hemodynamics of constrictive pericarditis. restrictive physiology restrictive physiology is...
TRANSCRIPT

Hemodynamics of constrictive pericarditis

Restrictive physiology
• Restrictive physiology is characterised by impediment to ventricular filling caused by – Increased ventricular stiffness-RCM– Increased pericardial restraint-CCP
• Constrictive pericarditis and restrictive cardiomyopathy share clinical features and hemodynamic findings

• Preserved systolic function.• Grade III diastolic dysfunction.• Elevation and equalization of diastolic pressures• Dip and plateau pattern in Ventricular pressure
tracing

Pericardium

• Pericardium-2 layers– Visceral-monolayer of mesothelial cells ,collagen
&elastin fibres– Parietal layer-collagen and elastin fibres– Visceral layer reflects back over origins of great
vessels– LA largely extrapericardial
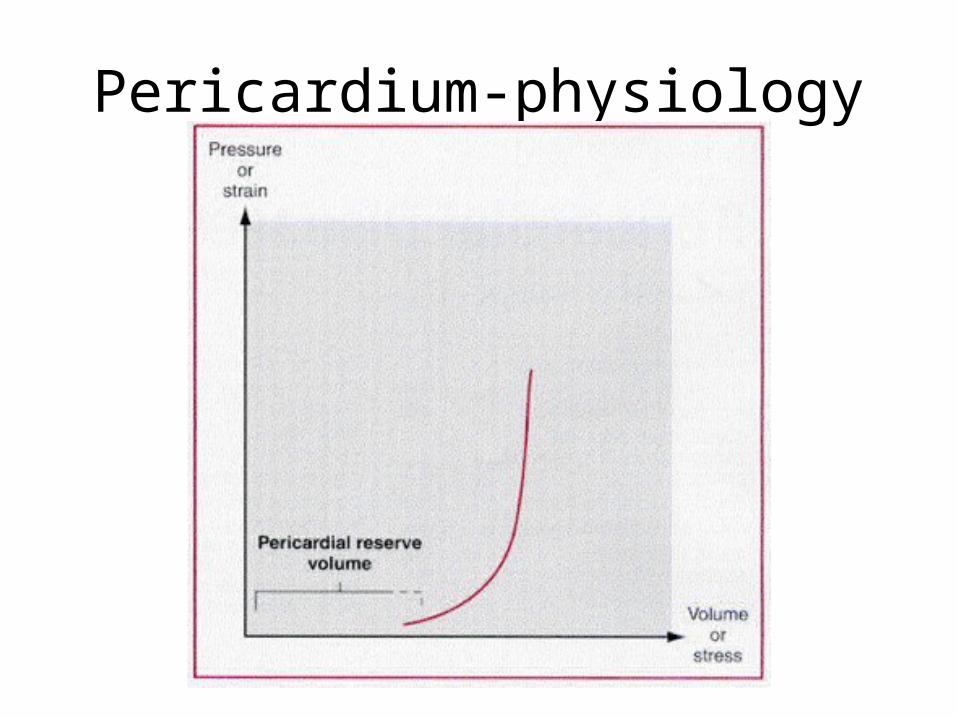
Pericardium-physiology

• Pericardium can restrain cardiac volume– Contact pressure exerted on the heart can limit
filling when upper limit of normal cardiac volume exceeded
• Contribute to diastolic interaction b/w cardiac chambers


Constrictive pericarditis
• Scarring of both visceral and parietal layers constraining cardiac chambers
• Causes– Tuberculosis– Ideopathic or viral pericarditis– Mediastinal irradiation– Open heart surgery– CRF – Connective tissue disorders

CCP-pathophysiology
• Marked restriction of filling• Ventricular interdependence• Failure of transmission of intrathoracic
pressures to intracardiac chambers

Restriction to cardiac filling
• Physiologic effect produced by constricting pericardium
• Gradual devt of systemic and pulmonary venous hypertension– Atrial pressures 10-18 mmHg-systemic venous congestion – 18 to 30 mmHg-effort dyspnea,orthopnea
• Fall in stroke volume– Increased HR,systemic vascular resistance– Inability to augment cardiac output during exercise-fatigue– Resting C.O.P falls-cachexia

Ventricular interdependence
• Filling of one ventricle limits the simultaneous filling of other ventricle owing to the shared mechanical constraint
• Coupled constraint-tamponade-greater ventricular interdependence
• Uncoupled constraint-modest interdependence-predominant effect on the thin walled RV

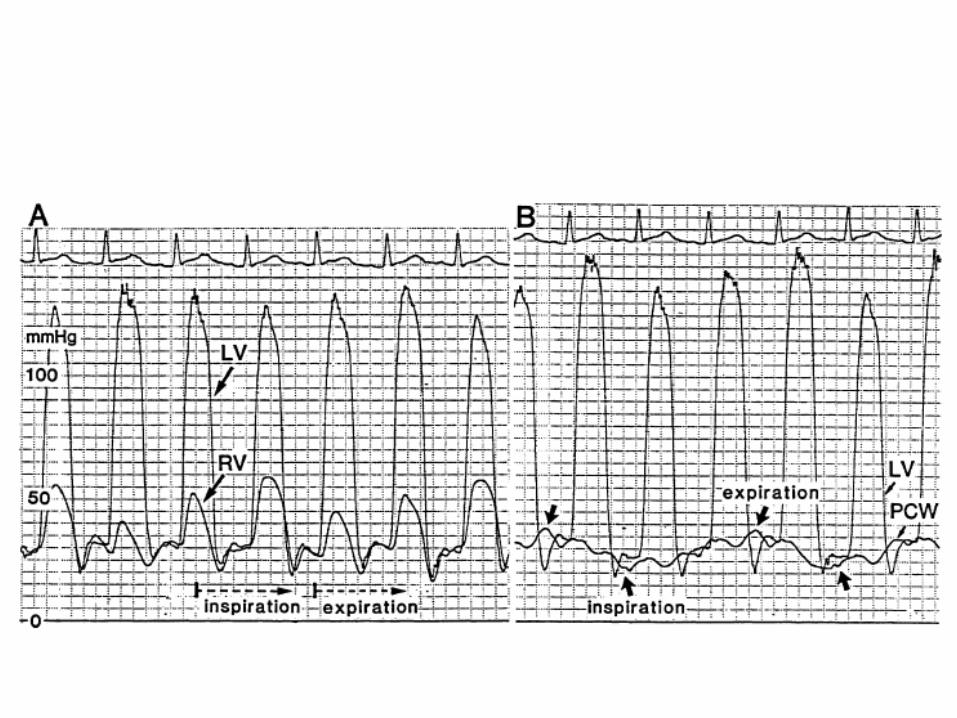
Loss of transmission of intrathoracic pressures
• Normal– Inspiratory decrease in ITP transmitted to all
cardiac chambers– Decrease in pressure in pulmonary veins and LV– Decrease in PCWP accompanied by corresponding
decrement in LV pressures– Gradient that drives LV filling maintained

Normal

• CCP– Pulmonary veins ,LA-extrapericardial – Inspiratory decrease in ITP transmitted to the
pulmonary vein and LA but not to LV– Decrease in PCWP not accompanied by
corresponding decrease in LV pressures– Less gradient that drives LV filling-inspiratory
decrease in LV filling– Allows increased RV filling and IVS shift to left– Opposite occurs in expiration

.
Hurrell D G et al. Circulation 1996;93:2007-2013
Copyright © American Heart Association

CCP

RA pressures

• Restricted filling-elevation of mean pressure• Early diastole-rapid filling-prom. Y descent
– Elevated RAP– Suction effect due to decreased ESV– Friedreich sign
• Abrupt cessation of ventricular filling-nadir of Y descent• kussmaul s sign
– Inspiratory increase in venous return-decr.ITP– Failure of transmission of decr.ITP to RV– Ventricular interdependence is modest


Ventricular pressure tracing

• Early diastole– Filling of ventricles unimpeded– Rapid-high RAP,decreased ESV– Ventricular RFW >7 mmHg
• Abrupt halt to ventricular filling once the limit set by the pericardium – Dip and plateau pattern
• Equalisation of LV &RV pressures –ventricular interdependence

• RVEDP>1/3 RVSP• Discordance b/w RVSP and LVSP during phases
of respiration



FEATURE SENSITIVITY% SPECIFICITY%
LVEDP – RVEDP < 5mm Hg 60 38RVEDP / RVSP > 1/3 93 38PA SP < 55 mm Hg 93 24LV RFW > 7 mm Hg 93 57RESPIRATORY ~ RAP < 3mm Hg 93 48
RESPIRATORY ~ PAWP – LV PG > 5mm Hg 93 81 LV – RV INTERDEPENDENCE 100 95
D G HURRELL CIRCULATION 1996

.
Hurrell D G et al. Circulation 1996;93:2007-2013
Copyright © American Heart Association


• Systolic area index– RV area/LV area in inspiration÷RV area /LV area in
expiration– >1.1 s/o CCP

FEATURE SENSITIVITY% SPECIFICITY%
LVEDP – RVEDP < 5mm Hg 46 54RVEDP / RVSP > 1/3 93 46PA SP < 55 mm Hg 90 29LV RFW > 7 mm Hg 45 44RESPIRATORY ~ RAP < 5mm Hg 71 37
SYSTOLIC AREA INDEX >1.1 97 100
D R Talreja JACC 2008;51:315

Echo-M mode
• Septum-– Rapid movements in early diastole and atrial
contraction• Postr wall
– Abrupt postr motion in early diastole and flat in diastole
• Sharp EF slope in MV M-mode


Echo Doppler
• Mitral peak E velocity>25 % increase in exp.• Tricuspid peak E velocity >25 % increase in
insp.• DT<160 ms,IVRT<60 ms• E/A ratio >2
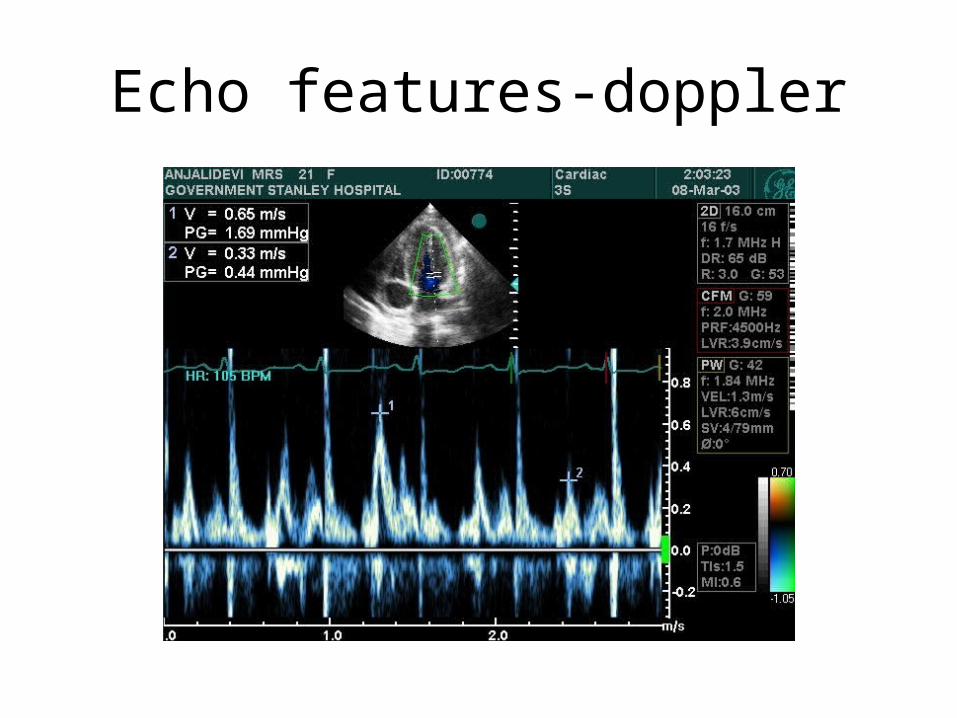
Echo features-doppler


PV doppler
• S <D• Prominent atrial reversal• Incresed velocities in expiration

Mitral and PV flow in CCP(TEE)

Hepatic vein Doppler
• S<D in inspiration,S>D in expiration• Diastolic flow reversal in expiration

HV diastolic flow reversal in expiration

TDI
• Mitral annular E’>8 cm/s• E/E’ <15



Variant forms
• Effusive constrictive– Failure of RAP to decline by at least 50% to a level
below 10 mm Hg when pericardial pressure decreased to 0 by pericardiocentesis
• Occult constriction– Features of constriction unmasked by volume
expansion• Localised constriction• Transient constriction