hepatitis c treatment in the direct acting antiviral...
TRANSCRIPT
1
Hepatitis C Treatment in the Direct Acting
Antiviral Era - The Pharmacist’s Role
R. Andy Rathbun PharmD, AAHIVP
HCV / HIV / ID Ambulatory Care Pharmacist
Kaiser Permanente, San Diego
2

Disclosure
Clinical investigator with research grants funded by Gilead Sciences, AbbVie, Merck, and Intercept Pharmaceuticals
All grants paid to institution only
3

Learning Objectives
1) Describe the natural history and health burden of hepatitis C
2) Evaluate the current recommendations and treatment options available for hepatitis C
3) Identify areas in which pharmacists can play a significant role in hepatitis C care
4) Develop a basic understanding of what hepatitis C care will look like in the future
4

Discovered in 1989 Previously known as Non-A / Non-B hepatitis
Blood-borne virus that causes inflammation of the liver Disease severity varies between mild short-lived illness to serious lifelong infection
HCV resides in the cytoplasm of hepatocytes Does not integrate into host DNA, unlike HIV Ability to achieve cure
Hepatitis C Virus (HCV)
Rice CM. Top Antivir Med 2011; 19(3):117-20 5
Image Source (Accessed September 12, 2016): http://admin2.aidsbg.info/upload/a111/hcv.jpg
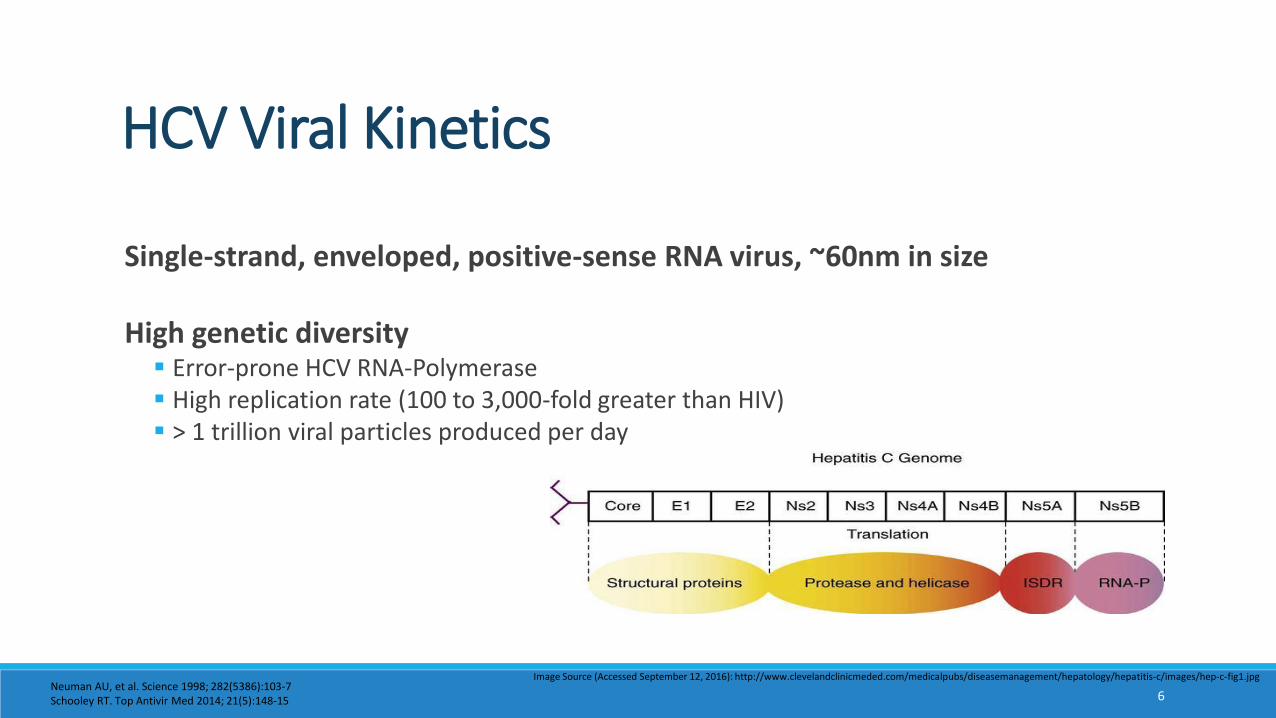
Single-strand, enveloped, positive-sense RNA virus, ~60nm in size
High genetic diversity Error-prone HCV RNA-Polymerase High replication rate (100 to 3,000-fold greater than HIV) > 1 trillion viral particles produced per day
HCV Viral Kinetics
Neuman AU, et al. Science 1998; 282(5386):103-7Schooley RT. Top Antivir Med 2014; 21(5):148-15 6
Image Source (Accessed September 12, 2016): http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/hepatology/hepatitis-c/images/hep-c-fig1.jpg
If a patient’s daily HCV production was laid end-to-end, how many lengths of a football field would it span?
Trivia Question
7
Image Source (Accessed September 12, 2016): http://clipartix.com/wp-content/uploads/2016/07/Football-field-materials-free-clip-art.png
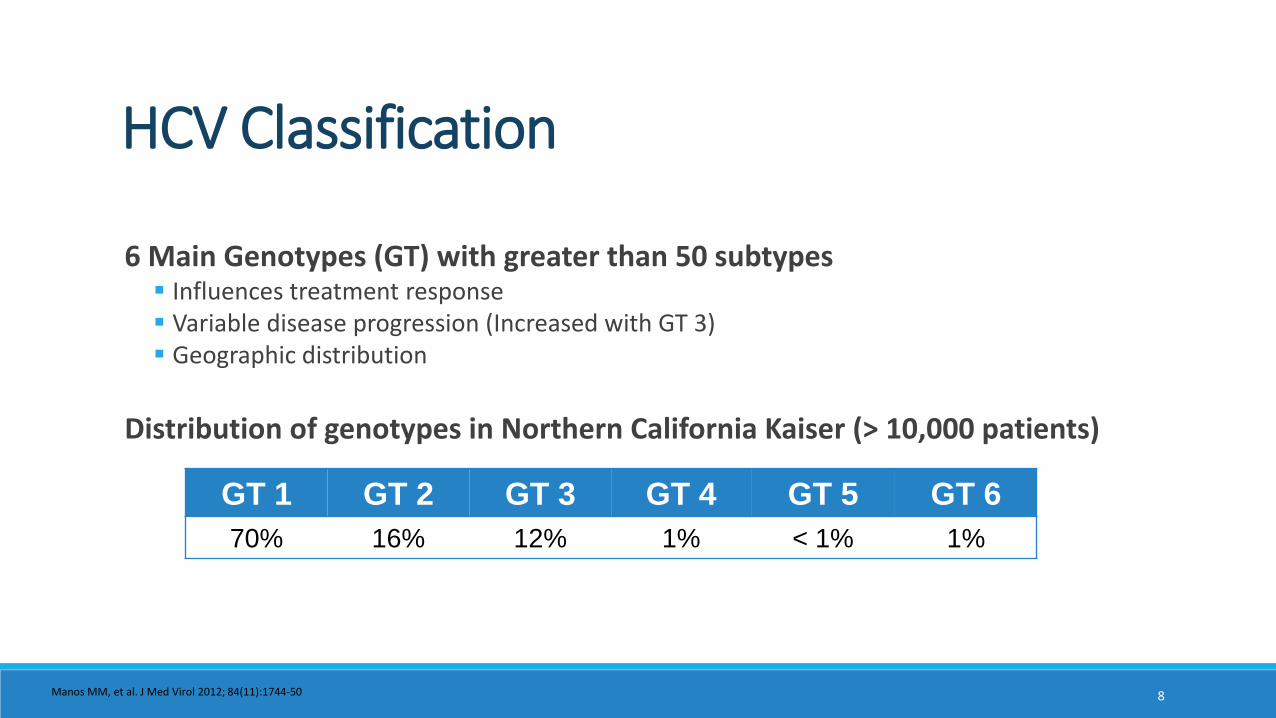
6 Main Genotypes (GT) with greater than 50 subtypes Influences treatment response Variable disease progression (Increased with GT 3) Geographic distribution
Distribution of genotypes in Northern California Kaiser (> 10,000 patients)
HCV Classification
GT 1 GT 2 GT 3 GT 4 GT 5 GT 6
70% 16% 12% 1% < 1% 1%
Manos MM, et al. J Med Virol 2012; 84(11):1744-50 8

3.2 million (1% to 1.5%) US persons living with HCV ~50 to 75% are undiagnosed
Baby boomers (birth 1945-1965) account for 75% of infections 5x greater risk of HCV infection Majority of these HCV infections occurred in 1970’s and 80’s
Epidemiology of Chronic HCV
MMWR 2012;61(No. RR-4)9
Image Source (Accessed September 12, 2016): https://encrypted-tbn1.gstatic.com/images?q=tbn:ANd9GcTE6RbIutqXCdN2qaL5L8c8LBO1_UzirStQRIBqpiX1y8SxED0R

HCV causes inflammation and injury to the liver Result of which is the progression of fibrosis (essentially scarring)
METAVIR scoring for liver fibrosis F0 to F4 categorization F0 = No fibrosis F4 = Cirrhosis
HCV as a Cause of Liver Damage
Naggie S. Top Antivir Med 2012; 20(5):154-161Sherman KE. Top Antivir Med 2011; 19(3):121-125 10
Image Source (Accessed September 12, 2016): http://baby-boomer-depot.com/wp-content/uploads/2012/09/Stages-of-Liver-deterioration-with-Hepatitis.jpg

Natural History and Progression of HCV
75 – 85%
20 - 30%
2 - 7% per year
11Image Source (Accessed September 12, 2016): Used with permission of Hepatitis C Online (Copyright © 2016 Hepatitis C Online – AWS)http://www.hepatitisc.uw.edu/pdf/evaluation-staging-monitoring/natural-history/core-concept/all

12
Risk of Accelerated Fibrosis
Factors Associated With Accelerated Fibrosis Progression
Host Factors
Non-modifiable Fibrosis stage Inflammation grade Older age at time of infection Male sex Organ Transplant
Modifiable Alcohol consumption Nonalcoholic fatty liver disease Obesity Insulin resistance
Viral Factors
HCV genotype 3 Coinfection with hepatitis B virus or HIV
AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.

Portal hypertension
Ascites
Encephalopathy
Variceal bleeding
Coagulopathy
Spontaneous bacterial peritonitis (SBP)
Hepatocellular carcinoma (HCC)
Hepatorenal syndrome
Hepatic hydrothorax
Complications of Cirrhosis
Sherman KE. Top Antivir Med 2011; 19(3):121-125 13
Image Source (Accessed September 12, 2016): http://en.wikipedia.org/wiki/File:Hepaticfailure.jpg

Extrahepatic Manifestations
Hematological B-Cell Non-Hodgkin’s Lymphoma Thrombocytopenia Mixed cryoglobulinemia
Dermatological Lichen planus Porphyria cutanea tarda Pruritus
Endocrine Disorders Thyroid disease Type II Diabetes
Central Nervous System Depression Weakness / myalgia Peripheral neuropathy
Rheumatologic Disorders Polyarthralgia Systemic Lupus Erythematosus Sjogren’s syndrome
Renal Glomerulonephritis Nephrotic Syndrome
Zignego AL, et al. Intern Emerg Med 2012; 7(Suppl 7):S201-208Jacobson IM, et al. Clin Gastroenterol Hepatol 2010; 8:1017-1029 14
Image Source (Accessed September 12, 2016): http://mddk.com/wp-content/uploads/2014/07/porphyria-cutanea-tarda-2.jpgImage Source (Accessed September 12, 2016): http://en.wikipedia.org/wiki/File:Cryoglobulinemia2.jpg

HCV is the leading cause of: Cirrhosis HCC Liver transplantation Liver-related deaths
From 2003 to 2013 HCV-associated deaths surpassed 60 other nationally notifiable infectious diseases combined
People with chronic HCV live on average 15 years less than people without HCV
Chronic HCV: Silent but Deadly
15Chhawal J, et al. Hepatology 2016 [Epub ahead of print; Accessed: 9/10/16]Ly KN, et al. Clin Infect Dis 2016;62(10):1287-8Mahajan R, et al. Clin Infect Dis 2014;58(8):1055-61
16
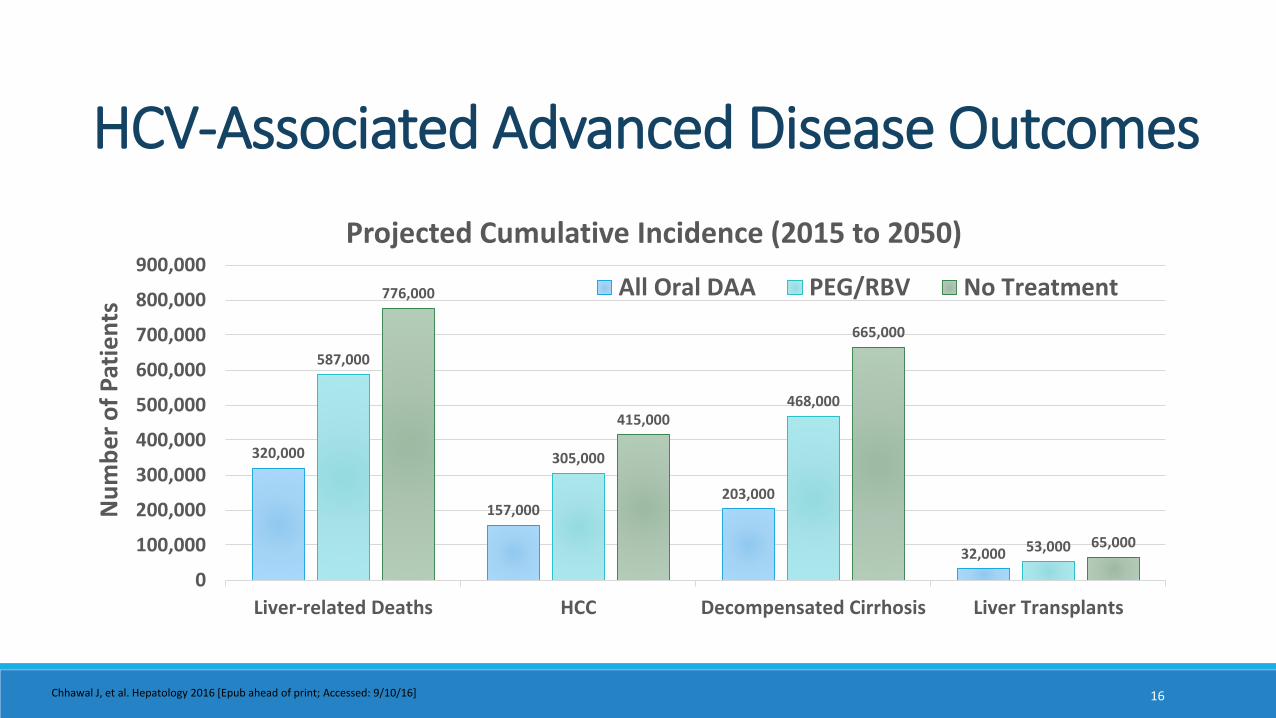
HCV-Associated Advanced Disease Outcomes
320,000
157,000203,000
32,000
587,000
305,000
468,000
53,000
776,000
415,000
665,000
65,000
0
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
900,000
Liver-related Deaths HCC Decompensated Cirrhosis Liver Transplants
All Oral DAA PEG/RBV No Treatment
Nu
mb
er
of
Pat
ien
ts
Projected Cumulative Incidence (2015 to 2050)
Chhawal J, et al. Hepatology 2016 [Epub ahead of print; Accessed: 9/10/16]

$0
$50,000
$100,000
$150,000
$200,000
$250,000
$300,000
No Chronic HCV HCV Non-Cirrhotic
HCVCompensated
Cirrhosis
HCVDecompensated
Cirrhosis
HCV HCC HCV LiverTransplant
$5,676 $19,596 $22,620 $40,320
$94,848
$259,068
Annual Healthcare Costs Between Non-HCV and Chronic HCV Patients
17
Economic Burden of Chronic HCVA
nn
ual
He
alth
care
Co
sts
Walker DR, et al. J Hepatol 2015;62 (Suppl):S593-594

GOALS OF THERAPY AND TREATMENT RECOMMENDATIONS
18

Virologic cure Sustained Virologic Response (SVR) = No HCV detected 12 weeks after treatment completion
Health-benefits of achieving SVR 70% risk reduction for liver cancer 90% risk reduction in liver transplant and liver-related mortality Improvement in all-cause mortality and liver-related health adverse consequences Reduced mortality related to extrahepatic manifestations
Goals of HCV Treatment
van der Meer, et al. JAMA 2012;308(24):2584-2593McCombs, et al. JAMA Intern Med 2014;174(2):204-212Morgan, et al. Ann Intern Med 2013;158(5):329-337
19

WHO Everyone with chronic HCV Exception = Short-life expectancy
Considerations in timing Extrahepatic manifestations Advanced liver disease Higher risk of accelerated fibrosis progression Earlier the better (Early fibrosis stages) Reduce risk of transmission
20
HCV Treatment: Who and When
Pharmacy Directors in charge of the medication budget may want to cover their ears
Image Source (Accessed September 12, 2016): http://images.popmatters.com/misc_art/b/brottman-monkeyear-splsh.jpg
AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.

1991 - 2011
interferon (IFN)
peginterferon(PEG)
ribavirin (RBV)
FDA Approved HCV Agents
2011 - 2013
NS3/4A Protease Inhibitor (PI)
boceprevir(BOC)
telaprevir(TVR)
2013 - 2014
NS3/4A Protease Inhibitor (PI)
simeprevir(SMV)
NS5B Polymerase Inhibitor
sofosbuvir(SOF)
2014 - 2015
NS5A Inhibitor
daclatasvir(DCV)
Combination DAA’s
ledipasvir/ sofosbuvir(LDV/SOF)
paritaprevir / ritonavir / ombitasvir+ dasabuvir(PrOD)
paritaprevir / ritonavir / ombitasvir(PrO)
2016
Combination DAA’s
PrOD Extended Release (XR)
sofosbuvir/ velpatasvir(SOF/VEL)
elbasvir/ grazoprevir(EBR/GZR)
21AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.

0
10
20
30
40
50
60
70
80
90
100
IFN (24) IFN (48) IFN/RBV(24)
IFN/RBV(48)
PEG (48) PEG/RBV(48)
PI +PEG/RBV(24-48)
DAA +PEG/RBV(12-48)
All OralDAA (8-24)
SVR
(%
)
1991
1998
2011
History of HCV Treatment Response2013 - Present
2001
22
Treatment (Duration = Weeks)
Figure Adapted from the US Food and Drug Administration, Antiviral Drugs Advisory Committee Meeting, April 27-28, 2011, Silver Spring, MD.AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.
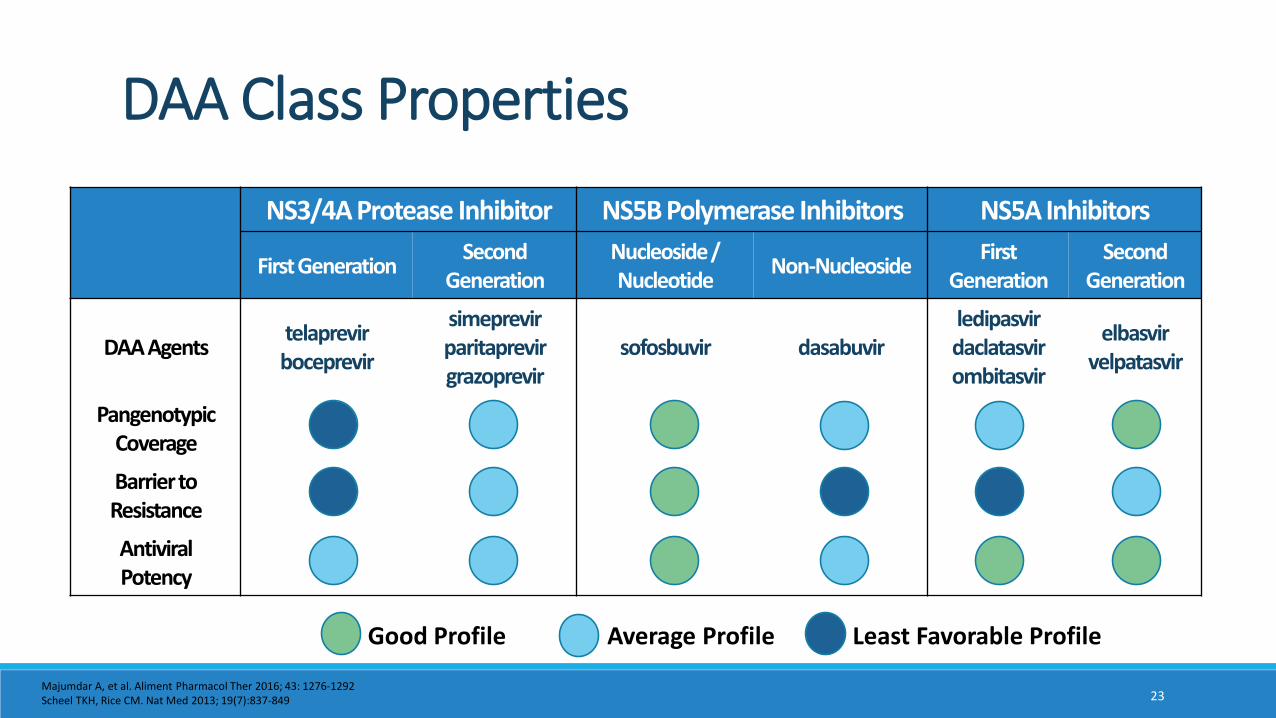
NS3/4A Protease Inhibitor NS5B Polymerase Inhibitors NS5A Inhibitors
First GenerationSecond
GenerationNucleoside/ Nucleotide
Non-NucleosideFirst
GenerationSecond
Generation
DAA Agentstelaprevirboceprevir
simeprevirparitaprevirgrazoprevir
sofosbuvir dasabuvirledipasvirdaclatasvirombitasvir
elbasvirvelpatasvir
PangenotypicCoverage
Barrierto Resistance
Antiviral Potency
DAA Class Properties
Good Profile Average Profile Least Favorable Profile
Majumdar A, et al. Aliment Pharmacol Ther 2016; 43: 1276-1292Scheel TKH, Rice CM. Nat Med 2013; 19(7):837-849 23

AASLD / IDSA National Guidelines
Factors influencing selection of recommended regimens Efficacy Treatment history Extent of liver disease Genotype Resistance Associated Variants (RAVs) Drug Interactions Patient comorbidities Side effect profile
Treatment Regimen Recommendations
24AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.

AASLD / IDSA Recommended Regimens
RegimenGenotype
1a 1b 2 3 4 5 6
elbasvir / grazoprevir X X X
ledipasvir / sofosbuvir X X X X X
PrOD ± ribavirin X^ X
PrO + ribavirin X
simeprevir + sofosbuvir X X
sofosbuvir / velpatasvir X X X X X X X
daclatasvir + sofosbuvir X X X
^ RBV included
25AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.

RegimenGenotype (GT)
(1a / 1b)Non-
CirrhoticCompensated
CirrhosisTreatment
Length (Weeks)
elbasvir / grazoprevir GT1a / GT1b + + 12
ledipasvir / sofosbuvir ± RBV GT1a / GT1b + + 8 - 12
PrOD + RBV GT1a only + - 12
PrOD GT1b only + + 12
simeprevir + sofosbuvir GT1a / GT1b + - 12
sofosbuvir / velpatasvir GT1a / GT1b + + 12
daclatasvir + sofosbuvir GT1a / GT1b + - 12
AASLD / IDSA RecommendationsTreatment Naïve & Previous PEG/RBV Failure (Genotype 1)
elbasvir / grazoprevir - GT 1a check for baseline NS5A RAVs, if present, consider alternative treatment or lengthen treatment to 16 weeks with Ribavirin ledipasvir / sofosbuvir - Alternative regimen of 8 weeks treatment duration in non-cirrhotic patients with baseline HCV viral load < 6 million copies ledipasvir / sofosbuvir + ribavirin used in Genotype 1a and 1b patients with cirrhosis and previous failure to PEG / RBV
26AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.
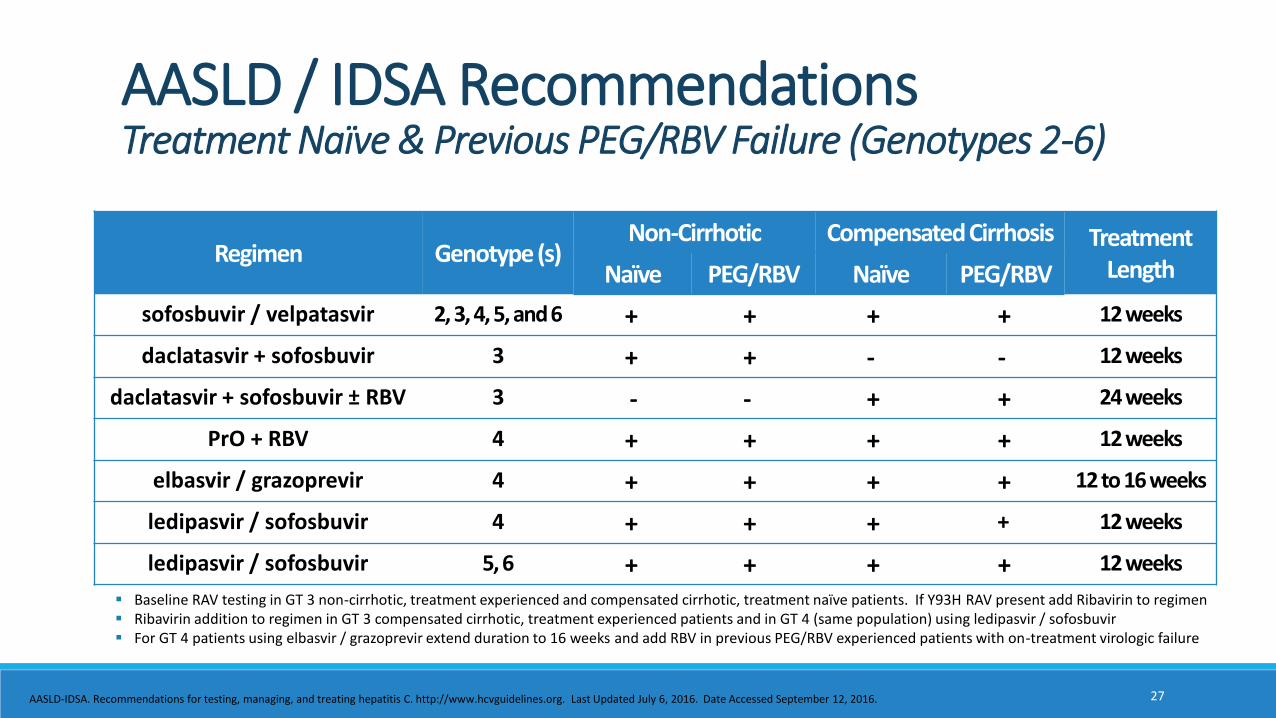
Regimen Genotype (s)Non-Cirrhotic Compensated Cirrhosis Treatment
LengthNaïve PEG/RBV Naïve PEG/RBV
sofosbuvir / velpatasvir 2, 3, 4, 5, and 6 + + + + 12 weeks
daclatasvir + sofosbuvir 3 + + - - 12 weeks
daclatasvir + sofosbuvir ± RBV 3 - - + + 24 weeks
PrO + RBV 4 + + + + 12 weeks
elbasvir / grazoprevir 4 + + + + 12 to 16 weeks
ledipasvir / sofosbuvir 4 + + + + 12 weeks
ledipasvir / sofosbuvir 5, 6 + + + + 12 weeks
AASLD / IDSA RecommendationsTreatment Naïve & Previous PEG/RBV Failure (Genotypes 2-6)
Baseline RAV testing in GT 3 non-cirrhotic, treatment experienced and compensated cirrhotic, treatment naïve patients. If Y93H RAV present add Ribavirin to regimen Ribavirin addition to regimen in GT 3 compensated cirrhotic, treatment experienced patients and in GT 4 (same population) using ledipasvir / sofosbuvir For GT 4 patients using elbasvir / grazoprevir extend duration to 16 weeks and add RBV in previous PEG/RBV experienced patients with on-treatment virologic failure
27AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.

RegimenTreatment Length
Non-cirrhotic Compensated Cirrhosis
Genotype 1
ledipasvir / sofosbuvir + RBV 12 weeks 24 weeks
Genotype 2
daclatasvir + sofosbuvir ± RBV 24 weeks 24 weeks
sofosbuvir / velpatasvir + RBV 12 weeks 12 weeks
Genotype 3
daclatasvir + sofosbuvir + RBV 24 weeks 24 weeks
sofosbuvir / velpatasvir + RBV 12 weeks 12 weeks
AASLD / IDSA RecommendationsRetreatment Previous SOF + RBV ± PEG Failures
28AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.

AASLD / IDSA RecommendationsRetreatment Previous Protease Inhibitor + PEG/RBV Failures
RegimenTreatment Length
Non-cirrhotic Compensated Cirrhosis
Genotype 1
ledipasvir / sofosbuvir + RBV 12 weeks 12 weeks
ledipasvir / sofosbuvir N/A 24 weeks
sofosbuvir / velpatasvir 12 weeks 12 weeks
daclatasvir + sofosbuvir ± RBV 12 weeks 24 weeks
elbasvir / grazoprevir + RBV 12 – 16 weeks 12 - 16 weeks
29
Previous Protease Inhibitors = telaprevir, boceprevir, simeprevir elbasvir / grazoprevir extend duration to 16 weeks in previous PEG/RBV experienced patients with on-treatment virologic failure
AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.

Previous simeprevir + sofosbuvir OR NS5A Inhibitor containing regimens (GT1)
Defer treatment = Non-cirrhotic and no other reasons for urgent treatment
Consideration for retreatment in cirrhosis or other reason for urgent treatment RAV Testing for both NS3/4A Protease Inhibitor and NS5A Inhibitors
30
AASLD / IDSA RecommendationsRetreatment Regimens Containing Multiple DAAs
AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.

RegimenDecompensated
CirrhosisSevere Renal Impairment
(CrCl < 30 mL/min)Recurrent HCV Post-Liver
Transplantation
elbasvir / grazoprevir No Yes N/A
ledipasvir / sofosbuvir Yes No Genotypes 1 and 4
PrOD ± ribavirin No Yes Alternative
simeprevir + sofosbuvir No No Alternative
sofosbuvir / velpatasvir Yes No N/A
daclatasvir + sofosbuvir Yes No Genotypes 1, 2, 3 and 4
sofosbuvir + ribavirin No No Genotype 2
AASLD / IDSA RecommendationsRenal, Decompensated Cirrhosis & Post-Liver Transplant
31
Decompensated cirrhosis and recurrent HCV post-liver transplantation: RBV eligible - Add RBV x 12 weeks / RBV ineligible - No RBV x 24 weeks PrOD is recommended in severe renal impairment for GT 1b and as an alternative with RBV in GT 1a Sofosbuvir + ribavirin is the preferred option in RBV eligible patients with GT 2 post-liver transplant recurrent HCV infection and decompensated cirrhosis
AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.

AASLD / IDSA RecommendationsHIV/HCV Coinfection
Priority population for treatment◦ Increased risk of liver disease progression
SVR rates similar to HCV monoinfected
Do not interrupt HIV treatment◦ PrO and PrOD use only for patients on HIV therapy◦ Stable on HIV therapy for 1 month before starting
HCV DAA(s) Antiretroviral Drug Interactions
daclatasvirEfaverinz; Etravirine; Nevirapine;
Cobicistat; Atazanavir boosted-ritonavir
elbasvir/ grazoprevirEfaverinz; Etravirine; Nevirapine;
Protease Inhibitors; Cobicistat
sofosbuvir/ velpatasvirEfaverinz,Etravirine, Nevirapine
Regimens containing TDF
ledipasvir/ sofosbuvir Regimens containing TDF
PrODEfaverinz; Etravirine; Nevirapine; Rilpivirine; Cobicistat; Darunavir
simeprevirEfaverinz; Etravirine; Nevirapine;
Protease Inhibitors; Cobicistat
32AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.

3- 10 tabs total daily scheduled Qday or BID
• PrO + RBV
• PrOD ± RBV
• PrOD XR ± RBV
2 tabs Qday
daclatasvir + sofosbuvir
simeprevir + sofosbuvir
1 tab Qday
• elbasvir / grazoprevir
• ledipasvir / sofosbuvir
• sofosbuvir / velpatasvir
Pill Burden and Administration
With Food Without Regards to Food
33Reference – Individual medication package insert (available on reference slide)

Warnings and Precautions
Serious Symptomatic Bradychardia
• Amiodarone with sofosbuvir and ledipasvir, velpatasvir, simeprevir, or daclatasvir
Hepatic Decompensation and Hepatic Failure (Moderate / Severe Hepatic Impairment)
• Not Recommended: simeprevir / Contraindicated: PrOD, PrOD XR, PrO, elbasvir/grazoprevir
ALT Elevations
• PrOD, PrOD XR, PrO, elbasvir/grazoprevir
Photosensitivity / Rash / Sulfa Allergy
• simeprevir
34Reference – Individual medication package insert (available on reference slide)
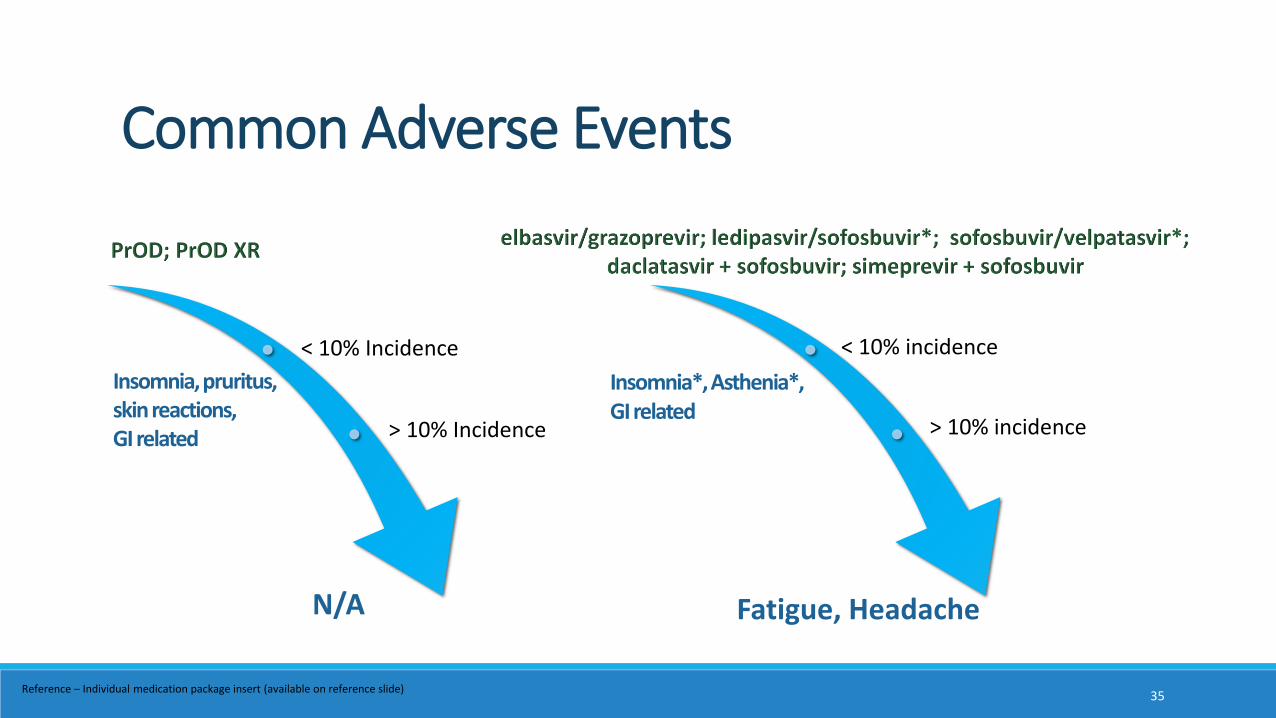
Common Adverse Events
Insomnia*, Asthenia*,GI related
Fatigue, Headache
Insomnia, pruritus,skinreactions, GI related
N/A
< 10% incidence
> 10% incidence
< 10% Incidence
> 10% Incidence
35Reference – Individual medication package insert (available on reference slide)
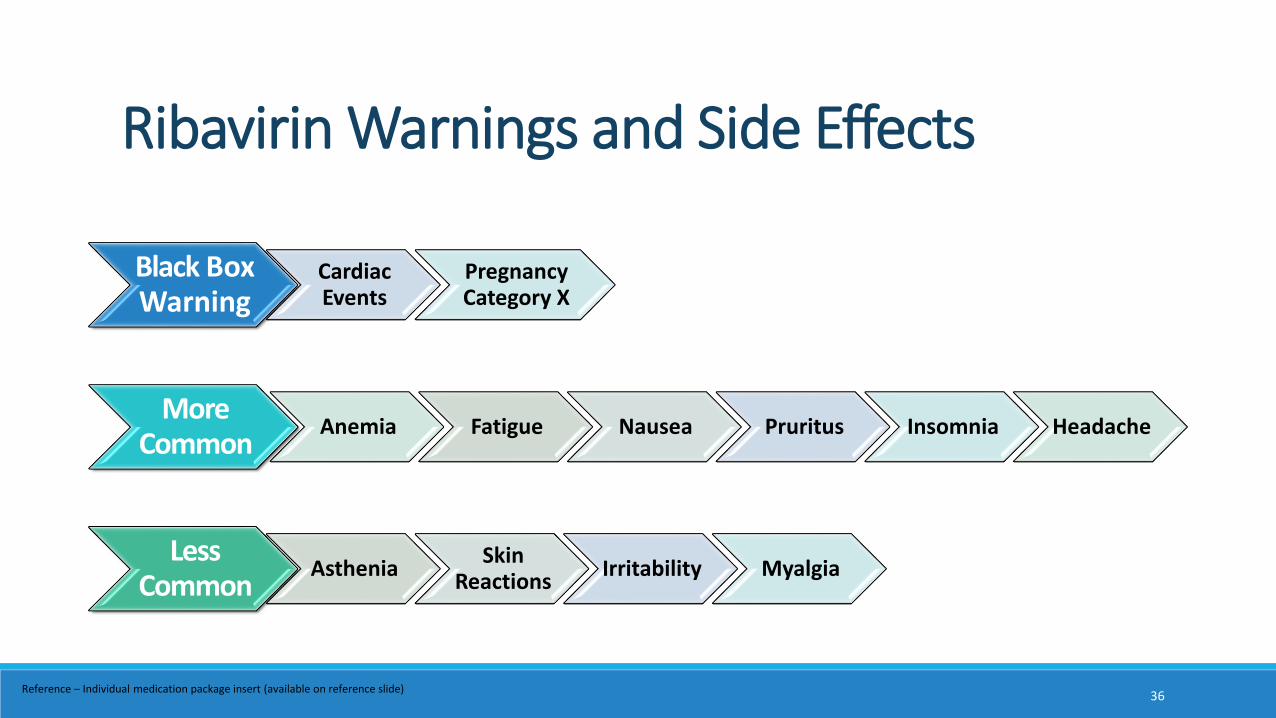
Ribavirin Warnings and Side Effects
Black Box Warning
Cardiac Events
Pregnancy Category X
More Common
Anemia Fatigue Nausea Pruritus Insomnia Headache
Less Common
AstheniaSkin
ReactionsIrritability Myalgia
36Reference – Individual medication package insert (available on reference slide)
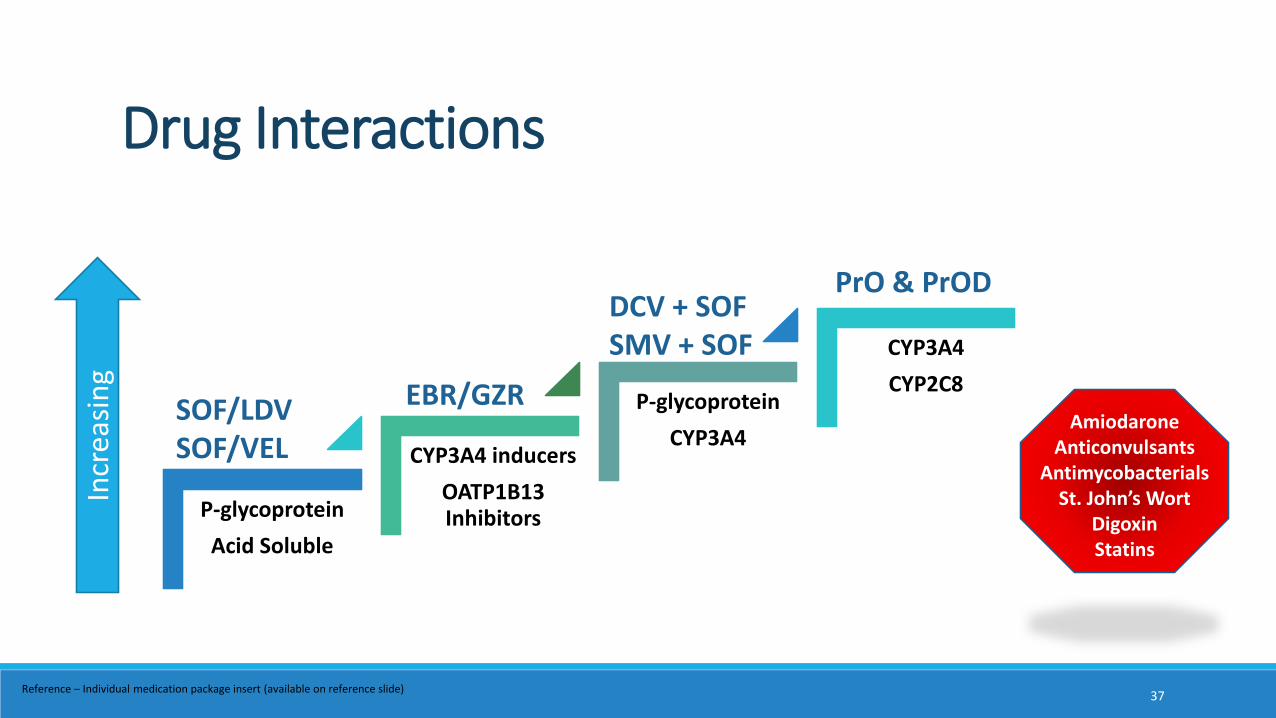
Drug Interactions
P-glycoprotein
Acid Soluble
CYP3A4 inducers
OATP1B13 Inhibitors
P-glycoprotein
CYP3A4
CYP3A4
CYP2C8SOF/LDVSOF/VEL
EBR/GZR
DCV + SOFSMV + SOF
PrO & PrOD
Incr
easi
ng
AmiodaroneAnticonvulsants
AntimycobacterialsSt. John’s Wort
DigoxinStatins
37Reference – Individual medication package insert (available on reference slide)

PHARMACIST ’S INVOLVEMENT
38
Pharmacist’s Primary Responsibilities Treatment referral review Patient treatment scheduling Patient education visit to review treatment plan Follow up on treatment Treatment outcomes
HEPATITIS C CLINICPharmacists R. Andy Rathbun, Lubna Kazi, Chrislynn Chew, Cindy NgoMDs Heather Patton, Mamie Dong, Lisa Nyberg, Anders NybergPAs Debbie Muratet, Brian FarbRN Coordinators Joyce Kreutzberg, Beth WaltersLVN Julita DioquinoSupport Coordinator RaChae TudaraPharmacy Leadership Jennigrace Bautista, Lina Delosreyes
Clinic Team
39

Pretreatment Evaluation
Medical history Previous HCV treatment / response Liver disease staging Transplant status Drug interaction evaluation
Treatment Readiness Comorbidities Adherence to care Substance abuse Coverage, expected costs, and financial
assistance
Labs (within 12 weeks of treatment) CBC, INR, AST, ALT, total and direct
bilirubin, ALK Phos, Scr and calculated CrCL HIV serology Hepatitis A and B serology (Immunization) HCV genotype / subtype (anytime) Quantitative HCV viral load Pregnancy testing RAV testing as appropriate Substance abuse panel as appropriate
40AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.

Regular clinic visits and/or telephone contact Adherence; Adverse Events; Drug Interactions
Labs including HCV viral load after week 4 and as appropriate
Early Discontinuation On-treatment virologic failure Drug specific recommendations for monitoring of liver toxicity or decompensation
elbasvir / grazoprevir PrO and PrOD based regimens
Monitoring During Treatment
41AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.

Monitoring of cirrhosis, regardless of treatment response HCC screening every 6 months Endoscopic esophageal varices screening
Failed to achieve SVR Disease progression assessment every 6 to 12 months Continued evaluation of retreatment appropriateness
Achieved SVR No advanced fibrosis = No additional follow up necessary
Monitoring After Treatment Completion
42AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.
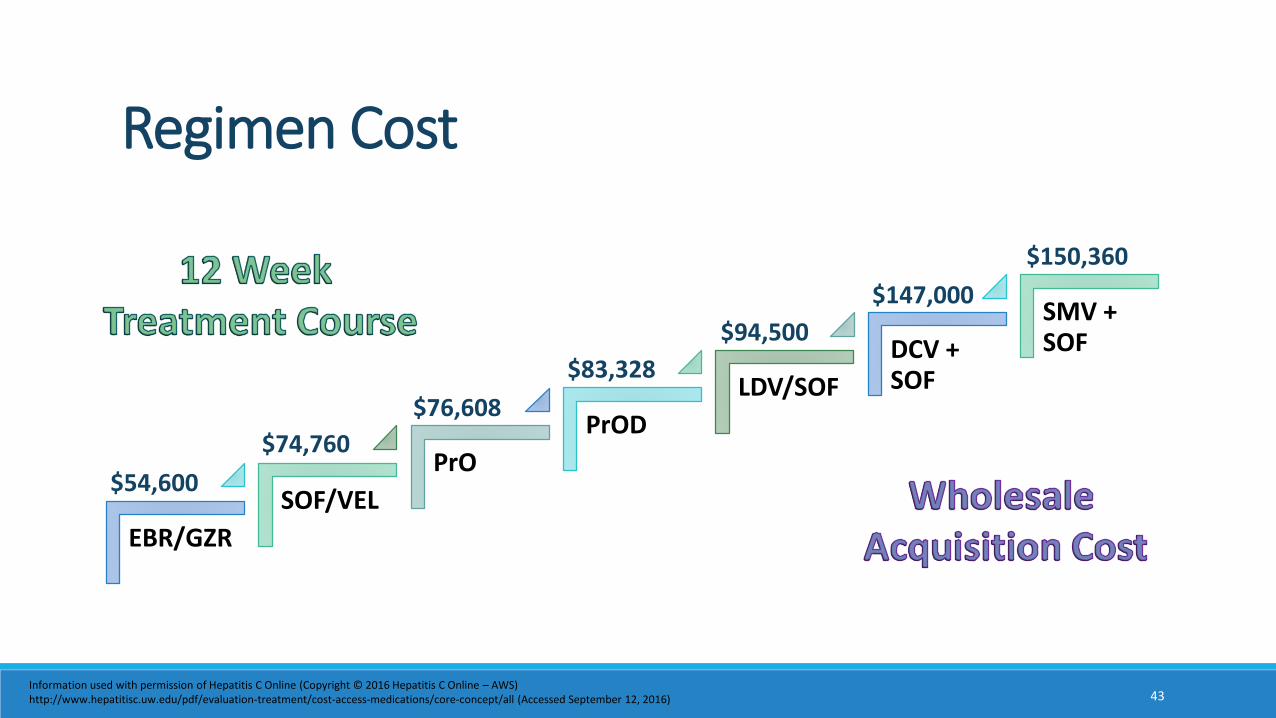
EBR/GZR
SOF/VEL
PrO
PrOD
LDV/SOF
DCV + SOF
SMV + SOF
Regimen Cost
$54,600
$74,760
$76,608
$83,328
$94,500
$147,000
$150,360
43Information used with permission of Hepatitis C Online (Copyright © 2016 Hepatitis C Online – AWS)http://www.hepatitisc.uw.edu/pdf/evaluation-treatment/cost-access-medications/core-concept/all (Accessed September 12, 2016)
Wholesale Acquisition Cost (WAC) treatment range $54,600 to >$300,000
Average national negotiated discount from WAC 2014 = 22% 2015 = 46%
Numerous cost-effective analysis demonstrate Increased quality-adjusted life expectancy (QALY) Cost-effectiveness in early and late-stage HCV disease
44
Financial Considerations
Linas. Top Antivir Med 2016;24(2):93-97AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September 12, 2016.

Formulary Restrictions
Reviewing expected co-pay with patient before treatment
Patient co-pay assistance Manufacturer programs Patient Access Network Foundation Patient Advocate Foundation (Co-Pay Relief)
45
Patient Affordability

Pharmacist Optimizing Care
Treatment evaluation Financial considerations Readiness to start treatment Regimen selection
Patient education Side effects, Drug interactions, Medication
administration
Treatment monitoring Safety, Adherence, Effectiveness
46
Image Source (Accessed September 12, 2016): https://upload.wikimedia.org/wikipedia/commons/thumb/a/a7/PharmacistsMortar.svg/2000px-PharmacistsMortar.svg.png

FUTURE OF HEPATITIS C
47

48
In Pursuit of “Perfectovir”
Pangenotypic Activity
SVR > 95%
1 pill Qday
Affordability
Special Populations
Minimal ToxicityDecompensated
Cirrhosis Short Duration
HCV Resistance
Retreatment Options Drug
Interactions
Treatment Needs MetRoom for Improvement
Dore GJ, et al. Clin Infect Dis 2015; 60(12): 1829-36

Investigational Agents
Drug Class
DosingEstimated
AvailabilityComments
ABT-493 + ABT-530NS3/4A PI +
NS5APO Qday 2017
Pangenotypic Potential for 8 wk treatment course Renal Impairment Retreatment
sofosbuvir + velpatasvir + voxilaprevir (GS-9857)
NS5B +NS5A +
NS3/4A PIPO Qday 2017 / 2018
Pangenotypic Potential for 8 wk treatment course Retreatment
MK-3682 + grazoprevir + (elbasvir OR MK-8408)
NS5B + NS3/4A PI +
NS5APO Qday 2018
Pangenotypic Potential for 8 wk treatment course
49
Investigational Agents – DAA Pipeline
Poordad F, et al. EASL 2016. Abstract GS11Kwo PY, et al. EASL 2016. Abstract LBO1Poordad F, et al. EASL 2016. Abstract SAT-157
Lawitz E, et al. EASL 2016. Abstract PS008 Gane EJ, et al. EASL 2016. Abstract SAT-138Gane EJ, et al. EASL 2016. Abstract 139
HCV is a chronic liver disease with potential long-term health implications
Treatment options are now available for almost every patient, offering much improved cure rates, with better tolerability and ease of use
Multiple treatment options will be available over the coming years that should increase access to cure and reduce treatment cost
Fiscal responsibility through quality optimization
Summary
50
What percentage of patients would be expected to develop cirrhosis after 20 to 30 years of being infected with chronic HCV?a) 5%
b) 25%
c) 50%
d) 75%
Test Question 1
51
Which FDA approved HCV regimen has an 8 week treatment duration as an alternative option available for some patients?a) sofosbuvir / ledipasvir
b) daclatasvir + sofosbuvir
c) elbasvir / grazoprevir
d) sofosbuvir / velpatasvir
Test Question 2
52
Which of the following options would be expected to have reduced efficacy when co-administered with omeprazole 40mg twice daily? a) paritaprevir / ritonavir / ombitasvir+ dasabuvir
b) daclatasvir + sofosbuvir
c) elbasvir / grazoprevir
d) sofosbuvir / velpatasvir
Test Question 3
53

1) Rice CM. Top Antivir Med 2011; 19(3):117-202) Neuman AU, et al. Science 1998; 282(5386):103-73) Schooley RT. Top Antivir Med 2014; 21(5):148-154) Manos MM, et al. J Med Virol 2012; 84(11):1744-505) MMWR 2012;61(No. RR-4)6) Naggie S. Top Antivir Med 2012; 20(5):154-1617) Sherman KE. Top Antivir Med 2011; 19(3):121-1258) Hepatitis C Online – AWS: http://www.hepatitisc.uw.edu/pdf/evaluation-staging-monitoring/natural-history/core-concept/all (Accessed September 12, 2016)9) AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Last Updated July 6, 2016. Date Accessed September
12, 201610) Zignego AL, et al. Intern Emerg Med 2012; 7(Suppl 7):S201-20811) Jacobson IM, et al. Clin Gastroenterol Hepatol 2010; 8:1017-102912) Chhawal J, et al. Hepatology 2016 [Epub ahead of print; Accessed: 9/10/16]13) Ly KN, et al. Clin Infect Dis 2016;62(10):1287-814) Mahajan R, et al. Clin Infect Dis 2014;58(8):1055-6115) Walker DR, et al. J Hepatol 2015;62 (Suppl):S593-59416) van der Meer, et al. JAMA 2012;308(24):2584-259317) McCombs, et al. JAMA Intern Med 2014;174(2):204-21218) Morgan, et al. Ann Intern Med 2013;158(5):329-33719) Figure Adapted from the US Food and Drug Administration, Antiviral Drugs Advisory Committee Meeting, April 27-28, 2011, Silver Spring, MD.20) Majumdar A, et al. Aliment Pharmacol Ther 2016; 43: 1276-1292
References
54
21) Scheel TKH, Rice CM. Nat Med 2013; 19(7):837-84922) Daklinza (daclatasvir) [package insert] 2015. Princeton, NJ, Bristol-Myers Squibb Company. Revised: February 2016.23) Sovaldi (sofosbuvir) [package insert]. 2013. Foster City, CA, Gilead Sciences, Inc. Revised: 6/201524) Harvoni (ledipasvir and sofosbuvir) [package insert] 2014. Foster City, CA, Gilead Sciences, Inc. Revised: 6/201625) Epclusa (sofosobuvir and velpatasvir) [package insert] 2016. Foster City, CA, Gilead Sciences, Inc. Revised: 6/201626) Olysio (Simeprevir) [package insert] 2013. Titusville, NJ, Janssen Therapeutics. Revised: 05/201627) Zepatier (elbasvir and grazoprevir) [package insert] 2016. Whitehouse Station, NJ, Merck Sharp & Dohme Corp. Revised: 1/201628) Technivie (ombitasvir, paritaprevir and ritonavir) [package insert] 2015. North Chicago, IL, AbbVie Inc. Revised: 6/2016 29) Viekira XR (dasabuvir, ombitasvir, paritaprevir, and ritonavir) extended-release [package insert] 2014. North Chicago, IL, AbbVie Inc. Revised: 7/2016 30) Copegus (ribavirin) [package insert] 2002. San Francisco, CA, Hoffman-La Roche, Inc c/o Genentech, Inc. Revised: 8/201531) Hepatitis C Online – AWS: http://www.hepatitisc.uw.edu/pdf/evaluation-treatment/cost-access-medications/core-concept/all (Accessed September 12, 2016)32) Linas. Top Antivir Med 2016;24(2):93-9733) Dore GJ, et al. Clin Infect Dis 2015; 60(12): 1829-3634) Poordad F, et al. EASL 2016. Abstract GS1135) Kwo PY, et al. EASL 2016. Abstract LBO136) Poordad F, et al. EASL 2016. Abstract SAT-15737) Lawitz E, et al. EASL 2016. Abstract PS008 38) Gane EJ, et al. EASL 2016. Abstract SAT-13839) Gane EJ, et al. EASL 2016. Abstract 139
References (continued)
55

1. Write down the course code. Space has been provided in the daily program-at-a-glance sections of your program book.
2. To claim credit: Go to www.cshp.org/cpe before December 1, 2016.
Session Code: