hematopoietic stem cell transplant for … cell disease: ... § in africa, newborn children born...
TRANSCRIPT

2/11/16
1
KarenSweiss, PharmD,BCOPClinical Assistant Professor
Clinical Pharmacist inHematologyandStemCell TransplantDepartmentofPharmacyPractice
Universityof I llinois College ofPharmacyChicago, IL
HEMATOPOIETICSTEMCELLTRANSPLANTFORSICKLECELLDISEASE:PERSPECTIVESFROM
CHILDHOODTOADULTHOOD
Disclosures• Ihave noactual orpotential conflict of interestin
relation tothis program/presentation.
Objectives• Definethepathogenesisandclinicalsequelaeofsickle
cell disease (SCD) inpediatric and adult patients
• Identify theindicationsforallogeneic hematopoieticstem cell transplantation in pediatricand adultpatientswithSCD
• Explaintheimmunologyunderlyingtheuseof allogeneic hematopoietic stem cell transplantation in SCD
• Compare theefficacyandtoxicityofthevarious preparative regimensusedinpediatricandadultpatientswithSCD

2/11/16
2
SickleCellDisease:AGlobalBurden• Incidence1
§ Affects 90,000to100,000Americans§ Occursamong~1outofevery 500BlackorAfrican-American births
§ InAfrica,newborn childrenbornwithSCDestimated tobe200,000to300,000
• Mortality2§ Killsnearlyhalfamillionpeopleannually
• EconomicCosts2
§ ForadultswithSCDthe average annualcostofmedicalcareexceeds 35,000USdollarsperyear
1h ttp ://www.cd c.go v/n cbddd /sicklecel l /d ata.h tml .Accessed November1 0 ,2 0 1 52Bo lano s-Meade Jetal . B lood Reviews.2 0 1 4;2 8:2 43 -8
SCD:Pathophysiology
h ttp ://sgugenetics.pbwo rks.com/w/page/6 1 1 7 2 3 0 4 /P athophysio lo gy%2 0 of%2 0 Sickle%2 0 Cel l%2 0AnemiaAccessed November 1 2 ,2 0 1 5
SCD:ClinicalSequelae
Rees DC etal . Lan cet.2 0 1 0 ;3 76 (9 75 7):2 01 8-3 1.

2/11/16
3
SCDMortalityRiskFactorsRisk Factor MSH
n=299CSSCDn=3764
CSSCDn=1056
Episode ofAcute ChestSyndrome (ACS) X X X
≥ 3pain crisis annually X
Hgb F <0.5 g/dL X X
Anemia withlow reticulocyte counts X
Renal Failure X X
Seizure History X
Elevated WBC X
Stroke X
Sickle cell lung disease and retinopathy X
Leg Ulcers XMSH:Mu ltice n te rStudyo fHyd roxyu re a in Sickle Ce ll Anemia,C SSCD:Coope rative StudyofSickle Ce ll Dise ase Hbg F:Fe tal Hemoglob in ,WBC :Wh ite Blood Ce ll
Steinberg MHetal . JAMA. 2 00 3;2 89 (13 ):16 45 -51 .P lattOSetal . NEn gl JMed .1 9 9 4;3 30 (23 ):1 6 39 -44 .P owarsDR etal . Med icin e (Bal timo re).2 0 05 ;84 (6):36 3 -7 6.
SCDManagement
Supportive
ErythropoietinStimulating Agents
Bloodtransfusion
IronChelation
Symptomatic
Analgesics
Bloodtransfusions
Antibiotics
Prevention
Penicillin/Vaccinations
Bloodtransfusions
Hydroxyurea
Rees DC etal . Lan cet.2 0 1 0 ;3 76 (9 75 7):2 01 8-3 1.
TreatmentofAdultSCD
Treatmentchallenges:§ Lack of compliance tolong-term medications§ Overuse and dependence of narcotics§ Loss of productivity§ Psychological symptoms inadulthood
Chakrabarti Setal . B io l B lood MarrowTran sp lan t. 20 04 ;1 0(1 ):23 -31 .
Clinical courseworsens inadulthood
TreatmentChallenges
Mortality sharplyincreases everydecade over 20
years old

2/11/16
4
Whatareothertreatmentoptionstoimprove
mortality forAdultSCDpatients?
Hematopoietic CellTransplant
(HCT)
SCDandTransplant:Ahistoricalperspective
As of 2013,there were 1238BMTs forSCT reported toCIBMTR andEBMT-Eurocord
Appelb aum FR . NEn gl JMed ;3 57 :1 4 72 -75C IBMTR:Cen ter fo r In tern ational B lood and MarrowTran sp lan tRegistryEBMT:Eu ropean B lood and MarrowTran sp lan t
SCDandHCTEBMT-Eurocord(1986– 2013)
CIBMTR(1986– 2012)
Transplantations forSCD
Total 611 627
TypeofDonor
HLA-identical 487 430
CordBlood relatedandunrelated
73 71
Haploidentical donor 34 61
Otherunrelateddonor 17 65
Overall Survival
1year 95%± 1% 96%± 2%
2year 94%± 1% 94%± 1%
Gluckman E.ASHedu cation book2 0 13 ;37 0 -3 7 6

2/11/16
5
BenefitversusriskinHCTforSCD• Prolonged lifespan• No clinical vaso-occlusive events• Improved quality of life• Cessation of anemia and RBCtransfusions
• Fewer hospitalizations
Benefits
• GVHD• Infertility• Delayed immunereconstitution/infection
• Treatment-related malignancy• Death
Risks
Shenoy S.Hemato lo gyAmSo c Hemato l Edu c P rogram.2 0 1 1 ;2 73-9
ChallengesinSCDpatients• Patient selection and timingof transplant
§ Stilladebate astowhoandwhentransplant shouldoccur
• Limited patient eligibility§ Disease andage-related comorbiditiesresultinhighermorbidityandmortality inolderpatients
• HCT not available tomost patients§ Socioeconomicsetting§ Absence ofmatchedrelated donor
• Serious concerns about transplant-related mortality§ GVHD, infertility, treatment-induced malignancy
Shenoy S.Hemato lo gyAmSo c Hemato l Edu c P rogram.2 0 1 1 ;2 73-9
ChallengesinSCDpatients
• Donoravailability§ 25% probability of being HLA-matched to sibling§ 19% chance of finding potential alleleic 8/8MUD
• Patientperception§ 62%werewillingto accept >10% TRM§ 30%willingtoaccept 30% TRM§ 50%werewillingto accept infertility§ 20%willingtoaccept chronic GVHD
Chakrabarti S.BoneMarrowTran sp lan t2 0 0 7 ;39 :44 7-4 51
TRM : tran sp lan t-related mo rtal i ty

2/11/16
6
HCTOptionsforSCD• Majorityof transplantsperformed• PreferredduetolowGVHD/graftfailure• Siblingswithsicklecell traitaresuitabledonors
Matchedsiblingdonor
• RelatedorunrelatedUCBtransplantshavebeenperformed• SlowerneutrophilrecoveryandlessGVHDUmbilical cord
• LimiteddataevaluatingMUD forSCD• SCURT(Sickle cell unrelateddonortransplant) study
Matchedunrelateddonor
• Post-transplantcyclophosphamide• Lowratesof GVHDandgraftfailure
HLA-haploidentical
Shenoy S.Hemato lo gyAmSo c Hemato l Edu c P rogram.2 0 1 1 ;2 73-9
FirstSCDtransplant
• First successfulHCTinan8yeargirlwithSCD1
§ Matched-siblingdonor(MSD) withsicklecelltrait§ Myeloablative conditioningregimen:CY120mg/kgover2daysandTBI11.5Gy
§ GVHD prophylaxis:MTXandmethylprednisolone§ Patient curedofbothAMLandSCD§ Proof-of-principleforfuture platforms tostudyHCTinSCD
• Walters etal2 studyof22patients§ MSD usingBu/CY/ATG§ EFS andOSat4years 91%and73%,respectively§ Graft failure19%
1John son FL.NEn gl JMed 19 8 4;31 1 :7 8 02WaltersMC etal . NEn gl JMed 1 9 9 6;33 5 (6):36 9 -7 6
IndicationsforHCTinPediatricSCD
Age<16yearsold
HLA-identical sibling
• Stroke• ACSw/recurrenthospitalizationsorpreviousexchangetransfusions• Recurrentvaso-occlusivepainorrecurrentpriapism• AbnormalMRIorimpairedneurophysiologicalfunction• Stage IorIIsickle lungdisease• Sickle nephropathy(moderatetosevereproteinuria,GFR30-50%predictedvalue)
• Bilateralproliferativeretinopathy• Osteonecrosisof multiplejoints• Redcell alloimmunizationduringlong-termtransfusiontherapy
SymptomaticSCD(1ormorebelow)
WaltersMC etal . NEn gl JMed .1 99 6 ;3 35 (6 ):3 69 -76 .

2/11/16
7
IndicationsforHCTinAdultSCD
Age≥16yearsold
HLA-identical sibling
• Irreversible end-organdamage• Stroke orclinically signif icant CNS event• Elevated TRV ≥2.6m/s• Sickle-related renal insuff iciency(Cr≥1.5times theULN orbiopsyproven)• Sickle hepatopathy( includingironoverload)• Reversible sickle complicationnotameliorated byhydroxyurea• TwoormoreVOCrequiring hospitalizationsforseveral years• AnyACSwhile onhydroxyurea
SymptomaticSCD(1ormorebelow)
Hsieh MM etal . B lood.20 11 ;11 8(5 ):11 97 -12 07.
HCTinpediatricSCD• Publishedresultsareexcellent
§ Fourlargeseriesreportoutcomesofmorethan250children
§ Medianagelessthan10years• Patients
§ DonorswereHLA-identicalsiblings§ High-riskpatientpopulation§ Receivedfullymyeloablativeconditioningregimens
• Outcomes§ Graftrejection7-18%§ OS93-100%§ HCTeliminatesvaso-occlusivesymptomsandreversessomeof theendorgandamage
Watlers MC etal . B io l B loodMarrowTran sp lan t20 15 ;pi i :S1 0 83 -8 79 1
MSDwithMACregimeninPediatricSCDVermylen etal1(n=50)
Walters etal2(n=50)
Bernaudin etal3 (n=185)
Panepinto etal4(n=67)
Dedeken et al5(n=50)
Lucarelli etal6(n=40)
Conditioningregimen Bu/CY± TLI Bu/CYATG oralemtuzumab
Bu/CY± ATG Bu/CY Bu/Cy± ATG Bu/Cy/ATG
GVHDprophylaxis CSA,ATG CSA,MTX CSA± MTX CSA,MTX CSA/MTXCSA/MMF formatchedUBT
CSA, MTX,methylprednisolone
Medianfollow-up(mo) 60 38 72 61 7.7years 5years
EFS 82% 84% 91% 85% 85.6% DFS91%
OS 96% 94% 96% 96% 94.1% 91%
GraftRejection 10% 10% 7% 13% 8% 0%
TRM 7% 6% 6.9% 0% 4% 9%
aGVHD≥II 20% 15% 20% 10% 10%(grade¾) 17.5%(grade¾)
cGVHD 20% 12% 14% 22% 20% 5%
1Vermylen etal , BoneMarrowTran sp lan t.1 9 9 8 ;22 (1):1 -62WaltersWC etal . B lood .20 0 0;9 5(6 ):1 91 8 -2 43Bernaud in etal , B lood 2 00 7 ;1 10 :27 4 9-5 64P anep in to etal , B r JHaemato l 2 0 0 7;1 37 :47 9-8 55Dedeken etal , B r JHaemato lo gy 2 0 1 4 ;1 6 5 (3):40 2 -6Lu carel l i etal , BoneMarrowTran sp lan t2 0 1 4 ;49 :1 3 76 -81
MSD:matched sib l in gdono rMAC :myelo ab lativecond ition in g
2/11/16
8
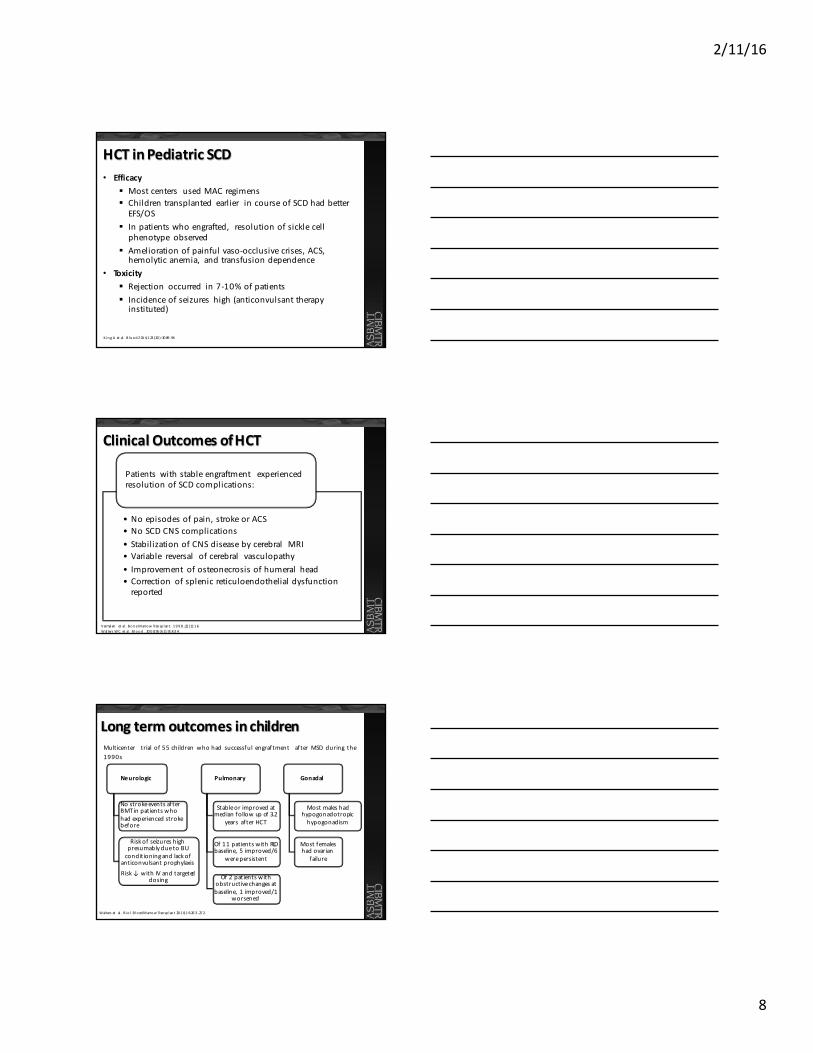
HCTinPediatricSCD• Efficacy
§ Mostcenters usedMACregimens§ Childrentransplanted earlier incourseofSCDhadbetterEFS/OS
§ Inpatientswhoengrafted, resolutionofsicklecellphenotype observed
§ Ameliorationofpainfulvaso-occlusivecrises,ACS,hemolyticanemia, andtransfusiondependence
• Toxicity§ Rejection occurred in7-10%ofpatients§ Incidenceofseizures high(anticonvulsanttherapyinstituted)
K ingAetal . B lood2 01 4;1 23 (20 ):30 89 -94
ClinicalOutcomesofHCT
• Noepisodesofpain,strokeorACS• NoSCDCNScomplications• StabilizationofCNSdiseasebycerebral MRI• Variable reversal ofcerebral vasculopathy• Improvement ofosteonecrosisofhumeral head• Correction ofsplenicreticuloendothelialdysfunctionreported
Patients withstableengraftment experiencedresolutionofSCDcomplications:
Vermylen etal . BoneMarrowTran sp lan t.1 9 9 8 ;22 (1):1 -6WaltersWC etal . B lood .20 0 0;95 (6 ):1 91 8 -2 4 .
Longtermoutcomesinchildren
Neurologic
NostrokeeventsafterBMTinpatientswhohadexperiencedstrokebefore
Riskof seizureshighpresumablyduetoBUconditioningandlackof
anticonvulsantprophylaxisRisk↓withIVandtargeted
dosing
Pulmonary
Stableorimprovedatmedianfollowupof 3.2
years afterHCT
Of11patientswithRLDbaseline, 5improved/6
werepersistent
Of2patientswithobstructivechangesatbaseline, 1improved/1
worsened
Gonadal
Mostmaleshadhypogonadotropichypogonadism
Mostfemaleshadovarian
failure
Multicenter trial of 55children whohad successful engraftment afterMSD during the1990s
Walterset al . B io l B lood MarrowTran sp lan t20 1 0;1 6:26 3 -27 2

2/11/16
9
Nonmyeloablative (NMA)RegimensinChildren• Effort toreduce transplant-related toxicity• Iannone etal
§ n=7,medianage 9years§ Fludarabine andTBI200cGy§ 2patientsreceived horse ATG§ GVH prophylaxis:MMF+tacrolimusorCSA
• Results§ ANC<0.5x109 formedian5daysand<0.2x109 for0days§ 1patientgrade IIaGVHD, 6/7patientshaddonorchimerism
§ All6patientshadgraft failure,autologoushematopoieticrecovery, anddiseaserecurrence whenimmunosuppressiontaperedoff
Iannone R etal . B io lB lood MarrowTran sp lan t.20 03 ;9:5 19 -52 8
NMARegimensinChildren
• Increaseingraftfailure attributed topatients beingsensitized tominorhistocompatibility antigens frompriorblood transfusions and tobeingimmunocompetent
• DonorTcellengraftmentwasnotsufficient toestablish stable donorchimerism
• Note:ATGwasnotgiven toall patientsand ISwastaperedoffanytimeb/w~30 to200days
Iannone R etal . B io lB lood MarrowTran sp lan t.20 03 ;9:5 19 -52 8
AlloHCT inAdultSCD
• Fewadultswereinpediatrictrials§ ↓ Survival,↑ acute GVHD
• Contributing Factors:§ End-organ damage§ Transfusions =↑ Risk of graftrejection§ Increased age=↑ Riskfor GVHD
• MACregimensaretootoxicforadultSCDpatients
Vermylen etal , BoneMarrowTran sp lan t.1 9 9 8 ;22 (1):1 -6 .Bernaud in Fetal , B lood .2 00 7;1 10 (7):2 74 9-5 6.

2/11/16
10
Selectionofconditioningregimen
Days Days Days
Patient Graft Patient Graft Patient Graft
Myeloablative Reduced-Intensity Nonmyeloablative
WBC
(x1
09/L)
WBC
(x1
09/L)
0 .5 0.5 0.5
Gyu rko cza B etal . B lood 20 14 ;12 4(3 ):34 4-5 3.
MACexperienceinyoungadultSCD• Kuentz et alreport French experience in15patientsolder
than16years ofage whoreceived MSD, medianfollow-up3.4years
• Bu/CY/ATG andGVHprophylaxiswithMTX/CSA
Outcome n=15Complications Cerebralhemorrhage(n=1)
Seizures(n=1)Pericarditis(n=1)Hemorrhagiccystitis(n=1)Subduralhematoma(n=1)Prolongedthrombocytopenia(n=1)
≥ gradeIIaGVHD n=8ModeratecGVHD n=2DFS 93%Chimerismat1year Fulldonor(n=12)
Mixeddonor(n=2)
Kuen tz etal , B lood 2 01 1;1 18 :44 91 -44 92
MACinAdultSCD
• “STRIDE” study: n=17(MSD) andn=5(MUD), medianage 22years• Nograft failure orSCDrecurrence• 1deathduetointracranial hemorrhage (PRES)• 21/22patientswithstableengraftment (median 9.7months)• OSandEFS 95%;2patientswithgradeIaGVHD; 3patientscGVHD
DAY - 8 - 7 - 6 - 5 - 4 - 3
Fludarabine 30mg/m2/dayBusulfan (Bu)13.2mg/kg (total)
Tacrolimus orCyclosporineMethotrexate
K rishnamu rti L, etal . American So cietyo fHemato lo gy (ASH)2 0 1 5 ;Ab str 54 3.
- 2 - 1 0
Bu Bu Bu Bu
Flu FluFlu
Flu Flu
Thymoglobulin 6mg/kg
ATGATG ATG ATG

2/11/16
11
Reduced-IntensityConditioning(RIC)inAdultSCD
• 2adultpatientswithend-stage SCDwithHLA-identical siblings• Bothpatients engrafted; however, duetoGVHD complications
diedwithin1year
DAY -5 -4 -3 -2 -1 0
ATG 30mg/kg/dayFludarabine 30mg/m2/day
Melphalan140mg/m2
Stem CellInfusion
TacrolimusMethotrexate onDay 1,3, 6
van Besien etal . BoneMarrowTran sp lan t.2 0 0 0 ;2 6(4 ):4 45 -9 .
FLU FLU FLU FLUMELATG ATG ATG ATG
RICandMUDinAdultSCD
• SCURT trial: n=29; median age 14years; median f/u25.2months• Graft rejection before D+100(n=3, 10%)• 1-year EFS 76%; 1-year OS 86%• Grade II- IV and III- IV aGVHD atD+180 31%and 17%respectively• cGVHD at 1-year was 62%(extensive 38%)• 7deaths (6fromGVHD, 1fromgraft rejection after 2nd transplant)• PRES in 35%of patients; CMV and EBV in23%of patients
DAY - 8 - 7 - 6 - 5 - 4 - 3
Fludarabine 150mg/m2
Melphalan140mg/m2
TacrolimusorCyclosporineMethotrexate7.5mg/m2 D+1,3,6
Methylprednisolone1mg/kg/dD+7toD+28
Shenoy S,etal . American So ciety o fHemato lo gy (ASH)2 0 1 5 ;ab str 7 21 .
- 2 - 1 0
Flu Flu Flu Flu Flu Mel
Alemtuzumab(day-22to-19)
+1 to+28
NMAconditioning
KeyPrinciples
• Stablemixeddonorandrecipientchimerism
• ClassictransplantationregimensusedforhematologicmalignanciestootoxicforSCDadultpatientswhohaveaccumulatedorganfailuresandcomorbiditiesbeforetransplant
• LessTRMandlowratesofacuteandchronicGVHDandgraftfailure

2/11/16
12
MixedDonorChimerism
Kean LS,etal . B lood 2 0 03 ;10 2 :4 58 2 -4 5 93
Mixeddonorchimerism
• Use less intense preparative regimens§ Reduced-intensity (RIC)ornonmyeloablative (NMA)§ Completeeradication ofrecipientbonemarrow andGVLnotnecessary
• Red cell compartment replaced with donor red cells§ Donorerythrocytes (HbAA) have survival andmaturationadvantage over recipient erythrocytes (HBSS)
§ Resultsinmajorityofdonor-derived erythropoiesis§ ResolutionofsymptomaticSCDovertime
Bo lano s-Meade,etal . B lood Rev2 0 1 4;28 (6 ):2 43 -8
Alemtuzumabmechanismofaction
• Originally developed for prevention of GVHD andgraftrejection
• Recombinant humanized monoclonal antibody whichbinds toCD52 on the cell surface and triggerscelllysis§ CD8, CD4, NKcells, monocytes- depleted up to 1year
§ B-cells transiently depleted§ Used inconditioning regimens for invivoT celldepletion (replaces ATG)
Haleet al . BoneMarrowTran sp lan t.2 0 02 ;3 0(1 2):7 97 -80 4.Jaglowski et al . B lood .20 10 ;11 6(1 9):3 70 5-1 4.

2/11/16
13
Pharmacyconsiderations:Alemtuzumab
• Test dose: 0.03mg/kg IV onD-7; 0.1mg/kg IVD-6; 0.3mg/kg IVD-5 toD-3• Infuse IVPB over 2hours
DOSINGANDADMINISTRATION
• APAP650-1000mgPO, diphenhydramine 50mg PO, hydrocortisone 100mg IVPoncall, epinephrine 0.4 mg SC oncall, meperidine 25-50mgIVP oncall
PRE-MEDICATIONS
• Bloodpressure, heart rate, temperature ( infusionreaction)• CMV PCRforCMV reactivation
MONITORING
• Infusion reactions (fever, chills, hypotension, rigors, etc)• Infection(CMV, HSV,PJP)
ADVERSEREACTIONS
Campath ® P rescrib in g in fo rmation
Sirolimus• Discovered in1975inEasterIsland(RapaNuitonative
islanders)hence itsoriginalname
• Chemicalstructure: carbocycliclactone-lactam macrolideantibiotic
• Pharmacokinetics§ Highlylipophilicdrug,highlyboundtoredbloodcells§ Poorbioavailability(~15%)§ Extensive hepaticmetabolism(CYP3A4)§ Substrate forp-glycoprotein§ Longhalflife(~57-62hours)henceoncedailydosing
IngleGR ,etal . Ann P harmaco ther 2 0 0 0 ;34 (9):1 04 4-5 5
Pharmacyconsiderations:Sirolimus
• Loading: 5mg PO every 4hoursx3doses; Maintenance: 5mg PO daily
DOSINGANDADMINISTRATION
• Target trough8-12ng/dL
THERAPEUTICDRUGMONITORING
• CYP3A4inhibitors ( i.e., voriconazole, diltiazem) and inducers ( i.e, phenytoin,rifampin)
DRUG INTERACTIONS
• Cytopenia• Myalgias/arthralgias• Delayedwound healing• Interstitial pneumonitis• Stomatitis/aphthous-like oralulcers• Hypercholesterolemia/hypertriglyceridemia
ADVERSEREACTIONS
• Proteinuria• Peripheral edema• Hypertension• Acneiformrash
IngleGR ,etal . Ann P harmaco ther 2 0 0 0 ;34 (9):1 04 4-5 5

2/11/16
14
Sirolimusmechanismofaction(MOA)• MacrolideantibioticwhichformsacomplexwithFKBP-12thatbinds
toinhibitmammaliantargetofrapamycin (mTOR)• HaltsT-cellproliferationbyinhibitingprogressionfromG1 toSphase
IngleGR ,etal . Ann P harmaco ther 2 0 0 0 ;34 (9):1 04 4-5 5
Sirolimusandmixedchimerism• MixedchimerismMOA
§ SirolimusdoesnotblockT-cellactivation(signal1)butbindstomTOR blockingproliferation(signal2)1
§ Signal1inabsenceofsignal2rendersTcellanergy andpromotesT celltolerance
• Murinemousetransplantationmodels2§ Compared 30daycourseofCSAtosirolimus§ Long-term highlevelchimerismwasattained onlyinsirolimus-treated mice
§ Mixedlymphocyte reactions demonstrated tolerance todonorcells
1Powel l JDetal . J Immuno l 1 9 9 9;1 62 (5):22 7 5-2 78 42P owel l JDetal . Tran sp lan tation 2 0 05 ;80 (11 ):15 41 -15 45
Sirolimusstomatitis• ClinicalPresentation
§ Solitary ormultiplelesionswithrapidonsetafter initiation§ Ovoidshapew/centralgray area surrounded byerythematous halo
§ Canbepainfulanddebilitating
• Villa etalreportedcaseseries§ Mediantime toonset55daysafter allogeneic SCT§ 92.9%ulcersonnon-keratinizedmucosa(mostlyventrolateral tongue)
§ 13patientsreceived topicalsteroids§ Clinicalimprovementinallpatients§ Mediantime toresolutionwas14days
1Vi l la Aetal . B io lB loodMarrowTran sp lan t.2 01 5;2 1(3 ):50 3-8
2/11/16
15
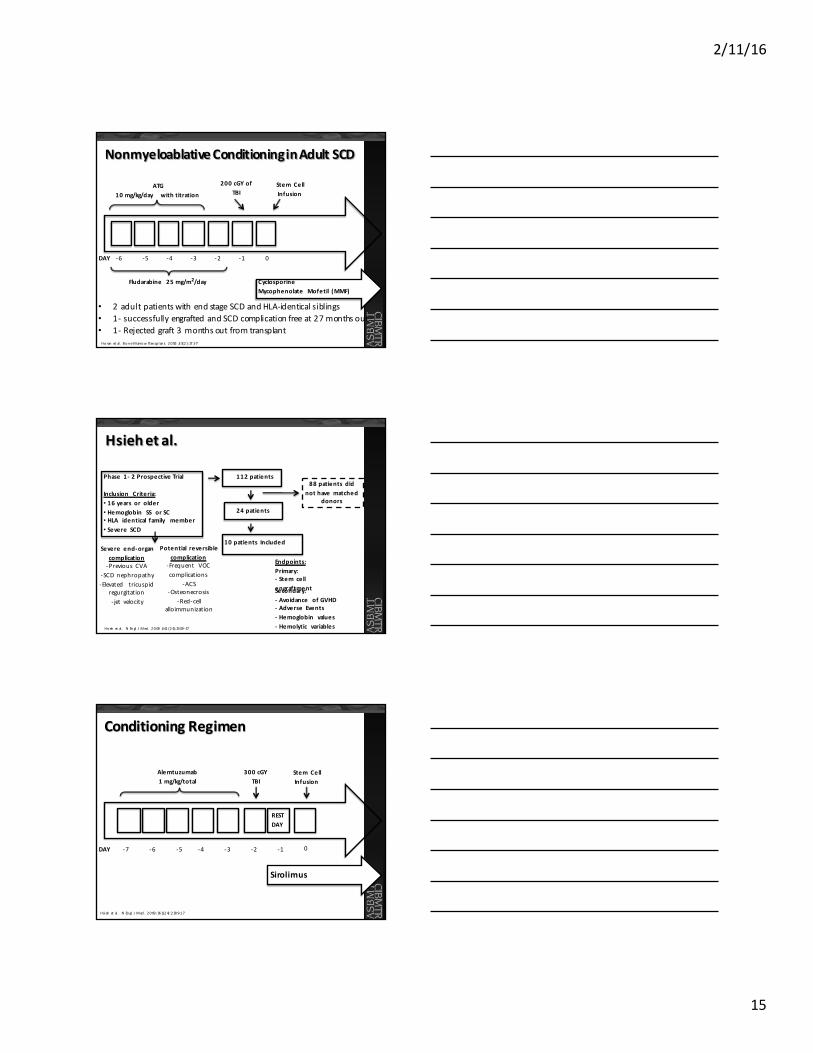
NonmyeloablativeConditioninginAdultSCD
• 2adultpatientswithendstageSCDandHLA-identicalsiblings• 1- successfullyengraftedandSCDcomplicationfreeat27monthsout• 1- Rejectedgraft3monthsoutfromtransplant
DAY -5 -4 -3 -2 -1 0
ATG10mg/kg/day withtitration
200cGYofTBI
Stem CellInfusion
CyclosporineMycophenolate Mofetil (MMF)
Ho ran etal . BoneMarrowTran sp lan t.2 0 05 ;3 5(2 ):17 1-7
Fludarabine 25mg/m2/day
-6
Hsiehetal.
Phase 1- 2ProspectiveTrial
Inclusion Criteria:• 16years or older• Hemoglobin SS orSC• HLA identical family member• Severe SCD
Hsieh etal . NEn gl JMed .2 0 09 ;3 61 (2 4):23 09 -17
Severe end-organcomplication-Previous CVA
-SCD nephropathy-Elevated tricuspid
regurgitation- jet velocity
Potential reversiblecomplication
-Frequent VOCcomplications
-ACS-Osteonecrosis
-Red-cellalloimmunization
Endpoints:Primary:- Stem cellengraftmentSecondary:- Avoidance ofGVHD- Adverse Events- Hemoglobin values- Hemolytic variables
88patients didnothavematched
donors
112patients
24patients
10patients Included
ConditioningRegimen
DAY -7 -6 -5 -4 -3 -2 -1 0
Alemtuzumab1mg/kg/total
300cGYTBI
Stem CellInfusion
Sirolimus
RESTDAY
Hsieh etal . NEn gl JMed .2 0 09 ;36 1(2 4):2 30 9-1 7

2/11/16
16
GraftOutcomes
• All10patientsalive,1graftrejection• Meanpercentageofdonormyeloidcellswas83.3%
Pt #Time sinceASCT
(months)Duration ofNeutropenia
(days)Duration ofLeucopenia
(months)Hgb(g/dl)
1 54 21 3.5 12
2 36 18 2.5 11.1
3 42 12 6 14.8
4 33 29 6 11.4
5 30 10 4 14.3
6 32 10 6 14.7
7 29 19 8 12.2
8 30 11 1.5 12.1
9 16 15 3.5 11.7
10 15 18 4 10.5
Median 30 15.5 4 12.65
Hsieh etal . NEn gl JMed .2 0 09 ;36 1(2 4):2 30 9-1 7
AdverseEvents
• AcuteorchronicGVHDdidnotoccurinanypatientEvent # of
patientsTimeafter
ASCTOutcome
CMVreactivation 1 14days Treatedwithfoscarnetand resolvedNarcotic withdrawal 3 Varying Hospital admittotapernarcotics
Abdominal Pain 2 3&12months Resolved
Transfusion-associated babesiosis 1 8months ResolvedExercise-related rhabdomyolosis 1 3 months Switched bactrimtopentamidineVentriculartachycardia 1 Previous to
ASCTRatecontrolled
Clostridium difficilecolitis 1 4months ResolvedCholelithiasis- induced acutepancreatitis
1 15months Resolved
Fever 1 1months Resolved
Hsieh etal . NEn gl JMed .2 0 09 ;36 1(2 4):2 30 9-1 7
Hsiehetal,2014• Study
• High riskSCDpatients• NMAregimen (extensionofpreviously reporteddata)
• Outcomes§ n=30§ 29patientssurvived median3.4years,noNRM§ 1patientdiedofintracranial bleedafter relapse§ 87%patientswithlong-term stable donorengraftment§ Mean donorTcelllevel48%andmyeloid86%§ NoaGVHD orcGVHD§ 15patientsdiscontinuedISTsuccessfully§ ↓ annualhospitalizationrate,↓mean weekly narcotic use
Hsieh etal , JAMA2 0 1 4;3 12 (1):4 8-5 6

2/11/16
17
Sirolimuscomplications
• 3patientsbeingtreatedforhyperlipidemia
Complication # ofpatients TimeafterASCT OutcomePneumonitis
Patient 3 1 16months Sirolimus switched tocyclosporine
Patient 9 1 4months Reduction ofgoal trough
Arthralgias
Patient 9 1 3months Reduction ofgoal trough andsupportive care
Patient 1 1 4months Reduction ofgoal trough andsupportive care
Hsieh etal . NEn gl JMed 2 0 0 9 ;36 1(2 4):2 30 9-1 7
NMAinadultSCD– UICexperience
DAY -7 -6 -5 -4 -3 -2 -1 0
Alemtuzumab1mg/kg/total
300cGYTBI
Stem CellInfusion
Sirolimus
RESTDAY
Saraf etal . B io l B loodMarrowTran sp lan t.2 01 5 .p ii : S10 8 3-8 79 1
UICexperience• Conditioning regimen
§ Alemtuzumab/TBI300cGy§ GVHD prophylaxiswithSirolimus§ n=13,age 17-40§ Manypatients hadhighhematopoietic celltransplantation-specificcomorbidityindex(HCT-CI) ≥3
• Outcomes§ 11patientshadsevereneutropenia(ANC<500)formediandurationof6days
§ Medianhospitalization33days§ 1patienthadsecondarygraftfailure(noncompliantwithIST)§ NocasesofaGVHDorcGVHD§ At1year,12/13patientsmaintainedstabledonorchimerism§ 1patienthadsirolimus pulmonarytoxicity§ 4/13patientsdevelopedinfection;3/13hadCMVreactivation
Saraf etal . B io l B loodMarrowTran sp lan t.2 01 5 .p ii : S10 8 3-8 79 1

2/11/16
18
Transientneutropenia
0
1
2
3
4
5
6
7
8
9
10
1 8 15 22 29
Neu
trop
hil C
ount
(x
109 /L
)
Day Post-Transplant
Saraf etal . B io l B loodMarrowTran sp lan t.2 01 5 .p ii : S10 8 3-8 79 1
Hemoglobinconcentration
0
2
4
6
8
10
12
14
16
18
Pre-HSCT 3 6 9 12
Hemoglobin
(g/dL)
Months Post-HSCT
Female
Male
Saraf etal . B io l B loodMarrowTran sp lan t.2 01 5 .p ii : S10 8 3-8 79 1
Sirolimusandchimerism
Saraf etal . B io l B loodMarrowTran sp lan t.2 01 5 .p ii : S10 8 3-8 79 1

2/11/16
19
Hemoglobinfractionation
0
10
20
30
40
50
60
70
80
90
100
Pre-transplant Day+30 Day+60 Day+90 Day+180 1 Year
Hem
oglo
bin
A (%
)
Hb AA Donor
Hb AS Donor
Saraf etal . B io l B loodMarrowTran sp lan t.2 01 5 .p ii : S10 8 3-8 79 1
PatientQualityofLife(SF-36score)
30.1 31
36.8 37
42.137.6
48.245.5
GENERALHEALTH BODILYPAIN
NormBasedSF-36Score
Pre-HSCT Day+30 Day+90 1Year
Saraf etal . B io l B loodMarrowTran sp lan t.2 01 5 .p ii : S10 8 3-8 79 1
HCT–specificComorbidityIndex(HCT-CI)HCT-CIscore
• TooldevelopedbySeattleFredHutchinsonCancerResearchCentertocaptureinformationon17differentorgan-specificco-morbidities
• HCT-CI>8associatedwith30%NRM
UICexperience• HCT-CIassessedbaselineinallpatientsatUIC
• AdultSCDpatientshavemanyco-morbiditiesandthisshowsthatthisregimensafeandeffectiveinpatientswithhighHCT-CI
Sorro r etal , B lood 2 00 5;1 06 :29 12 -2 91 9Saraf etal . B io l B loodMarrowTran sp lan t 2 01 5 .p ii :S1 08 3-8 79 1
HCT-CIscoreof UICcohort*Figure courtesyof Damiano Rondelli
andPritesh Patel
LowHCT-CI (n=2)Intermediate HCT-CI (n=1)High HCT-CI (n=10)

2/11/16
20
UICexperience• NMAregimenofalemtuzumab and low-doseTBI
§ Normalizeshemoglobinin92%ofpatientswithclinicallyaggressive SCD
§ ReducesSCD-related complications§ Improvescardiopulmonary function§ Improvesqualityoflife
• Sirolimus trough levels§ Lower trough levelsofsirolimus resultedinchimerismlevelsequivalent tothose observed withhigherlevels
§ Lesstoxicity(arthralgias, mucositis,pneumonitis)
• ABO incompatibility§ 2patientswere ABOmismatchedandsuccessfullyengrafted (firstreported)
ALTERNATIVEDONORTRANSPLANTATIONUMBILICALCORD
HLA-HAPLOIDENTICAL
Umbilicalcordbloodtransplant(UCBT)• CBisanalternativesourceofhematopoietic
stemcellsforpatientswithmalignantandnonmalignantdiseases
• HLA-identicalsiblingUCBT§ ↓ aGVHD and cGVHD§ Graft failure in10% of patients1
§ Not studied inadults
• UnrelatedUCBTmuchlesssatisfactory2§ High rateof primary graftfailure and TRM§ DFSonly 50%2
1Locatel l i etal . B lood2 0 1 3 ;12 2 (6):1 07 2 -782Ruggeri etal . B io l B lood MarrowTran sp lan t2 0 1 1 ;17 (9 ):1 3 75 -1 38 2

2/11/16
21
BMversuscordinpediatricSCDLocatellietal(n=389)
Locatellietal(n=96)
Stemcellsource BM HLA-siblingCBTConditioningregimen Bu/CY/Flu,or
Bu/Flu/TT±ATGBu/CY,Bu/CY/Flu,Bu/Flu/TT,Bu/Flu,orBu/CY/TT±ATG
GVHDprophylaxis CSA±MTX(76%) CSA ± MTX(30%)
Medianfollow-up(mo)
72 72
EFS 88% 83%OS 95% 97%GraftFailure n=29 (7.4%) n=10(10.4%)TRM n=18 n=3aGVHD ≥II 21% 10%cGVHD 42/355(12%) 6/84(7%)
• Eurocord and EBMT1
• Median f/u70months• Median age 8.1years (BMT) and
5.9(UCBT)• Thalassemia major orSCD• CBT versus BM
• Slower neutrophil recovery(19versus 23days)
• Less aGVHD• No extensive cGVHD• No dif ference inOS (p=0.92)• DFS 92%(BM)and90%(CB)• 21patients died of
transplant-related causes (18BMT and 3CB)
• Related UCBT suitable option forpatients
Lo catel l i etal . B lood 2 0 13 ;12 2(6 ):10 72 -78
RICandUCBTinPediatricAdultSCD
• SCURT trial: n=8; median age 13.7years, median follow-upof 1.8years• Neutrophil recovery @median of 22days; 6of 8patients had platelet recovery
(>50,000/mm3)by day 100• 3patients whoengrafted had 100%donorcells byday 100,5had autologous recovery• 2patients had grade II aGVHD, 1chronicextensive cGVHD (died of respiratory failure)• Conclusion: high incidence of graftfailure; SCURT cordblood arm suspended
DAY - 8 - 7 - 6 - 5 - 4 - 3
Fludarabine 150mg/m2
Melphalan140mg/m2
TacrolimusorCyclosporineMMF
B io l B lood MarrowTran sp lan t20 12 ;18 :12 65 -12 7 2
- 2 - 1 0
Flu Flu Flu Flu Flu Mel
Alemtuzumab(startingD-21)
+1 to+28
HaploidenticalSCT• Rationale
§ HLA-identical matched donors difficult tofind§ MAC prohibited inmost adult patients§ GVTeffect not necessary in non-malignantdiseases
• Post-transplantcyclophosphamide (PT-CY)§ Targets proliferating, allo-reactive Tcells§ Spares hematopoietic stem cells because of highlevelsof aldehyde dehydrogenase
§ Similar GVHDrisk and immune reconstitutioncompared toMSD
Bolano s-Meade.B lood 20 12 ;20 :42 85 -4 29 1

2/11/16
22
HLA-haploidenticalSCTinadults
• NMA regimen using Flu/CY/ATG andGVHD prophylaxis withCY andFK /MMF orsirolimus/MMF
• Median followup of 711days, median age 30years• n=14(HLA-haploidentical) and n=3 (HLA-matched sibling donors)• 11patients engrafted; median time toneutrophil and platelet recovery was 24days• 10patients asymptomatic and 6patients off IS• 1patient developed aGVHD (skin, resolved withouttreatment)• No deaths reported
DAY - 9 - 8 - 7 - 6 - 5 - 4
Flu 150mg/m2
CY14.5mg/kgD-6andD-5TBI2GyD-1
- 3 - 2 -1
RabbitATG0.5mg/kgonD-9and2mg/kgonD-8
andD-7
0 +1 +2 +3 +4
ATG ATG ATGFLU FLU FLU FLU FLU FLUCY CY TBI
CY CY
CY50mg/kg/dD+3andD+4FK/sirolimus (1year) andMMF(D+35)
Bo lano s-Meade.B lood 20 12 ;20 :42 85 -4 29 1
Conclusions• SCD patients need tobe completely immunoablated
§ Immunocompetent patients§ Alloimmunization
• Encouraging data in pediatrics usingMAC regimens§ Bu/Cy/ATG§ Longtermcomplications(gonadal,neurologic)
• MAC regimens have not been successful in adults§ HighTRMinadultswhohavemoreadvancedSCD§ NMAregimenssafeandeffectiveinadults§ SmalllevelchimerismamelioratesSCDsymptoms§ Alternativetransplantsbeingexplored(haplo-HCT,UBCT)
OverallSurvivalbyDonorSource
The3-yearOS~90%regardless of thesourceofHSCsGlu ckman E.ASHedu cation book2 0 13 ;37 0 -3 7 6

2/11/16
23
Supportivecaresconsiderations
• RBCexchange priortoHCT• Goal HBS < 30%
ALLOSENSITIZATION
• Penicillin VK• Acyclovir• Sulfamethoxazole-trimethoprim orpentamidine forPJPprophylaxis• Fluconazole
INFECTIONPROPHYLAXIS
• Maintain platelet count>50Kand Hemoglobin >9• Avoid use of growthfactoras it has showntoexacerbate SCD crises
PRECAUTIONS/CONTRAINDICATIONS
• These patients are opioid dependent and pain symptoms take time toresolveafter HCT
PAINMANAGEMENT
Saraf etal . B io l B loodMarrowTran sp lan t.2 01 5 .p ii : S10 8 3-8 79 1
ConclusionGrowing adultSCDpopulation:
↑ morbidity andmortality↑ hospitalizations andhealthcarecosts
Limited treatments for refractoryseveredisease
Addition ofalemtuzumab andsirolimus toAlloHCT processachievesmixedchimerism anddemonstrates asafeandeffectiveoption forAdultSCDwith severedisease
AlloHCT proven successful ineliminating symptomsandcomplications forpediatric SCDpatients, tootoxicforadults SCDpatients
Saraf etal . B io l B loodMarrowTran sp lan t.2 01 5 .p ii : S10 8 3-8 79 1
ARSQuestion#1
Myeloablativeconditioningregimensarepreferredforadultpatientsovernon-myeloablativeconditioningregimensduetodecreasetransplantrelatedmortalityandincreasechimerism.A. TrueB. False

2/11/16
24
Case1
PTisa21year-oldfemalewithSCDandisbeingconsideredforHCT.Shehasbeenadmittedseveraltimesforpaincrisisandacutechestsyndrome.Shehasosteonecrosisinherrightkneeandhadastroke1yearago.Sheisonchronicpartialexchangetransfusions.
ARSQuestion#2• Basedonthispatient’s PMH,whatisthe
indication forHCT?A. Multiple pain crisisB. History of strokeC. Osteonecrosis of 1jointD. None of theabove. Thispatient does not have
an indication for HCT
ARSQuestion#3
Themostappropriateconditioning regimenforheris?A. Bu16mg/kg,TBI800cGyB. Bu14mg/kg,FLU180mg/m2,ATGC. Bu12mg/kg,CY200mg/kg,alemtuzumabD. BU6.4mg/kg,FLU180mg/m
2

2/11/16
25
ARSQuestion#4MAisa5year-oldmalewithSCD.HehasanHLA-identicalsibling.HisPMHissignificantfor2episodesofACS,4episodesofvaso-occlusivecrises,andrecurrent priapism.BecauseofhisPMH,heisbeingconsideredforHCT.
ARSQuestion#4Whatisthemostappropriateconditioningregimenforthispatient?
A. Bu 16mg/kg, CY 200mg/kgB. TBI 200 cGy, FLU 24mg/m2, Cy500mg/m2
C. BU 6.4mg/kg IV, FLU180mg/m2
D. TBI 200 cGy, FLU 150mg/m2
KarenSweiss, PharmD,BCOPClinical Assistant Professor
Clinical Pharmacist inHematologyandStemCell TransplantDepartmentofPharmacyPractice
Universityof I llinois College ofPharmacyChicago, IL
HEMATOPOIETICSTEMCELLTRANSPLANTFORSICKLECELLDISEASE:PERSPECTIVESFROM
CHILDHOODTOADULTHOOD