guidelines for assistance to terminally ill children with cancer: a report of the siop working...
TRANSCRIPT

Guidelines for Assistance to Terminally Ill Children With Cancer: A Report ofthe SIOP Working Committee on Psychosocial Issues in Pediatric Oncology
Giuseppe Masera, MD,1* John J. Spinetta, PhD,2 Momcilo Jankovic, MD,1
Arthur R. Ablin, MD,3 Giulio J. D’Angio, MD,4
Jeanette Van Dongen-Melman, PhD,5 Tim Eden, MD,6
Antonio Gentil Martins, MD,7 Ray K. Mulhern, PhD,8
Daniel Oppenheim, MD, PhD,9 Reinhard Topf, PhD,10 and Mark A. Chesler, PhD11
This, the sixth official document of the SIOPWorking Committee on psychosocial issues inpediatric oncology, develops another importantand especially difficult topic: assistance for ter-minally ill children with cancer. This is pro-vided for the pediatric oncology community asa useful set of guidelines. It should be alwayspossible for a declining child to die withoutunnecessary physical pain, fear, or anxiety. It is
essential that he or she receive adequate medi-cal, spiritual, and psychological support, andthat the child at no point feels abandoned. Pal-liative care, in the terminal phase of cancer,should be tailored to the different needs anddesires of the child and the family, with the goalof providing the best possible quality of life forthe days that remain. Med. Pediatr. Oncol. 32:44–48, 1999. © 1999 Wiley-Liss, Inc.
Key words: palliative care; death and dying; childhood cancer; psychosocial issues
INTRODUCTION
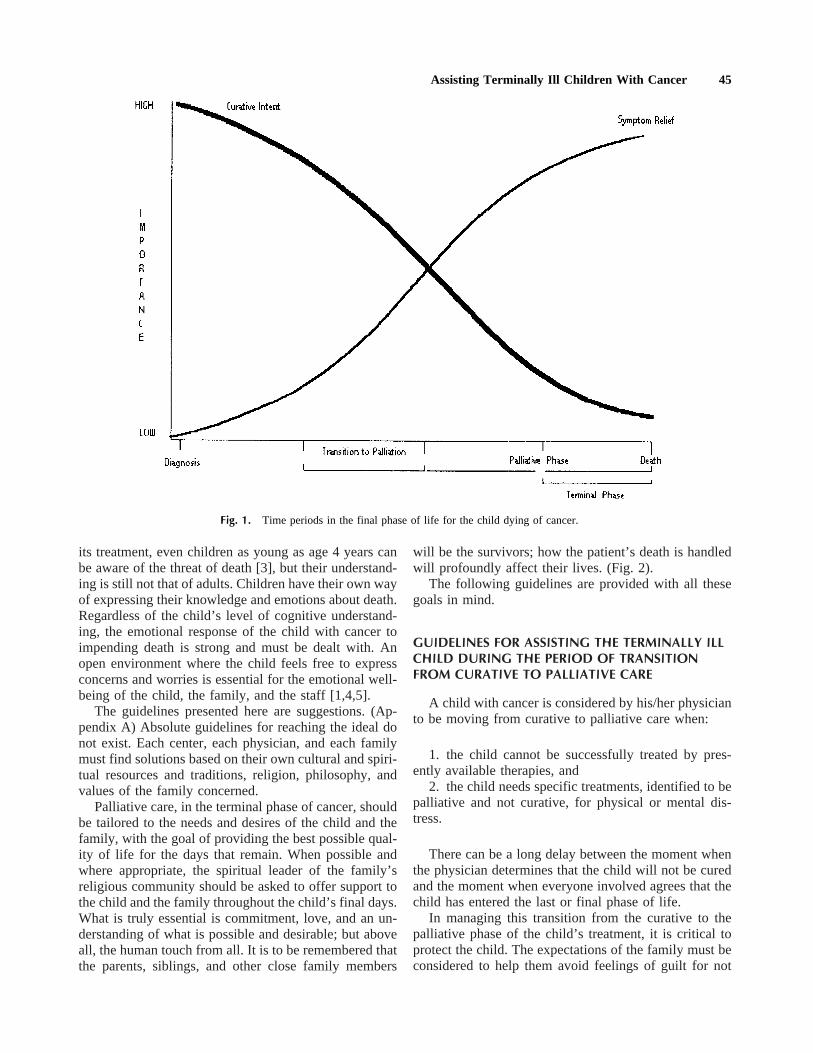
These guidelines refer to two time periods in the finalphase of life for the child dying of cancer. The first is theperiod when treatment is judged to be no longer effectiveand the difficult decision must be made by all concernedto move from curative intent to the palliative phase ofcare. The second is the period from the beginning ofpalliative care to the death of the child.
Key issues during these phases are the duration andquality of remaining life, and the rights of the child tocareful, compassionate management. This must includethe best palliative care the staff can provide.
It should be always possible for a terminally child todie without unnecessary physical pain, fear, or anxiety.Whatever the state of the child entering the terminalphase of the illness (Fig. 1), it is essential that he or shereceive adequate medical, spiritual, and psychologicalsupport; and that the child at no point feels abandonedeither by the health center or by his/her family.
The task of helping a child pass through and into theterminal phase of an illness is extremely trying both froman emotional and practical point of wiew. The personal,philosophical, and cultural values of the family and thehospital health care team members all influence whathappens. The staff members should be especially awareof their own personal stance on each of these underlyingvalues (while being careful not to impose them uponfamilies).
Until preadolescence, children, in general, understand
death at a level different from adults. However, childrenwith cancer often reach an understanding of what deathmeans at a much younger age than their healthy peers[1,2]. As a result of their experience with the illness and
1Clinica Pediatrica dell’Universita` di Milano, Ospedale S. Gerardo,Monza, Italy2Department of Psychology, San Diego State University, San Diego,California3Department of Pediatrics, University of California, San Francisco,California4Department of Radiation Oncology, University of Pennsylvania,Philadelphia, Pennsylvania5Department of Pediatrics, Sophia Children’s Hospital, UniversityHospital, Rotterdam, The Netherlands6Department of Pediatric Oncology, Christie Hospital and RoyalManchester Children’s Hospital, Manchester, United Kingdom7Instituto Portugues de Oncologia de Francisco Gentil, Lisbon, Portu-gal8Division of Behavioral Medicine, St. Jude Children’s Research Hos-pital, Memphis, Tennessee9Department de Pe´diatrie et Unitede Psychooncologie, Institut Gus-tave Roussy, Villejuif, France10Department of Pediatric Oncology, St. Anna Kinderspital, Vienna,Austria11Department of Sociology, University of Michigan, Ann Arbor,Michigan
*Correspondence to: Giuseppe Masera, Clinica Pediatrica dell’Uni-versitadi Milano, Ospedale S. Gerardo, 20052 Monza, Italy.
Received 7 April 1998; Accepted 1 June 1998
Medical and Pediatric Oncology 32:44–48 (1999)
© 1999 Wiley-Liss, Inc.
its treatment, even children as young as age 4 years canbe aware of the threat of death [3], but their understand-ing is still not that of adults. Children have their own wayof expressing their knowledge and emotions about death.Regardless of the child’s level of cognitive understand-ing, the emotional response of the child with cancer toimpending death is strong and must be dealt with. Anopen environment where the child feels free to expressconcerns and worries is essential for the emotional well-being of the child, the family, and the staff [1,4,5].
The guidelines presented here are suggestions. (Ap-pendix A) Absolute guidelines for reaching the ideal donot exist. Each center, each physician, and each familymust find solutions based on their own cultural and spiri-tual resources and traditions, religion, philosophy, andvalues of the family concerned.
Palliative care, in the terminal phase of cancer, shouldbe tailored to the needs and desires of the child and thefamily, with the goal of providing the best possible qual-ity of life for the days that remain. When possible andwhere appropriate, the spiritual leader of the family’sreligious community should be asked to offer support tothe child and the family throughout the child’s final days.What is truly essential is commitment, love, and an un-derstanding of what is possible and desirable; but aboveall, the human touch from all. It is to be remembered thatthe parents, siblings, and other close family members
will be the survivors; how the patient’s death is handledwill profoundly affect their lives. (Fig. 2).
The following guidelines are provided with all thesegoals in mind.
GUIDELINES FOR ASSISTING THE TERMINALLY ILLCHILD DURING THE PERIOD OF TRANSITIONFROM CURATIVE TO PALLIATIVE CARE
A child with cancer is considered by his/her physicianto be moving from curative to palliative care when:
1. the child cannot be successfully treated by pres-ently available therapies, and
2. the child needs specific treatments, identified to bepalliative and not curative, for physical or mental dis-tress.
There can be a long delay between the moment whenthe physician determines that the child will not be curedand the moment when everyone involved agrees that thechild has entered the last or final phase of life.
In managing this transition from the curative to thepalliative phase of the child’s treatment, it is critical toprotect the child. The expectations of the family must beconsidered to help them avoid feelings of guilt for not
Fig. 1. Time periods in the final phase of life for the child dying of cancer.
Assisting Terminally Ill Children With Cancer 45
having done everything possible. However, a real di-lemma is created for everyone if aggressive therapy iscontinued when the possibilities of cure are virtually notexistent.
With these caveats in mind, we suggest the followingguidelines for an effective assistance program during thetime of transition from the curative to the palliativephase.
1. Each center should develop a uniform philosophyon key issues (e.g., communication, support, pain con-trol) regarding the final phases of care for the dyingchild, producing local recommendations regarding treat-ment and care based on group discussion.
2. Along with the extended health care team, the par-ents of the child and the family physician should beinvolved in the decision-making process from the verybeginning of treatment throughout the course of the dis-ease, and most especially at the point of transition to theterminal phase. All members of the health care teamshould continuously be updated on the course of treat-ment. The decision to move from the intent to cure topalliative care should be made with the parents and thefull health-care team, certainly including the nurses. De-pending on age and level of development, the childshould also be involved in the decision, with older chil-dren especially participating more actively. The childshould know as much as possible and developmentallyappropriate about the seriousness of his/her situation.However, if the child wishes to remain less informed, thiswish should be respected, and whatever information isgiven should allow the child to retain a margin of hope.
3. Parental wishes may not always be in the best in-terest of the child. The parents may wish to shield thechild, which may only make the patient’s fear worse.Also, a conflict may arise when the family wishes tocontinue pursuing an unrealistic possibility of cure or, onthe contrary, when the family wishes to stop curativetreatment prematurely. When members of the health-careteam take time to try to understand and discuss the rea-sons for the family’s wishes, the inevitably painful con-flicts can usually be overcome.
4. The continuation of curative treatment beyond thepoint when cure is no longer possible should be avoided(the so-called ‘‘ruthless obstinacy’’ treatment).
GUIDELINES FOR ASSISTING THE TERMINALLY ILLCHILD DURING THE PERIOD OF PALLIATIVE CAREAND FOR ASSISTING THE FAMILY AFTER DEATH
The following are suggested as guidelines for the ter-minal phase of care, once the decision to move from thecurative to the palliative phase of treatment has beenmade and agreed upon by parents, competent siblings(when they have been involved in decision-making dur-
ing therapy), the child (as appropriate for age), and theextended health care team.
1. Medical decisions regarding palliative care shouldbe made by consultation within the comprehensive ‘‘car-ing’’ team and not by one physician acting alone. Whena group decision has been made that curative treatmentshould be discontinued and palliative care initiated, thecontrol of physical and psychological pain becomes para-mount. Physical pain control must be carried out withprofessional competence. The team must also control allother emerging symptoms, e.g., vomiting, constipation,bladder control.
2. Children who wish to stay at home should be al-lowed to do so whenever it is possible; the parents andthe children themselves should remain the ultimate arbi-ters in this decision. Some parents do not wish to havetheir child die at home. For those families that decide todo so, the physician should insure continual support ei-ther directly or through the use of other supportive ser-vices, depending on cultural customs and resources (e.g.,home care unit, hospice, visiting nurses).
Fig. 2. Sculpture by Rodin (1840–1917) of ‘‘The Mother and HerDying Son.’’
46 Masera et al.
3. The parents and the health-care team membersshould be attuned to the child in the terminal phase, andshould reflect on what the child communicates, both ver-bally and nonverbally. (Appendix B)
4. During the palliative phase of care, follow-up visitsand telephone calls by the physician should be offered tothe parents whose child is dying at home, so that theynever feel abandoned.
5. There should be bereavement counselling after thechild’s death on the part of the physicians and nursesconcerned to help clarify past care and help guide futuregrieving [6]. Parents (and when appropriate, siblings)should be invited to discuss with the physician both thelevel of care given to the child and the surviving familymembers’ present needs. Follow-up and counselling ses-sions for surviving siblings should be offered and pur-sued actively if accepted. Participants should be preparedto hear and deal with anger, accusations, and fault-finding during these sessions, especially shortly after thedeath.
6. Health-care teams should encourage bereaved par-ents and siblings to initiate self-help groups. Concernedfamily members should be enabled to discuss the psy-chosocial issues raised by the treatments and by the deathof the child, and for sharing their mourning and griefwith others. If necessary, professional psychological helpshould also be offered to those parents who feel the need.Routine contact with the family for at least 2 years onsignificant anniversary dates (e.g., birthday of patient,diagnosis, death, holidays) is often welcomed and ac-cepted as a manifestation of a continuing committment ofthe team to the psychologic health and well-being of thefamily.
7. After a child dies, that individual child’s medicalhistory should be evaluated. This evaluation should bemade by the health-care team as a group. It is very im-portant to reflect on all events, even minor ones, thatoccurred during the course of the child’s treatment. It iscritical to reflect on the choices that were made and why,in order to help the staff come to terms with their owngrieving and to learn from the experience in order to helpfuture families.
8. The center’s health-care team should be preparedto modify its overall philosophical goals and reset direc-tions and guidelines when appropriate, based on suchreview of individual cases and parental comments.
ACKNOWLEDGMENTS
We are grateful to the following for their valued con-tributions on this topic during general discussions: C.Epelman (Campinas, Brazil), M. Lo Curto and G. Fu-gardi (Palermo, Italy), W. Ben Arush (Haifa, Israel), M.Vaimmungum (Durban, South Africa), K. Sirkia’ (Hel-sinki, Finland), H. Kosmidis (Athens, Greece), K. Pe-
kkanen (Go¨teborg, Sweden), C. Dias and C. Tanaka (SaoPaulo, Brazil), H.P. Moe (Trondheim, Norway), J. Babic(Ljubjana, Slovenia), L. Hovi (Helsinki, Finland), L.S.Arya (New Delhi, India), C. Hendriks (Amsterdam, TheNetherlands), N. Platin (Ankara, Turkey), C. Lingner(Vienna, Austria), J. Challinor (San Francisco, CA), J.Kowalczyk (Warsaw, Poland), M.J. De Clercq (Ghent,Belgium), C. Freidank (Marburg, Germany), and L.Puukko (Helsinki, Finland).
REFERENCES
1. Spinetta JJ. The dying child’s awareness of death: A review. Psy-chol Bull 1974;81:841–845.
2. Waechter EH. Children’s awareness of fatal illness. Am J Nurs1971;71:1168–1172.
3. Bluebond-Lagner M, editor. The private worlds of dying children.Princeton, NJ: Princeton University Press; 1978.
4. Spinetta JJ, Maloney LJ. Death anxiety in the outpatient leukemicchild. Pediatrics 1975;56:1034–1037.
5. Lauer ME, Mulhern RK, Bohne JB, et al. Children’s perceptionsof their sibling’s death at home or hospital: the precursors ofdifferential adjustment. Cancer Nurs 1985;2:21–27.
6. Jankovic M, Masera G, Uderzo C, et al. Meetings with parentsafter the death of their child from leukemia. Pediatr HematolOncol 1989;6:155–160.
APPENDIX A: SUMMARY OF ESSENTIALRECOMMENDATIONS FOR ASSISTING TERMINALLYILL CHILDREN AND THEIR FAMILIES
1. Develop a uniform policy and approach within thecenter.
2. Reach a group decision with the entire health-careteam about a specific plan of palliative care best for eachindividual child.
3. Avoid a ‘‘ruthless obstinacy’’ approach; knowwhen to move from cure-oriented therapy to palliativecare.
4. Listen to the child, keep in touch with the family,and try to develop and retain a good relationship witheveryone involved.
5. Include in the final decision-making process theparents, the siblings and the child (depending on theirages and level of development), and the local familyphysician.
6. Control both physical and psychological pain aswell as other disturbing symptoms.
7. Enable the child to die at home when possible andif desired by the patient and the family.
8. Deal with issues of bereavement among the mem-bers of the health-care team.
9. Encourage postdeath follow-up visits for parentsand siblings, reflecting on the medical history of the childand acknowledging the ongoing needs of parents, sib-lings, and other family members (e.g., grandparents).
Assisting Terminally Ill Children With Cancer 47

APPENDIX B: TENDERNESS(By a dying child, Marcello, 7, to his mother)
I see your eyeslike fireslit in the night;they’ve criedthey’ve lovedthey’ve laughed,these eyes of yours.They’re lovingthey’re purethey’re sincerelike my special toy.I love themI feel themimprinted in my heart,these eyes of yours.Today I find themtired, yes...but as alwaystenderBelieve me, mom.
48 Masera et al.