health-related quality of life (hrqol). working group brad zebrack, phd, msw, mph, co-chair...
TRANSCRIPT
Health-Related Quality of Life (HRQOL)

Working GroupBrad Zebrack, PhD, MSW, MPH, Co-Chair• University of Michigan School of Social
Work
Barbara Jones, PhD, MSW• University of Texas School of Social Work
Anne Kirchhoff, PhD, MPH• Huntsman Cancer Institute, University of
Utah
Erin Kent, PhD• NCI
Kelly Trevino, PhD• Rowan University
Lynne Wagner, PhD, Co-Chair• Northwestern University, Robert H. Lurie
Comprehensive Cancer Center
Sheila Santacroce, PhD, RN, APRN• UNC School of Nursing and Lineberger
Comprehensive Cancer Center
Nina Kadan-Lottick, MD, MSPH• Yale University School of Medicine
Ashley Wilder Smith, PhD, MPH• NCI
Sarah R. Arvey, PhD• LIVESTRONG Foundation

Objectives and Strategy
• To identify gaps and recommendations via a systematic review of HRQOL literature (since 2000)
• Define search terms ‘Adolescent,’ ‘Young adult,’ + (PHYSICAL, PSYCHOLOGICAL, SOCIAL, SPIRITUAL/EXISTENTIAL, MEASUREMENT, METHODOLOGICAL)– Google Scholar, PsychInfo, CINHAL
• Define parameters for inclusion– Inclusion (Liberal): aged 15-39 years; younger and older also
included; patients, survivors, survivors of childhood cancer– Inclusion (Conservative): diagnosis at age 15-39 years– Exclusion: sample includes subjects aged <12/13 years or >40
years

Results of Literature ReviewRecords identified through
database search
Records/Titles screened (Liberal inclusion)
Records excluded: Not HRQOL, not 15-39 years
Records/Titles screened(Conservative inclusion)
Records excluded: Not AYA
PhysicalPsych, Social,
Spiritual/ExistentialMeasurement
& Methodology Total
Liberal inclusion 184 253 68 505Conservative inclusion 26 105 23 154
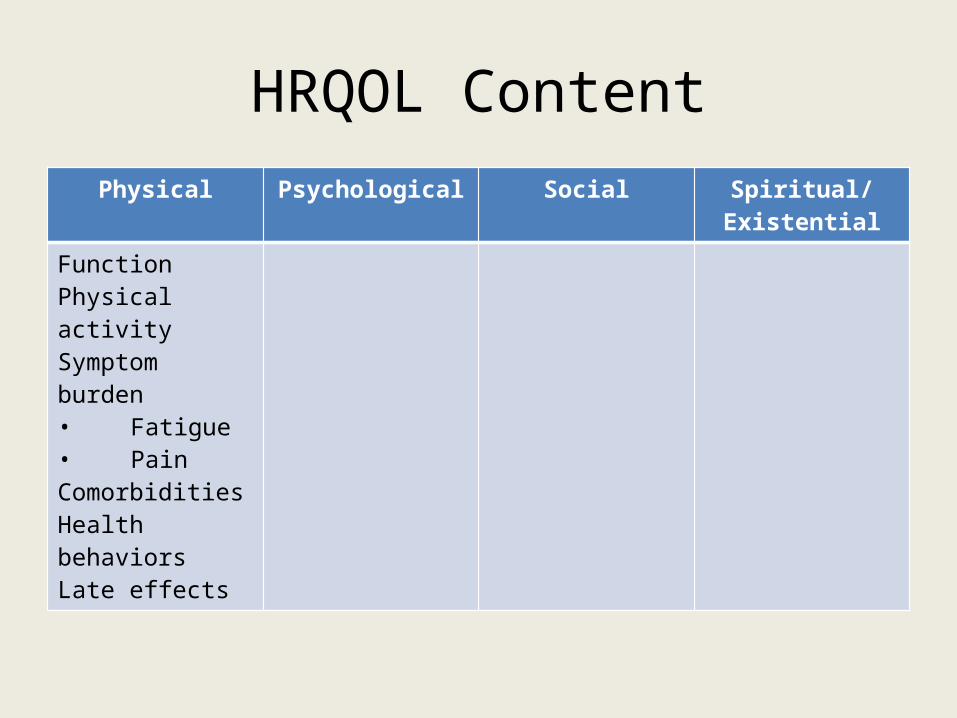
HRQOL ContentPhysical Psychological Social Spiritual/Existential
FunctionPhysical activitySymptom burden• Fatigue• PainComorbiditiesHealth behaviorsLate effects
Physical Well-Being• AYAs report:
– Poorer physical functioning than healthy peers or siblings (CCSS)– Better physical functioning compared to older survivors
• YAs reported greater symptom burden compared to older adults with the same cancer type– Breast: Moderate/severe drowsiness, hair loss, sx interference in
relationships– Colorectal: Moderate/severe pain, fatigue, nausea, distress, drowsiness,
shortness of breath, rash, and greater interference in general activity, mood, work, relationships and life enjoyment
• Diagnosis, type of treatment, age at treatment completion and time since treatment completion not correlated with HRQL

• AYAs on treatment have greater symptom burden than those post-treatment, though fatigue persists for years
• Fatigue and pain negatively affect HRQL
• AYAs report higher rate of comorbidities (24%) than non-cancer controls (14%), including cardiovascular disease, hypertension, asthma, and disability
Physical Well-Being

• AYAs report levels of physical activity comparable to controls, below recommended guidelines
• High proportion of AYAs report being overweight (20%) or obese (15%) with higher rate of obesity among AYAs (31%) than controls (27%)
• Rates of cigarette use among AYAs estimated at 16% and 26%– One study estimated use higher than non-cancer controls (18%)– One study found higher rate among age-related peers (25%)
and lower rate among older cancer survivors (4%)
Physical Well-Being

HRQOL GapsPhysical Psychological Social Spiritual/Existential
FunctionPhysical activitySymptom burden• Fatigue• PainComorbiditiesHealth behaviorsLate effects
GAPSOther symptoms (e.g., sleep, neuropathy, ADLs)Late effectsBiopsychosocial risk factors
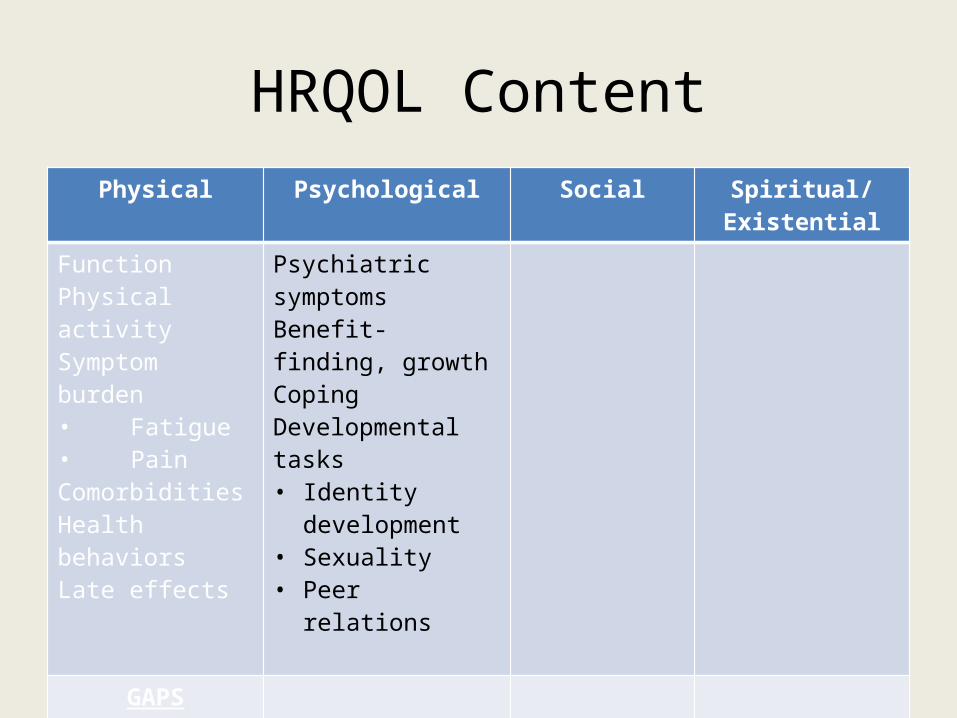
HRQOL ContentPhysical Psychological Social Spiritual/Existential
FunctionPhysical activitySymptom burden• Fatigue• PainComorbiditiesHealth behaviorsLate effects
Psychiatric symptomsBenefit-finding, growthCopingDevelopmental tasks• Identity
development• Sexuality• Peer relations
GAPSOther symptoms (e.g., sleep, neuropathy, ADLs)Late effectsRisk factors

Psychological Well-Being
• AYAs report higher prevalence of psychiatric symptoms (compared to normative data, non-cancer controls, older cancer patients)– 6%-41% distress– Study findings mixed with regard to identifiable risk
factors• age, time since diagnosis, education, employment status,
relationship status, cancer type/severity, treatment type, symptom burden, needs of daily living, fertility concerns, information needs, insurance status, health system characteristics

Psychological Well-Being
• Coping strategies employed– Acceptance, problem-solving– Support seeking– Emotional expression (through writing, blogs)– Seeking normalcy– Physical activity
• Benefit finding, meaning-making associated with positive outcomes
• Evidence of low levels of receipt/use of psychosocial care
Psychological Well-Being
• Existing interventions: promote achievement of developmental tasks– Identity development, sexuality, peer relationships
• Intervention modalities reported– Expressive therapy through arts, music, video-
making, writing, physical activity

HRQOL GapsPhysical Psychological Social Spiritual/Existential
FunctionPhysical activitySymptom burden• Fatigue• PainComorbiditiesHealth behaviorsLate effects
Psychiatric symptomsBenefit-finding, growthCopingDevelopmental tasks• Identity
development• Sexuality• Peer relations
GAPSOther symptoms (e.g., sleep, neuropathy, ADLs)Late effectsRisk factors
GAPSRisk/resilience factors

HRQOL ContentPhysical Psychological Social Spiritual/Existential
FunctionPhysical activitySymptom burden• Fatigue• PainComorbiditiesHealth behaviorsLate effects
Psychiatric symptomsBenefit-finding, growthCopingDevelopmental tasks• Identity
development• Sexuality• Peer relations
NormalcySocial networksStigmaWork/school and socioeconomic statusRelationships
GAPSOther symptoms (e.g., sleep, neuropathy, ADLs)Late effectsRisk factors
GAPSRisk/resilience factors

Social Well-Being
• AYAs compare selves to peers– Fertility concerns compromise sense of normalcy
• Social networks– Friends help– …but offer few opportunities to ask questions,
receive information, process feelings, develop coping strategies
Social Well-Being
• Stigma and unfair treatment– From peers, employers, government agencies
• Challenges in returning to work/school
• Low SES contributes to poor HRQOL
• AYAs less likely to be married/partnered; more likely to divorce.

HRQOL GapsPhysical Psychological Social Spiritual/Existential
FunctionPhysical activitySymptom burden• Fatigue• PainComorbiditiesHealth behaviorsLate effects
Psychiatric symptomsBenefit-finding, growthCopingDevelopmental tasks• Identity
development• Sexuality• Peer relations
NormalcySocial networksStigmaWork/school and socioeconomic statusRelationships
GAPSOther symptoms (e.g., sleep, neuropathy, ADLs)Late effectsRisk factors
GAPSRisk/resilience factors
GAPSRisk/resilience factorsFamily distress/impactSexual functionBody image/appearanceFinancial well-beingEducation

HRQOL ContentPhysical Psychological Social Spiritual/Existential
FunctionPhysical activitySymptom burden• Fatigue• PainComorbiditiesHealth behaviorsLate effects
Psychiatric symptomsBenefit-finding, growthDevelopmental tasks• Identity
development• Sexuality• Peer relations
NormalcySocial networksStigmaWork/school and socioeconomic statusRelationships
UncertaintyHope and gratitude
GAPSOther symptoms (e.g., sleep, neuropathy, ADLs)Late effectsRisk factors
GAPSRisk/resilience factors
GAPSRisk/resilience factorsFamily distress/impactSexual functionBody image/appearanceFinancial well-beingEducation

Spiritual/Existential Well-Being
• Coping with Uncertainty
• Expressions of Hope and Gratitude

HRQOL GapsPhysical Psychological Social Spiritual/Existential
FunctionPhysical activitySymptom burden• Fatigue• PainComorbiditiesHealth behaviorsLate effects
Psychiatric symptomsBenefit-finding, growthCopingDevelopmental tasks• Identity
development• Sexuality• Peer relations
NormalcySocial networksStigmaWork/school and socioeconomic statusRelationships
UncertaintyHope and gratitude
GAPSOther symptoms (e.g., sleep, neuropathy, ADLs)Late effectsRisk factors
GAPSRisk/resilience factors
GAPSRisk/resilience factorsFamily distress/impactSexual functionBody image/appearance Financial well-beingEducation
GAPSSpiritualityReligiosity: Development of faith, practice
Methodology and Measurement
• Lower rates of AYA study participation and retention as compared to older survivors
• Recruitment strategies vary in effectiveness (as per response rate)– Clinic-based recruitment, mailings, social media, population-
based (SEER)– Online approaches and registries for study recruitment have
mixed results re study accrual
• Study retention increased with use of peer participants, collateral contacts, and parental awareness of participation

Methodology and Measurement
• Peer outreach (peer-to-peer recruitment) increased retention in health care
• Online technology effective for intervention delivery– Use of social media outlets (e.g., Facebook) for
collecting PROs
• Evidence of higher response bias in reporting inflated levels of socio-emotional functioning
Methodology and Measurement
• Few HRQOL-specific measures with reported psychometric data– Minneapolis-Manchester QOL– PedsQOL– Cancer Needs Questionnaire
• Few specific content areas covered by use of standardized measures– Fatigue, Pain, Sleep– Depression, Distress, Neurocognitive function

Summary HRQOL Content & GapsPhysical Psychological Social Spiritual/
ExistentialFunctionPhysical activitySymptom burden• Fatigue• PainComorbiditiesHealth behaviorsLate effects
Psychiatric symptomsBenefit-finding, growthCopingDevelopmental tasks• Identity
development• Sexuality• Peer relations
NormalcySocial networksStigmaWork/school and socioeconomic statusRelationships
UncertaintyHope and gratitude
GAPSOther symptoms (e.g., sleep, neuropathy, ADLs)Late effectsRisk factors
GAPSRisk/resilience factors
GAPSRisk/resilience factorsFamily distress/impactSexual functionBody image/appearanceFinancial well-beingEducation
GAPSSpiritualityReligiosity: Development of faith, practice

Recommendations• Rigorous designs
– Comparison groups, disease- and treatment-specific sub-groups– Longitudinal studies w/repeated measures -- Important given relatively rapid
psychosocial & cognitive development– Comparative effectiveness evaluations of non-traditional interventions (e.g.,
videogames, movies, creative arts, social networking) compared to conventional interventions (e.g., psychotherapy, support groups)
• Instrumentation– Deeper evaluation of function, performance, coverage of content, validity,
reliability– Use of standardized measures and – Biomarkers with established AYA reference ranges or community norms
• Health disparities– Identify disparities in symptom burden (physical and psychosocial), and access to
supportive care services• By AYA characteristics: race/ethnicity, age sub-group, SES, language
Recommendations
• Intervention studies – Reduce symptom burden– Promote positive adaptation and coping– Target self-efficacy/self-management (symptoms,
surveillance of late effects & 2nd malignancies)– Involve friends, family, peers– Better understanding of role and potential of
social networking/social media