic ACTH secretion disorders,
they are usually low in adrenal neoplasms. Com-
puted tomography and magnetic resonance imaging
are also useful modalities in diagnosing a pituitary
adenoma.
Treatment options for hirsutism
The management of hirsutism includes cosmetic
and medical management. Although medical
management is required to suppress the cause,
cosmetic treatment is equally essential for patient
satisfaction.
Androgen hormones can be blocked at multiple
levels with the help of anti-androgen therapy. These
include OCPs, cyproterone acetate (CPA), finaster-
ide, spironolactone and flutamide. They may func-
tion via one or multiple mechanisms (Figure 6). In
women with PCOS, insulin sensitisers also seem to
play a role in reduction of hirsutism [14].
Combination OCPs
Combination OCPs commonly contain ethinyl es-
tradiol with a varying progestational agent. The
androgenic activity of progestational agents vary
widely. However, when combined with ethinyl
estradiol, the net effect of the OCP is antiandrogenic
[15]. This antiandrogenic effect is achieved by
decreasing ovarian androgen production and by
increasing the SHBG, thereby reducing the circulat-
ing androgen fraction [16] (Figure 7).
Hirsutism 145
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 11
/02/
14Fo
r pe
rson
al u
se o
nly.

The commonly prescribed OCPs for hirsutism
include a combination of 30 mg of ethinyl estradiol
with either 2 mg of CPA or 3 mg of drosperinone
(DRSP). A similar reduction in hirsutism scores has
been noted with OCPs containing CPA and DRSP
[17].
CPA is a 17-hydroxyprogesterone acetate deriva-
tive that competes with DHT for binding to the
androgen receptor and reduces LH levels which
decrease testosterone and androstenedione levels
[18].
DRSP, however, has both antiandrogen as well as
antimineralocorticoid activity. OCPs containing
DRSP affect adrenal steroidogenesis by reducing
synthesis and release of androgens in response to
ACTH, leaving adrenal production of cortisol un-
changed [6]. Therefore, this drug is effective in the
treatment of hyperandrogenism not only by causing
blockade of ovarian steroid production but also by
acting on the adrenals to reduce adrenal androgen
synthesis. OCPs containing ethinyl estradiol with
DRSP exert a significant antiandrogenic activity, and
is especially effective in improving facial hirsutism.
The beneficial effect is most obvious after six cycles
and continues thereafter at a slower rate [19].
The safety of DRSP has been a matter of concern,
especially with regard to venous thromboembolism.
A recent study based on 142,475 women years of
observation was conducted to compare risks of
adverse cardiovascular and other events associated
with the use of DRSP containing OCPs and other
OCPs. They concluded that the risks of serious
events in users of a DRSP containing OCP are
similar to those associated with the use of other
OCPs [20].
The addition of antiandrogens to OCPs as an add-
on therapy is controversial. However, a recent meta-
analysis included five comparisons of antiandrogens
combined with OCPs versus OCPs alone. These
comparisons showed no significant difference in end-
of-study hirsutism scores between treatment groups
[21]. Besides, addition of higher doses of CPA to
OCPs containing 2 mg of CPA provides no addi-
tional benefit [22].
CPA
CPA is a 17-hydroxyprogesterone acetate derivative
that competes with DHT for binding to the androgen
receptor and reduces LH levels which decrease
testosterone and androstenedione levels [10]. It is
not available in the United States but is used widely
in other countries both alone and as a component of
a combination OCP.
There are no clinical trials comparing CPA alone
with placebo. However, when CPA combined with
ethinyl estradiol as an OCP was compared to
placebo, there was a significant subjective reduction
in hair growth [22]. In studies where CPA was
compared with other drug modalities no difference in
clinical outcome was noted [22]. There were,
however, endocrinological differences in androgen
and estrogen levels between different drug therapies
[22].
Spironolactone
Spironolactone blocks the androgen receptor, inhi-
bits androgen production, and inhibits the 5a
Figure 6. Mechanism of action of anti-androgen drugs.
Figure 7. Mechanism of action of OCPs.
146 D. Shah & S. Patel
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 11
/02/
14Fo
r pe
rson
al u
se o
nly.

reductase enzyme. Because it is an aldosterone
antagonist and a diuretic, its side effects include
polyuria, nocturia, dizziness, and hyperkalemia.
Other side effects such as irregular menstrual cycles
experienced by some women, and feminisation of the
male fetus, may be taken care of by the addition of
OCPs.
Spironolactone is commonly used in the dose of
100 mg per day for the treatment of hirsutism. The
Cochrane Database review involved a study of
spironolactone versus placebo or other antiandrogens
for hirsutism [23]. They concluded that 6 months of
treatment with 100 mg/day spironolactone compared
with placebo was associated with a statistically
significant subjective improvement in hair growth
and Ferriman–Galwey scores. Further, spironolac-
tone 100 mg/day is superior to finasteride 5 mg/day
and low dose CPA 12.5 mg/day (first 10 days of
cycle) up to 12 months after the end of treatment
[23].
Finasteride
Finasteride is a 5a reductase inhibitor, which reduces
the conversion of testosterone to the more potent
DHT. It is prescribed in the dose of 5 mg per day for
the treatment of hirsutism. Because finasteride can
cause feminisation of the male fetus, women of
reproductive age group must use effective contra-
ception during its use and they should be warned that
a 3-month drug-free period is required before they
get pregnant [8].
In comparison with other antiandrogen therapies,
although finasteride is equally effective to CPA and
ethinyl estradiol combination [24,25], it seems less
beneficial when compared with spironolactone [23].
Flutamide
Flutamide is a nonsteroidal androgen receptor
blocker used in the dose of 250–500 mg per day for
the treatment of hirsutism. It can especially be used
in women in whom estrogen therapy is contra-
indicated. Flutamide can cause feminisation of the
male fetus and women of reproductive age group
must use effective contraception.
Although flutamide is effective in reducing hirsut-
ism, potential hepatotoxicity, occasionally fatal,
limits the usefulness of this drug in hirsutism.
Insulin sensitisers
Hirsutism is frequently encountered in women with
PCOS, who also exhibit relative insulin resistance.
Besides, obesity has a negative impact on the
efficacy of treatments for hirsutism, thus weight
loss is necessary for a successful treatment
program [26].
There is promising data regarding the effects of
insulin sensitisers in the treatment of hirsutism,
particularly in patients with PCOS [14]. Data suggest
that hirsutism may be effectively treated by reducing
hyperinsulinaemia [27].
In comparison with OCPs containing CPA,
the latter was found to be responsible for
profound suppression of androgen activity, in
contrast to metformin, which induced negligible
change [27].
Meta-analysis of comparisons of other antian-
drogens (spironolactone and flutamide) with
metformin, showed that the antiandrogen group
had significantly lower hirsutism scores than the
metformin group, but with large inconsistency across
studies [21]. Further, meta-analysis also revealed
that patients receiving a combination of flutamide
and metformin had significantly lower hirsutism
scores than patients receiving metformin alone [21].
Cosmetic treatment for hirsutism
Drugs are only partially effective on terminalised
hairs, and removal of these hairs is usually required.
Therefore, management of hirsutism is generally
based upon a dual approach: a pharmacological
therapy to reduce androgen secretion and/or andro-
gen action, and removal of terminal hair already
present. Electrolysis and laser photothermolysis are
considered the most effective cosmetic procedures,
although the effects of these methods should not be
considered permanent [28]. The application of
eflornithine hydrochloride 13.9% topical cream
may also be useful to ameliorate unwanted facial
hair growth [29].
Conclusion
Hirsutism has a significant negative impact on
psychosocial development and is usually a sign of
an underlying endocrine abnormality – namely,
androgen excess. A combination of one or more
treatments, including oral contraceptives, insulin
sensitisers, peripheral androgen blockade (spirono-
lactone, flutamide, CPA, or finasteride), and
mechanical/cosmetic amelioration and destruction
of unwanted hair (electrology and, potentially, laser
hair removal), is usually beneficial to the patient.
Overall, although hirsutism is a frequent and distres-
sing abnormality often signalling an underlying
endocrine disorder, a systematic approach to evalua-
tion will uncover the etiology, and combination
therapy will provide satisfactory treatment for most
patients.
Declaration of interest: The authors report no
conflicts of interest. The authors alone are respon-
sible for the content and writing of the study.
Hirsutism 147
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 11
/02/
14Fo
r pe
rson
al u
se o
nly.

References
1. Mofid A, Ahmad S, Alinaghi S, Zandieh S, Yazdani T.
Hirsutism. Int J Clin Pract 2008;62:433–443.
2. Nikolaoua D, Gilling-Smith C. Hirsutism. Curr Obstet
Gynaecol 2005;15:174–182.
3. Lobo RA, Goebelsmann U, Horton R. Evidence for the
importance of peripheral tissue events in the development of
hirsutism in polycystic ovary syndrome. J Clin Endocrinol
Metab 1983;57:393–397.
4. Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus
Workshop Group. Revised 2003 consensus on diagnostic
criteria and long-term health risks related to polycystic ovary
syndrome. Fertil Steril 2004;81:19–25.
5. The Rotterdam ESHRE/ASRM-Sponsored PCOS consensus
workshop group. Revised 2003 consensus on diagnostic
criteria and long-term health risks related to polycystic ovary
syndrome (PCOS). Hum Reprod 2004;19:41–47.
6. Kazer RR, Kessel B, Yen SSC. Circulating luteinizing
hormone pulse frequency in women with polycystic ovary
syndrome. J Clin Endocrinol Metab 1987;65:233–236.
7. Futterweit MD, Dunaif A, Yeh H-C, Kingsley P. The
prevalence of hyperandrogenism in 109 consecutive female
patients with diffuse alopecia. J Am Acad Dermatol
1988;19:831–836.
8. Olah KS. The modern management of hirsutism. Rev Gynecol
Pract 2004;4:211–220.
9. Hawkins LA, Chasalow FI, Blethen SL. The role of
adrenocorticotropin testing in evaluating girls with premature
adrenarche and hirsutism/oligomenorrhea. J Clin Endocrinol
Metab 1992;74:248–253.
10. Azziz R, Carmina E, Sawaya ME. Idiopathic hirsutism.
Endocrinol Rev 2000;21:347–362.
11. Hassa H, Mete Tanir H, Yildirim A, Senses T, Eskalen M,
Mutlu FS. The hirsutism scoring system should be population
specific. Fertil Steril 2005;84:778–780.
12. Ferriman D, Galiwey JD. Clinical assessment of body hair
growth in women. J Clin Endocrinol Metab 1961;21:1440–
1447.
13. Stanczyk FZ. Diagnosis of hyperandrogenism: biochemical
criteria. Best Pract Res Clin Endocrinol Metab 2006;20:177–
191.
14. Sahin Y, Kelestimur F. Medical treatment regimens of
hirsutism. Reprod Biomed Online 2004;8:538–546.
15. Koulianos G. Treatment of acne with oral contraceptives:
criteria for pill selection. Cutis 2000;66:281–286.
16. Harper JC. Antiandrogen therapy for skin and hair disease.
Dermatol Clin 2006;24:137–143.
17. Batukan C, Muderris II, Ozcelik B, Ozturk A. Comparison of
two oral contraceptives containing either drospirenone or
cyproterone acetate in the treatment of hirsutism. Gynecol
Endocrinol 2007;23:38–44.
18. Vincenzo D, Giuseppe M, Paola P, Musacchio MC,
Petraglia F, Cianci A. Evaluation of effects of an oral
contraceptive containing ethinyl estradiol combined with
drosperinone on adrenal steroidogenesis in hyperandrogenic
women with polycystic ovary syndrome. Fertil Steril 2007;88:
113–117.
19. Cem B, Ipek M. Efficacy of a new oral contraceptive
containing drosperinone and ethinyl estradiol in long term
treatment of hirsutism. Fertil Steril 2006;85:436–440.
20. Dinger JC, Heinemann LA, Habich DK. The safety of a
drosperinone- containing oral contraceptive: final results from
the European Active Surveillance study on Oral Contra-
ceptives based on 142,475 women-years of observation.
Contraception 2007;75:344–354.
21. Swiglo BA, Cosma M, Flynn DN, Kurtz DM, Labella ML,
Mullan RJ, Erwin PJ, Montori VM. Antiandrogens for the
treatment of hirsutism: a systematic review and meta-analysis
of randomised controlled trials. J Clin Endocrinol Metab
2008;93:1153–1160.
22. Van der Spuy ZM, le Roux PA. Cyproterone acetate for
hirsutism. Cochrane Database Syst Rev 2003;4:CD001125.
23. Farquhar C, Lee O, Toomath R, Jepson R. Spironolactone
versus placebo or in combination with steroids for
hirsutism and/or acne. Cochrane Database Syst Rev 2003;4:
CD000194.
24. Beigi A, Sobhi A, Zarrinkoub F. Finasteride versus cyproter-
one acetate-estrogen regimens in the treatment of hirsutism.
Int J Gynaecol Obstet 2004;87:29–33.
25. Sahin Y, Bayram F, Kelestimur F, Muderris I. Comparison of
cyproterone acetate plus ethinyl estradiol and finasteride in
the treatment of hirsutism. J Endocrinol Invest 1998;21:348–
352.
26. Koulouri O, Conway GS. A systematic review of commonly
used medical treatments for hirsutism in women. Clin
Endocrinol (Oxf) 2008;68:800–805.
27. Harborne L, Fleming R, Lyall H, Sattar N, Norman J.
Metformin or antiandrogen in the treatment of hirsutism in
polycystic ovary syndrome. J Clin Endocrinol Metab
2003;88:4116–4123.
28. Moghetti P, Toscano V. Treatment of hirsutism and acne in
hyperandrogenism. Best Pract Res Clin Endocrinol Metab
2006;20:221–234.
29. Azziz R. The evaluation and management of hirsutism. Obstet
Gynecol 2003;101:995–1007.
148 D. Shah & S. Patel
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 11
/02/
14Fo
r pe
rson
al u
se o
nly.