hand peripheral and csf biomarkers: pitfalls and promises · hand peripheral and csf biomarkers:...
TRANSCRIPT

HAND Peripheral and CSF Biomarkers:
Pitfalls and Promises
BJ Brew and T Burdo
October 26, 2016

Disclosures
• BJ Brew
• Relationships with commercial interests• Grants: NIH, NHMRC; Research support: Biogen Idec,
Viiv• Patent: QUIN mAB• Speakers Honoraria: Biogen Idec, Viiv, AbbVie• Employee of St Vincent’s Health Australia, University of
New South Wales, and University of Notre Dame
• Tricia Burdo:
• No relationships with commercial interests• No conflicts of interest

Overview
• Introduction
• Principles and Pitfalls
• Individual biomarkers
• How each biomarker fits into a practical framework

INTRODUCTION

ART has reduced the severity of HIV-associated neurocognitive disorders
Pre ART
Adapted from: McArthur, J. C. et al. (2016) Nat. Rev. Neurol.
Post ART (after 1996)
The Therapeutic Paradox

0
5
10
15
20
25
30
35
40
45
Cysique (C-S) Robertson (C-S) Robertson (L) Sevigny (L)
21---59
319-----807
276-----717
15---40
3639 38 37.5
Neuropsychological impairment rates in those with plasma VL<50 cpml
21---59
15---40

HIV comorbidities are associated with chronic low-grade inflammation
Adapted from: Freund. et al. (2010) Trends Molecular Med
Chronic Inflammation/
immune activation
Cardiovasculardisease
Bonediseases
Cancers
Frality
Metabolic diseases, diabetes
HAND
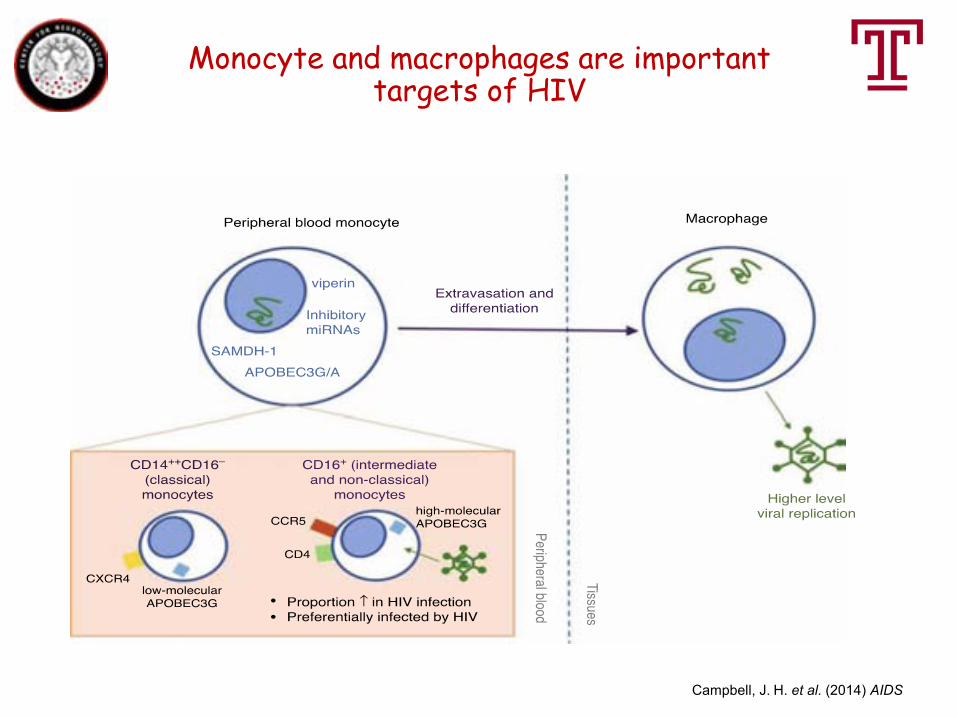
Monocyte and macrophages are important targets of HIV
Campbell, J. H. et al. (2014) AIDS

Changes of monocytes during HIV infection
Campbell, J. H. et al. (2014) AIDS

Overview of HAND pathogenesis pre cART
Adapted from Gonzalez-Scarano F et al. Nat Rev Immunol 2005;5:69-81
1
3
2
5
4
-Autophagy*
ubiquitin proteosome systemImmunoproteosome**
*Gougeon ML et al. Apoptosis 2009;14:501-508**Nguyen TP, et al. Am J Pathol 2010;176:893-902
Neurotropism: CCR5 > CXCR4
Migration of microbial translocation products

HAND Cellular Pathogenesis
Macrophages:
• Critical to HIV mediated neuropathogenesis
• Serve as viral reservoirs within the CNS
• Release inflammatory mediators and neurotoxic viral and host proteins
• Central to HIV-associated neuroinflammation and neurocognitive dysfunction
Astrocytes are also crucial but monocytes/macrophages are important from a systemic perspective

Possible causes of sustained CNS inflammation during ART
• Latent and low level infection in the brain (CSF viral escape)
• Microglia priming (circulating products translocated from gut)
• Macrophages- harbors HIV, produce virions and are long-lived
• Disturbed cellular energy (infected macrophages release ATP)
• Neuronal and synaptic protein dynamics are altered
• Contributions from cerebrovascular dysfunction, metabolic alterations, ART regimens
PRINCIPLES AND PITFALLS

Principles• 1. HAND has a unitary pathogenesis:
– HAND with viral suppression = HAND without viral suppression?
– HAND with HIV encephalitis = HAND without HIV encephalitis (just less inflammation)?
– ANI/MND have the same pathogenetic pathway?


Principles• HAND has a unitary pathogenesis:
– HAND with viral suppression = driven by viral components eg tat nef etc?
– HAND without viral suppression = driven by whole virus especially env?

HAND + HIVE = HAND – HIVE?
Modified from Desplats et al Neurol 2013
12---59
12---32
10---32
10---32
12---32
12---32
10---32
10---32
10---32
10---32
Neuropsychological impairmentSevere6/6
Severe6/6
Severe6/6
Mild/mod5/9 6/8
Mild/mod5/9 6/8
Mild/mod5/9 6/8

Gelman et al PLoS One 2012
HAND + HIVE = HAND – HIVE?

ANI/MND have the same pathogenetic pathway?
• 3 cases of ANI = HIVE (Cherner et al J Nvirol 2007)
• 10 cases of mild/moderate neuropsychological impairment = latent HIV only (Desplats et al Neurol 2013)

HAND NEUROVIROLOGY BRAIN
Latent infection
Productive infectionANI/MND
HAD
Principles• 2. HAND is driven by systemic and CNS
(CSF/brain) disease (HIV/inflammation)
• But:
– Systemic and CNS equally?
– To differing extents at different time points in HIV disease course?

Mild HAND is prevalent
It is driven by compartmentalized brain viral
latency burden/activity Mild HAND isRelatively uncommon
It is driven by peripheral viral latency burden/activity
Mild HAND is prevalent
It is driven by compartmentalized brain viral
latency burden/activity Mild HAND isRelatively uncommon
It is driven by peripheral viral latency burden/activity
HIV-associated dementiaBBB disrupted
Peripheral & CNS viral latency
Cysique and Brew unpublished

Principles• 3. Activity of HAND:
– Progressing– Regressing– Stable but subclinically active: “simmering pot”– Stable inactive: “legacy” ?evidence
• 4. Reparative and remodelling aspects: emerging evidence

Modified from Cysique et al Neurology 2009
Differing Biomarker effects
EFFECT OF RECENT ARV CHANGE ON BIOMARKER INTERPRETATION

Cysique et al under review

Principles• 5. Account for confounds:
– Substance misuse– Hepatitis C– Overlap with other conditions associated with
aging:• Vascular disease• Degenerative: Alzheimer’s, Parkinson’s

HIV
AGE
Pathogenesis of Neurodegenerative Diseases
Pathogenic insult
misfolded protein stress/toxic proteins
mitochondrial dysfunction
inflammation
transcription dysregulation
excitotoxicity
Oxidative/Nitrosative stress
cell dysfunction/death
Defence failure: Hsps, ER chaperones, Ubiquitin-proteasome, autophagy, Pic, ?PgP
inflammation
Modified from Brew et al J Neuroimm Pharm 2009
proteasome, autophagy, Pic, ?PgP
mitochondrial dysfunction
inflammation
Defence failure: Hsps, ER chaperones, Ubiquitin-proteasome, autophagy, Pic, ?PgP
inflammation
ARV

CSF Biomarkers and Age Effect
De Oliveira et al Sci Rep 2015

A new model of chronic HAND pathogenesis?
HIV HIV duration
AgeCVD
cART
↓NAA
↓NAA
↑ mIo↓NAA
↑ mIo
-
-
Inflammation
Inflammation
Inflammation
~ ↑ neopterin~ ↑ Cr
Cysique et al PLoS One 2014

Principles
• 6. Universality-Selectivity:
• all patients are vulnerable?
• It is now clear that only some patients are susceptible ––The principle of selectivity

Principles
• Biomarkers must developed within latter framework accounting for concepts of activity and repair

Principles: Approach
Price et al Neurology 2007
Metabolic
VascularTrophic
S1oob
neopterin
Marcotte et al JNIP 2013

Suggested Solutions
• “Clean” large data sets (not a “wash out” strategy)
• Well characterised:– Presence and duration of viral suppression– ARV history– CD4 history– HAND history– Neuropathology

PERIPHERAL BIOMARKERS

Tricia Burdo, Ph.D.
Associate Professor
Neuroscience
215-707-1618 (office)
[email protected] (email)[email protected]
Peripheral biomarkers in HIV-associated neurocognitive disorders

Biomarkers of HIV-associated dementia (HAD) before ART
Decrease CD4+ T cells:current if naïve - permissive effect when <200 cells/μl, even
<350 cells/μl (Bhaskaran K et al Ann Neurol 2008)Nadir if experienced (Cysique LA et al. Neurology 2006, Valcour V et al. J
Neurovirol 2006, Robertson et al 2007)AnaemiaLow PlateletsImpaired glucose tolerance esp diabetes (Valcour V et al JAIDS 2005)
Plasma viral loadCSF viral loadCCL2IL-6sCD14NeopterinKynurenineQuinolinic acid
But none is specific for HAND

Elevated CD16+ monocytes [Pulliam Lancet 1997,Williams Clin Invest 2005, Campbell Plos One 2011]
Elevated sCD14 (receptor for LPS) [Lyons 2011, Ancuta 2008, Royal 2016]
Elevated sCD163 (Burdo 2013, Royal 2016)- increased in MNDNeither correlate with npsych/HAND but none on cART (McGuire JNvirol 2015)
Loss of CCR2+ CD14loCD16hi monos (Ndhlovu 2015)
CCR2+ on CD14+CD16+ (increased in HAND, not differentiate between ANI, MDN, HAD) (Williams 2014 Neurology)
High HIV DNA levels in CD16+ monocytes [Kusao 2012, Valcour et al 2013, Cysique et al 2015]
Vascular disease: HT, CVD, hypercholesterolaemia (Wright et al 2010)
Peripheral biomarkers of HAND
CCR2+ on CD14+CD16+ (increased in HAND, not differentiate between ANI, MDN, HAD)
Monocyte related

Micro RNAs
• HAND associations:miR-3665 > miR-4516 > miR-4707–5p• But: small n, no ANI, not virally suppressed
Asahchop et al AIDS 2016

Plasma NFL elevated in HAD
Gisslen, 2016
But NFL is quickly hydrolysed – cannot use stored samples

Insights from the SIV-infected rhesus macaque model
CD16+ monocytes peak during acute infection and with AIDS
Williams K., J Clin Invest 2005 Burdo T., PLoS Pathogens 2010
Monocyte expansion in the first weeks of infection predicts the rate of disease progression

Burdo et al. PLos Pathogens, 2010
Monocyte expansion from bone marrow correlates with rapid AIDS, severity of SIVE and sCD163 levels
sCD163 plasma is the best correlate of BrdUmonocytes

Shedding of the scavenger receptor CD163
CD163 exclusively expressed on monocytes and M2
macrophages (Zwadlo, Exp Cell Bio, 1987, Pulford, Immunol. 1992, Backe, J. Clin. Pathol. 1991)
CD14+CD16+ monocytes have the highest expression
of CD163 (Buechler, JLB 2000)
CD163 is a receptor for bacteria, CD163 on tissue macrophages acts as an innate immune receptor and
inducer of local inflammation (Fabriek Blood 2009)
Shedding of sCD163 occurs following activation of TLR-4 by LPS; crosslinking of the Fcg receptor; oxidative
stress, PMA or thrombin stimulation (Hintz, J Leukoc Biol 2002; Weaver, J Leukoc Biol 2006; Sulahian, J Leukoc Biol 2006; Chung, Thromb Res 2011).
The simultaneous release of CD163 and TNF-α is mediated by the enzyme ADAM17/TACE under
inflammatory stimuli (Etzerodt, J Leukoc Biol 2010)
Moller, Scand J Clin Lab Invest, 2012

Burdo et al. JID 2011
sCD163 plasma is elevated in chronic and early HIV-infected subjects and monocyte activation persists with ART

sCD163 is elevated in plasma of impaired HIV-infected patients
Burdo et al. AIDS, 2013

sCD163 decreased in patients that remained unimpaired
sCD163 levels dropped in patients who were stably GDS-unimpaired across visits
Levels remained elevated in those who remained GDS-impaired
Burdo et al. AIDS, 2013

CSF BIOMARKERS

NEURAL BIOMARKERS

CSF NFL
• Correlates with HAND severity (Gisslen et al 2005)
• Decreases with cART (Mellgren et al Neurol 2007)
• Predicts HAND (Gisslen et al JID 2007) SIVE (Beck et al Eur J Pharmacol 2015)
• Not correlated with plasma sCD14 or sCD163 at least in ARV naïve pts (McGuire et al J Nvirol 2015)
Brown et al Mol Neurodegen 2014

CSF NFL
Gisslen et al EBioMedicine 2016

?sensitive enough for ANI/MND in suppressed ptsPeterson et al 2015

CSF NFL
McGuire et al JNvirol 2015

Tau
• Microtubule associated protein largely found in the CNS
• Inflammation can phosphorylate tau• The major reasons for discordant results in
HIV relate to:– Differing ages of patient– Differing ARV history
Brown et al Mol Neurodegen 2014

CSF S100b
• Mainly a marker of astrocytes• Pro-inflammatory• Inhibits GFAP• Neurotoxic• Correlates with HAND severity (Pemberton Brew 2001,
Woods et al JCEN 2010)
CSF GFAP
• Mainly a marker of fibrillary astrocytes
• Variable and limited data on rel’p to HAND (Sporer 2001) (Andersson 2006)

CSF Neopterin• Macrophage/microglia marker• Correlates with HAND severity in ART naïve
(Brew et al Ann Neurol 1990) and SIV (Beck et al Eur J Pharmacol 2015)
• Predicts HAND (Pemberton JID 1996)
• Common for mild elevation despite suppressive cART (Yilmaz et al 2013)
• ?Evidence for neurotoxicity• Correlates with plasma sCD163
Brown et al Mol Neurodegen 2014

CSF BBB
Calcagno et al J Nvirol 2016


IMMUNOLOGICAL BIOMARKERS
CSF sCD14
• Soluble form of the monocyte lipopolysaccharide (LPS) receptor which is cleaved and released from the membrane following the activation of monocytes
• Correlates with HAND severity (Lyons et al 2011)
Brown et al Mol Neurodegen 2014

CSF sCD163
McGuire et al JNvirol 2015

CSF Neopterin and NFL and sCD14
Jespersen et al BMC inf Dis 2016

CSF Kynurenine Pathway and cART in SIV
Drewes et al J Nvirol 2015

CSF QUIN/TRP Predicts SIVE

CSF CCL2
• Correlates with HAND Severity and risk (Sevigny et al 2004) (Anderson et al J Nvirol 2015) (Thames et al AIDS 2015)
• Correlates with neopterin (Price 2007 Neurology)

CSF YKL-40
• Human cartilage glycoprotein 39• Expressed on chondrocytes, synoviocytes,
neutrophils, and monocytes in several chronic inflammatory and neoplastic conditions (Bonneh-Barkay et al, 2008).
• Correlated with SIVE and increased CSF viral load (Bonneh-Barkay et al, 2008).
• Emerging data on correlation with HAND severity

CSF microRNAs
• miR125b (MMPs and cell-death proteins) and 146a (microglial infection)
• Correlate with HIVE (Pacifici J Cell Physiol 2013) but:– Small study (10 pts: 9 HAND – 4 with HIVE)– No data on ARVs or viral suppression

CSF microRNAs
Pacific et al J Cell Physiol

CSF MicroRNAs

VIRAL BIOMARKERS

CSF HIV DNA
• Insensitive – even with digital droplet PCR: 2 of 44 pts (de Oliveira et al Sci Rep 2015)
• ?related to insufficient volume of CSF• Issue of practicality….

TROPHIC FACTOR BIOMARKERS

CSF Progranulin
• Expressed by both neurons and microglia• Neuronal growth factor and modulator of
neuroinflammation• Lowered in HAND on suppressive cART (Suh
et al PLoS One 2014)
• ?through lack of neurotrophic support• Elevated in HIVE off cART (Suh et al PLoS One 2014)
CSF Insulin Like Growth Factors
• Pathway is disturbed but ?significance for HAND (Suh et al J Neuroinflamm)

CSF Growth Factors and HAND with cART
(HIVE: defects in adult neurogenesis in the hippocampus (Avraham et al. 2013; Lee et al. 2013)

METABOLIC BIOMARKERS

CSF Sphingolipids and Ceramide
• Sphingolipids elevated in mild-moderate HAND
• Ceramide elevated in more severe HAND• Similarity to lysosomal storage diseases• Shift from single to mutiple lipid specis with
HAND progression (Bandaru et al Neurol 2013)

CSF Lipids in HAND
Rahman and He Prog Neurobiol 2015

LATENCY BIOMARKERS

HAND BIOMARKERS
Desplats et al Neurol 2013

PRACTICAL FRAMEWORK FOR BIOMARKERS

How Can CSF Biomarkers Help?• Diagnosis:
– Presence– Severity– Activity
• Prediction:– HAND development– HAND treatment response: balance of
“drivers”• Immunological > viral?
• Identify and quantify latency

+ CART Sensitivity Activity Devlpmnt Response Latency
NFL yes Excellent Very good Very good Very good ?
Tau No Very good Very good ? Very good ?
S100b ? Yes Very good ? ? ? ?
GFAP ? ? ? ? ? ?
Neopterin Yes Very good Very good ?yes yes ?
BBB ?no Good ? ? ? ?
sCD14/sCD163 ? Very good ? ? ? ?
QUIN/TRP Yes (SIV) Very good ? ? ? ?
CCL2 ?yes Very good ? ? ? ?
YKL-40 ? Good ? ? ? ?
MicroRNA ? Good ? ? ? ?
HIV DNA ? Poor ? ? ? ?
HIV RNA (SCA) Yes Good ? ? ? ?
Growth Factors ? ? ? ? ? ?
Lipids Yes Good yes ? ? ?
BCL11b ? ? ? ? ? ?yes
More work needed

Collaborators and funding
Steve GrinspoonMarkella ZanniSara LoobyJanet LoMabel ToribioKatie FitchSuman Srinivasa
Ken WilliamsPatrick Autissier
TB’s Funding:R01 NS082116 (PI)U01 HL123336 (PI, sub)R01 AI123001 (PI, sub)R01 NR015738 (PI, sub)
Dr. Burdo has no disclosures
Burdo Lab:Jessica LakritzJake Robinson
Ron EllisScott Letendre
Xavier AlvarezCecily Midkiff
Andrew Miller
Walter Royal

Acknowledgements• Lucette Cysique UNSW
• Melissa Churchill RMIT
• Louise Pemberton CSU
• Edwina Wright Burnet Centre
• Magnus Gisslen SahlgrenskaUniversity
• Richard Price UCSF