harmonization of laboratory indicators, 09 03-2017
TRANSCRIPT

Harmonization of Laboratory Indicators
Ola H. ElgaddarMD, PhD, MBA, CPHQ, LSSGBLecturer of Chemical Pathology
Medical Research InstituteAlexandria University





Sources of Medical Errors
ØAvailable data used to focus on medicationrelated errors
ØHowever, in recent years, large scalesurveys have demonstrated that diagnosticerrors are a common occurrence includingerrors related to laboratory testing


Quality Indicators (QIs) …... Why?
ØAssess and monitor the quality system ofthe lab….......
ØPromotes and encourages investigationswhen errors occur….....

Quality Indicators (QIs) …... Why?
ØIdentify strategies and procedures forimprovement
ØEvaluate lab performance in relation tothe State-of-the-Art (i.e. benchmarking)

Quality Indicators (QIs) …... Why?
ØAccording to the ISO 15189:2012,clinical laboratories should identify criticalTTP activities and implement QIs in orderto highlight and monitor errors when theyoccur.
Harmonization
Harmonization, in music, is theimplementation of harmony, usually byusing chords, including harmonized scales

Harmonization – Lab Medicine
According to a patient-centeredviewpoint, harmonization is that theinformation should be comparableirrespective of the measurementprocedure used and where and/orwhen a measurement is made.

Provision of an accurateand actionable
laboratory information

Harmonization – Lab MedicineSCOPE = TTPØTests and test profiles requestØAnalytical processes and methodsØTerminologyØUnitsØReport formatsØReference intervalsØDecision limits
Back to
Are they harmonized??

Unfortunately, there is no consensuson common QIs covering the wholeTTP, nor there is an agreement oncommon terminology or targets!

Identifying a suitable State-of-the-Artis challenging, because it calls for theknowledge of error rates measured ina variety of laboratories throughoutthe world that differ in theirorganization and management,context, and population served

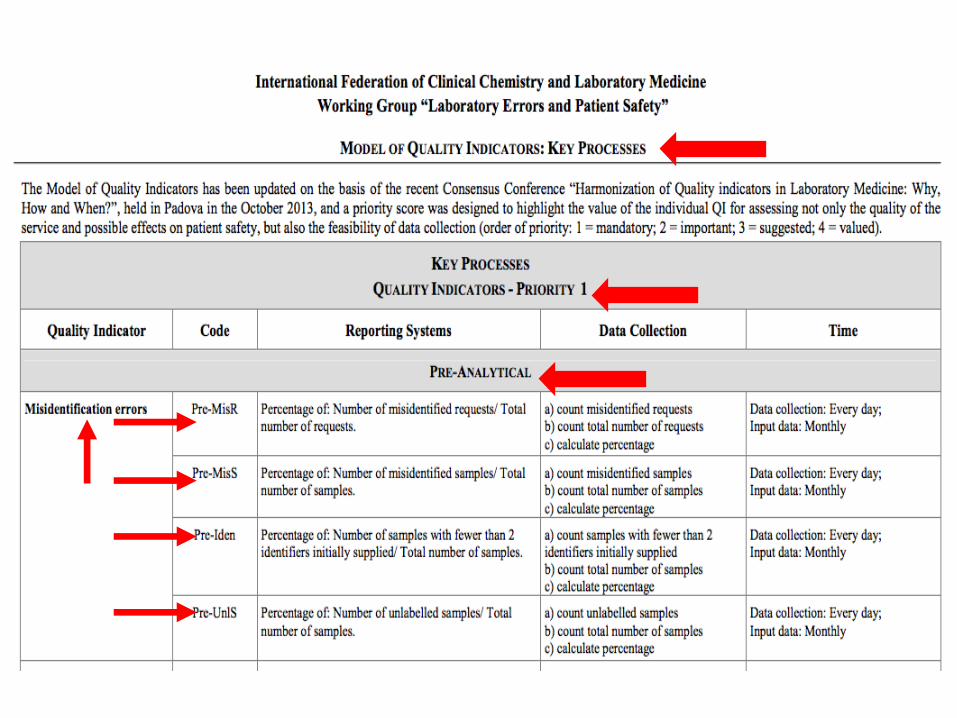
The Working Group “Laboratory Errors andPatient Safety” (WG-LEPS) of the IFCC has,since 2008, implemented a project aimed atdefining a common Model of QIs (MQI), aharmonized method for data collection,managed as an External Quality AssuranceProgram (EQAP) in which confidentiality isguaranteed


Preliminary MQI that was tested under realconditions by involving laboratories between 2008& 2013, then the main findings were discussed inthe Consensus Conference held in Padua in 2013

The achieved preliminary consensus onterminology, rationale, purpose andprocedures of data collection resulted in apreliminary set of reviewed and approvedquality indicators issued after the ConsensusConference, and used since 2014

A new MQI has beenissued after theConsensus Conferenceof Padua 2016, thatincludes:
Ø 53 measurements tomonitor
Ø 27 QIsØ Explanatory notesØ A priority index has
been assigned toeach quality indicator(“1” is the higherpriority; “4” the lower)

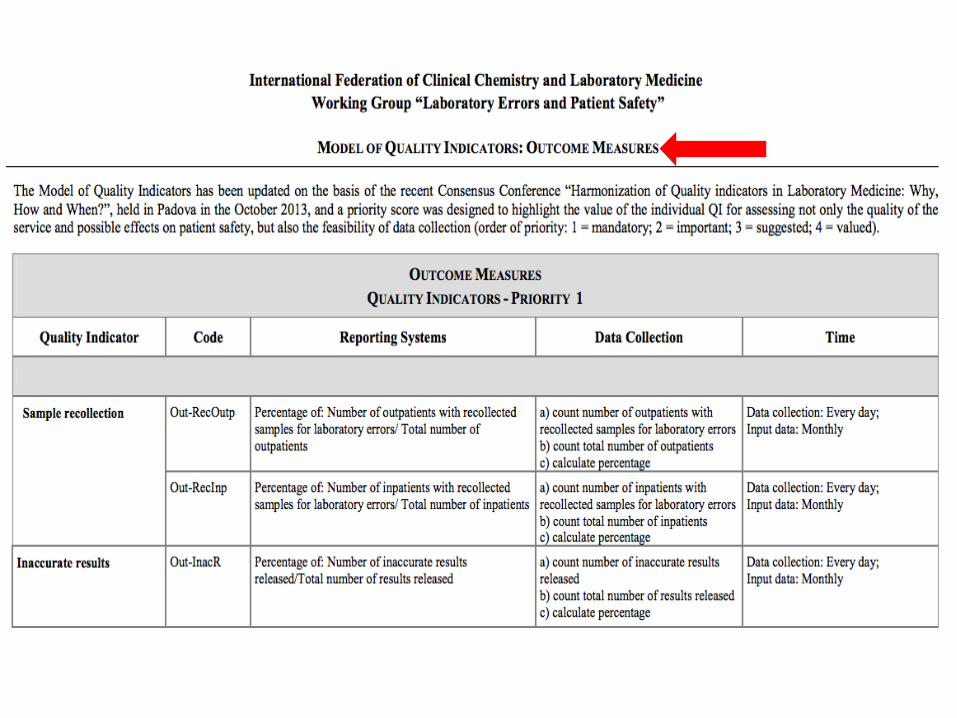
Indicators and measurementsØDifferent measures are often required toensure that an indicator is appropriatelymonitored.
ØIt is advisable to split an indicator intodifferent measures in order to considerall the events causing a specific error,and to benchmark data entered bydifferent laboratories to avoid misleadingcomparisons (Ex: In and outpatients)

All laboratories can use the new MQI, available in the website,since 2017. The laboratory results are collected on thespecifically-developed website (www.ifcc-mqi.com) andmanaged within an EQAP through which laboratory results areevaluated in comparison to the results of all participatinglaboratories.

In order to encourage laboratories toparticipate in the project, they are notcompelled to use all QIs proposed in themodel and they can, at least at the beginning,select the most appropriate QIs (chosen fromthose with “priority 1” assigned) and then, theymay eventually introduce and use further QIs.

A confidential report is periodically issued for eachlab containing the following information for each QI:
- Laboratory result;- Sigma value- Trend of the laboratory results and of the sigmavalues, over time;
- Distribution of frequency of laboratory results andof the sigma values.



Statistical data of QIs collected in the 2014, 2015 and 2016 (6 months)

QIs most widely used:
ØPre-analytical phase: a) unsuitablesamples and b) misidentified errors
ØAnalytical phase: a) unacceptableperformance in PT and b) tests withinappropriate IQC performance
ØPost-analytical phase: a) incorrectreports issued and b) inappropriate TAT

QIs most widely used:
For QIs of Outcome Measures and SupportProcesses, all indicators proposed in MQIappear to be used in a similar fashion, butonly by a small number of laboratories.

Most reported difficulties:
ØInadequate participation in QI datacollection by most labs, attributing this tothe ‘excessive’ number of QIs included inthe MQI
ØDifficulties in data collection, especiallywhen automated collection is unavailable.

Most reported difficulties:
ØDifficulty in meeting the deadline forcollecting and entering data in the MQI-dedicated website. Laboratories are moreinclined undertake the retrospectivecollection of data, with trans- missiondelayed by months or, in extreme cases, ayear.

