gynaecomastia
TRANSCRIPT

GYNAECOMASTIABY:
Dr PIRAH KORAIfcps-ii traineecmc larkana
Gynecomastia is the development of abnormally large mammary glands in males resulting in breast enlargement.
Gynaecomastia can happen in males of any age or weight.
Gynaecomastia is very common in boys going through puberty, happening in more than half of all normal adolescent males, and usually goes away over time. In older men, enlargement of the breast tissue happens in about one-third of men.
In about half of cases, enlargement is found in both breasts; in the other cases it only affects one breast.
Gynaecomastia can appear as a small lump that becomes tender as the mass becomes larger.
What is gynaecomastia?
Breast prominence due solely to excessive adipose is often termed
pseudogynaecomastia or sometimes lipomastia.
fat deposition without glandular proliferation, on exam fingers will not meet any resistance until they reach the nipple
What is Pseudogynaecomastia?

Gynecomastia has three peaks.
1. Infancy: 60-90% transient due to high maternal estrogen. Normally regresses over 2-3 week period.
2. Adolescence: 4-69% with wide variation due to examiner observation. Onset 10-12y/o and peaks 13-14y/o. Normally regresses w/in 18mo and persistence uncommon after 17y/o.
3. Older men: 24-65% with highest prevalence in the 50-80y/o.
Prevalence
Drugs: 10-25% (e.g: Digoxin, Furosemide, anabolic steroids, marijuana, opioids and excessive alcohol intake)
Idiopathic : 25% Persistent pubertal gynecomastia: 25% Cirrhosis or malnutrition: 8% Primary hypogonadism: 8% Testicular tumors: 3% Secondary Hypogonadism: 2% Hyperthyroidism: 1.5% Chronic renal insufficiency: 1%
Etiologies in patients seeking help for Gynecomastia

The basic mechanisms of gynecomastia include : 1.decrease in androgen production 2.an increase in estrogen production 3.increased availability of estrogen precursors for peripheral conversion to estrogen.
Androgen receptor blockade and increased binding of androgen to sex-hormone binding globulin (SHBG).
Estrogen-like or antiandrogen effects of Drugs
Pathophysiologic causes for Gynecomastia
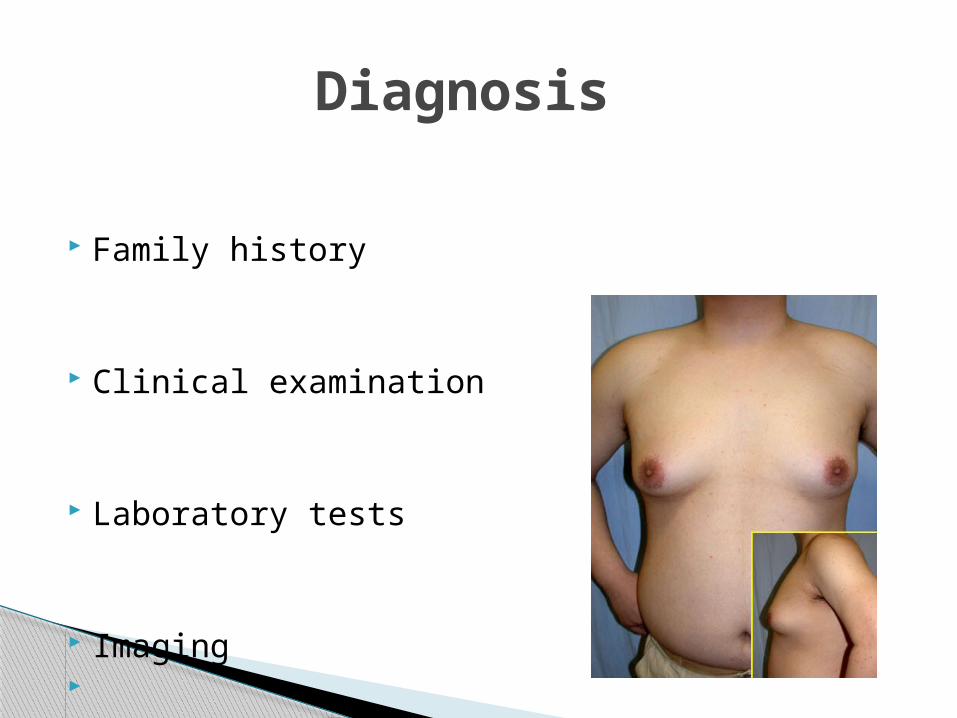
Family history
Clinical examination
Laboratory tests
Imaging
Diagnosis
◦Onset◦Bilateral/unilateral◦Pain◦Change in size◦Nipple discharge◦Drugs/medications◦PMH◦Family history
History

◦ Look for signs and sx of liver and kidney disease
◦ Evaluate for hyperthyroidism, eg. Weight loss, tachycardia, goiter, tremor, or exophthalmos.
◦ Seek for signs and sx that may suggest hypogonadism, eg. Impotence, decreased libido, strenght, and change in testicular size.
◦ Check for abdominal mass and testicular mass.
◦ Careful breast exam.
Complete Physical Exam
◦ if gynecomastia of recent onset, persistent, or painful/tender and has no clear physiologic etiology. BMP, LFT’s, TSH, LH, FSH, hCG, Prolactin, Estradiol,
Testosterone, Androstenedione
Imaging
◦ US and mammogram for any eccentric or discrete mass.
Laboratory tests

Treat the underlying cause
Watchful waiting
Medical options:
Androgens Anti-estrogens (as tamoxifen and
clomiphene)and aromatase inhibitors
Aromatase inhibitors such as Letrozole
TREATMENT
Liposuction
Gland excision
Skin sculpture
Reduction mammoplasty
Or a combination of these surgical techniques
Surgical options


Permanent numbness, compromise of blood supply, irregular contour, hematoma, seroma, wound
infection
Complications
