haemodynamic observations during percutaneous...
TRANSCRIPT

Br Heart J 1988;59:159-67
Haemodynamic observations during percutaneous
transluminal coronary angioplasty in the presence ofsynchronised diastolic coronary sinus retroperfusionKEVIN J BEATT, PATRICK W SERRUYS, PIM DE FEYTER,MARCEL VAN DEN BRAND, PIETER D VERDOUW, PAUL G HUGENHOLTZ
From the Catheterisation Laboratory and Laboratory for Clinical and Experimental Image Processing,Thoraxcenter, Erasmus University, Rotterdam, The Netherlands
SUMMARY Animal studies have demonstrated that synchronised coronary sinus retroperfusionwith arterial blood can provide effective perfusion of ischaemic myocardium. Preliminary clinicalstudies have shown that the technique can also be used with safety in human beings, and in thepresent study its effectiveness was assessed in three patients undergoing repeated coronary arteryocclusions during percutaneous transluminal coronary angioplasty. Arterial blood was removedvia an 8F catheter positioned in the femoral artery and delivered by a retroperfusion pumpingsystem to a 7F retroperfusion balloon catheter positioned in the anterior cardiac vein. Ischaemia-related indices were monitored both before and during coronary sinus retroperfusion. Theseindices included high fidelity left ventricular pressure recordings and pressure derived indices(including velocities of isovolumic contraction and relaxation), as well as electrocardiographicchanges and symptoms. Analysis of these variables showed that the ischaemic changes inducedduring coronary artery occlusion were not prevented by this type of coronary sinus retroperfusion.There was no major complication in any of the patients.
It may be that adaptation of the technique or the use of alternative end points will establish a
benefit, but further modifications of the delivery system are necessary for effective clinical use.
The effective preservation of acutely ischaemicmyocardium remains an elusive goal. Coronary sinusretroperfusion has been put forward as a practicaltechnique for providing temporary support ofjeopardised myocardium. The concept was originallytested in the clinical setting by Beck et al in the 1940swith disappointing results.' They used an aorta-to-coronary-sinus anastomosis with an artificiallyincreased coronary sinus outflow resistance to shunta proportion of the blood retrogradely. The increasein venous pressure, however, led to myocardialengorgement and eventual myocardial failure. In1976 Meerbaum et al ' introduced a synchroniseddelivery system that limited the delivery of arterialblood to the coronary sinus to diastole, therebyovercoming some of the original complicationsassociated with the continuous increase in pressure in
Requests for reprints to Dr Patrick W Serruys, CatheterizationLaboratory and Laboratory for Clinical and Experimental ImageProcessing, Thoraxcenter, Erasmus University, PO Box 1738, 3000DR Rotterdam, The Netherlands.
Accepted for publication 3 August 1987
the coronary venous system. This technique waseffective and safe in animal studies,3 and improvedmyocardial salvage, myocardial perfusion, andindices related to ischaemia.' Although there isbroad agreement on the safety of the procedure notall of the animal studies showed an improvement inmyocardial perfusion.78
Clinical studies confirmed the safety of theprocedure in human beings, and suggested that itmay be useful in unstable angina and during per-cutaneous transluminal coronary angioplasty.9"'Recently Gore et al reported the experience ofretroperfusion in five patients with acute ischaemia."The procedure had no adverse effects and despiteclinically encouraging results there was little objec-tive evidence to support its effectiveness. Wetherefore conducted a pilot study in three patients todetermine whether synchronised coronary sinusretroperfusion prevented transient loss ofmyocardialfunction, as assessed by central haemodynamicindices, during repeated occlusion of the coronaryartery in percutaneous transluminal coronary angio-plasty.
159
on 16 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.59.2.159 on 1 F
ebruary 1988. Dow
nloaded from
Beatt, Serruys, de Feyter, van den Brand, Verdouw, Hugenholtz
Patients and methods
PATIENT SELECTIONWe studied three patients who had easily provokedangina, a lesion ofthe proximal left anterior descend-ing artery with a large area of potentially ischaemicmyocardium, normal left ventricular anterior wallmotion, and no angiographically demonstrablecollateral supply to the potentially ischaemic area.
RETROPERFUSION SYSTEMOxygenated blood was delivered by a size 7 Fr singlelumen, Nycore, retroperfusion catheter (USCI Div-ision of Bard Inc. Billerica, MA, USA), 90 cm inlength, and with a lumen diameter of 0-56 mm. Thiscatheter consists of a balloon (maximal inflationdiameter 10 mm) positioned close to the tip of thecatheter that communicates with the central lumen ofthe catheter via a number of small holes. Thus whenblood is pumped through the catheter, the increase inintraluminal pressure producing the flow throughthe catheter also causes the balloon to inflate, whichin turn leads to occlusion of the coronary sinuslumen, thereby directing the delivered bloodretrogradely (fig la). When flow ceases during sys-tole, intraluminal pressure falls, the balloon deflates,and normal forward coronary sinus flow is resumed.The tip of the catheter was positioned in the great
cardiac vein, under fluoroscopic control with the aidof a 0-018 inch (Advanced Catheter Systems) hightorque guide wire, and the position was verified byinjection of contrast. Arterial blood was delivered tothe catheter via a USCI synchronised retroperfusionsystem, model EC-I. Blood was removed with aspecial multihole catheter (8F, 40 cm (USCI))introduced to the distal aorta via the femoral artery.There were three parts to the retroperfusion system:(a) a linear, constant force pump with a variablestroke volume; (b) a Hewlett Packard 7834 monitor todisplay selective electrocardiographic signals as wellas perfusion and aortic pressures; (c) a pump controldevice that allowed the onset and duration of thepump stroke to be adjusted in relation to the trigger-ing R wave. In addition, it allowed the volume ofblood delivered per minute to be controlled indepen-dently of the heart rate.
HAEMODYNAMIC AND ELECTROCARDIOGRAPHICMONITORINGLeft ventricular pressure was measured by a Millarmicromanometer catheter and digitised at 250 sam-ples per second. A beat to beat computer programwas used to analyse, display, and store the pressuresignals for off line analysis. Peak left ventricularpressure, left ventricular end diastolic pressure, peaknegative dP/dt, peak positive dP/dt, and the relation
between dP/dt/pressure and pressure linearlyextrapolated to pressure 0 (Vmax) (where Vmax isthe maximal velocity) were computed for eachmeasured beat. Tau,, the time constant for the first 40ms, taken from the bi-exponential model of theisovolumic relaxation period was also recorded. Thedefinition of the pressure derived indices and theirmethod of determination have been described else-where. 1214
Electrocardiograms from leads I, II, and V3 wererecorded throughout the procedure and in additionan intracoronary electrocardiogram was recordedfrom the intraluminal balloon guide wire in one ofthepatients. The ST changes are expressed in mV andwere recorded from the lead showing the maximalchange in ST segment during occlusions, measuredfrom the isoelectric line (P-Q interval) 0-08 secondsafter the J point.
PROTOCOLThe protocol was approved by the ethics committeeofthe Thoraxcenter. The data were collected accord-ing to the guidelines ofthe Food and Drugs Adminis-tration of the United States and the procedures wereperformed with the technical assistance of represen-tatives from the industry. Patients gave their infor-med consent to the study.A pacing wire was positioned in the right atrium,
and coronary angiography and left ventriculographywere performed. The catheter for monitoring pres-sure was then positioned in the left ventricle and theretroperfusion catheter was inserted into the coron-ary sinus. The catheter for dilating the coronaryartery was then introduced and the lesion wascrossed. Two control dilatations were performedwith haemodynamic monitoring before retroper-fusion was started. This was started at an initialmeasured flow rate of50 ml/min, increasing by 20 ml/min, up to 150 ml/min. Retroperfusion was thencontinued for 20 minutes. The extent of retroper-fusion was assessed visually by direct hand injectionof contrast (fig ib). Two further investigationalballoon dilatations were then performed.
Case reports
Patient 1-A 67 year old woman was admitted withchest pain at rest, which continued despite adminis-tration of intravenous isosorbide dinitrate. Coronaryangiography showed an isolated severe proximalstenosis in the left anterior descending artery and shewas therefore transferred to the Thoraxcenter for animmediate angioplasty. The retroperfusion catheterwas satisfactorily positioned via the right femoralvein. Four balloon dilatations were performed at 10atmospheres each-two before retroperfusion and
160
on 16 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.59.2.159 on 1 F
ebruary 1988. Dow
nloaded from

Coronary sinus retroperfusion during PTCA
- Great cardiac vein
Left anterior descendingcoronary artery
Anterior cardiac vein
Posterior interventricular vein
Fig 1 (a) Diagram showing the retroperfusion catheter positioned in the great cardiac vein. (b) Singleframe angiogramshowing the retroperfusion catheter positioned in the great cardiac vein. The anterior cardiac vein is clearly delineated by handinjection of contrast. This produces a myocardial blush and shows the venous to venous collateral circulation (arrows).
Coronarysinus
161
on 16 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.59.2.159 on 1 F
ebruary 1988. Dow
nloaded from
Beatt, Serruys, de Feyter, van den Brand, Verdouw, Hugenholtz
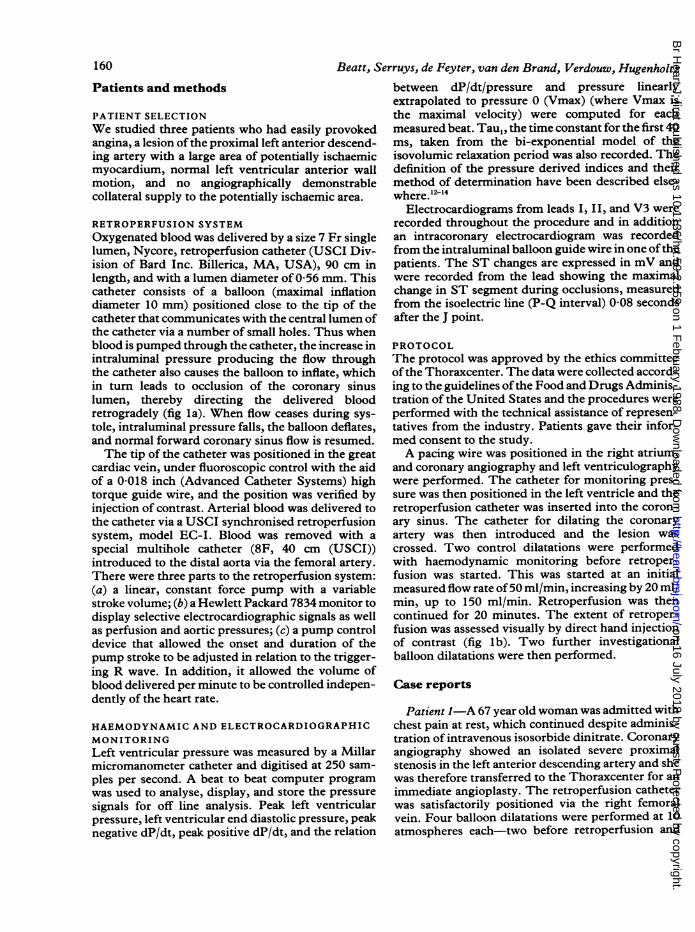
Table Time(s) to ST change (mV) inflation and time tonormalisation after deflation in patient I
Occlusion
Baseline I Baseline 2 SRP I SRP 2
Time to:0-2 mV 10 15 20 180 4mV 30 35 26 24
Normalisation(after deflation) 40 30 45 20
Baseline, before retroperfusion; SRP, during retroperfusion.
two afterwards. The duration of inflations rangedfrom 45 to 52 seconds. The stenosis of the leftanterior descending artery was successfully dilated toa <50% diameter stenosis. The table shows the timeto 0-2 mV and 0-4 mV ST changes during theocclusions. The measured indices of left ventricularpeak systolic pressure, left ventricular end diastolicpressure, positive dP/dt, negative dP/dt, Vmax, andTau,, changed progressively during occlusion, inkeeping with induced myocardial ischaemia. Figure2 shows the electrocardiogram, left ventricular pres-sure, and retroperfusion flow recordings at the end ofeach occlusion compared with the baseline record-ings. At the end ofeach occlusion there was 0-4 mV ofST elevation; there was considerable variability in
Lead 11
Lead V5
LV pressure tipmanometer
the time taken for the changes to occur and resolve(table 1).During each of the four occlusions there were
ischaemia-induced changes in the pressure derivedindices, with a more pronounced change in Vmax,Tau,, and + dP/dt during the two occlusions perfor-med with retroperfusion.
Patient 2-A 63 year old man was readmitted withchest pain at rest after a small anterior non-Q wavemyocardial infarction. The pain was associated withanterior ST depression and T wave inversion.Coronary angiography showed an occluded rightcoronary artery and a severe proximal stenosis in theleft anterior descending artery; it was thereforedecided to proceed to coronary angioplasty. Atangioplasty two 54 second inflations were performedbefore retroperfusion and one 174 second and one 54second inflation were performed during retroper-fusion. The maximal inflation pressure was 10atmospheres. There was ST depression of 0 1 mV atthe end of the first inflation, but not during thesecond inflation. The first inflation with retroper-fusion was increased to 174 seconds, with the patientcomplaining of mild pain shortly after 30 seconds.There was no progression to severe chest pain duringthe procedure and only slow progression in STchange-0 1 mV at 70 s and 0-2 mV at 140 seconds.
i ,(mV)
1 gX 0 t 1100
i ~~~~~~~~~~~~(mmHg)
LV pressure [100column &('PLmmHg)
Retroperfusionflow
'nn' ~~~nn r150L.. . . . I(.JU L0(ml/min)
Baseline Control Control Occlusion Occlusionocclusion occlusion with SRP with SRP
1 2 1 2
Fig 2 Left ventricular pressure and surface electrocardiograms in patient 1 before thefirst occlusion, at the end of the twocontrolled occlusions, and at the end of the two occlusions with synchronised retroperfusion (SRP). The retroperfusion flowtracing (b) shows the magnitude of theflow and the timing in relation to the cardiac cycle. The ST changes in lead V5 and thechanges in left ventricular pressure were similar for thefour occlusions.
162
on 16 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.59.2.159 on 1 F
ebruary 1988. Dow
nloaded from
Coronary sinus retroperfusion during PTCA
A-~~~~~~~~~-*
A~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~A0A 4~~~~~~~~~~~~~~~~~~~~~~~~~~~~ A3,.
A~~~
AdP/dt
\A.A~~~~~~~.*_0
0 - dP/dt
200 300Time after occlusion (s)
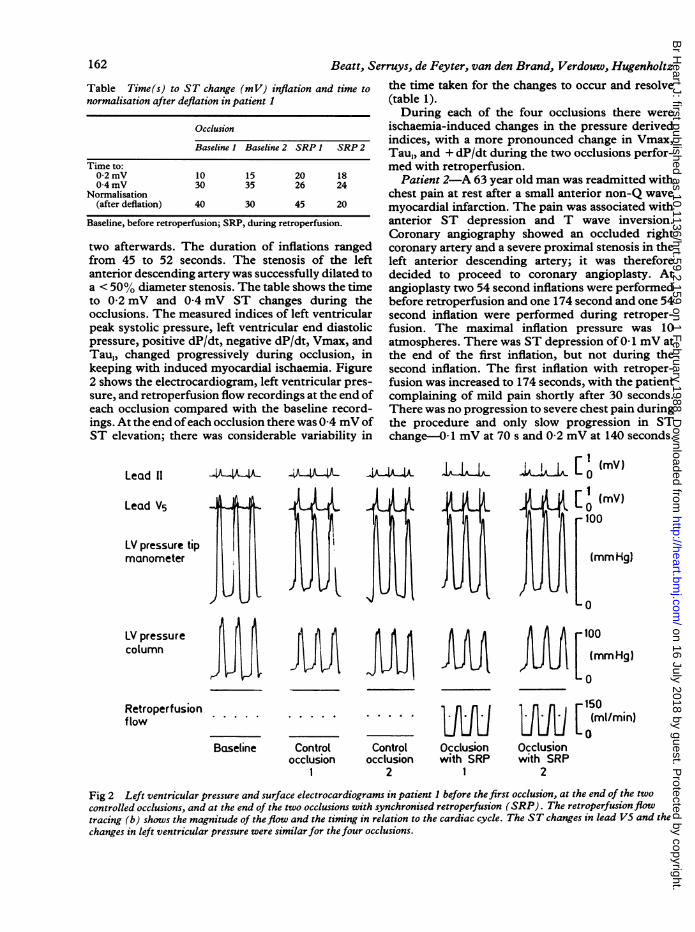
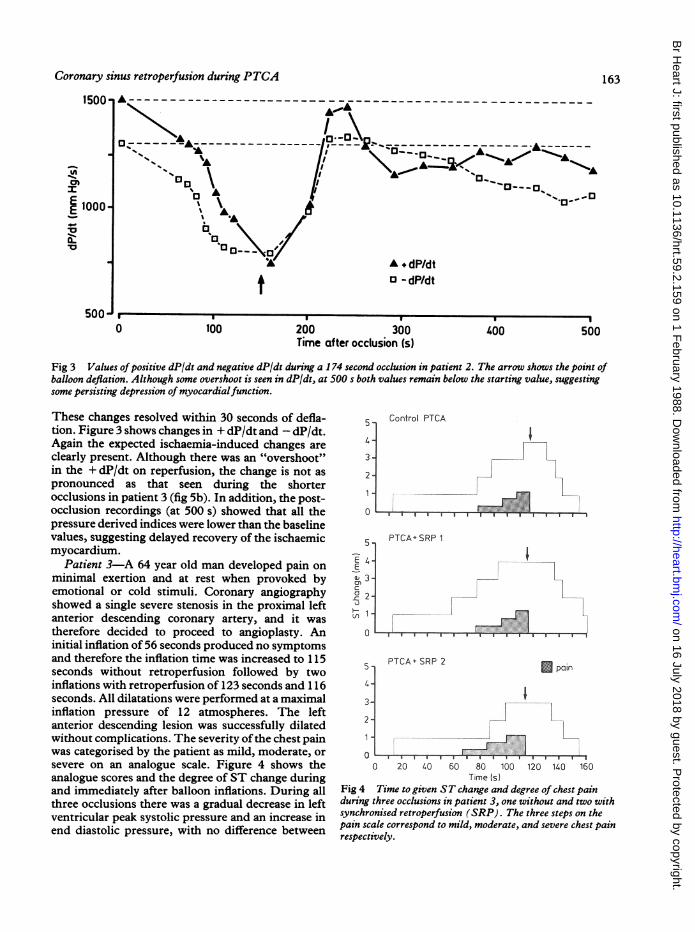
Fig 3 Values ofpositive dP/dt and negative dP/dt during a 174 second occlusion in patient 2. The arrow shows the point ofballoon deflation. Although some overshoot is seen in dP/dt, at 500 s both values remain below the starting value, suggestingsome persisting depression of myocardialfunction.
These changes resolved within 30 seconds of defla-tion. Figure 3 shows changes in + dP/dt and - dP/dt.Again the expected ischaemia-induced changes areclearly present. Although there was an "overshoot"in the + dP/dt on reperfusion, the change is not aspronounced as that seen during the shorterocclusions in patient 3 (fig 5b). In addition, the post-occlusion recordings (at 500 s) showed that all thepressure derived indices were lower than the baselinevalues, suggesting delayed recovery of the ischaemicmyocardium.
Patient 3-A 64 year old man developed pain onminimal exertion and at rest when provoked byemotional or cold stimuli. Coronary angiographyshowed a single severe stenosis in the proximal leftanterior descending coronary artery, and it wastherefore decided to proceed to angioplasty. Aninitial inflation of 56 seconds produced no symptomsand therefore the inflation time was increased to 115seconds without retroperfusion followed by twoinflations with retroperfusion of 123 seconds and 116seconds. All dilatations were performed at a maximalinflation pressure of 12 atmospheres. The leftanterior descending lesion was successfully dilatedwithout complications. The severity ofthe chest painwas categorised by the patient as mild, moderate, orsevere on an analogue scale. Figure 4 shows theanalogue scores and the degree of ST change duringand immediately after balloon inflations. During allthree occlusions there was a gradual decrease in leftventricular peak systolic pressure and an increase inend diastolic pressure, with no difference between
5
4a
3
2
5
E ,L
tocD 3-
2
u tI.
Control PTCA
I
PTCAfSRP 1I
PTCA SRP 25a
3-
2
*P
0 20 4O 60 80 100 120 11.0 160Time (s)
Fig 4 Time to given ST change and degree of chest painduring three occlusions in patient 3, one without and two withsynchronised retroperfusion (SRP). The three steps on thepain scale correspond to mild, moderate, and severe chest painrespectively.
1500
E 1000
50
500
0
t100 400 500
I I 5
I I
II
163
I
on 16 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.59.2.159 on 1 F
ebruary 1988. Dow
nloaded from
Beatt, Serruys, de Feyter, van den Brand, Verdouw, Hugenholtz
(x 1000)
I40
E@ 30-
L.20-3
0
1-
U'
a10-
c0Ci
0 20 40 60 80 100 120Time (s)
'aat
(x 1000)3.-
140 160 180 200 0 20 40 60 80 100 120 110 160 180 200Time (s)
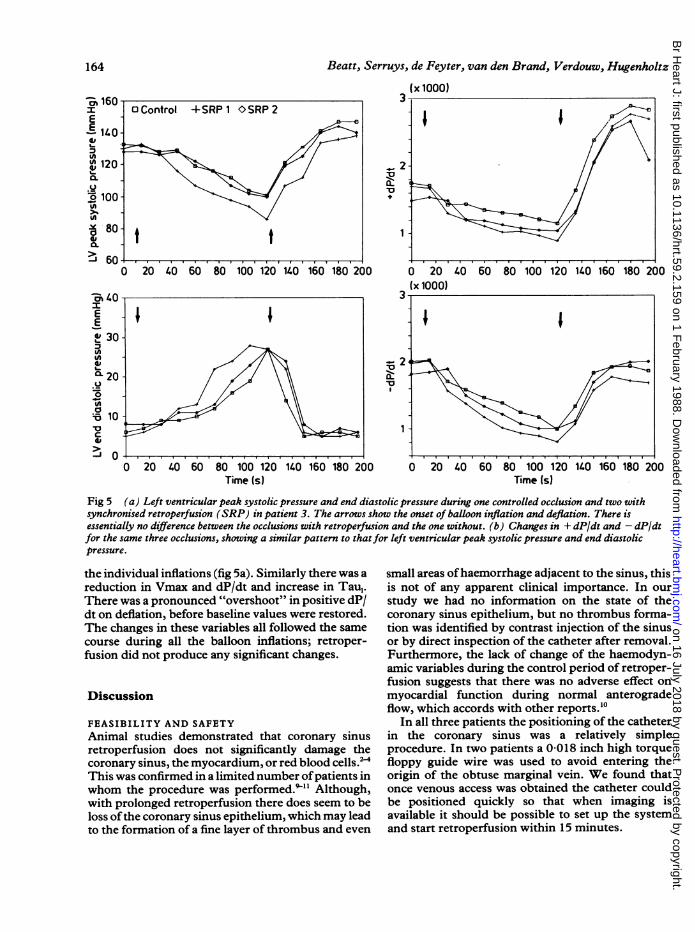
Fig 5 (a) Left ventricular peak systolic pressure and end diastolic pressure during one controlled occlusion and two withsynchronised retroperfusion (SRP) in patient 3. The arrows show the onset of balloon inflation and deflation. There isessentially no difference between the occlusions with retroperfusion and the one without. (b) Changes in + dP/dt and - dP/dtfor the same three occlusions, showing a similar pattern to thatfor left ventricular peak systolic pressure and end diastolicpressure.
the individual inflations (fig 5a). Similarly there was a
reduction in Vmax and dP/dt and increase in Tau,.There was a pronounced "overshoot" in positive dP/dt on deflation, before baseline values were restored.The changes in these variables all followed the samecourse during all the balloon inflations; retroper-fusion did not produce any significant changes.
Discussion
FEASIBILITY AND SAFETYAnimal studies demonstrated that coronary sinusretroperfusion does not significantly damage thecoronary sinus, the myocardium, or red blood cells.'2This was confirmed in a limited number ofpatients inwhom the procedure was performed."' Although,with prolonged retroperfusion there does seem to beloss ofthe coronary sinus epithelium, which may leadto the formation of a fine layer of thrombus and even
small areas ofhaemorrhage adjacent to the sinus, thisis not of any apparent clinical importance. In our
study we had no information on the state of thecoronary sinus epithelium, but no thrombus forma-tion was identified by contrast injection of the sinusor by direct inspection of the catheter after removal.Furthermore, the lack of change of the haemodyn-amic variables during the control period of retroper-fusion suggests that there was no adverse effect on
myocardial function during normal anterogradeflow, which accords with other reports.'0
In all three patients the positioning of the catheterin the coronary sinus was a relatively simpleprocedure. In two patients a 0-018 inch high torquefloppy guide wire was used to avoid entering theorigin of the obtuse marginal vein. We found thatonce venous access was obtained the catheter couldbe positioned quickly so that when imaging isavailable it should be possible to set up the systemand start retroperfusion within 15 minutes.
I
I~~~~~~~~~~~~~~~~~~~
I I I II I I
164
'O.-- 2 4
a: II
1
I I
on 16 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.59.2.159 on 1 F
ebruary 1988. Dow
nloaded from

Coronary sinus retroperfusion during PTCAMETHOD OF ASSESSMENTThere is no consensus about the most appropriatemethod of assessing improvement in myocardialperfusion and function during retroperfusion. Meth-ods which have been used to demonstrate animprovement with retroperfusion in animals includethe measurement of cardiac output, electrocar-diographic change, regional and global left ven-tricular function by echocardiography, and postmor-tem assessment of myocardial ischaemia by intravas-cular indicators.We chose to assess the effect of synchronised
retroperfusion on myocardial ischaemia duringangioplasty in three ways: (a) by evaluating theseverity of chest pain and the length of arteryocclusion before pain; (b) by monitoring the surfaceand in one case the intracoronary electrocardiogram;(c) by monitoring the left ventricular pressure and thepressure derived indices.The assessment by the assessor and patient ofchest
pain in a stressed patient during an interventionalprocedure in which an experimental device is used isto some extent subjective. The use of an analoguescale may help to reduce this, but we believe that suchan assessment will remain crude and will only berelevant when there are large changes.ST change is widely used as an index of ischaemia
although the variability of this measurement in thecontext of repeated coronary occlusion withintracoronary injections has not been well validated.Intracoronary electrocardiographic recordings takenfrom the balloon guide wire which overlies the area ofischaemic myocardium provides a more reliablemeasurement,'5 although'there may still be somevariability when there are sequential arteryocclusions, where alterations in the resting mem-brane potential may give a false impression of STchange.'6 Perhaps the most reliable forms ofmeasurement, particularly in assessing myocardialfunction, are left ventricular pressure and pressurederived indices. Serruys et al showed that measuredchanges correlate well with changes in regional andglobal left ventricular function and provide a reliableindex for comparison during repeated episodes ofischaemia."'
EFFECTIVENESS OF PROCEDUREAn analysis of the individual's angina threshold andthe documented ST change during coronary arteryocclusion failed to show any consistent change dur-ing retroperfusion. Similarly, the change in leftventricular pressure and pressure-derived indicesshowed the predicted ischaemia-induced changeswith no reversal during retroperfusion. Althoughthere was a certain amount ofvariability in the time tochest pain and any given ST change the pressure-
165
derived indices were more consistent, suggesting thatthis is a more reliable method of assessment (figs 4and 5). Several animal studies showed that retroper-fusion can be effective in improving myocardialischaemia and reducing infarct size. In our study wefailed to show any convincing benefit of retroper-fusion during acute myocardial ischaemia. There areseveral reasons why there might be a discrepancybetween animal and human studies, and among thesemust be the suitability of the given animal model.The results from canine studies have generally beenmore favourable, than those in pigs.89 Thecapacitance and compliance of the human coronarysinus system is not known and it may be that thisquantity of injected blood is insufficient to create thevenocapillary gradient necessary to provide effectiveretroperfusion. The resting flow in the great cardiacvein varies from 40 to 99 ml/min at rest.'4 Animalstudies have shown that myocardial function isreduced if the resting flow falls by 20%, althoughsome benefit in terms of myocardial salvage may beretained even when flow rates are reduced by as muchas 70%. '" Even if only a proportion of a retrogradeflow rate of 160 ml/min reaches the myocardium wemight expect some improvement in function.Because the flow is limited to diastole, however, alarge amount of the delivered blood is "washed out"before it reaches the capillary bed.
In our animal studies (unpublished data) weachieved effective retroperfusion in some cases withhigh flow rates and high coronary venous pressuresby selective positioning ofthe catheter. In the presentstudy we confirmed the position ofthe retroperfusioncatheter in the great cardiac vein throughout theprocedure in all three patients and demonstratedretrograde flow. Figure 2 shows a hand injection of10 ml of contrast (not synchronised) producing clearvisualisation of the anterior cardiac vein, with blush-ing ofthe myocardium, particularly in the septal area.The addition of contrast to the retroperfused bloodduring the procedure, however, suggested that syn-chronised delivery was much less effective at produc-ing a myocardial blush, and it may be that higher flowrates will be necessary to achieve this. One ofthe veryimportant considerations ofusing higher flow rates isthe ability ofthe venous system to drain the increasedvolume of blood. In this report the comparativelyslow deflation of the autoinflatable balloon is aserious limitation, and is one of the areas that needfurther development.We feel that we performed appropriate monitoring
to detect any improvement in the ischaemic state ofthe myocardium. The ischaemic response to repeatedocclusion of the coronary artery may be variable; inparticular the response may become blunted withrepeated occlusions. By performing the occlusions
on 16 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.59.2.159 on 1 F
ebruary 1988. Dow
nloaded from
166 Beatt, Serruys, de Feyter, van den Brand, Verdouw, Hugenholtzwith retroperfusion after the control occlusions, anyimprovement in the ischaemic response due to animprovement in anterograde flow may have beenfalsely attributed to the retroperfusion. Left ven-tricular function as assessed by our haemodynamicmeasurements, however, showed no improvementduring occlusions with retroperfusion in any of ourpatients. Improvement in ischaemia may not be theonly potential benefit of retroperfusion. Mohl et alhave developed the concept of pressure-controlledintermittent coronary sinus occlusion,'920 in whichthe coronary sinus is occluded cyclically until apredetermined pressure is reached. Using the tech-nique they have shown that toxic metabolites arewashed out and his may be important in reducingthe extent of infarction, particularly if subsequentreperfusion takes place. It is possible that this featuremay also be a benefit of retroperfusion duringtransient ischaemia,2' but the limitations of ourmodel prevented us from assessing this.
FUTURE APPLICATIONSThe use of coronary sinus retroperfusion has beenproposed in several clinical settings includingmyocardial infarction and unstable angina, retroper-fusion of thrombolytic and antiarrhythmic drugs,and for cardioplegia. It is doubtful whether theprocedure will become widely used in myocardialinfarction and unstable angina because more effectiveforms of treatment with greater potential are becom-ing available. Of the other medical proposals, thedelivery of thrombolytic and antiarrhythmic agentsare unlikely to be substantially more effective thanintravenous administration and the additional timeand expense of retroperfusion may not be justified.
If retroperfusion can be shown to be effective,however, it could become a valuable aid to percutan-eous transluminal coronary angioplasty. It wouldpermit longer occlusions in general and would meanthat more critical lesions such as those ofthe left mainstem could be dilated with reduced risk ofmyocardialdamage. It could also be useful in salvaging myocar-dium in those procedures in which a total occlusionoccurs, by providing effective perfusion of theischaemic area while the patient is prepared forbypass surgery.We feel the weight of our current data precluded
the use of this technique in additional patients. Wehave, however, been able to identify potentialmodifications which should substantially improvethe current delivery system. It remains to be seenwhether improved techniques of anterograde per-fusion will make retroperfusion obsolete, but anyfuture clinical trial must be conducted in a controlledmanner and its conclusions must be based on reliableand reproducable indices of myocardial ischaemia.
We thank Ken Spector and Edward Winters for theirhelpful advice and help and Gusta Koster and Anjavan Huuksloot for their work in compiling this paper.
K J B is a recipient of the joint fellowship from theBritish and Netherlands Heart Foundations.
References
1 Beck CS, Stanton E, Batiuchok W, Leiter E. Revas-cularization of heart by graft of systemic artery intocoronary sinus. JAMA 1948;137:436-42.
2 Meerbaum S, Lang TW, Osher JV, et al. Diastolicretroperfusion ofacutely ischemic myocardium. Am JCardiol 1976;37:588-98.
3 Drury JK, Yamazaki S, Fishbein MC, Meerbaum S,Corday E. Synchronized diastolic coronary venousretroperfusion: results of a preclinical safety andefficacy study. J Am Coll Cardiol 1985;6:328-35.
4 Yamazaki S, Drury JK, Meerbaum S, Corday E.Synchronized coronary venous retroperfusion:prompt improvement of left ventricular function inexperimental myocardial ischemia. JAm Coll Cardiol1985;5:655-63.
5 Farcot JC, Berdeaux A, Guidicelli JF, Vilaine JP,Bourdarias JP. Diastolic synchronized retroperfusionversus reperfusion: effects on regional left ventricularfunction and myocardial blood flow during acutecoronary occlusion in dogs. Am J Cardiol 1983;51:1414-21.
6 Smith GT, Geary GG, Blanchard W, McNamara JJ.Reduction in infarct size by synchronized selectivecoronary venous retroperfusion of arterialized blood.Am J Cardiol 1981;48:1064-70.
7 Carlson CS, Ratajezyk-Pakalska E, Cogan JJ, RapaportE. Effect of venous retroperfusion on experimentalmyocardial ischemia in the open-chest pig. J Surg Res1985;38: 105-12.
8 Berk L, Scheets OL, Sassan MA, et al. On the timecourse of systolic myocardial wall thickening duringcoronary artery occlusion and reperfusion in theabsence and presence ofsynchronized diastolic coron-ary venous retroperfusion in anesthetized pigs. In:Mohl W, ed. Clinics of CSI. Darmstadt: SteinkopfVerlag, 1986:277-80.
9 Farcot JC, Berland J, Cribier A, Letac B, BourdariasJP. Diastolic synchronized retroperfusion in thecoronary sinus during percutaneous transluminalangioplasty: preliminary experience [Abstract]. Circ-ulation 1985;72(suppl III):470.
10 Gore JM, Weiner BH, Sloan KM, et al. Humanexperience with synchronized coronary sinusretroperfusion (SCSR): feasibility and safety [Abs-tract]. J Am Coll Cardiol 1986;7:151A.
11 Gore JM, Weiner BH, Benotti JR. Preliminaryexperience with synchronized coronary sinusretroperfusion in humans. Circulation 1986;74:381-8.
12 Meester GT, Bernard N, Zeelenberg C, Brower RW,Hugenholtz PG. A computer system for real timeanalysis of cardiac catheterization data. Cathet Car-
on 16 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.59.2.159 on 1 F
ebruary 1988. Dow
nloaded from
Coronary sinus retroperfusion during PTCA 167diovasc Diagn 1975;1:112.
13 Brower RW, Meis S, Serruys PW. A model of asyn-chronous left ventricular relaxation predicting the bi-exponential pressure decay. Cardiovasc Res 1983;17:462-8.
14 Serruys PW, Wijns W, van den Brand M, et al. Leftventricular performance, regional blood flow, wallmotion, and lactate metabolism during transluminalangioplasty. Circulation 1984;70:25-36.
15 Friedman PL, Shook TL, Kirshenbaum JM, SelwynAP, Ganz P. Value of the intracoronary electrocar-diogram to monitor myocardial ischaemia duringpercutaneous transluminal coronary angioplasty.Circulation 1986;74:330-9.
16 Vincent GM, Abildskov JA, Burgess MJ. Mechanismof ischemic ST segment displacement. Evaluation bydirect current recordings. Circulation 1977;56:559-66.
17 Verdouw PD, ten Cate FJ, Schamhardt HC, van derHoek TM, Bastiaans OL. Segmental myocardialfunction during progressive coronary flow reduction
and its modification by pharmacologic intervention.In: Weiss HW, ed. Advances in clinical cardiology.New York: Gerhard Witzrock, 1980:270-83.
18 Gallagher KP, Kumada T, Koziol JA, McKown MD,Kemper WS, Ross J Jr. Significance of regional wallthickening abnormalities relative to transmuralmyocardial perfusion in anesthetized dogs. Circu-lation 1980;62:1266-74.
19 Mohl W, Roberts AJ. Coronary sinus retroperfusionand pressure-controlled intermittent coronary sinusocclusion (PISCO) for myocardial protection. SurgClin North Am 1985;65:477-95.
20 Mohl W, Punzengruber C, Moser M, et al. Effects ofpressure-controlled intermittent coronary sinusocclusion on regional ischaemic myocardial function.J Am Coll Cardiol 1985;5:939-47.
21 Chang B, Drury K, Meerbaum S, et al. Enhancedmyocardial washout and retrograde blood deliverywith synchronised retroperfusion during acutemyocardial ischemia. J Am Coll Cardiol 1987;9:1091-8.
on 16 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.59.2.159 on 1 F
ebruary 1988. Dow
nloaded from