heat temp,thermistor couple
TRANSCRIPT

Heat, Thermal Conductivity In
The Body, Sources of Heat Loss
During Anesthesia, Methods Of
Measuring Temperature,
Thermistors, ThermocouplesDr Bikash Subedi
Moderator: Dr Binod Gautam

Heat Vs Temperature
Heat Temperature • Energy form,total sum of
kinetic energy of molecules
• Calorimeter
• joules
• temperature is a numerical measure of how hot or cold!
• measure of the averagekinetic energy of molecules
• Thermometer
• Celsius, Fahrenheit, Kelvin
BA

10
5
10


Interconversion
• C/5 = {F-32}/9C= (F-32)X 0.555
• C= K-273.13
• Inc. in 1 0C ~ 1 .8 0F

Normal body temperature
• 37+/- 0.5 0 C
• regular circadian fluctuation of 0.5–0.7 °C
• lowest early morning/ highest evening
• Mid-cycle fluctuation in women
• Less precise in children may normally have a temp. 0.50C above the normal for adults

• the anus (rectum/rectal), vagina, or in the ear (otic) is about 37+/- 0.5 °C
• Temperature in the mouth (oral) is about 36.8 °C (98.2 °F)
• Axillary temp is about 36.5 °C (97.7 °F)

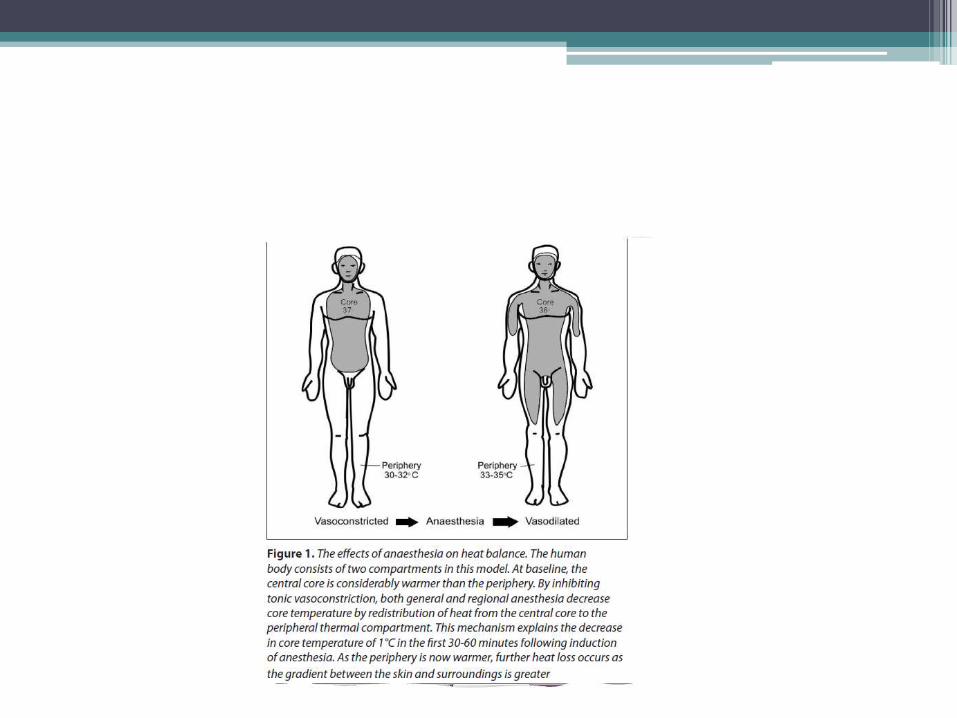
Core Vs Periphery
CORE PERIPHERY
• major thoracic and abdominal organs & Brain
• holds two-thirds of the body heat content
• Maintained within a narrow temp. range (36.6 to 37.4°C)
• limbs and skin and subcutaneous tissue
• About one-third
• varies widely.dependingon the environment
• usually 30-32°C.
This 5-7°C difference between core and peripheralbody temperature is maintained by vasoconstriction in the blood
vessels

Thermoregulation

Temp. control
• Ant/posterior Hypothalamus spinal cord
• Warm receptors>> cold
• skin and deep receptorsabdominal viscera , in/around large vessels
• Cold receptors>> heat


Transmission Cold signals – Via Aδfibres
warm signal – C fibres

HEAT GAIN
• Vasoconstriction (sympathetic activity) <36.5 0C- enhances insulation
• Chemical thermogenesis- Non shivering in neonates- effect of thyroid hormone on BMR
• Shivering (<36.0 0C)4-6 fold increase in heat production
• Muscular exercise
• Piloerection

Nonshivering Thermogenesis• metabolic process located primarily in brown
adipose tissue and controlled by the activity of the sympathetic nervous supply
• all the energy of metabolism is dispersed as heat without any ATP!
• Adrenaline and Noradrenaline stimulate uncoupled oxidative phosphorylation
• Conversion of T4 to T3 inside brown fat cells. T3
↑cellular metabolic rate

Thermal conductivity
• property of a material to conduct heat• watts per meter kelvin• Thermal Conductivity = heat × distance / (area ×
temperature gradient• Thermal capacity: Necessary amount of energy
needed to increase temperature by 1 kelvin
• Fat: very low thermal conductivity and thermal capacity
• Muscles and skin: higher thermal conductivity

Heat loss
• Physical mechanisms:• Radiation(40%)
• Convection (15-20%)
• Evaporation (20%)
• Respiration { 10% (8% humidification & 2% heating of air)}
• Conduction (5%)

Radiation
• Major type of heat loss (40%)
• Heat transfer is proportional to the difference of 4th power of the absolute temperature difference between the surfaces

Convection
• 2nd most important factor (30%)
• Heat loss in proportional to square root of the air speed

Evaporation
• accounts for 10% of heat loss• Evaporation of 1g water removes about 0.6
Kcal. Of heat• Insensible loss (600ml/d even without sweating)• Increased by sweating• In infants higher fraction of heat loss by
transpiration of water through thin skin( in preterms heat loss can be 1/5th of metabolic heat production)
• Heat loss from respiratory system trivial• Exposure of surgical wounds potentiates heat loss

Conduction
• Directly proportional to the temperature difference 2 adjacent surfaces and the strength of the thermal insulation separating them.
• <5%

Sweating
• Sympathetic cholinergic fibers
• prevented by nerve block or administration of atropine
• only mechanism by which the body can dissipate heat in an environment exceeding core temperature
• 0.6 kcal dissipated per gram of evaporated sweat

Intra-operative heat loss
(i) Exposure- cold OT- shed clothes, cold table, cold skin prep
(ii) Cold IV fluids
(iii) Cold irrigating fluids
(iv) Evaporative heat losses- dry anesthetic gases- body cavity exposure

• (v) Anesthetic drugs1. Volatiles- depress threshold for thermoregulation 2-3°C;- promote vasodilatation;- muscle relaxation -> impede shivering;2. Opioids- potent sympatholytics - depress threshold ~ = volatiles;3. Muscle relaxants- prevent shivering;4. Phenothiazines, barbiturates-> vasodilatation decTB;5. Vasodilators- promote heat loss.(v) Regional anesthesia- hypothalamic thermoregulation intact -> heat loss enhanced by vasodilatation and impaired shivering below the level of the block.

General Anesthesia
• decline in body temp. occurs in three phases
Phase I
Upto 1st hour. 1-1.5 0C
Rapid fall
Core to periphery redistribution
due to vasodilation
Phase II
2-3 hours.
Slower decline
↓BMR
Loss > production
Phase III
After 3-5 hrs
Plateau
Loss = production
vasoconstriction

Heat loss during GA


Hypothermia Considerations in
anesthesia• Widens interthreshold range from 0.4 - 3°C• ↓ Drug metabolism
DOA vecuronium is more than doubled in patients with a core temp. <35°C.
• ↑Solubility of inhaled anesthetic agents↓ MAC of 5% for every 10 decrease in core temp.
• delayed awakening• Left shift of the hemoglobin–oxygen saturation curve• ↓ BMR• Reversible coagulopathy (platelet dysfunction)• Poor wound healing• Cardiac arrhythmias and ischemia• Impaired renal function• Postoperative protein catabolism and stress response• CNS dysfunction

Physiologic Changes Associated with Hypothermia

MEDICAL CONDITIONS PREDISPOSING
TO HYPOTHERMIA•
1. Skin loss - burns, severe exfoliating dermatoses;2. Autonomic neuropathy -para/quadriplegia, diabetes, uraemia;3. Acute alcohol intoxication;4. Endocrinopathies - myxoedema, adrenal insufficiency;5. General debilitation;(6. Sickle cell diseases - hypothermia can precipitate a crisis).

SPECIAL CONSIDERATIONS
Neonates and infants• increased surface area to volume ratio
• thin skin with minimal insulating fat
• less effective efferent responses to cold temperatures.
• Infants <3 months cannot shiver
Measurement of Temperature

Monitoring recommendations
• Core body temperature should be measured in GA >30 minutes.
• During regional anesthesia when changes in body temperature are intended, anticipated, or suspected. 3.
• Unless hypothermia is specifically indicated (e.g., for protection against ischemia), effort should be made to maintain intraoperative core temperature higher than 36°C.

ASA recommendation
• “every patient receiving anesthesia shall have temperature monitored when clinically significant changes in body temperature are intended, anticipated or suspected.”
• For office-based sedation, regional anesthesia, or general anesthesia, the ASA also requires that “the body temperature of pediatric patientshall be measured continuously

Methods of measuring temperature
• Non – electrical technique
• Electrical technique
• Infrared ear and tympanic membrane thermometers

Non electric thermometers
• Mercury , alcohol
• Based on “ change in volume with temperature”
• Mercury thermometer - German physicist Daniel Gabriel Fahrenheit in 1714
• Mercury for higher temperature and alcohol for lower temperatures

Dial thermometers :
Bimetallic stripTwo dissimilar metals fixed together in a coil
Unequal Metal expansion leads to coil tightening and movement of level clock-wise

Bourdon gauge
•Actually a device to measure pressure which is attached to sensing element containing a small tube of mercury or a volatile fluid
•With temperature , volume or pressure changes in the sensing element which is recorded on bourdon gauge , and is calibrated in units of temperature.

Electrical technique
• Resistance thermometer
• The thermistor
• The thermocouple

Resistance thermometer
• Based on the fact that the electrical resistance of a metal increases linearly with temperature
• Consists of of : platinum wire resistor , a battery , ammeter
• Insensitive

Thermistor•a type of resistor whose resistance varies significantly with temp. more so than in standard resistors
•Is a small bead of metal oxide , the resistance of which falls exponentially as the temperature rises
•Used clinically in PA catheters , esophageal stethescopes , can be kept in body cavities
•Cheaper

platinum
thermistor

Thermocouple•Based on Seebeck’s effect
•At junction of 2 different metal ( copper and constantan) small voltage is developed ,magnitude of which is dependent on the temp. of the junction
•Reference junction should be kept at constant temperature
•Used in clinical hyperthermia


Infrared ear and tympanic membrane
thermometer• Based on emission of electromagnetic radiation by
objects and the intensity of radiation and thewavelength depend on the temperature of the object.
• At body temperature object primarily emits Infraredradiation
• The sensor is kept in ear canal or near ear drum , whichsenses the radiation and converts it into electric signal