health optimization program for elders (hope) - ncact · health optimization program for elders...
TRANSCRIPT

Health Optimization Program for Elders (HOPE)Transitional Care from Duke University Hospital to Skilled Nursing Facilities
HeidiK.White,MD,MHS,MedTammieShepherd,MHA,BSN,RN,ACMWilliamEnglish,MBA,MSHA
BACKGROUNDHealth Optimization Program for Elders (HOPE)
What is HOPE?Transitional care model designed to prevent avoidable
readmissions and other adverse outcomes during and after transition from the acute inpatient care setting to the post-acute
care setting for adult patients age 55 and older at Duke University Hospital
Acute HOPE SNF
SYSTEM LEVEL
PATIENT LEVEL
Why HOPE?
Too many patients, families, and providers experience a disconnect between hospital
care and skilled nursing facility care.
HospitalSkilled Nursing Facility ?
Why Now?
Hospital Readmission Penalties
Bundled Payments
Movement toward Capitated Systems w/ Shared Risk• Medicare Shared Savings Plan (MSSP)• Duke Connected Care• Duke Well
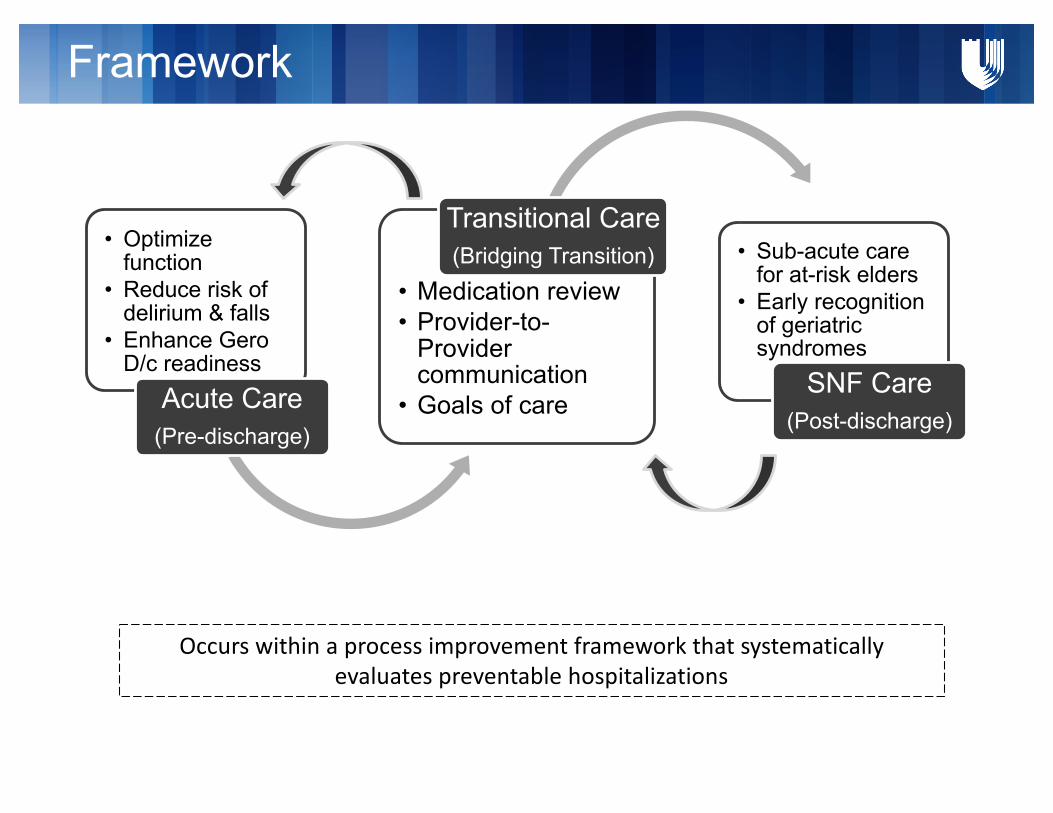
Framework
• Optimize function
• Reduce risk of delirium & falls
• Enhance GeroD/c readiness
Acute Care(Pre-discharge)
• Medication review• Provider-to-
Provider communication
• Goals of care
Transitional Care(Bridging Transition) • Sub-acute care
for at-risk elders• Early recognition
of geriatric syndromes
SNF Care(Post-discharge)
Occurswithinaprocessimprovementframeworkthatsystematicallyevaluatespreventablehospitalizations
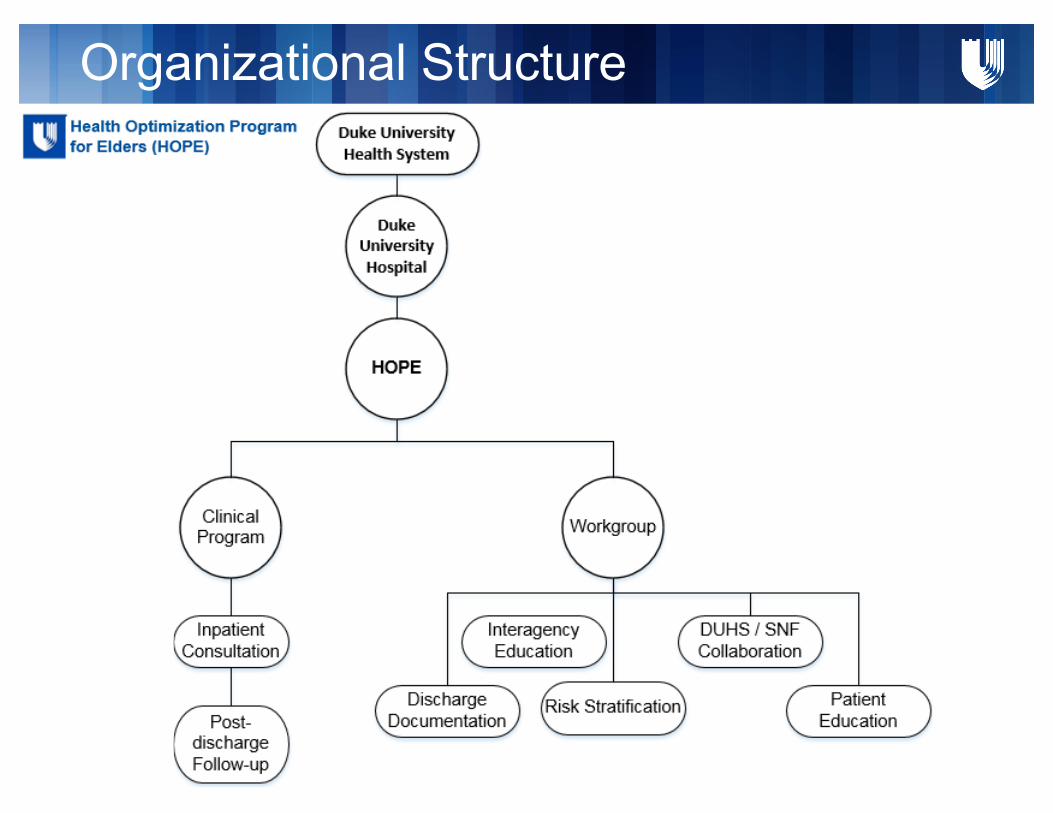
Organizational Structure
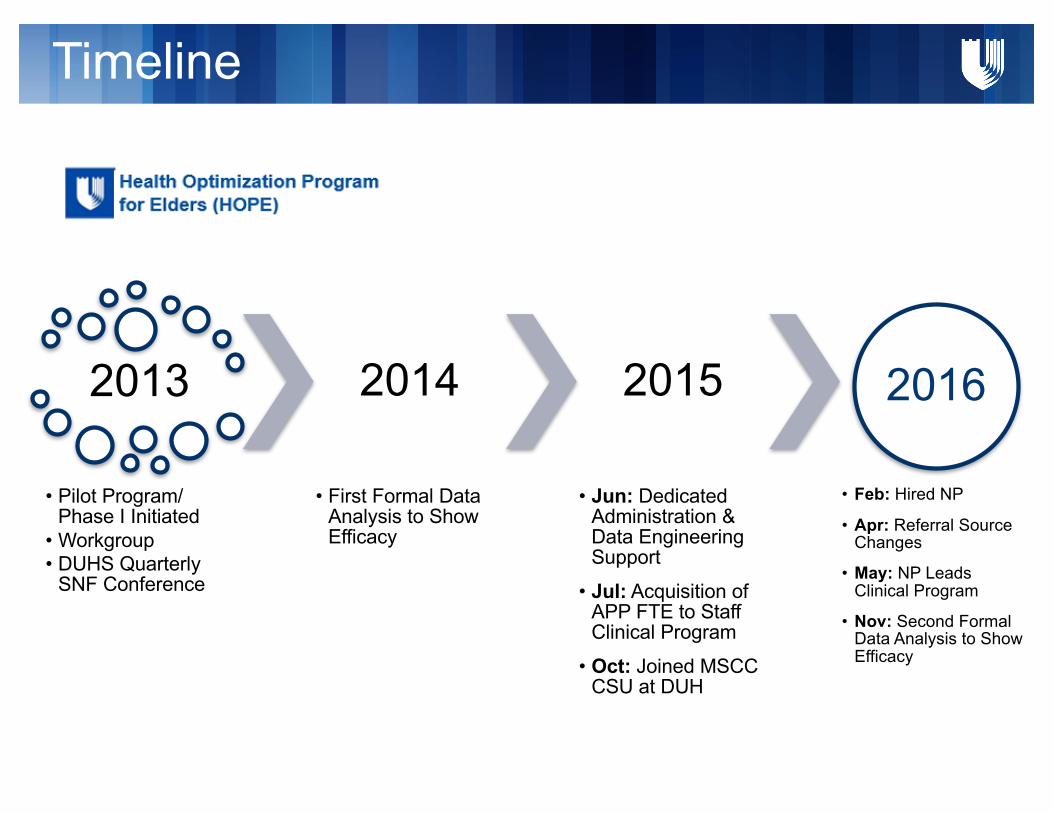
Timeline
2013
• Pilot Program/ Phase I Initiated
• Workgroup• DUHS Quarterly
SNF Conference
2014
• First Formal Data Analysis to Show Efficacy
2015
• Jun: Dedicated Administration & Data Engineering Support
• Jul: Acquisition of APP FTE to Staff Clinical Program
• Oct: Joined MSCC CSU at DUH
2016
• Feb: Hired NP
• Apr: Referral Source Changes
• May: NP Leads Clinical Program
• Nov: Second Formal Data Analysis to Show Efficacy
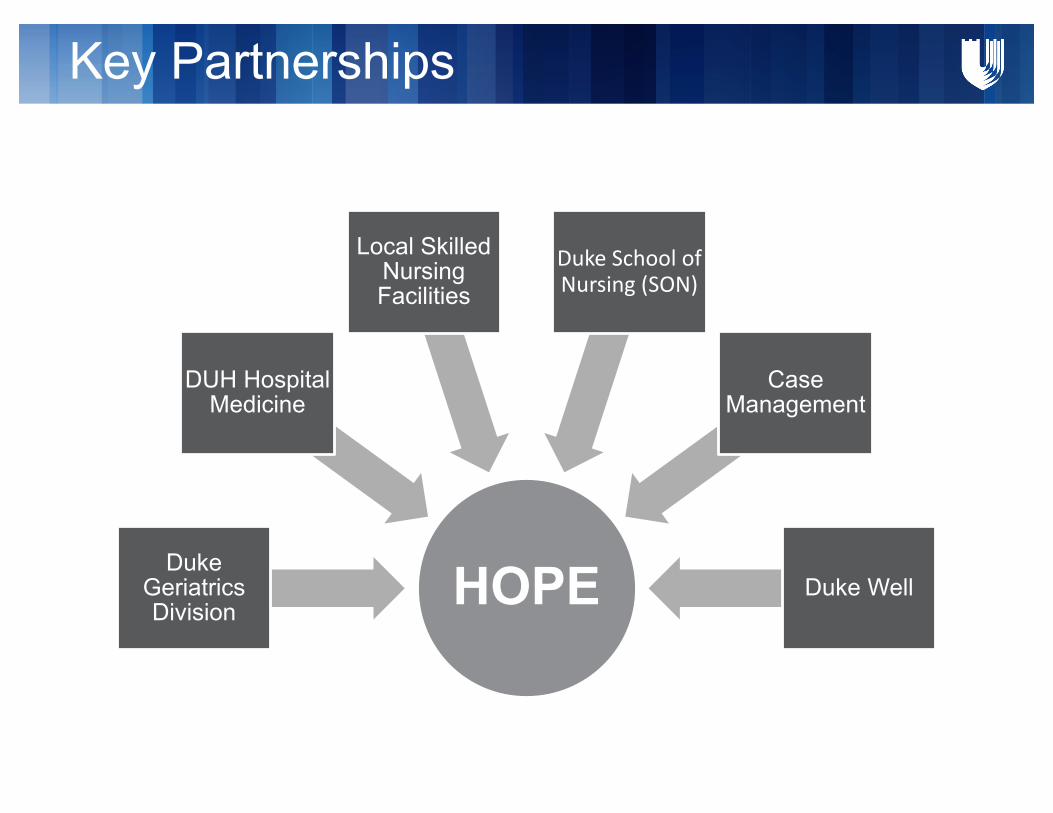
Key Partnerships
HOPEDuke Geriatrics Division
DUH Hospital Medicine
Local Skilled Nursing Facilities
DukeSchoolofNursing(SON)
Case Management
Duke Well
Duke SON & HOPE
• Student Collaborators– Patient Education Materials
• Nurses Improving Care for Healthsystem Elders (NICHE)– Interagency Education
Case Management & HOPE
Original Referral Source
Case managers requested HOPE referrals from hospitalists
Discharge Documentation
Used feedback from HOPE Workgroup to work with
EHR technicians to optimize discharge documents
First Efforts at Risk
Stratification
METHODS & RESULTSHealth Optimization Program for Elders (HOPE)
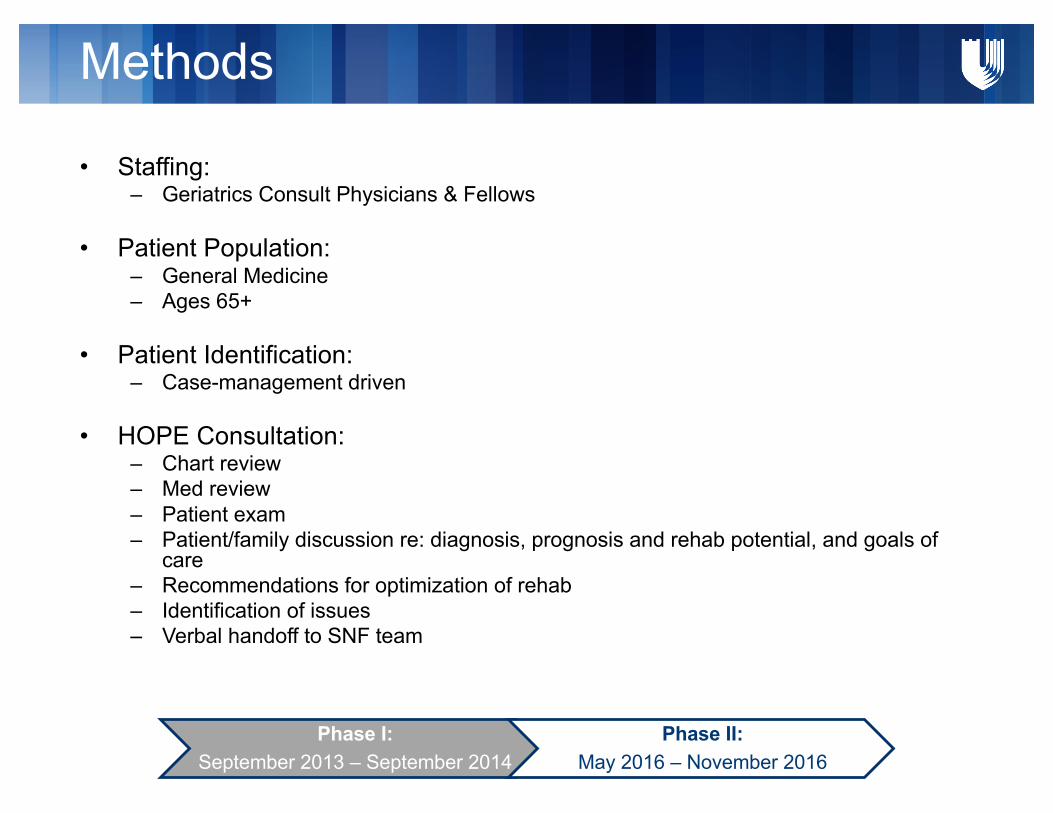
Methods
Phase I:September 2013 – September 2014
Phase II:May 2016 – November 2016
• Staffing: – Geriatrics Consult Physicians & Fellows
• Patient Population:– General Medicine– Ages 65+
• Patient Identification: – Case-management driven
• HOPE Consultation:– Chart review– Med review– Patient exam– Patient/family discussion re: diagnosis, prognosis and rehab potential, and goals of
care– Recommendations for optimization of rehab– Identification of issues– Verbal handoff to SNF team
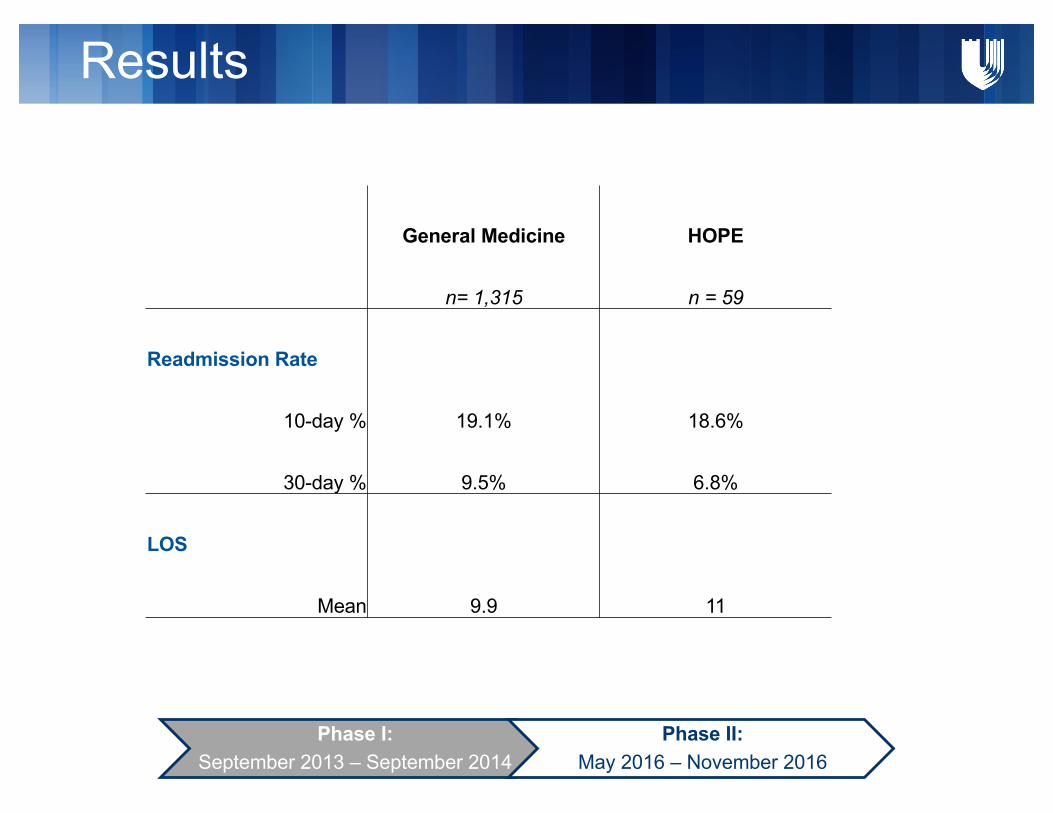
Results
Phase I:September 2013 – September 2014
Phase II:May 2016 – November 2016
General Medicine HOPE
n= 1,315 n = 59
Readmission Rate
10-day % 19.1% 18.6%
30-day % 9.5% 6.8%
LOS
Mean 9.9 11
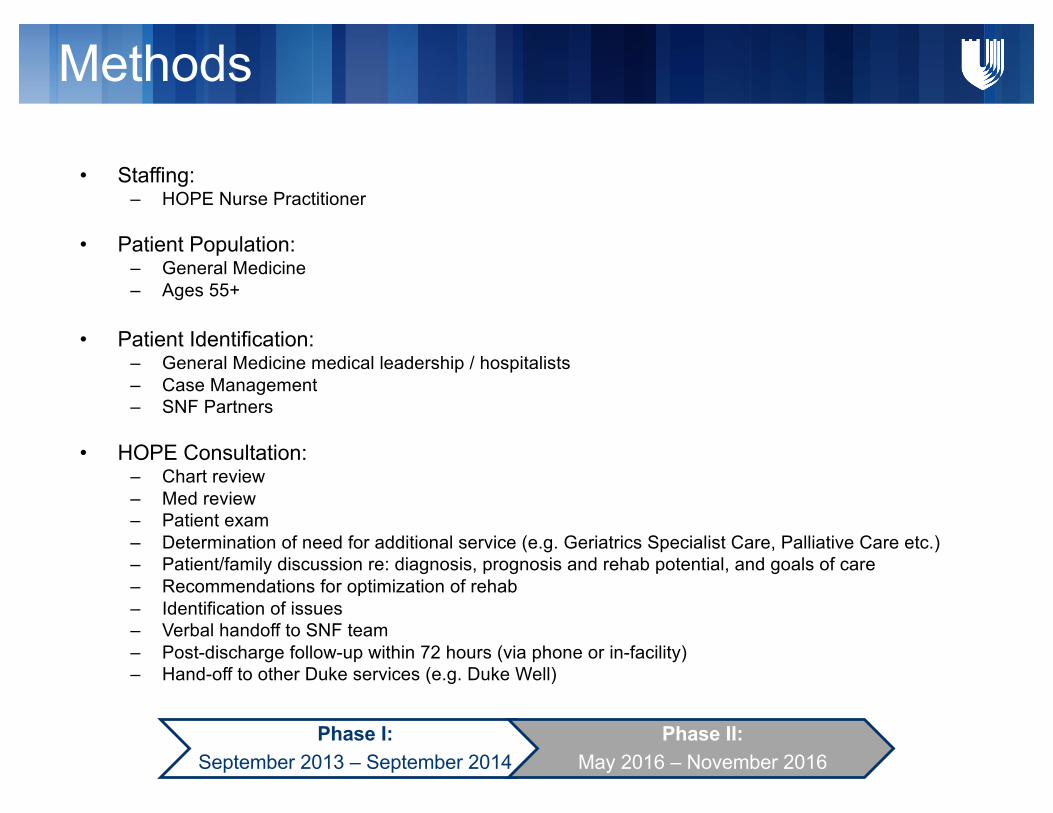
Methods
• Staffing: – HOPE Nurse Practitioner
• Patient Population:– General Medicine– Ages 55+
• Patient Identification: – General Medicine medical leadership / hospitalists– Case Management– SNF Partners
• HOPE Consultation:– Chart review– Med review– Patient exam– Determination of need for additional service (e.g. Geriatrics Specialist Care, Palliative Care etc.)– Patient/family discussion re: diagnosis, prognosis and rehab potential, and goals of care– Recommendations for optimization of rehab– Identification of issues– Verbal handoff to SNF team– Post-discharge follow-up within 72 hours (via phone or in-facility)– Hand-off to other Duke services (e.g. Duke Well)
Phase I:September 2013 – September 2014
Phase II:May 2016 – November 2016

Results
General Medicine HOPE
n= 540 n = 118Readmission Rate
7-day % 4.9% 2.2%14-day % 8.4% 6.5%30 day % 15.4% 10.1%90-day % 27.8% 25.9%
LOSMean 9.4 12.4
CMIMean 1.85 2.04
Phase I:September 2013 – September 2014
Phase II:May 2016 – November 2016
0%
2%
4%
6%
8%
10%
12%
14%
0
5
10
15
20
25
30
35
May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16
HOPEConsultVolume&Readmissions
Volume 7-dayReadmit 14-dayReadmit
CONCLUSIONS & NEXT STEPSHealth Optimization Program for Elders (HOPE)

Conclusions
• Proven potential to avoid discharge failures
• Post-discharge follow-up critical in correcting missteps and building relationships with SNF medical providers/nursing staff
• HOPE is a part of a broader transitional care plan
Next Steps
• Data Refinement
• Risk Stratification
• Assessment of protocolized hand-offs to appropriate services post-discharge