hanrahan waterborne diseases updated12 -...
TRANSCRIPT

© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Waterborne DiseasesJennifer Hanrahan, DO, MA
Chair, Infectious Disease Control CommitteeAssociate Professor, School of Medicine
Case Western Reserve University
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Financial Disclosures Jennifer Hanrahan, DO, MA Received consulting fees from Gilead Sciences, Inc. Advisory boards: Gilead Sciences, Inc., Cempra, and Astellas

© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Learning ObjectivesUpon completion, participants should be able to: Describe waterborne diseases Discuss when to suspect healthcare-acquired Legionella Explain methods to control Legionella spp in healthcare settings
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Outline Background on waterborne pathogens Case study Control and prevention methods for Legionella

© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Background on Waterborne Pathogens
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Global Impact Waterborne pathogens are among the most common causes of
disease worldwide with most diseases due to unsafe drinking water, poor sanitation, sewage and fecal contamination
More than 2 million deaths annually are caused by waterborne disease, most in children under age 5
Natural disasters such as floods, earthquakes, and hurricanes can cause disruption of drinking water and contamination with sewage
Even in the absence of natural disasters, more than 2.5 billion people do not have access to basic sanitation and are at risk of acquiring waterborne diseases
Ramirez-Castillo FY, et al. Pathogens. 2015;4:307-34; Watson JT, et al. Emerg Infect Dis. 2007;13:1-5.

© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Waterborne Pathogens Cryptosporidium Giardia Hepatitis A and E Legionella Naegleria fowleri Norovirus Salmonella/E. coli/Campylobact/Shigella Vibrio
Ramirez-Castillo FY, et al. Pathogens. 2015;4:307-34.
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Waterborne Illnesses Infection occurs after ingestion or inhalation of water mists OR
following exposure of non-intact skin to water contaminated with enteric pathogens
Water sources include drinking water, water parks, swimming pools, fountains, hot tubs, lakes, rivers, and flood waters after natural disasters
Contamination usually occurs when sewage containing enteric pathogens comes into contact with water sources
Food can also become contaminated by enteric pathogens via irrigation methods
Most waterborne pathogens are generally not healthcare acquired Ramirez-Castillo FY, et al. Pathogens. 2015;4:307-34; CDC. Waterborne Illnesses. www.cdc.gov;
CDC. Recreational water Illness. www.cdc.gov; CDC. Water Contamination. www.cdc.gov.

© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Symptoms of Waterborne Illnesses Diarrhea Conjunctivitis/ear infections Skin infections Hot tub lung
Ramirez-Castillo FY, et al. Pathogens. 2015;4:307-34;. CDC. Ear infections. www.cdc.gov;Elko L, et al. Curr Infect Dis Rep. 2003;5:398-406; ATS. Interstitial Lung Disease in a Hot Tub User. www.thoracic.org.
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Why Do Outbreaks Occur? Some pathogens are chlorine resistant Chlorine levels may be inadequate Not all water sources are chlorinated Water runoff after heavy rain can increase bacterial contamination
CDC. Effect of Chlorination on Inactivating Selected Pathogen. www.cdc.gov;Sinclair RG, et al. J Appl Microbiol. 2009;107:176-80; Kleinheinz GT, et al. Int J Microbiol. 2009;2009:876050.
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Challenges in Monitoring Waterborne Pathogens No one system of monitoring currently exists Methods that rely on indicator organisms such as E. coli may miss
other species Some organisms are difficult to culture Methods used have to be sensitive, specific, easy to perform, and
inexpensive
Ramirez-Castillo FY, et al. Pathogens. 2015;4:307-34.
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Milwaukee, WI: Cryptosporidium Outbreak In 1993, Milwaukee experienced the largest outbreak of drinking-water–related
Cryptosporidium in the US because of ineffective filtration at 1of 2 municipal water treatment plants More than 400,000 individuals (25% of Milwaukee’s population) became ill Costs exceded $96 million
First clues of the outbreak were pharmacies selling out of anti-diarrhea medications and increased ED visits for GI illness
69 people died; 93% had underlying HIV infection People were sick an average of 9 days with 12 stools per day; 1% were
hospitalized
Corso PS, et al. Emerg Infect Dis. 2003;9:426-31; Mac Kenzie WR, et al. N Engl J Med. 1994;331:161-7.

© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Flint, MI: Legionella and Shigella Outbreaks On 4/25/2014, Flint’s water source was changed from Lake Huron to Flint
River, resulting in the corrosion of pipes and increased lead and other contaminants in the water
Increased lead levels were found in children younger than 6 years Residents were advised to not drink the water on 10/15/15 Water contamination may have contributed to Legionella outbreak that
resulted in multiple deaths Outbreak of Shigella occurred because individuals were avoiding bathing in
the contaminated water Increase in skin rashes, but no clear cause found
Kennedy C, et al. MMWR Morb Mortal Wkly Rep. 2016;65:650-4; CDC. Flint Rash Investigation. www.atsdr.cdc.gov.
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Multiple States: Waterborne Pathogen Outbreaks Following Hurricane Katrina Skin lesions/rashes and MRSA outbreaks reported in shelters Outbreaks of Vibrio vulnificus and Vibrio parahaemolyticus 18 wound-associated cases, likely due to abrasions and contamination
with floodwater 4 non-wound associated cases of Vibro infection
More than1,000 cases of diarrhea reported in adults and children, some due to norovirus, salmonella, and Vibrio; all within 3 weeks after evacuation
CDC. MMWR Morb Mortal Wkly Rep. 2005;54:928-31;CDC. MMWR Morb Mortal Wkly Rep. 2005;54:961-4.

© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Case Study
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Case Study You are the director of infection prevention at a hospital located in
an area with recent flooding after a hurricane; the hospital experienced some flooding in non-patient-care areas, and construction is underway
It’s 4:55 pm on Friday afternoon, and you receive a call from a critical care physician concerned about a patient who was readmitted to the hospital with confusion, hyponatremia, and a right lower lobe infiltrate; the patient was discharged the week before after being admitted for an acute COPD exacerbation

© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Case Study On Monday morning, you look up the lab results on the patient The patient’s urine test is positive for the Legionella antigen What’s your next step?
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Legionella At least 60 species of Legionella, half of which have been associated with human
disease Majority of cases caused by L. pneumophila
Bacteria survive as intracellular parasites of amoebae, protozoa, or slime molds and can enter a non-replication state in low-nutrient environments, making them more resistant to biocides
Water conditions that promote bacterial growth include: Heat (68-122 F) Water stagnation Biofilm Sediment
OSHA. Legionairre’s Disease. www.osha.gov; CDC. Legionella (Legionnaires’ Disease and Pontiac Fever). www.cdc.gov;Lin YE, et al. Infect Control Hosp Epidemiol. 2011;32:166-73; Newton HJ, et al. Clin Microbiol Rev. 2010;23:274-98.

© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Legionella Transmission Legionella spp have been found in a wide range of aquatic habitats,
including lakes, streams, air conditioning cooling towers, potable water, fountains, and spa baths Colonization in hot-water-distribution systems in hospitals is common
Transmission occurs usually by the organism being inhaled from mist or aspirated
Exposure to contaminated soil has also been linked to infection One incident of person-to-person transmission reported
Newton HJ, et al. Clin Microbiol Rev. 2010;23:274-98;Lin YE, et al. Infect Control Hosp Epidemiol. 2011;32:166-73;
OSHA. Legionairre’s Disease. www.osha.gov.
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
2004
Legionella Epidemiology Reported Legionella cases have been on
the rise since 2000 More illnesses in the summer and early fall) Increased rainfall is associated with
increased risk True incidence may be higher due to
Legionella being underdiagnosed
Most outbreaks are community rather than healthcare-associated (nosocomial)
Cause of atypical CAP in some areasCDC. Legionella (Legionnaires’ Disease and Pontiac Fever). www.cdc.gov;
Garcia-Vidal C, et al. PLoS One. 2013;8:e61036;Soda EA, et al. MMWR Morb Mortal Wkly Rep. 2017;66:584-9;
CDC. Atypical Pneumonia. www.cdc.gov.
2011
2015
2014
2013
2002
2001
2000
2008
2012
2009
2.01.8
1.0
0.6
0
Legionnaires’ Disease Is on the Rise2000-2015*
Year*National Notifiable Diseases Surveilance System
Inci
den
ce
(Cas
es/1
00,0
00 P
op
ula
tio
n)
1.61.4
0.40.2
1.2
0.8
2003
2007
2010
2005
2006

© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Nosocomial Legionella Nosocomial cases of
Legionella are underrecognized and even one case may signal an outbreak
Argawal S, et al. Infect Dis Clin North Am. 2017;31:155-65; Soda EA, et al. MMWR Morb Mortal Wkly Rep. 2017:66;584-9.
16 of 21 Jurisdictions Reported Definite Cases of Healthcare-Associated Legionnaires’ Disease (LD) in 2015
*Alaska had no cases to report
Reported definite cases of healthcare-associated LDDid not report a definite case of healthcare-associated LDNot included in the analysis: jurisdictions reporting less than90% of Legionella infections to SLDSS, which contains information such as healthcare facility exposures
AZ
CO
TN
WY
WA
OR
CA
NVUT
NM
TX
OK
KS
SD
NDMT
ID
AK*
HI
LA
AR
MO
IA
MN
WI
IL IN
MI
OH
MEVT
PA
NY
VAWV
KY
ALMS
SC
NC
GA
FL
MA
DEMD NJ
DC
NYCNE
NH
RICT
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
People at Increased Risk of Legionella People 50 years or older Current or former smokers People with a chronic lung disease People with underlying illnesses like diabetes, kidney failure, or liver
failure People with weak immune systems or those on
immunosuppressants People with cancer
CDC. Legionella (Legionairre’s Disease and Pontiac Fever): Causes, How It Spreads, and People At Increased Risk. www.cdc.gov.

© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Factors That Can Lead to Legionella Growth Changes in water pressure due to construction or water main
breaks Can disrupt biofilm and free Legionella
Changes in municipal water quality Use of electronic-eye faucets More likely to be contaminated with Legionella than manual faucets
Failure to replace water system filters Allows for build-up of sediment and biofilm
Water stagnation in rarely used faucets, tubs, or showersCDC. Developing a Water Management Program to Reduce Legionella Growth and Spread in Buildings. www.cdc.gov;
Snydor ER, et al. Infect Control Hosp Epidemiol. 2012;33:235-40; Borella P, et al. Ann Ig. 2016;28:98-108.
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Clinical Signs and Symptoms of Legionella Symptoms include cough, fever, anorexia, headache, myalgia, nausea,
vomiting, diarrhea, mental status changes, seizures, and delirium Cough is purulent in 50% of patients, sputum is usually thin with few
WBCs Extra-pulmonary infection can occur but is rare
Pontiac Fever has symptoms of primarily fever and muscle aches and is a milder infection than Legionnaire’s disease
Cunha BA, et al. Lancet. 2016;387:376-85;CDC. Legionella (Legionnaires’ Disease and Pontiac Fever): Signs and Symptoms. www.cdc.gov.
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
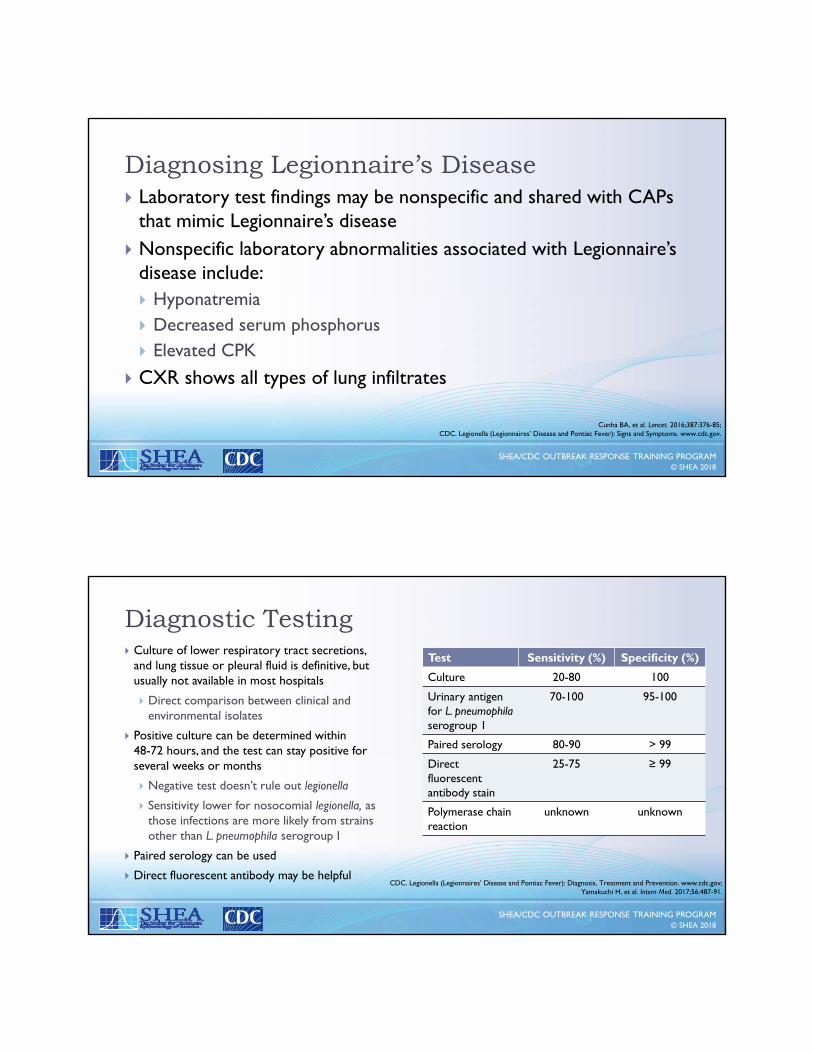
Diagnosing Legionnaire’s Disease Laboratory test findings may be nonspecific and shared with CAPs
that mimic Legionnaire’s disease Nonspecific laboratory abnormalities associated with Legionnaire’s
disease include: Hyponatremia Decreased serum phosphorus Elevated CPK
CXR shows all types of lung infiltrates
Cunha BA, et al. Lancet. 2016;387:376-85;CDC. Legionella (Legionnaires’ Disease and Pontiac Fever): Signs and Symptoms. www.cdc.gov.
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Diagnostic Testing Culture of lower respiratory tract secretions,
and lung tissue or pleural fluid is definitive, but usually not available in most hospitals
Direct comparison between clinical and environmental isolates
Positive culture can be determined within 48-72 hours, and the test can stay positive for several weeks or months
Negative test doesn’t rule out legionella
Sensitivity lower for nosocomial legionella, as those infections are more likely from strains other than L. pneumophila serogroup I
Paired serology can be used
Direct fluorescent antibody may be helpfulCDC. Legionella (Legionnaires’ Disease and Pontiac Fever): Diagnosis, Treatment and Prevention. www.cdc.gov;
Yamakuchi H, et al. Intern Med. 2017;56:487-91.
Test Sensitivity (%) Specificity (%)
Culture 20-80 100
Urinary antigen for L. pneumophilaserogroup 1
70-100 95-100
Paired serology 80-90 > 99
Direct fluorescent antibody stain
25-75 ≥ 99
Polymerase chain reaction
unknown unknown

© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Who Should Be Tested for Legionella? Anyone who has failed outpatient antibiotic therapy for pneumonia
Anyone admitted to the ICU with pneumonia or severe CAP
Immunocompromised patients
Patients with a travel history or an overnight stay in a healthcare facility within 14 days before the illness (10% of cases associated with travel)
Patients with pneumonia in the setting of an outbreak
Anyone with pneumonia ≥ 48 hours after admission to healthcare facility
Mandell LA, et al. Clin Infect Dis. 2007;44:S27-72;CDC. Legionella (Legionnaires’ Disease and Pontiac Fever): Diagnosis, Treatment and Prevention. www.cdc.gov.
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Investigation of Cases Case definition
If ≥1 definite healthcare-acquired (patient spent the entire prior 10 days in healthcare facility) or ≥ 2 possible healthcare-associated cases (patients spent part of prior 10 days in same facility before symptoms began) occurs, conduct an investigation
Exposure/epidemiologic history Environmental sampling
CDC. Guidelines for Preventing Health-Care–Associated Pneumonia. www.cdc.gov.

© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Control and Prevention Methods for Legionella
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Facility Requirements to Prevent Legionella Infections On June 2, 2017, the Centers for Medicare and Medicaid Services
at the Department of Health and Human Services issued a memo stating that:
Facilities (hospitals, CAHs, and LTC) must develop and adhere to policies and procedures that inhibit microbial growth in building water systems that reduce the risk of growth and spread of legionella and other opportunistic pathogens in water
CMS. www.cms.gov.
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Immediate Control Methods Superheat and flush Hyperchlorination Point-of-use filtration
Lin YE, et al. Infect Control Hosp Epidemiol. 2011;32:166-73.
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Long-Term Control Methods Copper-silver ionization (CSI)
Legionellae can develop tolerance to silver ions, and higher concentrations may be needed over time; copper can precipitate at alkaline pH, leading to decrease in efficacy
Monochloramine Chlorine dioxide
Useful over a broader range of pH (6.0-8.5)
Lin YE, et al. Infect Control Hosp Epidemiol. 2011;32:166-73;Dziewulski DM, et al. Am J Infect Control. 2015;43:971-6.

© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
CSI Copper and silver ions are both bactericidal against Legionella and other waterborne
pathogens Copper ion concentration should be tested weekly with a field colorimeter kit Silver ion concentration testing is more complex and should be done every 2
months
For a typical 250-bed hospital’s hot water recirculating line, the cost of an ionization system is ~$40,000 to $50,000 Relatively easy to install and maintain Elevated pH and low ion concentration may compromise efficacy Failures of the ionization system to prevent L. pneumophila in hospitals have
occurred due to resistant organisms and inadequate ion levels Lin YE, et al. Infect Control Hosp Epidemiol. 2011;32:166-73.
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Chlorine Dioxide Method used in Europe since the 1940s
Advantages of chlorine dioxide disinfection include: Superior penetration into biofilms compared with chlorine Biocidal action maintained over a wider pH range compared with chlorine and
CSI
Disadvantages include: Prolonged time before significant reductions in Legionella positivity rate Reactions with organic material and corrosion scale in piping can produce chlorite
and chlorate, which may pose health risks Challenging to maintain effective residual concentration
Cost varies depending on whether the equipment is purchased or leased
Lin YE, et al. Infect Control Hosp Epidemiol. 2011;32:166-73.
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Monachloramine This water treatment has not been evaluated as extensively as
chlorine dioxide or CSI Monochloramine provides a steady residual that penetrates biofilm
and has a wider working pH range than chlorine or CSI Disadvantages include that it may cause drinking water to take on
an ammonia odor, and it may cause an increase in other microorganisms (Mycobacterium species)
Lin YE, et al. Infect Control Hosp Epidemiol. 2011;32:166-73.
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
CDC. Developing a Water Management Program to Reduce Legionella Growth and Spread in Buildings. www.cdc.gov.

© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
CDC. Developing a Water Management Program to Reduce Legionella Growth and Spread in Buildings. www.cdc.gov.
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
CDC. Developing a Water Management Program to Reduce Legionella Growth and Spread in Buildings. www.cdc.gov.

© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Conclusions Outbreaks of a number of different waterborne diseases can occur
after natural disasters Disruption of water and fluctuations in water pressure can have
specific implications for healthcare facilities and can increase the risk of Legionella
Even one case of healthcare-acquired Legionella is concerning and warrants further investigation
A water-management policy is an important component of infection prevention
© SHEA 2018SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Additional References Rebmann T. Assessing Hospital Emergency Management Plans: A Guide for Infection
Preventionists. www.ncbi.nlm.nih.gov/pubmed/19699558
Crises and Emergency Risk Communication (CERC). Centers for Disease Control and Prevention. emergency.cdc.gov/cerc/index.asp
Emergency Preparedness and Response Preparation and Planning. Centers for Disease Control and Prevention. emergency.cdc.gov/planning/
Hospital All-Hazards Self-Assessment. Centers for Disease Control and Prevention. www.cdc.gov/phpr/healthcare/documents/hah_508_compliant_final.pdf
Hospital Emergency Management Program Checklist. California Hospital Association. www.calhospitalprepare.org/sites/main/files/file-attachments/emp_checklist_v080311.doc