guide to gastrostomy tubes - rchsd.org · guide to gastrostomy tubes - page 7. gastrostomy tubes...
TRANSCRIPT
Guide
Guide to Gastrostomy TubesC Rady Children’s Hospital, San Diego 2011
Reviewed October 2017
Introduction ………………………………………………………….....…………......…
Important Contact Information ……………………………………....…..........................
G-Tube & Feeding Information …………...............………….……………................….
Important Facts & When to Call the Doctor…………………………….....……..........…
Anatomy of Digestive System ………………………………………..…….…....………
Nissen Fundoplication Surgery ………………………………………………...…...……
Low Profile G-Tube (Mic-Key Button) ……..………......……….............................................
G-Tube (G-Tube) .........…….……………......………………..…................…….....……....
Care of Tube and parts ............................……………….............……….…............…..…
Daily Skin Care ………………......................................…………………....….....………
Placement checking/Venting and Feeding …………….…………………………………..
Medication Facts ....................................................................................................................
Tube Dislodgement and Balloon Facts…………………….…………………..…….....…
Going Home/ Travel Kit ………………….………………………………………....……
Medical Glossary ...................................................................................................................
Problem solving and common questions…………………………………….…….........…
Recommended Reading/Caregiver Support ...........................................................................
Caregivers Notes .....................................................................................................................
i
1
2
4
6
7
9
12
15
18
20
25
35
39
43
44
48
49
Table of Contents

Dear Parents and Caregivers,
As your child prepares to have a gastrostomy tube placed (also called g-tube), we realize that you will have many questions about the procedure and how it will affect your child’s life. This journal will give you important facts about your child’s g-tube surgery and care. The journal also reviews all areas of care your child will need following a g-tube placement. We believe your child deserves personalized care and you may find that some of your child’s care will differ from what is in this journal. It is important to always follow your child’s Physician or Surgeons plan.
We hope that this journal covers most of your questions and concerns. Our nurses, doctors, occupational therapists and all specialty teams are available to answer any other questions you may have. Do not hesitate to seek further information at any time!
When your child is discharged from the hospital, our Home Care team will help you learn to care for your child at home. There may be a few differences between your hospital routine and your home routine. There may also be some differences between supplies you will use while in the hospital and at home. Your Home Care team will be there to support, guide and instruct you in all areas.
At Rady Children’s Hospital, our goal is to work together as a team of surgical, medical, nursing, specialty groups and - most importantly - caregivers and children. We are here to provide you with the highest level of care for your child and ensure that you are fully informed and involved with all areas of care.
Sincerely,
Tips and Tubes Committee 2014Rady Children’s Hospital
Guide to Gastrostomy Tubes - Page i
Important Contact Information
If your child’s tube falls out on the weekend or outside of office hours, call Rady Children’s Hospital at (858) 966-1700. Ask for the on-call GI Physician/Surgeon.
Rady Children’s Hospital–San Diego3020 Children’s Way. San Diego, CA 92123Emergency Department Number: (858) 966-8005Rady Children’s Gastroenterology (GI) Services: (858) 966-4003Rady Children’s Gastroenterology (GI) Clinic & Nurse Specialist: (858) 966-1700 x. 5606 Rady Children’s Hospital - Main Number: (858) 966-1700Rady Children’s Occupational/Physical Therapy: (858) 966-5829Rady Children’s Referral Service: (800) 788-9029 or (858) 966-4096Rady Children’s Outpatient Pharmacy: (858) 966-4060Rady Children’s Home Care: (858) 966-4941Rady Children’s Hospital Website: www.RCHSD.org
GI Surgeon’s Name: __________________________ Phone # ______________________
GI Physician’s Name: _________________________ Phone # ______________________
Primary Care Physician (PCP) Phone #:__________________________
Home Pharmacy Phone #: ____________________________________
Home Care Phone #: ________________________________________
Medical Insurance Phone # __________________________________
Notes_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
Guide to Gastrostomy Tubes - Page 1
Personal G-Tube Information
Please follow the time guides below as to when you can place an emergency tube. It is important that you contact your child’s GI Surgeon/Physician before inserting an emergency tube if your child has had the tube for less than 12 weeks. Always contact your child’s GI Surgeon/Physician or Nurse Specialist if you have any concerns regarding the fit of your child’s tube.
Date of surgery or Tube placement: _______________________________________________________
Date Emergency Red Robin Tube can be inserted (6 weeks after surgery): ________________________
Date Emergency G-Tube can be inserted (6 weeks after surgery): _______________________________
Date when Emergency balloon check start (6 weeks after surgery): ______________________________
Type and brand of G-Tube: _____________________________________________________________
Size of low profile G-Tube (Mic-Key Button): ______________ French ______________ cm
Size of G-Tube: ______________ French
Size of red robin tube: ______________ French
Length Red Robin Tube to be inserted: ___________________ inches
Balloon volume: ____________ ml
Day of week extension tube to be changed: ______________________
Guide to Gastrostomy Tubes - Page 2
My Child’s Feeding Schedule
Only feeding formulas and medications that have been ordered by your child’s Physician, Dietician or Occupational Therapist should be given through the g-tube.
Type of feed: ______________________________________________________________
Special formula preparation Recipe: _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Day-time feeding schedule: ____________________________________________________________________________________________________________________________________________________________________________________________________
Night-time feeding schedule: ___________________________________________________________________________________________________________________________________________________________________________________________________
Daytime: _____________ ml per hour (pump program) Overnight: ____________ ml per hour (pump program)
Notes_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
Guide to Gastrostomy Tubes - Page 3
Important Gastrostomy Facts
1. If your child develops breathing difficulties during or immediately after feeding, stop the feeding immediately. Attach a 60 ml syringe to the extension or g-tube and place at a lower level than the stomach allowing gravity to empty stomach contents (see Pg. 21). Call 9-1-1 immediately if breathing difficulties continue.
2. Always keep your child’s travel kit with him/her. (Check Red Robin Tube and a Mic-Key Button Tube is inside).
3. If the original tube falls out during the first 6 weeks after surgery, cover the stoma (hole) with gauze, call your child’s GI Surgeon/Physician, and take your child to the Emergency Department immediately (take your travel kit with you).
4. If your child’s tube falls out more than 6 weeks after surgery call your child’s GI Surgeon/Physician. If you have been trained to insert a red robin tube or a mic-key button tube they may ask you to insert a new one. Do not force the tube into the stoma. Once tube is inserted, your child’s GI Surgeon/Physician will give you follow up instructions.
5. Never give feeds or medications through a red robin tube (this is a temporary tube). Never give feeds or medication through an emergently inserted g-tube if it is less than 12 weeks after surgery unless instructed to do so by your child’s Surgeon/Physician.
6. If your child’s tube starts to feel loose or there is increased leaking of fluid around the tube during the first 6 weeks after surgery, call your child’s GI Surgeon/Physician for instructions.
7. If your child’s tube feels loose or there is increased leaking of fluid around tube more than 6 weeks after surgery, you can check the balloon volume if you have been trained by a member of the hospital staff (see Pg. 10 /13). If more water needs to be added to the balloon call your child’s GI Surgeon/Physician for follow up. Only use sterile water (see Pg. 17) or distilled water to inflate the balloon.
8. Only feeding formulas and medications that have been ordered by you child’s Physician, Dietician or Occupational Therapist should be given through the G-Tube.
9. Rotate the mic-key button tube/g-tube 1/4 to 1/2 circle once a day if instructed to do so by hospital staff. Important: Never rotate a tube that has sutures inserted to hold it in place.
10. Remove all feeding bags and extension tubes after every feed and clean thoroughly.
11. If the g-tube falls out it is important that a new tube is inserted as soon as possible. (Follow instructions 3 and 4 on this page).
Guide to Gastrostomy Tubes - Page 4

When to Call Your Child’s Doctor
Complications with your child’s newly placed g-tube can be discussed with your child’s Primary Care Physi-cian (PCP), the GI clinic, or your child’s GI Physician or GI Surgeon. Once your child’s g-tube has been in place for a while, your child’s PCP or the GI clinic will be managing your child’s care. Please note that the
Nurse Practitioners in the GI clinic will be happy to help you address any question or concerns.
To reach your child’s Physician or Surgeon:(858) 966-1700, Ext. 0
and ask for your child’s physician or surgeon, or the GI physician or surgeon on call.
GI ServicesMain Clinic Phone Number: (858) 966-4003
GI Clinic & Nurse Specialist LineNurse Specialist Phone Number: (858) 966-1700, Ext. 5606
1. If the skin around the g-tube site feels warmer than normal, is sore to the or touch looks red.2. If there is fresh bleeding or puffy red tissue around your child’s g-tube site.3. If there is increased leaking around the g-tube site.4. If there is yellow or green drainage from the g-tube site that has a foul odor.5. If your child has vomiting, retching or diarrhea.6. If the feeding tube becomes blocked and you cannot remove the blockage.7. If your child has a fever over 101 degrees Fahrenheit, contact your child’s Primary Care Physician (PCP) first. 8. If there are any bloody secretions in the g-tube tubing. 9. If your child’s stomach remains full and swollen after venting, and he/she appears to have discomfort or pain.10. If your child’s g-tube falls out less than 12 weeks after insertion. 11. If you have difficulty inserting a replacement g-tube more than 12 weeks after insertion.
Guide to Gastrostomy Tubes - Page 5

Esophagus: carries food from the mouth to the stomach.
Stomach:is where food begins the process of digesting.
Duodenum: is the first part of the small intestines and lies just after the stomach.
Jejunum:is the middle of the small intestine.
Ileum: is the last part of the small intestine.
Large Intestine: is the final part of intestine.
Rectum and Anus: are where the waste products from the body come out.
Anatomy of the Digestive System
Stomach
Esophagus
Duodenum
Jejunum
Large Intestine
Rectum and Anus
Guide to Gastrostomy Tubes - Page 6
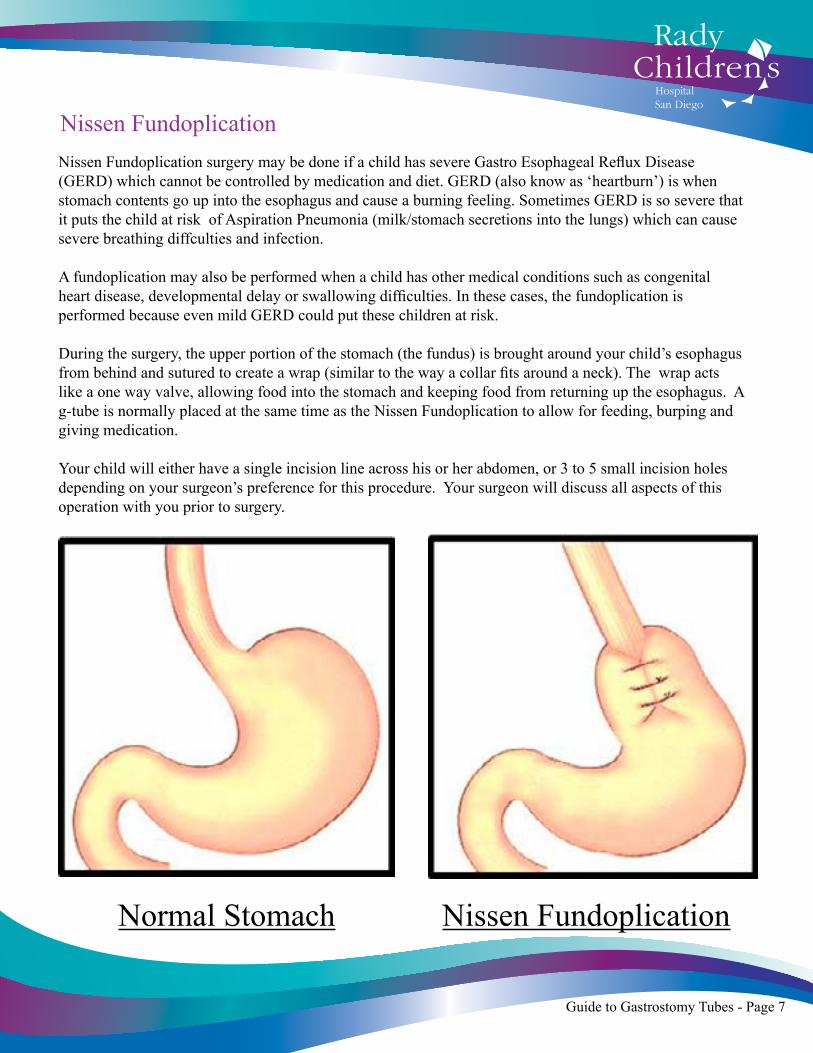
Nissen FundoplicationNissen Fundoplication surgery may be done if a child has severe Gastro Esophageal Reflux Disease (GERD) which cannot be controlled by medication and diet. GERD (also know as ‘heartburn’) is when stomach contents go up into the esophagus and cause a burning feeling. Sometimes GERD is so severe that it puts the child at risk of Aspiration Pneumonia (milk/stomach secretions into the lungs) which can cause severe breathing diffculties and infection.
A fundoplication may also be performed when a child has other medical conditions such as congenital heart disease, developmental delay or swallowing difficulties. In these cases, the fundoplication is performed because even mild GERD could put these children at risk.
During the surgery, the upper portion of the stomach (the fundus) is brought around your child’s esophagus from behind and sutured to create a wrap (similar to the way a collar fits around a neck). The wrap acts like a one way valve, allowing food into the stomach and keeping food from returning up the esophagus. A g-tube is normally placed at the same time as the Nissen Fundoplication to allow for feeding, burping and giving medication.
Your child will either have a single incision line across his or her abdomen, or 3 to 5 small incision holes depending on your surgeon’s preference for this procedure. Your surgeon will discuss all aspects of this operation with you prior to surgery.
Nissen FundoplicationNormal Stomach
Guide to Gastrostomy Tubes - Page 7

Gastrostomy tubes are inserted while your child is sedated under general anesthesia. A smallincision is made through the abdominal wall into the stomach. A tube is then inserted and held in place with a balloon which lies snug against the inside of the stomach wall. The tube may have some temporary sutures holding it in place for the first few days after surgery. Your child’s care can be discussed with the GI Surgeon or Physician before the surgery.
There are a few different types of gastrostomy tubes that can be used. Your child’s GI Surgeon or Physician will use the one that is the best fit for your child.
Gastrostomy Tube Placement
Esophagus
Stomach
G-Tube
Abdominal Wall
Guide to Gastrostomy Tubes - Page 8
StomachAbdominal
Wall
Esophagus
G- Tube

Low Profile Gastrostomy Tube (Mic-Key Button).
Mic-Key Button Tube Is small and easily hidden under clothing once the extension tube is removed between feeds. It lies flat against the skin and is held in place with an inflated balloon that lies snug against the inside stomach wall.
Mic-Key Button Extension TubeIs a detachable tube that attaches to the mic-key button for feeding, medications and venting. It can be removed from the mic-key button base when not in use. This tube should be removed after each feed and cleaned.
Feeding Port
Guide to Gastrostomy Tubes - Page 9
Balloon
Balloon Port
FeedingPort
Medication Port
Secur-lock Connector
Feeding Port
Clamp
Mic-Key Button Bolus Extension TubeIs a detachable tube that attaches to the mic-key button for bolus feeds, medications and venting. This tube should be removed after each feed and cleaned.
Feeding Port
Clamp
Secur-lock Connector
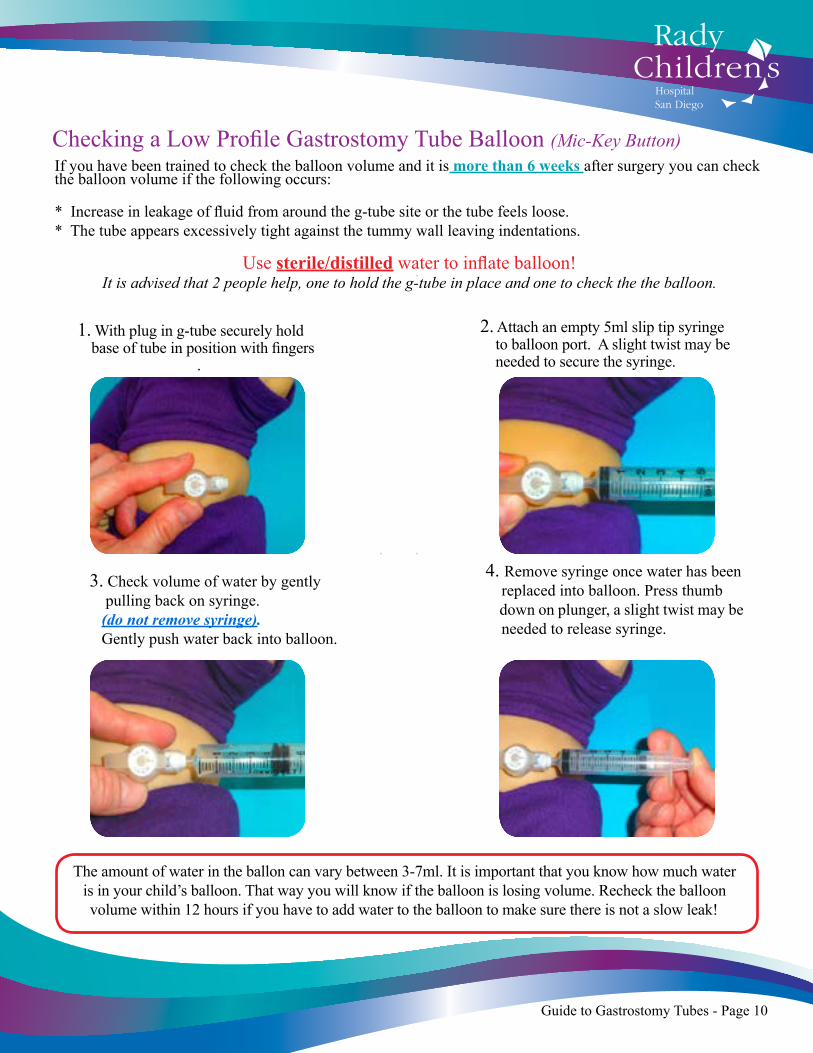
If you have been trained to check the balloon volume and it is more than 6 weeks after surgery you can check the balloon volume if the following occurs:
* Increase in leakage of fluid from around the g-tube site or the tube feels loose.* The tube appears excessively tight against the tummy wall leaving indentations.
Use sterile/distilled water to inflate balloon!It is advised that 2 people help, one to hold the g-tube in place and one to check the the balloon.
1. With plug in g-tube securely hold base of tube in position with fingers
.
2. Attach an empty 5ml slip tip syringe to balloon port. A slight twist may be needed to secure the syringe.
The amount of water in the ballon can vary between 3-7ml. It is important that you know how much water is in your child’s balloon. That way you will know if the balloon is losing volume. Recheck the balloon volume within 12 hours if you have to add water to the balloon to make sure there is not a slow leak!
3. Check volume of water by gently pulling back on syringe. (do not remove syringe). Gently push water back into balloon.
4. Remove syringe once water has been replaced into balloon. Press thumb down on plunger, a slight twist may be needed to release syringe.
Guide to Gastrostomy Tubes - Page 10
Checking a Low Profile Gastrostomy Tube Balloon (Mic-Key Button)
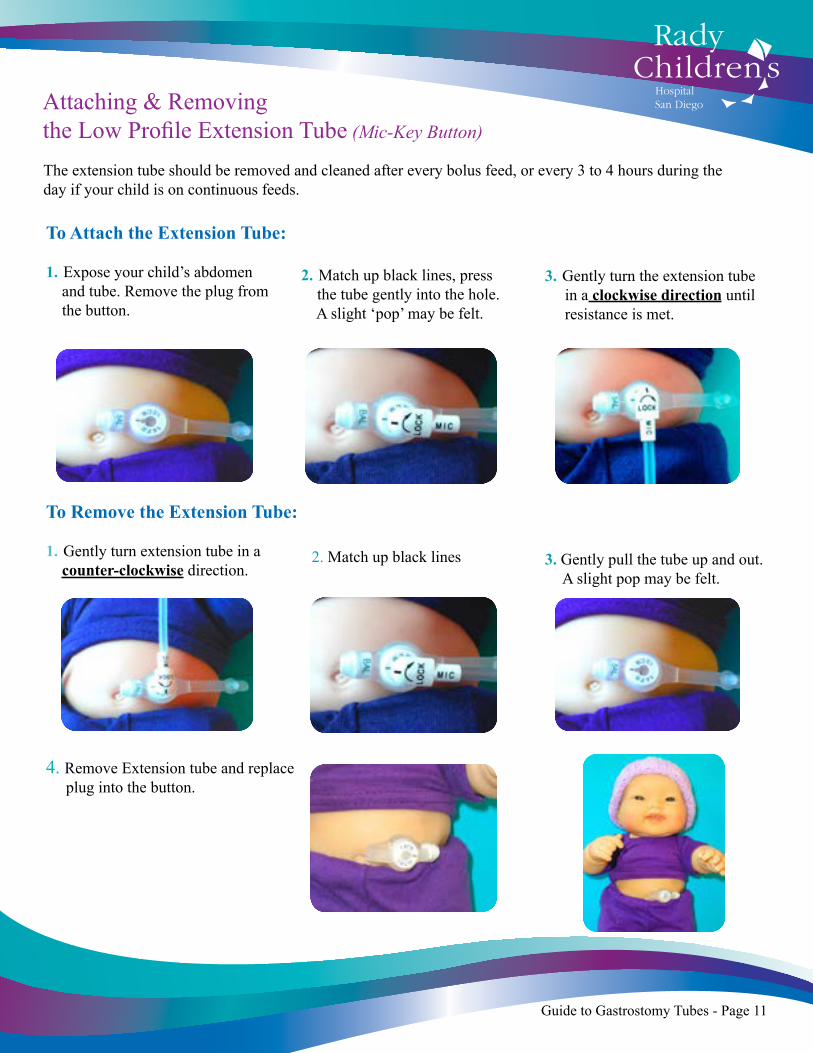
Attaching & Removing the Low Profile Extension Tube (Mic-Key Button)
The extension tube should be removed and cleaned after every bolus feed, or every 3 to 4 hours during the day if your child is on continuous feeds.
3. Gently turn the extension tube in a clockwise direction until resistance is met.
3. Gently pull the tube up and out. A slight pop may be felt.
To Attach the Extension Tube:
1. Expose your child’s abdomen and tube. Remove the plug from the button.
To Remove the Extension Tube:
1. Gently turn extension tube in a counter-clockwise direction.
4. Remove Extension tube and replace plug into the button.
2. Match up black lines, press the tube gently into the hole. A slight ‘pop’ may be felt.
2. Match up black lines
Guide to Gastrostomy Tubes - Page 11
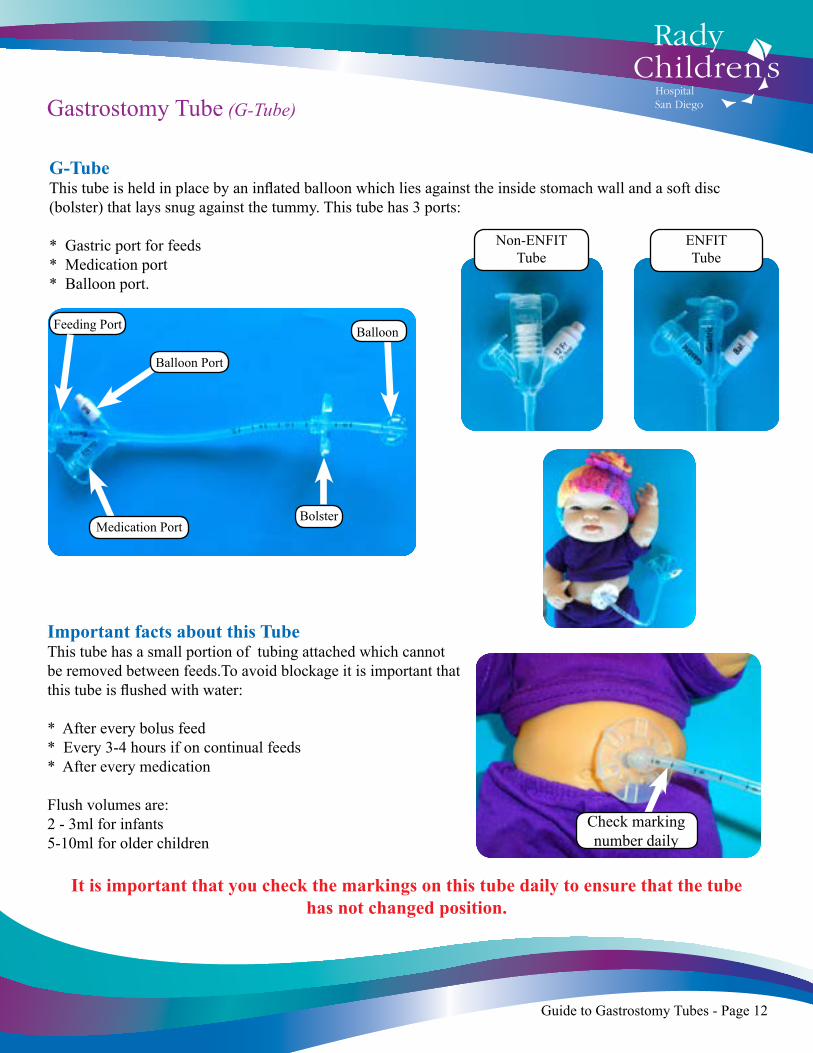
Gastrostomy Tube (G-Tube)
G-TubeThis tube is held in place by an inflated balloon which lies against the inside stomach wall and a soft disc (bolster) that lays snug against the tummy. This tube has 3 ports:
* Gastric port for feeds* Medication port * Balloon port.
Important facts about this TubeThis tube has a small portion of tubing attached which cannot be removed between feeds.To avoid blockage it is important that this tube is flushed with water:
* After every bolus feed* Every 3-4 hours if on continual feeds* After every medication
Flush volumes are:2 - 3ml for infants5-10ml for older children
It is important that you check the markings on this tube daily to ensure that the tube has not changed position.
Balloon Port
BolsterMedication Port
Balloon Feeding Port
Check marking number daily
Guide to Gastrostomy Tubes - Page 12
Non-ENFITTube
ENFITTube
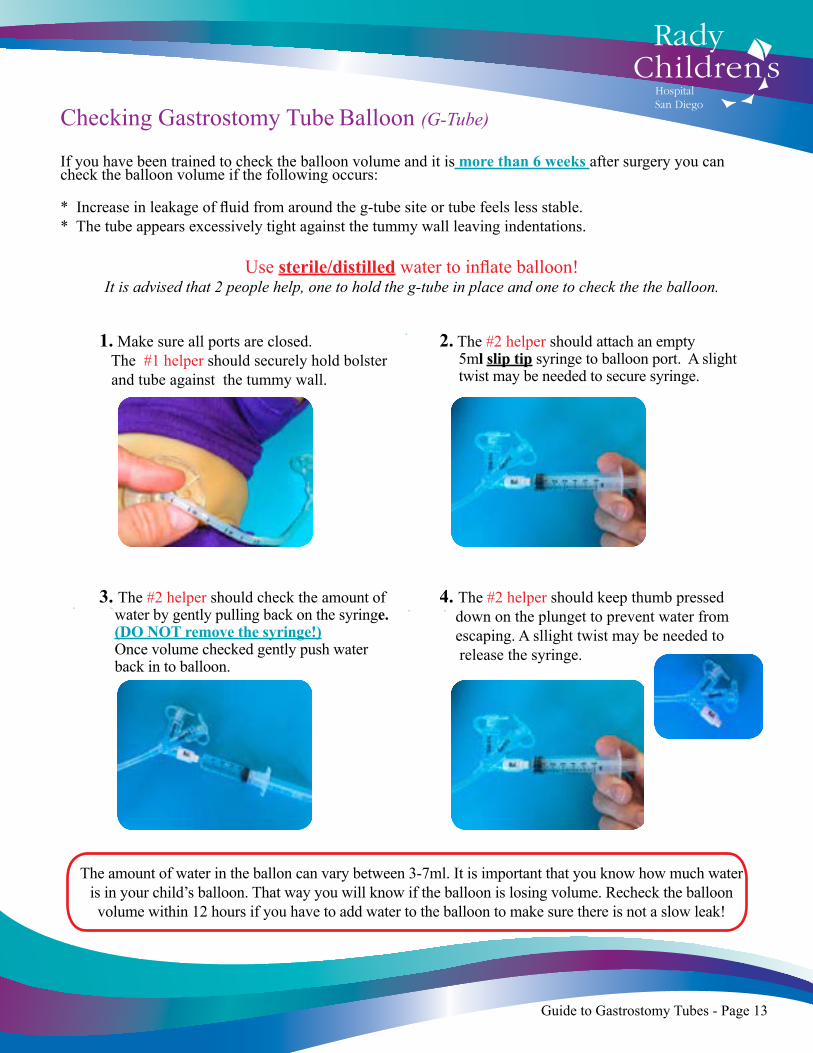
If you have been trained to check the balloon volume and it is more than 6 weeks after surgery you can check the balloon volume if the following occurs:
* Increase in leakage of fluid from around the g-tube site or tube feels less stable.* The tube appears excessively tight against the tummy wall leaving indentations.
Use sterile/distilled water to inflate balloon!It is advised that 2 people help, one to hold the g-tube in place and one to check the the balloon.
1. Make sure all ports are closed. The #1 helper should securely hold bolster and tube against the tummy wall.
2. The #2 helper should attach an empty 5ml slip tip syringe to balloon port. A slight twist may be needed to secure syringe.
The amount of water in the ballon can vary between 3-7ml. It is important that you know how much water is in your child’s balloon. That way you will know if the balloon is losing volume. Recheck the balloon volume within 12 hours if you have to add water to the balloon to make sure there is not a slow leak!
3. The #2 helper should check the amount of water by gently pulling back on the syringe. (DO NOT remove the syringe!) Once volume checked gently push water back in to balloon.
Checking Gastrostomy Tube Balloon (G-Tube)
4. The #2 helper should keep thumb pressed down on the plunget to prevent water from escaping. A sllight twist may be needed to release the syringe.
Guide to Gastrostomy Tubes - Page 13
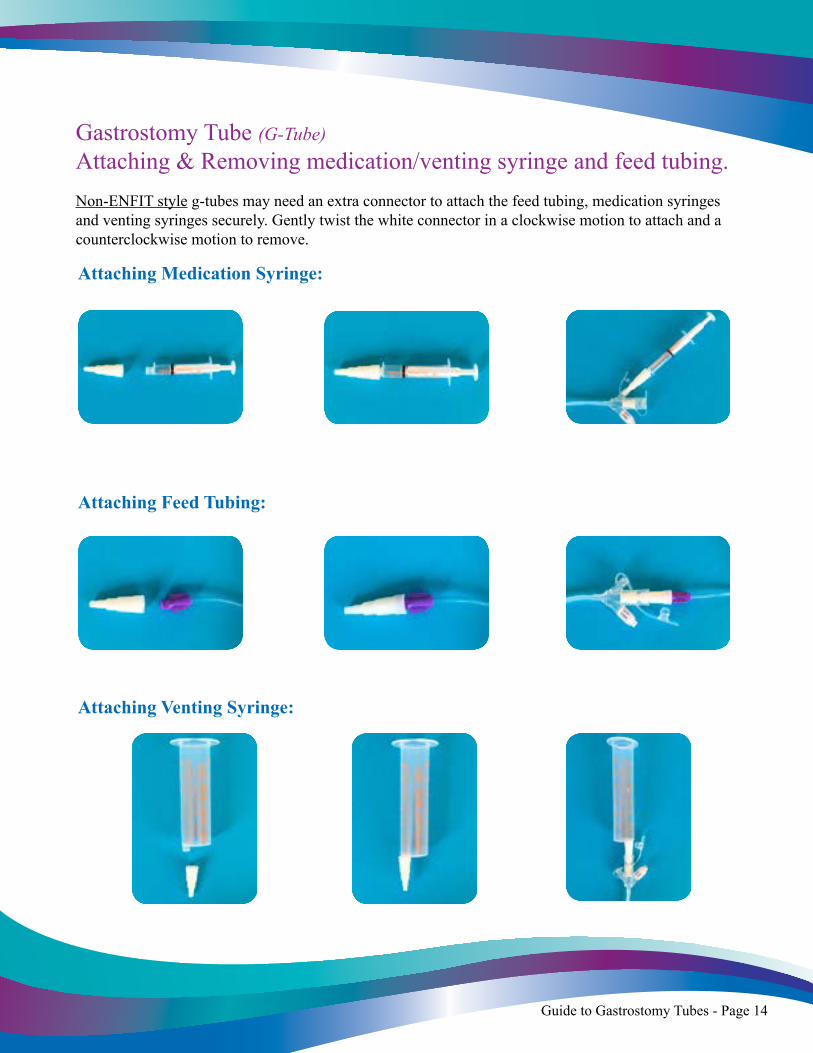
Gastrostomy Tube (G-Tube)Attaching & Removing medication/venting syringe and feed tubing.Non-ENFIT style g-tubes may need an extra connector to attach the feed tubing, medication syringes and venting syringes securely. Gently twist the white connector in a clockwise motion to attach and a counterclockwise motion to remove.
Attaching Feed Tubing:
Attaching Venting Syringe:
Attaching Medication Syringe:
Guide to Gastrostomy Tubes - Page 14
Preventing Tube Blockage
Remember: Your child’s tube need to be flushed with water at regular intervals to keep it in good working order.
It is important that you flush your child’s tube with water after every bolus feeding, as well as before and after every medication. If your child is on a continual feeding program, then flush the tube at least every 3-4 hours during the day (normally while changing your child’s formula).
Infants, 2 to 3 ml of water should be used to flush the tubes clear. Older children, 5 to 10 ml of water should be used to flush the tubes clear.
Check with your child’s nurse how much water is needed to flush your child’s tube.
A 12 inch mic-key extension tube requires approximately 3 ml to clear. A 24 inch mic-key extension tube requires approximately 5 ml to clear. A g-tube feeding port requires approximately 3 - 5 ml to clear.
Low Profile Gastrostomy Tube (Mic-key button): Flush water via extension tube after every bolus feeding. Flush water via extension tube every 3 to 4 hours during the day if continual feeding (when changing milk).
Gastrostomy Tube (G-Tube): Flush water via feeding port after every bolus feeding. Flush water via feeding port every 3 - 4 hours during the day if continual feeding (when changing milk).
Helpful Tips• Only give formula and milk preparations that have been prescribed by your child’s physician, dietician or feeding specialist.
• Only give medications that have been cleared by your child’s physician. Make sure the medication is given in the form that was prescribed by your child’s physician.
• The water you use to prepare your child’s formula can also be used to flush the tube.
Guide to Gastrostomy Tubes - Page 15
Care of EquipmentFormula Container and Syringes:
1. After each use, wash well with warm water and a little dish soap.2. Rinse well with clear warm water to ensure all soap is removed.3. Air dry on a clean towel.4. When the container and syringe are completely dry, store them in a clean and covered container.
Feeding Bag and Tubing:
1. After each use, wash with warm water.2. You may need to squeeze the tubing and bag to clear out all the milk.3. Rinse thoroughly with clean warm water.4. Air dry and store in a clean covered container.
How frequently to change equipment:
Your medical insurance coverage will determine how frequently you will change out your feeding bags and extension tubes. Please check with your Home Care team and your insurance provider to determine what supplies will be available to you.
Feeding bags can be used for 24 hours, or sometimes longer. It is important that your feeding bags are kept as clean as possible; therefore, thorough cleaning between feeds is advised. Many insurance companies will allow these bags to be discarded and changed every day.
The extension tubes can be used for a week, or sometimes longer. It is important that you remove your child’s extension tube and clean it thoroughly between feeds. Your insurance company will determine how frequently you will be able to change them. However, if at any point in time the tube starts to leak or the tube becomes difficult to clean, it is advisable that you discard and change it.
Guide to Gastrostomy Tubes - Page 16
Preparing Normal Saline and Sterile Water
Supplies Needed:
• Saucepan • Metal tongs • Glass jar with lids • Table salt • Tap water
Steps to Follow First:
1. Place glass jars, metal tongs and lids in large saucepan. 2. Fill pan with enough water to cover the jars and boil for 20 minutes. 3. Let cool.
Sterile Water (FOR USE IN G-TUBE BALLOON ONLY): 1. Place 2 cups boiled water in glass jar. 2. Place lid on jar. 3. Discard after 3 days.
Normal Saline (G-TUBE SITE CLEANING ONLY): Complete “Steps to Follow First”, then proceed: 1. Fill glass jar with 2 cups boiled water and add 1 teaspoon table salt. 2. Place lid on jar and shake solution to mix thoroughly. 3. Store normal saline in the refrigerator. 4. Discard after 3 days.
Notes_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
Guide to Gastrostomy Tubes - Page 17
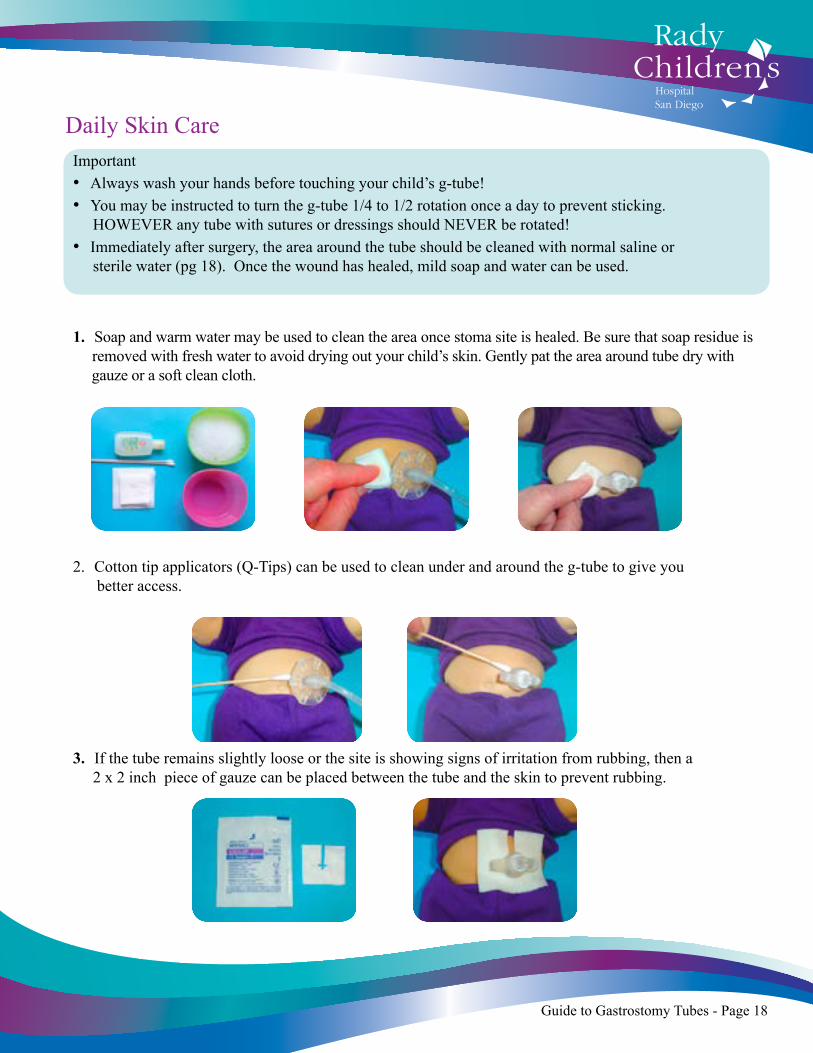
Daily Skin CareImportant• Always wash your hands before touching your child’s g-tube!• You may be instructed to turn the g-tube 1/4 to 1/2 rotation once a day to prevent sticking. HOWEVER any tube with sutures or dressings should NEVER be rotated! • Immediately after surgery, the area around the tube should be cleaned with normal saline or sterile water (pg 18). Once the wound has healed, mild soap and water can be used.
1. Soap and warm water may be used to clean the area once stoma site is healed. Be sure that soap residue is removed with fresh water to avoid drying out your child’s skin. Gently pat the area around tube dry with gauze or a soft clean cloth.
2. Cotton tip applicators (Q-Tips) can be used to clean under and around the g-tube to give you better access.
3. If the tube remains slightly loose or the site is showing signs of irritation from rubbing, then a 2 x 2 inch piece of gauze can be placed between the tube and the skin to prevent rubbing.
Guide to Gastrostomy Tubes - Page 18
Skin Care ProblemsIt is important that you check your child’s g-tube site daily for any changes including redness, puffiness, breaks in skin, bleeding or any discharge that has a foul odor.
Redness or irritation around your child’s g-tube site:This can be caused by leakage of fluid around the g-tube site, tape irritation, infection or the tube being pulled by your child.
* Keep skin around g-tube clean and dry
* A 2x2 inch piece of gauze may be placed between the skin and the g-tube. Change the gauze with every diaper change or anytime it gets wet.
* Try and expose as much of the site to air when possible.
* Take care not to over clean the site and damage the the fragile skin (once or twice a day is enough!) * Call your doctor if there is any unusual redness, the site feels warmer than usual or there is any smelly dishcarge (these are signs of infection).
* Barrier wipes and creams may be used if advised to do so by your child’s Surgeon/Physician or GI Nurse Specialist.
Leaking around g-tube:This can be caused by a leak in the balloon or your child pulling on the tube causing the stoma to become larger which can cause leaking
* Remove extension tube after each feed.
* Hide the tubing from your child under clothing to prevent him/her from playing with it.
* Vent your child’s tube before and after every feed and any time his/her tummy looks full.
* Check balloon volume if it is more than 6 weeks since surgery. (see Pg. 10/13)
Extra skin growth around g-tube site (Granulation):This can be caused by moisture and constant movement of the the tube against the skin.
* Place a 2x2 inch piece of gauze between skin and tube. Change gauze with every diaper change and when it gets wet. * If the skin continues to grow, contact the GI Clinic to schedule a nurse’s visit for further assessment.
* Contact your child’s doctor for further advice on treatment and care.
Guide to Gastrostomy Tubes - Page 19
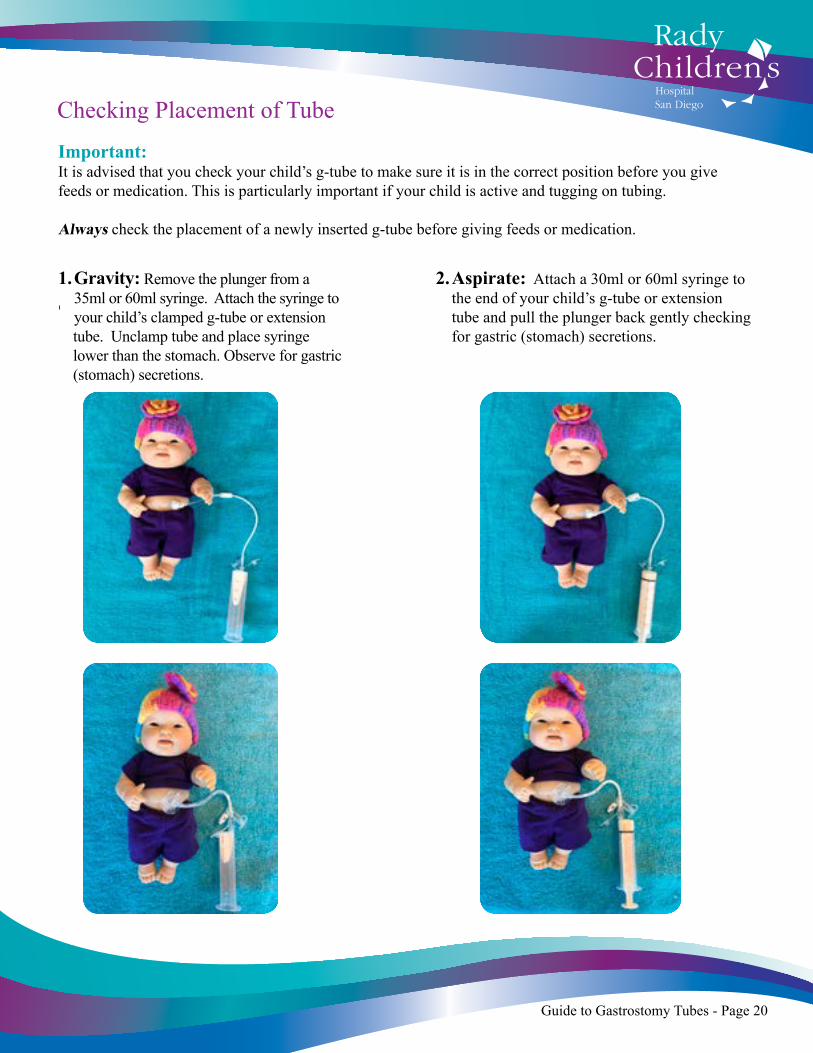
Important: It is advised that you check your child’s g-tube to make sure it is in the correct position before you give feeds or medication. This is particularly important if your child is active and tugging on tubing.
Always check the placement of a newly inserted g-tube before giving feeds or medication.
1. Gravity: Remove the plunger from a 35ml or 60ml syringe. Attach the syringe to your child’s clamped g-tube or extension tube. Unclamp tube and place syringe lower than the stomach. Observe for gastric (stomach) secretions.
2. Aspirate: Attach a 30ml or 60ml syringe to the end of your child’s g-tube or extension tube and pull the plunger back gently checking for gastric (stomach) secretions.
Checking Placement of Tube
Guide to Gastrostomy Tubes - Page 20
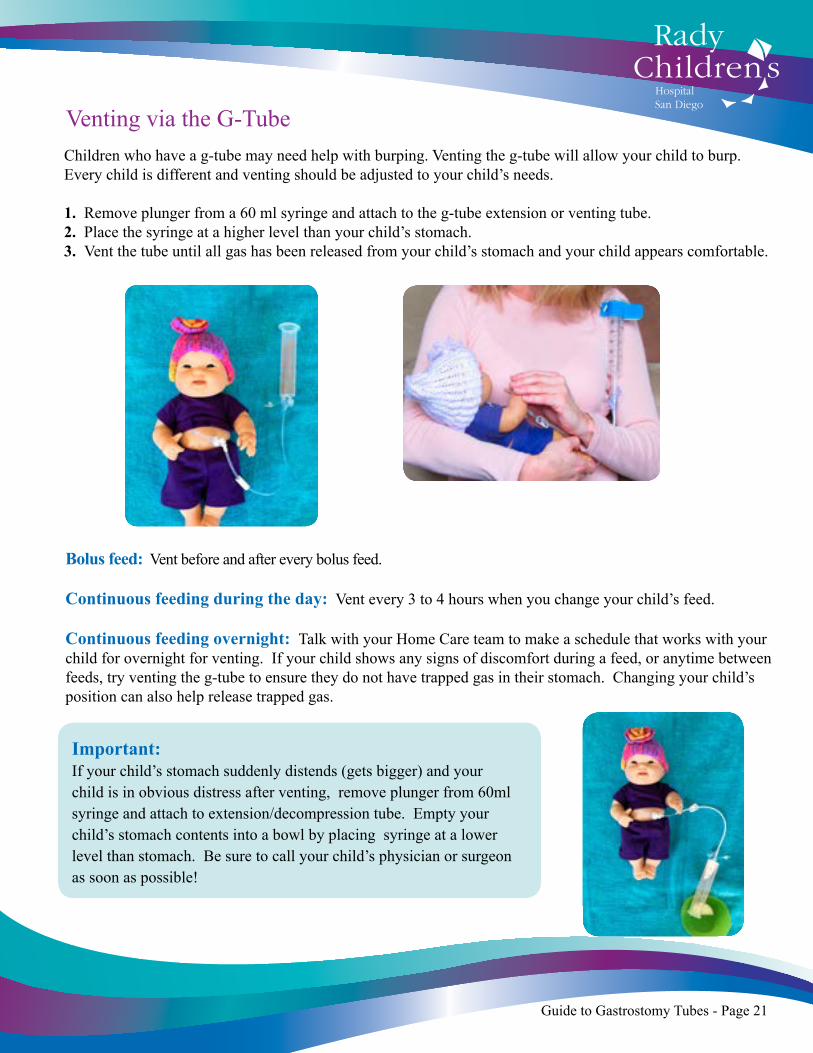
Venting via the G-TubeChildren who have a g-tube may need help with burping. Venting the g-tube will allow your child to burp. Every child is different and venting should be adjusted to your child’s needs.
1. Remove plunger from a 60 ml syringe and attach to the g-tube extension or venting tube.2. Place the syringe at a higher level than your child’s stomach.3. Vent the tube until all gas has been released from your child’s stomach and your child appears comfortable.
Bolus feed: Vent before and after every bolus feed.
Continuous feeding during the day: Vent every 3 to 4 hours when you change your child’s feed.
Continuous feeding overnight: Talk with your Home Care team to make a schedule that works with your child for overnight for venting. If your child shows any signs of discomfort during a feed, or anytime between feeds, try venting the g-tube to ensure they do not have trapped gas in their stomach. Changing your child’s position can also help release trapped gas.
Important: If your child’s stomach suddenly distends (gets bigger) and your child is in obvious distress after venting, remove plunger from 60ml syringe and attach to extension/decompression tube. Empty your child’s stomach contents into a bowl by placing syringe at a lower level than stomach. Be sure to call your child’s physician or surgeon as soon as possible!
Guide to Gastrostomy Tubes - Page 21

Types of Feeding
Continual Feeds: Based on your physician’s recommendation, your child may be on continuous feeds for the full 24 hours or strictly overnight. Continuous feeds are always delivered by a pump. Home Care services will deliver and teach you how to use your pump.
Important: It is important to stop continuous feeds every 3-4 hours during the day to clean the feeding bag and vent the g-tube.
Bolus Feeds: A bolus feed is when your child is given a set amount of feed over a set length of time (usually between 30 minutes to 2 hours). Bolus feeds may be given by pump or gravity feeding depending on length of time feeds have to be given over:
Pump feeding: Your child’s physician may want you to give feeds over the period of an hour or two. In this case the feeds will need to be delivered by pump. Your nurse will show you how to calculate the amount of milk and time to give the pump before you are discharged to leave the hospital.
Gravity feeding: Your child’s physician may want you to give feeds over a short period of time (between 20 to 30 minutes). Gravity feeding is completed using a 35ml or 60 ml syringe that is attached to your child’s extension tube. The speed of the feeding can be adjusted depending on the height that the syringe is placed above the stomach.
Important: Flush your child’s g-tube and extension tube water after every bolus feed or every 3-4 hours if your child is on continual feeding. Infants ............... flush 2-3ml of water Older Children ... flush 5-10ml of water
Guide to Gastrostomy Tubes - Page 22
Feedings
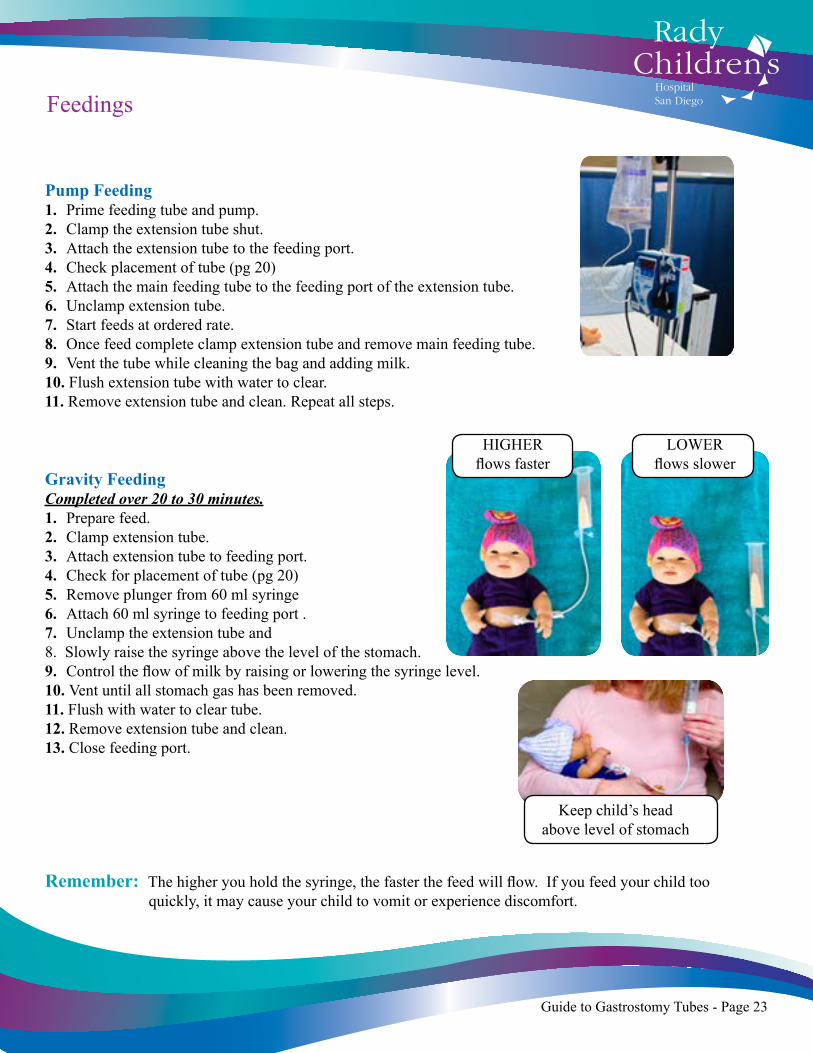
Pump Feeding1. Prime feeding tube and pump.2. Clamp the extension tube shut.3. Attach the extension tube to the feeding port.4. Check placement of tube (pg 20)5. Attach the main feeding tube to the feeding port of the extension tube.6. Unclamp extension tube.7. Start feeds at ordered rate.8. Once feed complete clamp extension tube and remove main feeding tube.9. Vent the tube while cleaning the bag and adding milk.10. Flush extension tube with water to clear.11. Remove extension tube and clean. Repeat all steps.
Gravity FeedingCompleted over 20 to 30 minutes.1. Prepare feed.2. Clamp extension tube.3. Attach extension tube to feeding port.4. Check for placement of tube (pg 20)5. Remove plunger from 60 ml syringe6. Attach 60 ml syringe to feeding port .7. Unclamp the extension tube and 8. Slowly raise the syringe above the level of the stomach. 9. Control the flow of milk by raising or lowering the syringe level.10. Vent until all stomach gas has been removed.11. Flush with water to clear tube.12. Remove extension tube and clean.13. Close feeding port.
Remember: The higher you hold the syringe, the faster the feed will flow. If you feed your child too quickly, it may cause your child to vomit or experience discomfort.
Guide to Gastrostomy Tubes - Page 23
HIGHERflows faster
LOWERflows slower
Keep child’s head above level of stomach

Even though your child is being fed by a g-tube, it is important to provide your child with oral stimulation and the social interaction that surrounds mealtime.
Feeding positions for infants under 6 months: Suggested Positions1. Cradle held2. Infant Seat3. Car Seat4. Wedge5. A Boppy
Feeding positions for infants 6 months and older:Typically mealtimes become more interactive as your child gets older and they start learning feeding skills. We encourage you to have your child supported in a highchair to give your child opportunities to interact with the family during mealtimes, and start exploring and imitating feeding behaviors.
Positioning: Daytime & Bolus Feeding
Your child may need to have continuous feeds overnight. The recommended position is usually your child lying on his or her back or side. Blankets, toys and crib bumpers should not be placed in or around your child’s crib. In special situations your doctor may suggest that you raise the head of your child’s crib or bed. Always follow your child’s Physician/Surgeons recommendations.
Infants should not lay on their stomach unless you are instructed to do so by their
doctor.
Positioning: Nighttime Feeding
Guide to Gastrostomy Tubes - Page 24
Guide to Gastrostomy Tubes - Page 25
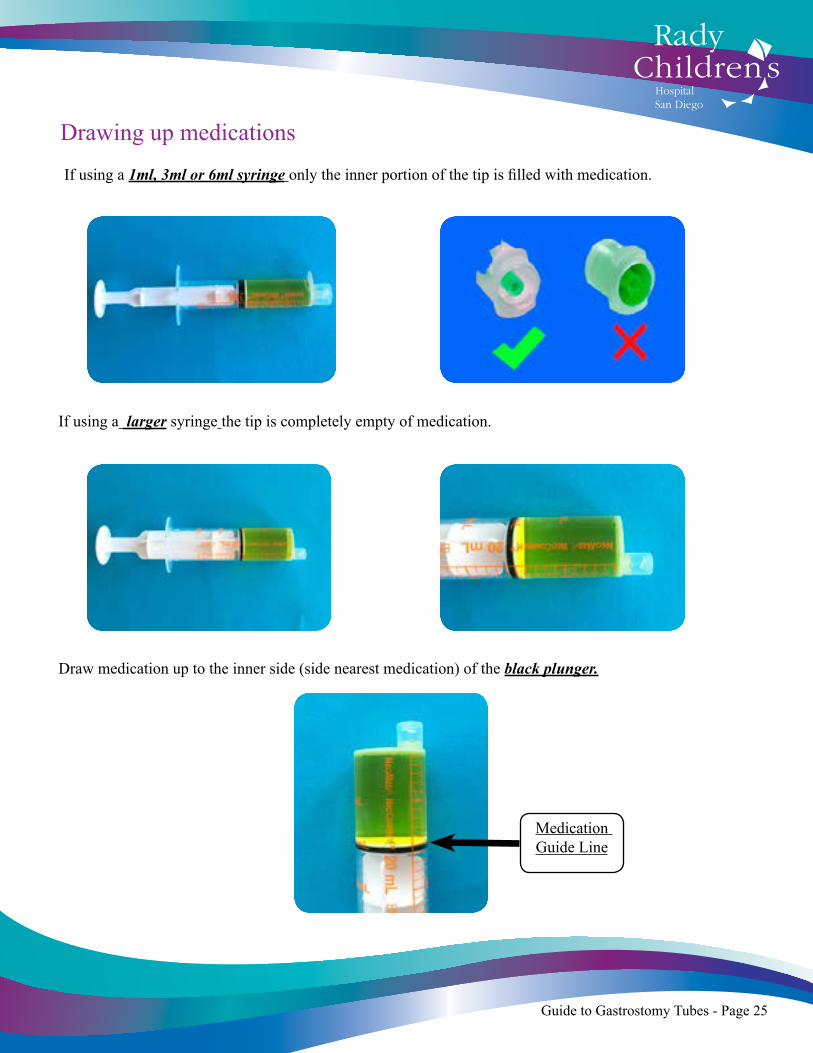
Drawing up medications
If using a 1ml, 3ml or 6ml syringe only the inner portion of the tip is filled with medication.
If using a larger syringe the tip is completely empty of medication.
Draw medication up to the inner side (side nearest medication) of the black plunger.
Medication Guide Line
Guide to Gastrostomy Tubes - Page 26
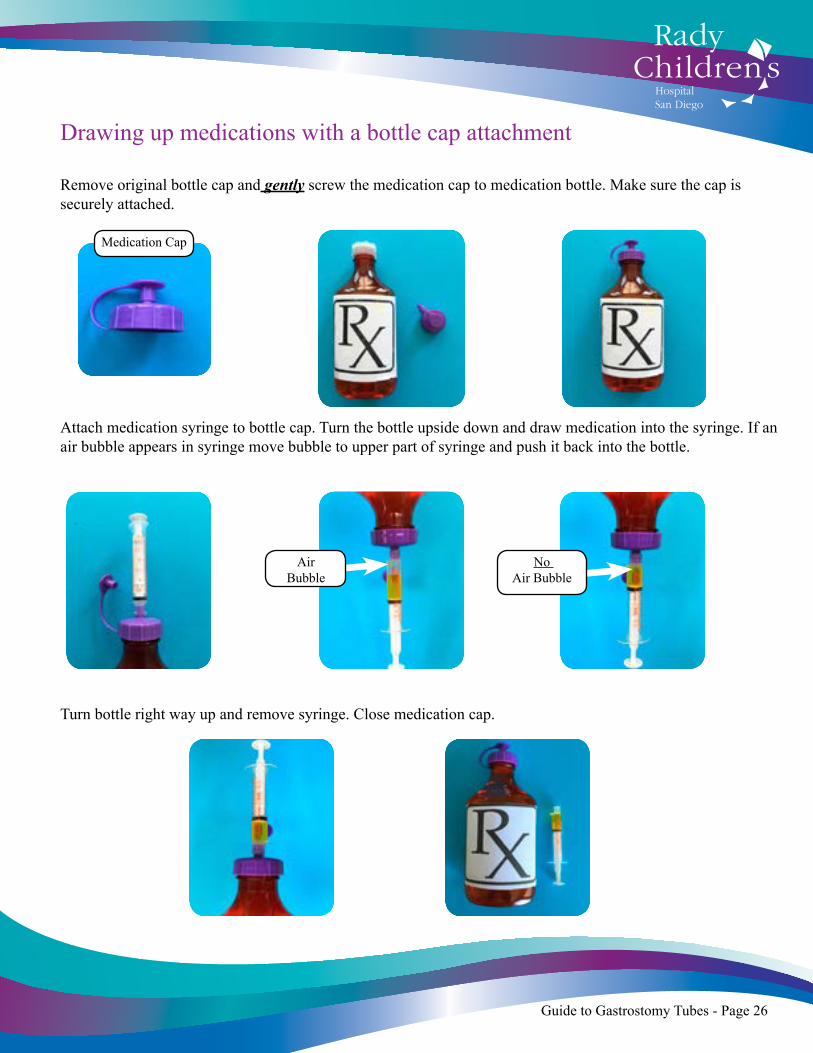
Drawing up medications with a bottle cap attachment
Remove original bottle cap and gently screw the medication cap to medication bottle. Make sure the cap is securely attached.
Attach medication syringe to bottle cap. Turn the bottle upside down and draw medication into the syringe. If an air bubble appears in syringe move bubble to upper part of syringe and push it back into the bottle.
Air Bubble
No Air Bubble
Medication Cap
Turn bottle right way up and remove syringe. Close medication cap.
Guide to Gastrostomy Tubes - Page 27
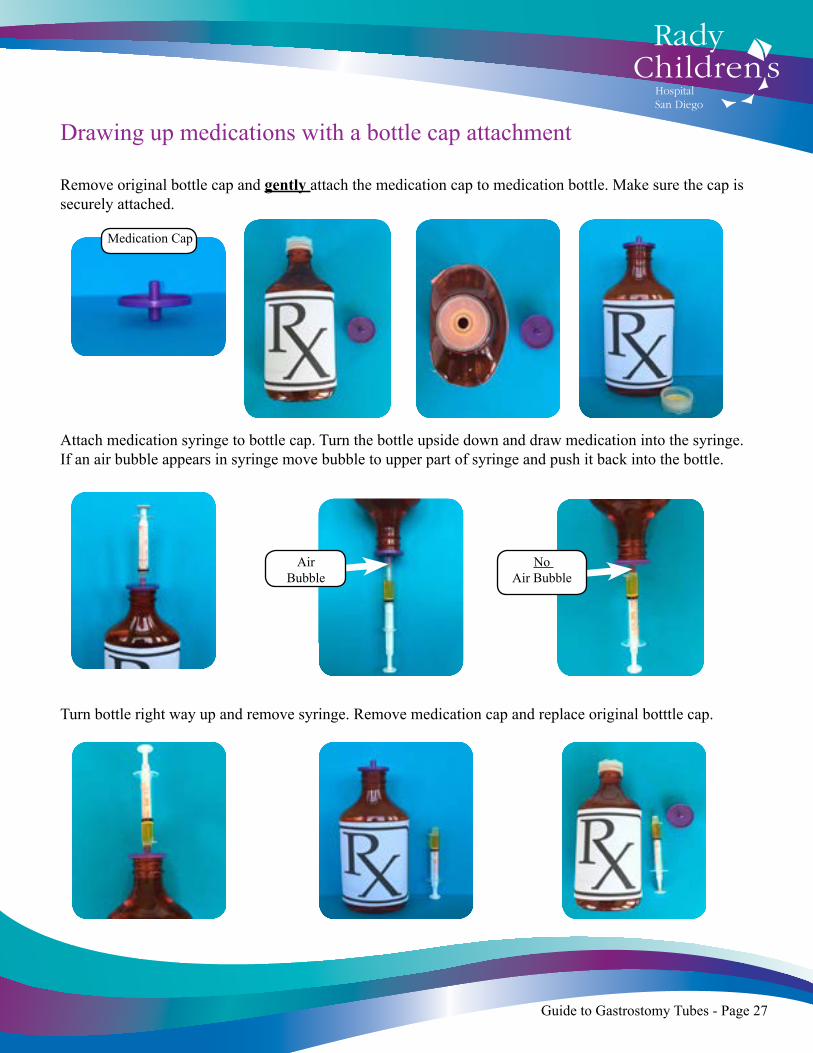
Drawing up medications with a bottle cap attachment
Remove original bottle cap and gently attach the medication cap to medication bottle. Make sure the cap is securely attached.
Attach medication syringe to bottle cap. Turn the bottle upside down and draw medication into the syringe. If an air bubble appears in syringe move bubble to upper part of syringe and push it back into the bottle.
Air Bubble
No Air Bubble
Medication Cap
Turn bottle right way up and remove syringe. Remove medication cap and replace original botttle cap.
Guide to Gastrostomy Tubes - Page 29
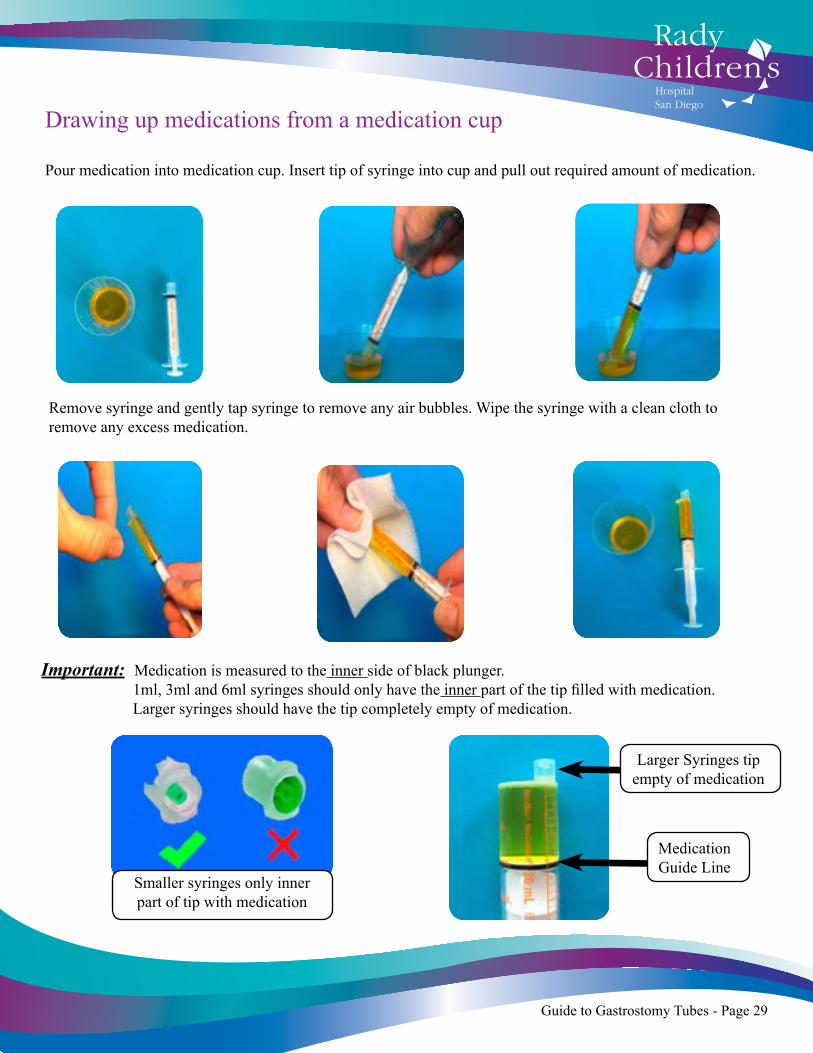
Drawing up medications from a medication cup
Pour medication into medication cup. Insert tip of syringe into cup and pull out required amount of medication.
Remove syringe and gently tap syringe to remove any air bubbles. Wipe the syringe with a clean cloth to remove any excess medication.
Important: Medication is measured to the inner side of black plunger. 1ml, 3ml and 6ml syringes should only have the inner part of the tip filled with medication. Larger syringes should have the tip completely empty of medication.
Medication Guide Line
Smaller syringes only inner part of tip with medication
Larger Syringes tip empty of medication

Guide to Gastrostomy Tubes - Page 29
How to administer crushed medication
Check with Pharmacist before crushing any medication tablets.
Pull plunger out of 35 ml or 60 ml syringe. Attach syringe to medication port of g-tube/extension tube (like a funnel).
Pour dissolved medication into the syringe and allow it to flow into tube by gravity. Flush the tube with water until completely clear of ALL medication..
Crush tablet with a pill crusher until it becomes a fine powder. Add water (2-5ml for infants, 5-10ml for older children) to powder and mix well until powder is dissolved.
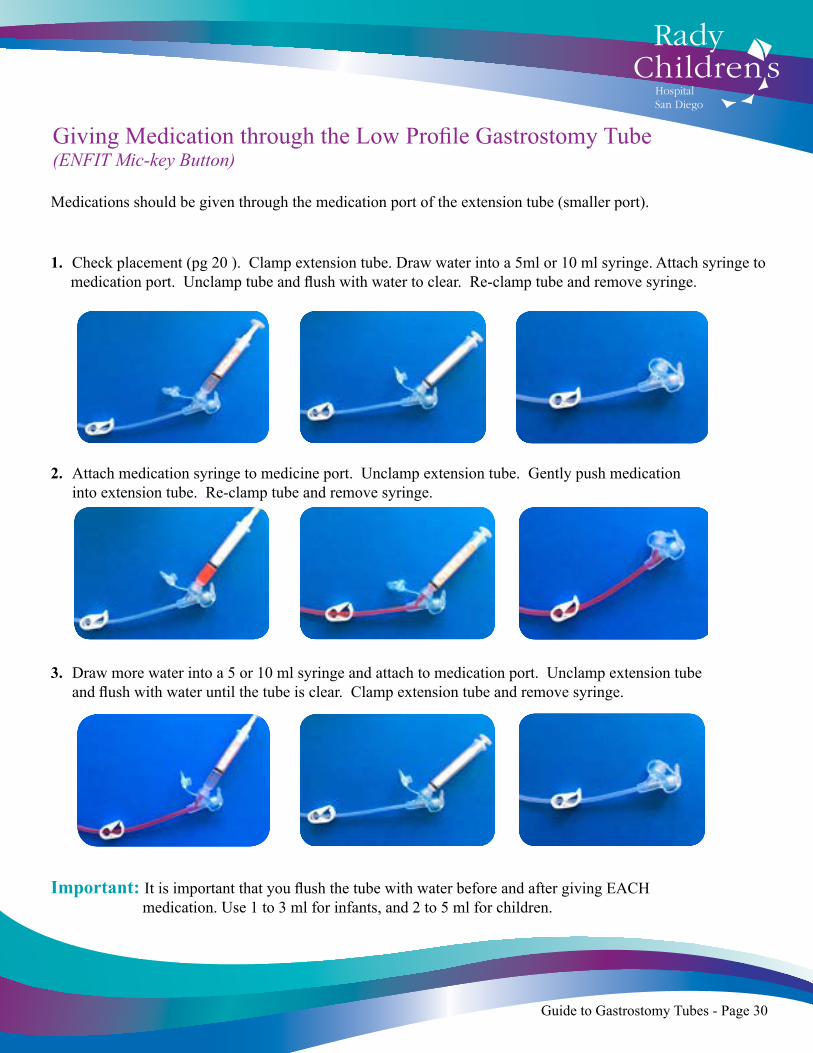
Giving Medication through the Low Profile Gastrostomy Tube (ENFIT Mic-key Button)
Medications should be given through the medication port of the extension tube (smaller port).
1. Check placement (pg 20 ). Clamp extension tube. Draw water into a 5ml or 10 ml syringe. Attach syringe to medication port. Unclamp tube and flush with water to clear. Re-clamp tube and remove syringe.
.
2. Attach medication syringe to medicine port. Unclamp extension tube. Gently push medication into extension tube. Re-clamp tube and remove syringe.
3. Draw more water into a 5 or 10 ml syringe and attach to medication port. Unclamp extension tube and flush with water until the tube is clear. Clamp extension tube and remove syringe.
Important: It is important that you flush the tube with water before and after giving EACH medication. Use 1 to 3 ml for infants, and 2 to 5 ml for children.
Guide to Gastrostomy Tubes - Page 30
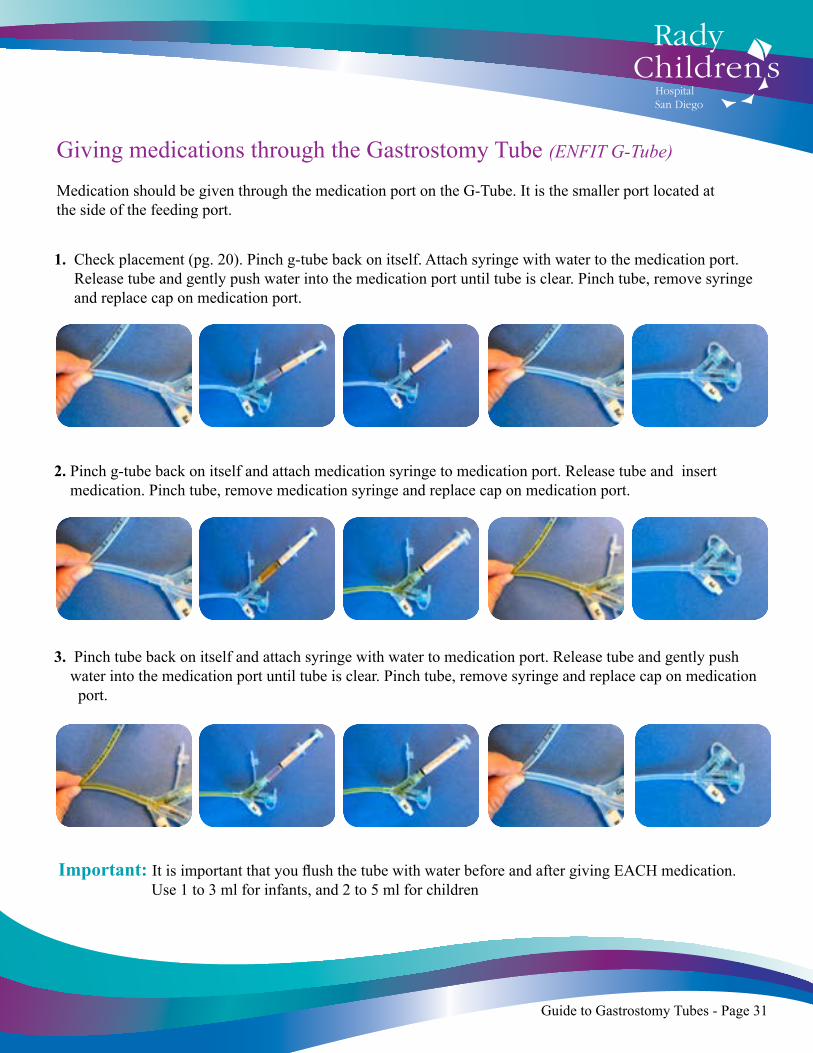
Giving medications through the Gastrostomy Tube (ENFIT G-Tube)
Medication should be given through the medication port on the G-Tube. It is the smaller port located at the side of the feeding port.
1. Check placement (pg. 20). Pinch g-tube back on itself. Attach syringe with water to the medication port. Release tube and gently push water into the medication port until tube is clear. Pinch tube, remove syringe and replace cap on medication port.
2. Pinch g-tube back on itself and attach medication syringe to medication port. Release tube and insert medication. Pinch tube, remove medication syringe and replace cap on medication port.
3. Pinch tube back on itself and attach syringe with water to medication port. Release tube and gently push water into the medication port until tube is clear. Pinch tube, remove syringe and replace cap on medication port.
Important: It is important that you flush the tube with water before and after giving EACH medication. Use 1 to 3 ml for infants, and 2 to 5 ml for children
Guide to Gastrostomy Tubes - Page 31
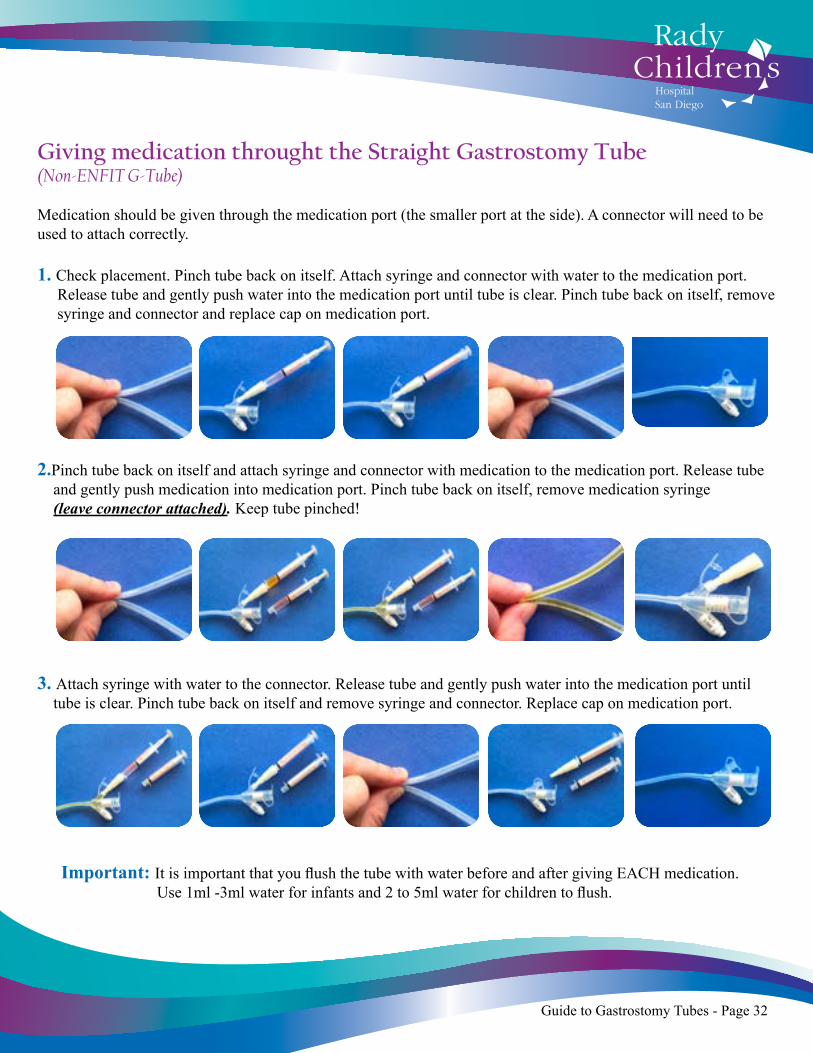
Important: It is important that you flush the tube with water before and after giving EACH medication. Use 1ml -3ml water for infants and 2 to 5ml water for children to flush.
Giving medication throught the Straight Gastrostomy Tube (Non-ENFIT G-Tube)
Medication should be given through the medication port (the smaller port at the side). A connector will need to be used to attach correctly.
1. Check placement. Pinch tube back on itself. Attach syringe and connector with water to the medication port. Release tube and gently push water into the medication port until tube is clear. Pinch tube back on itself, remove syringe and connector and replace cap on medication port.
2.Pinch tube back on itself and attach syringe and connector with medication to the medication port. Release tube and gently push medication into medication port. Pinch tube back on itself, remove medication syringe (leave connector attached). Keep tube pinched!
3. Attach syringe with water to the connector. Release tube and gently push water into the medication port until tube is clear. Pinch tube back on itself and remove syringe and connector. Replace cap on medication port.
Guide to Gastrostomy Tubes - Page 32

Important Medication Facts
It is important to understand the different types of medications your child is prescribed. Some medications need to be taken with food while others may not be given with food because food changes the effect of the medication.
Check with your child’s Physician and/or Pharmacist regarding special instructions for your child’s medications. Always check with your child’s Physician and Pharmacist before starting your child on any new medications to make sure there are no possible interactions with current medications or formula. Liquid medication is the only recommended type of medication to be given via g-tubes.
Some children have capsules or tablets prescribed. Check with your child’s Physician and Pharmacist to ensure that you can alter the way to give these medications.
Tablet
Capsule: powder inside
Capsule: soft gelatin
Capsule: slow release beads
Check with your child’s Pharmacist or Physician before crushing any medication. Crush the tablet into a fine powder with a pill crusher. Mix the powder with water until all the powder has dissolved (2-5 ml for infants and 5-10 ml for older children). Remove plunger from 20ml syringe and connect to the g-tube/extension tube medication port. Pour dissolved medication into the syringe barrel, like a funnel (pg 29.Flush the tube clear with water after giving the medication.
Remove the outer case and empty powder into a small dish. Mix the powder with water until all the powder has dissolved (2-5 ml for infants and 5-10 ml for older children). Remove plunger from 20ml syringe and connect to g-tube/extension tube medication port. Pour dissolved medication syringe barrel, like a funnel. (pg 29). Flush the tube clear with water after giving the medication.
These are NOT RECOMMENDED for g-tubes. Ask your child’s doctor for a liquid form of medication.
These are NOT RECOMMENDED for g-tubes. Ask your child’s doctor for a liquid form of medication
Guide to Gastrostomy Tubes - Page 33
Important Medication Facts continued ...
The following are guidelines to help you when your child needs to be given medication in a specific way.
Flush the tubing with water between each medication, making sure the tubing is clear from the previous medication before giving the next one.
Understanding Units of Measurement:
The medication can be given at any time during your child’s feed. Bolus feeds can be adjusted a little to fit in with the times of the medication. If your child is older and can take food by mouth, you can always give him/her a little snack to take with the medication.
Bolus Feeds:-The best time to give medications is usually half way between feeding times. Try pulling back stomach secretions with a syringe (see pg. 20). Give medication when you get the smallest amount of secretions returned.
Continual Feeds:-Stop the feeds for 15 - 20 minutes to allow the stomach to empty. Give medications and then leave feeds off for another 15 -20 minutes to allow the medication to be absorbed. If your child is on a strict diet you can increase his/her feed a little over the next hour to catch up on volume. Discuss with your child’s Physician the best way to do this.
To be given with food:
To be given on an empty stomach
1 cc = 1 ml
1 fl.oz = 30 ml
1 cup = 8 oz = 240 ml
Guide to Gastrostomy Tubes - Page 34
Tube Dislodgement!What to do if your child’s tube falls out.
There may be an occasion where your child’s g-tube may fall out. In most cases this happens accidentally while your child is playing; on other occasions it is due to the sutures or balloon becoming dislodged or deflated. A few simple tips will help you to reduce the chances of your child’s tube falling out:
1. Remove the extension tube when your child is not being fed.2. Keep the tubing secure and away from your child by hiding it under his or her clothing (e.g.onesies).3. Do not allow your child to pull or play with the tubing.4. Check the balloon volume if there is an increase of fluid leaking around the g-tube or the tube feels loose (Only check balloon if you have been trained and it is more than 6 weeks after surgery!)5. Important: Keep your child’s travel kit and new g-tube with you at all times!
In the event that your child’s tube does fall out:1. Do not panic! The stoma will start to shrink after the tube falls out, but you still have time to get things in place.
2. Check how many weeks after surgery your child is.
• If child is less than 6 weeks after surgery, cover stoma with gauze, call GI Surgeon/Physician immediately and go to Emergency Department for tube replacement (take travel kit with you)
• If child is more than 6 weeks after surgery, and you have been trained, you can place a mic-key g-tube or a Red Robin Tube (pg. 37/38) Call GI Surgeon/Physician for follow up instructions.
Important: Never force a tube into the stoma (hole)Never give any feeds or medications through a red robin tube.Always call your child’s GI Surgeon/Physician or Nurse Specialist before starting feeds on a newly placed g-tube if it is less than 12 weeks since surgery.
Between 6 and 12 weeks after surgery call your child’s GI Surgeon/Physicain for follow up instructions once the g-tube has been reinserted.
Always take your travel kit, with a new g-tube, to the Emergency Department.
Guide to Gastrostomy Tubes - Page 35
1. Sterile or Distilled water should be used in the balloon. Particles in tap water break down the silicone over time. However in an emergency if no sterile/distilled water is available, tap water can be used and switched out at a later date.
2. Ballons can have between 3 and 7ml inserted in them. This volume varies according to the individual child. It is advised that you know the accurate volume in your child’s balloon.
3. The g-tube should be checked for a good fit every day. The tube should lie snug against the tummy without making an indent in the skin. Contact your child’s GI Surgeon/Physician or Nurse Specialist if you have any concerns.
4. The balloon should not be checked until the tube has be inserted more than 6 weeks. If you have any concerns about the g-tube, call your child’s GI Surgeon/Physician or Nurse Specialist for advice,
5. If you have been trained and it is more than 6 weeks after the insertion of your child’s balloon you can check the balloon volume (pgs. 10 and 13) in the following situations: * Any time there is increased leaking of fluid around the g-tube. * Any time the tube starts to feel less stable than normal. 6. Great care should be taken when checking the balloon.
When the water is removed there is nothing holding the tube in place and it can easily fall out!!
Helpful Tips
* Make sure your child is secure . * It is advised that two people are present when checking the balloon. * Never remove the syringe when checking the balloon volume. * Never remove the hand securing the tube when checking balloon volume. * Never blindly add water to the balloon (over filling can burst the balloon!!) * If more water needs to be added replace the current volume immediately and then add the required amount. * If you need to add water recheck the balloon volume within 12 hours to ensure there is not a slow leak. * If balloon persists in losing volume contact your child’s GI Surgeon/Physician as soon as possible for a replacement tube.
Important Facts about Balloons
Guide to Gastrostomy Tubes - Page 36
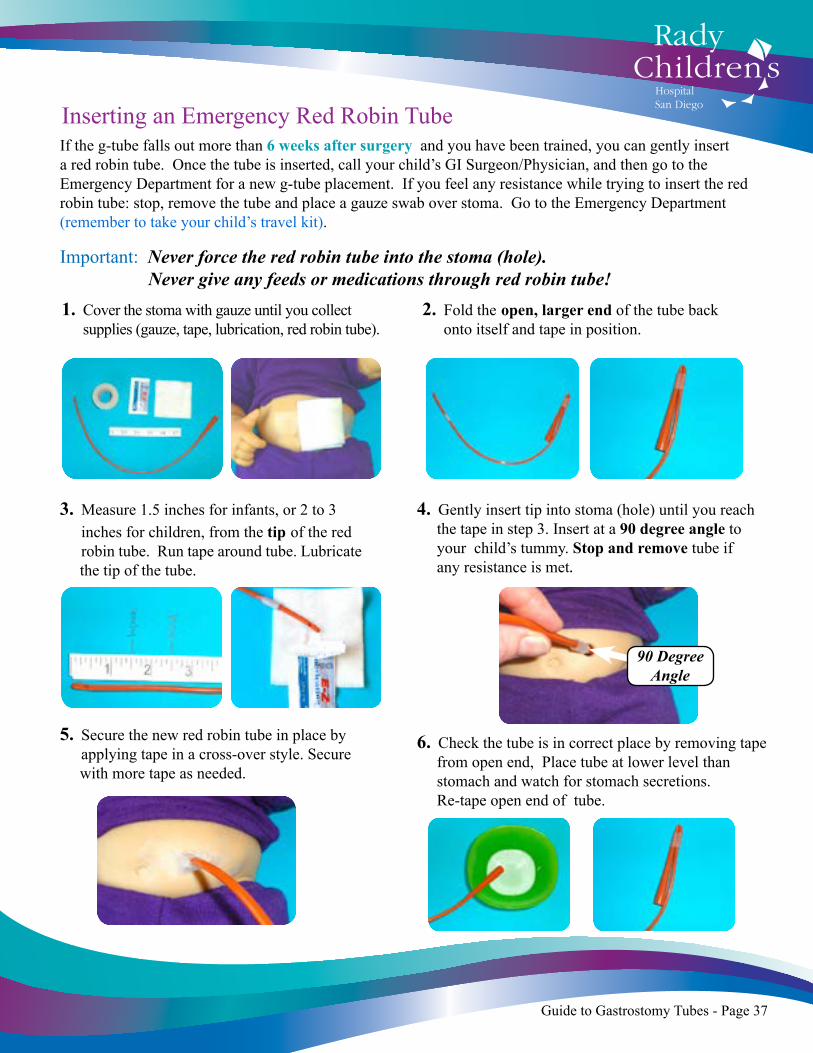
Inserting an Emergency Red Robin TubeIf the g-tube falls out more than 6 weeks after surgery and you have been trained, you can gently insert a red robin tube. Once the tube is inserted, call your child’s GI Surgeon/Physician, and then go to the Emergency Department for a new g-tube placement. If you feel any resistance while trying to insert the red robin tube: stop, remove the tube and place a gauze swab over stoma. Go to the Emergency Department (remember to take your child’s travel kit).
Important: Never force the red robin tube into the stoma (hole). Never give any feeds or medications through red robin tube!
3. Measure 1.5 inches for infants, or 2 to 3 inches for children, from the tip of the red robin tube. Run tape around tube. Lubricate the tip of the tube.
1. Cover the stoma with gauze until you collect supplies (gauze, tape, lubrication, red robin tube).
2. Fold the open, larger end of the tube back onto itself and tape in position.
4. Gently insert tip into stoma (hole) until you reach the tape in step 3. Insert at a 90 degree angle to your child’s tummy. Stop and remove tube if any resistance is met.
5. Secure the new red robin tube in place by applying tape in a cross-over style. Secure with more tape as needed.
6. Check the tube is in correct place by removing tape from open end, Place tube at lower level than stomach and watch for stomach secretions. Re-tape open end of tube.
90 Degree Angle
Guide to Gastrostomy Tubes - Page 37
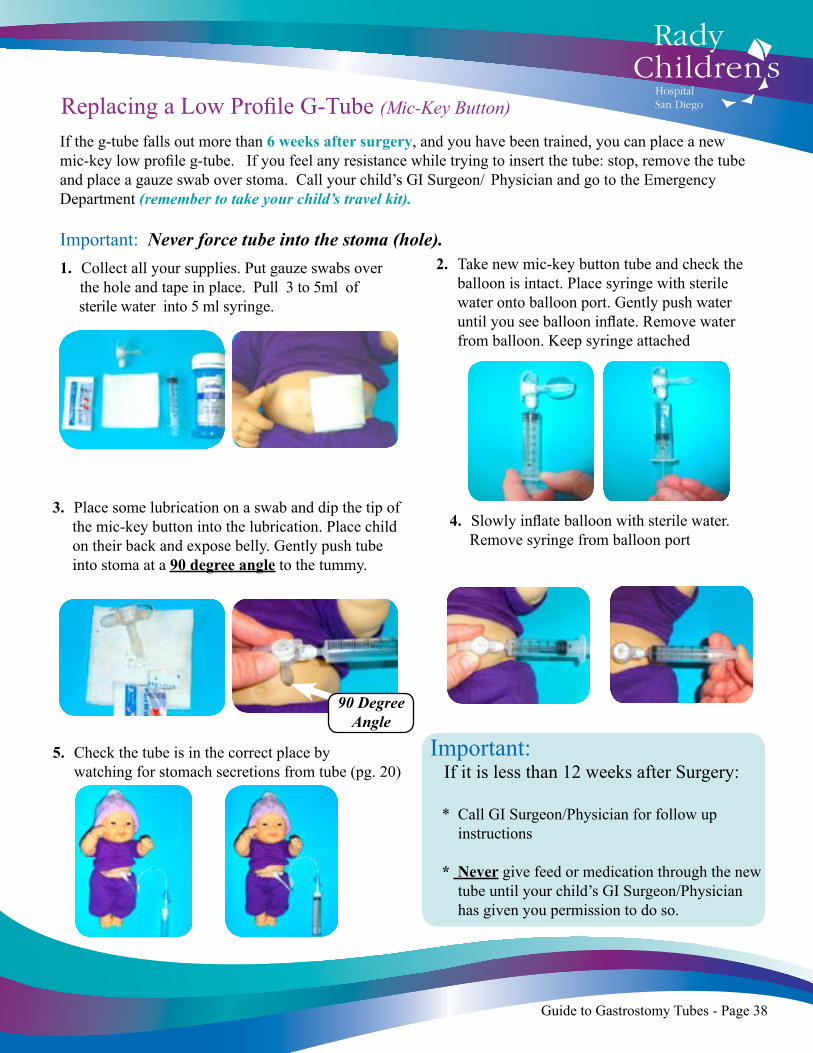
Replacing a Low Profile G-Tube (Mic-Key Button)
If the g-tube falls out more than 6 weeks after surgery, and you have been trained, you can place a new mic-key low profile g-tube. If you feel any resistance while trying to insert the tube: stop, remove the tube and place a gauze swab over stoma. Call your child’s GI Surgeon/ Physician and go to the Emergency Department (remember to take your child’s travel kit).
Important: Never force tube into the stoma (hole). 1. Collect all your supplies. Put gauze swabs over the hole and tape in place. Pull 3 to 5ml of sterile water into 5 ml syringe.
5. Check the tube is in the correct place by watching for stomach secretions from tube (pg. 20)
4. Slowly inflate balloon with sterile water. Remove syringe from balloon port
3. Place some lubrication on a swab and dip the tip of the mic-key button into the lubrication. Place child on their back and expose belly. Gently push tube into stoma at a 90 degree angle to the tummy.
2. Take new mic-key button tube and check the balloon is intact. Place syringe with sterile water onto balloon port. Gently push water until you see balloon inflate. Remove water from balloon. Keep syringe attached
90 Degree Angle
90 Degree Angle
Important: If it is less than 12 weeks after Surgery:
* Call GI Surgeon/Physician for follow up instructions
* Never give feed or medication through the new tube until your child’s GI Surgeon/Physician has given you permission to do so.
Guide to Gastrostomy Tubes - Page 38
Going Home
Before your child is discharged home it is advised that you spend as much time as possible at the hospital to become familiar and confident with all areas of your child’s g-tube care.
The bedside nurses will let you practice on our g-tube doll to make sure that you have training in all areas of care needed for your child’s g-tube. Before discharge, the nurses will expect you to carry out the majority of your child’s g-tube care.
Our goal is to make sure that you feel comfortable, and confident with your child and their new g-tube before you take them home.
Home Care and Equipment:Before discharge someone from the Home Care team will meet with you to go over all aspects of the care you will receive in the community. They will make sure that you have all the supplies you will need and they will arrange for the feeding pump and equipment to be delivered to you. Follow up meetings with a Home Care Nurse will also be made to match with your discharge date.
Occupational Therapy:Before discharge our Occupational Therapist may meet with you on a regular basis to discuss and practice exercises that you can carry out with your child to help them progress to oral feedings at your child’s skill level. Our Therapists will also make arrangements for you to come back to one of their clinics for follow up and support.
Primary Care and Specialty Clinic Follow-Up Appointments:Before discharge, we will ask you to make an appointment with your child’s primary care physician. We strongly suggest that your child’s first follow-up appointment is held within 24 hours from discharge. A copy of your child’s medical record will be sent to his or her primary care physician.
Your may be asked to make your child’s specialty clinic appointments prior to your child’s discharge from the hospital. We want to ensure that all areas of your child’s care is followed up on.
Guide to Gastrostomy Tubes - Page 39
Parents’ Travel Kit
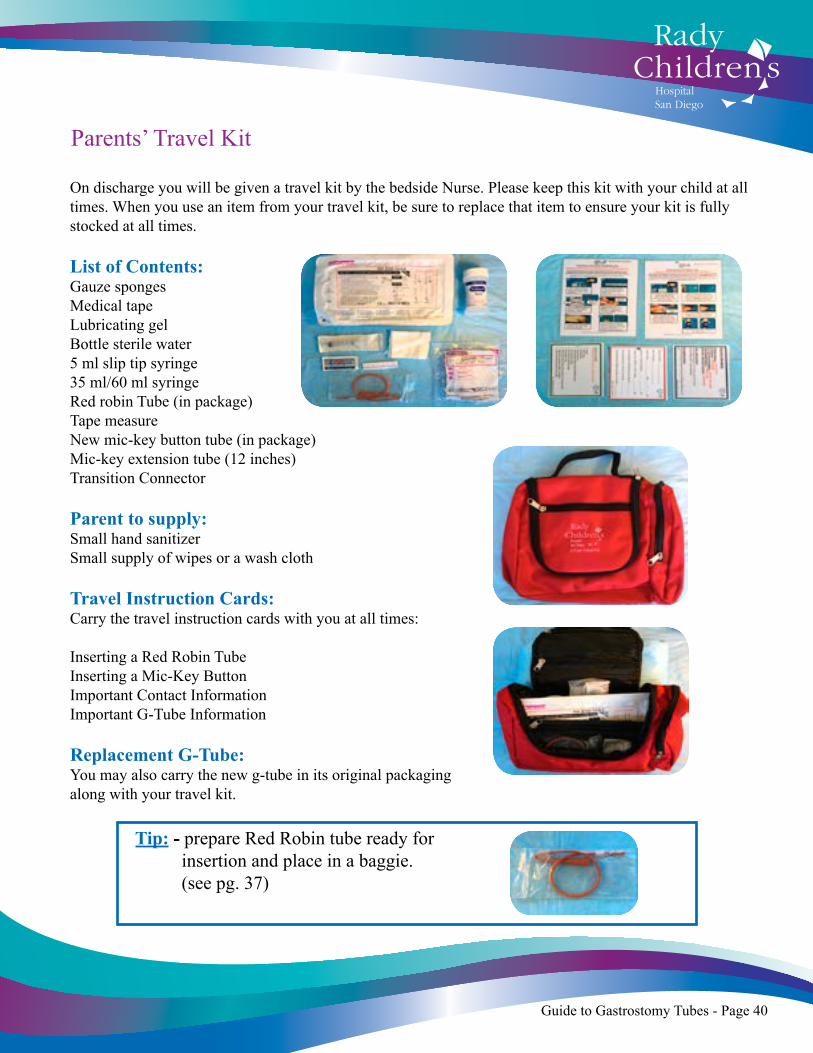
On discharge you will be given a travel kit by the bedside Nurse. Please keep this kit with your child at all times. When you use an item from your travel kit, be sure to replace that item to ensure your kit is fully stocked at all times. List of Contents:Gauze sponges Medical tapeLubricating gelBottle sterile water5 ml slip tip syringe35 ml/60 ml syringeRed robin Tube (in package)Tape measureNew mic-key button tube (in package)Mic-key extension tube (12 inches)Transition Connector Parent to supply:Small hand sanitizerSmall supply of wipes or a wash cloth Travel Instruction Cards:Carry the travel instruction cards with you at all times:
Inserting a Red Robin TubeInserting a Mic-Key ButtonImportant Contact InformationImportant G-Tube Information Replacement G-Tube:You may also carry the new g-tube in its original packaging along with your travel kit.
Tip: - prepare Red Robin tube ready for insertion and place in a baggie. (see pg. 37)
Guide to Gastrostomy Tubes - Page 40

Private Insurance
The Member Services number on the back of your insurance card will be helpful for you in determining your benefits for outpatient care, home equipment, supplies and home health (visits from a nurse or shift nursing in which a nurse cares for your child in your home for eight hours or more per day). The amount of benefit coverage will vary from plan-to-plan. Your discharge planner can help you with this information since she has already been discussing your child with a representative from the insurance company. The financial counselors at Rady Children’s can also help you with any questions you may have about insurance and your child’s stay. The medical unit secretary can help you contact your financial counselor.
Medi-CalIf your family’s income is within certain guidelines you may be eligible for Medi-Cal, which provides families with financial assistance for regular check-ups and special medical care. If you are applying for Medi-Cal, contact a financial counselor at Rady Children’s. The medical unit secretary can help you contact your financial counselor. If your child currently has Medi-Cal, contact your Medi-Cal representative about current eligibility. Your discharge planner will discuss what the Medi-Cal plan will cover for outpatient care, home equipment, supplies and home health visits (these are visits in which a nurse cares for your child in your home for a set amount of time during the day as dictated by your medical coverage)
CCS is a statewide, tax-supported program for specialized medical care and rehabilitation. Children who have a medically eligible diagnosis may receive financial assistance for medical expenses through CCS. A family may be eligible for both Medi-Cal and CCS. A child who is covered by private insurance may also be eligible for CCS for both the inpatient stay and for outpatient care, equipment and supplies. CCS can be helpful when there is need for services that are not covered by your insurance plan. There are financial criteria for the family that your financial counselor can assist you with. Your discharge planner will discuss your child’s eligibility and will make the referral to CCS during the inpatient stay of your child if they qualify.
Supplemental Security Income (SSI)
If your child has a disability that will last more that one year, you may receive a monthly income. Both the amount received and eligibility are dependent on family income. Families with a wage earner and private insurance may still be eligible. For more information about SSI, call (800) 772-1213.
Financial Resources
Insurance
California Children’s Services (CCS)
Guide to Gastrostomy Tubes - Page 41
Financial Assistance
In Home Support Services (IHSS): Children who require special help for their care at home and who are also receiving SSI may also be eligible for IHSS. You may use the money to help care for your child. For more information, you can call IHSS at (866) 351-7722.
W.I.C. (Women, Infants, Children): This is program that provides food supplements to pregnant and/or breast feeding women and children at nutritional risk under the age of 5. There is an income guideline that must be met. WIC will also cover many specialty formulas that your child may require. To learn more about WIC services, call (800) 500-6411.
Anderson Dental Center Endowment: The endowment is dedicated to enhancing dental care for children with disabilities, special needs and early childhood cavities by providing limited funding for children up to age 18. Eligible families are typically uninsured or underinsured and are otherwise unable to obtain dental treatment. Treatment funding is provided at reduced rates. Call Rady Children’s Healthcare Referral at (800) 788-9029 to apply.
SDG&E: Your family may qualify for a discounted energy bill based on your income. See your discharge planner for an application.
Additional Family Resources
San Diego Regional Center: A state-funded program for diagnosing and serving individuals who have developmental disabilities or young children at high risk for developmental disabilities. The Regional Center will provides multiple services including diagnosis, treatment programs, transportation and respite services. For more information, call (858) 576-2996.
Exceptional Family Resource Center (EFRC): EFRC provides families with emotional support, factual information and encouragement in order to help children reach their full potential. Agency services include education and lending library, local, regional and national resources, referral to community-based programs, support groups and disability-specific support groups. For information call (800) 281-8252.
Outreach and Early Intervention Program: This is a family-focused program that provides services to promote optimal development and minimize developmental delays in infancy. One of the services offered is respite care. Ask your discharge planner about a referral for this service.
San Diego Network of Care: A comprehensive resource for services provided in San Diego County. You can access their website at http://sandiego.networkofcare.org.
HowKidsDevelop.com: A collaborative website with information on the Developmental Screening and Enhancement Program (DSEP), Children’s Care Connection (C3), First Five Healthy Development Services Initiative (HDSI) and Rady Children’s Hospital Developmental Services.
Guide to Gastrostomy Tubes - Page 42

Guide to Gastrostomy Tubes - Page 43
Medical GlossaryBalloon port: Allows the balloon to be inflated and deflated.
Bolster: A round plastic disk resting on the skin of your childs tummy which holds the g-tube securely in place.
Bumper: A small rubber disk that lies inside your childs stomach holding the PEG Tube in place.
Clamp: Keeps the tube closed when not in use preventing leakage of milk.
Decompressing the Stomach: Emptying the stomach of air and feedings.
Esophagus: Tube that carries food from the mouth to the stomach.
Feeding port: Where the feeding tube or extension tube will attach to give liquid feeds.
Fundus: The upper part of the stomach.
Fundoplication: A surgical operation that takes the upper portion of the stomach and wraps around esophagus.
Gastric port: Where feeding tube attaches to a g-tube for feeding or medications. Gastric Secretions or Gastric: Stomach secretions and contents.
Gastro-Esophageal Reflux Disease (GERD): gastric secretions going from the stomach into the esophagus.
Gastrostomy: A surgical opening (hole) into the stomach.
Gastrostomy Tube (G-Tube): A tube that is placed into the gastrostomy hole.
Gastro-Jejunal Tube (G-J Tube): A tube that is placed into the gastrostomy hole, into the stomach and then out to the jejunum below. This tube provides access to both the stomach and the jejunum via separated ports.
Jejunum: A tube that lies below the stomach and carries food away.
Jejunal port: Where main feeding tube attaches to a G-J tube for jejunal feeding.
Medicine port: A port for giving liquid medications.
Mic-key bolus extension tube: Tube is used for venting, checking tube placement and bolus feeding.
Mic-key extension tube: This extension tube can be used for venting, checking tube placement and feeding.
Red Robin Tube: A temporary tube that is placed in a gastrostomy hole when the g-tube falls out.
Secur-Lok connector: This end of the extension tube fits directly into the gastric (stomach) and Jejunal ports of the mic-key button tubes.
Silicon balloon: Holds the tube in place when it is inflated with sterile water.
Stoma: A small hole through the abdomen where your child’s g-tube is inserted.
Venting: Burping your child through the g-tube.
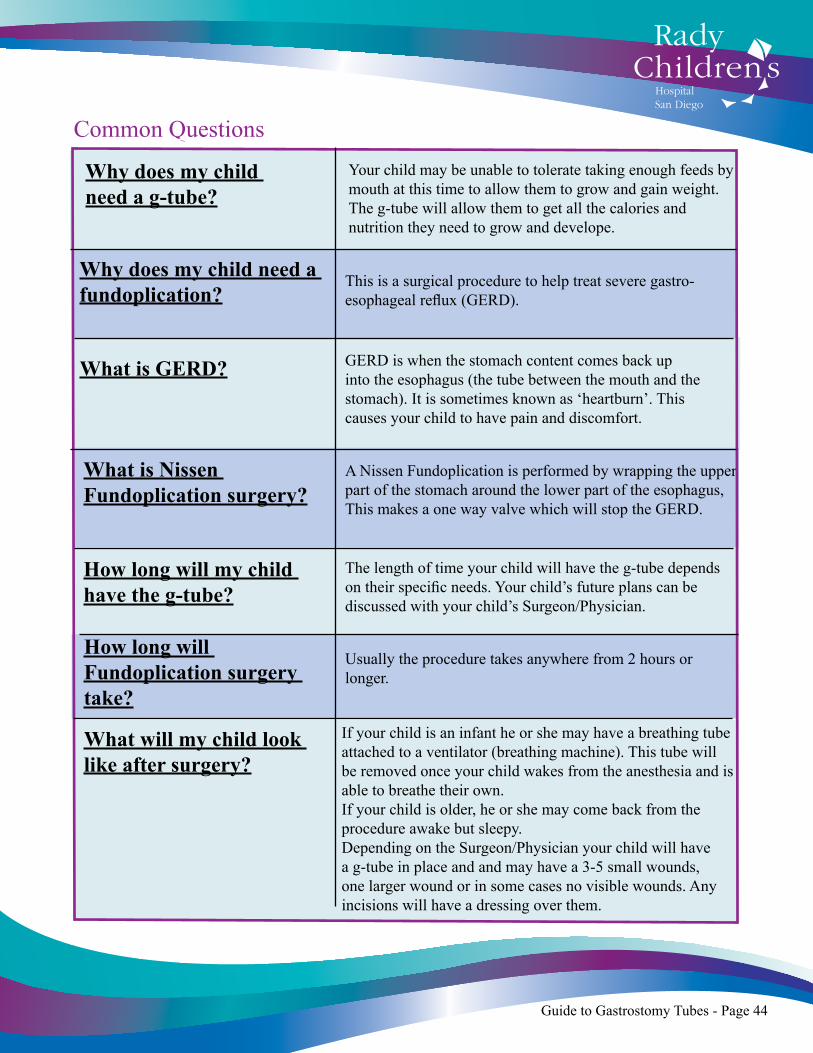
Your child may be unable to tolerate taking enough feeds by mouth at this time to allow them to grow and gain weight. The g-tube will allow them to get all the calories and nutrition they need to grow and develope.
Why does my child need a g-tube?
Why does my child need a fundoplication?
What is GERD?
How long will my child have the g-tube?
This is a surgical procedure to help treat severe gastro-esophageal reflux (GERD).
GERD is when the stomach content comes back up into the esophagus (the tube between the mouth and the stomach). It is sometimes known as ‘heartburn’. This causes your child to have pain and discomfort.
What is Nissen Fundoplication surgery?
A Nissen Fundoplication is performed by wrapping the upper part of the stomach around the lower part of the esophagus, This makes a one way valve which will stop the GERD.
The length of time your child will have the g-tube depends on their specific needs. Your child’s future plans can be discussed with your child’s Surgeon/Physician.
How long will Fundoplication surgery take?
Usually the procedure takes anywhere from 2 hours or longer.
What will my child look like after surgery?
If your child is an infant he or she may have a breathing tube attached to a ventilator (breathing machine). This tube will be removed once your child wakes from the anesthesia and is able to breathe their own. If your child is older, he or she may come back from the procedure awake but sleepy.Depending on the Surgeon/Physician your child will have a g-tube in place and and may have a 3-5 small wounds, one larger wound or in some cases no visible wounds. Any incisions will have a dressing over them.
Common Questions
Guide to Gastrostomy Tubes - Page 44
Common QuestionsContinued
How will a Nissen Fundoplication benefit my child?
The fundoplication will prevent your child from having severe reflux with feeds. This will help to reduce the negative feelings that he/she assosciate with feeding. The g-tube will allow your child to be given the nutrition and fluids they need to grow and develope until they are ready to start eating food by mouth again.
When can I hold my child?
Your child will be sore after surgery and we will make sure that they get adequate pain medication. It is sometimes best to let him/her rest and heal in bed for the first few hours/days after surgery. Discuss with your child’s nurse when you will be able to hold him/her.
When will my child start getting breastmilk/formula through the g-tube?
Once your child has recovered from surgery your doctor will decide when to start feeds. Usually we start with a clear liquid called pedialyte and then progress to breastmilk or formula. We normally start with small amounts of milk given continaully and increase as your child can tolerate it.
Is it safe for my child to eat food or milk by mouth?
Can I give my child a bath when they have a g-tube?
Your child’s Doctor and Occupational Therapist will discuss when it is possible for your child to eat food by mouth. Your Occupaitonal Therapist will show you some exercises to encourage your child’s development and prepare him/her for taking foods by mouth.
Your child can have a tub bath once the incisions and site have healed. This is normally around 14 days after surgery. Discuss with your child’s GI Surgeon/ Physician when your child is safe to start having tub baths.
Guide to Gastrostomy Tubes - Page 45
Constipation can be caused by a change in formula or medication. It can also be caused by a change in feeding schedule. Let your doctor know if constipation continues.
This can be caused if the feeding has gone in too fast, from spoiled formula or breast milk. It can also happen if a new medication or formula is being given. Diarrhea can also be a sign of infection.1. Try giving feed at a slower rate.2. Only keep formula for 24 hours once you have mixed it.3. Keep formula in fridge once it has been mixed.4. Always wash your hands before preparing milk formula.5. Call your doctor if diarrhea continues or your child has any other signs of illness.
This can be caused if the feeding has gone in too fast, if the formula is too cold, too hot or spoiled. It can also happen if a new medication or formula is being given. Vomiting can also be a sign of infection.1. Try giving feed at a slower rate.2. Try warming formula up to room temperature.3. Only keep formula for 24 hours once you have mixed it.4. Keep formula in fridge once it has been mixed.5. Always wash your hands before preparing milk formula.6. Call your doctor if vomiting continues or your child has any other signs of illness.
If your child developes diffculty breathing during or immediately after a feeding, STOP THE FEEDING AT ONCE. Empty the stomach immediately (pg. 21). If breathing problems continue, call 911
Child has constipation
Child has diarrhea
Child is vomiting
Child has difficulty breathing.
Problem Solving
Guide to Gastrostomy Tubes - Page 46
Problem SolvingContinued
This can be caused by thick formulas or medications.1. Try gently flushing with warm water.2. Call your doctor if you are unable to unblock the tube.
Cover, stoma with gauze and get your travel kit. 1. Less than 6 weeks after surgery, cover stoma with gauze and then go to Emergency Dept.2. More than 6 weeks after surgery and you have been trained, place red robin tube and then call Surgeon/Physician and go to Emergency Dept.3. More than 6 weeks after surgery and you have been trained, place g-tube and then call Surgeon/ Physician for follow up care.
Sometimes the medication port of the extension tube starts to become loose and pops off, letting milk leak out.1. Always make sure you push the plug into the medicine port after giving medications and before starting feeds.2. If it continues to leak, change out the extension tube.
Leakage can occasionally occur around the g-tube site and can be caused by feeds being given too fast, too much feed being given, reduced inflation of the balloon and the need for a new larger sized g-tube.1. Try giving feed at a slower rate.2. Check the amount of water in the balloon and top up if needed.3. If your child has suddenly gone through a growth spurt, check with your doctor to see if he/she require a larger g-tube.4. Keep the tube out of your child’s reach to stop them playing and pulling on it. Secure it under his/her clothes.
Tube blocked
G-Tube falls out
Extension tubing Leaking
Leaking around the G-Tube site
Guide to Gastrostomy Tubes - Page 47

Recommended ReadingCaregiver Support;www.KCDigestiveHealth.comwww.tubiefriends.comwww.oley.org www.mic-key.com/facebookwww.mic-key.com/blogwww.mealtimenotions.orgwww.emdn-mitonet.co.uk/PDF/bookGTube.pdf (Helpful book for older children!)
Acknowledgements; Photographs ... Linda Black RNC - NIC, CLE, RNMConcept, Design and Layout ... Linda Black RNC - NIC, CLE, RNMCollaborative Team .. Rady Children’s Hospital Tips and Tubes Committee 2014
References:Reckling, A, PsyD. (2007) When Jeremy Jones’ Stomach Stopped Working. Mitochondrial Disease Action Committee. http://www.mitoaction.org/pdf/bookGTube.pdf
Mic-Key Tube Care and Usage (2010). Kimberly-Clark Worldwide, Inc.http://www.mic-key.com/resources/mic-keystar-care--usage-guide.aspx
Su W, Berry M, Puligandla PS, Aspirot A, Flageole H, Laberge JM. Predictors of gastroesophageal reflux in neonates with con-genital diaphragmatic hernia (2007). http://www.ncbi.nlm.nih.gov/pubmed/17923189
History of the Nissen Fundoplication (2011). TEF/Vater Internatioanl. http://www.tefvater.org/esophageal/fundoplications.html
Cu S, BS; Sidman J, MD. Rates and Risks of Gastrostomy Tubes in Infants With Cleft Palate (2011). http://archotol.ama-assn.org/cgi/content/abstract/137/3/275
Fundoplication - Open Surgery (2005). EBSCO Publishing.http://www.doctorsofusc.com/condition/document/14813
Minard G, MD. The History of Surgically Placed Feeding Tubes (2006).http://ncp.sagepub.com/content/21/6/626.abstract
Gastrostomy Tubes (2011). The Regents of the University of California. http://pedsurg.ucsf.edu/conditions--procedures/gastrostomy-tubes.aspx
Agrawal S. All About NJ, GJ, and J Tubes (2009). Complex Child E-Magazine.http://www.articles.complexchild.com/oct2009/00158.pdf
Sexton E, Holden C. Jejunostomy Tubes (2007). Tracheo-Oesophageal Fistula Support. http://www.tofs.org.uk/index.php/what_is_tof_oa/procedures/jejunostomy_tubes
Enteral Feeding: Enteral Feeding Tubes & Accessories (2009). Kimberly-Clark Worldwice, Inc. http://kchealthcare.or-live.com/digestivehealth/enteralfeeding/product/acc.cfm
Would Ostomy and Continence Nurses Societyhttp://www.wocn.org
Guide to Gastrostomy Tubes - Page 48
My Journal
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
Guide to Gastrostomy Tubes - Page 49
My Journal
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
Guide to Gastrostomy Tubes - Page 50

3020 Children’s WaySan Diego, CA 92123
(858) 966 1700www.RCHSD.org