handbook for clinical supervisors - oxford deanery · the latest foundation handbook ... named...
TRANSCRIPT

2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 1
Handbook / Field Guide for Supervisors of Medical and Dental trainees working in HE Thames Valley
Jane Siddall, Associate Dean for Educator and Faculty Development
John Derry, Director CDU and Associate Dean
Tony Jefferis, Deputy Dean
Simon Street, GP Associate Dean
Greg Simons, GP Associate Dean
Chris Morris, Associate Dean for Quality
Amit Gupta, Associate Dean for International Medical Graduates
2nd edition Sept 2013
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 2
This handbook has been produced using material from the
Gold Guide, (4th edition, 2010)
GMC guidance (The Trainee Doctor, July 2011 and Tomorrow’s Doctors, Oct 2011)
NACT guidance (Managing the Trainee in Difficulty, 2008),
The Oxford Deanery workshops for both Clinical and Educational Supervisors
‘Best practice’ from Employment Tribunal experience, (August 2011).
The UK Foundation Programme Reference Guide, (July 2012).
Oxford Deanery Policies (2012)
NHS Medical Careers website (2012)
The British Dyslexia Association (2012)
The Equality Act (2010)
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 3
Contents Introduction: Background and importance of supervision Chapter 1 Definitions and Differences Chapter 2 What are the essential responsibilities of clinical supervisors? Chapter 3 Feedback on Performance Chapter 4 The International Medical Graduate Chapter 5 ‘Something isn’t right’ Appendices A: ARCP outcomes B: Generation y: what they expect C: The Oxford Deanery Descriptors of Behaviour D: Adult checklist for Dyslexia PGMDE polices are accessible from the home page of the HE Thames Valley website at http://thamesvalley.hee.nhs.uk/ The third tab along the top banner ‘Oxford PGMDE’ takes the reader to the familiar Oxford Deanery homepage. Policies which may be especially useful include Policy for approving and recognising medical and dental trainers
(covers training requirements, time, duties etc, found in the Educator Development section)
Equality and Diversity Bullying and Harassment IMG policy Less than fulltime training Trainee in difficult / supporting the trainee Guidance for pregnant trainees
And can be found in the ‘About…’ Oxford Deanery section’ of the website
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 4
Introduction Forward by the Post-Graduate Dean : The expectations on those undertaking educational roles have increased enormously in the last few years. There is now a requirement to properly induct, plan, assess, deliver specific curriculum objectives and vitally, record many aspects of doctors’ performance during training. There is abundant evidence that well trained and supported doctors work safely, and that those who aren’t are more likely to be involved in adverse events which may damage their professional standing, the reputation of the department, Trust or training programme as well as patient harm. I am delighted that our team of Associate Deans has produced this field guide for trainers in medical and dental practice across our patch. It is intended to be a ’quick look book’ to help busy clinical and educational supervisors navigate through an increasingly complex training landscape. It is not, however, a replacement for effective supervision.
Dr Michael Bannon Postgraduate Dean
Background There are comprehensive national frameworks for Foundation, General Practice and Specialty Trainees, and local PGMDE policies, which can be accessed on the internet. Most, if not all, can be accessed through the HETV website and clicking on the relevant tabs in the PGMDE / Deanery area of the site. The latest Foundation handbook (2012) can be downloaded from the Foundation Programme NHS website at http://www.foundationprogramme.nhs.uk Why is training (and support) for trainers important?
During 2012 the GMC opened a consultation on the recognition and approval of non-GP trainers. The outcome of the consultation was published in August 2012 as the GMC ‘Approving and Recognising Trainers: the Implementation Plan’. Trainers must have training, and have been updated as required under the Oxford Deanery policy for Approving and Recognising Medical and Dental trainers.
The GMC plan relates to:
named educational supervisors in postgraduate training
named clinical supervisors in postgraduate training
lead co-ordinators of undergraduate training at each local education provider
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 5
doctors responsible for overseeing students’ educational progress for each medical school.
Other doctors whose practice contributes to the teaching, training or supervision of students or trainee doctors, on a more sessional or occasional basis. such as senior trainees and most specialty doctors who observe practice are not included in the GMC plan, but the Deanery has commissioned training in supervision for such staff.
The GMC trainer standards
The GMC already has existing standards for postgraduate training set out in The Trainee Doctor (in section 6 of the 2011 publication) and for undergraduate education in Tomorrow’s Doctors. These address
the differing levels of supervision trainees require during the entire post-graduate training programme, (6.29 to 6.31)
the expectation that the Post Graduate Medical education team will support the trainer and that job plans will factor time for the trainer to facilitate trainee development (6.32-6.36)
the expectation that trainers understand the structure and purpose of the training programme, and their role in training (6/38- 6.39)
and for GP training, section 6.37 stipulates that GP trainers must be trained and selected in accordance with the Medical Act 1983.

2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 6
Chapter 1
Definitions and Differences Definitions
The GMC has defined the roles of both clinical and educational supervisors, which are:
Named clinical supervisor: a trainer who is responsible for overseeing a specified trainee’s clinical work for a placement in a clinical environment and is appropriately trained to do so. He or she will provide constructive feedback during that placement, and inform the decision about whether the trainee should progress to the next stage of their training at the end of that placement and/or series of placements. Named educational supervisor: a trainer who is selected and appropriately trained to be responsible for the overall supervision and management of a trainee’s trajectory of learning and educational progress during a placement and/or series of placements. Every trainee must have a named educational supervisor. The educational supervisor’s role is to help the trainee to plan their training and achieve agreed learning outcomes. He or she is responsible for the educational agreement and for bringing together all relevant evidence to form a summative judgement at the end of the placement and/or series of placements. It is expected that educational supervisors should have all the attributes expected of trained clinical supervisors. Being an educational supervisor does not necessarily preclude a trainer from having any other educational role, and is it desirable for senior educators to be active educational supervisors. PGMDE definitions of other key supervisors are: Academic supervisors are responsible to help the trainee to plan their research activity and achieve agreed outcomes. Even if he or she has a clinical contract, they should not normally be the trainee’s educational or clinical supervisor. He or she is required to provide an annual report on a trainee for the ARCP panel. A sessional supervisor is a clinician who supervises a trainee for individual sessions, and who may be required to provide formal assessment and feedback on the trainee to their clinical, or educational, supervisor.
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 7
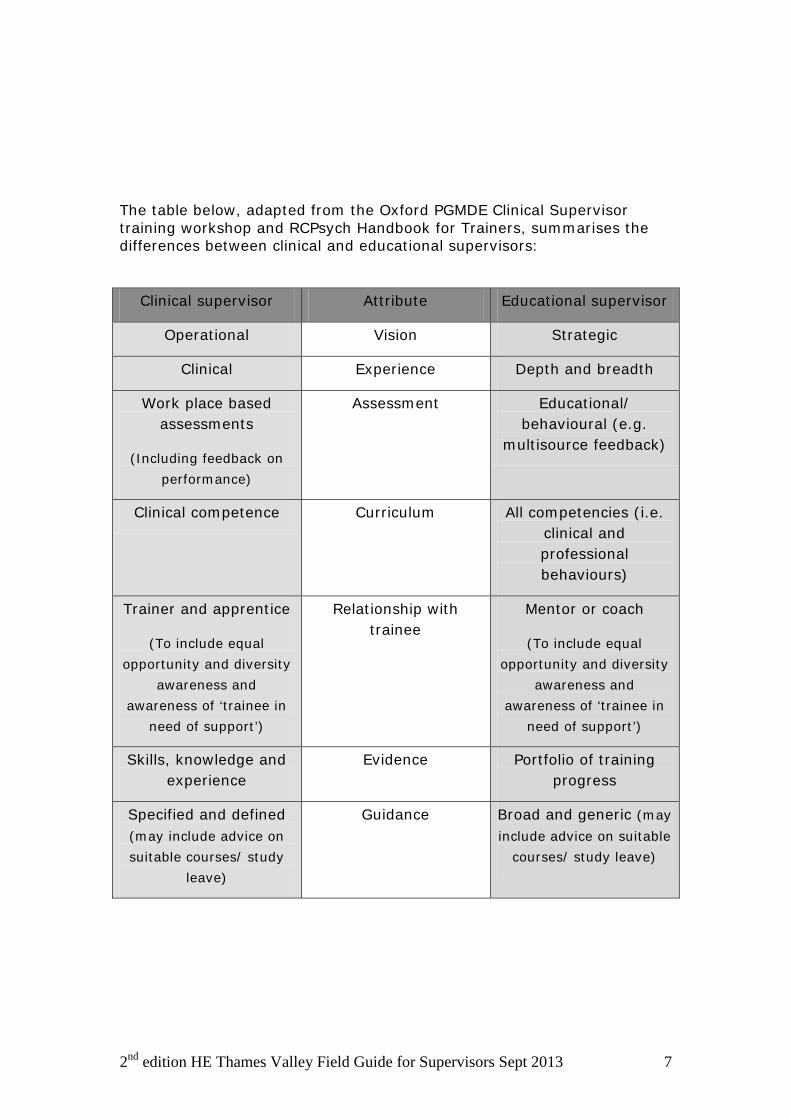
The table below, adapted from the Oxford PGMDE Clinical Supervisor training workshop and RCPsych Handbook for Trainers, summarises the differences between clinical and educational supervisors:
Clinical supervisor Attribute Educational supervisor
Operational Vision Strategic
Clinical Experience Depth and breadth
Work place based assessments
(Including feedback on performance)
Assessment Educational/ behavioural (e.g.
multisource feedback)
Clinical competence Curriculum All competencies (i.e. clinical and professional behaviours)
Trainer and apprentice
(To include equal opportunity and diversity
awareness and awareness of ‘trainee in
need of support’)
Relationship with trainee
Mentor or coach
(To include equal opportunity and diversity
awareness and awareness of ‘trainee in
need of support’)
Skills, knowledge and experience
Evidence Portfolio of training progress
Specified and defined (may include advice on suitable courses/ study
leave)
Guidance Broad and generic (may include advice on suitable
courses/ study leave)
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 8
Chapter 2 What are the ‘essential’ responsibilities of Clinical Supervisors? It is important to make early contact with the trainees allocated to you, ideally face to face, but if not, by email to arrange a meeting. A suggested algorithm is at the end of this chapter. It is important that CSs inform a trainee’s Educational Supervisor of anything which is noteworthy, but should include involvement in Serious Incidents, complaints from patients and health / probity issues (see Chapter 4) as these events are noted at ARCP and inform the revalidation process.
Your knowledge of the curriculum As a clinical supervisor (CS), one is not expected to produce the annual assessment report for the ARCP, but a CS should know what skills the trainee should develop, or acquire, during the phase of training with you. This should be available on your Royal College website. CSs do not personally have to sign off every workplace based assessment, but it is good practice for a proportion to be completed by a consultant. Some colleges require the final one confirming independent competence for a procedure to be signed by a consultant. Whilst a clinical supervisor will not be suggesting the likely outcome of the ARCP to a trainee (this is the responsibility of the Educational Supervisor), it is worth being aware of the possible outcomes and what the trainee needs to achieve. (See Appendix A for detail on forms and ARCP outcomes) The e-portfolio All foundation trainees use an electronic portfolio, and increasingly, trainees in all specialties are being registered through the Royal Colleges. Each specialty has a slightly different set of sections to be completed by trainees and their assessors, which is outside the scope of this handbook. However, your local College / Specialty Tutor should have a good understanding of your eportfolio system, or there may be a member of your School Board who has been charged with ensuring consultants know how to navigate the system. Your specialty Head of School may organise formal training on eportfolio from time to time.
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 9
Work place based assessments (WPBAs) All trainees are required to demonstrate their acquisition of relevant clinical skills and behaviours in a structured manner, as described in the relevant specialty curriculum. A clinical supervisor is expected to facilitate this process by aiding learning using WPBA tools formatively, to give constructive feedback on performance and advice on how to improve further, and summatively, when a trainee is observed carrying out the procedure or consultation independently. There are three steps in the assessment process:
Evidence by observation of trainee, e.g. ‘I see evidence of your findings’
Relevance by explanation, e.g. ‘if you don’t record your findings, no-one else will know what you did’
Competence by evaluation, e.g. ‘these notes do not contain enough information’
And finally, giving feedback to trainee. What sorts of work place based assessments are there and how can they be fitted into my job plan? Fundamentally, there are three types of activity that trainees undertake where a more senior clinician should observe practice, and feedback to the trainee, using forms delivered by the Foundation Programme or relevant medical Royal College. The forms can be found in the relevant specialty eportfolio and / or college website. These are
One where the trainee carries out a practical procedure, such as a cannulation, insertion of a chest drain or a hysterectomy. (DOPs, OSATS or other acronyms, dependent upon specialty).
Mini clinical examinations, where the trainee is observed for part of a consultation with a patient. The focus for assessment may be one of: the presentation of the patient’s history, the taking of a history, the examination, proposed management and explanation of investigations.
Case based discussions, where the trainee may discuss a real case, or a condition which is rare, but of which the specialty curriculum demands evidence of at least some supervised discussion (such as a pregnant woman with cystic fibrosis).
The first two activities can usually be easily accommodated ‘on the job’ in theatres, on ward rounds, and occasionally in clinic consultations. Case based discussions will need some time setting aside, but it is possible to pool resources and invite other trainees and run an interactive and

2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 10
discursive tutorial session. These could time tabled for a number of afternoons a year within the teaching timetable, with one or two supervisors leading each session.
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 11
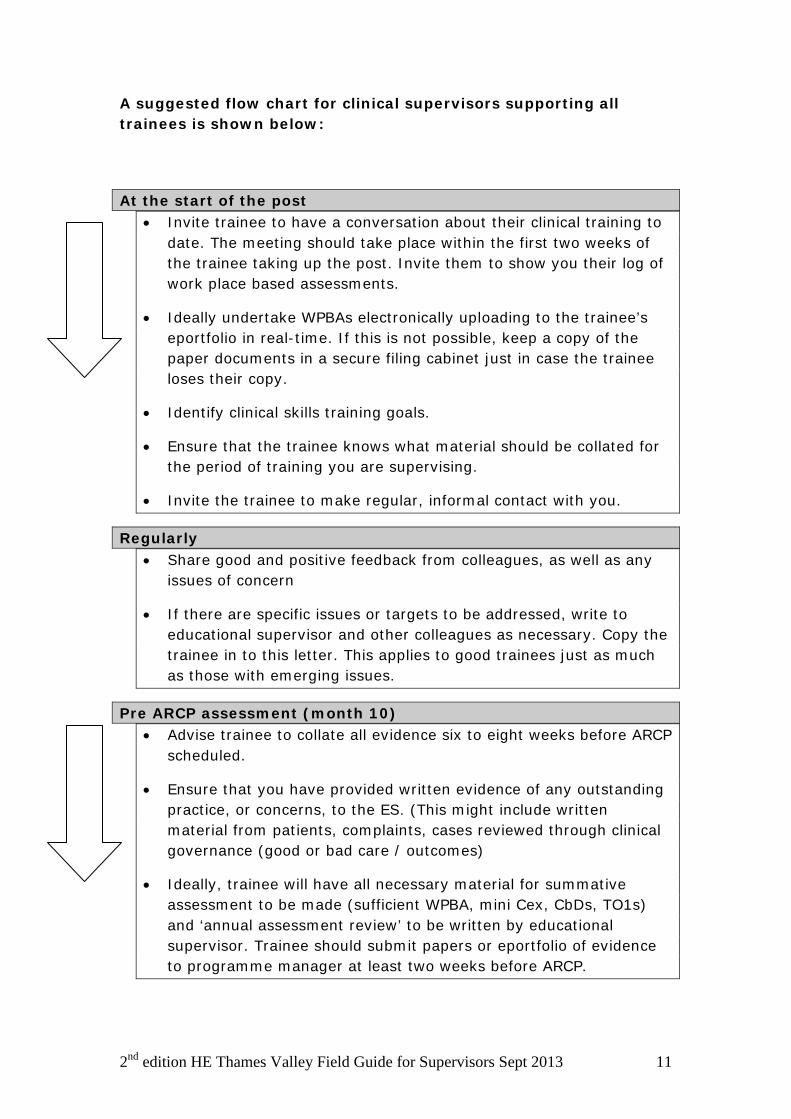
A suggested flow chart for clinical supervisors supporting all trainees is shown below:
At the start of the post • Invite trainee to have a conversation about their clinical training to
date. The meeting should take place within the first two weeks of the trainee taking up the post. Invite them to show you their log of work place based assessments.
• Ideally undertake WPBAs electronically uploading to the trainee’s eportfolio in real-time. If this is not possible, keep a copy of the paper documents in a secure filing cabinet just in case the trainee loses their copy.
• Identify clinical skills training goals.
• Ensure that the trainee knows what material should be collated for the period of training you are supervising.
• Invite the trainee to make regular, informal contact with you.
Regularly • Share good and positive feedback from colleagues, as well as any
issues of concern
• If there are specific issues or targets to be addressed, write to educational supervisor and other colleagues as necessary. Copy the trainee in to this letter. This applies to good trainees just as much as those with emerging issues.
Pre ARCP assessment (month 10) • Advise trainee to collate all evidence six to eight weeks before ARCP
scheduled.
• Ensure that you have provided written evidence of any outstanding practice, or concerns, to the ES. (This might include written material from patients, complaints, cases reviewed through clinical governance (good or bad care / outcomes)
• Ideally, trainee will have all necessary material for summative assessment to be made (sufficient WPBA, mini Cex, CbDs, TO1s) and ‘annual assessment review’ to be written by educational supervisor. Trainee should submit papers or eportfolio of evidence to programme manager at least two weeks before ARCP.
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 12
It is best practice to (i) Keep copies of invitations sent to trainee by using
‘read receipts’ on email (ii) Sign all entries made by yourself into any trainee’s
eportfolio

2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 13
Chapter 3 Feedback on performance What is effective feedback? ‘Information about a performance or behaviour which leads to action to affirm, or develop, that performance or behaviour’. Ideally, feedback should be given close in time to the event, and should be in a private setting (particularly if behaviour modification is mooted). It should also be clear; avoid sandwiching the bit which needs improvement between two nuggets of praise as the trainee will miss hearing the awful bit. Feedback should increase the trainee’s insight and motivate them to either continue (or modify if necessary) their practice or behaviours. It is helpful to have a benchmark the level expected of the trainee. However, if the goal is perceived to be unrealistic, trainee motivation will drop off. Thus, feedback needs to be offered using the Norcini and Burch (2007) headings:
S specific N non-judgemental B balanced P promotes reflection T timely
For example, you have just observed a consultation between a patient with recurrent episodes of cramping abdominal pain and a trainee, where the patient mentioned a fear that the pain may be a symptom of cancer, and alluded to a relative having been diagnosed with colon cancer a few years earlier. The trainee did not pick up on this thread of concern, simply suggesting that a colonoscopy would be a useful investigation. Aca clinical supervisor, you might open the feedback conversation with, ‘What do you think was the patient’s greatest concern today?’ If your are checking a set of notes where the trainee has failed to record important negative findings during an examination, for example there being no weakness in the limbs of an elderly patient admitted following a collapse at home, the feedback should not be ’these notes are useless’, but something along the lines of ‘it is really valuable to state that she did not have any weakness on admission, so that the team on duty overnight will be aware of a deterioration if this develops’. It can also be tricky to give feedback to a trainee who is doing well, but finding something to gently challenge them is educational in a way that the report ’well you obviously can do that OK’ is not. In these circumstances, open questions such as ‘is there anything you would do
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 14
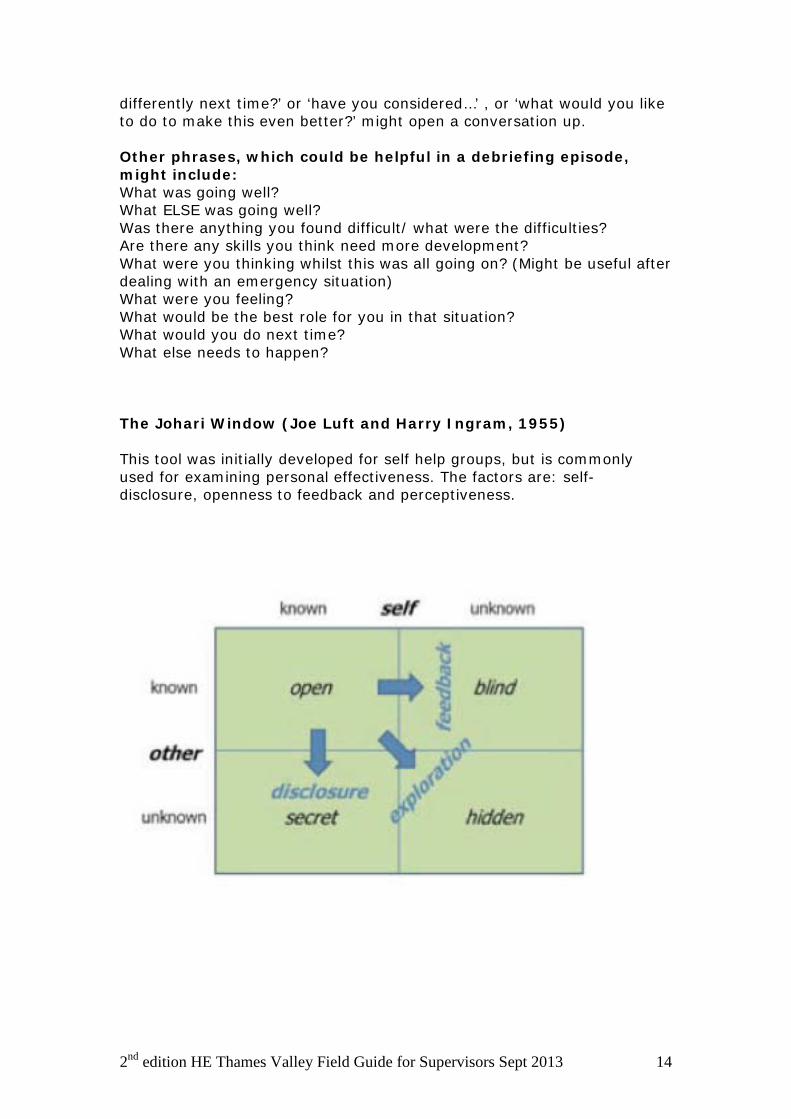
differently next time?’ or ‘have you considered…’ , or ‘what would you like to do to make this even better?’ might open a conversation up. Other phrases, which could be helpful in a debriefing episode, might include: What was going well? What ELSE was going well? Was there anything you found difficult/ what were the difficulties? Are there any skills you think need more development? What were you thinking whilst this was all going on? (Might be useful after dealing with an emergency situation) What were you feeling? What would be the best role for you in that situation? What would you do next time? What else needs to happen? The Johari Window (Joe Luft and Harry Ingram, 1955) This tool was initially developed for self help groups, but is commonly used for examining personal effectiveness. The factors are: self-disclosure, openness to feedback and perceptiveness.

2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 15
And with a shared dialogue the windowpanes change size It may be worth remembering that even experienced supervisors can find it challenging to give positive feedback to learners. Frequently, there is a mismatch between teachers’ and learners’ perceptions of the adequacy and effectiveness of feedback. (Ramani S and Krakov SK, Twelve tips for giving feedback effectively in the clinical environment. Medical Teacher, 2012;34: 787-791 )
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 16
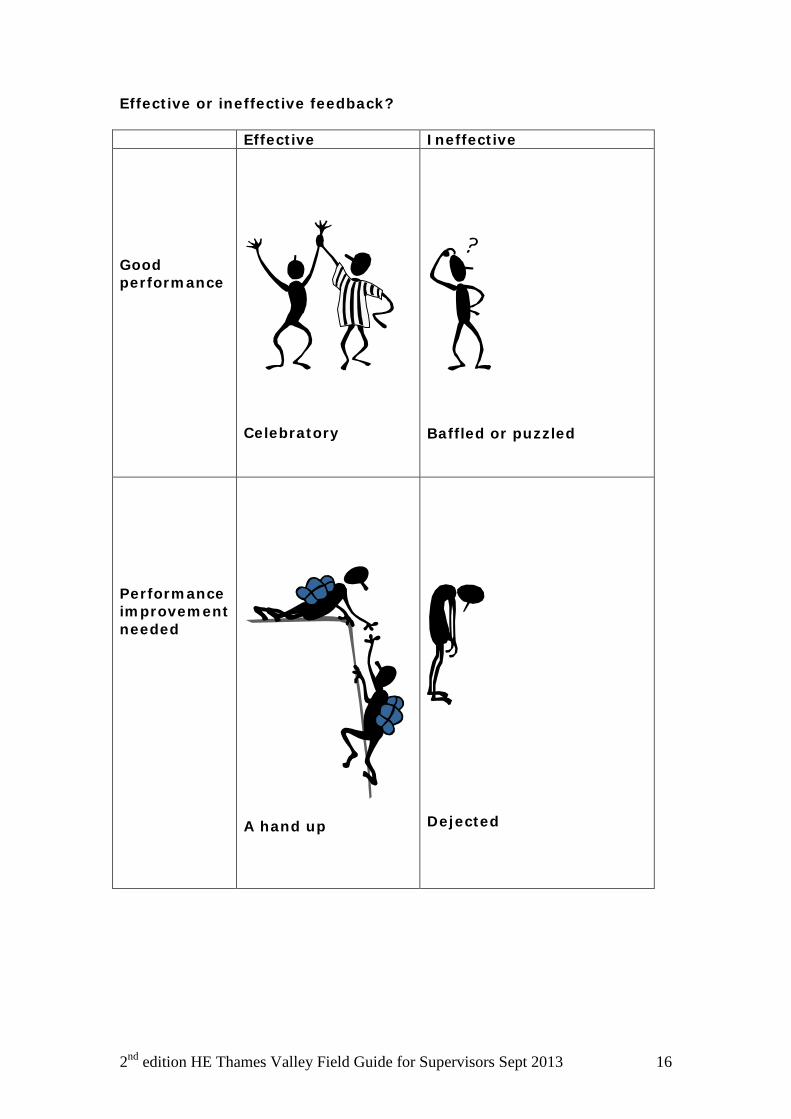
Effective or ineffective feedback? Effective Ineffective Good performance
Celebratory
Baffled or puzzled
Performance improvement needed
A hand up
Dejected
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 17
Chapter 4 The International Medical Graduate trainee International medical graduates constitute 32% of the medical workforce with more than one-in-three hospital doctors and one-in-five general practitioners having qualified overseas. In 2006, there were major changes in the immigration laws which have led to a substantial change in the demographics and numbers of international medical graduates applying. Any NHS organisation wanting to employ a doctor from outside the EEA has to prove that the post could not be filled by a doctor who qualified in the UK or the EEA. Information regarding exceptions to this rule and detailed guidance on IMG recruitment and training issues is available at http://www.oxforddeanery.nhs.uk/trainees/img_doctors.aspx. Induction programme IMGs should attend the Trust run Induction Programme, normally on the first day or two days at the start of the new appointments (in the first week of August or February). Attendance at this is compulsory, as it will provide all the vital local information about working in any particular Trust. The deanery aims to set up an induction programme specifically for IMGs details of which would be announced on this website. Support
The BMA have published a very useful document entitled: "Working and Training in the United Kingdom National Health Service - a guide for International Medical Graduates (IMGs)", available through its website. The Deanery's Associate Director for Overseas Doctors (IMGs), Dr Amit Gupta has responsibility for matters specific to doctors who have qualified outside the UK, whether in the EEA countries or elsewhere, or whose nationality does not allow automatic right of permanent residence in the UK. These include:
• Guidance regarding visa status • Career guidance in relation to overseas status • Advice in connection with training and non-training posts • Assistance with the Medical Training Initiative Scheme • Provision of induction for IMGs • Advice to doctors enquiring from overseas about postgraduate
training • Support for refugee and asylum-seeking doctors in the Oxford area
Both IMGs and their supervisors can contact Dr Amit Gupta, the Associate Dean for IMGs through the Deanery for specific advice at [email protected]

2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 18
The CDU can also help with mentoring and confidential coaching for doctors who for whatever reason finds they are in personal or career difficulty. The CDU can be contacted on [email protected].
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 19
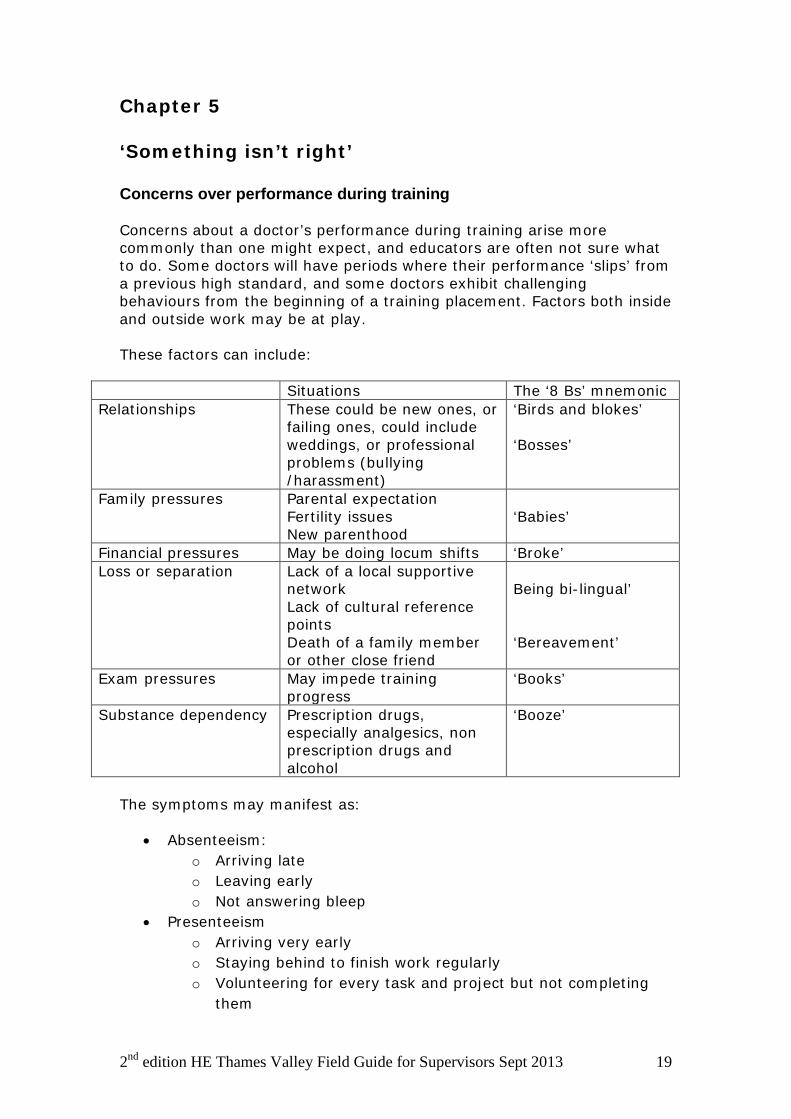
Chapter 5 ‘Something isn’t right’ Concerns over performance during training Concerns about a doctor’s performance during training arise more commonly than one might expect, and educators are often not sure what to do. Some doctors will have periods where their performance ‘slips’ from a previous high standard, and some doctors exhibit challenging behaviours from the beginning of a training placement. Factors both inside and outside work may be at play. These factors can include:
Situations The ‘8 Bs’ mnemonic Relationships These could be new ones, or
failing ones, could include weddings, or professional problems (bullying /harassment)
‘Birds and blokes’ ‘Bosses’
Family pressures Parental expectation Fertility issues New parenthood
‘Babies’
Financial pressures May be doing locum shifts ‘Broke’ Loss or separation Lack of a local supportive
network Lack of cultural reference points Death of a family member or other close friend
Being bi-lingual’ ‘Bereavement’
Exam pressures May impede training progress
‘Books’
Substance dependency Prescription drugs, especially analgesics, non prescription drugs and alcohol
‘Booze’
The symptoms may manifest as:
• Absenteeism: o Arriving late o Leaving early o Not answering bleep
• Presenteeism o Arriving very early o Staying behind to finish work regularly o Volunteering for every task and project but not completing
them
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 20
• Lack of rapport with peers o Nurses o Colleagues at same level o Junior or student colleagues
• Higher incidence of name appearing in grumbles, formal complaints or case reviews than peers
• Poor attention to paperwork o Reviewing patient’s results and following them up o Uneven accrual of WPBAs o Failure to register with NHS e-portfolio
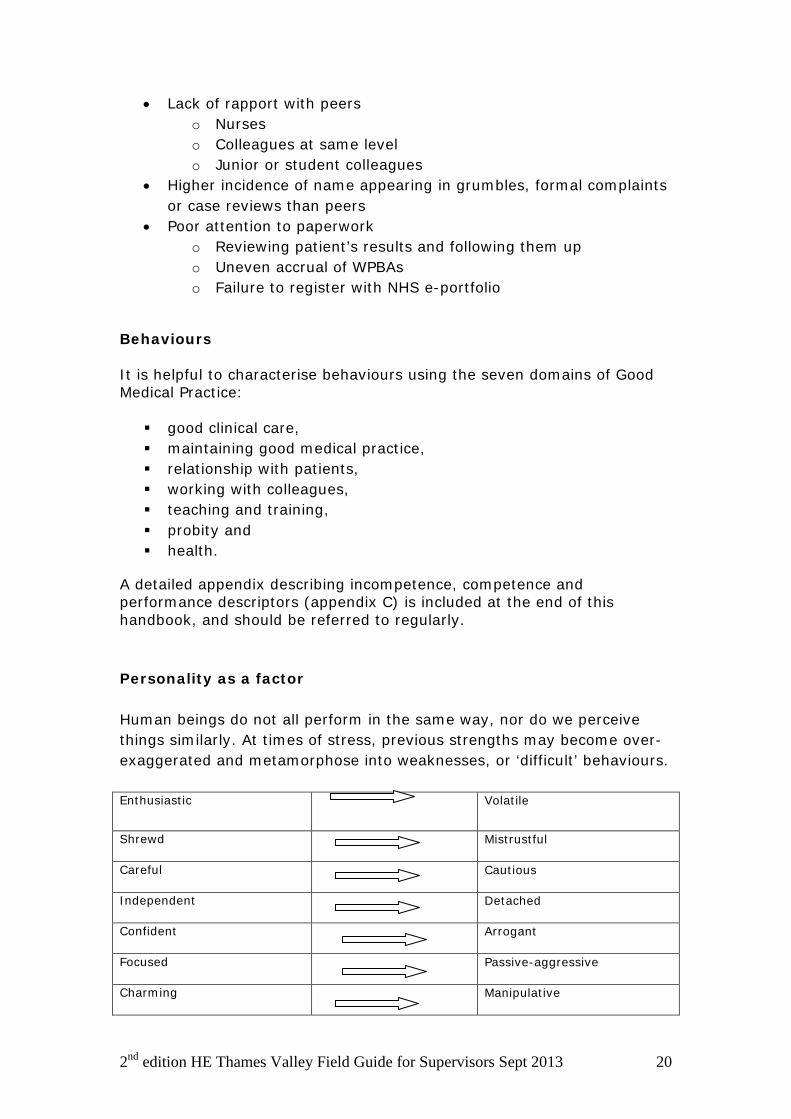
Behaviours It is helpful to characterise behaviours using the seven domains of Good Medical Practice: good clinical care, maintaining good medical practice, relationship with patients, working with colleagues, teaching and training, probity and health.
A detailed appendix describing incompetence, competence and performance descriptors (appendix C) is included at the end of this handbook, and should be referred to regularly. Personality as a factor Human beings do not all perform in the same way, nor do we perceive things similarly. At times of stress, previous strengths may become over-exaggerated and metamorphose into weaknesses, or ‘difficult’ behaviours. Enthusiastic
Volatile
Shrewd Mistrustful
Careful Cautious
Independent Detached
Confident Arrogant
Focused Passive-aggressive
Charming Manipulative
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 21
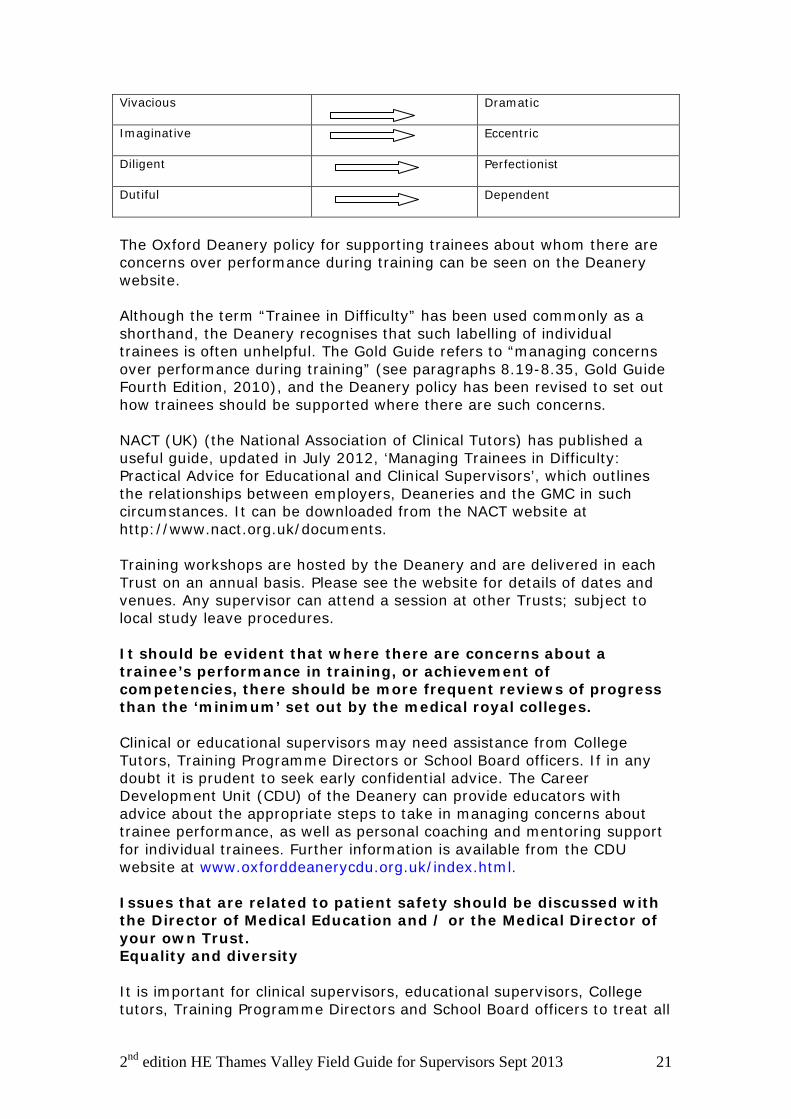
Vivacious Dramatic
Imaginative Eccentric
Diligent Perfectionist
Dutiful Dependent
The Oxford Deanery policy for supporting trainees about whom there are concerns over performance during training can be seen on the Deanery website. Although the term “Trainee in Difficulty” has been used commonly as a shorthand, the Deanery recognises that such labelling of individual trainees is often unhelpful. The Gold Guide refers to “managing concerns over performance during training” (see paragraphs 8.19-8.35, Gold Guide Fourth Edition, 2010), and the Deanery policy has been revised to set out how trainees should be supported where there are such concerns. NACT (UK) (the National Association of Clinical Tutors) has published a useful guide, updated in July 2012, ‘Managing Trainees in Difficulty: Practical Advice for Educational and Clinical Supervisors’, which outlines the relationships between employers, Deaneries and the GMC in such circumstances. It can be downloaded from the NACT website at http://www.nact.org.uk/documents. Training workshops are hosted by the Deanery and are delivered in each Trust on an annual basis. Please see the website for details of dates and venues. Any supervisor can attend a session at other Trusts; subject to local study leave procedures. It should be evident that where there are concerns about a trainee’s performance in training, or achievement of competencies, there should be more frequent reviews of progress than the ‘minimum’ set out by the medical royal colleges. Clinical or educational supervisors may need assistance from College Tutors, Training Programme Directors or School Board officers. If in any doubt it is prudent to seek early confidential advice. The Career Development Unit (CDU) of the Deanery can provide educators with advice about the appropriate steps to take in managing concerns about trainee performance, as well as personal coaching and mentoring support for individual trainees. Further information is available from the CDU website at www.oxforddeanerycdu.org.uk/index.html. Issues that are related to patient safety should be discussed with the Director of Medical Education and / or the Medical Director of your own Trust. Equality and diversity It is important for clinical supervisors, educational supervisors, College tutors, Training Programme Directors and School Board officers to treat all
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 22
trainees equally and without discrimination. This is of particular importance when the trainee’s problems begin to impact on their performance, as less than equal treatment might be alleged through either Deanery appeals panels or even Employment Tribunals. The same standards of communication and support to all trainees should be applied from the outset. I recommend an electronic file for every trainee with whom you have any dealings, password protected of course, and any paper material should be kept securely under lock and key. The Oxford Deanery policy can be viewed on the website. Harassment People can become upset by something done (or not done), or said, to them. Most perceived "offences" or slights are simple miscommunication; an apology and explanation is all that is necessary to restore team harmony. Trainees may report such worries to you. The PGMDE does not condone these behaviours either from trainees towards colleagues, nor from trainers and other health care staff towards trainees or peers. Harassment can take various forms and may be directed against males or females, ethnic minorities or subgroups, towards people because of their age, sexual orientation, physical or mental disability, or some other characteristic. It may involve action, behaviour, comment or physical contact which is found to be objectionable by the recipient or which causes offence and can result in the recipient feeling threatened, humiliated, patronised or isolated. It can also create an intimidating work environment. Individual perceptions about certain types of behaviour will vary, so what is acceptable for one person, may be inappropriate or unacceptable behaviour to another. Harassment may be persistent or occur on a single occasion. It may be intentional or unintentional on the part of the perpetrator, but it is the impact of the behaviour on the recipient, and the deed itself, which constitutes harassment. Concerns about health If there are any concerns about an individual’s health affecting training, the doctor should be encouraged to see their own GP. If there is a possibility that a doctor’s health may be affecting their work, then the employer may ask for an occupational health assessment. Further information and guidance is available from the CDU website at http://www.oxforddeanerycdu.org.uk/health/guidance_for_trainers/index.html, and from NCAS at http://www.ncas.nhs.uk/resources/handling-health-concerns/
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 23
Dyslexia in relation to Postgraduate Medical and Dental Education and Training Dyslexia is one of a group of conditions called Specific Learning Difficulties in Adults, which also includes Dyspraxia or Development Co-ordination Disorder, Dyscalculia, and Attention Deficit Disorder. Further information about these is available on the British Dyslexia Association website – see http://www.bdadyslexia.org.uk/about-dyslexia/adults-and-business/dyslexia-and-specific-learning-difficulties-in-adu.html. Hereafter in these notes the term “dyslexia” will be used to refer to all the Specific Learning Difficulties in Adults. Specific information about dealing with dyslexia in postgraduate medical and dental education and training is hard to find. There is useful information on the BMA website produced by the BMA Medical Students Committee – see http://bma.org.uk/developing-your-career/studying-medicine/common-challenges-while-studying/studying-with-dyslexia but this does not refer to what happens after qualification. The GMC website includes references to dyslexia under its Gateways guidance – see http://www.gmc-uk.org/education/undergraduate/gateways_guidance.asp for general information about this guidance. In summary: GMC Gateways guidance This advisory guidance is aimed primarily at medical schools. It
will also interest organisations involved in postgraduate medical training and many individuals, including disabled doctors, students and potential students.
It provides practical suggestions to help schools ensure that disabled students do not face unnecessary barriers to successful medical careers.
The advisory guidance originally resulted from a partnership led by the GMC and financially supported by 11 medical schools. Matched funding was provided through Gateways to the Professions, set up by the Department for Education and Skills (England), as it then was. The guidance has been to revised to take account of developments including the 2009 edition of Tomorrow’s Doctors and the Equality Act 2010.
The guidance does not lay down new requirements, quality assurance standards or ‘policies’ from the GMC or any of the other organisations involved.
Section 4.2 of the guidance covers the legal definition of ‘a disabled person’ (copied from GMC guidance – the emphasis is added):
The Equality Act 2010 defines a disabled person as: ‘A person (P) has a disability if P has a physical or mental impairment which has a long-term and substantial adverse effect on P’s ability to carry out normal day-to-
day activities.’
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 24
As this is a legal definition, it is ultimately for a court or tribunal to determine to whom it applies. Where there is doubt about whether an individual will be covered, it is best practice to assume that they will be and focus on identifying reasonable adjustments that will assist them.
The effect of an impairment is long-term if: It has lasted for at least 12 months It is likely to last for at least 12 months or It is likely to last for the rest of the life of the person affected. A ‘substantial’ adverse effect is defined in the Act as one that is
‘more than minor or trivial’. Medical schools, postgraduate deaneries and employers
should use this definition when considering how to assess and support disabled applicants, students and employees. They should also encourage a greater understanding of who is protected by the Act, and seek to protect the rights of disabled people in their use of all the services at university and medical school.
People with a range of impairments and long-term health conditions are included in this definition, such as people who are hard of hearing or have mental health issues, multiple sclerosis, cancer or HIV. Importantly, others who would not usually describe themselves as disabled people, such as those with dyslexia, may be protected by the Act if the effects of the impairment are 'long term' 'adverse' and 'substantial' on normal day-to-day activities. People with hidden disabilities such as epilepsy are also covered.
It is not clear from the above to what extent The Equality Act 2010 places any obligation on Postgraduate Deaneries in relation to doctors and dentists in training that have diagnosed or suspected dyslexia. There are certainly obligations under the Act for the employers of doctors and dentists in training.
There is most useful and comprehensive guidance for employers on the British Dyslexia Association website (see http://www.bdadyslexia.org.uk/about-dyslexia/adults-and-business.html). For example, there is:
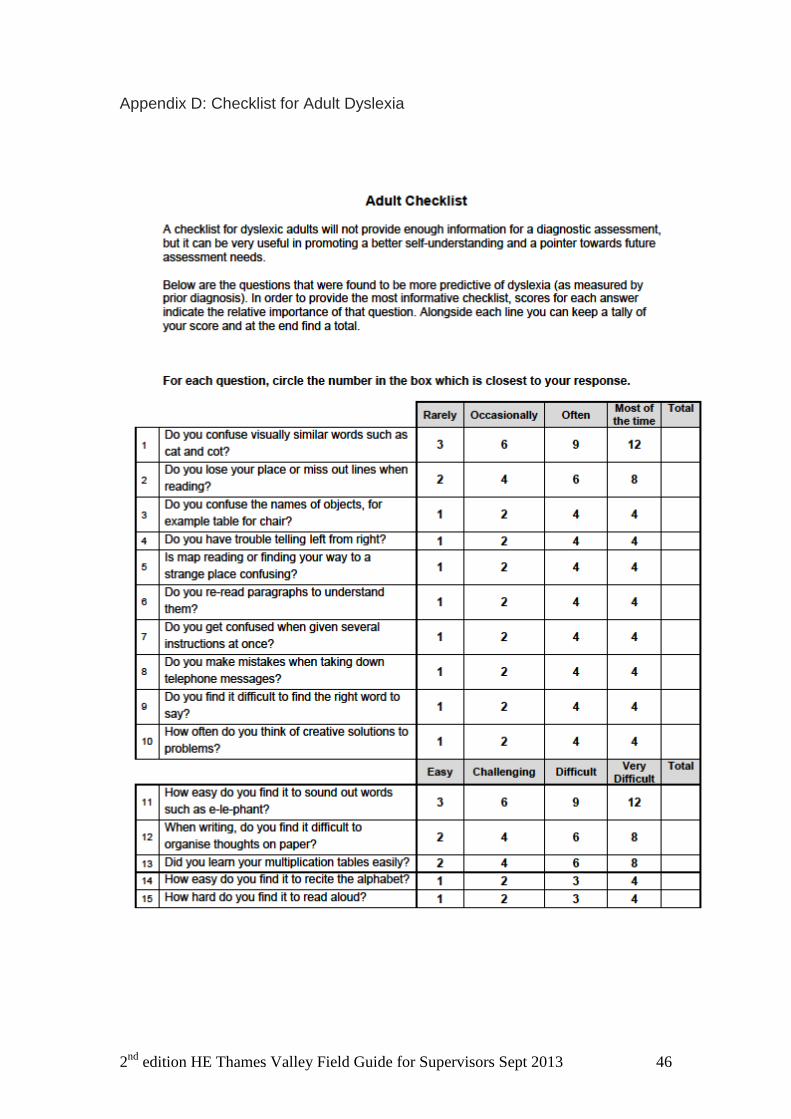
An Adult Dyslexia Checklist which can be used as a screening tool for adult dyslexia – see http://www.bdadyslexia.org.uk/files/Adult%20Checklist.pdf This test is said to be 90% accurate in predicting dyslexia.
Some relevant text copied from the BDA guidance follows:
o There is no legal requirement to disclose a disability. However
once the employer has been informed of an employee’s dyslexia
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 25
or been given a copy of an assessment report, they are on notice that they have a duty under the Equality Act.
o Disciplinary proceedings around performance issues are frequently dyslexia related. Many are off sick with stress as a result. In many circumstances they could seek redress under the Equality Act in an Employment Tribunal.
o Assessment. Where an employee has not been previously assessed for dyslexic difficulties (post 16 years), the first step would be for the employer to arrange for the employee to have a full diagnostic assessment:
This should by carried out by a Chartered Psychologist specialising in adult dyslexia. The cost could be around £500 or more.
However in the case of a job not involving significant paperwork, a screening test such as the one linked to our website may be sufficient. This test is 90% accurate in predicting dyslexia.
Most large employers and those in the public sector would be expected to fund a dyslexia assessment for an employee as part of their duty under the Equality Act. A small employer may help with the cost. For recommendations of appropriate psychologists for a diagnostic assessment, contact your nearest Local Dyslexia Association.
Workplace Need Assessment for doctors with dyslexia
Following the diagnostic assessment, (or where an employee is able to show an existing adult assessment report), a workplace needs assessment should be arranged with a dyslexia specialist. This will detail the most appropriate accommodations and support, (reasonable adjustments) that would be successful in mitigating any weak areas and reduce stress. This is not something that either the individual or the employer would be able to work out for themselves.
Workplace needs assessments can normally be obtained from Access to Work, part of the Jobcentre organisation.
The application to Access to Work should be made by the employee. For information on this process see Dyslexia Support in the Workplace.
Independent dyslexia workplace consultants can also be appointed to do an assessment. Their report can still be submitted to Access to Work for the grant to the individual for items and training recommended.

2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 26
Implementing Reasonable Adjustments.
Reasonable Adjustments should be put in place as soon as possible. Failure to implement Reasonable Adjustments would be a breach of the Equality Act. Reasonable Adjustments are not a quick overnight remedy. Depending on the individual circumstances, it may take 2 or 3 months for measures to become embedded and for any associated training and learning to become effective.
External sources of support for trainees There are a number of well-regarded external sources of support, and it is strongly recommended that supervisors direct trainees to them and do not try to act as, for example, marriage guidance counsellors, or ‘doctors’ to their trainees. The agencies which may be suitable include: Medic Support Funded by the Oxford Deanery to provide a free
and confidential counselling service for doctors and dentists in training. See http://www.oxforddeanerycdu.org.uk/health/help_for_trainees/medic_support.html
The CDU See the CDU website for more information at
http://www.oxforddeanerycdu.org.uk/index.html
‘Doctors for Doctors’ A BMA service for medical students and qualified
doctors. Contact on 08459 200169
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 27
Appendix A: Forms usually collated by the Educational Supervisor and ARCP outcomes These are described in detail in ‘The Gold Guide’. Increasingly these forms are lodged in the specialty eportfolio. Both trainee and Educational Supervisor normally have access to the same site: other assessors may be invited by the trainee sending an ‘e ticket’ to log-in. The Educational Agreement (EA) It should be signed by both the trainee and their Educational Supervisor at the start of each year of training. The form looks like this:
The Trainee’s Personal Development Plan (PDP) This should be written by the trainee at the start of the training year, and reviewed after each assessment, as a minimum (due at 4, 8 and 11+ months)
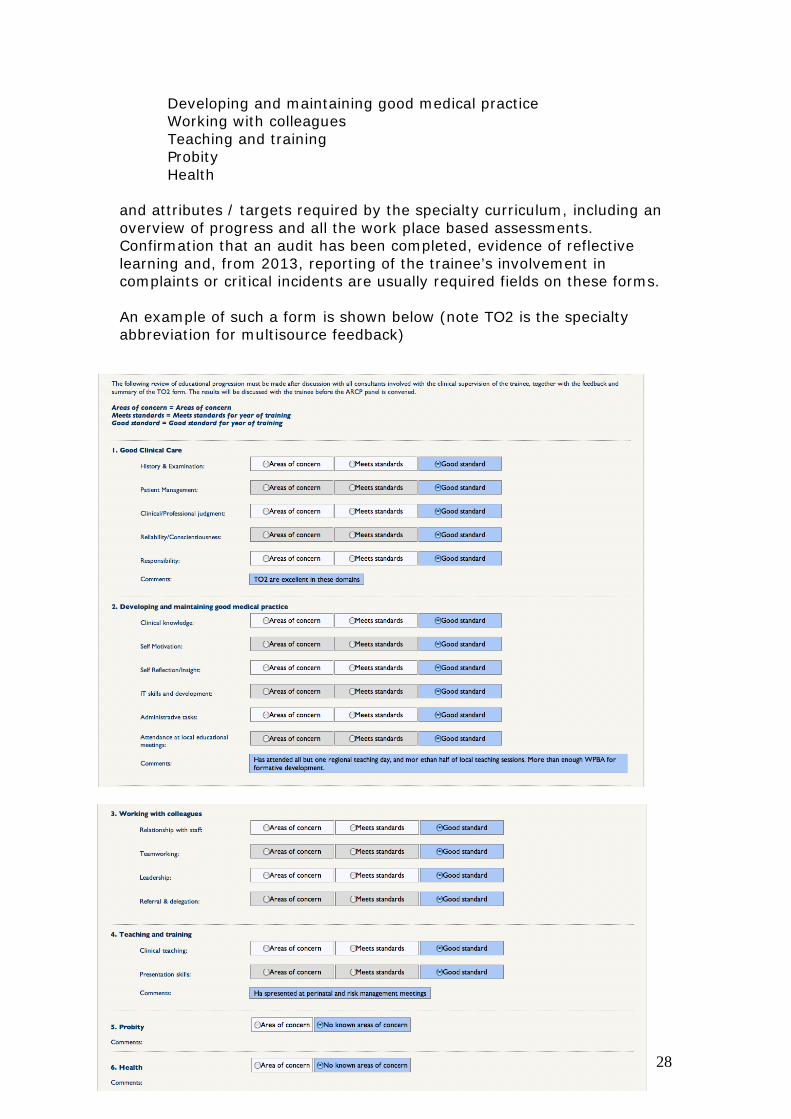
The Annual Assessment Review Form (AARF) This document forms the summative assessment of a trainee’s progress during the preceding year and is an integral part of the evidence required for the ARCP panel review. It will include the domains laid out by the GMC: Good clinical care
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 28
Developing and maintaining good medical practice Working with colleagues Teaching and training
Probity Health
and attributes / targets required by the specialty curriculum, including an overview of progress and all the work place based assessments. Confirmation that an audit has been completed, evidence of reflective learning and, from 2013, reporting of the trainee’s involvement in complaints or critical incidents are usually required fields on these forms. An example of such a form is shown below (note TO2 is the specialty abbreviation for multisource feedback)
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 29
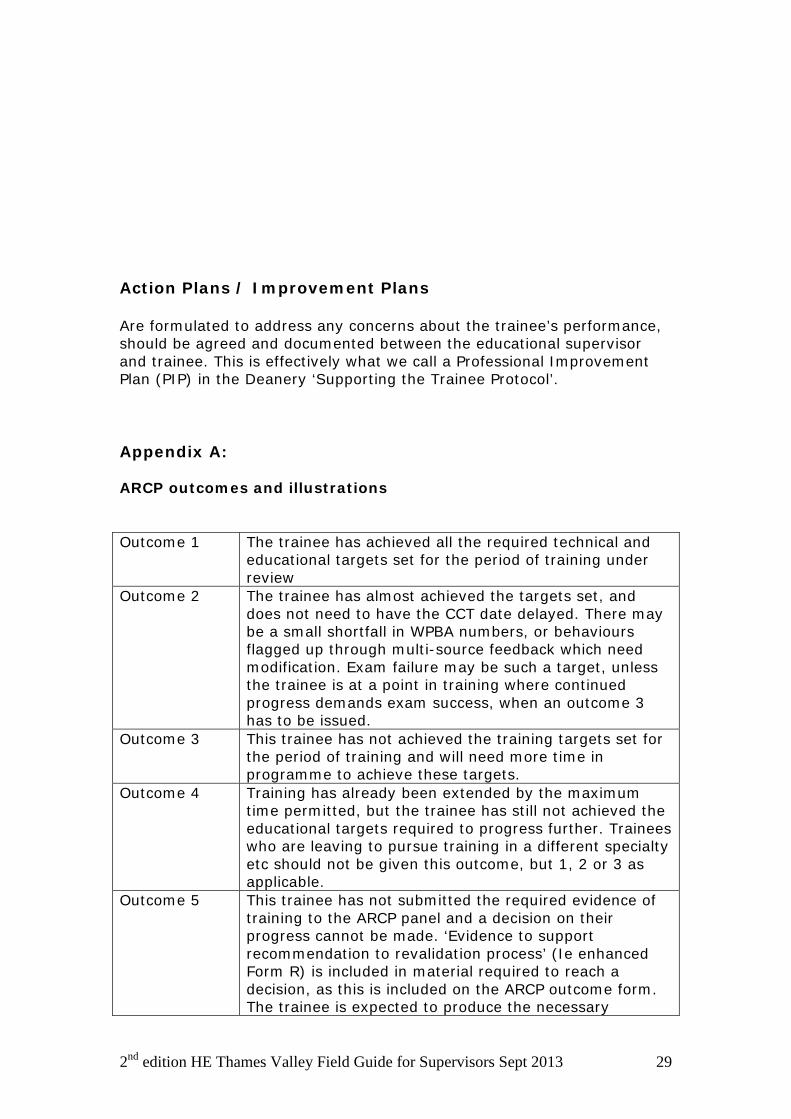
Action Plans / Improvement Plans Are formulated to address any concerns about the trainee’s performance, should be agreed and documented between the educational supervisor and trainee. This is effectively what we call a Professional Improvement Plan (PIP) in the Deanery ‘Supporting the Trainee Protocol’. Appendix A: ARCP outcomes and illustrations Outcome 1 The trainee has achieved all the required technical and
educational targets set for the period of training under review
Outcome 2 The trainee has almost achieved the targets set, and does not need to have the CCT date delayed. There may be a small shortfall in WPBA numbers, or behaviours flagged up through multi-source feedback which need modification. Exam failure may be such a target, unless the trainee is at a point in training where continued progress demands exam success, when an outcome 3 has to be issued.
Outcome 3 This trainee has not achieved the training targets set for the period of training and will need more time in programme to achieve these targets.
Outcome 4 Training has already been extended by the maximum time permitted, but the trainee has still not achieved the educational targets required to progress further. Trainees who are leaving to pursue training in a different specialty etc should not be given this outcome, but 1, 2 or 3 as applicable.
Outcome 5 This trainee has not submitted the required evidence of training to the ARCP panel and a decision on their progress cannot be made. ‘Evidence to support recommendation to revalidation process’ (Ie enhanced Form R) is included in material required to reach a decision, as this is included on the ARCP outcome form. The trainee is expected to produce the necessary
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 30
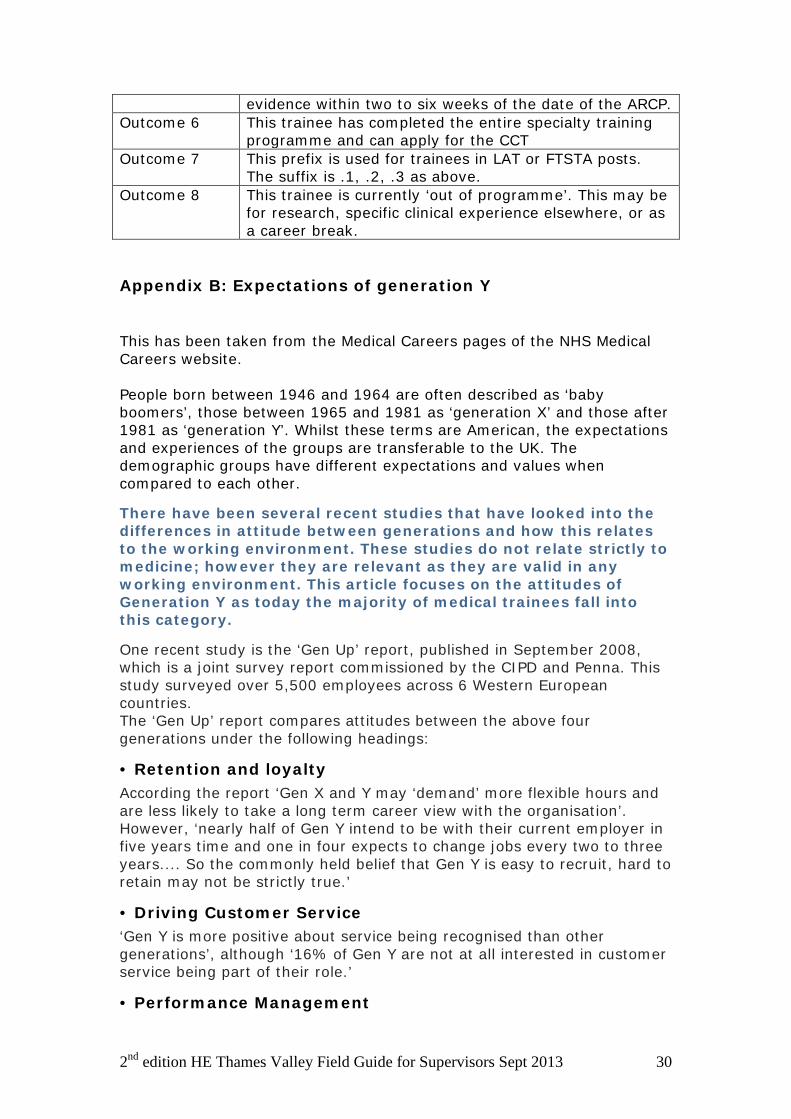
evidence within two to six weeks of the date of the ARCP. Outcome 6 This trainee has completed the entire specialty training
programme and can apply for the CCT Outcome 7 This prefix is used for trainees in LAT or FTSTA posts.
The suffix is .1, .2, .3 as above. Outcome 8 This trainee is currently ‘out of programme’. This may be
for research, specific clinical experience elsewhere, or as a career break.
Appendix B: Expectations of generation Y This has been taken from the Medical Careers pages of the NHS Medical Careers website. People born between 1946 and 1964 are often described as ‘baby boomers’, those between 1965 and 1981 as ‘generation X’ and those after 1981 as ‘generation Y’. Whilst these terms are American, the expectations and experiences of the groups are transferable to the UK. The demographic groups have different expectations and values when compared to each other.
There have been several recent studies that have looked into the differences in attitude between generations and how this relates to the working environment. These studies do not relate strictly to medicine; however they are relevant as they are valid in any working environment. This article focuses on the attitudes of Generation Y as today the majority of medical trainees fall into this category.
One recent study is the ‘Gen Up’ report, published in September 2008, which is a joint survey report commissioned by the CIPD and Penna. This study surveyed over 5,500 employees across 6 Western European countries. The ‘Gen Up’ report compares attitudes between the above four generations under the following headings:
• Retention and loyalty According the report ‘Gen X and Y may ‘demand’ more flexible hours and are less likely to take a long term career view with the organisation’. However, ‘nearly half of Gen Y intend to be with their current employer in five years time and one in four expects to change jobs every two to three years.... So the commonly held belief that Gen Y is easy to recruit, hard to retain may not be strictly true.’
• Driving Customer Service ‘Gen Y is more positive about service being recognised than other generations’, although ‘16% of Gen Y are not at all interested in customer service being part of their role.’
• Performance Management
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 31
‘Gen Y is much less tolerant of under-performance. Nearly one in five Gen Ys believe that the best solution for under-performance is for someone to be fired’.
• Mobile and Flexible Working ‘As a generation, Gen Y are the first to truly adopt technology to manage their life/work balance as the boundaries of office and personal life become blurred.’
• Internal communication ‘Gen Y is actually the most positive generation about communication. They may be expected to be more demanding of internal communication given the fact that they are used to ‘information at their fingertips’.
• Leadership and Management ‘Gen Y may find that older generations demonstrate less trust for senior management. Gen Y are also more likely to rate senior mangers well including the fact that they make work priorities clear.’ The report also finds that ‘Gen Y are the most trusting of the organisation as they have not been exposed to significant downsizing or economic uncertainty.’ This characteristic may now be subject to change, however, with the effects of the current recession.
• Career development ‘Gen Y may find some generational conflict in terms of career development’.
’Gen Y may find development conversations with other Gen Y much easier to manage – conversations are likely to stretch beyond the current organisation’. The Baby Boomer may be surprised at the ‘self- sufficiency’ of Gen Y as they expect to manage their own career development’.
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 32
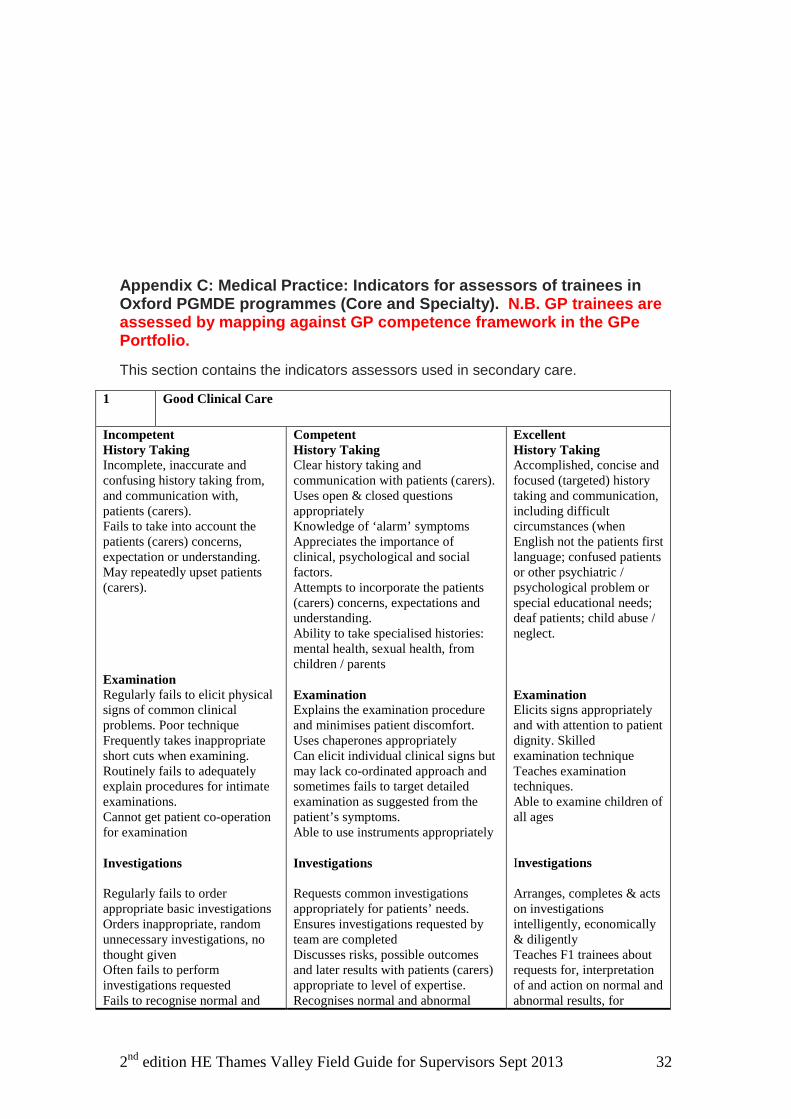
Appendix C: Medical Practice: Indicators for assessors of trainees in Oxford PGMDE programmes (Core and Specialty). N.B. GP trainees are assessed by mapping against GP competence framework in the GPe Portfolio.
This section contains the indicators assessors used in secondary care.
1 Good Clinical Care
Incompetent History Taking Incomplete, inaccurate and confusing history taking from, and communication with, patients (carers). Fails to take into account the patients (carers) concerns, expectation or understanding. May repeatedly upset patients (carers). Examination Regularly fails to elicit physical signs of common clinical problems. Poor technique Frequently takes inappropriate short cuts when examining. Routinely fails to adequately explain procedures for intimate examinations. Cannot get patient co-operation for examination Investigations Regularly fails to order appropriate basic investigations Orders inappropriate, random unnecessary investigations, no thought given Often fails to perform investigations requested Fails to recognise normal and
Competent History Taking Clear history taking and communication with patients (carers). Uses open & closed questions appropriately Knowledge of ‘alarm’ symptoms Appreciates the importance of clinical, psychological and social factors. Attempts to incorporate the patients (carers) concerns, expectations and understanding. Ability to take specialised histories: mental health, sexual health, from children / parents Examination Explains the examination procedure and minimises patient discomfort. Uses chaperones appropriately Can elicit individual clinical signs but may lack co-ordinated approach and sometimes fails to target detailed examination as suggested from the patient’s symptoms. Able to use instruments appropriately Investigations Requests common investigations appropriately for patients’ needs. Ensures investigations requested by team are completed Discusses risks, possible outcomes and later results with patients (carers) appropriate to level of expertise. Recognises normal and abnormal
Excellent History Taking Accomplished, concise and focused (targeted) history taking and communication, including difficult circumstances (when English not the patients first language; confused patients or other psychiatric / psychological problem or special educational needs; deaf patients; child abuse / neglect. Examination Elicits signs appropriately and with attention to patient dignity. Skilled examination technique Teaches examination techniques. Able to examine children of all ages Investigations Arranges, completes & acts on investigations intelligently, economically & diligently Teaches F1 trainees about requests for, interpretation of and action on normal and abnormal results, for
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 33
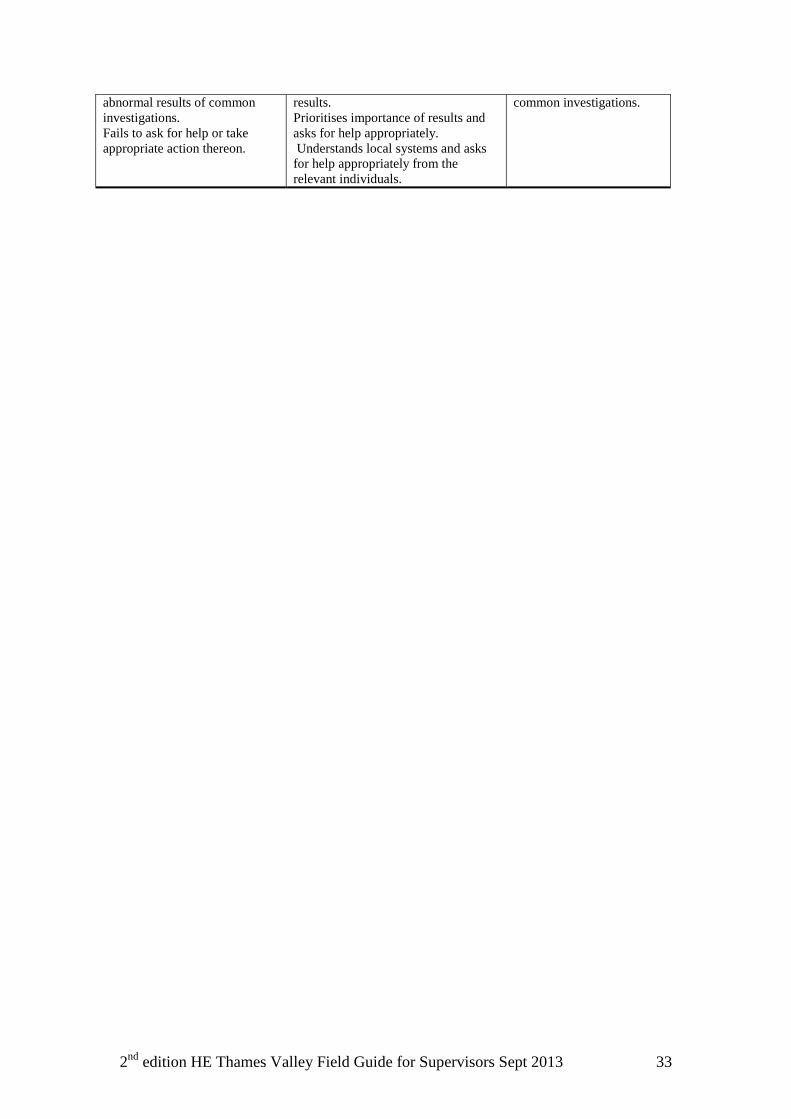
abnormal results of common investigations. Fails to ask for help or take appropriate action thereon.
results. Prioritises importance of results and asks for help appropriately. Understands local systems and asks for help appropriately from the relevant individuals.
common investigations.
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 34
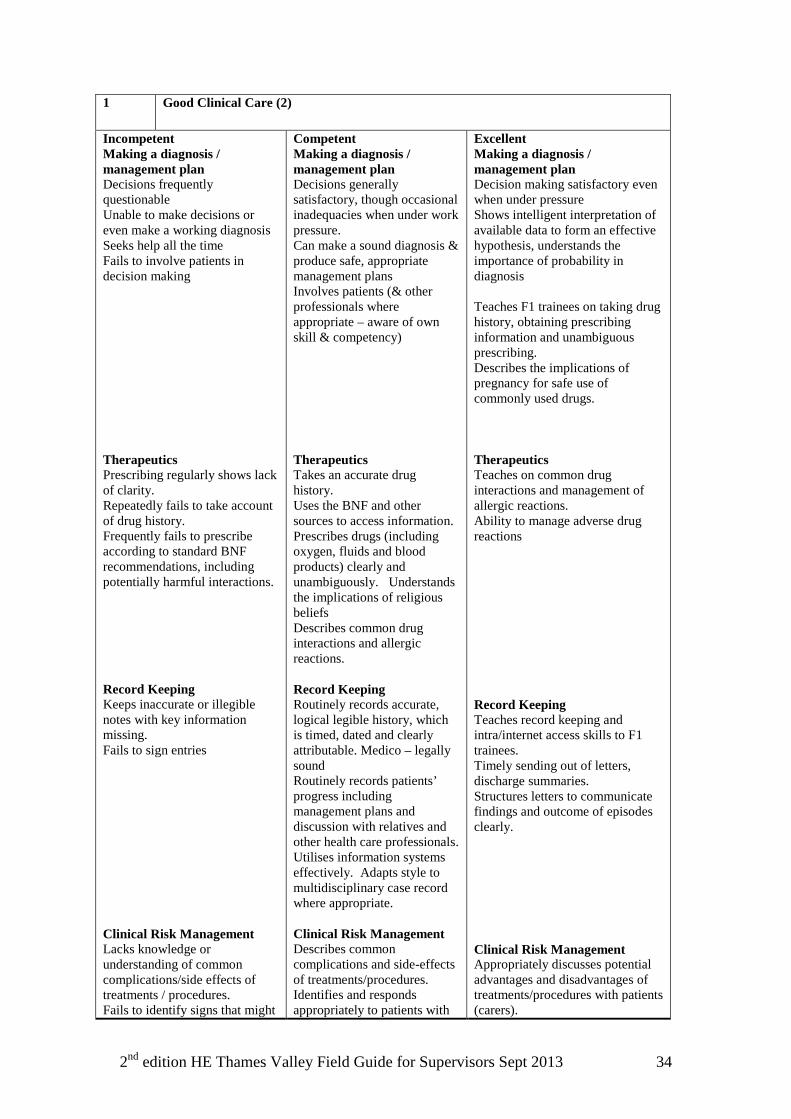
1 Good Clinical Care (2)
Incompetent Making a diagnosis / management plan Decisions frequently questionable Unable to make decisions or even make a working diagnosis Seeks help all the time Fails to involve patients in decision making Therapeutics Prescribing regularly shows lack of clarity. Repeatedly fails to take account of drug history. Frequently fails to prescribe according to standard BNF recommendations, including potentially harmful interactions. Record Keeping Keeps inaccurate or illegible notes with key information missing. Fails to sign entries Clinical Risk Management Lacks knowledge or understanding of common complications/side effects of treatments / procedures. Fails to identify signs that might
Competent Making a diagnosis / management plan Decisions generally satisfactory, though occasional inadequacies when under work pressure. Can make a sound diagnosis & produce safe, appropriate management plans Involves patients (& other professionals where appropriate – aware of own skill & competency) Therapeutics Takes an accurate drug history. Uses the BNF and other sources to access information. Prescribes drugs (including oxygen, fluids and blood products) clearly and unambiguously. Understands the implications of religious beliefs Describes common drug interactions and allergic reactions. Record Keeping Routinely records accurate, logical legible history, which is timed, dated and clearly attributable. Medico – legally sound Routinely records patients’ progress including management plans and discussion with relatives and other health care professionals. Utilises information systems effectively. Adapts style to multidisciplinary case record where appropriate. Clinical Risk Management Describes common complications and side-effects of treatments/procedures. Identifies and responds appropriately to patients with
Excellent Making a diagnosis / management plan Decision making satisfactory even when under pressure Shows intelligent interpretation of available data to form an effective hypothesis, understands the importance of probability in diagnosis Teaches F1 trainees on taking drug history, obtaining prescribing information and unambiguous prescribing. Describes the implications of pregnancy for safe use of commonly used drugs. Therapeutics Teaches on common drug interactions and management of allergic reactions. Ability to manage adverse drug reactions Record Keeping Teaches record keeping and intra/internet access skills to F1 trainees. Timely sending out of letters, discharge summaries. Structures letters to communicate findings and outcome of episodes clearly. Clinical Risk Management Appropriately discusses potential advantages and disadvantages of treatments/procedures with patients (carers).
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 35
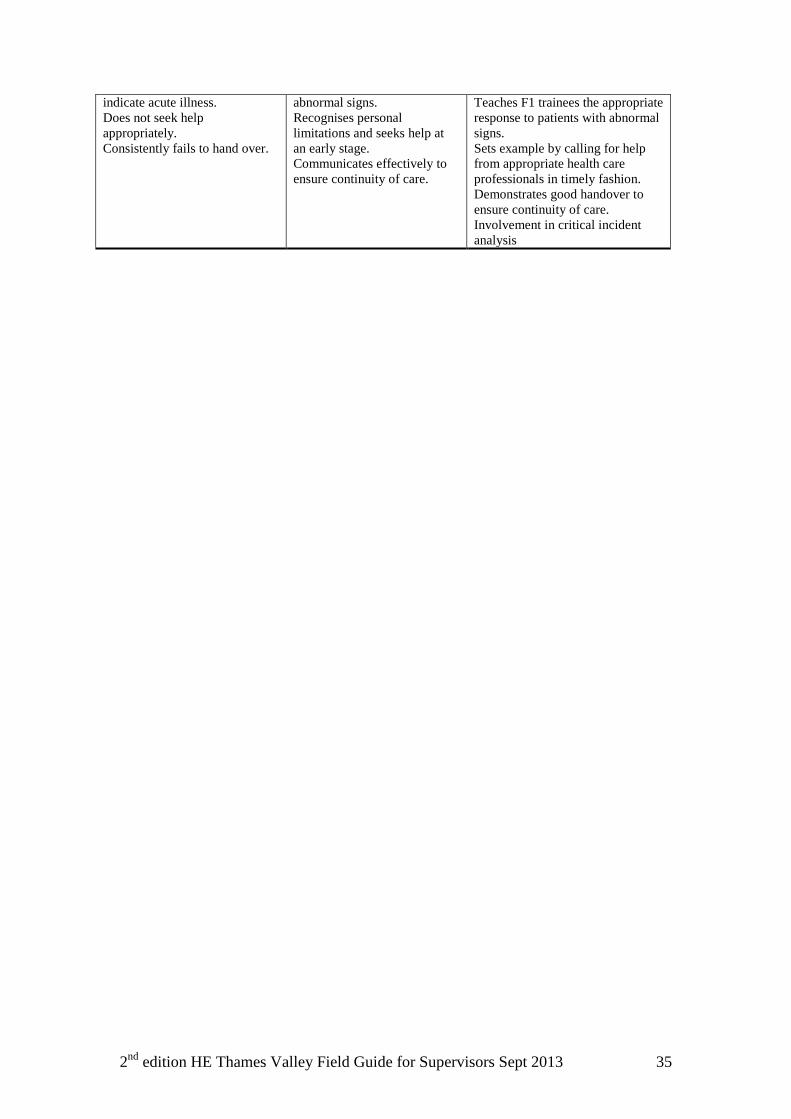
indicate acute illness. Does not seek help appropriately. Consistently fails to hand over.
abnormal signs. Recognises personal limitations and seeks help at an early stage. Communicates effectively to ensure continuity of care.
Teaches F1 trainees the appropriate response to patients with abnormal signs. Sets example by calling for help from appropriate health care professionals in timely fashion. Demonstrates good handover to ensure continuity of care. Involvement in critical incident analysis
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 36
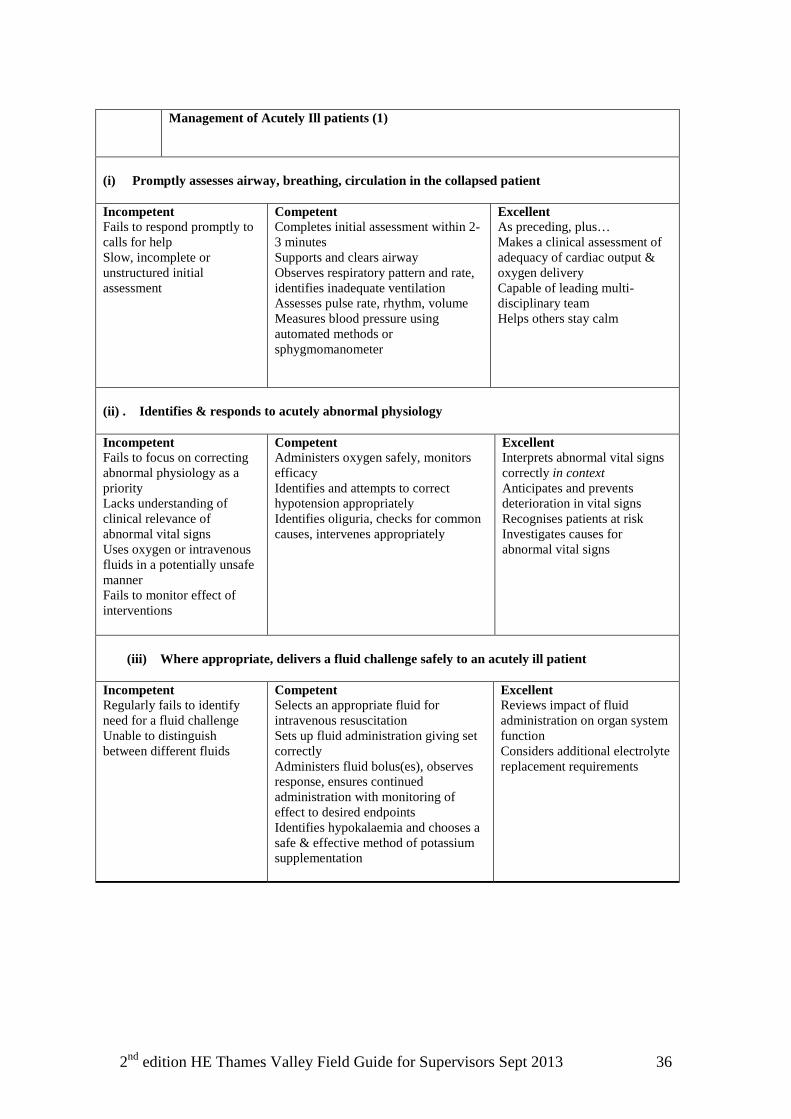
Management of Acutely Ill patients (1)
(i) Promptly assesses airway, breathing, circulation in the collapsed patient Incompetent Fails to respond promptly to calls for help Slow, incomplete or unstructured initial assessment
Competent Completes initial assessment within 2-3 minutes Supports and clears airway Observes respiratory pattern and rate, identifies inadequate ventilation Assesses pulse rate, rhythm, volume Measures blood pressure using automated methods or sphygmomanometer
Excellent As preceding, plus… Makes a clinical assessment of adequacy of cardiac output & oxygen delivery Capable of leading multi-disciplinary team Helps others stay calm
(ii) . Identifies & responds to acutely abnormal physiology Incompetent Fails to focus on correcting abnormal physiology as a priority Lacks understanding of clinical relevance of abnormal vital signs Uses oxygen or intravenous fluids in a potentially unsafe manner Fails to monitor effect of interventions
Competent Administers oxygen safely, monitors efficacy Identifies and attempts to correct hypotension appropriately Identifies oliguria, checks for common causes, intervenes appropriately
Excellent Interprets abnormal vital signs correctly in context Anticipates and prevents deterioration in vital signs Recognises patients at risk Investigates causes for abnormal vital signs
(iii) Where appropriate, delivers a fluid challenge safely to an acutely ill patient
Incompetent Regularly fails to identify need for a fluid challenge Unable to distinguish between different fluids
Competent Selects an appropriate fluid for intravenous resuscitation Sets up fluid administration giving set correctly Administers fluid bolus(es), observes response, ensures continued administration with monitoring of effect to desired endpoints Identifies hypokalaemia and chooses a safe & effective method of potassium supplementation
Excellent Reviews impact of fluid administration on organ system function Considers additional electrolyte replacement requirements
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 37
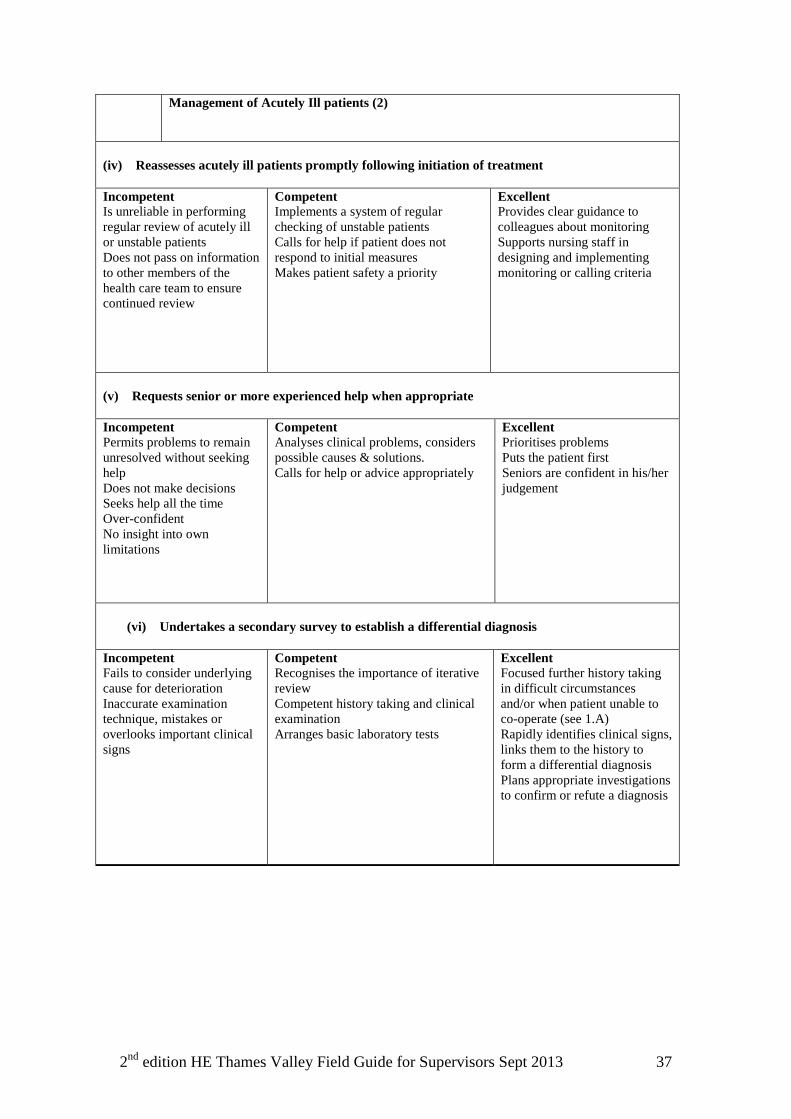
Management of Acutely Ill patients (2)
(iv) Reassesses acutely ill patients promptly following initiation of treatment Incompetent Is unreliable in performing regular review of acutely ill or unstable patients Does not pass on information to other members of the health care team to ensure continued review
Competent Implements a system of regular checking of unstable patients Calls for help if patient does not respond to initial measures Makes patient safety a priority
Excellent Provides clear guidance to colleagues about monitoring Supports nursing staff in designing and implementing monitoring or calling criteria
(v) Requests senior or more experienced help when appropriate Incompetent Permits problems to remain unresolved without seeking help Does not make decisions Seeks help all the time Over-confident No insight into own limitations
Competent Analyses clinical problems, considers possible causes & solutions. Calls for help or advice appropriately
Excellent Prioritises problems Puts the patient first Seniors are confident in his/her judgement
(vi) Undertakes a secondary survey to establish a differential diagnosis
Incompetent Fails to consider underlying cause for deterioration Inaccurate examination technique, mistakes or overlooks important clinical signs
Competent Recognises the importance of iterative review Competent history taking and clinical examination Arranges basic laboratory tests
Excellent Focused further history taking in difficult circumstances and/or when patient unable to co-operate (see 1.A) Rapidly identifies clinical signs, links them to the history to form a differential diagnosis Plans appropriate investigations to confirm or refute a diagnosis
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 38
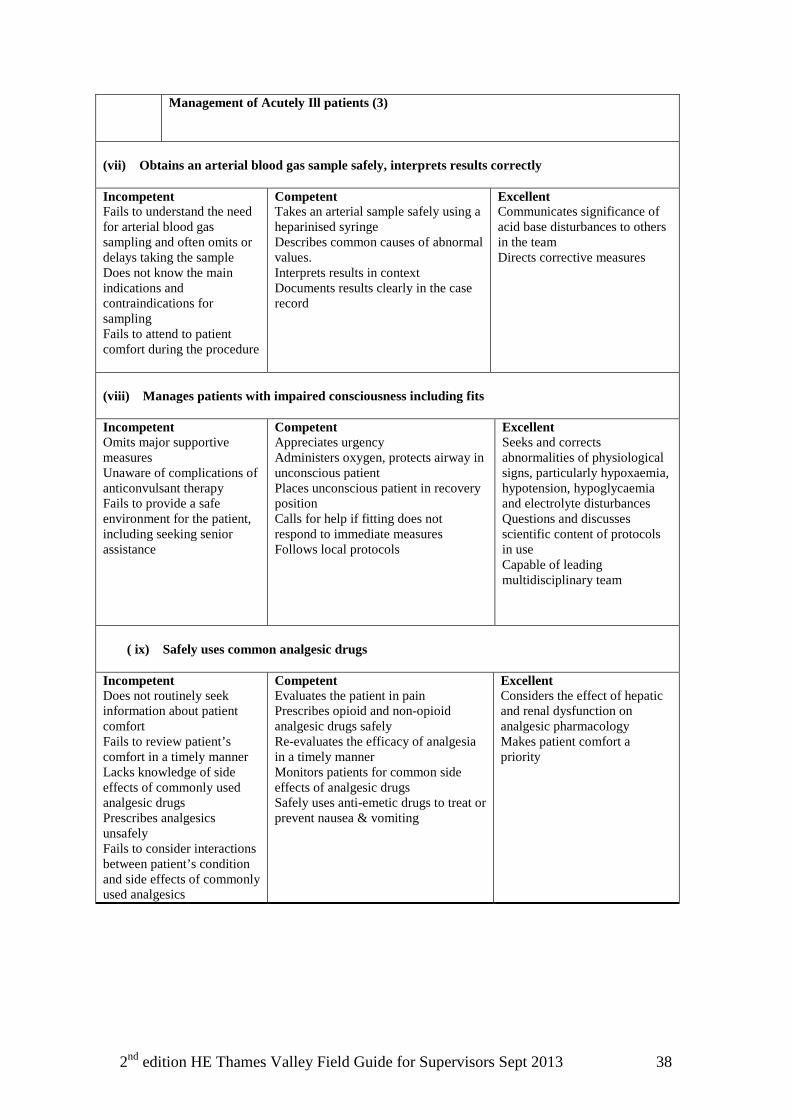
Management of Acutely Ill patients (3)
(vii) Obtains an arterial blood gas sample safely, interprets results correctly Incompetent Fails to understand the need for arterial blood gas sampling and often omits or delays taking the sample Does not know the main indications and contraindications for sampling Fails to attend to patient comfort during the procedure
Competent Takes an arterial sample safely using a heparinised syringe Describes common causes of abnormal values. Interprets results in context Documents results clearly in the case record
Excellent Communicates significance of acid base disturbances to others in the team Directs corrective measures
(viii) Manages patients with impaired consciousness including fits Incompetent Omits major supportive measures Unaware of complications of anticonvulsant therapy Fails to provide a safe environment for the patient, including seeking senior assistance
Competent Appreciates urgency Administers oxygen, protects airway in unconscious patient Places unconscious patient in recovery position Calls for help if fitting does not respond to immediate measures Follows local protocols
Excellent Seeks and corrects abnormalities of physiological signs, particularly hypoxaemia, hypotension, hypoglycaemia and electrolyte disturbances Questions and discusses scientific content of protocols in use Capable of leading multidisciplinary team
( ix) Safely uses common analgesic drugs
Incompetent Does not routinely seek information about patient comfort Fails to review patient’s comfort in a timely manner Lacks knowledge of side effects of commonly used analgesic drugs Prescribes analgesics unsafely Fails to consider interactions between patient’s condition and side effects of commonly used analgesics
Competent Evaluates the patient in pain Prescribes opioid and non-opioid analgesic drugs safely Re-evaluates the efficacy of analgesia in a timely manner Monitors patients for common side effects of analgesic drugs Safely uses anti-emetic drugs to treat or prevent nausea & vomiting
Excellent Considers the effect of hepatic and renal dysfunction on analgesic pharmacology Makes patient comfort a priority
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 39
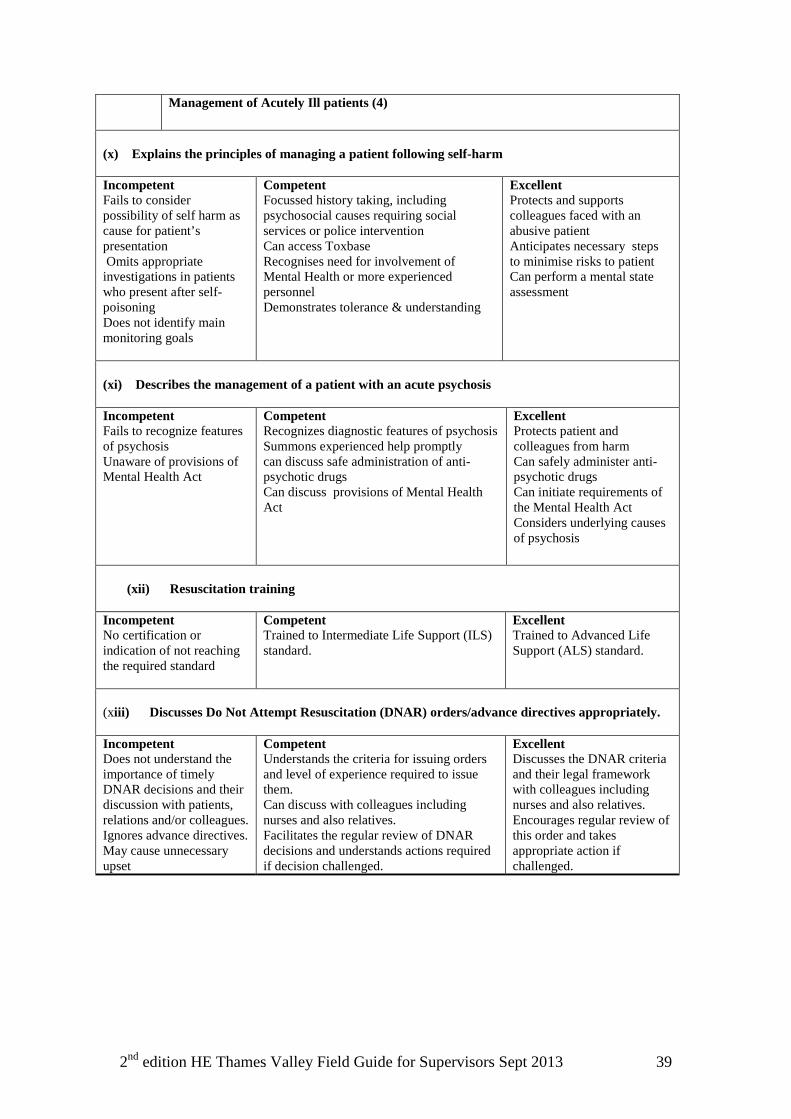
Management of Acutely Ill patients (4)
(x) Explains the principles of managing a patient following self-harm Incompetent Fails to consider possibility of self harm as cause for patient’s presentation Omits appropriate investigations in patients who present after self-poisoning Does not identify main monitoring goals
Competent Focussed history taking, including psychosocial causes requiring social services or police intervention Can access Toxbase Recognises need for involvement of Mental Health or more experienced personnel Demonstrates tolerance & understanding
Excellent Protects and supports colleagues faced with an abusive patient Anticipates necessary steps to minimise risks to patient Can perform a mental state assessment
(xi) Describes the management of a patient with an acute psychosis Incompetent Fails to recognize features of psychosis Unaware of provisions of Mental Health Act
Competent Recognizes diagnostic features of psychosis Summons experienced help promptly can discuss safe administration of anti-psychotic drugs Can discuss provisions of Mental Health Act
Excellent Protects patient and colleagues from harm Can safely administer anti-psychotic drugs Can initiate requirements of the Mental Health Act Considers underlying causes of psychosis
(xii) Resuscitation training
Incompetent No certification or indication of not reaching the required standard
Competent Trained to Intermediate Life Support (ILS) standard.
Excellent Trained to Advanced Life Support (ALS) standard.
(xiii) Discusses Do Not Attempt Resuscitation (DNAR) orders/advance directives appropriately. Incompetent Does not understand the importance of timely DNAR decisions and their discussion with patients, relations and/or colleagues. Ignores advance directives. May cause unnecessary upset
Competent Understands the criteria for issuing orders and level of experience required to issue them. Can discuss with colleagues including nurses and also relatives. Facilitates the regular review of DNAR decisions and understands actions required if decision challenged.
Excellent Discusses the DNAR criteria and their legal framework with colleagues including nurses and also relatives. Encourages regular review of this order and takes appropriate action if challenged.
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 40
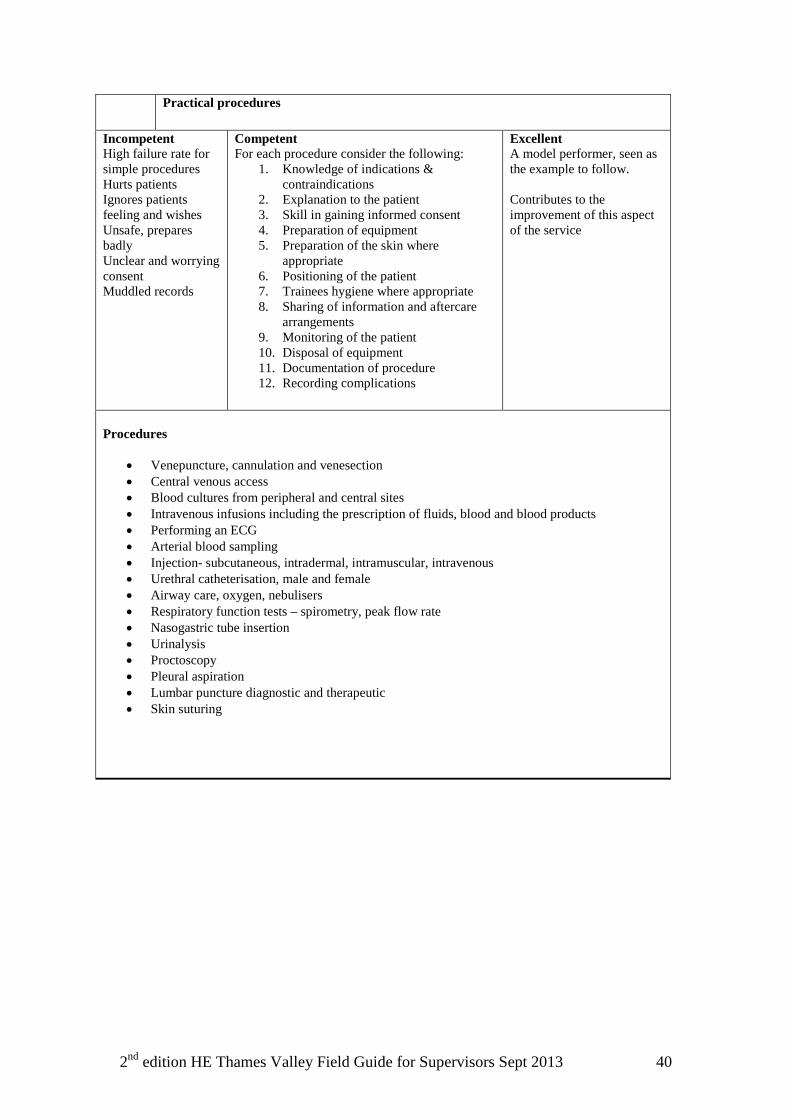
Practical procedures
Incompetent High failure rate for simple procedures Hurts patients Ignores patients feeling and wishes Unsafe, prepares badly Unclear and worrying consent Muddled records
Competent For each procedure consider the following:
1. Knowledge of indications & contraindications
2. Explanation to the patient 3. Skill in gaining informed consent 4. Preparation of equipment 5. Preparation of the skin where
appropriate 6. Positioning of the patient 7. Trainees hygiene where appropriate 8. Sharing of information and aftercare
arrangements 9. Monitoring of the patient 10. Disposal of equipment 11. Documentation of procedure 12. Recording complications
Excellent A model performer, seen as the example to follow. Contributes to the improvement of this aspect of the service
Procedures
• Venepuncture, cannulation and venesection • Central venous access • Blood cultures from peripheral and central sites • Intravenous infusions including the prescription of fluids, blood and blood products • Performing an ECG • Arterial blood sampling • Injection- subcutaneous, intradermal, intramuscular, intravenous • Urethral catheterisation, male and female • Airway care, oxygen, nebulisers • Respiratory function tests – spirometry, peak flow rate • Nasogastric tube insertion • Urinalysis • Proctoscopy • Pleural aspiration • Lumbar puncture diagnostic and therapeutic • Skin suturing
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 41
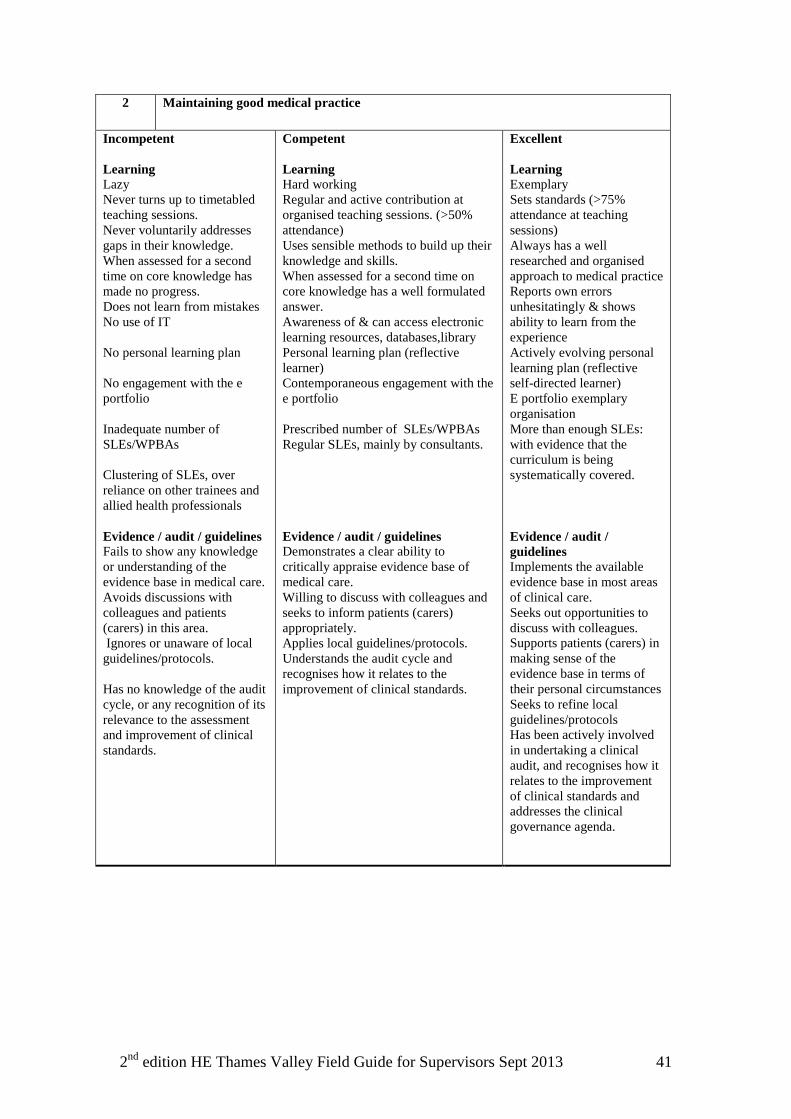
2 Maintaining good medical practice
Incompetent Learning Lazy Never turns up to timetabled teaching sessions. Never voluntarily addresses gaps in their knowledge. When assessed for a second time on core knowledge has made no progress. Does not learn from mistakes No use of IT No personal learning plan No engagement with the e portfolio Inadequate number of SLEs/WPBAs Clustering of SLEs, over reliance on other trainees and allied health professionals Evidence / audit / guidelines Fails to show any knowledge or understanding of the evidence base in medical care. Avoids discussions with colleagues and patients (carers) in this area. Ignores or unaware of local guidelines/protocols. Has no knowledge of the audit cycle, or any recognition of its relevance to the assessment and improvement of clinical standards.
Competent Learning Hard working Regular and active contribution at organised teaching sessions. (>50% attendance) Uses sensible methods to build up their knowledge and skills. When assessed for a second time on core knowledge has a well formulated answer. Awareness of & can access electronic learning resources, databases,library Personal learning plan (reflective learner) Contemporaneous engagement with the e portfolio Prescribed number of SLEs/WPBAs Regular SLEs, mainly by consultants. Evidence / audit / guidelines Demonstrates a clear ability to critically appraise evidence base of medical care. Willing to discuss with colleagues and seeks to inform patients (carers) appropriately. Applies local guidelines/protocols. Understands the audit cycle and recognises how it relates to the improvement of clinical standards.
Excellent Learning Exemplary Sets standards (>75% attendance at teaching sessions) Always has a well researched and organised approach to medical practice Reports own errors unhesitatingly & shows ability to learn from the experience Actively evolving personal learning plan (reflective self-directed learner) E portfolio exemplary organisation More than enough SLEs: with evidence that the curriculum is being systematically covered. Evidence / audit / guidelines Implements the available evidence base in most areas of clinical care. Seeks out opportunities to discuss with colleagues. Supports patients (carers) in making sense of the evidence base in terms of their personal circumstances Seeks to refine local guidelines/protocols Has been actively involved in undertaking a clinical audit, and recognises how it relates to the improvement of clinical standards and addresses the clinical governance agenda.
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 42
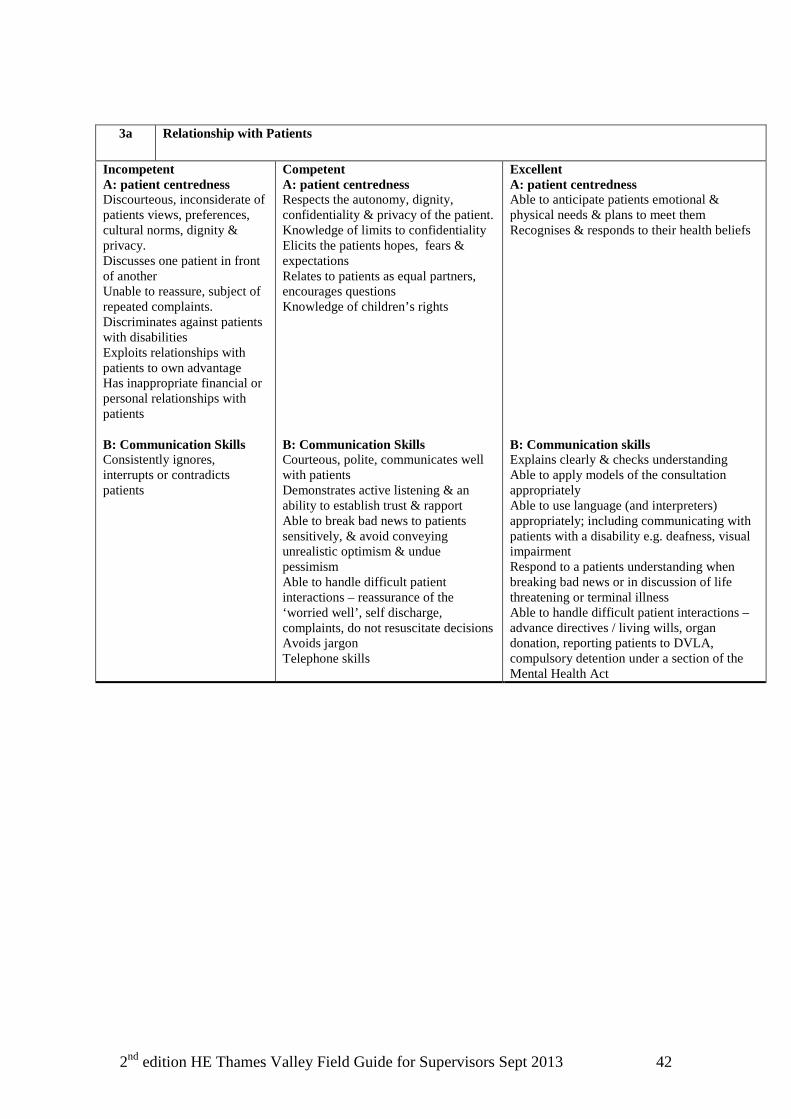
3a Relationship with Patients
Incompetent A: patient centredness Discourteous, inconsiderate of patients views, preferences, cultural norms, dignity & privacy. Discusses one patient in front of another Unable to reassure, subject of repeated complaints. Discriminates against patients with disabilities Exploits relationships with patients to own advantage Has inappropriate financial or personal relationships with patients B: Communication Skills Consistently ignores, interrupts or contradicts patients
Competent A: patient centredness Respects the autonomy, dignity, confidentiality & privacy of the patient. Knowledge of limits to confidentiality Elicits the patients hopes, fears & expectations Relates to patients as equal partners, encourages questions Knowledge of children’s rights B: Communication Skills Courteous, polite, communicates well with patients Demonstrates active listening & an ability to establish trust & rapport Able to break bad news to patients sensitively, & avoid conveying unrealistic optimism & undue pessimism Able to handle difficult patient interactions – reassurance of the ‘worried well’, self discharge, complaints, do not resuscitate decisions Avoids jargon Telephone skills
Excellent A: patient centredness Able to anticipate patients emotional & physical needs & plans to meet them Recognises & responds to their health beliefs B: Communication skills Explains clearly & checks understanding Able to apply models of the consultation appropriately Able to use language (and interpreters) appropriately; including communicating with patients with a disability e.g. deafness, visual impairment Respond to a patients understanding when breaking bad news or in discussion of life threatening or terminal illness Able to handle difficult patient interactions –advance directives / living wills, organ donation, reporting patients to DVLA, compulsory detention under a section of the Mental Health Act
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 43
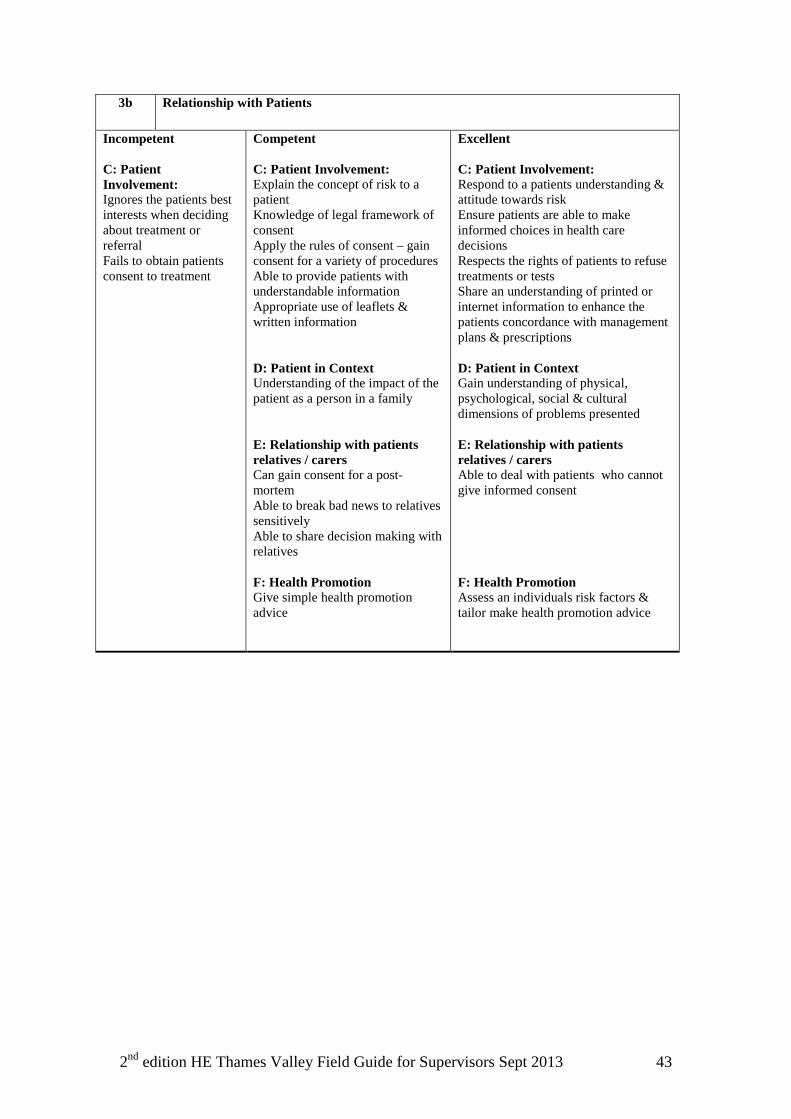
3b Relationship with Patients
Incompetent C: Patient Involvement: Ignores the patients best interests when deciding about treatment or referral Fails to obtain patients consent to treatment
Competent C: Patient Involvement: Explain the concept of risk to a patient Knowledge of legal framework of consent Apply the rules of consent – gain consent for a variety of procedures Able to provide patients with understandable information Appropriate use of leaflets & written information D: Patient in Context Understanding of the impact of the patient as a person in a family E: Relationship with patients relatives / carers Can gain consent for a post-mortem Able to break bad news to relatives sensitively Able to share decision making with relatives F: Health Promotion Give simple health promotion advice
Excellent C: Patient Involvement: Respond to a patients understanding & attitude towards risk Ensure patients are able to make informed choices in health care decisions Respects the rights of patients to refuse treatments or tests Share an understanding of printed or internet information to enhance the patients concordance with management plans & prescriptions D: Patient in Context Gain understanding of physical, psychological, social & cultural dimensions of problems presented E: Relationship with patients relatives / carers Able to deal with patients who cannot give informed consent F: Health Promotion Assess an individuals risk factors & tailor make health promotion advice
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 44
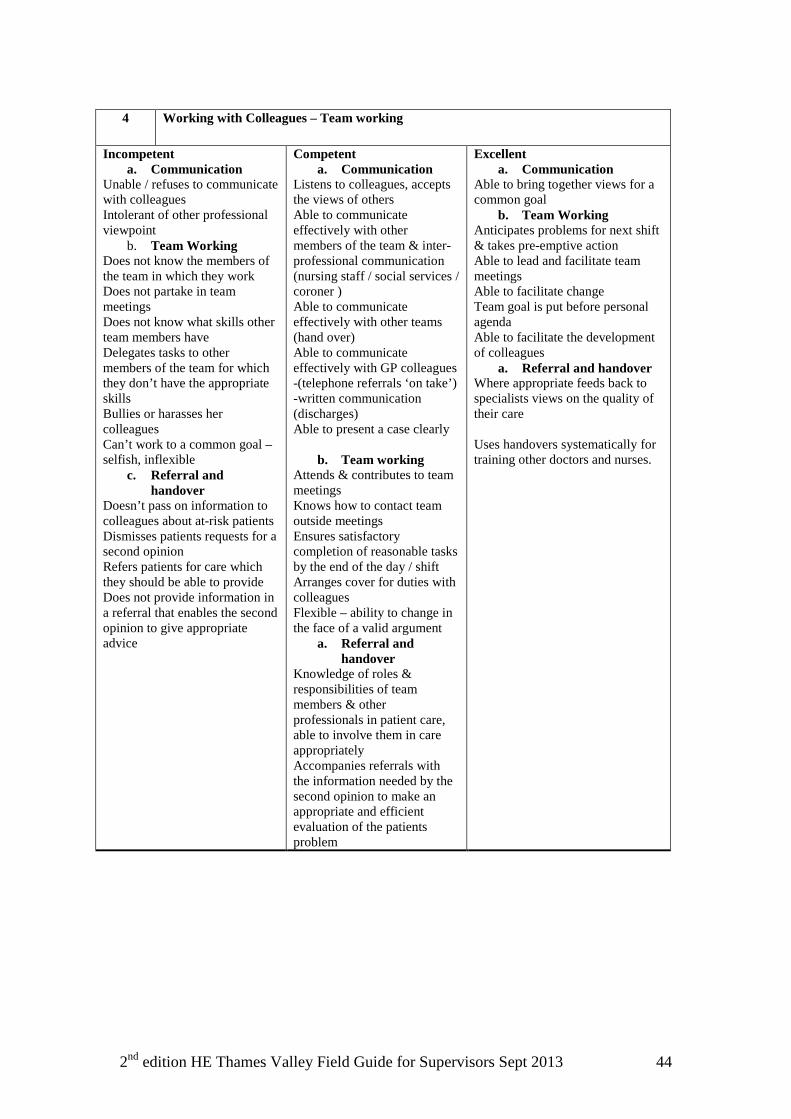
4 Working with Colleagues – Team working
Incompetent a. Communication
Unable / refuses to communicate with colleagues Intolerant of other professional viewpoint
b. Team Working Does not know the members of the team in which they work Does not partake in team meetings Does not know what skills other team members have Delegates tasks to other members of the team for which they don’t have the appropriate skills Bullies or harasses her colleagues Can’t work to a common goal – selfish, inflexible
c. Referral and handover
Doesn’t pass on information to colleagues about at-risk patients Dismisses patients requests for a second opinion Refers patients for care which they should be able to provide Does not provide information in a referral that enables the second opinion to give appropriate advice
Competent a. Communication
Listens to colleagues, accepts the views of others Able to communicate effectively with other members of the team & inter-professional communication (nursing staff / social services / coroner ) Able to communicate effectively with other teams (hand over) Able to communicate effectively with GP colleagues -(telephone referrals ‘on take’) -written communication (discharges) Able to present a case clearly
b. Team working Attends & contributes to team meetings Knows how to contact team outside meetings Ensures satisfactory completion of reasonable tasks by the end of the day / shift Arranges cover for duties with colleagues Flexible – ability to change in the face of a valid argument
a. Referral and handover
Knowledge of roles & responsibilities of team members & other professionals in patient care, able to involve them in care appropriately Accompanies referrals with the information needed by the second opinion to make an appropriate and efficient evaluation of the patients problem
Excellent a. Communication
Able to bring together views for a common goal
b. Team Working Anticipates problems for next shift & takes pre-emptive action Able to lead and facilitate team meetings Able to facilitate change Team goal is put before personal agenda Able to facilitate the development of colleagues
a. Referral and handover Where appropriate feeds back to specialists views on the quality of their care Uses handovers systematically for training other doctors and nurses.
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 45
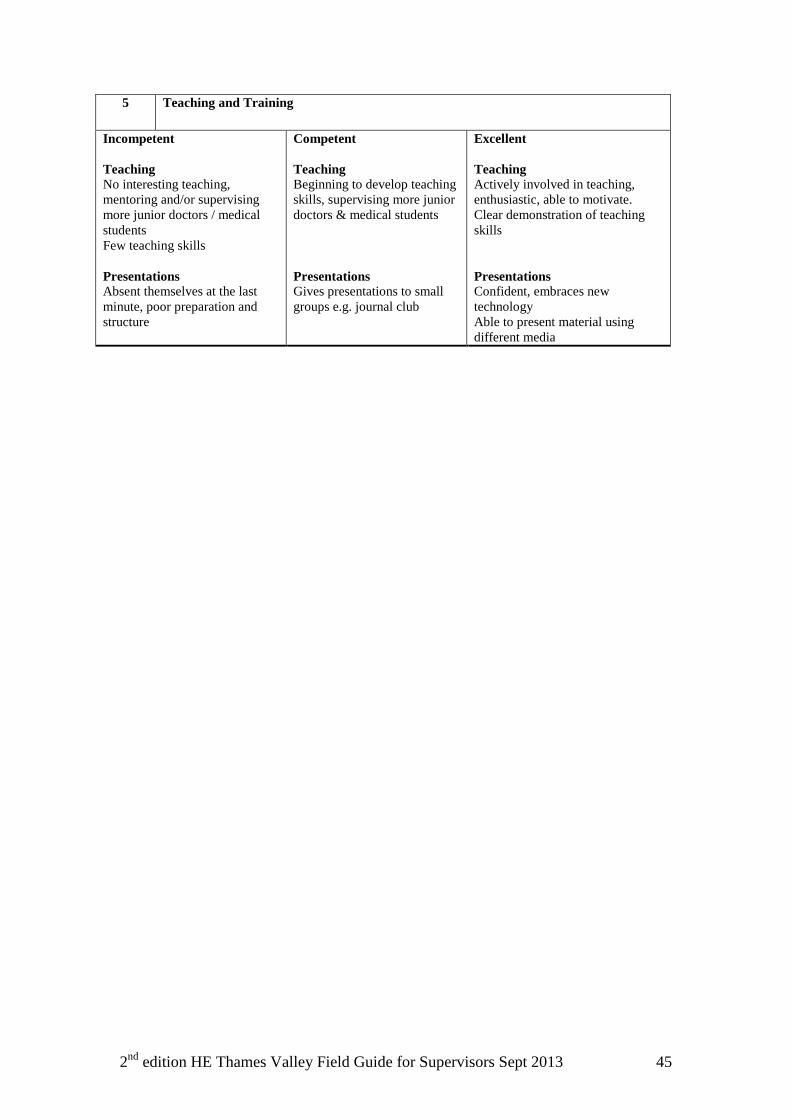
5 Teaching and Training
Incompetent Teaching No interesting teaching, mentoring and/or supervising more junior doctors / medical students Few teaching skills Presentations Absent themselves at the last minute, poor preparation and structure
Competent Teaching Beginning to develop teaching skills, supervising more junior doctors & medical students Presentations Gives presentations to small groups e.g. journal club
Excellent Teaching Actively involved in teaching, enthusiastic, able to motivate. Clear demonstration of teaching skills Presentations Confident, embraces new technology Able to present material using different media
2nd edition HE Thames Valley Field Guide for Supervisors Sept 2013 46
Appendix D: Checklist for Adult Dyslexia