hcd_2011_md anderson study
TRANSCRIPT

E74: Teaming Up
Does unit decentralization impact teamwork and
operational efficiencies?
Pamela Redden, MS, BSN,RN, EDAC, Director, Clinical Facilities Development
UT MD Anderson Cancer Center
Janet Sisolak, Project Director
UT MD Anderson Cancer Center
Debajyoti Pati, PHD, FIIA, LEED AP.
Executive Director, CADRE; Rockwell Endowment Professor, Texas Tech

Acknowledgments
HKS Architects
- Study sponsor and institutional support
Center for Advanced Design Research &
Evaluation (CADRE)
Texas Tech University
- Institutional support

Learning Objectives
Understand the impact of decentralization on
the way nurses spend their time (efficiency).
Understand the impact of decentralization on
walking distance.
Understand the potential influence of
decentralized operations on presenteeism and
acute stress of care providers.
Understand the impact of decentralization on
care providers’ teamwork and collaboration.

Agenda
Drivers of decentralization
Key questions
The evidentiary challenge
The MD Anderson project
Study data
Key findings

INTRODUCTION
Bed utilization:
• Male – Female
• Smoker – Non
Smoker
• Infection
Build fewer beds
Increase
flexibility
Driver of Decentralization: Single Room

Key Area of Change # 1
Increase in floor
area per patient:
• Larger footprint
for the same
number of beds

Key Area of Change # 2
Support space
optimization:
• Race track
configuration
• Decentralization

Hypothesized Impact Areas
Patient focused
- More time with patient
Improved efficiencies
- Reduced non-productive time
- Reduced walking distance
Collaboration, teamwork and mentoring?
Stress reduction?
- Chaos, noise
- Socialization
Productivity improvement

Agenda
Drivers of decentralization
Key questions
The evidentiary challenge
The MD Anderson project
Study data
Key findings

Key Questions
Does decentralization influence time spent
in walking, queues, and hunting and
gathering?
Does it reduce non-productive tasks?

Key Questions
Does decentralization influence staff
interaction and collaboration?

Agenda
Drivers of decentralization
Key questions
The evidentiary challenge
The MD Anderson project
Study data
Key findings

The AECOM Study
Six units
Three hospitals
Measurements:
- Functional space use
- Patient visibility
- Noise level
- Nurse perception of
work environment
Findings:
- Time spent on
telephone/ computer/
admin higher in
centralized
- Consultation/
interaction less
frequent on
decentralized
Centralized vs. Decentralized Nursing Stations: Effects on
Nurses’ Functional Use of Space and Work Environment
(Terri Zborowsky, et al.)

The Taiwan Study
Two units
Two hospitals
Measured:
- Staff interaction
- Patient falls
Findings:
- Less communication
in decentralized
model
- Less patient fall
events in
decentralized model
Impact of Architectural Design on Communication among
Hospital Staff. (Chai Hui Wang)

The WHR Study
Four units
One hospital
Measured:
- Patient satisfaction
- Nurse satisfaction
- Communication
- Walking distance
- Medical outcomes
- Organizational outcomes
Findings:
- Increase in patient
satisfaction
- No significant
differences in any
other parameters
The Effects of Nursing Unit Spatial Layout on Nursing
Team Communication Patterns, Quality of Care and
Patient Safety (Franklin Becker et al)

Agenda
Drivers of decentralization
Key questions
The evidentiary challenge
The MD Anderson project
Study data
Key findings


Location - the heart of the Texas Medical Center, Houston, TX
M.D. Anderson Cancer Center Background

• Texas Medical Center (42 member institutions, 13 major hospitals with 66,000 employees)
• A healthcare component of the University of Texas
• Founded in 1941, M. D. Anderson has grown to over 18,000 faculty and staff.
• More than $2.2 billion annual revenue
M.D. Anderson Cancer Center Background

• 1998 – 1999
20% growth in patients
• 1999 – 2008
80% growth in patients
75% increase in employee
115% increase in research
revenue
• 2012 Projections
50% growth in patients
from 2006
M.D. Anderson Cancer Center Growth

Then and Now

THE BEFORE CONTEXT

Typical Nursing Floor
(4) 13-bed Units
All Private Rooms
Central Nurse Station
Racetrack Design
Service & Public Elev.
Albert B. and Margaret M. Alkek Hospital

Central Nursing
Station
Documentation
Station
Albert B. and Margaret M. Alkek Hospital

Albert B. and Margaret M. Alkek Hospital
Typical Amenities include:
• Murphy bed for family members
• TV/ Lodgenet
• Storage for luggage, clothing

Unit Configuration
Centralized work concept
Open medication prep
areas
Family waiting areas
small/lacking
Wayfinding challenges

THE AFTER CONTEXT

Expansion Project – Initiated in 2005
503,000 Square Feet
Added
11 Additional Floors
- 8 Inpatient Units
- Pharmacy
- Facilities support
- Mechanical / Electrical
Observation Deck
Current Operating Beds =
702
Future Operating Beds =
962

1. Need to maximize
the number and
size of patient
rooms per floor
using current
industry and best
practice standards
2. Need to improve
wayfinding for
families and
visitors
3. Need to add
family spaces &
amenities on floor
2 2
11
3
NN
Design Challenges – Patient/Family

1. Need to increase
access to nursing
stations
2. Need to improve
staff and patient
circulation
3. Need to improve
support and staff
areas
1 1
22
3 3
NN
Design Challenges – Staff

Key Goals and Objectives
The new Alkek patient units will be designed
reviewing current evidence-based concepts
in a manner that:
Promotes patient and family centered care
Maximizes efficiency of work effort for all
members of the care team
Includes ergonomic considerations that
minimize the physical burden of patient care
delivery
Promotes interdisciplinary collaboration

Key Goals and Objectives
Additionally, key design elements should be
considered in relation to these guiding
principles:
Promote safety for patients
Enhance support for patients and their families,
recognizing that the family plays an active role in
the healing process
Meet/exceed the needs of the care givers -
integrate technology, maximize staff productivity,
increase time at the patient bedside, minimize
footsteps, enhance ergonomics

Design
Design-Build project McCarthy/HKS
Nursing Leadership Design Team 2006
Surveys on design topics- staff, physicians, caregivers,
patients
Focus Groups
- Medical Team Members
- Staff
- Patients & Family Members
Bulletins & Postings
SharePoint Site

Design Solutions - Patients/family
1. Increased footprint
to accommodate
more rooms per
floor
2. Improved
wayfinding on unit
3. More family
waiting
4. Added consult
room
1
11
1
33
22
44
NN

1. Improved staff
circulation within
core
2. Decentralized
staff stations at
patient rooms
3. Decentralized
meds and
equipment
3. Created team
rooms
1 1
22
3
3
3
3 4
44
4
Design Solutions - Staff
N

Inpatient Floors 15–17:Typical patient room
Increased room size (ranges from 251 s.f.–298 s.f.)
Outboard toilet improves visibility of patient
ADA-sized toilet enhances accessibility
Improved family space
Easier access to patient
Caregiver work area within patient room
PPE alcove outside room

Inpatient Rooms
Room Zones
• Family Zone
- Sleep Sofa
- Additional Storage for Family
- Individual Television
• Patient Zone
- Flexible Acuity
- Desk Work Area
- Headwall Ergonomics
• Staff Zone
- Hand washing sink inside room
- Locked medication storage
- C5 mobile computer

Decentralized Nurse/Staff Stations
• Decentralized nurse/staff stations with
patient view window
• Improved view of patients for
assessment purposes
• Encourages staff time with
patients
• Decreases staff travel time
• Distributed supplies/linen
• Creates quieter environment
Storage rooms and alcoves
• Maintain hallways free of equipment
• Support service areas (Lab, Nutrition)
TEAM
MEDS
SUPPL
Y
Unit Staff Support Areas

Unit Staff Support Areas
Medication Rooms
• Locked medication rooms added to
each pod on the new units
• Addresses Joint Commission
standards for medication security
• Permits focused, uninterrupted
medication preparation by the
nursing staff
Team Station
• Fully outfitted admin area for Roving
Patient Service Coordinator/Staff
utilization
• Central Physiologic Monitoring

Team Room
Team Rooms
• Multi-purpose rooms located on each
pod to foster interdisciplinary
collaboration and teamwork
• MediaScape Smart Media
Collaboration Table from
Steelcase – data network
connections w/ ability to display
images from on-board desktop
computers or laptops.
• Web conferencing capable
• Educational Initiatives
• Glass walls of Team Rooms can
be reconfigured if future utilization
changes

STAFF AMENITIES – INPATIENT UNITS
• Staff Tranquility/Working Mother’s Room
• Locker Room ~ Staff Shower
• Staff Lounge
• Shared Multi-disciplinary Desks
• Conference Room
Staff Amenities

CLINICAL OPERATIONS

Unit Model
STAFFING
Staffing typically 2-3 patients/RN
Support staff: CNAs and PSCs
Clinical Nurse Leader, AD, ANMs
PATIENTS
Leukemia
Lymphoma
Stem Cell Transplant
“Mixed” hematology


Goals of the QI Project
Assist in adaptation to the new unit design
Identify new processes for
Communication
Collaboration
Task completion
Larger unit footprint
Seek opportunities
Education and training
Modify design elements

Study Protocol
14 staff data points for day shift/14 data points
for night shift (per unit)
RNs carried PDAs and completed
corresponding pedometer logs
PDA vibrates 30 times/12 hours, tasks and
location entered
Filled out surveys

Study Protocol

Pre Occupancy Data Collection
“Pre” Data Collection
January 18 – 31, 2011
G11 (Stem Cell Transplant) Alkek
Hospital
P6 (Hematology) Lutheran Pavilion
February 1 – 7, 2011
G9 East (Lymphoma Service) Alkek
Hospital
Written Surveys for 2 weeks – January 15
– 31.

Activation and Occupancy
“Bed shortage”/high census impacts
Phased occupancy
November 8, 2010 G16 G10W 26 beds to G16 48
beds
March 7, 2011 G17E: 12 beds open
March 14, 2011 G17W: 12 beds open
May 16, 2011 G15: G9E to G15

Post Occupancy Data Collection
“Post” Data Collection
September 8 – 22, 2011
G11 & G17 SW
September 26 – October 9, 2011
G15 & G17 SE
Written Surveys for 2 weeks – September 1 – 15

Activation and Occupancy
Activation
Management Team
Operations
PlanningMove
ManagementCommunications Training
Facility
Readiness
•Programs/Service
s
•Policies
•Systems/Procedu
res
•HR Functions
•Process Design
•Operating Budget
•Scheduling/
Sequencing
•Packing/
Labeling
•Department
Relocation
Management
•On-Going Staff/
Employee
Communication
•Opening Events
•Patient
Communication
•General Facility
Communications
•Operation
Simulations
•Training &
Orientation
•Master Training
Schedule
•Facility
Planning/
Development/
Construction
•Furniture/
Equipment/
Signage
•Facility
Completion/
Startup

Activation and Occupancy

Activation and Occupancy
Training and Education
Orientation methods
First new floor challenges
New workflow
New team members

Educational Resources

Educational Resources
• Short computer-based training modules developed to assist with
training utilizing Camtasia PowerPoint Voice Over Program
• Vocera
• Bedside supply cabinets
• Biohazard and linen pass-thru cabinets
• Team Rooms
• Multidisciplinary workrooms
• Medical team rounds
• Unit orientation
• Medication room

Operational Factors
Children’s Cancer Hospital Expansion needed temporary inpatient
unit.
Issues with showers and smoke dampers requiring moves of patients
floor to floor before full occupancy.
Increase in monitored beds-
decrease in ICU census

Operational Factors
Operating a 24 bed “unit” vs. 13 bed “pod”
Physician and medical team “centralized practice” concept
Staff rotations
Unit culture/staff roles

Post Occupancy Reviews
Staff feedback sessions August, 2011
Themes:
o “Unit Spread Out”, harder to find people/staff
o Patient assignments now need to consider
geography
o “View windows” yes or no?
o Pod vs. Unit function
o Like new medication room/system
o Team room use by medical staff
o Push button locks vs. badge

Agenda
Drivers of decentralization
Key questions
The evidentiary challenge
The MD Anderson project
Study data
Key findings

DATA TYPES

Data Types
Nursing time:
- Rapid Modeling PDA
Walking distance:
- Pedometer
Acute stress:
- Current Mood State Questionnaire
Presenteeism:
- Koopman Stanford Presenteeism
Scale (Modified)
Staff interaction and collaboration

PDA TCAB Data Classification
Task Type- Value adding
- Non value adding
- Necessary
Task Category- Direct care
- Indirect care
- Administrative
- Personal
- Waste
- Documentation
- Other
Task Location- Nurse station
- Patient room
- On the unit
- Patient medication
- Supply storage
- Conference room
- Off unit
- Documentation server
- Other
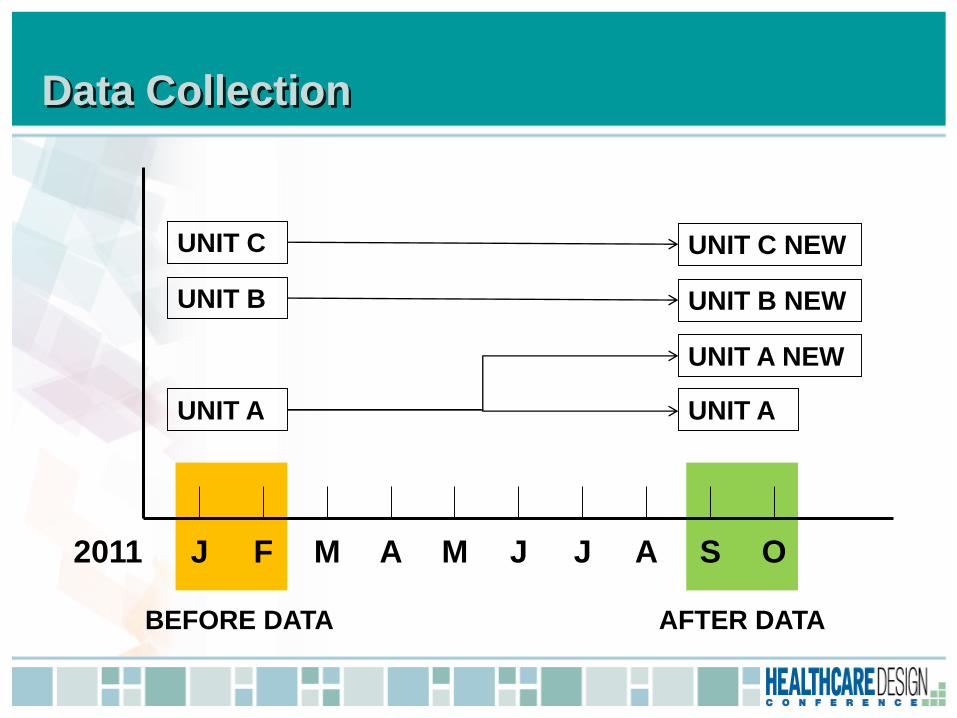
Data Collection
J F M A M J J A S O
BEFORE DATA AFTER DATA
UNIT A
UNIT B
UNIT C
UNIT A
UNIT A NEW
UNIT B NEW
UNIT C NEW
2011

Agenda
Drivers of decentralization
Key questions
The evidentiary challenge
The MD Anderson project
Study data
Key findings

Identifying Patterns of Change
Multiple unit
comparison benefit

Identifying Patterns of Change
Care processes, physical environment, culture
and policies interact
PATIENT
PATIENT OUTCOMES
PHYSICAL ENVIRONMENT
CAREGIVER CARE PROCESSES
GROUP PHENOMENA: CULTURE RELATIONSHIPS
POLICIES

Identifying Patterns of Change
Performances change after intervention
The key question is consistency

Task Category: Documentation
15
17
19
21
23
25
27
29
31
33
Unit A Unit B Unit C
Before
After

Task Location: Nurse Station
25
27
29
31
33
35
37
39
41
43
45
Unit A Unit B Unit C
Before
After

Task Location: On The Unit
0
2
4
6
8
10
12
14
16
Unit A Unit B Unit C
Before
After

Task Location: Medication
0
2
4
6
8
10
12
14
Unit A Unit B Unit C
Before
After

Task Location: Supply Storage
0
0.5
1
1.5
2
2.5
Unit A Unit B Unit C
Before
After

Walking Distance
1.5
2
2.5
3
3.5
4
Unit A Unit B Unit C
Before
After

Documentation
15
17
19
21
23
25
27
29
31
33
Before After After New

Nurse Station
30
31
32
33
34
35
36
37
38
39
Before After After New

On The Unit
5
5.5
6
6.5
7
7.5
Before After After New

Medication
0
2
4
6
8
10
12
14
Before After After New

Supplies
0
0.5
1
1.5
2
2.5
Before After After New

Walking Distance
1.5
2
2.5
3
3.5
4
Before After After New

IMPLICATIONS

Implications
Documentation
increase
Is it because
documentation
stations/servers
are more
accessible in a
decentralized
configuration?

Implications
Nurse station
use decrease
Is it because the
need for
documenting
inside a nurse
station is
reduced?

Implications
On unit location
increase
Associated with
nurse station use
decrease?
Does this
represent an
increase in inter-
personnel
collaboration/
interaction.

Implications
Medication room
location
increase
Because of easier
access?

Supply storage
location
decrease
Are supplies
being delivered
inside patient
rooms?

Implications
Walking
distance
increase?
Counter intuitive
Does this
represent an
increase in inter-
personnel
collaboration/
interaction.

SUMMARY

Lessons Learned
Operational planning vs reality
- Paper intensive processes
- Added Telemetry reduced ICU census
- Geographic patient assignments new reality
- Chemo and blood products require two-nurse checks
- Feelings of isolation
- Missed ‘teachable moments’ for new staff
- Infection control discussions
- Medications “at the bedside” on the wish list
- Cannot get all supplies to the bedside
