healthcare - amazon web servicesaapcperfect.s3.amazonaws.com/5548a1af-4c9f-49a2-bfe0-bfa... ·...
TRANSCRIPT

www.aapc.com
HEALTHCAREBUSINESS MONTHLYCoding | Billing | Auditing | Compliance | Practice Management
April 2016
MS-DRG May Spell TROUBLE: 32
CMS looks at time for mechanical ventilation billing
Rock the Mock Audit: 48
Don’t let an external audit keep you up at night
The Doctor Said What? 52
Have a laugh at ridiculous physician notes

AnaheimSeptember 19-21, 2016Disneyland Hotel
Atlantic City October 6-8, 2016Harrah’s Atlantic City
$695 $345 THROUGH MAY 3112 CEUS | 2.5 DAYS
HBM - Full Page Regional Conferences - v5.indd 1 2/26/2016 2:21:44 PM

www.aapc.com April 2016 3
[contents]■ Coding/Billing ■ Practice Management ■ Auditing/Compliance
[continued on next page]
Healthcare Business Monthly | April 2016
28 CPT® 2016: Percutaneous Biliary Interventional Coding
David Zielske, MD, CIRCC, CCVTC, COC, CCC, CCS, RCC
48 Rock the Mock Audit Lisa Jensen, MHBL, FACMPE, CPC
58 What (Not) to Wear While Job Hunting
John Verhovshek, MA, CPC
COVER | Coding/Billing | 35
Balance Billing: Is It Legal?By Mary Pat Whaley, FACMPE, CPC

4 Healthcare Business Monthly
Healthcare Business Monthly | April 2016 | contents
18
42
54
■ Added Edge16 Search Online for Healthcare Business Monthly Articles Michelle A. Dick
■ Coder’s Voice20 CMS EHR Toolkit Gives a Glimpse into Potential Compliance Issues Sheri Poe Bernard, CPC, COC, CPC-I, CCS-P
■ Coding/Billing18 Examine Integumentary and Musculoskeletal Coding Changes John Verhovshek, MA, CPC
26 Conquer Common Billing Errors Judy A. Wilson, CPC, CPCO, CPPM, CPB, CPC-P, COC, CPC-I, CANPC
32 MS-DRG May Spell TROUBLE for Mechanical Ventilation Billin Leonta (Lee) Williams, RHIT, CPC, CPCO, CCS, CCDS
38 The Ins and Outs of Inpatient Psychiatric Facility Perspective Payment System
Heather Greene, MBA, RHIA, CPC, CPMA
■ Auditing/Compliance42 The Latest on HIPAA: The Gun Check Rule Sue Miller
44 2016 OIG Work Plan: Part B Risk Areas Michael D. Miscoe, JD, CPC, CASCC, CUC, CCPC, CPCO, CPMA
■ Practice Management52 The Doctor Said What? Lori A. Cox, MBA, CPC, CPMA, CPC-I, CEMC
54 The Nine “Cs” of Clinical Documentation Improvement Ken Camilleis, CPC, CPC-I, COSC, CMRS, CCS-P
DEPARTMENTS7 Letter from CEO
8 Letters to the Editor
8 Chat Room
9 I Am AAPC
10 AAPC National Advisory Board
12 AAPC Chapter Association
13 Local Chapter News
14 Ethics Committee
66 Minute with a Member
EDUCATION60 Newly Credentialed Members
Online Test Yourself – Earn 1 CEU www.aapc.com/resources/publications/
healthcare-business-monthly/archive.aspx
COMING UP: • Member of the Year • MIPS Is Coming • New Chapter Association • Category III Codes • Influence Providers
On the Cover: To avoid the pitfalls of balance billing, Mary Pat Whaley, FACMPE, CPC, explains how to stay in line with private carrier rules and follow updated Medicare and Medicaid guidance. Cover image by istock.com/DNY59. Cover design by Kamal Sarkar.

CPC CIC CRCCOC
Students that complete our courses are TWICE AS LIKELY to pass the certi�cation exam.
For more information or to enroll visit: www.aapc.com/exam-prep
Looking to get
certi�ed?CPPMCPB CPCOCPMA
ICD-10 integrated and interactive lectures with all coding and billing courses.
6 Healthcare Business Monthly
Volume 3 Number 4 April 1, 2016Healthcare Business Monthly (ISSN: 23327499) is published monthly by AAPC, 2233 South Presidents Drive, Suites F-C, Salt Lake City UT 84120-7240, for its paid members. Periodicals Postage Paid at Salt Lake City UT and at additional mailing office. POSTMASTER: Send address changes to: Healthcare Business Monthly c/o AAPC, 2233 South Presidents Drive, Suites F-C, Salt Lake City UT 84120-7240.
Serving 155,000 Members – Including You!ve
ndor
inde
x
Director of PublishingBrad Ericson, MPC, CPC, COSC
Managing EditorJohn Verhovshek, MA, CPC
Editorial Michelle A. Dick, BS
Renee Dustman, BS
Graphic Design Mahfooz Alam
Kamal Sarkar
Advertising Jon Valderama
Address all inquires, contributions, and change of address notices to:
Healthcare Business MonthlyPO Box 704004
Salt Lake City, UT 84170(800) 626-2633
©2016 Healthcare Business Monthly. All rights reserved. Reproduction in whole or in part, in
any form, without written permission from AAPC® is prohibited. Contributions are welcome.
Healthcare Business Monthly is a publication for members of AAPC. Statements of fact or
opinion are the responsibility of the authors alone and do not represent an opinion of AAPC,
or sponsoring organizations.
CPT® copyright 2015 American Medical Association. All rights reserved.
Fee schedules, relative value units, conversion factors and/or related components are not as-
signed by the AMA, are not part of CPT®, and the AMA is not recommending their use. The
AMA is not recommending their use. The AMA does not directly or indirectly practice medi-
cine or dispense medical services. The AMA assumes no liability for data contained or not
contained herein.
The responsibility for the content of any “National Correct Coding Policy” included in this
product is with the Centers for Medicare and Medicaid Services and no endorsement by the
AMA is intended or should be implied. The AMA disclaims responsibility for any consequenc-
es or liability attributable to or related to any use, nonuse or interpretation of information con-
tained in this product.
CPT® is a registered trademark of the American Medical Association.
CPC®, COCTM, CPC-P®, CPCOTM, CPMA®, and CIRCC® are registered trademarks of AAPC.
HEALTHCAREBUSINESS MONTHLYCoding | Billing | Auditing | Compliance | Practice Management
Go Green!Why should you sign up to receive Healthcare Business Monthly in digital format?
Here are some great reasons:
• You will save a few trees.
• You won’t have to wait for issues to come in the mail.
• You can read Healthcare Business Monthly on your computer, tablet, or other mobile device—anywhere, anytime.
• You will always know where your issues are.
• Digital issues take up a lot less room in your home or office than paper issues.
Go into your Profile on www.aapc.com and make the change!
April 2016
Ask the Legal Advisory BoardFrom HIPAA’s Privacy Rule and anti-kickback statute, to compliant coding, to fraud and abuse, there are a lot of legal ramifications to working in healthcare. You almost need a lawyer on call 24/7 just to help you make sense of all the new guidelines. As luck would have it, you do! AAPC’s Legal Advisory Board (LAB) is ready, willing, and able to answer your legal ques-tions. Simply send your health law questions to [email protected] and let the legal professionals hash out the answers. Select Q&As will be published in Healthcare Business Monthly.
Medical Coding Legal Advisory Committee:
Timothy P. Blanchard, JD, MHA, FHFMA Julie E. Chicoine, JD, RN, CPC Michael D. Miscoe, JD, CPC, CPCO, CPMA, CASCC, CCPC, CUC Christopher A. Parrella, JD, CPC, CHC Robert A. Pelaia, Esq., CPC Stacy Harper, JD, MHSA, CPC
American Medical Association ......................................13, 53 www.amastore.com
HealthcareBusinessOffice, LLC ............................................33 www.HealthcareBusinessOf fice.com
ZHealth Publishing, LLC ..................................................... 25 www.zhealthpublishing.com
www.aapc.com April 2016 7
Letter from CEO
You Are AAPC’s StrengthAAPC is a membership organization, a collection of peers who help to improve healthcare for
the whole country through our expertise in managing the business of healthcare. Be-ginning this month, AAPC celebrates our roles and common goals a number of ways.
Be Part of the Fellowship at ConferenceAAPC’s annual national conference, HEALTHCON, runs April 10-13, at Disney’s Coronado Springs Resort in Orlando, Florida. In addition to sharing and learning about industry trends and so-lutions with other industry experts, attendees get the chance to make new friends and catch up with old acquaintances. This fellowship is important to AAPC, and essential to members. Also at HEALTHCON, we will celebrate both our 2015 Member of the Year and Chapter of the Year. The Member of the Year is someone who not only exemplifies the professional values of AAPC, but also has contributed to their colleagues’ success. The person we’re praising this year has done all that and more, and I’m excited to be a part of the celebration. The honorees will be fea-tured in upcoming editions of Healthcare Business Monthly.For those of you who can’t make it to HEALTHCON this year, AAPC is also holding regional con-ferences in Anaheim, California, September 19-21, at the Disneyland Hotel, and in Atlantic City, New Jersey, October 6-8, at Harrah’s.
Local Chapters: Our GrassrootsAAPC’s more than 500 local chapters are unique in our industry, and it’s in our chapters where most of AAPC’s networking happens. Few membership organizations can boast the enthusiasm and dedication of our chapter officers and attendees. Chapter members are privy to interesting, in-sightful, and useful presentations; fun social events; and caring community projects put on by local chapters all over the country. This year’s Chapter of the Year stands out, but does not stand alone.
Get Excited for May MAYniaNext month is May MAYnia, when all chapters open doors to new and existing members through special activities and speakers. Chapters compete to increase attendance the most, so be certain to attend your chapter’s meeting next month. If you haven’t taken advantage of the intelligence, sup-port, and experience of your local chapter, try it! You have nothing to lose, and everything to gain. You can find out where and when your local chapter meets on AAPC’s website at www.aapc.com/local-chapters/find-local-chapter.aspx.
Support Each Other and Strengthen Healthcare I’m grateful for the opportunity to meet many of you at these events. Our strength is our member-ship. I gather strength from you and what you do to make AAPC such a vital organization. There are many new opportunities ahead of us, such as value-based payment, ongoing code updates, clin-ical documentation improvement, and other movements. Together, we are raising the business of healthcare to new levels.
Sincerely,
Jason J. VandenAkkerCEO
Together, we are raising the business of healthcare to new levels.

8 Healthcare Business Monthly
Please send your letters to the editor to: [email protected] to the Editor
Chat Room
CHAT
ROO
M
Spreading AAPC Love through Social MediaIf you post on AAPC’s Facebook page, many AAPC members and employees read your threads. Our staff enjoys reading your posts and appreciates your feedback — especially when you spread positive messages to fellow members. Here are two posts that caught our eye this month:
On February 15, Petersburg, Va., Local Chapter President Cynthia Briggs CPC, CPMA, shared a positive experience she had with AAPC Customer Service Representative Cindy Gigante. And later that month, our very own Vice President of Strategic Development Rhonda Buckholtz, CPC, CPCI, CPMA, CRC, CHPSE, CENTC, CGSC, CPEDC, COBGYN, took a moment to share her AAPC pride. Thanks ladies for spreading the love!
Michael S. Mix UpOur apologies to Michael Strong, MSHA, MBA, CPC, CEMC, and Michael Stearns, CPC, CFPC, for getting their bio photos mixed up on page 37 of the March edition.
Speak Up and Be Heard!Do you have a question regarding information found in Healthcare Business Monthly? Or maybe you have a difference in opinion you would like to share with your peers?
Write us at: [email protected].
www.aapc.com
HEALTHCAREBUSINESS MONTHLYCoding | Billing | Auditing | Compliance | Practice Management
March 2016
Fight for Insurance Carrier Payment: 27
Have a game plan that gets you paid
The NPP Scope of Practice Scoop: 48
Meet state practitioner authorization requirements
Time Is Ticking on Old Accounts: 55
Manage unpaid claims now to increase revenue
March2016_HBM.indd 1 11/02/16 9:33 pm
Michael Strong, MSHA, MBA, CPC, CEMC
Even Better Bronchoscopy in 2016On page 24 of the March issue, in the article “Better Bronchos-copy in 2016,” the second paragraph lists the wrong deleted code. CPT® 61620 is not deleted; add-on code 31620 is deleted, effective January 1, 2016.

www.aapc.com April 2016 9
I always wanted to work in the medical field. My original plan was to become a medi-
cal assistant and use that position to pay for nursing school. Two years into working and halfway through my bachelor’s degree pro-gram, I was diagnosed with systemic lupus erythemosis.My immune system forced me to consider a new career, and medical coding seemed in-teresting.I finished school fairly quickly. A lot of the classes were the same as a pre-nursing major, but if anybody had bad luck, I felt like I did.
Hurdle OneOne month before graduation, the govern-ment postponed the ICD-10 implementa-tion; however, my school had already started teaching ICD-10 because ICD-9 was slated to be obsolete by graduation. This meant I didn’t know ICD-9 well enough to sit for a certification exam.
Hurdle TwoMy school was AHIMA accredited and encouraged us to take the Certified Cod-ing Specialist (CCS) test; however, the test was suspended indefinitely within weeks of graduation. All of my exam preparation was in vain.
Hurdle ThreeI had to self-teach myself ICD-9 because I
racked up a huge tuition bill and ran up my credit card with books and study materials.I began to work with a medical coder. She stated that medical coding was a progres-sive career and that outpatient was the best way to ease into the career and find where my niche would be.I was psyched and decided to sit for the Cer-tified Professional Coder (CPC®) exam. Al-though I had been out of school for a year, I was already working with codes and felt fairly confident and ready. Unfortunately, I failed by an earth-shattering 1 percent. The road seemed so long, my career advance-ment was once again stalled, and I began to question whether this was truly the ca-reer for me.My husband believed I could pass and en-couraged me to study. For four weeks, I studied day and night. I applied my studies to the coding I was doing at work. My hus-band and my father bought all the study ma-terials AAPC had available. One month lat-er, I passed the exam!
Jump Those Hurdles and Never Give UpIt was all about not giving up and having a strong desire to be in the field. I believe my obstacles have shaped me to be committed to the business side of healthcare and I am extremely proud of having the letters CPC® behind my name.
I Am AAPC
#IamAAPCHealthcare Business Monthly wants to know why you chose to be a healthcare business professional. Explain in less than 400 words why you chose your healthcare career, how you got to where you are, and your future career plans. Send your stories and a digital photo of yourself to: Michelle Dick ([email protected]) or Brad Ericson ([email protected]).
LEANDREA ABERCROMBIE, CPC
#Ia
mA
AP
C
#IamAAPC

10 Healthcare Business Monthly
Region 7 – Mountain/Plains
As a follow up to the January article “The National Advisory Board Is Here to Serve You,” we are spotlighting each of the eight
regions and the National Advisory Board (NAB) members who rep-resent them. In February, we featured Region 5 – Southwest repre-sentatives; this month, we’re zoning in on Region 7.
Region 7 - Mountain/PlainsThe Mountain/Plains region is comprised of Idaho, Utah, Arizona, New Mexico, Montana, Wyoming, Colorado, North Dakota, South Dakota, Nebraska, and Iowa. This region covers the largest number of states, with 14,662 members and 64 chapters.
Glenda Hamilton, CPC, COC, CPC-P, CPMA, CEMC, and Angelica Stephens, RHIT, CPC, COC, COSC, CPMA, CCS-P, are the NAB representatives who promote, serve, and support AAPC and its Region 7 members. These representatives are unique in that they are from two totally opposite ends of the United States: Albuquerque, New Mexico, and Cherry Hill, New Jersey. When they became Region 7 representatives, it was like “east meeting west.” Although they hale from opposite ends of the country, they have the same professional goals.
Hamilton and Stephens have a “one team” philosophy, and they are passionate about strengthening AAPC members and paying it forward. “I am passionate about everything I do,” Stephens said at the first NAB meeting. That’s what being a NAB member is about: loving what you do and wanting to share it with everyone.
Glenda Hamilton, CPC, COC, CPC-P, CPMA, CEMC Hamilton has more than 26 years of experience in practice management, coding, reimburse-ment, education, auditing, and consulting. She joined Cooper University Hospital in 2005 as a clinical documentation educator, and is now senior compliance auditor. Hamilton also runs her own consulting business, offering expert witnessing for attorneys.
Hamilton has been certified since 2003. An active member of the Cherry Hill, New Jersey, local
■ AAPC NATIONAL ADVISORY BOARD
Two representatives team up to promote, serve, and support AAPC and its Region 7 members.
www.aapc.com April 2016 11
Regional SpotlightNATIONAL ADVISORY BOARD
chapter, she has held multiple officer positions over the past 10 years, including vice president (twice), president (twice), member development officer, and education officer. She assists others with charitable acts and helps members to find jobs. Her professional ethics have influenced current officers with great success.
Angelica Stephens, RHIT, CPC, COC, COSC, CPMA, CCS-PStephens also obtained her first certification in 2003. Over the past 20 years, she has accrued experience in coding, reimburse-ment, education, audits, and management. Her career has exposed her to several specialties, but her favorite is orthopedics. Always eager to learn, Stephens is studying home health coding and consulting for private practice.
Stephens worked as an auditor in a compliance department for three years before taking on the role of revenue services manager for an orthopedic practice in Albuquerque, New Mexico. She now holds the position of member development officer of the Albuquer-que, New Mexico, local chapter, and is a member of the advisory board for the HIT Program at the local community college.
Making Region 7 StrongerWe hope you allow your NAB representatives to serve as a conduit to AAPC to ensure your voice is heard and your needs are met. Stephens and Hamilton are looking forward to meeting you at HEALTHCON in Orlando, Florida, on April 10-13. Feel free to contact these representatives any time to share positive or negative feedback, seek guidance, or to just say, “Hi!” You can reach Hamilton at [email protected] and Stephens at [email protected].
You Wanted Low Priced CEUs?How about $2.50 per Webinar!
+ 12 Months of Access to 40+ Live Events & Entire Library of 100+ On-Demand Webinars
+ Receive 2 CEUs per Webinar (Live & On-Demand)
+ Topics Cover 21+ Specialties
+ 12-Month Subscription Starting at $295 (Volume Discounting Available for Your Office)
800-626-2633aapc.com/webinars

12 Healthcare Business Monthly
By Judy A. Wilson, CPC, CPCO, CPPM, COC, CPC-P, CPB, CANPC, CPC-I
AAPC Chapter Association
Life can throw you curve balls. Most of the time, you dodge them or knock them out of
the ball park. But when one knocks you for a loop, and you need help getting back on your feet, look no further than your AAPC local chapter. Whether you find yourself homeless because of a natural disaster or experienc-ing financial difficulty due to illness, your chapter officers will gladly help you apply for assistance through Project AAPC and the Hardship Scholarship Fund.
Project AAPCEstablished in 2010, Project AAPC fur-ther developed former AAPC Chapter As-sociation Chair Jill Young’s, CPC, CEDC, CIMC, vision for chapter members to help one another by donating to the American Red Cross or Feeding America after a dev-astating event. Project AAPC donated more than $10,000 to those organizations dur-ing the Nashville floods of 2010, all of which was collected by AAPC members and AAPC staff. After finding out that some of our members were unable to get the help they needed from those organizations, the AAPC Chapter Association board decided to donate all Project AAPC money directly to chap-ter members in need. Project AAPC assists chapter members with money for food, lodg-ing, and basic necessities when there is a prov-en need. Since its inception, Project AAPC has helped many chapter members subjected to a devas-tating event. For example:
• Members recently affected by the South Carolina flood;
• A member with a severe illness preventing her from working; and
• A member who couldn’t afford a bus pass to get back and forth to work.
Hardship Scholarship Fund The Hardship Scholarship Fund was estab-lished in 2012 to help chapter members who have fallen on difficult times due to loss of job or the inability to find a job. The finan-cial help is used for members to keep their credentials, and can be applied to the cost of the ICD-10-CM proficiency exam, renewing national memberships, or purchasing cod-ing books. The Hardship Scholarship Fund is not given for additional credentials or non-essential needs. It provides for AAPC educational services, books, etc., but it does not cover workshops through AAPC or other organizations. This fund’s main purpose is to help struggling chapter members keep the original credential they worked so hard to obtain. Some things to keep in mind when applying for this fund:
• You must be an AAPC member in good standing.
• You must be active in your local chapter.• Consider first reaching out to your
local chapter for a scholarship.To date, the Hardship Scholarship Fund has helped over 336 members, at a cost of $55,333.85, and more than $103,220.19 has been contributed to the fund.
How to ApplyThe application for the Hardship Scholar-ship Fund can be found on AAPC’s official website at www.aapc.com/memberarea/chapters/scholarship-application.aspx. Remember to be
specific in the application about what you are doing for yourself and why exactly you need help. There is always hope and support, so please reach out when it is needed by you or another chapter member.
Pay It ForwardThe Scholarship Application Review Committee is made up of past AAPC Chapter Association board members serving in an anonymous and voluntary role. This ensures the process is fair to all. The funds are supported through donations made by members and local chapters. If funds run too low, the ability to grant scholarships will be put on hold until more funds become available. Talk to your chapter about budgeting for a gift to these funds, so we can keep helping our members who are in need. You can also make a personal donation. Personal donations should be in the form of a check, payable to the AAPCCA Hard-ship Scholarship Fund or Project AAPC, and mailed to: AAPCCA-Project AAPC/ AAPCCA-Hardship Scholarship Fund 2233 S. Presidents Drive Salt Lake City, UT 84120
Judy A. Wilson, CPC, COC, CPCO, CPPM, CPC-P, CPB, CPC-I, CANPC, has been a medical coder/biller for more than 35 years. For the past 25 years she has been the business administrator for Anesthesia Specialists, a group of nine cardiac anesthesiologists who practice at
Sentara Heart Hospital. Wilson served on the AAPC Chapter Association board of director from 2010- 2014, and is serving from 2015-2017. She is also on the board of directors of Bryant & Stratton College in Virginia Beach, Va. Wilson is a PMCC instructor and teaches classes in the Tidewa-ter area. She serves on the National Advisory Board for American Academy of Billers for AMBA, has presented at several AAPC regional and national conferences, and is a member of the Chesapeake, Va., local chapter.
Experiencing Hard Times
T H E R E ’ S H E L P
Project AAPC and the Hardship Scholarship Fund are here to help chapter members.
T H E R E ’ S H E L P
12 Healthcare Business Monthly
www.aapc.com April 2016 13
Local Chapter News
Houston’s New Year Celebration Fosters SuccessThe Houston, Texas, local chapter kicked off 2016 with a “Happy New Year!” theme chapter meeting. The entire chapter was very excited about the first meeting of 2016, which everyone agreed was a success.President Drieca D. Hopkins, CPC, CBCS, said, “Our speaker for the evening, Steven Woods, SHR-CP, PHR, did an awesome pre-sentation called ‘Preparing Your Resume for the Job You Want, Not the Job You Had.’” According to Hopkins, “It was beneficial for seasoned coders as well as newbies, giving us great tips on resume writing and what re-cruiters expect to see on resumes.” Houston also had a recruiter from K-Force present and share career opportunities.Houston’s Member Development Officer Carmen Chaisson-Hunt, CPC, was in-strumental in sharing multiple job oppor-tunities with the attendees, as well as creat-ing the chapter’s Facebook page. As a return-ing officer, Hopkins said she is “excited for a
Houston rings in the new year with Instagram selfies.
Houston shows members that everything is bigger in Texas, even local chapter meetings.
complete new board for 2016 — sharing new and bright ideas.”The chapter made a toast to 2016 with a little bit of the “bubbly” (sparkling cider). “It was a great time of mixing and mingling; it was infor-mative, as well as fun,” said Hopkins.
“We want our meetings to be informative, engaging, and fun! Our goal is to get more member involvement, educate more on ICD-10, promote certification, and be a BIG help to our uncertified members,” said Hopkins. That’s the way they do things in Texas: BIG!
Series includes:
This six-book series comes straight from the source of CPT code—the AMA—and exclusively provides the CPT Editorial Panel’s Guidelines instructions on ICD-10-CM documentation and coding.
To learn more, visit amastore.com or call (800) 621.8335.
Crack specialty coding with the American Medical Association’s 2016 CPT® Coding Essentials series—the perfect companion to your CPT® Professional codebook
Cardiology 2016General Surgery & Gastroenterology 2016Obstetrics and Gynecology 2016Ophthalmology 2016Orthopedics: Lower Extremities 2016Orthopedics: Upper Extremities And Spine 2016
Houston classes it up with fancy meeting flyers.

14 Healthcare Business Monthly
A Question of
■ AAPC Ethics Committee
What do you do when coding productivity is more important than ethics at your workplace?
I have noticed AAPC has an abundance of information regarding coder ethics, but not very much information of how the ethical coder is to react in a “not-so-ethical” environment. Many of the coders I know are employed in an environment where eth-ics fall far below productivity on the scale of importance. How are we to stand up to this type of pressure? We are repeatedly beaten down for pro-ductivity numbers, and the terms “quality,” “accuracy,” and “ integrity” are not even part of the vocabulary. It’s all well and good to demand a level of ethics of your membership, but your membership has to be able to work under circumstances that are quite a different story. And the membership needs to work to pay your dues. Why do you constantly pander to the health systems and push the “ethical” agenda? The members are paying the dues, give us recourse to do what is ethical.Be ethical, be respectful, be responsible. But please, tell us how to deal with monopoly health systems who don’t care about our ethics or if we are employed and able to pay our membership dues, but still expect us to be “caring people, caring for people.”
Thank you for your question. You raise an excellent issue. There are often competing demands and your commitment to professional and ethical behavior will help you make correct choices. I would point out that the AAPC Code of Ethics addresses more than just the quality of your professional work. Although I understand that the demands of productivity can sometimes impact quality, the Code of Ethics is not designed to punish mistakes. And while you should strive to be both efficient and accurate, there is a breaking point. That’s your em-ployer’s problem, not yours. When you’re pushed to be more produc-tive, it’s likely that quality and accuracy will suffer. If that is the case, your obligation is merely to raise the issue with your employer. If they are willing to compromise quality for perceived productivity, so be it. You have met your obligation by raising the concern. Because your employer, as an entity, is not likely subject to the AAPC Code of Eth-ics, you can’t make them do the right thing. That’s the job of law en-forcement and/or carrier special investigative units.The Ethics Committee would never waste time on a case where your coding was deemed inaccurate because you weren’t given sufficient time to do your job properly, especially where you expressed the con-
cern with your employer. The impact of those mistakes will fall where they belong, on the practice. The practice will be forced to re-fund overpayments or may suffer payment delays or denials because of those mistakes. Although the practice may seek to place the blame on you for the errors, the evidence of your previously-raised concerns would undermine such allegations. Relative to your work as a coder, the Code of Ethics would come into play only if you purposefully or negligently misrepresented services for the purpose of receiving some personal benefit. That doesn’t seem to be the issue here.Productivity improvement and efficiency are not improper goals for any organization; they are key to profitability. There is a bal-ance, however, that must be found. At some point, pure productivity based on how many claims you must code becomes counterproduc-tive when you have insufficient time to ensure codes reported are jus-tified or accurate. As to your question relative to the motive behind the Code of Eth-ics, it’s in no way a form of pandering. AAPC members can be found working on behalf of providers, payers, and the government. Our eth-ical standards exist because we cannot call ourselves a professional or-ganization without them. All professions impose and enforce ethical standards on their members. Our commitment to ethical conduct, as well as educational standards as measured through testing, is what separates us from others who have not had to demonstrate their com-petence in the areas of coding, billing, auditing, practice manage-ment, or compliance. For that reason, AAPC credentialed members have more value in the marketplace. Ultimately, you are the only per-son who can determine how you will act or react in a given circum-stance. The Code of Ethics is a guide to help ensure you act or react in a professional manner.
Michael D. Miscoe, JD, CPC, CASCC, CUC, CCPC, CPCO, CPMA, is president-elect of AAPC’s National Advisory Board, serves on AAPC’s Legal Advisory Board, and is AAPC Ethics Committee chair. He is admitted to the practice of law in California as well as to the bar of the U.S. Supreme Court and the U.S. district courts in the southern district of California and the western district of Pennsylvania. Miscoe has over 20 years of experience in healthcare coding and over 18 years as a forensic coding and compliance expert. He has provided expert analysis
and testimony on coding and compliance issues in civil and criminal cases and represents healthcare providers in post-payment audits and HIPAA OCR matters. Miscoe speaks on a national level, and is published nationally on a variety of coding, compliance, and health law topics. He is a member and past president of the Johnstown, Pa., local chapter.
By Michael D. Miscoe, JD, CPC, CASCC, CUC, CCPC, CPCO, CPMA
istoc
k.com
/trav
elling
light

I find the CMS 1500 claim editchecker to be the most helpful tool ever
created by coding-mankind. I also love thefact that everything is in one place: LCD, NCCI edits, Fee Schedule, etc.
The premier online coding tool from the largest coding credentialing organization.
Lay Descriptions
CPT Crosswalks
ICD-10 Bridges
Fee Schedules
NCDs & RVUs
Survival Guides
Real Time Claim Scrubber
CPT Modifiers
ICD-9 Crosswalks
CCI Edits Checker
Medicare LCD lookup
CMS Transmittals
Specialty Newsletters
EARN UP TO20 CEUsWITH YOUR ANNUAL SUBSCRIPTION
Vanessa M.
Start Your FREE Trial Today!
Visit aapc.com/coder todayor call 800-626-2633
Free 14 Day Trial
HBM-April-2016-AAPC-Coder-FullPage.indd 1 2/25/2016 2:54:44 PM
16 Healthcare Business Monthly
■ ADDED EDGEBy Michelle A. Dick
Search Online for Healthcare Business Monthly articles Looking for guidance on a particular topic you remember seeing in our magazine? Here’s how to find it on the Web.
Whether you’re stuck on a particular code, modifier, or bundling rules, or have lim-
ited resources to find guidance unique to your specialty, chances are the answers you seek are somewhere in Healthcare Business Monthly’s archives. AAPC makes it easy for you to find the article you’re looking for on-line.
It’s at Your FingertipsMany times members contact us, asking:
• “I remember reading an article in Healthcare Business Monthly magazine about a year ago with guidance on code … Can you email me the article?” or
• “Do you have information on interventional radiology? I think I saw guidance in a past issue, and I’d like to use it for a presentation handout.”
In fact, all Healthcare Business Monthly articles are on the AAPC website in the News & Blog section, and you can search through them using keywords.
For example, you remember recently seeing guidance on percutaneous vertebroplasty CPT® code 22510, but can’t remember what article or month it appeared in the magazine. Here’s how to find the article:
• Log on to AAPC’s website using your user name and password.
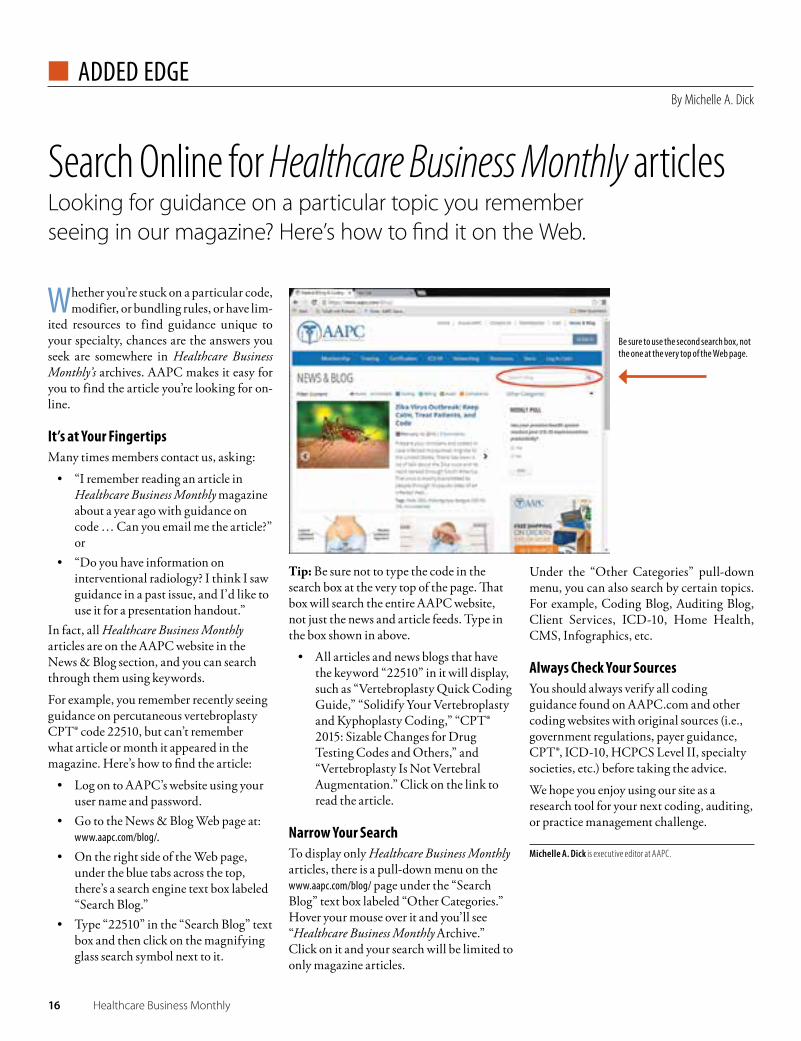
• Go to the News & Blog Web page at: www.aapc.com/blog/.
• On the right side of the Web page, under the blue tabs across the top, there’s a search engine text box labeled “Search Blog.”
• Type “22510” in the “Search Blog” text box and then click on the magnifying glass search symbol next to it.
Tip: Be sure not to type the code in the search box at the very top of the page. That box will search the entire AAPC website, not just the news and article feeds. Type in the box shown in above.
• All articles and news blogs that have the keyword “22510” in it will display, such as “Vertebroplasty Quick Coding Guide,” “Solidify Your Vertebroplasty and Kyphoplasty Coding,” “CPT® 2015: Sizable Changes for Drug Testing Codes and Others,” and “Vertebroplasty Is Not Vertebral Augmentation.” Click on the link to read the article.
Narrow Your SearchTo display only Healthcare Business Monthly articles, there is a pull-down menu on the www.aapc.com/blog/ page under the “Search Blog” text box labeled “Other Categories.” Hover your mouse over it and you’ll see “Healthcare Business Monthly Archive.” Click on it and your search will be limited to only magazine articles.
Under the “Other Categories” pull-down menu, you can also search by certain topics. For example, Coding Blog, Auditing Blog, Client Services, ICD-10, Home Health, CMS, Infographics, etc.
Always Check Your SourcesYou should always verify all coding guidance found on AAPC.com and other coding websites with original sources (i.e., government regulations, payer guidance, CPT®, ICD-10, HCPCS Level II, specialty societies, etc.) before taking the advice.
We hope you enjoy using our site as a research tool for your next coding, auditing, or practice management challenge.
Michelle A. Dick is executive editor at AAPC.
Be sure to use the second search box, not the one at the very top of the Web page.

It’s as easy as
Access Your AAPC Passport Savings Today!
○ Visit aapc.com/passport to register for your Passport number. You’ll need the unique AAPC code: ATBOHC15 to register. Your Passport number will be emailed to you.
○ Download the Passport mobile app by searching for “Passport Mobile” in your phone’s marketplace.
○ Enter your Passport number and start saving!
In addition to the mobile app, you can view participating savings byvisiting https://aapc.passportcorporate.com
1 Register at aapc.com/passport
2 Download the Passport mobile app
3 Login and save!
It’s as easy as
Access Your AAPC Passport Savings Today!
○ Visit aapc.com/passport to register for your Passport number. You’ll need the unique AAPC code: ATBOHC15 to register. Your Passport number will be emailed to you.
○ Download the Passport mobile app by searching for “Passport Mobile” in your phone’s marketplace.
○ Enter your Passport number and start saving!
In addition to the mobile app, you can view participating savings byvisiting https://aapc.passportcorporate.com
1 Register at aapc.com/passport
2 Download the Passport mobile app
3 Login and save!
It’s as easy as
Access Your AAPC Passport Savings Today!
○ Visit aapc.com/passport to register for your Passport number. You’ll need the unique AAPC code: ATBOHC15 to register. Your Passport number will be emailed to you.
○ Download the Passport mobile app by searching for “Passport Mobile” in your phone’s marketplace.
○ Enter your Passport number and start saving!
In addition to the mobile app, you can view participating savings byvisiting https://aapc.passportcorporate.com
1 Register at aapc.com/passport
2 Download the Passport mobile app
3 Login and save!
It’s as easy as
Access Your AAPC Passport Savings Today!
○ Visit aapc.com/passport to register for your Passport number. You’ll need the unique AAPC code: ATBOHC15 to register. Your Passport number will be emailed to you.
○ Download the Passport mobile app by searching for “Passport Mobile” in your phone’s marketplace.
○ Enter your Passport number and start saving!
In addition to the mobile app, you can view participating savings byvisiting https://aapc.passportcorporate.com
1 Register at aapc.com/passport
2 Download the Passport mobile app
3 Login and save!

18 Healthcare Business Monthly
Within the Surgery section of CPT®, the new year brings just two new Integumentary codes, and deletes a single Musculoskele-
tal code. Minor changes such as these are easy to overlook, but cost-ly to ignore.
Integumentary UpdatesFiducial markers serve as radiologic landmarks. Using imaging guid-ance, each marker is placed in or near a tumor and becomes the “tar-get” to facilitate precise delivery of radiation treatments. CPT® adds two codes to describe placement of these devices:
10035 Placement of soft tissue localization device(s) (eg, clip, metallic pellet, wire/needle, radioactive seeds), percutaneous, including imaging guidance; first lesion
+10036 each additional lesion (List separately in addition to code for primary procedure)
Report 10035 and 10036 per lesion, not per marker (several markers may be placed per lesion). Claim 10035 for placement of soft tissue markers at an initial lesion and +10036 for each additional lesion tar-geted beyond the first.The American Medical Association’s (AMA) CPT® Changes 2016: An Insider’s View provides an example of proper application for 10035:
A 62-year-old female presents with previously biopsied left axillary lymph node metastases secondary to invasive ductal breast carcinoma. She is now referred for neoadjuvant che-motherapy. Marking of the positive lymph node is requested prior to the initiation of neoadjuvant chemotherapy.
Note that CPT® includes several codes that specifically describe placement of localization devices in the breast, either with (19081-19086) or without (19281-19288) biopsy. CPT® Changes 2016 clar-ifies, “10035 and 10036 have been established to capture marker placements into areas such as the axilla and/or groin tissue.” Do not report 10035/10036 if 19081-19086 or 19281-19288 better describe the location of the marker.Per CPT® Assistant (May 2015):
To report bilateral image-guided breast biopsies, report code 19081, 19083, or 19085 [depending on the type of imaging used; e.g., stereotactic, ultrasound, or MRI] for the initial biopsy. The contralateral image-guided breast
By John Verhovshek, MA, CPC
■ CODING/BILLING
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
Examine Integumentary and Musculoskeletal Coding ChangesOverlooking minor changes can be a costly mistake.
istock.com/kot63
www.aapc.com April 2016 19
Integumentary/MusculoskeletalCODING/BILLING
To discuss this article or topic, go to www.aapc.com
biopsy and each additional image-guided breast biopsy are then reported with code 19082, 19084, or 19086. Similarly, to report bilateral marker placement, report code 19281, 19283, or 19285 [again, depending on the type of imaging used] for the initial marker placement. The contralateral and each additional breast image-guided marker placement are then reported with code 19282, 19284, or 19286.
Marker placement includes imaging guidance. Do not separately re-port:
76942 Ultrasonic guidance for needle placement (eg, biopsy, aspiration, injection, localization device), imag-ing supervision and interpretation
77002 Fluoroscopic guidance for needle placement (eg, biopsy, aspiration, injection, localization device)
77012 Computed tomography guidance for needle placement (eg, biopsy, aspiration, injection, localization device), radiological supervision and interpretation
77021 Magnetic resonance guidance for needle placement (eg, for biopsy, needle aspiration, injection, or placement of local-ization device) radiological supervision and interpretation
There are no guideline or parenthetical instruction revisions in the Integumen-tary chapter for 2016.
Open Treatment of Rib Fracture Is No Longer SupportedCode 21805, which previously described open treatment of rib fracture without fixation, is deleted for 2016 as an “obsolete service.” CPT® Changes 2016 explains, “In current practice, when an injured rib is treated in an open fashion, it is either resected or treated with some form of internal fixation. Because existing codes for open rib fixation and codes for rib excision (21600) may be used to identify open rib treatments, code 21805 has been deleted without replacement …”Instruction in the CPT® codebook tells us to report 21899 Unlisted procedure, neck or thorax for external rib fixation. CPT® further directs us to report an evaluation and management (E/M) service for closed treatment of an uncomplicated rib frac-ture (e.g., the fracture is reduced without surgical intervention). Turn to 21811-21813 for open (surgical) treatment of rib fracture(s) with internal fixation (the use of plates, screws, nails, and wires to stabilize the rib fracture).There are no guideline or parenthetical instruction revisions in the Musculoskel-etal chapter for 2016.
John Verhovshek, MA, CPC, is managing editor at AAPC and a member of the Hendersonville-Asheville, N.C., local chapter.
Code 21805, which previously described open treatment of rib
fracture without fixation, is deleted for 2016 as an “obsolete service.”
istock.com//elnur

20 Healthcare Business Monthly
By Sheri Poe Bernard, CPC, COC, CPC-I, CCS-P
■ CODING/BILLING
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
Coder’s Voice
CMS EHR Toolkit Gives a Glimpse into Potential Compliance Issues
The toolkit clarifies risks and provides guidance, but more can be done to address software and user pitfalls.
Without any fanfare, the Centers for Medicare & Medicaid Servic-es (CMS) last year published its Electronic Health Records Toolkit, offering coders, facilities, and providers a glimpse of the regulatory risks that CMS assigns to improper EHR use. Anyone with an EHR who hasn’t reviewed the CMS documents should access the Toolkit and distribute all or parts of it to providers, coders, and legal coun-sel, as appropriate. Although the Toolkit falls short of answering many questions regard-ing documentation and coding compliance, it gives a glimpse into what CMS considers the important regulatory issues associated with electronic records, and provides some rudimentary guidance.
istoc
k.com
/pan
dpsto
ck

www.aapc.com April 2016 21
CMS ToolkitCODING/BILLING
For example, the Toolkit file, “Ensuring Proper Use of Electronic Health Record Features and Capabilities: A Decision Table,” states these best practices:
… providers must recognize each encounter as a stand-alone record, and ensure the documentation for that encounter reflects the level of service actually provided.
It further recommends creation of an internal policy, in which: … providers should weigh efficiency against the potential for inaccurate, fraudulent, or unmanageable documentation.
Regarding authorship of an EHR entry, the Toolkit advises:Each entry not solely authored by the user must be validated in a manner similar to bibliographic notations and include the name, date, time, and source of the data. This can be satisfied by system software design that routinely provides validation.
Documents in the CMS Electronic Health Records Toolkit in-clude:
• Program Integrity Issues in Electronic Health Records: An Overview
• Resource Handout Resources for Program Integrity in Electronic Health Records
• Detecting and Responding to Fraud, Waste, and Abuse Associated With the Use of Electronic Health Records Booklist
• Preparing for and Responding to Audits of Electronic Health Records Checklist
• Detecting and Investigating Unauthorized Access to Electronic Health Records – A Case Study
• Compliance Checklist for Electronic Health Records• A Compliance Program for Electronic Health Records Fact
Sheet• Ensuring Proper Use of Electronic Health Record Features
and Capabilities: A Decision Table• Documentation Integrity in Electronic Health Records • Conducting Internal Monitoring and Auditing – Job Aid• Manual Review of Electronic Health Records – Job Aid
CMS Hasn’t Defined Clinical Documentation ExpectationsCMS became a key player in the EHR arena in 2009, when the federal government enacted the Health Information Technolo-gy for Economic and Clinical Health (HITECH) Act as part of the American Recovery and Reinvestment Act. HITECH was de-signed to stimulate adoption of EHRs capable of advancements in patient care quality, including e-prescribing and interoperabili-ty. Incentives of up to $44,000 per provider were offered for time-ly implementation of EHRs, along with a small penalty of approx-imately $500 per year for Medicare-participating providers who failed to implement compliant EHR systems within the CMS timeline.The Office of the National Coordinator for Health Information Technology (ONC) developed an EHR certification program to limit risks to providers and facilities shopping for EHRs, and to en-sure providers receiving the incentive purchase “legitimate” EHRs. The ONC certification covers issues identified by the U.S. De-partment of Health and Human Services (HHS) as critical to na-tional EHR success, mostly involving format structure that is easi-ly transmitted and retrieved, but that is also secure and private and has “meaningful use.”These certification programs were in place when EHR purchases under HITECH began, but it’s important to understand that the EHR “certification” criteria predominantly address administrative and information technology-related content. Some clinical issues were included when they satisfied HHS initiatives such as perfor-mance measures and e-prescribing; however, certification failed to
Although CMS waited six years after HITECH to publish its first EHR guidance, the CMS Toolkit remains fuzzy in its vision regarding clinical documentation and coding issues
relating to EHRs.

22 Healthcare Business Monthly
CMS ToolkitCO
DING
/BIL
LING
address non-compliant, day-to-day coding and clinical documen-tation features in EHRs, which focused on time-saving macros (of-ten mislabeled as templates) and quick-pick lists of codes. Certifi-cation had little to do with clinical documentation excellence or coding accuracy and compliance; some clinical and coding advo-cates are hopeful that the Toolkit will fix some of that deficiency. Although CMS waited six years after HITECH to publish its first EHR guidance, the CMS Toolkit remains fuzzy in its vi-sion regarding clinical documentation and coding issues relating to EHRs. For example, with the EHR feature called “populating by default,” a review of systems (ROS) or physical exam is already filled out for the provider for a new date of service. The form shows all systems are normal. The provider changes only the systems hav-ing abnormalities in the review or exam. The problem with “populating by default” is that it reports work the provider may not have performed because it assumes all body systems were reviewed and a complete physical exam was per-formed. This plays havoc with evaluation and management (E/M) leveling.
Although stating that populating by default may result in the re-porting of services that were not delivered, the Toolkit falls short of outlawing “population by default;” instead, saying the provid-er should verify the validity of auto-populated information. It of-fers no best practices solution for populating by default, although a simple best practice might be to turn off this function in the EHR.
EHR Problem Areas to WatchIn some instances, in “Ensuring Proper Use of Electronic Health Record Features and Capabilities: A Decision Table,” CMS states in the “best practices” field that there are none to report at this time. It’s not known whether we can look to CMS for more detailed and helpful guidance in the future. Many providers and coders to-day cite degradation of the clinical record as a result of templates, micros, macros, and copy/paste, and are looking for a fix. “The medical record is becoming so large and unwieldy as to be in-decipherable,” Steven J. Stack, MD, chair of the American Medi-cal Association (AMA), said in an address to CMS in 2013. “CMS should provide clear and direct guidance to physicians concerning the permissible use of EHR clinical documentation for the purpos-es of coding and billing.” EHR improvement aligns with CMS goals, too. The Evaluation and Management Services Guide issued by CMS states:
Clear and concise medical record documentation is critical to providing patients with quality care and is required in order for providers to receive accurate and timely payment for furnished services. Medical records
Many providers and coders today cite degradation of the clinical record as a result of templates, micros, macros, and copy/paste, and are looking for a fix.
Top EHR MisconceptionsYou can improve your income with electronic health records (EHRs).Vendors may promise EHRs provide an easy way to cut costs by reducing the number of employees needed in a practice, and increase income by improving provider productivity. Although the need for file clerks may be reduced with EHRs, the number of coders, schedulers, and other office personnel will likely remain steady, or grow. Increased productivity may come with time, but to date this either hasn’t panned out in the short term for most practices, or has resulted from non-compliant up-coding.
What EHRs should provide is enhanced levels of patient care, easier use of some mandated programs, increased efficiency in compliant documentation and coding practices, and safe-guards for patient health.
Automated E/M levelers in EHRs save time and ensure optimal coding levels.Some EHRs will automatically calculate the E/M level for an office visit, but because issues of medical necessity and failure to require qualitative features in the history of present illness; review of systems; past, family, and social history; physical exam; and clinical assessment, the EHR coding is unlikely to fare well in an audit.
You’re stuck with the features in an EHR.Many of the documentation features within an EHR can be edited by your information technology team or the vendor. If a feature is being misused or is simply one that you suspect may not be compliant, modify the system. EHRs are modifi-able. Vendors may require a significant fee for modifications.
All features within a government certified EHR are acceptable to all payers.Many EHR features raise compliance questions. The U.S. Department of Health and Human Services sent a letter to U.S. hospitals in September 2012 stating that the cut-and-paste feature of some EHRs “risks medical errors as well as overpayments,” and said, “CMS has the authority to address inappropriate increases in coding intensity in its payment rules and CMS will consider future payment reductions as warranted … We will continue to escalate our efforts to prevent fraud.”
Just because a feature is available in a certified EHR does not make it compliant with payer rules. Have your compliance department review the documentation and coding per-formed through your EHR.

www.aapc.com April 2016 23
CMS ToolkitCODING/BILLING
chronologically report the care a patient received and are used to record pertinent facts, findings and observations about the patient’s health history. Medical record documentation assists physicians and other health care professionals in evaluating and planning the patient’s immediate treatment and monitoring the patient’s health care over time.
Stephen Levinson, MD, CHCA, author of AMA publications Practical E/M and Practical EHR, identifies five intrinsically flawed design and functionality features that are prevalent in most current EHRs. These flaws, according to Levinson, are capable of disrupt-ing both compliance and physicians’ medical diagnostic process:
1. Failure to consider medical necessity (which Medicare defines as “the overarching criterion for payment”) into guidance for appropriate levels of care, documentation, and code selection. According to the AMA’s CPT guidelines for E/M, considering (and documenting) the nature of the presenting problem(s) pro-vides confirmation and support for medical necessity.
2. Failure to guide and require documentation of the qualitative (i.e., individualized descriptive) aspects of care as defined in 1997 Documentation Guidelines.
Required qualitative data includes, for: à Chief compliant: “stated in the patient’s own words”
(rather than a forwarded copy of previously entered diagnosis);
à HPI: the “chronological description” of the course of the patient’s illness;
à PFHS and ROS: “supplementing” with pertinent positive and negative responses to inquiries about details of the positive responses to questions in these history areas;
à PE: “specific abnormal and relevant negative findings”; and à Clinical assessment: patient-specific and visit-specific
descriptions of diagnoses (e.g., location, severity, extent, and status relevant to previous encounters).
3. Non-compliant coding engines (based on the non-sanctioned, incomplete, and non-compliant “scoring sheet” introduced as a coding short cut in 1995.
4. Use of data entry shortcuts that create non-compliant “cloned” pseudo documentation through automated function.
5. Use of data entry shortcuts that replace documentation of clin-ical assessment (i.e., “ impressions”) with ICD billing language and codes, a process that limits clinical descriptions and elimi-nates documentation of differential diagnoses.
These EHR documentation problem areas should be identified and addressed because they are subject to the financial and emotion-al devastation of negative Medicare or Office of Inspector Gener-al (OIG) audits.Levinson also advises, “It is important to distinguish between EHR utilization of (compliant) templates vs. (non-compliant) macros.”Templates are pre-loaded frameworks that include history ques-tions to be asked with individualized documentation of the re-sponses or exam elements to be examined with individualized doc-umentation of the findings.
Providers can save time and money using EHR coding pick lists or coding prompts.EHRs include current codes from the major code sets, and providers can use these lists to code encounters and either submit these codes directly or have them reviewed by coding/billing staff before submission. But nearly all systems lack code instructions, guidelines, and information from Coding Clinic or CPT® Assistant. Most providers are not certi-fied coders and do not have the breadth of understanding to select codes compliantly. Truncated code descriptions in some EHRs also contribute to coding errors.
Certified coders should be excluded from EHR selection teams.Some vendors exclude coding staff from EHR selection, and suggest that certified coders are not qualified or interested. Neither is true. Coders can help providers and office manag-
ers understand the coding and compliance implications of EHR features. Their input is crucial to successful coding fol-lowing implementation.
EHR templates (i.e., macros) provide more detailed documentation.EHRs certainly provide more documentation, but not neces-sarily more detail. EHR templates catalog body systems and most allow the provider to select a button stating the system is normal or abnormal, or yes or no. Free text, where provid-ers can enrich the record by describing qualitative details, is limited in most EHRs. Instead of stating “yes” to shortness of breath (SOB), free text allows the provider to state, “SOB on exertion. Says he can no longer negotiate stairs at home, and became dyspneic in relating this to me. O2 on room air was 87.” It is the qualitative information within the health record that provides the most information to clinicians and coders.
Purchasing a federally certified EHR ensures it will be completely compliant.Certified EHRs are equipped with software that makes them compliant with portability, privacy, and security require-ments, as well as some clinical tools including tracking preventive care and performance measures and the ability to detect and advise about prescriptions that could cause allergic or drug interactions. Certified EHRs are not equipped to contribute in any meaningful way to clinical documenta-tion or coding compliance, and most do not follow the 1997 Documentation Guidelines for Evaluation and Management Services, the CMS policy on medical necessity as overarching criteria for E/M and payment, or avoidance of cloning prac-tices and templates as outlined in documents published by CMS beginning in 1999 and continuing to 2015.

24 Healthcare Business Monthly
CMS ToolkitCO
DING
/BIL
LING
To discuss this article or topic, go to www.aapc.com
ResourcesCMS, Electronic Health Records Toolkit, “Program Integrity: Electronic Health Records” files: www.cms.gov/Medicare-Medicaid-Coordination/Fraud-Prevention/Medicaid-Integrity-Education/electronic-health-records.html
CMS, Ensuring Proper Use of Electronic Health Record Features and Capabilities: A Decision Table, Table 1: www.cms.gov/Medicare-Medicaid-Coordination/Fraud-Prevention/Medicaid-Integrity-Education/Downloads/ehr-decision-table.pdf
CMS, Medicare Learning Network®, Evaluation and Management Services Guide: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/eval_mgmt_serv_guide-ICN006764.pdf
“Macros include the templated questions, plus pre-loaded gener-ic negative history responses and normal exam findings … As au-tomatic or single-click tools, the macro loads a completed clini-cal document before the patient has even been evaluated,” Levin-son said.Levinson also emphasizes that coders and auditors require com-prehensive and compliant tools that consider medical necessi-ty when reviewing EHR documentation and coding. The com-monly-employed, non-compliant scoring sheet not only offers in-adequate and incorrect E/M coding in paper records, but it com-pletely lacks tools to address the aforementioned five deficiencies of EHRs. Practical E/M’s compliant audit forms for paper charts were published as part of a CD accompanying the second edition of Practical E/M in 2008. These forms were subsequently enhanced to consider all the above EHR danger areas; PDFs of these coding and audit charts were made available through AAPC in conjunc-tion with Levinson’s 2013 AAPC Workshop, Advanced E/M Cod-ing for EHRs (www.aapc.com/workshops/em-coding-ehr.aspx).
Sheri Poe Bernard, CPC, COC, CPC-I, CCS-P, is a coding education and risk adjustment consultant and author of the AMA publication, Netter’s Atlas of Surgical Anatomy for CPT® Coding. Her 20-year career in coding and reimbursement includes developing coding curric-ulum and references for AAPC, the AMA, DecisionHealth, Elsevier, Optum360, and Staywell. Bernard is a member of the Salt Lake City, Utah, local chapter.
These EHR documentation problem areas should be identified and addressed because they are subject to the financial and emotional devastation of negative Medicare or Office of Inspector General (OIG) audits.
istoc
k.com
/MKu
rtbas
26 Healthcare Business Monthly
By Judy A. Wilson, CPC, CPCO, CPPM, CPB, CPC-P, COC, CPC-I, CANPC
■ CODING/BILLING
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
Financial problems can be directly related to billing errors that could have been avoided simply by reviewing information. Errors can
cause delayed payment, costly fines, and lost revenue if not caught. Let’s take a look at a few of the top billing errors, and discuss how to prevent them.
Verify InsuranceThe number one reason, by far, for denied claims is failure to verify insurance. Some of the common denials associated with not verify-ing insurance information are:1. Subscriber is not eligible on the date of service.2. Services are not covered or maximum benefits have been met.3. Services were not authorized or authorization is required.When you see these denials, I am sure you ask, “Why didn’t some-one take care of this before we filed the claim?” With people chang-ing jobs and moving more often, insurance information can change at any time. For this reason alone, your office should verify a patient’s insurance eligibility at every visit.
For example, you might establish parameters in your billing practice disallowing a claim that requires a pre-authorization to be filed with-out the authorization number. At the very least, a person should call carriers on every patient prior to a procedure to verify eligibility and the limits of the patient’s benefits. It takes a little longer, but it’s well worth the extra time on the front end. Remember: Each time you start over with a claim, you are losing money and filing inaccurate claims.
Be Sure Your Information Is CompleteAnother common error is inaccurate or incomplete patient informa-tion. Even the smallest error in a patient’s name can get a claim de-nied. This is why your front desk person is a valuable employee: He or she can help to reduce denials by checking to make sure the patient’s name is spelled correctly and that you have the right date of birth and sex (for starters). The front desk person can also verify if the policy is valid and if you need a group number or authorization number prior to processing the claim.
Avoid three frequent billing blunders to keep revenue streams flowing.
Conquer Common BILLING ERRORS
istoc
k.com
/dina
2001

www.aapc.com April 2016 27
Billing ErrorsCODING/BILLING
Be sure authorizations obtained are for procedures performed, and procedure codes and diagnostic codes reflect as much. This is anoth-er common billing error that is easily corrected by taking the time to look over the claim before processing. Always use the most current coding books. Some offices may think that it’s too expensive to get new books every year, but claim denials can be much more costly. Criminal allegations may arise if you use procedure and diagnosis codes incorrectly. If the provider is still using handwritten charts and their writing is illegible, you cannot transcribe what you think the documentation says. If it’s incorrect, you now have a false claim. This is where the electronic health record has helped to reduce billing errors.
Avoid Duplicate BillingLastly, let’s look at duplicated billing, as this is a very common bill-ing error, as well. Duplicate billing for the same procedure or treatments is considered fraud, and a practice can be fined for duplicate billing. If a claim is
not paid within a timely matter, never “just” rebill the claim. Take the time to contact the insurance carrier to check on the status of the claim. Most carriers allow you to check claim status online, but the alternative is to call them.All systems now should have a way to check how long a claim has been outstanding. Your office insurance representative should fol-low up on all claims aged over 30 days.To reiterate: Never simply re-bill a claim that has not been paid. Re-billing can lead to another denial for duplicate billing, or worse du-plicate payment, which may subject your practice to fraud.To avoid these common errors, take time to verify and input patient information correctly, and check your procedure and diagnosis cod-ing prior to billing. These basic steps will keep your revenue flowing. Plus, it’s always easier to do it right the first time.
Judy A. Wilson, CPC, COC, CPCO, CPPM, CPC-P, CPB, CPC-I, CANPC, has been a medical coder/biller for more than 35 years. For the past 25 years, she has been the business adminis-trator for Anesthesia Specialists, a group of nine cardiac anesthesiologists who practice at Sentara Heart Hospital. Wilson has served on the AAPC Chapter Association board of directors since 2010. She is also on the board of directors of Bryant & Stratton College in Virginia Beach,
Va. Wilson is a PMCC instructor and teaches classes in the Tidewater area. She serves on the National Advisory Board for American Academy of Billers for AMBA, has presented at several AAPC regional and national confer-ences, and is a member of the Chesapeake, Va., local chapter.
Slow down and take extra time to verify and input patient information correctly, and check your procedure
and diagnosis coding prior to billing.

28 Healthcare Business Monthly
By David Zielske, MD, CIRCC, CCVTC, COC, CCC, CCS, RCC
■ CODING/BILLING
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
For 2016, the biggest CPT® coding changes affecting intervention-al radiology occur within the subspecialties of urinary, biliary, and
neurologic intervention. In March, we covered urinary intervention. This month, we’ll discuss the major changes in percutaneous biliary interventional coding. Next month, we’ll cover CPT® updates for percutaneous neurologic intervention.
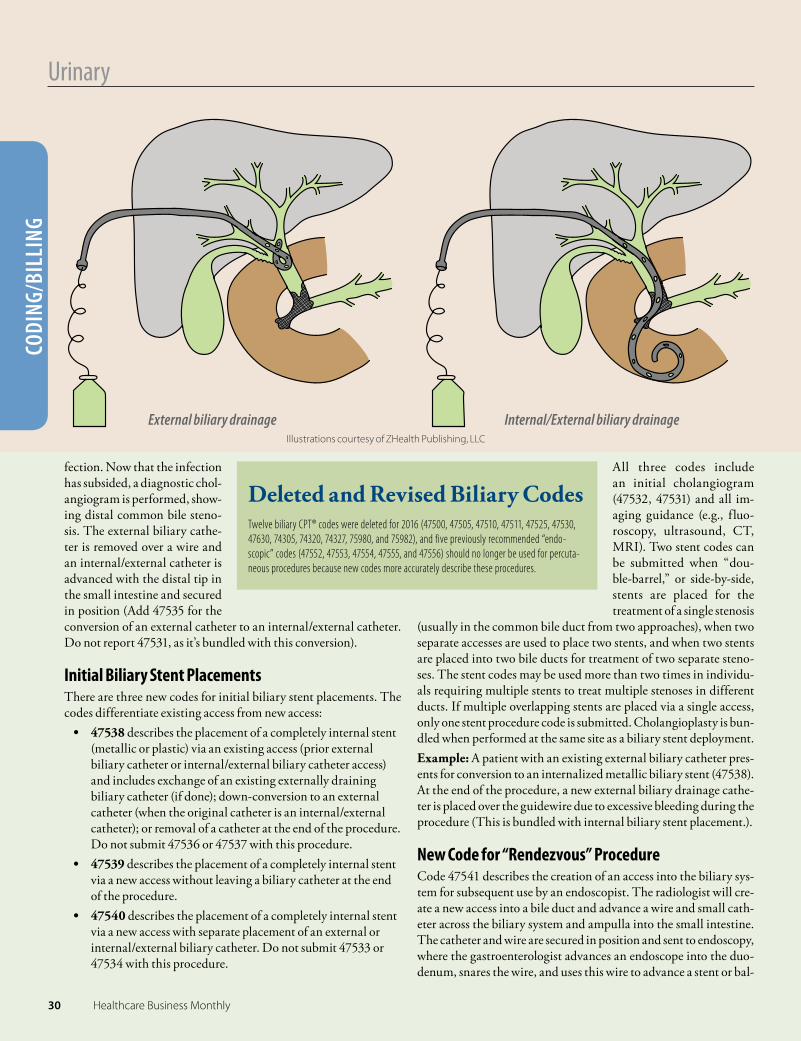
Anatomically SpeakingThe biliary system is divided into right- and left-sided bile ducts; how-ever, these ducts divide further into multiple smaller branches that may be individually accessed and drained, depending on the pathol-ogy treated (e.g., Klatskin tumor is a cholangiocarcinoma that has in-volved and caused bifurcation occlusions of the common bile duct. As
it grows further, it may compromise additional ducts requiring three or four catheters for successful drainage). Terminology for biliary procedures refers to either “catheters” (which are externally accessi-ble, such as an internal/external biliary drainage catheter) or “stents” (which are not externally accessible, such as a metallic biliary stent).
New Codes for 2016There are 14 new biliary intervention codes for 2016 (see “New Bil-iary Intervention Codes for 2016 on page 29”). These codes include both the surgical and supervision and interpretation (S&I) compo-nents of the procedure. As well, all of the new codes bundle the use of imaging guidance, including fluoroscopy, ultrasound, computed to-mography (CT), and magnetic resonance imaging (MRI).
CPT® guidelines instruct us to code separately for each catheter placement, replacement, conversion, or removal. Catheter procedure codes are based on each individual catheter via a separate access site.Here’s a rundown of how to apply the new codes.
CholangiographyCholangiography (47532 and 47531) is performed to evaluate the biliary system for patency, stones, stric-tures, malignancy, and leaks. These abnormalities can occur anywhere in the collecting system, but most often are between the ampullary sphincter of the distal common bile duct and the bifurcation of the more proximal common bile duct.The cholangiogram may be performed via a new ac-cess (placing a needle or catheter through the right side or anterior abdominal wall into the right or left bile ducts respectively) or via a pre-existing cathe-ter, usually an existing biliary catheter. Contrast is injected and imaging is performed and interpret-ed. The procedure is reported with 47532 when performed via a new access, or with 47531 when performed via an existing access. Because imaging guidance is performed, be sure the ultrasound, CT, or MRI tech does not charge a guidance code when the access uses one of these imaging guidance mo-dalities.
CPT® 2016:Percutaneous Biliary Interventional CodingPart 2: New codes change the way you should report these procedures.
Biliary obstruction at the distal common bile duct
Illustrations courtesy of ZHealth Publishing, LLC
28 Healthcare Business Monthly

www.aapc.com April 2016 29
UrinaryCODING/BILLING
Cholangiography is bundled with the new external biliary catheter, internal/external catheter, and biliary stent placement codes. The cholangiogram codes may be used as a base code for +47542, +47543, and +47544, but only if a catheter is not placed, replaced, or converted. Example: A patient has an existing external biliary drainage catheter. Diagnostic cholangiogram is performed (47531), demonstrating a distal common bile duct stenosis. Cholangio-plasty is performed (+47542). No tubes are left in place at the end of the procedure.The following codes involve placement of an external or inter-nal/external biliary drainage catheter:• 47533 describes the initial placement of a percutaneous
external biliary drainage catheter via a new access, and includes diagnostic imaging 47532. Submit 47533 once for each external biliary drainage catheter placed via a new access at the same session.
• 47534 describes the initial placement of a percutaneous internal/external biliary drainage catheter via a new access, and includes diagnostic imaging 47532. Submit 47534 once for each internal/external biliary drainage catheter placed via a new access at the same session.
• 47535 describes the conversion of an existing external biliary drainage catheter to an internal/external catheter (removal of the external catheter and placement of the internal/external catheter over a wire, which requires crossing of the distal common bile duct into the small intestine), and includes diagnostic imaging. Submit 47535 once for each biliary catheter conversion at the same session.
• 47536 describes the exchange of an existing external biliary drainage catheter/external biliary drainage catheter or exchange of an existing internal/external catheter for a lesser external catheter, and includes diagnostic imaging. Submit 47536 for each catheter exchanged at the same session.
• 47537 describes the removal of an existing external or internal/external biliary drainage catheter, and includes diagnostic imaging. Submit 47537 once for each catheter removed at the same session.
Example: The patient recently underwent external biliary drainage catheter placement for biliary obstruction and in-
New Biliary Intervention Codes for 2016
Diagnostic cholangiography 47531 Injection procedure for cholangiography, percutaneous, complete diagnostic procedure including im-
aging guidance (eg, ultrasound and/or fluoroscopy) and all associated radiological supervision and in-terpretation; existing access
47532 new access (eg, percutaneous transhepatic cholangiogram)
Percutaneous biliary drainage catheters 47533 Placement of biliary drainage catheter, percutaneous, including diagnostic cholangiography when per-
formed, imaging guidance (eg, ultrasound and/or fluoroscopy), and all associated radiological super-vision and interpretation; external
47534 internal-external
47535 Conversion of external biliary drainage catheter to internal-external biliary drainage catheter, percutaneous, including diagnostic cholangiography when performed, imaging guidance (eg, fluoroscopy), and all associated radiological supervision and interpretation
47536 Exchange of biliary drainage catheter (eg, external, internal-external, or conversion of internal-external to external only), percutaneous, including diagnostic cholangiography when performed, imaging guid-ance (eg, fluoroscopy), and all associated radiological supervision and interpretation
47537 Removal of biliary drainage catheter, percutaneous, requiring fluoroscopic guidance (eg, with concur-rent indwelling biliary stents), including diagnostic cholangiography when performed, imaging guid-ance (eg, fluoroscopy), and all associated radiological supervision and interpretation
Percutaneous biliary stent placements 47538 Placement of stent(s) into a bile duct, percutaneous, including diagnostic cholangiography, imag-
ing guidance (eg, fluoroscopy and/or ultrasound), balloon dilation, catheter exchange(s) and cathe-ter removal(s) when performed, and all associated radiological supervision and interpretation, each stent; existing access
47539 new access, without placement of separate biliary drainage catheter
47540 new access, with placement of separate biliary drainage catheter (eg, external or internal-external)
Three add-on procedures: cholangioplasty, biopsy, and stone extraction+47542 Balloon dilation of biliary duct(s) or of ampulla (sphincteroplasty), percutaneous, including imaging
guidance (eg, fluoroscopy), and all associated radiological supervision and interpretation, each duct (List separately in addition to code for primary procedure)
+47543 Endoluminal biopsy(ies) of biliary tree, percutaneous, any method(s) (eg, brush, forceps, and/or needle), including imaging guidance (eg, fluoroscopy), and all associated radiological supervision and interpre-tation, single or multiple (List separately in addition to code for primary procedure)
+47544 Removal of calculi/debris from biliary duct(s) and/or gallbladder, percutaneous, including destruc-tion of calculi by any method (eg, mechanical, electrohydraulic, lithotripsy) when performed, imaging guidance (eg, fluoroscopy), and all associated radiological supervision and interpretation (List sepa-rately in addition to code for primary procedure)
Access placement to assist with endoscopic biliary procedure47541 Placement of access through the biliary tree and into small bowel to assist with an endoscopic biliary
procedure (eg, rendezvous procedure), percutaneous, including diagnostic cholangiography when performed, imaging guidance (eg, ultrasound and/or fluoroscopy), and all associated radiological su-pervision and interpretation, new access
www.aapc.com April 2016 29
30 Healthcare Business Monthly
UrinaryCO
DING
/BIL
LING
fection. Now that the infection has subsided, a diagnostic chol-angiogram is performed, show-ing distal common bile steno-sis. The external biliary cathe-ter is removed over a wire and an internal/external catheter is advanced with the distal tip in the small intestine and secured in position (Add 47535 for the conversion of an external catheter to an internal/external catheter. Do not report 47531, as it’s bundled with this conversion).
Initial Biliary Stent PlacementsThere are three new codes for initial biliary stent placements. The codes differentiate existing access from new access:
• 47538 describes the placement of a completely internal stent (metallic or plastic) via an existing access (prior external biliary catheter or internal/external biliary catheter access) and includes exchange of an existing externally draining biliary catheter (if done); down-conversion to an external catheter (when the original catheter is an internal/external catheter); or removal of a catheter at the end of the procedure. Do not submit 47536 or 47537 with this procedure.
• 47539 describes the placement of a completely internal stent via a new access without leaving a biliary catheter at the end of the procedure.
• 47540 describes the placement of a completely internal stent via a new access with separate placement of an external or internal/external biliary catheter. Do not submit 47533 or 47534 with this procedure.
All three codes include an initial cholangiogram (47532, 47531) and all im-aging guidance (e.g., fluo-roscopy, ultrasound, CT, MRI). Two stent codes can be submitted when “dou-ble-barrel,” or side-by-side, stents are placed for the treatment of a single stenosis
(usually in the common bile duct from two approaches), when two separate accesses are used to place two stents, and when two stents are placed into two bile ducts for treatment of two separate steno-ses. The stent codes may be used more than two times in individu-als requiring multiple stents to treat multiple stenoses in different ducts. If multiple overlapping stents are placed via a single access, only one stent procedure code is submitted. Cholangioplasty is bun-dled when performed at the same site as a biliary stent deployment. Example: A patient with an existing external biliary catheter pres-ents for conversion to an internalized metallic biliary stent (47538). At the end of the procedure, a new external biliary drainage cathe-ter is placed over the guidewire due to excessive bleeding during the procedure (This is bundled with internal biliary stent placement.).
New Code for “Rendezvous” ProcedureCode 47541 describes the creation of an access into the biliary sys-tem for subsequent use by an endoscopist. The radiologist will cre-ate a new access into a bile duct and advance a wire and small cath-eter across the biliary system and ampulla into the small intestine. The catheter and wire are secured in position and sent to endoscopy, where the gastroenterologist advances an endoscope into the duo-denum, snares the wire, and uses this wire to advance a stent or bal-
External biliary drainage Internal/External biliary drainageIllustrations courtesy of ZHealth Publishing, LLC
Deleted and Revised Biliary CodesTwelve biliary CPT® codes were deleted for 2016 (47500, 47505, 47510, 47511, 47525, 47530, 47630, 74305, 74320, 74327, 75980, and 75982), and five previously recommended “endo-scopic” codes (47552, 47553, 47554, 47555, and 47556) should no longer be used for percuta-neous procedures because new codes more accurately describe these procedures.
30 Healthcare Business Monthly

www.aapc.com April 2016 31
To discuss this article or topic, go to www.aapc.com Urinary
CODING/BILLINGloon to complete that portion of the procedure. A cholangioplasty or stent placement by the radiologist can be submitted separately. If the radiologist leaves in a drainage catheter, 47533 or 47534 should be submitted instead of 47541. Do not submit 47541 when a pre-existing catheter is accessed to perform the rendezvous pro-cedure. When done via an existing access, submit a code describing a catheter exchange, removal, or conversion (e.g., 47535-47537).
New Add-on CodesCodes +47542, +47543, and +47544 require a base code, which can be any of the catheter placement, conversion, or exchange codes, as well as diagnostic cholangiogram codes 47532 and 47531.
• +47542 describes cholangioplasty (balloon dilation) of any bile duct for treatment of a stenosis or occlusion, and can also be used to report balloon dilation of the ampullary sphincter (sphincteroplasty) for subsequent stone extraction. Submit +47542 once per treatment site, for a maximum of two sites treated per session. If more than two separate sites are treated with balloon dila-tion, no additional codes are submitted for the additional chol-angioplasties. This may limit the number of cholangioplasties submitted in patients with sclerosing cholangitis. This limita-tion does not apply to stent placements.Cholangioplasty at the site of a stent placement during the same session is bundled and not separately coded. Because of add-on code edits, it may not be possible to submit +47542 with a biliary stent code (47538-47540), even when done in different ducts. Do not use this code when a balloon catheter is used for stone extraction.
• +47543 describes an endoluminal biopsy (brush, needle, or alligator forceps) of the biliary ductal system (common bile duct, intrahepatic bile ducts). If multiple bile ducts are biopsied, do not report additional procedure codes because all ducts biopsied are described by using this single code. Submit +47543 only once per date of service.
• +47544 describes percutaneous biliary stone extraction by any method, and includes removal of stone(s) with a basket and/or pushed through the ampulla with a balloon. Do not use this code for removal of debris or sludge, and do not use
it with an attempted procedure modifier if stone retrieval is attempted, but no stones are identified. Use this code only once per session.
A catheter placement, replacement, conversion, or removal code can additionally be submitted if done. An imaging code (47531 or 47532) can be submitted instead if the above catheter codes are not performed. Code +47544 may be used for stone extraction from the gall bladder via a cholecystostomy tube. The three add-on procedure codes vary in the number of times each code can be submitted per day, and depend on access sites/approach-es, location, and extent of the lesions treated and the specific limita-tions on the codes submitted. Example: The patient has an internal/external catheter in place via a left anterior duct approach. The patient has a known filling defect in the region of the distal common bile duct, and is here for biopsy. The catheter is removed over a guidewire and a sheath is placed up to the abnormality. A brush biopsy followed by alligator forceps bi-opsy are performed and sent for pathology (+47543). A new inter-nal/external stent is placed over the wire (exchange of biliary drain-age catheter, 47536).
Same Old Code May Be Used with New CodesPercutaneous cholecystostomy, which includes placement of a drainage catheter into the gallbladder (47490 Cholecystostomy, per-cutaneous, complete procedure, including imaging guidance, catheter placement, cholecystogram when performed, and radiological super-vision and interpretation), remains unchanged in 2016. This pro-cedure may be reported with new codes for tube check (47531), tube change (47536), tube removal (47537), and stone extraction (47544). With the new codes added in 2016, a comprehensive set of biliary codes is now available to describe almost every procedure performed in the biliary system. The opportunity for coding specificity has never been better.
David Zielske, MD, CIRCC, COC, CCVTC, CCC, CCS, RCC, or Dr. Z, is the founder and CEO of ZHealth, LLC, and ZHealth Publishing, LLC. He practiced as an interventional radiologist for 15 years and has 16 years of experience as a coding reviewer and educator. Dr. Z is Board Certified in Radiology with the Certification of Added Qualification (CAQ) in Interventional Radiology (ABR) (1995, 2005). He was on the AAPC National Advisory Board from 2005-
2009, and is a member of the Nashville, Tenn., local chapter.
With the new codes added in 2016, a comprehensive set of biliary codes is now available to describe almost
every procedure performed in the biliary system.
www.aapc.com April 2016 31

32 Healthcare Business Monthly
By Leonta (Lee) Williams, RHIT, CPC, CPCO, CCS, CCDS
■ CODING/BILLING
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
A mechanical ventilator is a device used to perform artificial res-piration on a patient whose natural ability to breathe is compro-
mised. Mechanical ventilation may be ordered for various reasons, but it is generally used to get air into lungs, expel carbon dioxide from lungs, or breathe for someone who can’t do it on their own. Mechan-ical ventilation may also be used to help someone short of breath due to a chronic lung disease. Invasive mechanical ventilation — usual-ly accomplished by endotracheal (ET) intubation or an artificial air-way, such as a tracheostomy — may be reasonable and necessary when there are clinical indicators or lab values confirming the patient can-not maintain adequate ventilation.
Look at the TimeFor billing, compliance, and reimbursement pur-poses, document the procedure appropriately, with the dates and time (in hours) of when the mechan-ical ventilation began and when it concluded. To calculate the number of hours of continuous me-chanical ventilation by ET intubation during a hos-pitalization, begin counting from the start of intu-bation; the clock stops after weaning, extubation, or patient discharge/transfer. When a patient pres-ents to the hospital already intubated, counting be-gins when the patient is admitted.
Documentation Must Support DRG Assignment
The 2016 Office of Inspector General (OIG) Work Plan includes re-view of Medicare payments for inpatient claims where the use of a ventilator was billed. There is a difference in Medicare Severity-Di-agnosis Related Group (MS-DRG) assignment and payment based on the procedure code billed. An OIG audit for 2009-2011, with a length of stay of four days or less, discovered an error rate of greater than 95 percent in mechanical ventilation billing to Medicare. A to-tal of 377 claims were reviewed and 363 of those claims showed an overpayment. To prevent overpayments, hospitals should have an internal audit sys-tem to monitor this service and validate the MS-DRG assignment. In performing an internal audit, look for supporting documentation in the medical record such as physician orders, nursing notes, respirato-ry therapy notes, operative notes, and provider progress notes.In ICD-9-CM, the procedural codes identifying continuous inva-sive mechanical ventilation are 96.70 Continuous Invasive Mechan-ical Ventilation of Unspecified Duration; 96.71 Continuous Invasive Mechanical Ventilation for Less than 96 Consecutive Hours; and 96.72 Continuous Invasive Mechanical Ventilation For 96 Consecutive Hours Or More. ICD-10-PCS requires you to be more specific:
5A1935Z Respiratory Ventilation, Less than 24 Consecutive Hours
5A1945Z Respiratory Ventilation, 24-96 Consecutive Hours
5A1955Z Respiratory Ventilation, Greater than 96 Consecutive Hours
MS-DRG May Spell TROUBLE for Mechanical Ventilation BillingCMS is looking for time to support billed services.
Remember these key points when reporting mechanical ventilation: • Calculate the duration of time in hours, not days.• Weaning time should be included in the calculation of total billable time.• The billable time for patients arriving to the hospital on ventilation begins when the
patient is admitted.• Time stops once the patient is extubated or transferred/discharged.• Ventilation support provided during a surgical procedure may be considered integral to the
procedure and not separately coded.• Ventilation support for an extended period following surgery may be coded if there is sup-
porting provider documentation as to why the service is medically necessary.
istoc
k.com
/Pau
lVint
en
www.aapc.com April 2016 33
MS-DRGCODING/BILLING
To discuss this article or topic, go to www.aapc.com
The Centers for Medicare & Medicaid Services (CMS) revised the language for several MS-DRGs related to respiratory ventilation to reflect the title change of “Greater than 96 Consecutive Hours.” For example:
MS-DRG 870 Septicemia or Severe Sepsis with Mechanical Ventilation 96+ Hours
MS-DRG 871 Septicemia or Severe Sepsis without Mechanical Ventilation 96+ Hours with MCC
MS-DRG 872 Septicemia or Severe Sepsis without Mechanical Ventilation 96+ Hours without MCC
The message here is to make sure clinicians are documenting start and stop times, as well as supporting diagnoses.
Lee Williams, RHIT, CPC, CPCO, CCS, CCDS, has over 13 years of health information manage-ment experience as a coding director, educator, trainer, and practice manager. She is the found-er and past president of the Covington, Ga., local chapter and serves on AAPC’s National Adviso-ry Board, representing Region 4.
Look for supporting documentation in the medical record such as physician orders, nursing notes, respiratory therapy
notes, operative notes, and provider progress notes.
Resources
Merck Manual, “Overview of Mechanical Ventilation,” Jesse B. Hall, MD, and Pamela J. McShane, MD2016 OIG Work Plan: https://oig.hhs.gov/reports-and-publications/workplanOIG, Medicare Payments for Inpatient Claims with Mechanical Ventilation (A-09-12-02066)AHA Coding Clinic. 2015. Update on AHA Coding Clinic for ICD-10-CM and ICD-10-PCS Part ICMS, ICD-10-CM and ICD-10-PCS MS-DRG Definitions Manual: www.cms.gov/ICD10Manual/version33-fullcode-cms/fullcode_cms/P0001.html
Check out our website for our newest course, The Where’s and When’s of ICD-10!
Continuing education. Any time. Any place. ℠
Be with the family and earn CEUs!
Need CEUs to renew your CPC®? Stay in town. At home. Use our CD courses anywhere, any time, any place. You won’t have to travel, and you can even work at home.
• From the leading provider of computer-based interactive CD courses with preapproved CEUs
• Take it at your own speed, quickly or leisurely • Just 1 course can earn as many as 18.0 CEUs • Apple® Mac support with our Cloud-CD™ option • Windows® support with CD-ROM or Cloud-CD™ • Cloud-CD™ — lower cost, immediate Web access • Add’l user licenses — great value for groups
Finish a CD in a couple of sittings, or take it a chapter a day — you choose. So visit our Web site to learn more about CEUs, the convenient way!
Our coding courses with AAPC CEUs: • The Where’s and When’s of ICD-10 (16 CEUs) • Dive Into ICD-10 (18 CEUs) • E/M from A to Z (18 CEUs) • Primary Care Primer (18 CEUs) • E/M Chart Auditing & Coding (16 CEUs) • Demystifying the Modifiers (16 CEUs) • Medical Coding Strategies: CPT® O’view (15 C’s) • Walking Through the ASC Codes (15 CEUs) • Coding with Heart — Cardiology (12 CEUs)
HealthcareBusinessOffice LLC: Toll free 800-515-3235 Email: [email protected] Web site: www.HealthcareBusinessOffice.com
(All courses with AAPC CEUs
also earn CEUs with AHIMA.
See our Web site.)

2017 CODE BOOKS ARE HERE!VIEW OUR NEW LOOK
FIRST BOOK SHIPS FREEWITH COUPON CODE “SHIPSFREE”
800-626-2633 | www.aapc.com/medical-coding-books
?

www.aapc.com April 2016 35
By Mary Pat Whaley, FACMPE, CPC
CODING/BILLING ■
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
Balance Billing: Is It Legal?Stay in line with private carrier rules and follow updated Medicare and Medicaid guidance.
Balance billing is charging the patient for any balance on their account after insurance has paid its portion. The question on everyone’s mind
is: Does the patient truly owe the balance after insurance pays?The simple answer is, if there is a contract between the insurance plan and the physician practice, the practice may collect up front from the patient:
• Co-pays• Co-insurance• Deductibles• Any amount due for services the plan does not cover
If there is no contract between the insurance plan and the physician prac-tice, the practice is not limited in what they may bill the patient.Of course, it isn’t really that simple. Knowing when you can or can’t bal-ance bill takes a bit more explanation.

36 Healthcare Business Monthly
Balance BillingCO
DING
/BIL
LING
When to Balance Bill, and When Not ToIf a physician has a contract with an insurance plan and the con-tract states (hopefully, correctly) that the patient is not responsi-ble for the deductible, co-pay, or co-insurance for a specific service, then billing the patient is illegal. Likewise, if a physician has a contract with an insurance plan and has permissibly collected the deductible, co-pay, or co-insurance, billing the patient for anything above the allowable rate is illegal. For Medicaid providers, balance billing is legal:
• If the physician does not have a contract with the insurance plan.
• If the services are non-covered services (think cosmetic surgery) by the insurance plan.
• If the patient chooses to opt-out of using their insurance and be a self-pay patient for any particular service.
Here’s the rub: Sometimes (actually, many times) the insurance company is not right. It fails to pay for things that should be paid,
and informs the patient that they have no balance. That informa-tion may be confirmed by the insurance plan when the patient calls, simply because the company is referencing its own informa-tion. Some reasons why an insurer might process the services in-correctly are:
• There is a glitch in their system.• They will not pay until the patient provides information to
determine coordination of benefits.• The patient’s enrollment or COBRA information has not
caught up in the system.• They have incorrect information about the physician’s
participation in the network.
Special Case: The Qualified Medicare BeneficiaryMedicare recently updated information related to balance billing patients who are qualified Medicare beneficiaries (QMBs).The QMB Program helps Medicare beneficiaries of modest means pay all or some of Medicare’s cost sharing amounts (i.e., premiums, de-ductibles, and co-payments). To qualify, patients must be eligible for Medicare and must meet certain income guidelines. The in-come guidelines change April 1 each year. The QMB program provides:
• Payment of Medicare Part A monthly premiums (when applicable);
• Payment of Medicare Part B monthly premiums and annual deductible; and
• Payment of co-insurance and deductible amounts for services covered under both Medicare Parts A and B.
Note: Medigap premiums are not covered by the QMB.Eligibility criteria for this program require:
• The individual to be eligible for Medicare Part A insurance (even if not currently enrolled); and
• The monthly income to be at or below 100 percent of the annual federal poverty level, which is issued annually by the U.S. Department of Health and Human Services.
Note: Individuals who are eligible for Medicare Part A, but not enrolled, may conditionally enroll in Medicare Part A at any time
Balance Billing TerminologyContracted plan: An agreement between an insurer and a physician stating the phy-sician agrees to accept a specific dollar amount for each service, regardless of what the physician actually charges for the service.
Allowable: The contracted amount the physician has agreed to accept as complete payment for a service. The allowable is made up of the portion the insurance will pay and the portion the patient must pay.
Write-off: The difference between the physician’s charge and the allowable, which may not be collected from either the insurance plan or the patient.
Accepting assignment: A physician who accepts assignment agrees to the insurance plan’s allowable and write-off amounts.
Some people equate accepting assignment with being a participating physician, but a physician can participate in Medicare and not accept assignment.
In-network: This originally meant the physician was contracted with a preferred pro-vider organization (PPO), but now often means a physician is contracted with any plan. This most often comes up when a patient is referred to an out-of-network provider for services, or when a patient undergoes a surgery or procedure in a hospital that is in-network, but the anesthesiologist, radiologist, pathologist, intensivist (critical care), hospitalist, emergency room doctor, or neonatologist is not.

www.aapc.com April 2016 37
To discuss this article or topic, go to www.aapc.com Balance Billing
CODING/BILLINGduring the year, after which they may apply for QMB to cover the cost of the Medicare Part A premium.If a patient is eligible for the QMB program, purchasing addition-al Medigap coverage for Medicare premiums, deductibles, and/or co-payments may be unnecessary. Review the benefits covered by the Medigap policy to see if the plan covers services other than the Medicare cost-sharing that may be useful to the patient.
QMB Provider Certification for Title 19The QMB program pays the 20 percent Medicare Part B co-in-surance if the service provider is certified as a Medicaid provid-er. Note, however, a provider may choose to treat only QMB pa-tients and not all Medicaid recipients. The provider may also lim-it the QMB patients he or she sees. Providers have no obligation to treat Medicaid patients, or anyone in particular (I’m asked this question a lot!).
Medicare Update on Balance BillingAccording to MLN Matters® SE1128 Revised, February 1, 2016:
Federal law bars Medicare providers from balance billing a QMB beneficiary under any circumstances … QMB is a Medicaid program for Medicare beneficiaries that exempts them from liability for Medicare cost sharing. State Medicaid programs may pay providers for Medicare deductibles, coinsurance and copayments. However, as permitted by federal law, states can limit provider reimbursement for Medicare cost sharing under certain circumstances. …Medicare providers must accept the Medicare payment and Medicaid payment (if any) as payment in full for services ren-dered to a QMB beneficiary. Medicare providers who violate these billing prohibitions are violating their Medicare Provid-er Agreement and may be subject to sanctions. … Despite fed-eral law, erroneous balance billing of QMB individuals per-sists. Many QMBs are unaware of the balance billing guide-lines (or concerned about undermining provider relation-ships) and want to pay the cost-sharing amounts.
How to Ensure Compliance with QMBProviders who participate in original Medicare and Medicare Ad-vantage Replacement Plans — not just Medicaid participants — must follow balance-billing prohibitions. QMBs retain balance billing protection when they receive care in other states. QMBs cannot waive their QMB status and pay Medi-care cost-sharing. Find out how to file for monies that Medicaid pays for QMBs. Un-derstand the processes you need to follow to request reimburse-ment for Medicare cost-sharing amounts if they are owed by your state. To bill your state, you may need to complete a state provider registration process and be entered into the state payment system.Here’s how to identify QMB patients in your patient population:
• Learn what your state’s QMB card looks like.• Find out if your state system can be queried to identify
QMBs.• Contact the commercial Medicare plans you accept to learn
what their QMB card looks like.• Make sure your billing staff exempt QMB individuals from
Medicare cost-sharing billing and related collection efforts.
Mary Pat Whaley, FACMPE, CPC, has more than 30 years’ experience managing physi-cian practices of all sizes and specialties in the private and public sectors. She is board cer-tified in Medical Practice Management. Whaley draws 30K+ visitors to her website (man-agemypractice.com) monthly, and is a Healthcare LinkedIn Thought Leader with 275,000+ followers. She is the originator of Credit Card on File for medical practices. Whaley’s mission is to create sustainable financial viability for small independent physician practices. She is a member of the Durham, N.C., local chapter.
If a physician has a contract with an insurance plan and has collected the deductible, co-pay, or co-insurance, billing the
patient for anything above the allowable rate is illegal.
Resources
Shots Health News, NPR, “States Make Laws to Protect Patients from Hidden Medical Bills,” Michelle Andrews, July 15, 2015: www.npr.org/sections/health-shots/2015/07/15/422964973/states-make-laws-to-protect-patients-from-hidden-medical-bills
MLN Matters® SE1128 Revised, February 1, 2016: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/se1128.pdf

38 Healthcare Business Monthly
By Heather Greene, MBA, RHIA, CPC, CPMA
■ CODING/BILLING
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
Part of our responsibility as healthcare business professionals is to understand the financial realities of healthcare delivery
and reimbursement. For those of us working in mental health, this means learning the “ins and outs” of the Inpatient Psychiatric Fa-cility Perspective Payment System (IPF PPS).
IPF PPS BackgroundIn section 124 of the Balanced Budget Refinement Act (BBRA) mandated the secretary of the U.S. Department of Health & Hu-man Services (HHS) to develop a per diem PPS for inpatient hospi-tal services furnished in psychiatric hospitals and psychiatric units. The PPS had to:
• Include an adequate patient classification system to reflect the differences in patient resource use and costs among psychiatric hospitals and psychiatric units;
• Maintain budget neutrality; and• Permit the HHS secretary to require psychiatric hospitals
and psychiatric units to submit information necessary for developing the PPS.
The HHS secretary was required to report to congress describing the development of the PPS.
The new system applies to Medicare patients, and the Centers for Medicare & Medicaid Services (CMS) decided to use the current PPS for consistency; however, instead of using a diagnosis related group (DRG) payment, the facilities would be paid per diem, using adjustments to a federal per diem base amount. The adjustments were derived using regression analysis to determine relevant factors to predict patient resources. The payment adjustors include both facility-specific and patient-specific adjustments.The final IPF PPS was developed using regression analysis data obtained from the 2002 cost report file and 2002 Medicare Pro-vider Analysis and Review (MEDPAR) data for IPF stays. The ef-fective date for implementing IPF PPS was for cost reporting pe-riods beginning on or after January 1, 2005. The PPS was based on the final federal per diem rate for Medicare patients and is up-dated yearly.
Formulating Base and Adjustment Rates Each year, the base rate is set and then adjusted using several fac-tors to formulate the calculated base rate for an individual facility. For 2016, the federal per diem rate is $745.19. Providers who fail to report quality data for fiscal year (FY) 2016 will receive a proposed FY 2016 per diem rate of $730.56 (a 2 percent reduction).
The Ins and Outs of Inpatient Psychiatric Facility Perspective Payment System
Account for DRG and comorbidity adjustments and ensure all active medical treatments and diagnoses are documented.
istoc
k.com
/hoo
desig
ns

www.aapc.com April 2016 39
IPF PPSCODING/BILLING
The IPF PPS is based on a federal per diem base rate that includes both inpatient operating and capital-related costs (including routine and ancillary ser-vices), and excludes certain pass-through costs (i.e., bad debt and direct medical education). The base rate also provides patient-level and facility-level ad-justments including wage index, teaching adjust-ments, and an add-on for rural facilities. The payment for an individual patient is further ad-justed for factors such as the DRG classification, age, length of stay, and the presence of specified co-morbidities. Additional payments are provided for cost outlier cases, and qualifying emergency depart-ment (ED) electroconvulsive therapy (ECT) treat-ments. The IPFs affected by the PPS are freestand-ing psychiatric facilities, distinct part psychiatric units of acute care hospitals, and distinct part units of critical access hospitalsSeveral factors may adjust the payment: The federal wage index adjustment, which is applied to the labor portion of the service, an add-on of 17 percent for facilities in rural areas, and an adjustment made for qualified teaching facilities of 0.515 percent.
In Alaska and Hawaii, there are varying cost of living adjustment factors. Alaska ranges from 1.23 to 1.25 percentage points, and Ha-waii ranges from 1.119 to 1.25 percentage points. Another adjustment of 1.31 for first day is given if the facility has a qualified emergency room (ER). To qualify, the ER department must be licensed, advertised, and staffed, and 33 percent of patients sought urgent treatment for ER conditions. Finally, if the patient receives an ECT, there is an adjustment of $320.19.There are also patient-specific adjustment factors. Patients under 45 years of age receive an adjustment factor of 1.00. This increas-es by 0.01 every five years after age 45, until age 64. For ages 65-69, the adjustment factor is 1.10; for ages 70-74, the adjustment is 1.13; for ages 75-79, the adjustment is 1.15; and for those who are 80 years old or older, the adjustment factor is 1.17. There are 17 Medicare severity-diagnosis related group (MS-DRG) categories that receive adjustment factors. For example, DRG 885 receives an adjustment factor of 1.00 and DRG 881 receives 0.99, as shown in Table A on the preceding page.
Name of Specific DRG DRG Adjust
Degenerative nervous system disorders with MCC 056 1.05
Degenerative nervous system disorders without MCC 057 1.05
Nontraumatic stupor and coma with MCC 080 1.07
Nontraumatic stupor and coma without MCC 081 1.07
Operating room procedure with principal diagnoses of mental illness 876 1.22
Acute adjustment reaction and psychosocial dysfunction 880 1.05
Depressive neuroses 881 0.99
Neuroses except depressive 882 1.02
Disorders of personality and impulse control 883 1.02
Organic disturbances and mental retardation 884 1.03
Psychoses 885 1.00
Behavioral and developmental disorders 886 0.99
Other mental disorder diagnoses 884 0.92
Alcohol/Drug abuse or dependence, left against medical advice 894 0.97
Alcohol/Drug abuse or dependence with rehabilitation therapy 895 1.02
Alcohol/Drug abuse or dependence without rehabilitation therapy with MCC 896 0.88
Alcohol/Drug abuse or dependence without rehabilitation therapy without MCC 897 0.88
Table A: There are 17 MS-DRG categories that receive adjustment factors.
Abbreviations & DefinitionsAdjustment factor (ADJ) – Payment for an individual patient is adjusted, due to certain factors.
Inlier – A time covered by the Medicare Severity-Diagnosis Related Group (MS-DRG) payment period of a claim that includes fully paid days, coinsurance days, or days after benefits have exhausted.
Outlier – An additional payment made by Medicare for high-dollar claims, intended to protect hospitals from large financial losses due to unusually expensive cases.
Comorbidity – The presence of one or more additional disorders (or diseases) co-occurring with a primary disease or disorder, or the effect of such additional disorders or diseases. The additional disorder may also be a behavioral or mental disorder.
Comorbidity ADJ – Adjustment factor reimbursement based on a comorbidity category.

40 Healthcare Business Monthly
IPF PPSCO
DING
/BIL
LING
How CCs and MCCs Change PaymentMany patients have comorbidities. For psychiatric facilities, some of these will add an adjustment factor, as shown in Table B. This is different from the Medicare hospital inpatient prospective pay-ment system, where a complication or comorbidity (CC) or major complication or comorbidity (MCC) would change the DRG, thus changing the payment; rather, comorbid conditions that fall into a comorbidity category add another adjustment factor. The IPF PPS has 17 comorbidity categories, each containing codes of comorbid conditions. Each comorbidity grouping will receive a grouping-specific adjustment. The facility can receive a single co-morbidity adjustment per comorbidity category; however, it can also receive an adjustment for more than one comorbidity catego-ry per encounter. Comorbidities are specific patient conditions that are secondary to the patient’s principal diagnosis and that require treatment during the stay. The diagnoses that relate to an earlier episode of care and have no bearing on the current hospital stay are excluded and must not be reported on the facility’s claim. According to the 2015 IPF PPS final rule, comorbid conditions must exist at the time of ad-mission or develop subsequently, and must affect the treatment re-ceived, length of stay, or both.The physician of record must connect any conditions the patient may have with the treatment during the encounter. These condi-tions, if treated, must be well documented throughout the chart. It’s not enough simply to list the name of a condition; there must be documentation to support the condition’s treatment or how the condition is affecting the mental condition’s therapeutic treatment.
Table B: The IPF PPS has 17 comorbidity categories, each with an adjustment factor.
Description of comorbidity Adjustment factor
Developmental disabilities 1.04
Coagulation factor deficits 1.13
Tracheostomy 1.06
Renal failure, acute 1.11
Renal failure, chronic 1.11
Oncology treatment 1.07
Uncontrolled diabetes-mellitus with or without complications 1.05
Severe protein calorie malnutrition 1.13
Eating and conduct disorders 1.12
Infectious disease 1.07
Drug and/or alcohol induced mental disorders 1.03
Cardiac conditions 1.11
Gangrene 1.10
Chronic obstructive pulmonary disease 1.12
Artificial openings — digestive and urinary 1.08
Severe musculoskeletal and connective tissue diseases 1.09
Poisoning 1.11
Comorbidity AdjustmentsAnother patient-specific adjustment factor relates to the length of stay. A variable per diem adjustment factor depends on several things. For example, day one depends on if your facility has a qualified ER. If it does, the adjustment factor is 1.31; if not, the adjustment factor is 1.19, as shown in Table C on the next page. The adjustments recognize the higher cost incurred in the early days of a stay.Resources
CMS.gov Inpatient Psychiatric Facility PPS: www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/InpatientPsychFacilPPS/index.html
Tools and Worksheets: www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/InpatientPsychFacilPPS/tools.html
IPF PPS Regulations and Notices: www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/InpatientPsychFacilPPS/IPF-PPS-Regulations-and-Notices.html
The Medicare Claims Processing Manual, chapter 3 - Inpatient Hospital Billing, section 190.5.2 Application of Code First: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c03.pdf

www.aapc.com April 2016 41
To discuss this article or topic, go to www.aapc.com IPF PPS
CODING/BILLING
Table C: Other adjustment factors include length of stay.
Variable Per Diem Adjustments
Day 1— Facility without a qualifying emergency department
Day 1 — Facility with a qualifying emergency department
Day 2 1.12 Day 13 0.99
Day 3 1.08 Day 14 0.99
Day 4 1.05 Day 15 0.98
Day 5 1.04 Day 16 0.97
Day 6 1.02 Day 16 0.97
Day 7 1.01 Day 17 0.97
Day 8 1.01 Day 18 0.96
Day 9 1.00 Day 19 0.95
Day 10 1.00 Day 20 0.95
Day 11 0.99 Day 21 0.95
Day 12 0.99 After Day 21 0.92
Code First RulesA significant concern arises when we have to follow the “Code First” rule. The Medicare Claims Processing Manual, chapter 3 - Inpa-tient Hospital Billing, section 190.5.2: Application of Code First (last updated October 30, 2015) has been pivotal in explaining the Code First rule. The manual explains how CMS handles this rule, and how to calculate your DRG adjustment factor when the pa-tient’s condition results in a principal diagnosis that is the etiology of the manifestation treated in the facility. Diagnosis code F02.81 Dementia in other diseases classified elsewhere with behavioral disturbance is designated as “ NOT ALLOWED AS PRINCIPAL DX” code.The three-digit code F02 Dementia in other diseases classified else-where is designated a Code First diagnosis, indicating that all diag-nosis codes that fall under the F02 category (codes F02.80 Demen-tia in other diseases classified elsewhere without behavioral disturbance and F02.81) must follow the Code First rule. The code F02 appears in the ICD-10-CM, as follows:
Code first the underlying physiological condition, such as:F02.80 Dementia in other diseases classified elsewhere without behavioral disturbanceNOT ALLOWED AS PRINCIPAL DXF02.81 Dementia in other diseases classified elsewhere with behavioral disturbanceNOT ALLOWED AS PRINCIPAL DX
According to Code First requirements, the provider would code the appropriate physical condition first: for example, G20 Parkinson’s disease as the principal diagnosis code and F02.81 as a secondary di-agnosis or comorbidity code on the patient claim.The purpose of this example is to demonstrate proper coding for a Code First situation. In this case, the principal diagnosis groups to one of the 15 DRGs, or 17 MS-DRGs, for which CMS pays an adjustment. Had the diagnosis code grouped to a non-psychiatric DRG/MS-DRG, the Pricer would search the first of the other diag-nosis codes for a psychiatric code listed in the Code First list to as-sign a DRG adjustment.Final note: All diagnostic and non-diagnostic outpatient servic-es (excluding ambulance) provided one day immediately preced-ing the date of the admission are considered to be inpatient servic-es and are included on the inpatient claim, unless the patient does not have Medicare.
Documentation Is KeyAs health information management or coding professionals, you should work to educate practitioners and clinicians on required documentation, so you can fully and accurately account for a pa-tient’s DRG and comorbidity adjustments. You should ensure all active medical treatment and diagnoses are captured in the medical record documentation, and remind practitioners to connect clinical dots to substantiate treatment patients receive.
Heather Greene, MBA, RHIA, CPC, CPMA, is assistant vice president of compliance and process improvement for Haven Behavioral Healthcare, Inc. She has approximately 20 years of experience in a variety of health information management roles. Greene performs coding and documentation audits, physician education, and process improvement for the Haven Be-havioral Health, Inc. psychiatric facilities. She is a member of the Florence, Ky., local chapter.
It’s not enough simply to list the name of a condition; there must be documentation to support the
condition’s treatment or how the condition is affecting the mental condition’s therapeutic treatment.

42 Healthcare Business Monthly ■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
■ AUDITING/COMPLIANCE
istoc
k.com
/SKa
pl
As of January 6, there’s a new HIPAA fi-nal rule. Formally known as the Health
Insurance Portability and Accountability Act (HIPAA) Privacy Rule and the Nation-al Instant Criminal Background Check Sys-tem (NICS) final rule, it’s been nicknamed the “gun check” rule. Effective February 5, 2016 this rule requires an FBI check to de-termine whether an individual who wants to purchase a firearm from a federally licensed vendor is diagnosed with mental illness.
Note: Parts of this article appeared in Litmos, an online blog: www.litmos.com/blog/healthcare/latest-hipaa-final-rule.
If your organization is a covered entity that cares for people with mental illness, you need to understand the nuances of the new rule, and be ready to report to the NICS when necessary.The HIPAA Privacy Rule has been added on to at Section 512 “Uses and disclosures for which an authorization or opportunity to agree or object is not required (k) Standard: Uses and disclosures for specialized govern-ment functions, (7) National Instant Crimi-nal Background Check System.”Per the revised rule:
• If a covered entity orders involuntary commitments or makes other adjudications regarding an individual’s mental health, or that serve as repositories of the relevant data, they are permitted to use or disclose the information needed for NICS reporting of such individuals either directly to the NICS or to a state repository of NICS data.
• If a covered healthcare entity also has
a role in the relevant mental health adjudications or serves as a state data repository, it now may disclose the relevant information for NICS reporting purposes under this new permission, even if it’s not designated as a HIPAA hybrid entity or required by state law to report it.
• It does not create an express permission for covered entities to disclose to NICS for reporting purposes the protected health information of individuals who are subject to state-only mental health prohibitors.
If you are a covered entity that must report to the NICS, the preamble states that you must report the data elements the NICS needs to create a record, plus there is more that you’re permitted to share with NICS. The elements needed to create the NICS record are:
• The individual’s name • The individual’s sex • The individual’s date of birth
The Federal Mental Health Prohibitor The federal mental health prohibitor makes individuals ineligible to purchase a firearm because they have been “committed to a men-tal institution” or “adjudicated as a mental de-fective.” Department of Justice regulations de-fine these categories to include persons:
• Who have been involuntarily committed to a mental institution for reasons such as mental illness or drug use;
• Have been found incompetent to stand trial or not guilty by reason of insanity; or
• Otherwise have been determined by a court, board, commission, or other lawful authority to be a danger to themselves or others or unable to manage their own affairs as a result of marked subnormal intelligence or mental illness, incompetency, condition, or disease.
• The record documenting the involuntary commitment or adjudication
• The entity from which the record initiated (your business name)
Additional data you may send include the in-dividual’s:
• Social Security number • State of residence • Height• Weight • Place of birth • Eye color • Hair color • Race
These additional elements will help authori-ties weed out false positives.The new section in the HIPAA Privacy Rule does not name any data elements outlined above. This gives the covered entity the flex-ibility to report the data required and re-quested by the federal government and any state requirements your state may have for your area.
Sue Miller has a 10-page memorandum explaining the new HIPAA final rule in depth. You may contact her at [email protected] or (978) 505-5660.
The Latest on HIPAA: The Gun Check RuleIf you provide care for patients with mental illness, understand the nuances of this final rule.
By Sue Miller

Be Our Guest
Thank You to Our HEALTHCON Exhibitors and SponsorsӀ Alpha II, LLCӀ Altegra HealthӀ American Health Information Management Association (AHIMA)Ӏ American Medical AssociationӀ ArroHealthӀ AviacodeӀ Barcharts, IncӀ BC AdvantageӀ Career StepӀ CHRISTUS HealthӀ Cigna HealthSpringӀ CodebustersӀ Coding Network, LLC (THE) Ӏ CodingAIDӀ Columbia Southern UniversityӀ CSI Healthcare ITӀ DecisionHealthӀ ElsevierӀ EvidentӀ Excite Health PartnersӀ F. A. Davis CompanyӀ Find-A-CodeӀ Florida Hospital Medical GroupӀ FTI Connsulting Health SolutionsӀ Gables Insurance Recovery, Inc.Ӏ GeBBS Healthcare SolutionsӀ HCA Physician Services GroupӀ HCTecӀ HCProӀ Health Information AssociatesӀ Healthicity
Ӏ IMO-Intelligent Medical ObjectsӀ ionHealthcareӀ Kelly Services, Inc.Ӏ KIWI-TEKӀ Langley Provider GroupӀ Libman EducationӀ Litmos HealthcareӀ MAAP HealthcareӀ Matrix Medical Network Ӏ Maxim Health Information ServicesӀ McGraw-Hill EducationӀ MedKoder, LLCӀ Mid-Atlantic Permanente Medical GroupӀ myTRICARE.comӀ NAMASӀ Ohana Healthcare LLCӀ Optum360Ӏ Panacea | MedLearn PublishingӀ Perry Johnson & AssociatesӀ RCM Health Care ServicesӀ Reimbursement Management Consultants, IncӀ Surgicode LLCӀ The Coding InstituteӀ The College of St. ScholasticaӀ Ultimate Medical AcademyӀ United Audit Systems, Inc.Ӏ Wolters Kluwer Ӏ Zhealth Publishing, LLC
PLATINUM
GOLD
SILVER
BRONZE

44 Healthcare Business Monthly
■ AUDITING/COMPLIANCEBy Michael D. Miscoe, JD, CPC, CASCC, CUC, CCPC, CPCO, CPMA
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
2016 OIG Work Plan: Part B Risk AreasPut these OIG compliance efforts on a high priority focus list for your provider.
The Office of Inspector General’s (OIG) annual work plan for 2016 outlines significant new areas, as well as ongoing target areas, on which the federal agency will focus its reviews and audits of U.S. Department of Health and Human Services (HHS) programs and operations this year. Let’s take a look at what’s on the OIG’s radar for Medicare Part B providers. Similar to the approach we took with Part A, published in Healthcare Business Monthly last month, we’ll review the new and revised focus areas only.
Medical Equipment and Supplies – Policies and PracticesFor medical equipment and supplies, the OIG is honing in on the policies and practices of:
• Power mobility devices – lump-sum purchase versus rental• Competitive bidding for medical equipment items and
services – mandatory post-award auditOIG will determine the reasonableness of the Medicare fee sched-ule by comparing Medicare payments made for orthotic brac-es to the amounts paid by non-Medicare payers, such as private
insurance companies, to identify potentially
wasteful spending. NEW! Osteogenesis stimula-tors – OIG will look at lump-
sum purchase versus rental. They will determine whether poten-
tial savings can be achieved by Medi-care and its beneficiaries if osteogene-
sis stimulators are rented over a 13-month pe-riod, rather than acquired through a lump-sum purchase.
Medical Equipment and Supplies – Billing and Payments
Regarding billing and payments of medical equip-ment and supplies, the OIG is focusing on:• Power mobility devices – supplier compliance
with payment requirements• Nebulizer machines and related drugs – supplier
compliance with payment requirements• Effectiveness of system edits for diabetes testing
supplies to prevent inappropriate payments for blood glucose test strips and lancets to multiple suppliers
NEW! Orthotic braces – OIG will review Medicare Part B pay-ments for orthotic braces to determine whether durable medical equipment, prosthetics, orthotics, and supplies (DMEPOS) sup-pliers’ claims were medically necessary and were supported in ac-cordance with Medicare requirements. OIG makes clear that com-pliance with documentation requirements and utilization guid-ance outlined in the local coverage determinations (LCDs) is-sued by the DMEPOS Medicare administrative contractor will be the focus of its analysis. DME suppliers should review published Medicare guidance to ensure compliance.NEW! Increased billing for ventilators – OIG has noticed a sig-nificant increase in billing for ventilators (specifically, HCPCS
istoc
k.com
/mac
gyve
rhh

www.aapc.com April 2016 45
AUDITING/COMPLIANCE
Work Plan
Level II code E0464 Pressure support ventilator with volume control mode, may include pressure control mode, used with non-invasive in-terface (e.g., mask). From 2013 to 2014, OIG reports a 127 percent increase in allowed amounts for E0464. OIG believes that suppli-ers may be inappropriately providing/billing for ventilators for pa-tients with non-life-threatening conditions, and not meeting the medical necessity criteria for ventilators. The Medicare National Coverage Determinations Manual, Section 280.1, stipulates that ventilators are covered for the treatment of severe conditions asso-ciated with “neuromuscular diseases, thoracic restrictive diseases, and chronic respiratory failure consequent to chronic obstructive pulmonary disease.” Ventilators are not considered reasonable and necessary when the patient has a condition for which the relevant LCD indicates a continuous positive airway pressure or respirato-ry assist devices is appropriate. DME suppliers should review pub-lished LCD guidance to ensure compliance.
Medical Equipment and Supplies – Quality of Care and Safety OIG is reviewing quality of care and safety measures for DME in regards to:
• Access to DME in competitive bidding areas
Other Providers – Policies and Practices For other providers’ policies and practices, the OIG is focusing on:
• Ambulatory surgical centers (ASCs) – payment system• End-stage renal disease facilities – payment system for renal
dialysis services and drugs NEW! ASC quality oversight – OIG will review Medicare’s quality oversight of ASCs. Previous OIG work found problems with Medicare’s oversight system, including finding spans of five or more years between certification surveys for some ASCs, poor Centers for Medicare & Medicaid Services’ (CMS) oversight of state survey agencies and ASC accreditors, and little public infor-mation on the quality of ASCs. CMS requires that ASCs become Medicare certified by a state survey and certification agency or pri-vately accredited to show they meet the conditions. Because cer-tification is a condition of payment, payments to ASCs without
proper or current certification are deemed as overpayments. For this reason, ASCs should verify compliance with state accredita-tion requirements.
Other Providers – Billing and Payments For other provider billing and payments, the OIG is targeting:
• Ambulance services – questionable billing, medical necessity, and level of transport ASC anesthesia services; payments for personally performed services
• Chiropractic services – Part B payments for non-covered services
• Chiropractic services – portfolio report on Medicare Part B payments
• Imaging services – payments for practice expenses• Selected independent clinical laboratory billing
requirements• Annual analysis of Medicare clinical laboratory payments• Physical therapists – high use of outpatient physical therapy
services by independent therapists• Portable X-ray equipment – supplier compliance with
transportation and set-up fee requirements• Sleep disorder clinics – high use of sleep-testing procedures
(CPT® 95810 Polysomnography; age 6 years or older, sleep staging with 4 or more additional parameters of sleep, attended by a technologist and 95811 Polysomnography; age 6 years or older, sleep staging with 4 or more additional parameters of sleep, with initiation of continuous positive airway pressure therapy or bilevel ventilation, attended by a technologist)
• Inpatient rehabilitation facility payment system requirements
• ASC versus hospital outpatient payments NEW! Physicians referring/ordering Medicare services and supplies – OIG will review select Medicare services, supplies, and DME referred/ordered by physicians and non-physician practi-tioners (NPPs) to determine whether the ordering provider was a Medicare-enrolled physician or NPP. If the referring/ordering
Because this is a mere summary of the Part B provider portion of the 2016 OIG Work Plan, you
are encouraged to review it in its entirety to ensure applicable risk areas are well understood.

46 Healthcare Business Monthly
Work PlanAU
DITI
NG/C
OMPL
IANC
ETo discuss this article or topic, go to www.aapc.com
physician or NPP is not eligible to order or refer, then the claims are not compensable. You should internally validate that the order-ing provider of services, supplies, and DME is currently enrolled. A review of past claims is also recommended. If the ordering pro-vider is not an eligible (Medicare enrolled) provider, the payments associated with claims made pursuant to any order from such a provider should be disclosed and refunded.NEW! Anesthesia services – non-covered services. OIG will re-view Medicare Part B claims for anesthesia services to determine whether the patient had a related and covered Medicare service. Medicare will not pay for items or services that are not reasonable and necessary. Specifically, where the anesthesia procedure was re-lated to the performance of a non-covered procedure, the anesthe-sia is non-covered, as well. Anesthesia providers should review past claims for compliance, and voluntarily disclose and refund any in-appropriate payments. Make necessary modification to policies and procedures to ensure compliance.NEW! Physician home visits – reasonableness of services. OIG will determine whether Medicare payments to physicians for eval-uation and management (E/M) services performed in the home were reasonable and made in accordance with Medicare require-ments. Since January 2013, Medicare made $559 million in pay-ments for physician home visits. Physicians are required to docu-ment the medical necessity of a home visit in lieu of an office or outpatient visit. Providers should review past claims for compli-ance and voluntarily disclose and refund any inappropriate pay-ments. Make necessary modification to policies and procedures to ensure compliance.NEW! Prolonged services – reasonableness of services. OIG will determine whether Medicare payments to physicians for pro-longed E/M services were reasonable and made in accordance with Medicare requirements. The necessity of prolonged servic-es is considered by CMS to be rare and unusual. The Medicare Claims Processing Manual, publication 100-04, chapter 12, sec-tion 30.6.15.1, includes requirements that must be met to bill a prolonged E/M service. Providers should review past claims for noncompliance and voluntarily disclose and refund any inappro-priate payments. NEW! Histocompatibility laboratories – supplier compliance with payment requirements. OIG will determine whether pay-ments to histocompatibility laboratories were made in accordance with Medicare requirements. From March 31, 2013, through Sep-tember 30, 2014, histocompatibility laboratories reported $131
million in reimbursable costs. Histocompatibility laboratories are reimbursed based on reasonable costs, which must be related to the care of patients, as well as reasonable, necessary, and prop-er. Histocompatibility laboratories should review past claims and cost reports for noncompliance and voluntarily disclose and re-fund any inappropriate payments. Histocompatibility laborato-ries should make necessary modification to policies and proce-dures to ensure compliance.
Get to Know the OIG Work PlanBecause this is a mere summary of the Part B provider portion of the 2016 OIG Work Plan, you are encouraged to review it in its en-tirety to ensure applicable risk areas are well understood. For each focus area affecting your provider, be certain to review appropriate CMS interpretive guidance, LCDs, and any referenced regulatory provisions cited in the OIG Work Plan to ensure you completely understand and comply with CMS expectations, particularly with respect to documentation content and coverage limitations.
Michael D. Miscoe, JD, CPC, CASCC, CUC, CCPC, CPCO, CPMA, is president-elect of AAPC’s National Advisory Board, serves on AAPC’s Legal Advisory Board, and is AAPC Ethics Committee chair. He is admitted to the practice of law in California as well as to the bar of the U.S. Supreme Court and the U.S. district courts in the southern district of Cali-fornia and the western district of Pennsylvania. Miscoe has over 20 years of experience in healthcare coding and over 18 years as a forensic coding and compliance expert. He has
provided expert analysis and testimony on coding and compliance issues in civil and criminal cases and rep-resents healthcare providers in post-payment audits and HIPAA OCR matters. Miscoe speaks on a national level, and is published nationally on a variety of coding, compliance, and health law topics. He is a member and past president of the Johnstown, Pa., local chapter.
Resources
For details pertaining to ongoing reviews, which are listed in this article only by name, or for details regarding risk areas associated with Part C, Part D, and Medicaid programs, please refer to the 2016 OIG Work Plan: http://oig.hhs.gov/reports-and-publications/archives/workplan/2016/oig-work-plan-2016.pdf.
Medicare National Coverage Determinations Manual, §280.1: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/ncd103c1_part4.pdf
Medicare Claims Processing Manual, publication 100-04, chapter 12, § 30.6.15.1: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf
For details regarding coverage requirements for histocompatibility laboratories, see 42 CFR §§ 413.9(a), (b), and (c)(3): www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ClinicalLabFeeSched/downloads/413_9.pdf
For requirements pertaining to cost reporting, see 42 CFR §§ 413.24(a), (c): www.gpo.gov/fdsys/pkg/CFR-2011-title42-vol2/pdf/CFR-2011-title42-vol2-sec413-24.pdf

HEALTHICITY.COM/AUDITMANAGER
Customize, manage, train and simplify your audit process. We streamlined your audit process by merging audit workflow, management, and reporting capabilities into one easy-to-use, web-based solution.
Smart Design.Intelligent Auditing.

48 Healthcare Business Monthly
■ AUDITING/COMPLIANCEBy Lisa Jensen, MHBL, FACMPE, CPC
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
Rock the Mock AuditKnow how your practice would fare in a government audit.
Does the thought of an external audit keep you up at night? Well, fear no more! By conducting “mock” or self audits, you can uncov-er potential issues before a regulator or payer does. During such an audit, an outside consultant or staff within your company assumes the role of enforcement officials and conducts the level of investi-gation that is anticipated from the regulator.Mock audits prepare your practice or facility for an official audit by walking you through the process of documentation requests, which involves identifying the information you will be asked to disclose and designating personnel responsible for gathering, pre-
paring, and presenting that information. With this knowledge in hand, you can focus on resolving issues uncovered during the mock audit.
How to Get StartedFirst, determine how many resources and how much time you can expend on an audit. For example:
• Is there someone who will be in charge and who is able to keep the focus and energy moving towards the end goal?
• Do you have access to the reports you need to identify your audit target areas?
• Are the providers on board with this idea? And will they be open to the feedback, corrective actions, and results you will find?
Asking yourself these questions will help you to anticipate and ad-dress obstacles you may encounter during the mock audit. You also must know what you agreed to with your payers. Review the websites and contracts of top payers to learn what each health plan requires as part of its integrity program or claims review pro-cess. Take note of the time periods for records review, whether an auditor is allowed to visit the practice site, and the frequency with which auditing can occur for each plan.
Identify Risk AreasWith limited resources and dollars, you’ll need to define the scope of the mock audit to your highest risk areas. Start by determining if past risk areas have been resolved. If no issues rise to the top, use resources such as benchmarking data and common error reports to assess risk. Good resources are the Centers for Medicare & Medic-aid Services (CMS), the Office of Inspector General (OIG), Com-prehensive Error Rate Testing, Medical Group Management As-sociation (MGMA) survey data, specialty society member Web tools, etc. The OIG’s top hits for auditing can be found in the OIG Work Plan. Common targets of the OIG are:
• Improper application of modifier 25 Significant, separately identifiable evaluation and management service by the same physician or other qualified health care professional on the same day of the procedure or other service and modifier 59 Distinct procedural service;
istoc
k.com
/pbo
phot
ograp
her

www.aapc.com April 2016 49
AUDITING/COMPLIANCE
Mock Audit
• Up-coding (especially relative to evaluation and management (E/M) services);
• Unbundling of global surgery; and • Overuse of diagnostics without supporting medical
necessity.Compare your CPT® and HCPCS Level II utilization data with CMS data available on the Medicare Utilization for Part B web page (www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/MedicareFeeforSvcPartsAB/MedicareUtilizationforPartB.html). For example, open the 2014 “Medicare Part B Physician/Supplier National Data - Calendar Year Evaluation and Management Codes by Specialty” file. To use this data file, copy the Internal Medicine utilization under “Allowed Services” for each E/M code you are interested in reviewing onto a spreadsheet, as shown in Chart A.
Chart A: CMS Internal Medicine 2014
CPT® Frequency Percentage
99201 8,184 1%
99202 90,835 5%
99203 494,415 30%
99204 784,102 47%
99205 282,662 17%
Total 1,660,198
Next, calculate a percentage for each code. For example, divide the frequency number that internal medicine physicians coded 99201 (8,184) by the total of new patient codes reported (1,660,198). The result tells us that internal medicine physicians coded 99201 ap-proximately 1 percent of the time when billing Medicare for a low-level, new patient office visit in 2014.
Chart B
Internal Medicine Bell Curve
99201 99202 99203 99204 99205
1%5%
30%
47%
17%

50 Healthcare Business Monthly
Mock AuditAU
DITI
NG/C
OMPL
IANC
E
Generate a similar billing utilization report from your practice management system. Follow the same procedure to calculate the frequency use of each code in your practice. These percentages can then be used to create a bell curve (as shown in Chart B). Al-though coding above, below, or at the national bell curve for your specialty does not necessarily mean you’re coding accurately (or not), knowing how your personal bell curve stacks up offers a clue to areas your coding may deserve a closer look. To simplify this process, AAPC offers the E/M Utilization Bench-marking Tool (www.aapcps.com/resources/em_utilization.aspx). This tool compares a physician’s, or an entire practice’s, evaluation and management (E/M) CPT® code utilization to peers in the same specialty. The distribution of utilization by code within each E/M subcategory is benchmarked to the distribution of paid Medicare claims for physicians in the same specialty, nationally.
Time to AuditAfter you identify the areas, providers, and codes that should be targeted, it’s time to conduct the audit. Pulling a sample of, for in-stance, 10 charts per provider or 10 percent of total targeted charts may be a good way to start, and keep the workload manageable. External consultants may have other recommendations based on the total volume of your practice and the types of services you bill. The coding should be consistent with the auditing tools provid-ed by your Medicare carrier, private payers, and standard coding auditing guidance, including those found in the CPT® and ICD codebooks.
Tip: AAPC’s Healthicity medical auditing software provides two viable solutions for internal auditing: Audit Manager is an all-in-one audit management solution that simplifies the audit workflow and takes the guesswork out of the audit process; Audit Services enables you to pool from our nationwide network of credentialed auditors to conduct medical chart reviews, medical record and documentation review, and audit validation. For more information, visit: www.aapc.com/audit-management-software.aspx.
Share the ResultsShortly after the review session, be sure each provider receives a re-port (in table format) summarizing your overall findings. For ex-ample, the report might show there were three instances in which a service was billed as 99212 Office or other outpatient visit for the evaluation and management of an established patient, which requires at least 2 of these 3 key components: A problem focused history; A prob-
lem focused examination; Straightforward medical decision making, but documentation would have supported 99213 Office or other outpatient visit for the evaluation and management of an established patient, which requires at least 2 of these 3 key components: An ex-panded problem focused history; An expanded problem focused exam-ination; Medical decision making of low complexity. You should also provide each physician with a copy of his or her charts with the re-viewers’ comments. If you’re concerned that some providers may disregard the feed-back, you can place a redacted summary for all providers to see. In this summary, let each provider know which data represents their results, but block out the others. They can see how they did in comparison with their peers. Many find this sort of competi-tion very motivating.
Make a Positive Change Be sure you do something about the errors, inconsistencies, and other issues you find. For example:
• Do policies and procedures need to be updated or corrected?
• Are there areas where additional education may be needed? • Does your electronic health record template require some
refining or a complete overhaul?The same people who conduct the audit should notify manage-ment of the actions needed to address areas of weakness. Man-agement should determine procedures for correcting these errors. These procedures may vary from payer to payer. Overpayments may need to be refunded or corrected bills resub-mitted. Although this may amount to “waving a red flag” in front of the insurer, it’s usually better to come forward than to play the game of wait and see. For significant errors, consult your health-care attorney before acting on your findings. Like preventive medicine, proactive internal reviews allow you to correct over-coding before it causes overpayment, and to correct under-coding before it turns into under-billing.
For information on this year’s OIG Work Plan, check out “2016 OIG Work Plan: Part B Risk Areas” on pages 44-46 of this is-sue of Healthcare Business Monthly and “2016 OIG Work Plan: Part A Risk Areas” on pages 44-46 of March’s Healthcare Busi-ness Monthly.
www.aapc.com April 2016 51
To discuss this article or topic, go to www.aapc.com
AUDITING/COMPLIANCE
Mock Audit
To gain support … you might create T-shirts, candy bar wrappers, and notes with sayings such as, “I Rock the Mock, “Be Audit You Can Be!”
“Keep Calm and Audit On,” or “Don’t make me use my audit voice.”
Overcome ObstaclesIf a physician refuses to adapt his or her coding and documenta-tion patterns to ensure compliance with applicable regulations, disciplinary action may be warranted.A very real danger is that you will conduct the audit and identify errors, but will have no support to correct them. Knowing there is an issue that your practice has done nothing to correct can create a huge liability risk. To gain support, make the process as fun as possible. For example, you might create T-shirts, candy bar wrap-pers, and notes with sayings such as, “I Rock the Mock,” “Be Au-dit You Can Be!” “Keep Calm and Audit On,” or “Don’t Make Me Use My Audit Voice.”
Lastly, remember that rules change and people change, so periodic internal audits are necessary. Keep the audit process fresh and rel-evant, and do your best to identify risk areas before they become real problems.
Lisa Jensen, MHBL, FACMPE, CPC, is the senior manager of external audit at Providence Health Plans in Beaverton, Ore. She has a master’s degree in Healthcare Business Leader-ship. Jensen has been a Certified Professional Coder (CPC®) since 1996 and a Fellow in the American College of Medical Practice Executives (FACMPE) since 2008. She is a member of the Portland Columbia River, Ore., local chapter.
AAPC VIRTUAL WORKSHOPS NOW AVAILABLE!AAPC VIRTUAL WORKSHOPS NOW AVAILABLE!
Find a virtual workshop near you: Find a virtual workshop near you: Find a virtual workshop near you:
www.aapc.com/Workshopswww.aapc.com/Workshops
AAPC's virtual workshopsgives you more of whatyou need:
AAPC's virtual workshopsgives you more of whatyou need:
AAPC's virtual workshopsgives you more of whatyou need:
• Up to 6 CEUs• 4 hours of virtual presentation• Authored and presented by leading experts• In-depth information on critical topics
• Up to 6 CEUs• 4 hours of virtual presentation• Authored and presented by leading experts• In-depth information on critical topics
• Up to 6 CEUs• 4 hours of virtual presentation• Authored and presented by leading experts• In-depth information on critical topics
Workshop Features:Workshop Features:Workshop Features:
• Interactive and hands-on exercises with case studies
• 4-hours includes presentation and skill-building practice
• Access on-demand recording
• Interactive and hands-on exercises with case studies
• 4-hours includes presentation and skill-building practice
• Access on-demand recording
• Interactive and hands-on exercises with case studies
• 4-hours includes presentation and skill-building practice
• Access on-demand recording
800-626-2633 | aapc.com/workshops

52 Healthcare Business Monthly ■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
By Lori A. Cox, MBA, CPC, CPMA, CPC-I, CEMC
■ PRACTICE MANAGEMENT
About a year ago, a group of my coding friends and I started an email string we called, “A Little Humor.”
We would like to share some of our discoveries (taken from redacted provider documentation) with you, along with our comments.
• “To that end I recommend to the daughter that they proceed rectally to the emergency room.” Make sure to back in to the ER.
• “Hand pain – she is to keep her abdomen with orthopedics.” Her hand can go home with her, however.
• “She was milking a car at work.” Is that 2 percent or low-gas milk?• “Blood pressure 135/75 is the gold.” What’s the silver and
bronze blood pressure (BP), I wonder?• “Mother presents to ER with her 6-year-old for redness and
facial swelling.” The child appeared normal, so the doctor asked, “In what context does he have these symptoms” (e.g., what is the child doing when symptoms appear). The mother answered, “When he’s blowing up a balloon.” No comment needed.
• “Patient was placed on the operating tablet.” I guess you can use tablets for more than just getting on Facebook.
• “Hypertension with diabetes. Her blood pressure is cold.” Wonder what warm BP would be?
• “She is stressed because he has invited another woman into their home ‘to help get her on her feet.’ This woman is sharing the bed with them.” I would be stressed, too!
• “Patient states that she will lose weight one day, when her family stops cooking so much.” If only it were that easy.
• “Her biggest complaint [is] she would like to have bacon in her diet.” You can’t live without Bacon.
• “8 year old white male was at work around 9:30 a.m. when a heavy metal piston device smashed his finger.” I guess they start working ‘em early in some places.
• “He went outside to attempt the fetus chickens.” Feed. Feed the chickens.
• “A teenage driver lost control throwing a banana out the window.” That’s what you get for littering, kids.
• “Pt’s trial of a small amount of alcohol each afternoon may not be working well, according to her daughter.” Maybe the dose needs to be adjusted?
• “Male with an ax in his head. He states his wife did it because he asked her if it ‘was that time of the month.’” And yes, he lived.
Many thanks to the team who shared their hillarious notes: Karen Lavigne, CPC, CPMA, CRC; Marcelle Viator, CPC, CRC; Kris-tie Fissler, CPC, CPMA, COC, COSC; Brenda Stevens, CPC, CPMA, CRC; Jen Bueddeman, CPC, CRC; Kelley Sorenson, CPC; Dawn Catanese, CPC, COC, CRC; and Colette Bohon, CPC, CRC.
Send in Your Funny Doctors’ Notes We’d like to hear your funny stories. Submit your laughs to [email protected] for possible inclusion in future editions of Healthcare Business Monthly.
Lori A. Cox, MBA, CPC, CPMA, CPC-I, CEMC, is the coding team leader at MedKoder, and has over 17 years’ experience in multiple areas of healthcare. She has been certified since 2002 and is the Region 5 Representative for the AAPC NAB. Cox is the treasurer for the Quincy, Ill./Hanni-bal, Mo., local chapter.
The Doctor Said What
Humor is mankind’s greatest blessing. — Mark Twain
When medical situations get serious, sometimes the medical record becomes humorous.
istoc
k.co
m/I
gor Z
akow
ski

AMA
Series includes:
Crack specialty coding with the American Medical Association’s 2016 CPT® Coding Essentials series—the perfect companion to your CPT® Professional codebook
CPT® Coding Essentials for Cardiology 2016CPT® Coding Essentials for General Surgery & Gastroenterology 2016CPT® Coding Essentials for Obstetrics and Gynecology 2016CPT® Coding Essentials for Ophthalmology 2016CPT® Coding Essentials for Orthopedics: Lower Extremities 2016CPT® Coding Essentials for Orthopedics: Upper Extremities And Spine 2016
Strengthen your knowledge and simplify your research with the new 2016 CPT® Coding Essentials series. This six-book series includes illustrations and plain English descriptions for code selection in a CPR® code-driven format. Each book focuses on CSM reimbursement and medical necessity information.
This is the only specialty series that comes straight from the source of CPT code—the AMA—and exclusively provides the CPT Editorial Panel’s Guidelines instructions on ICD-10-CM documentation and coding.
Each CPT® Coding Essentials title includes CPT code for surgeries, medicine and ancillary services, paired with: • Illustrations and plain English descriptions of the service represented by the code • Official, code-specific instructions and parenthetical information from the AMA’s CPT Professional codebook • ICD-10-CM codes mapped by coding experts • RVUs, global periods and modifier payment rules • References to CMS’s Pub 100 and the AMA’s CPT® Assistant newsletter
To learn more, visit amastore.com or call (800) 621.8335.
54 Healthcare Business Monthly
By Ken Camilleis, CPC, CPC-I, COSC, CMRS, CCS-P
■ PRACTICE MANAGEMENT
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
Work together to ensure CDI is maximized in all practitioner documentation.
Clinical documentation affects the entire revenue cycle. If a medical note is not properly documented, a domino effect leads to inaccurate coding, which affects billing and financial management of the prac-tice. Poor documentation may also affect quality of patient care be-cause all elements aren’t captured accurately or considered based on a practitioner’s findings. Because of this, clinical documentation im-provement (CDI) plays a key role across the spectrum of healthcare business management.
The Nine “Cs” of Clinical Documentation Improvement
shut
tersto
ck.co
m

www.aapc.com April 2016 55
CDIPRACTICE M
ANAGEMENT
The fundamental basis for CDI is to improve the clinical note, which contains information about the encounter such as the pa-tient’s symptoms (i.e., the reason for the visit) and history of present illness, data measured and recorded, examination observations, an assessment, a definitive diagnosis, and a care management plan. A clinical note may reflect a variety of services and formats, such as a progress note compiled by a doctor or staff nurse during an encoun-ter with a patient in the office or outpatient setting, a summary of laboratory findings and recommendations, a radiological interpre-tation or report, and an operative note.A clinical note is a like a snapshot. Physicians may see dozens of pa-tients a day, and if the information isn’t recorded in the progress note or operative report, it’s probably lost for good. Will a physician re-ally remember how many minutes he spent counseling a patient on smoking cessation or what the specific dimensions of a skin wound repair were if this information is not documented at the time of the encounter? This accentuates one of the assertions of the coders’ creed: “If it’s not documented, it didn’t happen.” To assess the quality of your providers’ clinical documentation, you may want to refer to what I call the “Nine Cs of CDI.”
1. ClarityThe doctor may be able to read his own handwriting, but if you can’t make it out, the documentation is worthless. It shouldn’t be your re-sponsibility to decipher something illegible or ambiguous, and risk miscoding based on that interpretation. Providers who are still us-ing pen and ink need to be enlightened to the 21st century, where we have sophisticated electronic health record (EHR) templates. Shockingly, some practitioners with EHRs are still in the habit of preparing their notes manually and relying on a scanner to transmit them; this should be discouraged while using technological resourc-es should be encouraged.
2. Consistency Medical notes must not contain any words or sentences that could be interpreted as inconsistent with the diagnosis assessed or the pro-cedure performed. Consistency of documentation is important not only for coding accuracy, but also for compliance. It’s easy to slip up on this if close attention is not paid to the chronology of the patient’s present illness and treatment. In the event of an external audit or a payer request for supporting documentation, the documenter must be able to back up a claim of medical necessity. Inconsistencies in the encounter note diminish the preparer’s credibility.
3. CompletenessAs we strive to capture the entire clinical picture of the patient, it’s important for the physician to document all information pertinent to the patient’s diagnosis, such as any current and recently discon-tinued medications and changes in condition status. For example:
• If a patient is diagnosed with septic arthritis or bursitis, the organism causing the sepsis should be documented.
• If a patient returns with lower sugar readings a week after diabetes was assessed as out of control, controlled diabetes (reflected by the lower readings) should be documented for the current encounter.
• Hypoxia caused by respiratory failure should be documented for accuracy of coding, as well as clarity of the illness severity.
• If a lysis of adhesions was performed, what organs or structures were released? If an acquired absence of an organ is relevant to a physician’s finding, it should be documented and picked up by you.
It may not be sufficient to simply document “status post surgery” because you may need to know whether a complication was actual-ly post-procedural or caused by the surgery. Be sure to list any po-tentially related comorbid conditions. Key elements missing from the clinical note disservice the coders and billers, as well as quali-ty of care.
4. CohesionThere are many different styles of clinical notes, but whether the practitioner uses a SOAP, CHEDDAR*, or narrative format, the un-derlying document should outline the patient’s chief complaint and other related subjective data, as well as objective data, and smooth-ly segue into the assessment of the patient’s condition and the course of action the provider will pursue.
*SOAP stands for subjective, objective, assessment plan and CHEDDAR stands for chief complaint, history of presenting illness, examination, details, drugs and dosages, assessment, return visit information or referral.
5. Coder FriendlinessPhysicians sometimes document in terms only they understand. You may need to learn quickly about what is documented; Internet re-searching often helps, but it’s not a cure-all. You and your physicians should educate each other.

56 Healthcare Business Monthly
CDIPR
ACTI
CE M
ANAG
EMEN
T
For example, if an orthopedic surgeon treats an open fracture, he can simply add the word “open” to his diagnosis, or at least docu-ment that a skin wound was caused by the fracture. If the treatment was performed on the proximal humerus, the specific location (sur-gical neck, greater tuberosity, etc.) will help you to code more pre-cisely, instead of selecting an unspecified code within this anatom-ic site. Physicians should also try to minimize the amount of unfa-miliar abbreviations they enter into clinical notes.
6. ConcisionIdeal documentation stays on point with the patient’s current prob-lem and the reason for seeking medical care. It’s not necessary to enumerate (or copy and paste) the patient’s entire medical history or medication regimen, or make statements in the note that have no bearing on treatment of the condition being managed or a re-lated procedure being performed. Despite extreme severity of cer-tain comorbid illnesses that must remain a part of the patient’s re-cord of active problems, a specialist does not need to reiterate condi-tions if they are not relevant to the encounter. Concise documenta-tion speeds up the coding process because you aren’t bogged down reading superfluous text.
7. CompartmentalizationSometimes physicians will document everything they are sup-posed to, but in no particular order or pattern. This may cause you to overlook information germane to accurate coding. Most EHR packages provide medical practice staff with the capa-bility to design sophisticated templates from which they can fill in the details of their progress note in a timely, cost-effective man-ner. In the EHR, the most valuable feature of the compartmental-ization process is the ability to standardize the location of any key element within the note. This greatly eases validating a charge or coding the note from scratch, saves time, and creates a much less error-prone workflow. For instance, if a patient is given an inhalation treatment or a vac-cination, the details of this procedure (drug dosage, constituents, etc.) can be entered into a field called “Orders,” and you will always know to look there for this piece of data.
8. Cleanliness A clinical note riddled with grammatical and typographical errors lacks professionalism and can create repercussions down the reve-nue cycle, including the possibility of a payer audit. Language bar-
riers can sometimes cause transcription of incorrect information, such as “50 mg” instead of “15 mg.” With medical terms, you have to be especially careful with spelling and pronunciation because words may look and sound similar (e.g., hypertension vs. hypoten-sion). It’s important for all clinical staff, including medical assis-tants who act as data processors and transcriptionists, to be proper-ly trained in CDI. This may require someone validating their work before it gets submitted.
9. Credibility Credibility is one of the most important facets of CDI. When cod-ing for professional services, medical staff — including on-site and off-site coders — cannot use “working diagnoses” to code actual findings. Words such as “question of,” “probable,” or “likely” pre-ceding a clinical diagnostic term negate that term because no actu-al diagnosis has been established. If the physician has determined the actual diagnosis, he or she should not add words in the docu-mentation that cast doubt on the finding.During the dictation and transcription process, you must be care-ful with “cloned” documentation, which is boilerplate text lifted (i.e., copied and pasted) from one patient visit to the next (or even from one patient to another). Such habits are fraught with peril, es-pecially if cloned text hasn’t been proofread for parameters that can vary from encounter to encounter or patient to patient. As deemed necessary, subordinate data entry should be quality-controlled at a checkpoint before a claim is submitted. This check-point should primarily be the responsibility of the clinical staff be-cause the workflow may completely bypass you if no major edits are caught between the EHR and the billing pipeline.
Will a physician really remember how many minutes he spent counseling
a patient on smoking cessation or what the specific dimensions of a skin wound repair were if this information is not documented at the time of the
encounter?

www.aapc.com April 2016 57
To discuss this article or topic, go to www.aapc.com CDI
PRACTICE MANAGEM
ENT
CDI Is More Important than EverThe clinical note is a legal document. Physicians, coders, billers (and anyone else involved in healthcare) are touched by the clini-cal note. It’s the source from which you abstract information to se-lect optimal codes for reporting to payers. We all must work as a team to ensure we are maximizing the CDI factor in all practitio-ner documentation. With ICD-10 now a reality, specificity of doc-umentation is more important than ever, and more stringent gov-ernmental and payer regulations reflecting CDI are in our future. Coders and clinical staff should convene periodically or as needed to address CDI, reviewing general issues discussed here, as well as those that are specialty-specific.
Ken Camilleis, CPC, CPC-I, COSC, CMRS, CCS-P, is an educational consultant and PMCC instructor with Superbill Consulting Services, LLC. He is also a professional coder for Signa-ture Healthcare, a health system covering much of southeastern Massachusetts. Camilleis’ primary coding specialty is orthopedics. Camilleis is a member of the Cape Coders local chapter, in Hyannis, Mass.
1. Make sure someone other than the documentor can read every element in the note.
2. Avoid any inconsistencies in a clinical note.
3. Capture all clinical information that may affect patient care.
4. Use clear paragraph structure, where sentences adhere together, so as not to break the reader’s train of thought.
5. Strive to document in a coder-friendly manner to the extent possible.
6. Cut to the chase. Don’t document what isn’t relevant to the encounter.
7. Ease the validation process by standardizing location of common key elements.
8. Perform quality assurance checks to find obvious errors and questionable transcriptions in clinical notes.
9. Make sure the note is credible in all respects.
CDI Checklist for Clinicians

58 Healthcare Business Monthly
By John Verhovshek, MA, CPC
■ PRACTICE MANAGEMENT
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
Looking for work is hard enough: Don’t hurt your chances with a wardrobe that fails to make a good impression. Here are a few in-
sights from individuals “on the front lines,” with the responsibility to fill open positions within their organizations.The consensus: Be neat, polished, professional, and not too flashy. And remember: You’re never fully dressed without a smile.
Geanetta Agbona, CPC, CPC-IEducator, CGS Medical Billing Service, Charlotte, N.C.On any interview, strive to appear polished, accomplished, skilled, and competent. Your attire should impel me to belive you are an expert in your field.
Pam Brooks, MHA, CPC, COC, PCSCoding manager, Wentworth-Douglass Hospital, N.H.I always recommend a prospective employee check out the dress code of the organization prior to any interviews. What’s deemed appropriate attire in some parts of the country may not be so appropriate in others — never assume.
Aside from that, I recommend business attire:
• For women: a dark skirt or dress trousers, light-colored blouse, and jacket or cardigan.
• For men: shirt and tie, jacket optional. No, to the golf shirt. Being overdressed is better than being inappropriately dressed.
Never wear jeans, sneakers, sweatshirts, t-shirts, or anything too short, tight, or revealing. Women should wear stockings and low heels. Keep jewelry simple. You want the interviewer to see you, and not be distracted by your outfit.
Most hospitals have rules about multiple tattoos, multiple pierc-ings, unnatural colored hair, and overwhelming cologne. I once had an asthma attack and had to usher a job candidate out of my office because she had marinated herself in cologne earlier that day.
Rhonda Buckholtz, CPC, CPC-I, CPMA, CENTC, CGSC, CPEDC, COBGC, CRC, CHPSEVice president strategic development, AAPCResearch the organization at which you are applying to learn their standards. You don’t want to out-dress the CEO, but you also want
What (Not) to Wear While Job HuntingTo play the role of a successful employee, you have to look the part.

www.aapc.com April 2016 59
to appear polished and professional. Your appearance weighs heavily on first impressions. Clean, well-pressed clothes are a must. Don’t wear heavy scents or heavy makeup that will distract interviewers. The best thing you can wear is your smile; show them that you want to be there.
MariaRita Genovese, CPC, PCSAdministrator, oncology revenue cycle, Thomas Jefferson University, Philadelphia, Pa.What to wear to an interview:
• Clean, well-fit clothing — nothing tight or clingy• Ladies: Wear a dress/skirt with a jacket or cardigan sweater, or a
pantsuit• Men: Wear a suit and tie. A cardigan sweater in place of a jacket is
acceptable.• Appropriate footwear: no sneakers, platform heels, or flip-flops• Stockings for ladies• Moderate makeup• Moderate jewelry — nothing that jangles• No colognes or other fragrant products — someone at the office
may be allergic• A smile
Ellen Maura Wood, CPC, CMPE Practice manager, Seacoast General Surgery, Dover, N.H. No matter if you’re dropping off your resume cold or going to an interview, dress professionally. That means business attire. For a man: blazer, tie, and pressed pants. For a woman: stockings (no open toe shoes or flip flops), pressed pants or dress/skirt. Dresses and skirts shouldn’t be much above the knee. I look at fingernails, too. We work in the medical field, so cleanliness is important. When I went to business school over 30 years ago, I learned something that always stuck with me: Clean and polish your nails before an interview. I’ve done it before every interview I’ve ever gone to.
I used to tell my daughters, even if they were just getting after-school jobs, dress like you want the job!
John Verhovshek, MA, CPC, is managing editor at AAPC and a member of the Hendersonville-Asheville, N.C., lo-cal chapter.
The best thing you can wear is your smile; show them that you want to be there.
To discuss this article or topic, go to www.aapc.com Job Huntingist
ock.c
om/M
ichale
l Jung
PRACTICE M
ANAGEMENT

60 Healthcare Business Monthly
NEWLY CREDENTIALED MEMBERS
Magna Cum LaudeMagna Cum LaudeMagna Cum Laude
Ajomol Atlin, COC-AAlecia Cartwright, CPC, CRCAzaruddin Mahammad, CICBaswaraj Banjanagari, CICJennifer Borsody, CPC-AJessa May Taniñas, CPC-AJoan Opleda Salvatus, CPC-AJoseph Paul, CICJulia Haun, CPCJyothirmayee Gaddamedi, CPC-A, CICLalitha devi Veeramsetti, CICLeigh Ann Mahjoobi, COC-ALinabelle De Venecia, CPC-ALindsey Wheeler, CPC-AMaria Orta, CPC-AMary Gannon-McMurry, CPC-APadmavathy Narayanan, CICPradeep Kumar Gattlola, CICPradeep Pagidimarri, CICRaja Shekar Devanaboina, CPC-A, CICRajesh Kumar Natchimuthu, CPC, CICRakesh Gaddam, CICSanthosh Reddy Mandadi, COC-A, CICShiela Marie Ong, CPC-ASona Thirumoorthy, CICSuganya Subramanian, CICSwapna Marepally, CICSwathi Gaddam, CICVikram Reddy, CICVinay Kumar Daram, CIC
CPC®CPCCPCAarti B Menghrajani, CPCAbraham Grimas, CPCAdam Walker, CPCAfrica Ware, CPCAgnieszka Popowski, CPCAimee Haydel, CPCAlex Gonzalez, CPCAlfredo Nasiff Hadad, CPCAlisa R Hillock, CPCAlisha Eifert, CPCAltrese Jacob, CPCAlyson Merrill, CPCAmber Meade, CPCAmell M Solano, CPCAna Cruz, CPCAnays Fundora, CPCAndrea Checovich, CPCAndrea Hochstatter, COC, CPC, CEDCAnessa Marie Uberroth, CPCAngela Barber, CPCAngela Jean Hall, CPCAngelique Rodriguez, CPCAnna Melendez, CPCAnuradha Lakshminarayanan, COC, CPCAramis Paz, CPCArathy Radhakrishnan, CPCArlene Padron Alfonso, CPCAshley Creel, CPCAshley Meyers, CPCAshok Reddy Marella, COCAthena Parscal, CPCAutumn Cope, CPCAwilda Agosto, CPCBarbara Helen Sweeney, CPC
Becky Quarry, CPCBelinda Phelps, CPCBelkis Diaz, CPCBernadine Bell, CPCBirgit Otto, CPC, CPMABiswajita Lenka, CPCBree Safranski, CPCBrenda Honeycutt, CPCBrenda Keller, CPCBrenda Nielsen, CPCBrianna Guinn, CPCBrittany Etheredge, CPCBrooke Swindal, CPCCarlos Trujillo, CPCCarmen G Perez Fundora, CPCCarolyn Booker-Cruz, CPCCarrie M Hook, CPCCassandra J. Whitehead, CPCCassie Ihrke, CPCCatherine Lynn Chidzik, CPCCecilia Harris, CPCCecilia Sosa, CPCCeleste Sowder, CPCChaine Socorro, CPCChandrani Roy, CPCChanthini Kothakulamparambil Venugo-palan, CPC
Chinh Nguyen, CPCChristine M Leite, CPCChristine Nguyen, CPCCiara Quarles, CPCCindy Carpenter, CPCConstance Holte, CPCCornelia Wallace, CPCCourtney Long, CPCCristina Garcia, CPCCrystal Callahan, CPCCrystal Ramos, CPCCynthia Berry, CPCCynthia R Brannock, CPCDaidy Guanche, CPCDana Birt, CPCDanielle Wilkinson, CPCDavina Manson, CPCDawn Shaw, CPCDawn Zellner, CPCDayci Torres, CPCDeanna Clunie, CPCDeborah Barker, CPCDede Kelly, CPCDenise Ehrensberger, CPCDenise Gardenia Cruz, CPCDiana Hang, CPCDiana Mahalbasic, COCDiana R Seymour, CPCDiana Roque-Gamez, CPCDonna Spurlock, CPCDonna Tabernacki, CPCDustin Berg, CPCDwaain Straker, CPCEbony Fair, CPCEbony Jones, CPCElizabeth Alfaro, CPCElizeth Milagros Garcia, CPCEmily Dillow, CPCEmily Narvais, CPCErin Brockmeier, CPCErin Kay Cox, CPCErin Puett, CPCErin Reed, CPCEuna Ball, CPCFelicia Burton, CPCFelicia M Cephus-Williams, COC, CPC,
CPC-I, CEMC, CGSCGinger Whitley, CPCHannah Gross, CPCHarish T, CPCHeather Boothe, CPCIliana Rojas, CPCJackie Anne Zupon, CPCJayanna Coleman, CPCJeanetta Hambrick, CPCJennifer Guffey, CPCJennifer Jarrard, COC, CPCJennifer Robbins, CPCJennifer Rose Huffman, CPCJessica Brown, CPCJessica Francis, CPCJody Tenold, CPCJohna Popovich, CPCJosephinemary Samuelasirvatham, COC, CPC
Julia Nicole Duran, CPCJulie Ann Bradley, CPCKaren L Becraft, CPCKaren Lynn Edgar, CPCKaren Megge, CPCKaren Ranero, CPCKatherine Mallette, CPCKathleen Lyman, CPCKathryn Walter, CPCKathy Bates, CPCKatie Campbell, CPCKatrina Rieta, CPCKeesha L Coram, COC, CPC, CRCKeisha Martinez, CPCKelli Bearden, CPCKelli Kienker, CPCKelly Bronnenberg, CPCKelly Thrower, CPCKemi J Hubbard, CPCKhristina Valdez, CPCKimberley Ramsey, CPC, CPBKimberly Mahany Dixon, CPCKimberly Porter, CPCKimberly Williams, CPCKristen Dennis, CPCKristin Birmingham, CPCKristina Marthaler, CPCKristina Martinez, CPCKristy Nickson, CPCLabiba Alam, CPCLameka Michael, CPCLana Jean Groth, CPCLatoya Calloway, CPCLaura Cirilli, CPCLaurie Robertson, CPCLaxmibhavani Dharavathu, CPCLeanna Manley, CPCLena Rae Ragland, CPCLeslie Koehn-Fertel, CPCLeticia L Gonzalez, CPCLina E Rivero, CPCLinda Grimes, CPC, CPC-P, CPMALisa Alonso, COC, CPCLisa G Palmer, CPCLisa K Wilson, CPCLisa Lash, CPCLisa M Cona, CPCLorenza Ortiz, CPCLoretta Lee, COCLori Cronise, CPCLori Hillman, CPCLori Taggart, CPCLori Warren, CPCLorie Ann Fitzer, CPC
Lorretta Maria Dixon, CPCLucy Mitha, COC, CPCLuz M Paras, CPCLynette Lara, CPCMandy Norris, CPCMarcella Soto, CPCMarcia Hernandez, CPCMargaret Ann Wilson, CPCMaria De Luna, CPCMaria Eugenia Trujillo, CPCMaria Lorena Angel, CPCMaria Saura, CPCMarianela Delgado Medina, CPCMarielena Urquiola, CPCMarla Vance, CPCMarvette Sherell Smith, CPCMary Ashley Adkins, CPCMary Duke, CPCMary V Balentine, CPCMasheena Larkin, CPCMayda Rodriguez, CPCMayon Marie Tahal, CPCMeagan Peluso, CPCMelisa Falcon Garcia, CPCMelissa Leeds, CPCMelissa A Cruz, CPCMelissa F Young, CPCMelissa Schave, CPCMelodie Ortiz, CPCMeredith Ray, CPCMichelle Brewer, COC, CPCMichelle Pena, CPCMichelle Trotter, CPCMila Nazarenko, CPCMirtza Pi, CPCMohamed Fayiz Nalakath Kuttikattil, CPCMonica D Henderson, CPCMonica Trumpler, CPCNahed Ibrahim, CPCNanette Turner, CPCNatasha Brown, CPCNora Nervar Balabarcon, CPCNorma Francisco Bonus, CPCOsleidys Perez, CPCPatricia Clarke, CPCPushpaLatha Subbiah, COCRachel Stone, COC, CPCRajat Kumar Yadav, CPCRajesh Nakka, COCRandi Butcher, CPCRanney Romero, CPCRasathithecla Lucas, COC, CPCRashana I Smith, CPCRegina Hollins, CPCRenee Garrison, CPCRizelle Mauleon, CPCRobert Warburton, CPCRonda Eden, COC, CPCRoxana Perez, CPCRuthie joy Punay, CPCSafal Chariyampadath, CPC, CPC-PSamantha L Popella, CPCSamantha Carlton, CPCSamantha Ruiz, CPCSantina Mayo, CPCSantor LaRay Wayans, CPCSarah Leggitt Sones, CPCSaranya Ganesan, COC, CPCShahid Mahmood, CPCShameka Houston, CPCShanmuga Nagarajan Chickannan, COCShannon McNamee, CPCSharon Winters, COC, CPC
Shashikumar Natarajan, COC, CPCSherry Ann Coates, CPCSheyla Reyes, CPCShiCoah Yarbrough, CPCShimeka Johnson, CPCO, CPC-P, CPB, CPMA, CPPM
Sima Kaufman, CPCSindhuja Chalamalasetty, CPCSonja Winstead, CPCSonya Gee, CPCSravana Jyothi Vedurupaka, CPCSrinivasan Arumugam, CPCStacie Watie, CPCStephanie Anderson, CPCStephanie Durboraw, CPCStephanie T Baumert, COC, CPCSteve John Meyer, CPCSubhashini Manohar, CPCSuneethi Venkatesh, COC, CPCSureshgujjanapudi Gujjanapudi, CPC, CPC-P
Susan Anding, CPCSusan Smith, CPCSusanne J Tuck, COC, CPCSusanne Rancourt, COC, CPCSushma Bellaby, CPC, CPBSusithra Somasundaram, COC, CPCSuzanne Murphy, CPCTammy Ragsdale, CPCTammy Schmarkey, CPCTara Hamilton, CPCTasha Turner, CPCTeneka Taylor, CPCTeresa M Stenquist, CPCTeresa Mercer, CPCTeresa Soffa, CPCTeri L Roath-Baum, CPCThiencuong Nguyen, CPCTiffany Asher, CPCTina Knospe, CPCTonya L Johnson, CPCTonya Millsap, COCTracy Y Riedl, CPCTramaine Lewis, CPCTsion Tesfaye, CPCUyen Hodgdon, CPCVicky Marie Bowen, CPCVudari Kalpana, CPCWanda J Russell, CPCWendy Bahaw, CPCYajaira D Vazquez, CPCYaneris Lopez, CPCYaney Curbelo, CPCYara Romain, CPCZia Ahmed, COC
ApprenticeApprenticeApprenticeAalapati Anusha, COC-AAbhilash S, CPC-AAbhisha Surabhi, COC-AAbigail Rich, CPC-AAblessin Johnson, CPC-AAche. Shravan, CPC-AAda Chin, CPC-AAdam Gold, CPC-AAdapa Deepak Kumar, CPC-AAdele Ciruti, CPC-AAdrianna Brinker, CPC-AAdrianne Hughes, CPC-AAdrienne Lozano, CPC-A

www.aapc.com April 2016 61
NEWLY CREDENTIALED MEMBERSAdunola Ademiluyi, CPC-AAfrah Abdulkareem, CPC-AAfshan Shamim, CPC-AAhmed Al Saedi, CPC-AAhmed Unnisha Shaik, COC-AAhuva Sclair, COC-AAide Romero, CPC-AAiza Uy, CPC-AAjesh Jose, COC-AAkash Jain, CPC-AAkhila Addhu, COC-AAkkamolla Santhosh Reddy, COC-AAkshaya Ashok Kumar, CPC-AAkshaya Penkar, CPC-AAlan Willoughby, CPC-AAlberto Alfonso, CPC-AAlegria Edono Mallorca, CPC-AAlejandra McClain, CPC-AAlejandra Torres, CPC-AAlessandra Bentley, CPC-AAlex Walker, CPC-AAlex Hoover, CPC-AAlexa Banegas, CPC-AAlexandra Mickiewicz, CPC-AAlfie Acabo, CPC-AAlfred Blas, CPC-AAlice Li, CPC-AAlice Mierzwa, CPC-AAlicia Edwards, CPC-AAlicia Gray, CPC-AAlicia Scrip, CPC-AAlicia Shevokas, CPC-AAlisa Kolomenskaya, CPC-AAlison Bryan, CPC-AAlison McKinney, CPC-AAlissa Rosario, CPC-AAllyson Schulte, CPC-AAlma VanWinkle, CPC-AAlwen Alilaen Elevado II, CPC-AAlyssa Woodward, COC-AAlyxandria Guzman, CPC-AAmali Auxilia, CPC-AAmanda Casner, CPC-AAmanda Conklin, CPC-AAmanda Gutzmann, CPC-AAmanda Loy, CPC-AAmanda Lupfer, CPC-AAmanda Raemhild, CPC-AAmanda Smith, COC-AAmarendra Nath Bai, COC-AAmarjeet Singh, CPC-AAmber Perez, CPC-AAmber Todi, CPC-AAmber Underwood, CPC-AAmir Khan, CPC-AAmit Kumar Shrivasta, CPC-AAmy J Hull, CPC-AAmy Keeney, COC-AAmy Messacar, CPC-AAmy Phillips, CPC-AAmy Simon, CPC-AAmy Speidel, CPC-AAmy Trujillo, CPC-AAnagha Bhusari, CPC-AAndrea Boger, CPC-AAndrea Dixon, CPC-AAndrea Johnson, CPC-AAndrew Bulgin, CPC-AAnesha Spencer, CPC-AAngela Banks, CPC-AAngela Kaatz, CPC-AAngela Zito, CPC-AAngelica Macalalag, CPC-A
Angelina Mullins, CPC-AAngelo Alpuerto Hernandez, CPC-AAngie Sanders, CPC-AAnil Kumar Boorgula, COC-A, CPC-AAnil Kumar Boorgula, COC-A, CPC-AAnil Shreedhar Shet, CPC-AAnil Singh, CPC-AAnita Anderson, CPC-AAnitha H.K, CPC-AAnjana K R, CPC-AAnjana Seena, COC-AAnna Barrios, CPC-AAnna Lachance, CPC-AAnna Shvedchenko, CPC-AAnthony Campbell, CPC-AAnthony Shepps, CPC-AAnuja Lad, CPC-AAnuradha Singh, COC-AAnurag Anant Jadhav, CPC-AAnurag Malik, CPC-AAnurag Sharma, COC-AAparnanagaveni Vennapusapalli, CPC-AApoorva Srivastava, CPC-AApril Rojas, CPC-AApril Zabele, CPC-AArchana Poola, CPC-AArchival Sotto Nadal Jr, CPC-AArdith Charles-Harris, CPC-A, CGSCArelia Huff, CPC-AArjun Kumar, CPC-AArlene Santos, CPC-AArlhyn Aguirre, CPC-AArsha George, COC-AArti Singh, CPC-AArun Raju, COC-AArun T Raj, COC-AAruna Selvaraju, CPC-AAshita Patel, CPC-AAshlee Anderson, CPC-AAshlee Harover, CPC-AAshley Ischar, CPC-AAshley Marie Ambeau, CPC-AAshley Mekmorakoth, CPC-AAshley Michelle Culbreth, CPC-AAshley Nicole Riley, CPC-AAshley Pineda, CPC-AAshlyn Breanna Tanner, CPC-AAstha Bhatnagar, CPC-AAswinkumar Swarnaraj, CPC-AAthira Chelladwora Raj, CPC-AAthira G, COC-AAudra Clarke, CPC-AAudrey Precious Raquinio, CPC-AAustin Wentworth, CPC-AAuyna Bethancourt, CPC-AAzeemuddin Mohammed, CPC-AAzharuddin Mohammed, COC-ABalabhadra Misra, COC-ABalaji Kathirvel, COC-ABandaru Chaithanya, COC-ABanupriya Mohanam, CPC-ABarb Dufresne, CPC-ABarbara Blood, CPC-ABarbara Young, CPC-ABaskar Balaji, COC-ABaskaran R, COC-ABeeram Sampath Kiran, CPC-ABelinda Mabry, CPC-ABellamkonda Naresh, CPC-ABency Mol, CPC-ABeth Shaddock, CPC-ABeverly Benito, CPC-ABhagirath Reddy Palla, COC-A
Bhagwant Singh, CPC-ABharath Devendhiran, CPC-ABhaskar Reddy M, COC-ABhavya Suren, COC-ABhoopal Reddy Katipally, COC-ABhulaxmi Garikapati, COC-ABillie Persons, CPC-ABindhu Sundaram, CPC-ABlanca Patricia Baker, CPC-ABlerina Ducellari, CPC-ABobbili Sunil, CPC-ABonnie Wallace, CPC-ABonnie Yoder, CPC-ABrandy Marten, CPC-ABrandy Mills, CPC-ABriana Gilbert, CPC-ABridget Ferland, CPC-ABridget Hrycek, CPC-ABridget Miller, CPC-ABrie Patterson, CPC-ABrighty Devakirubai, CPC-ABrittany Howell-Blaszczyk, CPC-ABrittany Wassell, CPC-ABrittney Miller, CPC-ABrittney Pritchett, CPC-ABryan Pfeiffer, CPC-ACandi A. Anderson, CPC-ACarine Kimon, CPC-ACarla Martinez, CPC-ACarlee Lugo, CPC-ACarlie Scholer, COC-ACarly Batzel, CPC-ACarol Bagal, CPC-ACarol Berry, CPC-ACarol L Keyes, CPC-ACarole Flagler, CPC-ACasey Thavy, CPC-ACassandra Forsman, CPC-ACassey Hattaway, CPC-ACassie Anderson, CPC-ACatherine Foster, CPC-ACatherine Renteria, CPC-ACathy Halstensgaard, CPC-ACelia Mendez, CPC-AChaitali Ambekar, CPC-AChandralekha Chinnakannu, COC-AChandraSekhar Raju, CPC-AChandrasekhar Singh, CPC-ACharizze Anne Sauro, CPC-ACharles Allender, CPC-AChelsea Thomas, CPC-AChenchaiah Ramisetti, COC-ACherish Scott, CPC-ACheryl Rockwell, CPC-ACheryl Tinsley Hayes, CPC-AChethana Gobbali Kumara, CPC-ACheyenne Jorgensen, CPC-AChristina Coleman, CPC-AChristina Fuller, CPC-AChristina O’Marrah, CPC-AChristine Stello, CPC-AChristopher Dukart, CPC-ACielo Marcelino Hipolito, CPC-ACindy Brister, CPC-ACindy Howard, CPC-ACindy McNamara, CPC-AClarence Alindogan Nicolas, CPC-AClaudia Nogueira, CPC-AClaudia Salcedo, CPC-AColby Ware, CPC-AColleen Blevins, CPC-AConnie Jones, CPC-AConnie-Diane Whalen, CPC-A
Courtney Dumais-Myers, CPC-ACourtney Johnson, CPC-ACrystal Marie Akins, CPC-ACynthia Ballard, CPC-P-ACynthia Cates, CPC-ACynthia Dawkins, CPC-ACynthia Rodriguez, CPC-ACynthia Schmied, CPC-AD.Mukesh Kumar, CPC-ADaisy Santiago, CPC-ADamon W Cohoon, CPC-ADanaize Garcia, CPC-ADanavian Sims, CPC-ADanelle Davis, CPC-ADaniel Hunt, CPC-ADaniel Salazar, CPC-ADanielle Freeman, CPC-ADanielle Stokman, CPC-ADanyel Speaks, CPC-ADara Crookshank, CPC-ADarlene A Delibro, CPC-ADarshana Nagwenkar, CPC-ADavid Hufham, CPC-ADavid Jaime, CPC-ADavid Jr Ruiz, CPC-ADawn Gabree, COC-ADawn Hubbard, CPC-ADawn Lynn Klyczek, CPC-ADawn Potter, CPC-ADayami Estrabao, CPC-ADeanna Elizabeth Perry, CPC-ADeanna K Iwen, CPC-ADeAnna Lerschen, CPC-ADeanna Marie Duquesne, CPC-ADebbie Peck, CPC-ADebbie Schreppel, CPC-ADebi Metevia, CPC-ADeborah Hanner, CPC-ADebra Downham, CPC-ADebra Grabowski, CPC-ADebra McMahon, CPC-ADebra Sargent, CPC-ADebra Whittum, COC-ADee Hart, CPC-ADeepa Narayanagowda, CPC-ADeepak Saxena, CPC-ADeepti Katyal, CPC-ADeLisa Smith, CPC-ADetra Parker, CPC-ADharmateja Pennada, COC-ADiana Kim Hager, CPC-ADiana Nicholson, CPC-ADianne Henson, CPC-ADianne Potochniak, CPC-ADilip Chaudhari, CPC-ADinah St. Victor, CPC-ADivya Chollati, CPC-ADivya Francis, CPC-ADivya Manisi, CPC-ADivya N, CPC-ADivyabharathi Selvaraj, CPC-ADizon Winnifred, CPC-ADolly Flowers, CPC-ADongababu Bandaru, CPC-ADonn Polson, CPC-ADr Poornima, COC-ADurgadevi Ramalingam, CPC-AEddagotla Himan Kumar, CPC-AEdna Louise Compton, CPC-AEdward Masong Tenorio, CPC-AEfstratia Eleftheriou, CPC-AEinat Berkman, CPC-AElias Abelardo Bequer, CPC-A
Elizabeth Allison, CPC-AElizabeth Beardsley, CPC-AElizabeth Green, COC-A, CIRCCElizabeth Molina, CPC-AElizabeth Nash, CPC-AEllen R Beason, CPC-AEllyssa Norkin, CPC-AElvira E Lara, CPC-AEmily Dunbar, CPC-AEmily Robinson, CPC-AEmily Russo, CPC-AEric Flores, CPC-AErika Joy Arrieta, CPC-AErika Lemieux, CPC-AErika Parsons, CPC-AErika Ravenscraft, CPC-AErin Coleman, CPC-AEstrella Tapec, CPC-AEva Silegy, CPC-AEvelina Krivtsova, CPC-AEzhildevi Mohanmari, CPC-AFaith Yonzon Secula, CPC-AFrennylyn Gambayan, CPC-AG Shiva Shankari, CPC-AGabriell Johnson, CPC-AGail Gaul, CPC-AGary Neu, CPC-AGayathri Arya. K, COC-AGayatri Atikela, COC-AGeetha K, COC-AGenine Santiago Neo, CPC-AGentry Jackson, CPC-AGerardo Labra, CPC-AGhouse Mohammad, COC-AGilberto Alcocer III, CPC-AGlenn Mark Najorra, CPC-AGleybis Martinez, CPC-AGouthami Rakasi, CPC-AGovil Packia Muthu Pounraj, CPC-AGowtham Kumar Inaganti, COC-AGowthaman Inbaraj, CPC-AGrace Lebeda, CPC-AGraciela Flynn, CPC-AGretchen Stenson, CPC-AGuohong Li Watkins, CPC-AHammurabi Kabbabe, CPC-AHarendra Rai, COC-AHarika Kotha, COC-AHayley Simmons, CPC-AHeather Kocourek, CPC-AHeather Sinkevitch, CPC-AHeather Sweat, CPC-AHector Brea Jr., CPC-AHeidi Nystrom, CPC-AHeidi Ricks, CPC-AHelyn Adams, CPC-AHemalatha Kovoori, COC-AHemalatha Lakkala, CPC-AHemlata Sharma, CPC-AHeng Saely, CPC-AHepsibha Sanamula, CPC-AHilda Griffin, CPC-AHolly P Nelson, CPC-AHolly Rietscha, CPC-AHudson R Harris, CPC-AHusnaara Shaikh, CPC-AIan, CPC-AImran Ahmed Khan, CPC-AImran Mohammed Shaik, COC-AInga Chandler, CPC-AIvette Cano, CPC-AIvy Grace Silvestre, CPC-AJacci AR, CPC-A

62 Healthcare Business Monthly
NEWLY CREDENTIALED MEMBERSJacintha Clara Pinto, CPC-AJacob Camandona, CPC-AJacqueline Ang - Bigtas, CPC-AJaggarao Jalumuru, CPC-AJagruti Vyas, CPC-AJaime Lomax, CPC-AJakkena Purushottam, COC-AJalyn Ashley Branscum, CPC-AJama Dunn, CPC-AJamie Carney, CPC-AJamie Donnelly, CPC-AJamie Short, CPC-AJan Michael Saludar Barroga, CPC-AJana Aplin, CPC-AJane Gabriel, CPC-AJane Marie Tyler, CPC-AJanet Hosterman, CPC-AJanet Kemp, CPC-AJanet Scheltema, CPC-AJanet Steed, CPC-AJanice Diesta Go, CPC-AJanice Gentile, CPC-AJanice Wong, CPC-AJankee Patel, CPC-AJansi Venkatesan, COC-AJason Carden, CPC-AJason Maddox, CPC-AJason Smith, CPC-AJavaji Kartheek, CPC-AJayanthi Balumurali, CPC-AJayanthi Narasiman, CPC-AJayanti Kushwaha, CPC-AJazil VP, CPC-AJean Ruby, CPC-AJeff Schultz, CPC-AJennifer Holmes, CPC-AJennifer Huskey, CPC-AJennifer Lynn Prohoroff, CPC-AJennifer Miller, CPC-AJennifer Miskowsky, CPC-AJennifer Paige Golden, CPC-AJennifer Prince, CPC-AJennifer Rickards, CPC-AJennifer Sandau, CPC-AJennifer Slagle, CPC-AJennifer Ziesemer, CPC-AJenny Parkin, CPC-AJenny Wilson, CPC-AJerika Celine Matias, CPC-AJerin John, CPC-AJess Ayers, CPC-AJessica Gomez, CPC-AJessica Hamilton, CPC-AJessica Hernandez, CPC-AJessica Johnson, CPC-AJessica Nicole Litton, CPC-AJessica Reilly, CPC-AJessica Rentz, CPC-AJessica Schroeder, CPC-AJessica Short, CPC-AJessica Smith, CPC-AJessica Wilson, CPC-AJessy Ancy Varghese, CPC-AJestine Bugner, CPC-AJewel Abraham, CPC-AJiji Joboy, COC-AJill Keetch, CPC-AJill Kepner, CPC-AJill Maruska, CPC-AJincy George, CPC-AJitender Rawat, CPC-AJ’Lyn Carruth, CPC-AJo Nell Grover, COC-A
Joanna Chowaniec, CPC-AJoanna Michell Alcasid, CPC-AJoanna Ordonez, CPC-AJodi Bonham, CPC-AJodi Cihal, CPC-AJoel Arun Kumar Rajarathinam, CPC-AJoemar Maglalang, CPC-AJohanna Luber, CPC-AJohn Ivan Reyes Torres, CPC-AJoseph DeLoreto, CPC-AJoseph Garrett, CPC-AJoseph Linson, CPC-AJoseph Luigi Torres, CPC-AJosie Fonua, CPC-AJoy Wilson, CPC-AJoyce Bowden, CPC-AJoyce Piper, CPC-AJuan Montanez, CPC-AJudy Lyn McCue, CPC-AJudy Zamora, CPC-AJulia Keiser, CPC-AJulia Keiser, CPC-AJulia Stephenson, CPC-A, CPPMJulie Ahrendt, CPC-AJulie Dillon, CPC-AJulie Hoffman, CPC-AJulie Wieneke, CPC-AJulie Wysner, CPC-AJulissa Tuya, CPC-AJullianne Tanya Regencia, CPC-AJustin Dipiazza, CPC-AJustine Malecki, CPC-AJyothisree Vadlakonda, CPC-AJyoti Anand, CPC-AKabde Ankita, COC-AKaeylor Joseph, CPC-AKakarla Venkata Hemanth, COC-AKalpana Janagam, COC-AKalpana Kannan, CPC-AKamala Shaddock, CPC-AKara Flaugher, CPC-AKaran Shinde, CPC-AKaren Shewmaker, CPC-AKaren Wisby, CPC-AKari A. Willingham, CPC-P-AKarthik Katakam, COC-AKarthik Nalla, COC-AKarthik Raman, COC-AKassia Lynn Olszewski, CPC-AKatherine Kreamer, CPC-AKatherine Licerio, CPC-AKathleen Casey, CPC-AKathleen Murphy, CPC-AKathryn Arena, CPC-AKathy Hansen, CPC-AKatie Hoffer, CPC-AKatie Rebeca Sousan, CPC-AKatrina Medina, CPC-AKavya Allam, CPC-AKay Johnson, CPC-AKayla DeMott, CPC-AKayla Herrera, CPC-AKayla Kerns, CPC-AKayla Rice, CPC-AKayla Sauls, CPC-AKayti Shipley, CPC-AKela Hamilton, CPC-AKelli Quilici, CPC-AKellie Wilson Phillips, COC-AKelly Benoit, CPC-AKelly Black, CPC-AKelly Buchanan, CPC-AKelly Heeg, CPC-A
Kelsi Mikel Brown, CPC-AKendra Quach, CPC-AKeneath Anne Villarin, CPC-AKenneth Gary, CPC-AKenneth Jay Cabrito, CPC-AKerri Miller, CPC-AKetananandrao Jadhav, CPC-AKevin McFadden, CPC-AKevin Raj, CPC-AKhadija Bowen, CPC-AKhaleelur Rahman, CPC-AKim Johnson, CPC-AKim Lecus, CPC-AKim Piotrowicz, CPC-AKimberly Myers, CPC-AKimberly Aguirre, CPC-A, CPBKimberly Cooper, CPC-AKimberly Cotter, CPC-AKimberly Erickson, CPC-AKimberly Jones, CPC-AKimberly M Hamilton, CPC-AKimberly McLain, CPC-AKimberly Pence, CPC-AKimberly Wilson, CPC-AKira Hamill, CPC-AKirk Neal, CPC-AKolla Ravindar Reddy, CPC-AKompally Kiran, COC-AKorina Solis, CPC-AKosgi Chandana, CPC-AKothanda Raman P B, COC-AKrishnateja Kolusu, CPC-AKrista De Kerillis, CPC-AKristalyn Thompson, CPC-AKristen Machen, CPC-AKristen ONeill, CPC-AKristen Orange, CPC-AKristina Louise Crowner, CPC-AKristina Richwine, CPC-AKristine Joyce Acosta, CPC-AKruti Dineshbhai Patel, CPC-AKrystal L Libertucci, CPC-AKuldeep Singh, CPC-AKuppuswamy K, CPC-AKuril Rahul, COC-AKyla Keith, CPC-AKyle Deters, CPC-ALaarnie Mallari, CPC-ALakshmanudu Bommana Boina, COC-A, CPC-A
Lakshmisri Mariappan, CPC-ALarry Walton, CPC-ALaura Egloff-Slater, CPC-ALaura Parrish, CPC-ALaura Sinitsky, CPC-ALauren Bilbrey, CPC-ALauren Elizabeth Sherman, CPC-ALaurice Joy Micmic, CPC-ALaurie Bouzarelos, CPC-ALaurie Burrell, CPC-ALaurie Crawford, CPC-ALavanya Reddy Kandadi, COC-ALaverne Howard, CPC-ALaymar Lopez, CPC-ALeah Dormitorio Peregrino, CPC-ALeeah Harris, CPC-ALeena Gogada, COC-ALeenus Patrick Obed, CPC-ALeiann Kinder, CPC-ALeighanne Smith, CPC-ALeonard Melgarejo, CPC-ALeslee Colbert, CPC-ALeslie A Knueppel, CPC-A
Leslie Alexander, CPC-ALeslie Boyd, CPC-ALeteia Ann Holt, CPC-ALeydis Perez, CPC-ALi Shao, CPC-ALillian Thayer, CPC-ALily Thakur, CPC-ALimaris Perez, CPC-ALindleigh Wirth, CPC-ALindsey Adkins, CPC-ALindsey McKane, CPC-ALisa Arbeene, CPC-ALisa Duncan, CPC-ALisa Marie Wilson, CPC-ALisa Miller, CPC-ALisa Molnar, CPC-ALisa Pedicini, CPC-ALisa Tibbs, CPC-ALiz Crociani, CPC-ALiza Peñaflorida, CPC-ALizeth M Cruz, CPC-ALori A Kahler, CPC-ALori Azzouz, CPC-ALori Pendleton, CPC-ALoribeth Carbonell, CPC-ALorie Bryant, CPC-ALouie Allam, CPC-ALoukya Boppana, COC-ALovakumar Korumilli, COC-ALove Brunson, CPC-ALucnol Jean-Pierre, CPC-ALynda Ross, CPC-ALynette Singh, CPC-ALynne Lanneau, CPC-ALynzee Ringeisen, CPC-AM. Naga Saikiran, CPC-AMa. Ailyn Benz Nicolas, CPC-AMa. Dianne Zafe Reso, CPC-AMa. Lourdes Loyola Maglalang, CPC-AMa. Virginia Quinan, CPC-AMachangar Akshitha, CPC-AMacy Loden, CPC-AMadelyn Aldridge, CPC-AMadhu Keerthi Dhanalakota, COC-AMadhura Walke, COC-AMadhusmita Bhaisora, CPC-AMagdalena Sandu, CPC-AMagnolia T. Reyes, CPC-AMahendar Reddy G R, COC-AMahender Reddy Mechala, COC-AMahesh Boora, COC-AMahesh Jaya Poojari, COC-AMahesh Vavilala, COC-AMajlinda Laska, COC-AMaj-Maj Melendres, CPC-AMalathi Durairaj, CPC-AMalia Dyck, CPC-AMalini Rishikesh, CPC-AMallorie Oneal, CPC-AMallory Pemberton, CPC-AMamatha Kalyani Yellagandula, COC-AMamatha Pulyala, COC-AManasa Devi Kancharla, CPC-AMangali Laxmaiah, COC-AManikanta Tirumala, COC-AManisha Pasupuleti, CPC-AMarcela Marie Johnson, CPC-AMarcy Smith, CPC-AMargiemel Castro Adviento, CPC-AMaria DiFiore, CPC-AMaria Elishah Ruth Corpuz, CPC-AMaria Martens, CPC-AMariam Thomas, CPC-A
Maridol Nina Mutia Taladua, CPC-AMarie C Lillie, CPC-AMariela Manzanares, CPC-AMarielle Lopez, CPC-AMarion Isaiah Dimapilis Garcia, CPC-AMarissa Lesky, CPC-AMaritzabel Garcia, COC-A, CPC-A, CRCMarkondaiah Anthati, COC-AMarlene Rogers, CPC-AMarren Gilchrist, CPC-AMary Ann Jones, CPC-AMary Ann Kompinski, CPC-AMary Boyer, CPC-AMary C. Ward, CPC-AMary Catherine Keiper, CPC-AMary Davenport, CPC-AMarye Minor, CPC-AMatin Raje, CPC-AMatta Sanjay Kumar, CPC-AMatthew Garis, CPC-AMaximilian Golec, CPC-AMeenaben Mahida, CPC-AMegan Fry, CPC-AMegan Herrick, CPC-AMegan Walter, CPC-AMeghan Morris, CPC-AMelissa Beller, CPC-AMelissa Hottinger, CPC-AMelissa Mackler, CPC-AMelissa Neuharth, CPC-AMelody Dawson, CPC-AMelody Karamba, CPC-AMeridith Roe Hall, CPC-AMerrisa Hall, CPC-AMichael Dexter Sy, CPC-AMichele Calvin, CPC-AMichele Payne, CPC-AMichele Reinert, CPC-AMichelle Chu, CPC-AMichelle Dallaire, CPC-AMichelle Norat, CPC-AMichelle Sartelle, CPC-AMichelle Zuniga, CPC-AMickey (Warren) McCandless, CPC-AMisty Yandell, CPC-AMoganapriya Prakash, CPC-AMohammad Imran Baig, CPC-AMohammed Chand Basha, COC-AMohan, CPC-AMohana Rajendran, CPC-AMohsina Hassan, COC-AMona Bedros, CPC-AMonica Smith, CPC-AMonika Shivaji Mane, CPC-AMonisha Chand, CPC-AMorgan Dodson, CPC-AMoyah Hardin, CPC-AMrignalini Ranjan, CPC-AMuppirisetty Balaji, CPC-AMuthumari Durga Nachiyappan, CPC-AMuthuselvi Gurusamy, COC-AMylinda Hawks, CPC-AN. Madhury, CPC-AN.B. Lakshmi Priya, CPC-ANadya Soho, CPC-ANaga Jyothi Swarna, CPC-ANagalakshmi Yandamuri, CPC-ANagaraju Arroju, COC-ANagaraju Mamidi, COC-ANagarjun V, COC-ANagavel Suresh, CPC-ANakicia Turner, CPC-ANakisha Murry Gordon, CPC-A

www.aapc.com April 2016 63
NEWLY CREDENTIALED MEMBERSNallavelly Smitha Varma, COC-ANancy G Fernandez, CPC-ANancy Ma, CPC-ANancy Prabha, COC-ANancy Ryan, CPC-ANandhakumar P, COC-ANaresh Krishna Pattapu, COC-ANaresh Kumar, CPC-ANaresh Nukala, COC-ANatalia Jessica Javier, CPC-ANatalie Anderson, CPC-ANatalie Savage, CPC-ANatalie Toth, CPC-ANataraj M, CPC-ANaveen Chinnam, COC-ANaveen kumar Manchala, COC-ANaveen Manga, COC-ANaveen Mokide, CPC-ANaveena Josephin, COC-ANazima Anwar Khan, CPC-ANeha Parte, CPC-ANeil Radovan, CPC-ANelaine Grace Tan, CPC-ANelissa Anne Flojo, CPC-ANess-Lee Guerrero, CPC-ANethula Sravani, CPC-ANick Fenn, CPC-ANicole Fuller, CPC-ANicole M Fuentes, CPC-ANicole Parrish, CPC-ANicole R Nichols, CPC-ANicole Robinson, CPC-ANicole Williams, CPC-ANigam Gupta, COC-ANikhil Prabhakar Patil, CPC-ANikitagangaram Palkar, CPC-ANila Sankar, CPC-ANilam Mandave, CPC-ANina Kristine Sabio, CPC-ANiquela Cole, CPC-ANirmala Boyapati, COC-ANisha Darling, COC-ANithiya K, COC-ANitin Kumar Jaiswal, CPC-ANitin Makkar, COC-ANitin Verma, CPC-ANydia Altamirano, CPC-AOlanike Dada, CPC-AOlivia Malardo, CPC-AOmkaram Venkata Ramesh Babu, CPC-AOummaly Barrie, CPC-APadma Sree Donthula, CPC-APadmanav Dash, COC-APaige Evans, CPC-APambala Rohini Priyanka, CPC-APamela Coats, CPC-AParimala Nelaturi, COC-AParminder Kaur, CPC-AParveen Banu, CPC-APatil Vaidhyanath Reddy, CPC-APatrice Feddes, CPC-APatricia Blosser, CPC-APatricia Camille Jomento, CPC-APatricia Campos Hernandez Franco, CPC-A
Patricia Depew, CPC-APatricia Flynn, CPC-APatricia Grabill, CPC-APatricia M Gibson, CPC-APatrick John Martinez Roca, CPC-APaul A Spaziante, CPC-APaul Ryan Tolentino Valencia, CPC-APaula Perry, CPC-A
Paula Richards Broek, CPC-APayton Pelto, CPC-APeddinidinesh Nageshwarrao, CPC-APeereddy Amani, CPC-APeggy Ann Hefner, CPC-APenny Hand, CPC-APhilip Don Nelo Deus, CPC-APhillip Brizendine, CPC-APinky Yadav, CPC-APolukonda Nalini, CPC-APoonam Jawala, COC-APoonam Kasawlekar, CPC-APotineni Seshendra, CPC-APradeep Reddy Thada, COC-APrajakta Digambar Bagde, CPC-APratik Parab, CPC-APrincess Joy Tumambing, CPC-APriscilla Brzezinski, COC-APriscilla Pereira, CPC-APriya Ravikumar, CPC-APriya Venuganandam, CPC-APriyanka Kumari, COC-APriyanka Rajendran, CPC-APuli Manga, COC-APuneet Gunjikar, CPC-APushpa Suralkar, CPC-APushpalatha Dhadal, CPC-APushpalatha Sivalingam, COC-AQerimane Kelmendi, CPC-AR. Radha Krishna, CPC-ARachael Mahan, CPC-ARacheal Ann Hill, CPC-ARachel Best, CPC-ARachel Hofmeister, CPC-ARachel Reyes, CPC-ARaghava Rahul Ravutu, COC-ARaghavender Dhanwada, COC-ARajalakshmi Saminathan, COC-ARajesh Puthiyedath, CPC-ARakesh Bashabattini, COC-ARakesh Rao, COC-ARakesh Varma Baindla, COC-ARamakrishna Gadasu, COC-ARamesh Cherukupally, COC-ARamesh Subramanian, COC-ARamya Srikumari Vikraman, CPC-ARamya Subramanian, CPC-ARamya Vadiraj, CPC-ARanda Dissing, CPC-ARandi Anderson, CPC-ARani Ghogare, CPC-ARani Joseph, CPC-ARanil Kalarikkal Ravi, COC-ARaquel Perez, CPC-ARasika Narayan Bagade, CPC-ARatheesh Nair, CPC-ARavali Doddi, COC-ARavi Kumar Kasanagottu, CPC-ARavi Prema, CPC-ARavikiran Yengali, CPC-ARavindra Kunwar, COC-ARaviteja Anumolu, COC-ARebecca J Oliver, CPC-ARebecca Polyniak, CPC-ARebecca Schilling, CPC-ARebecca Wells, CPC-ARegina Mary, CPC-ARekha Patel, COC-ARemi Rangasamy, COC-ARemya G Kurup, COC-ARenee M LaRocque, CPC-ARenee Fox, CPC-ARenju Raju, COC-A
Renu Jayavel, CPC-ARenuka Ellappareddy, CPC-ARenuka Modugu, CPC-AReshma Rajan, CPC-AReshmi Venugopala Prabhu, CPC-ARevathi Chitharanjan, CPC-ARex Salvado, CPC-AReynaldo Llana, CPC-ARhonda Riffe, CPC-ARichard Tamunday, CPC-ARichelle Bedoya, CPC-ARinolucy Menguito Cantong, CPC-ARiswanaParveen Iqbal, CPC-ARitesh Ranjan, CPC-ARiyaz Khan, COC-ARobert Huffman II, CPC-ARobin Bonner, COC-A, CPC-ARobin Newsome, CPC-ARobin Schermerhorn, CPC-ARobyn Hunter, CPC-ARohit Anand, CPC-ARohit Kumar. S, CPC-ARoland Hernandez Jr, CPC-ARomir Aglugub, CPC-ARona Gigante De Asis, CPC-ARoni Berlin, CPC-A, CPBRosalie Tabios, CPC-ARosalyn Balmes, CPC-ARosalyn Jamison-Charles, CPC-ARose Deleta McLean, CPC-ARosie Guerrero, CPC-ARowell Ramon Zaragoza, CPC-ARoxana Q Mendoza, CPC-ARoxane Chinoy, CPC-ARubeshkumar Gopal, CPC-ARuby Ann Moreno Non, CPC-ARuby Cabe, CPC-ARuby grace Edward, CPC-ARupali Raghunath Rokade, CPC-ARuthika Sundaragiri, CPC-ARyan Johns, COC-AS Shabana Begum, CPC-ASabnapriya Somasundaram, CPC-ASabrina Bostian, CPC-ASabrina Crawford, CPC-ASabrina Romero, CPC-ASabrina Torres, CPC-ASahana K, CPC-ASai Reddy Samala, COC-ASai Srinivas, COC-ASai Susmitha Daggubati, CPC-ASamantha Litmer, CPC-ASamantha Maguire, CPC-ASampath M, CPC-ASamrat Penjarla, COC-ASamrin Fathima Imtiaz Hussain, CPC-ASana Mirasahab Shaikh, CPC-ASandeep Sikar, COC-ASandhya Pandiri, CPC-ASandip Wagh, CPC-ASandra Bales, CPC-ASandra Kimura, CPC-ASandy Guthrie, CPC-ASanitha Narayanan, CPC-ASanjay Patil, CPC-ASanjaykumar Bhupathi, COC-ASankararao Gullipalli, COC-ASanthi Bandaru, CPC-ASanthi Muttha, CPC-ASarah Dobrovolny, CPC-ASarah Perkins, CPC-ASarath Chandran Chandran, CPC-ASaravani Thiyagarajan, CPC-A
Sarina Alexis Fullmer, CPC-ASaritha Reddy G, CPC-ASasidhar Aradyula, CPC-ASatartia Christine Collins, CPC-ASateesh Gummadi, CPC-ASathishkumar Munuswamy, COC-ASathya Priya Kittusami, CPC-ASchani Marie O’Brien, CPC-ASchmeca Lawrence, CPC-ASebi Pappachan, COC-ASeema Atul Paradkar, CPC-ASeema Kumar, CPC-ASeetha Arumugam, CPC-ASelena Cameron, CPC-ASelvarani Suresh, CPC-ASenthil Venkatesan, CPC-AShabbir Hussain K Mohammed, CPC-AShaira Myn Herrera, CPC-AShalini Dillibabu, CPC-AShanice Johnson, CPC-AShankar Chandragiri, CPC-AShannon Saunders, CPC-AShanthi Priya, CPC-AShara Elaine Klem, CPC-ASharada Kalakota, CPC-ASharat Kumar, CPC-ASharon Erickson, CPC-AShashi Kant, CPC-A, CICShashi Kiran, COC-AShawn Gantz, CPC-AShawna Wallace, CPC-AShay Peterson, CPC-ASheeba Inasu, CPC-ASheeooli Nag, CPC-ASheetal Vasoya, CPC-ASheila Lund, CPC-AShelley Shafer, COC-ASherbanu Ahmed Sayyed, CPC-ASheri Vickery, CPC-ASherita Mitchell, CPC-ASherri Pearce, COC-ASherri Shink, CPC-ASherry Bounds, CPC-ASherry De Castro Balbuena, CPC-ASherry Deig, CPC-ASheryl Denny, CPC-AShibashish Mohanta, COC-AShifa Mahzabin, CPC-AShikha Pathak, COC-AShirley Belken, COC-AShoban Raj A V, CPC-AShobhit Kumar, CPC-AShridhar Ekanekar, COC-AShrutidhar Kanhaiya, CPC-AShrutiyogesh Kini, CPC-AShumaila Ansari, CPC-AShwetha Ayathan, COC-ASibbie Pauline Frazier, CPC-ASiddhanta Mishra, CPC-ASiddhartha Madala, COC-ASilpa C, CPC-ASilvia C Quant, CPC-ASimeon Sampathkumar, COC-ASimone Thompson, CPC-ASimple Patel, CPC-ASneha Dhake, CPC-ASnehajagannath Patil, CPC-ASonakshi Singh, CPC-ASonia DaSilva, CPC-ASonia Luke, CPC-ASonia Rawat, CPC-ASoniya T Joseph, CPC-ASophia Bell, CPC-A
Soumyashree Choudhury, CPC-ASowmya Pappu, CPC-ASowmya Rangan, CPC-ASravani Goli, CPC-ASravanthi Gorusu, COC-ASreerag Vageeswari, COC-ASridhar Rao Muthineni, COC-ASriharsha Bugude, COC-A, CPC-ASrilekha Baskar, CPC-ASrinivas Kanthala, CPC-ASrinivas Reddy Narahari, COC-ASrinivas Thatipamula, COC-ASrinivas Vadde, COC-ASrinivasan Govardhanan, CPC-ASrinuvali Shaik, COC-ASruthi Reddy G, CPC-ASruthy Hari, COC-AStacey A Sam, CPC-AStacy Ann Johnson, CPC-AStarla Ehrisman, CPC-ASteffi Shae Uy, CPC-AStellaMary Arokiasamy, CPC-AStephanie Clarke-Mahoney, CPC-AStephanie Marie Reed, CPC-AStephanie Miranda Shore, CPC-AStephanie Ristau, CPC-AStephanie Wright, CPC-AStephen Dong, CPC-AStephen Ledford, CPC-ASubbaravamma Kommareddy, CPC-ASucheta Sarkar, CPC-ASuchita Gawand, CPC-ASudha Paramasivam, COC-ASudhir Kumar, CPC-ASudhir Mohan, CPC-ASujith kumar Telly, COC-ASujiva Kumari Anton, CPC-ASuman Kalaidoss, COC-ASuman Shreyaah, CPC-ASumanreddy Samala, COC-ASumit Kumar, CPC-ASumitnagsen Shishupal, CPC-ASundaravani Elangovan, CPC-ASuneel Kumar, COC-ASunil Kumar Metta, COC-ASunny Puri, CPC-ASurekha Banda, COC-ASuresh Bellam, CPC-ASurja Sikha De Roy, CPC-ASusan Gonzalez, CPC-ASusan Marini, CPC-ASusan Scott, CPC-ASusan Smith, CPC-ASusan Valadas, CPC-ASushil Kumar, CPC-ASushma Chintha, CPC-ASushma Kamuni, COC-ASuzanne Carino, CPC-ASwathi Kethireddy, CPC-ASwathi Mangelipelly, CPC-ASwathi Shyamsunder, CPC-ASwathisaranya Chitikila, CPC-ASweety Pavithran, CPC-ASyamala Chityal, CPC-ASyed Shakeer Ali, CPC-ASylvia Emmanuelle Krieg, CPC-ATadi Sivaparvathi Reddy, CPC-ATalluri Kranthi Kumar, COC-ATamara Detillo, COC-A, CPC-ATamara Ingram, CPC-ATamara Yamin, CPC-ATammy Alexander, CPC-ATammy Derk, CPC-A

64 Healthcare Business Monthly
NEWLY CREDENTIALED MEMBERSTanya Reppert, CPC-ATapaswi More, CPC-ATasha Tribune, CPC-ATaylor Brnik, CPC-ATaylor Thompson, CPC-ATehzibali Saiyad, CPC-ATeja Babu Addanki, COC-ATejpattie Lachman, CPC-ATeonna Benning, CPC-ATeresa Bezek, CPC-ATeresa Klein, CPC-ATeresa Luciana Anderson, CPC-ATerra Clarke, CPC-ATerrence Gaylon, CPC-ATerri-Karlene Peart, CPC-AThelma Josephs, CPC-ATheresa Milligan, CPC-AThota Venkatesh, COC-AThumma Thomas Reddy, COC-ATiana Broadhead, CPC-ATiff Weilbacher, CPC-ATiffany Buckmiller, CPC-ATiffany Gandy, CPC-ATiffini Hunter, CPC-ATracey Bonner, CPC-ATracey Henderson, CPC-ATracy Doyle, CPC-ATracy Holcombe, CPC-ATracy Lynn Ellis, CPC-ATracy Marshall, CPC-ATricia M Brown, CPC-ATy Moltmann, CPC-ATylar S Melton, CPC-AUday Banu Brundam, COC-AUma Devi Nagappan, CPC-AUma Maheswari, CPC-AUmesh D, CPC-AUpinder Walia, CPC-AUrszula Ochman, CPC-AUsharani Rajaraman, CPC-AV N S Manikanta Perumalla, COC-AV Chaitanya Prasad, CPC-AV Gangadhar Reddy, CPC-AV Prema Latha, CPC-AVaishnavi Deenadayalan, COC-AValerie Gillen, CPC-AValerie Morris, CPC-AVandana Teckchandani, COC-AVandana Vanam, CPC-AVanessa Blacano, CPC-AVanessa Carter Ray, CPC-AVani Kammari, CPC-AVarshil Patel, CPC-AVasanthi Paulraj, CPC-AVasanthi Ramineni, CPC-AVeena Raju, COC-AVeeralakshmi Nallaiah, CPC-AVemulapalli Namrata, CPC-AVenkata Apparao Yandrapu, COC-AVenkatachalapathy Thoppayan, COC-AVenkateswara Raju Bollepally, CPC-AVenu Gopal, COC-AVernetta Dunbar, CPC-AVeronica Bentley, CPC-AVeronica Lynn Hurley, CPC-AVevie Gilliam, CPC-AVicki Halverson, CPC-AVicki Hersey, CPC-AVictor Changanaqui, CPC-AVida Carmen Del Rio, CPC-AVidhi Shrimali, CPC-AVidhyalakshmi Ranganathan, CPC-AVidya Marudhavanan, COC-A
Vijay Kumar Dunka, CPC-AVijaya Thatha, CPC-AVijayakumar Manickam Pillai, COC-AVikki N Perry, CPC-AVincent Legaria, CPC-AVineet Chauhan, CPC-AVinni Narayanasamy, CPC-A, CRCVinothkumar Vijayarangan, COC-AVirendra Kumar Singh, CPC-AVirginia O’Brien, CPC-AVML Eswararao Gummadi, COC-AVonda Mendez, CPC-AWanda Williamson, CPC-AWendy Hoachlander, CPC-AWendy Silver, CPC-AWesley Woodard, CPC-AWillard Perry, CPC-AWilly Ferrer Pagarigan, COC-AXay Chao, CPC-AYacquelyn Sosa, COC-AYaima Ramos, CPC-AYamily Simon, CPC-AYarabolu Sahithi, CPC-AYasmin Shaik, COC-AYilian Lopez, CPC-AYn Shivakumari, COC-AYoga Priya N Narayanan, CPC-AYurisay Vergara, CPC-AYuvaraj Venkatesan, CPC-AYvonne Ogden, CPC-AZacarias Cometa, CPC-AZaria Morales, CPC-AZayd Hamza, CPC-AZoila de La Cruz, CPC-AZullyn Ball, CPC-A, CPMA
SpecialtiesSpecialtiesSpecialtiesAbhinav Kumar Maurya, CPC-A, CICAfiya Richards, CPC, CPMAAileen Panganiban, CICAjudia Rupal Damjibhai, CICAlexandra Garkey, CPBAlexis Perez, CPBAlfredo Ramones, CICAlisa Hermansen, CPC, CPC-I, CRCAlva Elano, CRCAlvin Cyrel Albino, CICAmaechi Lawrence Ofunne, CPC, CPMA, CEMC, CGSC, CPRC
Amanda Castro, CPBAmanda Proctor, CPC, CRCAmit Dhingra, CICAmy Fields, CPC, CRCAmy M Decker, CPC, CRCAmy Powell Gross, CPB, COBGCAmy Shilliam, CPC, CPCOAmy Walker, COC, CPC, CPB, CPMA, CEDC, CRC
Anand Babu Ponnusamy, COC, CPC, CICAnanda Kumar, CPC, CRCAnandhan Sivagnanam, CPC, CPMAAndrea Crowe, CPB, COBGCAndrea Mitchell, CPC, CRCAngela D Brown, CPC, COSCAngela Larsen, CPC, CRCAngela S Romero, CPC, CEMCAngela Swartz, CPC, CPBAngelica Gatchalian, CICAngelique Wilson, CPC, CRCAnirudh Ekbote, CPC, CIC
Ann Wurtinger, CPC, CICAnne Brown, CPC, CPB, CPMA, CIMCAnne C Strout, COC, CPC, CRCAnne Turla Solomon, CICAntoinette Hill, CRCAnuradha Sankarraj, CICAnusha Bonasu, CICAparna Ravinuthala, CRCApril Christine Adams, CPC, CRCAraceli Linn, CPC, COBGCArejay Tabaquero, CRCArisa Lynn Widrick, CPC, CPMAArlene E Wilkins, CPC, CRCAsaithambi Dhanapal, COC, CPC, CICAshfaq Mohammad, CICAshlea Kerley, CPCOAshvini Arun Jagtap, CPC-A, CICAsokar Arasu, CPC, CPMA, CANPCAudrey Bergstrom, CPBAvinash Daripally, CICBarbara A Williams, CPC, CRCBarbara Gonzalez, COC, CPC, CPMA, CRC
Barbara Reyes, CPC, CPMABart Stein, CPC, CPCO, CEMCBecky Bertrand, CPC, CEMCBecky Dunn, CPCOBelissa Cipreni Thompson, CRCBeth Ann Buchanan, CPC, CANPCBeth Anne Hickey, CPC, CFPCBhaskar Kolli, CICBhuvaneshwari Palanisamy, CICBianca Otto, CPMABirgit Otto, CPC, CPMABlummenroth Otto, CPMABrenda Brock, CPC-A, CPBBridget Jones, CPC, CRCBridget Nutter, CPC, CPBBronwyn Hadlock, CPCOC Juliette Morell, CPC, CPMACamille VanDerSteen, CPC, CIRCC, CCCCandice Dyxse Czelusniak, CPC, CRCCara Erlenwein, CPC-A, CHONCCaren Joy Mesias, CICCarey Ketelsen, CRCCarla B Williams, CPC, CEMC, CGSCCarletta Ellen Vasknetz, CPC, CPMACarol Sager, CPCOCaroline Faulkner, CICCaroline R Epperly, CPC, COSCCarrie E Caldewey, CPC, CPMACatherine A Phipps, CPC, CPMA, COBGC, CRC
Cathy L Smith, CPBChad Benjamin Peterson, CPC, CEMCChad Tubbs, CIRCCChaitanya Pamba, CICChandra Lynn Stephenson, COC, CPC, CPCO, CPB, CPMA, CPC-I, CANPC, CCC, CEMC, CFPC, CGSC, CIC, CIMC, COSC, CRC
Chandrashekar Reddy Muttannagari, CICChaniece Evans, CPC-A, CPMACharles Solomon Raja, CPC, CPMA, CGSC
Charles Zulauf, CPC, CICCheryl Bendana, CICCheryl Ben-David, CPC, CRCCheryl R Berzat, CPC, CPMA, CIMCCheryl Reynolds, CPC, CRCChristine Coppola, CPC, CRCChristine Peterson, CPC, CEMCChristine Smith, CPC, CRC
Christy Szolis, COC, CPC, CRCCindy Nixon Hall, CPC, CGSCCindy Y Lopez, CPC, CPMAClemente Guido, CPBCourtney Jones, CPC, CPCOCrystal Romat, COC, CPC, CRCCynthia Leslie, CPC, COBGCCynthia Lynn Hubbard, CPC, CGICDana Radack, CPC, CRCDaniel Richard Francis, COC, CPC, CICDaniel Rowden, COC, CPC, CPCO, CPMA, CIC
Daniela Simoski, CPC-A, CPBDanielle Ann Misin, CPC, CPMADanielle Shanklin, CEDCDarby Amezcua, CPPMDarwin Roque Santos, CICDawn Lambert, COC, CPPMDawn M Fenwick, CPC, CPBDeanna Householder, CPBDeborah Lloyd, CPC-A, CRCDebra Ann Keyes, CPC, CCCDebra Johnson-Phythian, CPMA, CRCDelia Delatorre, CRCDenise Majoris, CPC, CRCDiane Gotkin, CPC, CRCDiane Herbeck, CPC, CPBDiane Walczak, CPC, CPMA, CUCDivya G Gopinathan, CRCDivya Jyothi Gadapa, CICDonita Mallak, CPC, CPB, CGSCDonna Barrameda Cabugos, CRCDonna Lynn Barker, CPC, CPCO, CPMA, CPC-I
Donna Stefonetti, CRCDoris V Branker, CPC, CIRCC, CPC-I, CANPC, CEMC
Durga Devi, CICDwijesh Udvij, COC, CPC, CICEdward Bosita Ringor, CPC, CRCEileen Pinares, CPC, CPMA, CPC-I, CRCElaine Fischer, CPC, CRCElan Neuman, CPPMElizabeth A Williams, CPC, CPBElsa Brinkman, CPC, CGICEnriqueta Almeida, CPC, CPMA, CPPMEric Stephens, CPPMErina Master, CPPMErlinda S Balaan, CPC, CPEDC, CRCErra Samatha, CICErwin Salud, CICEsther Walker, CPBEvelynn McCulloch-Owens, CCS, CPC-A, CRC
Fallon Charisse Brown, CPC, CPMAFasiya Ahamed, CPC, CPMAFathima Begum Jaffer ali, CRCFrances Easter, CRCGaddala Jhansirani, CICGadeela Narender Reddy, CICGail A Volpi, COC, CPC, CIC, CRCGail Bricker, CPC, CPBGanesh Bhoje, CPC, CICGolla Pavani, CICGowsalya M Murugesan, CRCGraciela Alvarez, CPC, CPMAGuia Zhao, CPC, CICGurram Sudhaveeru, CICHanna Roman, CRCHannah Howald, CPC, CPMA, CPPMHarika Sambu, CICHarikrishna Soorishetty, CICHarriet Thomas-Fryer, COC, CPC-P,
CPMA, CRCHeather McCallum, CPC, CCCHelen Kirkland, CPBHilda Garcia, CPC, CPMAHillary Julien, CPCOHimanshu Sharma, CPC-A, CICHollie Lindley, CPBImamsaheb Shaik, CICInay Iriban, CPC, CPMAIndhira Kalaiparthiban Rajendran, CICInes Agnes Morales, CICIzel Silva, CPC, CPMA, CRCJade Ariel Reeves, CPC, COBGCJagjeet Singh, CICJamie Addler, COC, CPB, CPMAJamie Jo Pool, CPC, CPBJamie Taylor, CPBJan Lambert, CRCJan Marie Flanders, COC, CPC, CASCCJana Gustafson, COC, CPC, CPCO, CPMA, CRC
Jana Morgan, CPBJanice Douglas, CPC, CPMA, CEMCJanice Raffa, CPC-A, CRCJanis Stelzner, CPC, CRCJason Knowles, CPCOJaveed Mohamed Kalil, CPC, CICJayalakshmi Kulanthaimani, CRCJayesh Ramteke, CPC, CRCJefferson Esperida, CRCJelene Roxas, CPBJennie E Moody, COC, CPC, CRCJennifer Kniffen, CPC, CGSCJennifer L Deal, CPC, CPMA, CEMCJenny Harvey, CPC, CPMAJerame Capacia-Castro, CRCJessica Fenolio, COC, CPB, CASCCJhan Jester Solmoro, CPC-A, CICJoan Aileen Del Mundo, CICJoan M Bartholomew, COC, CPC, CRCJoan Marie Dion, CPC, CRCJodi Long, CPBJody Hart, CPC, CRCJody Mortensen, CPC, CEMCJohn Philip Martinez, CICJohn Ray Elders, COC, CRCJohn Sauder, CPC, CPPMJonel Gomez, CPCOJoseph Hughes, CPPMJoy Anne Monteverde, CRCJoyce Daquipil, CICJudith Andrea Facey, CPC-P, CRCJudith Carol Quesnel, COBGCJudybeth Fernandez, CPC, CPC-P, CRCJulia Brauer, CPBJulianne Thomas, CPC, CRCJustine Basa Asilo-Daelo, CPC, CPMAKamaal Ahmed, CICKaren Fan, COC, CPC, CRCKaren Summers Clinard, CPC-P-A, CRCKaren Tinoco, CPC, CPMA, CRCKaren Webb, CPC, CANPC, CIC, CPCDKaren Worrell, CPBKaren Y Manigault, CPC, CPMA, CEDC, CEMC
Kari Leigh Giles, CPC, CRCKarthick Jayaraj, CPC, CEDCKarthikeyan Thandapani, CICKasinath Thalikota, CICKathleen Guzzi, CPC, CICKathleen M Skolnick, COC, CPC, CPCO, CPB, CPMA, CPPM, CPC-I, CEMC, CRC
Kathryn Jones, CPC, CRC

www.aapc.com April 2016 65
NEWLY CREDENTIALED MEMBERSKathryn Joyce Phillis, CPC, CPB, CPC-IKathryn R. Melton, CPC, CRCKathy LaPierre, CPC, CPMA, CEDC, CEMC
Katie Lee Cheong, CPC, CENTCKatrina Woodring, CPC, CPC-P, CPC-I, CRC
Kawana N Scott, CPC, CPMA, CEDCKayla Williams, CPC, CEDCKellie Louise Zimmerman, CPC, CRCKelly Moritz, CICKelly Johnson, CPC, CPC-P, CENTC, CFPC
Kelly McCormick, CPC, CPC-P, CRCKelsey Storey, CPC, COBGCKendra Hamiel, CPBKilona Kara, CPC-A, CRCKim F Turner, CPC, COSCKim Fields, CPC, CRCKim Montenegro, CPC, CPMA, CPC-I, COSC, CSFAC
Kim Morvant, CPC, CRCKimberly J Fields, CPC-A, CPMAKimberly Salazar, CRCKimberly T Dues, CPC, CRCKimothy Williams, CPC, CPBKristina Bolio, CRCKristina Marie Metrejean, CPC, CPBKristine Diana West, CPC, CPMAKurt Alyn Kaskie, CPC, CRCKushali Cherukumalli, CICKynet Watkins, CPCOLaBrena Settles, CPCOLanileen Caisip, CICLarry Roberson, CPC, CPMA, CRCLaura Duffy, CPC, CPMALaurie Elliott, CPBLeann Haven, CPPMLenette Russell, CPBLeyiset Crespo, CPC, CRCLiana Urdanivia, CPC, CPMALibest J Larez, CPC-A, CPB, CPMALilian Russo, CPC, CPMA, CUCLina Liza Arcilla Alcances, CPC, CPC-I, CIC
Linda D Hall, CPC, COSCLinda Manuli Huckin, CPC, CICLinda Marshburn, CPPMLinda R Farrington, CPC, CPMA, CPC-I, CRC
Linda Thomas, CPC, CRCLisa Maria McIlquham, CPBLisa Bradshaw, COC, CPC, CHONCLisa Griswold, CPC, COSCLisa Janell Fouts, CPC, CPMALisa L Rogers, CPC, CRCLisa M. Noles, CPC, CPCO, CPC-ILisa Magnotti, CPC, CRCLisa Purnell, CPC, CPCO, CPMA, CRCLisa Sandusky, CPC, CPMA, CANPCLisa Swanson, COC-A, CPC-A, CPC-P-A, CPB
Lokesh Gupta, CPC, CRCLori Lingo, CPC, CRCLourdes Suarez, CPC, CPMALourdes Valbuena, CPC, CPMA, CEMCLynda Knighton, CPMAMachaelle M Diaz, CPC, CPMA, CRCMajas Fayaz, CRCMalakondaiah Gotha, CPC-A, CICMalana Skolnick, COC, CPC, CPCO, CPMA, CPPM, CEMC, CRC
Malissa Amend, CPC, CPMA
Manjunath Ballappa, CICManuel De Jesus Grullon, CPC, CPMA, CRC
Maram Harish, CRCMarbella Patino, CPC, CPMAMarcie Small, CCS, CPC-A, CRCMarcy Short, CPPMMaria A Joseph, CPC, CPCO, CPMA, CEDC, CEMC
Maria Boyd, COC, CPC, CPC-P, CEMCMarie Bergin, CPC, CCVTCMark Anthony Marlangawe, CICMarnetia Spratley-Pruden, CPC, CPMA, CANPC, CRC
Marsha Sporhase, CPC, CPMA, CRCMartha L Gaviria, CPC, CPMA, CRCMartha Tokos, CPC, CPMA, CPC-I, CRCMary Elizabeth Grimmett, CPC, CRCMary Jane Dickey, CPC, CPBMary M Murphy, CPC, CRCMary Rountree, COC, CICMary-Jo Griffith, CPC, CPC-I, CEMC, CGIC, CGSC, COSC
Maryline Medina, CPC, CRCMathanagopal Pandiarajan, CRCMatilde Perez Chon, CPC-A, CRCMaya Mohan, CICMcKenzie Harrison, CPMAMelanie Rae Edwards, CPC, CPCO, CPMA
Melissa Brownlow, CPC, CPMAMelissa Burke, CPC-A, CRCMelissa Troiano, CPMA, CPPMMichele Brassell, CPC, CRCMichele Gibbs, CPPMMichele R Hayes, CPC, CPMA, CPC-I, CEMC, CGIC, CRC
Michelle D Reese, CPC, CRCMichelle Hartley, COC, CPC, CRCMichelle Lopez, CPC, COBGCMichelle M Mesley-Netoskie, CPC, CPPMMichelle R Davis, CPC, CPB, COBGCMichelle Santos, CICMikel Miller-Edwards, CPC, CPMAMildred I Hanna, CPC, CPCOMohammed Mazheruddin, CICMonica Marie Diaz, CPC, CRCMuthaiya Murugappan, CICNadia Campbell-Johnson, CPMANafeeza Abzal, CPC, CGSCNagaraj Varadharaju, CRCNajuma Syeduebrahim, CICNancy Martin, CPC, CPPMNancy Zizelman, CPC, CPB, CRCNandhakumar Deenadhayalan, CPC, CICNanette Driscoll, CPC, CPMA, CPPMNarda J Mattos, CPC, CPMANarendathu Cherla, COC-A, CICNasir Mire, COC-A, CPMANathan L Kennedy, Jr, CPC, CPB, CPPM, CPC-I
Naveen Kumar Nanamala, CICNaveen Kumar Ch, CICNaveena E Dineshkumar, CICNeelima Akula, CRCNeelima Haneesha Dara, CICNicole K Worobel, CPC, CPMA, CGSCNieve Garcia, CPC, CGICNilesh Tukaram Lad, CPC, CICPalani Balasubramaniam, CPC, CPMA, CEMC
Pam Wayman, CPC, CCC, CCVTCPamela Joan Bess, CPB
Pamela Trisler, CPC, CRCPatrice Zezza, CPC, CRCPatricia A Smith RHIT, CPC, CPMA, CEMC
Paula J Dubel, COC, CPC, CPC-I, CICPauline Hernandez, CPBPedro Camejo, CRCPeter Wamen Lau, CPBPhoebe L Moore, COC, CPC, CRCPhyllis Ingram, CPBPichi Reddy Boggula, CRCPradeep Kalmat, CPBPragati Yadav, COC-A, CICPrithviraj Reddy Patlolla, CICPriyanka Bharathi, CICPulla Rao Rao Penke, CICRacheal Hernandez, CPBRachel A Hively, CPC, CPMARachelle Rea, CPC, CRCRahul Ghanshyam Thorave, CICRahul Sukhdev Talekar, CICRajasekharnaik G, CICRajat Puri, CPC-A, CICRajesh Mannam, CICRajesh Singam, CPC-A, CICRajeswari Muthaiah, CPC, CPMARajkumar Santhanam, CICRajmohan Alagarsamy, CPC-A, CICRaju Shivanathri, CICRakesh Kumar, CICRakesh Yemineni, CPC-A, CICRamasubbu Subburayalu, COC, CPC, CPCO, CPC-P, CIRCC, CPB, CPMA, CPPM, CANPC, CASCC, CCC, CCVTC, CEDC, CEMC, CENTC, CFPC, CGIC, CGSC, CHONC, CIC, CIMC, COBGC, COSC, CPCD, CPEDC, CPRC, CRC, CRHC, CSFAC, CUC
Ramon Lucero Radoc, CPC, CRCRanjani Venkat, CICRanjith Telu, CICRavi Mannela, CICRaviKumar Alluri, CICRavikumar Dobbala, CICReather M Westbrook, CPC, CRCRebecca Erickson, CPBRebecca Lynn Hanif, CPC, CPCO, CPMARenee Connor, COC, CPC, CPC-I, CANPC, CEDC, CEMC, CRC
Rhazel Adoyo, CRCRichard Carreon, CICRita D Bobbitt, CPC, CRCRobin Doerfler, CPC-A, CRCRobin Henry, CPC, CPPMRochelle G Johnson, CFPCRoni Berlin, CPC-A, CPBRoshan Lal, CPC-A, CICRuby Catherine O’Brochta-Woodward, CPC, CPB, CPMA, COSC, CSFAC
Ruchira Narayanan, CPC, CRCRuth Spinelli, CPC, CPMA, CICSahera Banu, CICSaisree Ravindranath, CPC, CPMASambaiah Deshini, CICSamira Khalaf, CPCOSandra Chamberlin, CPC, CPC-I, CRCSangareddy Paidi, CICSanoop George, COC-A, CPMASarah E Pross, CPC, CPB, CFPCSarah E Pross, CPC, CPB, CFPCSarah Malin, CPC-A, CPBSarah Marcelle, CPC, CRCSarah Spivey, CPC, CRC
Saravanan Thangarasu, CPC-A, CICSaravanan Thulasingam, COC, CPC, CPMA, CEMC
Sateesh Rayapati, CPC-A, CICSateesh Reddy Malle, COC-A, CICSavita Kumari, CPC-A, CICScott Smith, CPC-A, CPMAShadrach Viswanth Chembeti, CICShaik Ahmed Sharief, CICShakeda Jenrette, CPEDCShalini Nanjappan, COC, CPMASharon M Casto, CPC, CEDC, COSCShashi Kant, CPC-A, CICShashikala Elumalai Mrs, COC-A, CICSheryl T Witter, COC, CPC, CPC-I, CRCShivashankar Sadila, CICShravya Vaddiraju, CICShu Zhen Liu, CPC, CIRCC, CCC, CCVTCShuvendu Kumar Sahoo, CICShyam sunder goud Panjala, CICSiddharthi Nagaraj, CRCSilvia Lassales, COC, CPC-P, CPMA, CRCSindhuja Gothandaraman, CICSmita Suresh Bandre, CPC, CEMCSobih Abdurahman, CPPMSonia Devereaux, CPBSophia Scott, CPC, CRCSreedhar Kondapalli, CPMASridhar Chitla, CICSrujana Jagati, CICStacey Howe, CPMAStephanie Johnson, CEDCStephanie Darlington, COC, CPC, CICStephanie Garst, COC, CPC, CPMAStephanie Reynolds Garrick, CPC, CPMASubodh Awana, CPC-A, CICSudheer Kumar Bachu, CICSue E Davis, CPC, CRCSukendhar Reddy Malipatlolla, CICSukumar Vankavarasa, CICSummer Johnson, CPBSunday A Adesina, CPCOSunil Raj Natarajan Krishnamma, COC, CIC
Sunny Samrat Meka, CICSuresh Jumple, CPC-A, CICSuriya Gunasekaran, CICSurya Prakash Kakumanu, CICSusan Jantz, CRCSusan Mecodangelo, COC, CPC, CRCSuyin Cecilia Borrero, CPC, CPMASuzanne Maureen Santellanes RN, CPC, CPMA, CRC
Swetha Jagari, CICSydra Wynette Paige, CPC, CIRCCSylvia Ramones, CICTabitha Sauls, CRCTakeda McTear, CPC, CPMATammy Darlene Harris, CPC, CRCTammy G Phillips, CPC, CPMATammy Marie Anderson, CPMA, CEMCTanya E Perales, CPC, CCCTawana Johnson McIver, COC, CPC, CPC-P, CPC-I, CIC
Teena Long, CPC-A, CPMATeresa Suzanne Bartrom, CPC, CPBTeri Mauro, CPBTerri A King, CPC, CRCThelma Stewart, CPC, CPMATheresa Thompson, CPC, CCC, CCVTCTheresa W Burnett, CPC, CRCThirukumaran Jayasankar, CPC-A, CICThirumozhi Mgk, CPC, CIC
Thirupathi Puppala, CICThomasina L Young, CPC, CPCO, CPMA, CRC
Tichelle Lyons, CPBTiffiney R McDaniel, CPC, CIRCCTina Jonas, CPC, CPMATonya Berndt, CPBTracy Bowers, CPC, CPB, CPPMTracy Rink, CPC, CEDC, CEMCTrina Empey, CPC, CRCTyling M Batista, CPC, CPMA, CEMCUma Maheswari, CPC, CICUsha Pandiyan, CPC-A, CICVaitheeswaran Purusothaman, CPC, CPMA
Vamshi Krishna Aluvala, CICVanitha Mourthy, CICVaralakshmi Joseph, CICVenkata Krishna Suresh Pendyala, CPMAVenkatesh Kanuri, CICVickie Hicks, CPC, COBGC, CRCVictoria Angela Holmes, CPC, CIRCCVictoria Russell, CPBVidyasagar Godishala, COC-A, CICVijay Pralhad Tiwari, CPC, CICVijay Sundarraj, CPPMVijaya Kumar Bhathula, CPC-A, CICVijayakrishna Soorishetty, CICVijaykumar Tammali, CICVinni Narayanasamy, CPC-A, CRCVirginia N Hylton, CPC, CRCVishal Balasaheb Gaikwad, CICVishnu Pavani Kakumanu, CICViswa Manoj Pikkili, CICVivian Washington, COC, CPC, CPMA, CPC-I
Wendy Ann Higham, CPC, CPBWendy Droppleman, CPC, CPMAYanira Zeigler, CPC, CPMAYesenia Hernandez, CPC, CRCYiliana Pena, CPC, CPMA, CRCYogesh Pal, CPC-A, CICYolanda Michelle Stewart, CPC-A, CICYolanda Thomas, CPC, CIRCCYsabel Lopez, CPC-A, CPCO, CPMAZahoor Thekkidi Chalil, CICZaida Cabrejos, CEDC

66 Healthcare Business Monthly
Minute with a Member
Jeremy Padgett, CPC-AStudent, DeLand, Florida
GOT A MINUTE?If you are an AAPC member who strives to advance the business of healthcare, we want to know about it! Please contact Michelle Dick, executive editor, at [email protected], to learn how to be featured.
Going back to college and getting my certification for billing and coding was the best decision I ever made.
Tell us a little bit about how you got into coding, what you’ve done during your coding career, and where you work now.I became a healthcare business profession-al because I wanted to make a better life for myself and I was tired of dead-end jobs. I knew that healthcare was the right choice for me — I had previous experience work-ing as a care provider for my aunt, and then for an autistic child. I never thought about medical billing and coding, however, until a relative suggested it. Going back to college and getting my certification for billing and coding was the best decision I ever made. I really enjoy it. My plans are to obtain a master’s degree in billing and coding and to open my own medical billing and coding office.
What is your involvement with your local AAPC chapter?I am a member, and I am open to helping any way I can with my local chapter.
What AAPC benefits do you like the most?I like the help I receive from the organi-zation when looking for a job. Also, the help they gave me in my preparation for the Certified Professional Coder (CPC®) test, mainly from Professor Ramsey at Florida Tech, who helped me a lot.
How has your certification helped you?My certification has opened many doors for me that I did not know were there. I also enjoy the fact that, as a certified cod-er, I am able to meet many interesting peo-ple in my field.
Do you have any advice for those new to coding and/or those looking for jobs in the field?Stay at it. It’s not an easy field, but if you have the proper training, you can do it. Nev-er give up.
What has been your biggest challenge as a coder? I think by biggest challenge was learning CPT® coding.
If you could do any other job, what would it be? Medical billing and coding is the job for me.
How do you spend your spare time? Tell us about your hobbies, family, etc.I spend my spare time watching pro wres-tling and going to pro wrestling events. I am also a big fan of the Florida State Seminoles and the Green Bay Packers.

Powered by
800-626-2633aapc.com/practicode
Land Your Dream JobAccelerate your career and remove your apprentice
designation with Practicode.
Practicode gives you the experience you need to get the job you want. With over 600 real-world coding exercises, you’ll earn one year of coding experience and get closer
to removing your apprentice status. It’s your career. Take control of it.
Powered by
800-626-2633aapc.com/practicode
Land Your Dream JobAccelerate your career and remove your apprentice
designation with Practicode.
Practicode gives you the experience you need to get the job you want. With over 600 real-world coding exercises, you’ll earn one year of coding experience and get closer
to removing your apprentice status. It’s your career. Take control of it.

HEALTHICITY.COM/COMPLIANCEMANAGER
We reinvented compliance management through a complete, flexible solution that complies with all seven OIG recommendations to ensure you’re compliant, even when audited.
All-in-oneCompliance For All