governing body - nhs sutton ccg board... · x the fire alarm is a continuous single tone and if it...
TRANSCRIPT

SUTTON CLINICAL COMMISSIONING GROUP
GOVERNING BODY
Wednesday 2nd
March 2016
2:00pm–5:00pm
Meeting Room 1,
Priory Crescent,
Cheam, SM3 8LR

SUTTON CLINICAL COMMISSIONING GROUP
GOVERNING BODY
Wednesday 2nd March 2016
(Part 1, 2:00pm-4.00pm, Part 2, 4.15pm-5.00pm)
Meeting Room 1, Priory Crescent, Cheam, Sutton SM3 8LR
AGENDA - PART I
Chair: Dr Brendan Hudson
Presented by ENC
WELCOME & INTRODUCTIONS
1. Welcome & Apologies for Absence
Dr Brendan
Hudson
2. Venue Safety Announcement
Dr Brendan
Hudson 01
3. Register of Declared Interests
Governance Body members are asked to declare if their entry
upon the Register of Declared Interests (attached) is not a full,
accurate and current statement of any interests held.
Dr Brendan
Hudson 02
4. Minutes of previous meeting
To approve the minutes of the Sutton Clinical Commissioning
Group Governing Body meeting held on 6th January 2016.
Dr Brendan
Hudson 03
5. Matters Arising
To review any matters arising and the action log following the
meeting held on 6th January 2016.
Dr Brendan
Hudson
04
FOR APPROVAL
6. GP and CCG IT Procurement
Jonathan Bates 05
7. Delegation of Primary Care Commissioning / Governance of
Primary Care Committee
Dr Brendan
Hudson 06
8. Practice Engagement in Clinical Commissioning 2016/17
Jonathan Bates
/ Paul Sarfaty 07
9. Review of Investments & QIPP 16/17 Geoff Price /
Jonathan Bates 08
FOR DISCUSSION
10. 2016/17 Operating Plan - update
Geoff Price 09
11. Contracting Round - update
Geoff Price Verbal
12. Performance & Quality Report
Jonathan Bates 10
AG
EN
DA

Page 2 of 2
13. Finance Report: Month 10
Geoff Price 11
14. QIPP Report: Month 9
Jonathan Bates 12
15. Board Assurance Framework
Geoff Price 13
FOR INFORMATION
The remaining items are for note only and no discussion is anticipated unless
matters have been raised with the Chair in advance of the meeting.
16. Approved Minutes of Committees of the Sutton CCG
Governing Body
Executive Committee: 16.12.15, 13.01.16, 27.01.16,
10.02.16
Finance Committee: 18.11.15, 16.12.15
Quality Committee: 19.11.15, 17.12.15
SWL Joint Committee for Primary Care: 12.11.15
14
17. Questions from the Public
Members of the public can submit questions relating to the
agenda if raised with the Chair 48 hours prior to the meeting. The
Chair will make every effort to ensure questions are responded to
at the meeting however there may be occasions where time
constraints preclude this. If a question cannot be answered at the
meeting, or a fuller response is required, a written reply will be
sent as soon as possible.
Dr Brendan
Hudson
18. Any Other Business
19. Meeting Close
20. Date of Next Meeting
The Sutton Clinical Commissioning Group Governing Body meets
bi-monthly on Wednesday afternoons. The usual start time will be
2.00pm, with occasional need to extend the meeting time.
The next meeting will take place on Wednesday 4th May 2016,
2.00pm, at Priory Crescent, Cheam, Sutton SM3 8LR.
Closure of Part I
To resolve that the public now be excluded from the meeting, on the basis that publicity would be
prejudicial to the public interest by reason of the confidential nature of the business to be
conducted in the second part of the agenda.
AG
EN
DA

MEETING ROOM 1 SAFETY NOTICE
PRIORY CRESCENT
For the purpose of this safety notice the wall on which the screen is situated is
deemed to be the front
The emergency exit is marked and is to the left of the room
The toilets are in the front of the room to the left of the screen
A Fire alarm is not scheduled during this meeting
The fire alarm is a continuous single tone and if it does sound we should all leave the building
by the emergency exit
The emergency assembly point is on the footpaths out on Priory Crescent
Please do not block the access for emergency vehicles
If you are aware of anyone with a sight or physical impairment please offer them assistance
No one should re-enter the building unless the Fire Marshall (IN HIGH VISBILITY JACKET)
declares it safe to do so
Screen
Entrance /
Alternative exit
Toilets
Entrance /
Emergency Exit
EN
C 0
1

Sutton Clinical Commissioning Group – Governing Body Register of Declared Interests 2014/15 (date of most recent update 22/05/15)
All interested declared as of 01.04.14 unless otherwise stated
Details Start date with CCG: 01.04.13 unless otherwise stated
Interest
Governing Body Members
Dr Brendan Hudson Clinical Chair
Partner and Principal of The Grove Practice,
83 Grove Road, Sutton, SM1 2DB
Member of British Medical Association,
RCGP and Liberal Democrats
Wife - Tutor at Carshalton College
Occasional Interviews with Sutton Guardian
Newspaper
Former Councillor for Sutton Council
Member of Sutton GP Services Ltd
Dr Chris Elliott Clinical Chief Officer
Sutton Healthcare Services - Director
Benhill and Belmont GP Practice -Partner
Member of Sutton GP Services Ltd
Nominated GP for an intermediate care residential facility in Sutton
Jonathan Bates Chief Operating Officer
No interests declared
Paul Sarfaty Lay Member: Chair of the Audit Committee/ Vice Chair
Feughside Limited – Director
Air Products & Chemicals Inc. (APD) - Shareholder
Consultant for Caldwell and Braham, a firm of Chartered Accountants based in the City of London.
EKF Diagnostics Holdings plc: Shareholder
Geoff Price Chief Finance Officer
No interests declared E
NC
02

Sutton Clinical Commissioning Group – Governing Body Register of Declared Interests 2014/15 (date of most recent update 22/05/15)
All interested declared as of 01.04.14 unless otherwise stated
Sally Brearley Lay Member: Patient and Public Engagement Lead and Chair of the Quality Committee
National Nursing Research Unit, Kings
College London - Visiting fellow
Member, NHS England Clinical Priorities
Advisory Group.
Chair, NHS England London Region Health
in the Justice System Patient and Public
Voice Group.
Fellow in Patient and Public Involvement,
Faculty of Health, Education and Social
Care, Kingston University and St George's
University of London.
Member of the South London Health
Innovation Network Musculoskeletal
Advisory Board.
Patient representative, NHS 11
Futures/Digital Urgent Care Board.
Dr Les Ross Secondary Care Consultant Member
No interests declared
Dr Jonathan Cockbain GP Board Member
GP Partner – Chesser GP Practice
Member of Sutton GP Services Ltd
Dr Dino Pardhanani GP Board Member
GP Partner - Mulgrave Road
Dr Nicola Lang Director of Public Health Start date 02.06.14
Director of Public Health – London Borough of Sutton
Offender health work with NHS England on offender-related issues
Director of Public Health Lead for Offender Health, London ADPH
Karol Selvey Primary Care Nurse Board Member
Nurse Practitioner/Partner at The Old Court House - Dr Grice & Partners
Member of Sutton GP Services Ltd
EN
C 0
2

Sutton Clinical Commissioning Group – Governing Body Register of Declared Interests 2014/15 (date of most recent update 22/05/15)
All interested declared as of 01.04.14 unless otherwise stated
Participating Observers
Details Interest
David Williams Healthwatch
Chair of Old Court House Surgery Patient Participation Group
Chair, Patient Reference Group
Healthwatch Sutton - Director
Appearances on Radio St Helier on behalf of Healthwatch Sutton
My son is a Planning Officer with the London Borough of Sutton
Dr Lindsey Roberts Local Medical Committee
Salaried GP Wallington Family Practice
Lead with in practice for anticoagulation
service and IUCD/implant service.
My husband is a consultant cardiac surgeon
working for UCLH
Director of Roberts Medical Limited
Mrs Gillian Bennett Patient Reference Group
Representative for the Grove Road GP
Surgery on the Patients’ Representative
Group
Shareholdings in Astrazeneca
EN
C 0
2

`
Page 1 of 12
Minutes of Part 1 of the Sutton Clinical Commissioning Group Governing Body
Wednesday, 6th January 2016 Priory Crescent, Cheam, SM3 8LR
Chair: Dr Brendan Hudson JB Jonathan Bates Chief Operating Officer SB Sally Brearley Lay Member JC Dr Jonathan Cockbain Clinician/GP Board Member CE Dr Chris Elliott Chief Clinical Officer BH Dr Brendan Hudson Chair/Clinical Leader NL Dr Nicola Lang Director of Public Health - London Borough of Sutton DP Dr Dino Pardhanani Clinician/GP Board Member GP Geoff Price Chief Finance Officer LR Les Ross Secondary Care Consultant PS Paul Sarfaty Lay Member: Audit & Governance Lead KS Karol Selvey Nurse Practitioner Participating Observers: DW David Williams Healthwatch Sutton Director In Attendance: SH Sian Hopkinson Director of Performance & Primary Care MH Mary Hopper Director of Quality KM Kay McCulloch Programme Director, SWL Collaborative Commissioning CR Carolyn Reynolds Head of Primary Care Commissioning SR Sue Roostan Director of Commissioning - SCCG JW Jane Walker Head of Corporate Governance LR Dr Lindsey Roberts Local Medical Council representative Apologies GB Gillian Bennett Patient Reference Group
WELCOME & INTRODUCTIONS
1. Welcome & Introductions BH welcomed all present.
2. Venue Safety Announcement BH informed the meeting of all necessary procedures and facilities.
3. Register of Declared Interests BH requested the Governing Body members to declare if their entry upon the Register of Declared Interests, attached to the agenda, was not a full, accurate and current statement of any interests held. DP confirmed that he was no longer a nominated GP for an intermediate care residential facility in Sutton and asked for the Register of Interest to be amended.
JW
EN
C 0
3

`
Page 2 of 12
It was also noted that all Sutton CCG practices were mentioned in the Estates Strategy at item 6 on the agenda. There were no further declarations made by members of the Governing Body.
4.
Minutes of previous meetings The minutes of the Sutton Clinical Commissioning Group Governing Body meeting held on Wednesday 4th November 2015, were agreed as an accurate record, noting a couple of minor typographical errors which would be amended.
5. Matters arising & action log Matters Arising Primary Care Delegation – Application to NHS England BH confirmed that that he had discussed the issue of training with regards to primary care commissioning committees for both CCG clinical members and also patient groups with other CCG Chairs across SWL who agreed that a training plan would be need to be put into place. Final Devolution Collaborative Agreement JB introduced the Final Devolution Collaborative Agreement which had been submitted to the Governing Body at its November meeting in draft form. The Governing Body delegated final approval to the CCG Chair who duly signed off the final documents. On 15th December, London’s CCGs, London Councils, the GLA, NHS England London Region and Public Health England London Region agreed to work closely together to go further and faster in integration and collaboration using devolution as a tool to achieve this. National bodies – including NHS England and Public Health England - and central government have agreed to support this agenda by being active partners in the pilots and demonstrating their commitment to health and care devolution in London. JB summarised the three documents circulated to Governing Body members:
- London Health & Care Collaboration Agreement - London Health Devolution Agreement - Summary for CCG Chief Officers & Chairs including
challenges and opportunities of devolution. JB stated that although all three documents where pertinent, section 9 of the London Health & Care Collaboration Agreement setting out governance and section 10 and 11 outlining the programme of work associated resources were particularly important for the Governing Body to note.
EN
C 0
3

`
Page 3 of 12
BH confirmed that all SWL CCGs had signed up to the Devolution Collaborative Agreement. NOTED The Governing Body NOTED the final version of the documentation, signed off under Chair’s Action. Action Log It was noted that all the actions on the action log had now been completed and would be updated and submitted to the next meeting of the Governing Body.
FOR APPROVAL
6. Estates Strategy GP introduced the final draft Estates Strategy which was required to be submitted to NHSE by the end of December 2015. GP confirmed that an earlier draft had been submitted to the Executive Committee on the 25th November and to the Board Seminar on 2nd December 2015. Comments received following both these meetings had now been incorporated into the draft together with the primary care sections being expanded and updated. GP highlighted the fact that bids for capital development 2016/17 would now be to the Primary Care Transformation Fund. NHSE had written to CCGs, included at Appendix 2.1 of the draft strategy, Primary Care Transformation Fund – Approach to Funding 2016 to 2019 setting out the proposals for primary care estates development which would require CCG sign off and financial support. It was noted that the development of an integrated NHS Estates Strategy for South West London was expected to be completed during 2016. GB stated that the Strategy was a dynamic document that would be refined on an on-going basis. Governing Body members raised the following key points:
- It was noted that processes were in place at A&E departments to encourage and support non-registered patients to register with a GP. SR confirmed that Sutton CCG had a lower rate of unregistered patients to other neighbouring CCGs.
- The Estates Strategy was initially focusing on Primary Care but would take forward work around Acute and Mental Health in due course.
- It was noted that many practices had worked hard to improve their practices and the Strategy would look at
EN
C 0
3
`
Page 4 of 12
where it may or may not be feasible to move practices to more appropriate facilities, especially those practices still working out of outdated or inappropriate premises.
APPROVED The Governing Body RATIFED the Estates Strategy.
7. Public Sector Equality Duty Annual Report MH introduced the CCG’s annual public sector equality report which was due to be published by 31 January 2016. The report highlights the progress made in respect of Equality and Diversity responsibilities between January and December 2015. The activities highlighted within the report identify how the CCG is meeting the three aims of it general equality duty:
Eliminate unlawful discrimination, harassment and victimization,
Advance equality of opportunity, and
Foster good relations between those who share a protected characteristic and those do not.
MH stated that one of the specific duties under the Equality Act 2010, was that public bodies must publish annually by the given date (January 31) showing how they are meeting the general equality duty. APPROVED The Governing Body APPROVED the Public Sector Equality Duty Annual Report.
8. South West London (SWL) Collaborative Commissioning – Governance Proposals for Phase of Programme Delivery CE presented a number of slides which introduced a paper setting out proposed governance arrangements for a single programme of work across South West London and Surrey Downs, which the CCG Governing Body were asked to review and approve. The paper included:
Proposed governance structure, roles and responsibilities
Terms of Reference for Programme Board
Terms of Reference for Clinical Board
Description of the role of the Tripartite in the Programme It was noted that the Terms of Reference for the Finance & Activity Committee had now been agreed and would be circulated to the Governing Body. The slides included details on:
Developing a single programme of work
KM
EN
C 0
3

`
Page 5 of 12
Leadership and programme management
Role of the Tripartite
Proposed governance structure.
BH stated that he was please to see that Clinical Leads had been included on the Programme Board. Governing Body members also noted that PPI representatives would be invited to the care pathway groups where it was felt that they would add more value. APPROVED The Governing Body Approved the proposed Governance arrangements.
9. Planning for Commencement of the Local Audit Arrangements PS introduced a letter dated 24th December 2015, from NHS England, in relation to Planning for Commencement of the Local Audit Arrangements. The Department of Health announced in September that health bodies would move to the new audit framework in 2017/18 under the Local Audit and Accountability Act 2014. This means that NHS Trusts and CCGs would select and appoint their own auditors and directly manage their contracts for the audits for the financial year starting in April 2017, with the legislation requiring that the auditors are appointed by 31 December 2016. The first stage of the new process was for CCGs and NHS Trusts to set up Auditor Panels, to advise and oversee the auditor appointments. The recommended solution is that the CCG uses the members of
the Audit Committee as that panel. To do so, a Board resolution is
required to approve the establishment of the panel.
PS confirmed that Sutton CCGs current External Audit
arrangement with Grant Thornton ended on 1st April 2017 and
there was a requirement to appoint a new External Auditor by the
end of December 2016.
PS also confirmed that this arrangement would also cover the
Merton & Sutton Charitable Funds.
APPROVED
The Governing Body approved the establishment of the
Auditor Panel made up of members of the Audit Committee
and agreed for this Panel to appoint External Auditors by the
end of December 2016.
EN
C 0
3

`
Page 6 of 12
10. Healthy London Partnership – Beyond 15/16 JB introduced a paper which provided a summary of programme progress and outlined the proposed governance arrangements for the future. JB stated that since the launch of the Collaborative Transformation Programme Prospectus in March 2015, the Healthy London Partnership had established itself in line with the agreed operating model and mobilising the thirteen collaborative programmes. In mobilising the programmes, extensive engagement with CCGs and SPGs has taken place to ensure alignment of programmes across the commissioning system. Feedback was clear that pan-London activity should build on local work and demonstrate value; HLP programme leads therefore tested scope, deliverables and timelines with their respective CCG and SPG leads and revised where necessary. Governing Bodies were being asked to:
NOTE the progress to date of the Healthy London Partnership
AGREE to support longer term commitment to the Health London Partnership for 2016/17 and 2017/18
AGREE the proposed planning process and the financial planning assumption for 2016/17 and 2017/18
AGREE proposed ongoing governance arrangements AGREED The Governing Body agreed the recommendations as detailed above.
FOR DISCUSSION
11. South West London (SWL) Collaborative Commissioning Programme Update KM attended the meeting and provided a further update on the SWL Collaborative Commissioning Programme including progress on the following areas which were priority for the next three months:
The set up of the Strategic Planning Group
Agreement of the financial baseline
Out of Hospital level of ambition
Acute provider work
Clinical service model definition
KM agreed to ask the communications team to produce ‘easy read’
summaries of the updates.
PS raised concern as to the current financial situation, especially
for acute trusts, and whether the Programme was realistic.
EN
C 0
3
`
Page 7 of 12
The Governing Body noted the update.
12. 2016/17 Planning Guidance and Draft CCG Plan SR presented a paper which sets out the first draft plan on a page and includes the ‘Delivering the Forward View: NHS planning guidance 2016/17 - 2020/21, which was received on the 22nd December 2015. The plan on a page is the first draft and does not include the CCG vision for the coming year; this is still in development and will be included at a later stage. It does include three additional areas that have been deemed priority areas for the CCG. These are: Sutton Homes of Care, Children’s services and Primary care. SR confirmed that the draft will be updated to reflect the current guidance once the technical guidance was released and will also be dependent on the allocation of funds received by Sutton CCG. SR stated that the key focus of the planning guidance was that all systems are required to submit sustainability and transformation plans that are system wide i.e. SW London by the end of June 2016. One year organisational plans would be required although these would need to complement the transformation plans and triangulate across the system. The first draft of these plans was required by the end of February 2016 with final plans completed by the 11th April 2016. The final plan would need to be approved by the Governing Body. JB stated that the scale of the work was a real challenge and recognised the pressure in the system especially for SR and her team. GP confirmed that the CCG would be informed of their financial allocation over the next couple of weeks. NOTED The Governing Body noted the first draft plan on a page and the potential impact for Sutton CCG in relation to the new planning guidance.
13. Primary Care Full Delegation – Outcome of Financial Due Diligence GP presented the financial due diligence review that had been requested by Sutton CCG to help the Governing Body to consider the financial risks associated with the proposed transfer of responsibilities for the management of primary care contracts from NHS England.
EN
C 0
3

`
Page 8 of 12
This review concluded that there was a level of financial risk to the CCG in taking on Level 3 delegated commissioning responsibility. The level of risk is related to the budget setting process, QIPP requirements and the historic approach to accruing for costs at a GP Practice level. A number of recommendations have been made in this document to help the CCG mitigate these risks. JB stated that the risks identified needed to be considered in the context of the opportunities that Level 3 delegated commissioning may provide, such as the scope for improved system-wide pathway management is significant and should be weighed up against the likely short-term financial challenge that the CCG would inherit if they decide to proceed with Level 3 delegation. GP confirmed that the second component of due diligence, relating to legal matters, had not yet been received. The GP Plenary would have access to this information in February and it will be shared with Governing Body Members when it becomes available. It was noted that the Governing Body would want to take account of the previous shared wider benefits of delegated primary care commissioning informing a final view. JB stated that following review of the due diligence it was felt that the CCG should ask NHS England to indemnify the CCG for past rent review gaps. The Governing Body agreed and requested that the recommendations of the paper be amended to reflect this. JB confirmed that running costs would not increase if the CCG took on the responsibility of delegated primary care commissioning and there was a risk around the capacity of the organisation especially around the knowledge and understanding of primary care budgets. GP stated that there was a need to manage expectations of practices and there was a need for Governing Body members and clinical leads to work with practices to ensure they are aware of the situation. The Governing Body were asked to:
consider the points set out in this paper and the broader
context to move to individual CCG delegated commissioning
make a recommendation for consideration by the Plenary of
Members at their meeting on 28th January 2016
inform SWL Collaborative Commissioning the outcome of
your discussion, so that the implications for the SWL Joint
Committee for Primary Care Co-Commissioning can be
discussed by all Chief Officers and Chairs.
GP
GP
EN
C 0
3

`
Page 9 of 12
To ask NHS England to indemnify the CCG for past rent
review gaps.
AGREED The Governing Body agreed the recommendations as detailed above.
14. Performance & Quality Report: Month 5 JB presented the month 6 report to inform and provide assurance to the Governing Body about the performance, quality and safety of service provision commissioned by NHS Sutton CCG. JB highlighted the following key areas:
Performance against referral to treatment time (RTT) target achieved at aggregate level for every month of 2015/16
Cancer waiting times and continued pressure on 62 day wait standards and progress against action plan at Epsom and St Helier Trust
Diagnostic test waiting time standard achieved in Month 6
In September there were 2 patients breaching the 52 week standard
A&E 4 hour wait pressures at Epsom and St Helier and St George’s in Month 6
London Ambulance Service failure to meet response time standards at London level, however improving performance in Sutton
Healthcare Acquired Infection rates are within thresholds
Improving Access to Psychological Therapies performance is achieving waiting time standards, but not meeting access or recovery standards
Dementia diagnosis rate has increased to over 61.5% but remains below national target
SWL Sector CCGs’ Contracted Mental Health Performance (Appendix 2). Access for Working Age Adults and Older People is not meeting waiting time standards.
GP Out of Hours service is achieving all performance standards (Appendix 3)
CQC inspection of Epsom and St Helier University Hospitals NHS Trust in November, with report expected to be published in spring of 2016. Concerns have been raised in relation to Critical Care Services at the trust and the CCG is extensively involved in quality improvement plans to ensure these services are fit for purpose.
CQC report published for London Ambulance Service: whilst the report gave the Service a ‘good’ rating for its care of patients, it highlighted a number of areas of concern and rated the service to be ‘inadequate’ overall. The NHS Trust Development Authority has placed the service into special measures.
EN
C 0
3

`
Page 10 of 12
JB stated that details in relation to the Quality Premium had already been circulated to the Governing Body. RTT JB stated that following previous discussions at Management Team and the Executive Committee it was agreed to explore the possibility of improving 18 week referral to treatment times at Epsom and St Helier Trust (ESTH). It was also agreed in principle that this would be funded up to a maximum of £1M. In order for ESTH to improve performance additional activity with the independent sector may need to be commissioned. JB stated that this will improve the SCCGs resilience for meeting the RTT constitutional standard.
NOTED The Governing Body noted the report and agreed to explore the possibility of improving 18 week referral to treatment times together with funding up to a maximum of £1M.
15. Finance Report: Month 6 GP presented the finance report which stated that the CCG was reporting on plan year to date (the 9 months ended 31 December 15) and full year forecast. The report uses month 07 prescribing and month 08 acute data as the basis for M09 reporting. In terms of the full year forecast, overall the CCG was reporting meeting plan for both program and running costs for year to date and full year forecast. The Governing Body noted the following key points:
A full year forecast overspend on continuing health care costs of £3.2 million
Overall acute spend was forecast to be in line with contracts. A year end agreement was reached with ESH and SWLEOC in December 15.
A full year forecast overspend on Mental health and Learning Disability services of £700k mainly due to high cost placements.
A full year forecast underspend on prescribing of £250k
Overall QIPP savings targets were being met
All other commissioned services were on plan.
The net overspend of £3.3 m is covered by reserves.
GP was pleased to inform the Governing Body that the CCG had been informed of its 201516 Charge Exempt Overseas Visitor allocation which corrects the shortfall in allocation received in 201415.
EN
C 0
3

`
Page 11 of 12
NOTED The Governing Body noted the report.
16. QIPP Report: Month 8 JB introduced the QIPP report for month 8. The current forecast outturn was 99.9% of the net target. This represented almost no change in the year end position as forecast at M7 (100.4%). The year-to-date achievement was ahead of plan (107%) at M8, an improvement on M7 (104%). It was noted that many of the schemes were performing at or above plan. NOTED The Governing Body discussed and noted the QIPP report.
17. Board Assurance Framework GP presented the Board Assurance Framework (BAF) which sets out the principal risks to CCGs objectives and how these risks are being managed. It was noted that the risks had recently been reviewed with risk owners and updated accordingly. The report highlighted any changes since the last report in terms of additions and deletions and changes to risk scores. JB stated that it was important for Governing Body members to note that the CCG currently have five red risks compared to one at the same time last year. GP confirmed that a more detailed report on the BAF had been discussed at the Audit Committee on 3rd December 2015 The Governing Body noted and reviewed the BAF.
18. Chief Clinical Officers Report CE thanked all CCG staff for their ongoing support and hard work which was recognised by the Governing Body. CE reported that the CCG was now attracting National attention with regards to the Sutton CCG Vanguard.
FOR INFORMATION
19. GP and CCG IT Procurement Update The Governing Body noted the update which provided details of the draft timeline for the Procurement, the membership of the SWL IT LPF Collaborative Working Group and the proposed membership of the Sutton CCG IT Project Board. The Governing Body noted the update.
EN
C 0
3

`
Page 12 of 12
20. Safeguarding Adults Policy and Prevent Policy Sutton CCG
The Governing Body noted the Safeguarding Adult Policy and the Prevent Policy for Sutton CCG, which ensure organisational compliance with the Care Act 2014 and the Prevent Duty Statutory Guidance 2015. This Policy had been approved at the December meeting of the Quality Committee. The Governing Body noted the policy.
21. Governing Body Member and Sutton & Cheam Locality Lead
Appointments
The Governing Body were pleased to note the appointment of
Pippa Barber to the post of Governing Body Member - Independent
Nurse. Pippa had confirmed her start date with Sutton CCG as of
the 2nd March 2016.
BH also advised the Governing Body that Dr Senthooran
Kathirgama Kanthan had been appointed to the post of Sutton and
Cheam Locality Lead.
22. Approved Minutes of Committees of Sutton CCG Governing Body The Governing Body received and noted the approved minutes of the following committees:
Executive Committee: 11.11.15, 25.11.15, 09.12.15
Finance Committee: 21.10.15
Quality Committee: 15.10.15
SWL Joint Committee for Primary Care: 03.09.15
22. Questions from the Public BH advised the Governing Body that a question had been received from The Patients Group at Wells Court Surgery. This was attached at Appendix 1 to the minutes. A written response would be actioned outside of the meeting.
BH
23. Any Other Business There was no further business to discuss.
24. Meeting Close Part one of the meeting closed at 4.00pm.
25. Date of next meeting The next meeting will take place on Wednesday 2nd March 2016, 2pm at Sutton CCG, Priory Crescent, Cheam, Sutton SM3 8LR.
EN
C 0
3


Sutton CCG Governing Body - Matters Arising /Action Points from previous meetings.
Date Item Title and Action Required Lead Comments Status
6 Jan 2015 3 Register of Declared Interest
JW To amend Register to reflect changes to DP declaration of interest.
Register updated and attached to March GB papers.
6 Jan 2015 8 SWL Collaborative Commissioning – Governance Proposals
KM To circulate the ToR for the Finance & Activity Committee to the Governing Body members.
To be circulated once received from KM.
6 Jan 2015 12 Primary Care Full Delegation – Outcome of Financial Due Diligence
GP Second component of due diligence, relating to legal matters, to be shared with Governing Body members. Ask NHSE to indemnify the CCG for past rent gaps.
Circulated.
GP to provide a verbal update
at GB meeting in March.
6 Jan 2015 22 Question from the public BH To provide written response to the question received from The Patients Group at Wells Court Surgery.
Actioned.
EN
C 0
4

1
Report to the Sutton Clinical Commissioning Group Governing Body
Date of Meeting: 2nd March 2016 Agenda No: 6 ENCLOSURE: 05
Title of Document: GP and CCG ICT procurement
Purpose of Report: For Approval
Report Authors: Sian Hopkinson, Director of Performance & Primary Care
Lead Director: Sian Hopkinson
Executive Summary:
The procurement of ICT services for GP practices and the CCG corporate functions is underway and the timeline is shown below:
16/3/2016 Final moderation meeting; Preferred bidder for South West London IT Lead Provider Framework (LPF) Call-off contract agreed by Merton, Sutton and Wandsworth CCGs
18/3/2016 NHS England’s LPF support team to provide CCG Governing Bodies with report on outcome
24/3/2016 (12 noon)
CCG Governing Bodies to have ratified decision
24/03/2016 Notification to suppliers of LPF procurement outcome
25/03/2016 - 04/04/2016
Standstill period
5/4/2016 Preferred bidder announced
1/8/2016 Commencement of new service
Key sections for particular note (paragraph/page), areas of concern etc: Note the timeline outlined above.
Recommendation(s): The Governing Body is requested to:
NOTE the timeline outlined above and in particular the requirement for the Governing Body to ratify the decision by noon on 24th March 2016.
APPROVE the proposal that the ratification is delegated to Governing Body members, due to time sensitivity and that these members are the Chair, Dr Brendan Hudson; GP Member, Dr Dino Pardhanani; and Chief Operating Officer, Jonathan Bates.
Committees which have previously discussed/agreed the report: Executive Committee 24/2/16
EN
C 0
5

2
Financial Implications: The affordability caps for the services specified are:
GP ICT £400k pa
CCG ICT £90k pa
It is therefore expected that the reprocurement of CCG ICT services will generate a saving on the current budget of approx. £114k (full year effect). The GP ICT budget for 2016/17 is currently set at £483k and it is expected that this will continue to be required for the entirety of ICT services in general practice. The service specification is for core services only, with additional services funded separately from the main service level agreement.
Equality Impact Assessment: The CCG is committed to monitoring the compliance with the Equality duty of the providers from whom we commission services.
Information Privacy Issues: The procurement is currently underway so no further details can be shared until the process is complete.
Communication Plan: Contract award will be announced at the May 2016 Governing Body meeting, held in public.
EN
C 0
5

Page 1 of 15
Report to the Sutton Clinical Commissioning Group Governing Body
Date of Meeting: 2nd March 2016 Agenda No: 7 ENCLOSURE: 06
Title of Document: Delegated Commissioning of Primary Care - Outcome of Plenary and Planning for 1st April 2016
Purpose of Report: For Review and Comment
Report Authors: Siân Hopkinson, Director of Performance & Primary Care Carolyn Reynolds, Head of Primary Care Commissioning
Lead Director: Siân Hopkinson, Director of Performance & Primary Care
Executive Summary: Sutton CCG GP Practices voted at a Plenary of Members on 16th September 2015 to submit an application for delegated commissioning of primary care from April 2016. The Member Practices considered the due diligence reports at a further Plenary on 11th February 2016 and voted in favour of continuing with plans to take on this responsibility. Notes of the Plenary are included as Appendix 1. The governance arrangements require the establishment of a dedicated Primary Care Committee aligned to national guidance. The Terms of Reference for the Primary Care Commissioning Committee, which also describe the membership of the Programme Board are attached as Appendix 2. It should be noted that these will be reviewed every six months for the first year of delegation and annually thereafter. The CCG submitted their Delegation Agreement for signing by NHS England on 26th February 2016. Further information is available here: https://www.england.nhs.uk/commissioning/pc-co-comms/resources/delegation-agreement-qas/
Key sections for particular note (paragraph/page), areas of concern etc: The membership of the Primary Care Commissioning Committee is at page 9 of this report and of the Primary Care Programme Board is at page 13.
Recommendation: The Sutton CCG Governing Body is asked to:
NOTE the support for delegation from the Plenary of Members
APPROVE the establishment of a Primary Care Commissioning Committee which will be decision making, as described in the attached Terms of Reference
EN
C 0
6
Page 2 of 15
Committees which have previously discussed/agreed the report: Previous versions of the Terms of Reference have been discussed by the Executive Committee and Governing Body Seminar. This report was discussed at the Executive Committee on 24/2/16
Financial Implications: Primary care commissioning will bring additional financial responsibilities and risks.
Equality Impact Assessment: The CCG is committed to monitoring the compliance with the Equality duty of the providers from whom we commission services. This is done through the quality and contracting process.
Information Privacy Issues: The information contained in this report will be in the public domain when presented to the Governing Body. The Primary Care Commissioning Committee will meet in public.
Communication Plan:
EN
C 0
6

Page 3 of 15
APPENDIX 1 NOTES TAKEN AT THE PLENARY
THURSDAY 11TH FEBRUARY 2016
Background GP members named in the Sutton CCG Constitution attended the Plenary on Thursday 11th February 2016 and were asked to: Review the due diligence reports and confirm their support for the CCG to continue with its application for delegation of primary medical services from NHS England from 1st April 2016 Executive summaries of both the legal and financial due diligence reports were sent out to all practices two weeks prior to this meeting. The following questions and answers were raised at the meeting:
Questions
Answers
Concern raised that there are no working GPs on the Primary Care Committee that is a sub group of the Governing Body and will make final decisions on primary care.
The CCG has based Committee membership on guidance for managing conflicts of interest. The membership of this Committee includes an independent GP advisor and the LMC and a salaried Sutton GP are included as non voting attendees to bring views from general practice. There will also be a Primary Care Programme Board that will replace the current steering group. This will include a practice nurse, practice manager, independent GP, GP partner salaried GP and will make recommendations to the Primary Care Committee. The LMC are represented on both groups and commended the CCG for allowing them to have such a presence. Membership and terms of reference for these groups will be reviewed every six months during the first year.
EN
C 0
6

Page 4 of 15
Questions
Answers
Not sure why the CCG needs to go for delegation now – why not go in shadow form for one more year to try and improve the position from NHSE
If we delay for another year, we will continue in co-commissioning with NHSE which involves all decisions having to go through a Joint Committee that involves a large number of people across South West London and is a very unsatisfactory way of making decisions for the local populations. The CCG has reviewed the due diligence reports and feels ready to go for delegation now, knowing the financial and organisational risks that are involved. Mitigation will be sought from NHSE for the rent review back payments and accruals as highlighted in the reports.
A vote was taken by way of a show of hands and the result was as follows:
22
Yes
0
No
1
Abstention
2
Unable to vote due to incorrect proxy forms
The process was overseen by Dr Theodora Kalentzi, Medical Director/ LMC SecretaryLondonwide LMCs and Londonwide Enterprise Ltd. The agreement to proceed with the application for delegation was therefore carried.
EN
C 0
6
Page 5 of 15
APPENDIX 2
Delegated commissioning of primary care - Terms of Reference
FEBRUARY 2016
EN
C 0
6

V260216 SH 6
NHS Sutton CCG Primary Care Commissioning Committee
Terms of Reference
Introduction
1. Simon Stevens, the Chief Executive of NHS England, announced on 1 May 2014 that
NHS England was inviting CCGs to expand their role in primary care commissioning
and to submit expressions of interest setting out the CCG’s preference for how it
would like to exercise expanded primary medical care commissioning functions. One
option available was that NHS England would delegate the exercise of certain
specified primary care commissioning functions to a CCG.
2. In accordance with its statutory powers under section 13Z of the National Health
Service Act 2006 (as amended), NHS England has delegated the exercise of the
functions specified in Schedule 2 of the Delegation Agreement to these Terms of
Reference to NHS Sutton CCG (the CCG).
3. The CCG has established the CCG Primary Care Commissioning Committee
(“Committee”). The Committee will function as a corporate decision-making body for
the management of the delegated functions (Schedule 2 of the Delegation
Agreement) and the exercise of the delegated powers.
4. The ongoing relationship the Committee will have with NHS England will be revised
on an ongoing basis, though is currently outlined as in Schedule 2 of the Delegation
Agreement.
5. It is a committee comprising representatives of the following organisations:
NHS Sutton Clinical Commissioning Group
NHS England
London Borough of Sutton
Londonwide Local Medical Committee
Sutton Healthwatch
A non-partner, salaried GP from a practice in Sutton
Statutory Framework
6. NHS England has delegated to the CCG authority to exercise the primary care
commissioning functions set out in Schedule 2 of the Delegation Agreement in
accordance with section 13Z of the NHS Act.
EN
C 0
6

V260216 SH 7
7. Arrangements made under section 13Z may be on such terms and conditions
(including terms as to payment) as may be agreed between the NHSE Board and the
CCG.
8. Arrangements made under section 13Z do not affect the liability of NHS England for
the exercise of any of its functions. However, the CCG acknowledges that in
exercising its functions (including those delegated to it), it must comply with the
statutory duties set out in Chapter A2 of the NHS Act and including:
a) Management of conflicts of interest (section 14O);
b) Duty to promote the NHS Constitution (section 14P);
c) Duty to exercise its functions effectively, efficiently and economically (section
14Q);
d) Duty as to improvement in quality of services (section 14R);
e) Duty in relation to quality of primary medical services (section 14S);
f) Duties as to reducing inequalities (section 14T);
g) Duty to promote the involvement of each patient (section 14U);
h) Duty as to patient choice (section 14V);
i) Duty as to promoting integration (section 14Z1);
j) Public involvement and consultation (section 14Z2).
9. The CCG will also need to specifically, in respect of the delegated functions from
NHS England, exercise those set out below:
a) Duty to have regard to impact on services in certain areas (section 13O);
b) Duty as respects variation in provision of health services (section 13P)
10. The Committee is established as a Committee of the CCG Governing Body (which in
the remainder of this document is referred to as the CCG Board) in accordance with
Schedule 1A of the “NHS Act”.
11. The Committee, in common with all CCG Board Committees is formally accountable
for furnishing the Finance and Audit Committees with the formal reports it requires to
assure the CCG Board that Primary Care Co-Commissioning is being effectively
governed and managed.
12. The members acknowledge that the Committee is subject to any directions made by
NHS England or by the Secretary of State.
EN
C 0
6

V260216 SH 8
Role of the Committee
13. The Committee has been established in accordance with the above provisions to
enable the members to make collective decisions on the review planning and
procurement of primary care services in Sutton under delegated authority from NHS
England.
14. The overall scope of the Committee draws together three core functions as follows:
a) The primary care co-commissioning functions formally delegated by NHS
England to the CCG as a new CCG function from 1st April 2016
b) The duty to improve quality in primary care-already an existing CCG function
since April 2013
c) Oversight and assurance of the development of the CCG's overarching
Primary Care Strategy - a new function
15. In performing its role the Committee will exercise its management of the functions in
accordance with the agreement entered into between NHS England and the CCG,
which will sit alongside the delegation and terms of reference.
16. The functions of the Committee are undertaken in the context of a desire to promote
increased co- commissioning to increase quality, efficiency, productivity and value for
money and to remove administrative barriers.
17. The role of the Committee shall be to carry out the functions relating to the
commissioning of primary medical services under section 83 of the NHS Act.
18. This includes the following:
a) GMS, PMS and APMS contracts (including the design of PMS and APMS
contracts, monitoring of contracts, taking contractual action such as issuing
branch/remedial notices, and removing a contract);
b) Newly designed enhanced services (“Local Enhanced Services” and
“Directed Enhanced Services”);
c) Design of local incentive schemes as an alternative to the Quality Outcomes
Framework (QOF);
d) Decision making on whether to establish new GP practices in an area;
e) Approving practice mergers; and
f) Making decisions on ‘discretionary’ payment (e.g., returner/retainer schemes).
EN
C 0
6
V260216 SH 9
19. The CCG will also carry out the following activities:
See Schedule 2 of the Delegation Agreement for the scope of the delegated co-
commissioning functions.
20. The Committee is accountable for exercising the agreed delegated functions from
NHS England; these functions operate at practice level and not at individual Primary
Care Contractor level.
Geographical Coverage
21. The Committee will comprise of decisions relating to primary care in Sutton.
Membership
22. The Committee shall consist of:
Voting members:
CCG Board Lay Member (Chair)
CCG Board Lay Member (Vice Chair)
CCG Chief Operating Officer
CCG Chief Finance Officer
CCG Board Independent Nurse
CCG Board Independent Secondary Care Consultant
Independent GP Advisor
Non-voting attendees:
Health and Wellbeing Board (’HWBB’) representative
London Borough of Sutton Public Health representative
Sutton Healthwatch representative
Londonwide Local Medical Committee (‘LMC’) representative
1 salaried Sutton CCG GP (non-partner)
NHS England Representative
No person who is a practising clinician in the CCG area may be a voting member of
the Committee.
23. The Chair of the Committee shall be a CCG Board Lay Member, however this should
not be the Chair of the Audit Committee.
EN
C 0
6

V260216 SH 10
24. The Vice Chair of the Committee shall be a CCG Board Lay Member, who could be
the Chair of the Audit Committee.
25. Voting members will be CCG Chief Operating Officer, CCG Chief Finance Officer,
Independent GP Advisor, Board Independent Secondary Care Consultant and Board
Independent Nurse.
26. Non-voting attendees will be Sutton Healthwatch representative, LMC
representative, Public Health representative, HWBB representative, Sutton CCG GP
(non-partner) and NHS England representative.
27. The Committee may appoint ad-hoc members to advise it on specific matters within
its terms of reference from time to time as appropriate.
28. There will be an annual review of the Committee’s membership to support its efficient
functioning.
Conflicts of Interest
29. Conflicts of Interests will be managed in accordance with the CCG Constitution that
outlines the current policy; ‘Standards of Business Conduct and Managing Conflicts
of Interest Policy’.
30. Where a Committee member has, or may have, a conflict of interest, arrangements
will be put into place to manage that conflict of interest in accordance with the
Constitution and the Conflicts of Interest Policy.
Meetings and Voting
31. The Committee will operate in accordance with the CCG’s Constitution and Standing
Orders. The Secretary to the Committee will be responsible for giving notice of
meetings. This will be accompanied by an agenda and supporting papers and sent to
each member representative no later than 5 days before the date of the meeting.
When the Chair of the Committee deems it necessary in light of the urgent
circumstances to call a meeting at short notice, the notice period shall be such as
s/he shall specify.
32. The Committee will make decisions within the bounds of its remit.
33. The decisions of the Committee shall be binding on NHS England and the CCG.
34. Each voting member of the Committee shall have one vote. The Committee shall
reach decisions by a simple majority of members present, but with the Chair having a
second and deciding vote, if necessary. However, the aim of the Committee will be to
achieve consensus decision-making wherever possible.
EN
C 0
6

V260216 SH 11
35. Members of the Committee have a collective responsibility for the operation of the
Committee. They will participate in discussion, review evidence and provide objective
expert input to the best of their knowledge and ability, and endeavour to reach a
collective view.
36. Meetings of the Committee:
a) shall be held in public, subject to the application of 36(b);
b) the Committee may resolve to exclude the public from a meeting that is open
to the public (whether during the whole or part of the proceedings) whenever
publicity would be prejudicial to the public interest by reason of the
confidential nature of the business to be transacted or for other special
reasons stated in the resolution and arising from the nature of that business
or of the proceedings or for any other reason permitted by the Public Bodies
(Admission to Meetings) Act 1960 as amended or succeeded from time to
time.
Quorum
37. The Committee will be Quorate with four of the seven voting members in attendance,
with at least one Lay member and one clinician present. Where the Sutton CCG GP
or other non-voting observers have a conflict of interest they will excluded from the
agenda item discussion and decision.
Confidentiality
38. Members of the Committee shall respect confidentiality requirements as set out in the
CCG Constitution or Standing Orders.
Frequency of meetings
39. The committee shall meet monthly, though the format of these meetings will alternate
between a formal meeting in public and a seminar in private for developmental
purposes. At least six meetings will be held in public over the financial year.
Urgent Decision Making
40. The Committee has a statutory duty to make a range of decisions relating to the
commissioning of primary care medical services.
41. In the vast majority of cases these decisions can be made by the committee as part
of business as usual. However, there may be occasion, when an urgent situation
arises that requires a decision or actions to be agreed either immediately or
before the next Committee takes place.
EN
C 0
6

V260216 SH 12
42. Urgent Decision Making (UDM) meetings, in person or via teleconference, can be
called by the chair (or vice-chair in their absence) and the Chief Operating Officer
and the Chief Finance Officer. This is outlined in Schedule 5 of the Delegation
Agreement.
43. A minimum of two voting members of the Committee must be present in person or on
the teleconference, one of whom should be a Board Lay Member and the other
should be a clinician, for it to be quorate.
44. A meeting will be convened by the Committee Chair (or Committee Vice-Chair in
their absence) and the Chief Operating Officer and the Chief Finance Officer.
Consultation will be made with the Committee Vice-Chair and all other available
members of the Committee unless in exceptional circumstances where a time delay
cannot be permitted. If other Committee members are not consulted they will be
informed at the earliest possible time.
45. All decisions will be reported at the next available Committee meeting.
Other Matters
46. The Committee may delegate tasks to such individuals, sub-committees or individual
members as it shall see fit, provided that any such delegations are consistent with
the parties’ relevant governance arrangements, are recorded in a scheme of
delegation, are governed by terms of reference as appropriate and reflect appropriate
arrangements for the management of conflicts of interest.
47. The Committee may call additional experts to attend meetings on an ad hoc basis to
inform discussions.
Reporting
48. The Committee will present its minutes and an executive summary report to the
London Area Team of NHS England and the Board of Sutton CCG, following each
meeting, for information, including the minutes of any sub-committees to which
responsibilities are delegated under paragraph 47 above.
49. There is a statutory requirement that the Committee publishes a register of its
decisions, outlining the management of any Conflicts of Interest.
50. The CCG will also comply with any reporting requirements set out in its constitution.
Review of Terms of Reference
51. It is envisaged that these Terms of Reference will be reviewed bi-annually in year
one and annually thereafter, reflecting experience of the Committee in fulfilling its
EN
C 0
6

V260216 SH 13
functions. NHS England may also issue revised model terms of reference from time
to time.
Role of Primary Care Programme Board
52. A Primary Care Programme Board has been formed to support the Committee in the
execution of its functions. It is accountable to the Committee and its functions
include:
a) Supporting the development of the Primary Care strategy including the
strategic approach to improving quality.
b) Constructing the annual work plan for the Committee to approve.
c) The CCG core members of the Primary Care Programme Board are:
Director of Performance and Primary Care
Chief Finance Officer,
Head of Primary Care Commissioning
Independent GP advisor
Sutton CCG GP Partner (not an officer of the CCG)
Salaried Sutton CCG GP (non-partner)
Lead Locality Practice Nurse
Lead Locality Practice Manager
Locality Manager
Commissioning Manager
Other members of the CCG and NHS England Primary Care teams on an ad
hoc basis as required.
E
NC
06

V260216 SH 14
[Schedule 1 – Delegation agreement -to be added when final arrangements confirmed]
Schedule 2 – Delegated functions
Delegated Functions from 1st April 2016:
a) decisions in relation to the commissioning, procurement and management of Primary
Medical Services Contracts, including but not limited to the following activities:
i) decisions in relation to Enhanced Services;
ii) decisions in relation to Local Incentive Schemes (including the design of such
schemes);
iii) decisions in relation to the establishment of new GP practices (including branch
surgeries) and closure of GP practices;
iv) decisions about ‘discretionary’ payments;
v) decisions about commissioning urgent care (including home visits as required)
for out of area registered patients;
b) the approval of practice mergers;
c) planning primary medical care services in the Area, including carrying out needs
assessments;
d) undertaking reviews of primary medical care services in the Area;
e) decisions in relation to the management of poorly performing GP practices and
including, without limitation, decisions and liaison with the CQC where the CQC has
reported non-compliance with standards (but excluding any decisions in relation to
the performers list);
f) management of the Delegated Funds in the Area;
g) Premises Costs Directions functions;
h) co-ordinating a common approach to the commissioning of primary care services
with other commissioners in the Area where appropriate; and
i) such other ancillary activities as are necessary in order to exercise the Delegated
Functions.
Reserved Functions remaining with NHS England:
a) management of the national performers list;
b) management of the revalidation and appraisal process;
EN
C 0
6

V260216 SH 15
c) administration of payments in circumstances where a performer is suspended and
related performers list management activities;
d) Capital Expenditure functions;
e) section 7A functions under the NHS Act;
f) functions in relation to complaints management;
g) decisions in relation to the Prime Minister’s Challenge Fund; and
h) such other ancillary activities that are necessary in order to exercise the Reserved
Functions;
Schedule 3 - List of Members of Primary Care Commissioning Committee
From 1st April 2016, the Committee shall consist of:
Voting members:
CCG Board Lay Member (Chair) Sally Brearley
CCG Board Lay Member (Vice Chair) Paul Sarfaty
CCG Chief Operating Officer Jonathan Bates
CCG Chief Finance Officer Geoff Price
CCG Board Independent Nurse Pippa Barber
CCG Board Independent Secondary Care Consultant Mr Les Ross
Independent GP Advisor Dr Simon Elliott
Non-voting attendees:
Health and Wellbeing Board (’HWBB’) tbc
London Borough of Sutton Public Health Dr Niki Lang
Sutton Healthwatch David Williams
Londonwide Local Medical Committee (‘LMC’) Julie Freeman
1 salaried Sutton CCG GP (non-partner) Dr Assad Pasha
NHS England William Cunningham-Davis
EN
C 0
6

Report to the Sutton Clinical Commissioning Group
Governing Body
Date of Meeting: 2nd March 2016
Agenda No: 8 ENCLOSURE: 07
Title of Document: Practice Engagement in Clinical Commissioning
16/17
Purpose of Report:
For approval
Report Authors:
Dr Farhan Rabbani – GP locality Lead, Wallington
L Naidu – Locality manager, Sutton CCG
Lead Director:
Sue Roostan – Director of
Commissioning and Planning
Executive Summary: Following on from the success of this year’s GP Engagement scheme, the planning of next year’s scheme is well underway. A draft scheme has been proposed which preserves the many positive aspects of this year’s scheme, incorporating achievable, measurable, quality and cost effective outcomes. These outcomes will;
Support the delivery of Sutton CCG organisational objectives
Provide Practices with an element of choice to maximise engagement and participation
Support early identification of long term conditions
Support appropriate referral decisions and processes
Encourage shared learning and quality review through audit
Build on work already started to improve the quality of antibiotic prescribing
Encourage attendance at locality meetings, joint workshops, PM and PN forums, PRG events and safeguarding forums
Key sections for particular note (paragraph/page), areas of concern etc: The scheme takes account of changes as a result of the PMS review process and the
recently announced CCG financial allocation.
The 24th February 2016, Executive Committee requested that further account was
taken of the requirement to deliver Constitutional Standards, particularly the
Dementia Diagnosis standard which is yet to be given full consideration in light of its
importance to the CCG.
EN
C 0
7

Page 2 of 7
Recommendation(s):
The Governing Body are asked to:
APPROVE the content of the Sutton GP engagement scheme 16/17
DELEGATE final sign off of the GP Engagement Scheme to the Vice-Chair and Chief Operating Officer, in dialogue with the Locality Leads, to reflect the focus Dementia Diagnosis.
Committees which have previously discussed/agreed the report:
Sutton Clinical Commissioning Group Executive Committee 16/12/15 & 24/02/16
Financial Implications:
The value of the scheme remains at £2/head of weighted population (approx.
£360,000)
Other Implications:
None
Equality Impact Assessment:
Information Privacy Issues:
None
Communication Plan:
Proposed launch of scheme with Practice’s
Circulation of papers and practice sign up – 17th March 2016
Scheme begins April 2016
EN
C 0
7

Page 3 of 7
1 Purpose: The purpose of the 2016-17 Sutton Engagement Scheme (SES) is to support Sutton GP Practices and their Localities to actively engage in high quality, cost effective clinically-led commissioning and service redesign by financially compensating Practices for the input required to achieve measurable, quality and cost effective outcomes. Funding will be made available to each Practice to support engagement in clinical commissioning through Localities and on delivery of outcomes. 3 Eligibility Criteria: All NHS GP practices within the Sutton Localities (Sutton & Cheam, Carshalton and Wallington) 4 Duration: The SES covers the period from 1st April 2016 to 31st March 2017 5 Payments Overall funding of the scheme will be £2 per head of capitation based on weighted list size as at 1st April 2016. The attached spread sheet (Engagement scheme payments) details the funds available to each practice on achievement as follows: Requirements:
5 Engagement with Locality meetings, Practice Manager and Practice Nurse Forums, etc.
1. Practices will be expected to have GP representation at Locality meetings.
Locality meetings will be a minimum of two hours in duration.
A deputy clinician or managerial representative can be sent with prior
notification to the Chair.
2. Practice attendance and participation at quarterly plenaries, and relay
information and action points to the Practice’s clinical and managerial team.
3. Practice Manager or practice representative at monthly Practice Manager Forums and sharing of information with the team.
EN
C 0
7

Page 4 of 7
4. Practice Nurse or Nurse Practitioner attendance at monthly forum and sharing of information.
5. Attendance by safeguarding lead GP to 4 meetings/events in year (2x adult 2 x children) and cascade learning to wider practice team
6. Timely response to audit requests, e.g. high cost patient audit enquiries.
7. Patient engagement in Patient Reference Group forum (each practice to send at least one representative)
To achieve full payment of this aspect of the scheme Practices’ Members will be required to
attend;
A minimum 11 locality meetings/year
9 of 12 PM forums
9 of 12 PN forums
3 of 4 quarterly PRG meetings
All 4 plenary sessions (4/year)
All 4 safeguarding forums
Payments for the 2016/17 engagement scheme will be made in two parts;
March 2016 - 50% - paid at sign up
June 2017 – 50% - paid subject to achievement
6 Practice Based Engagement - Outcomes:
Criteria No.
Description
1
Prescribing
A) Undertake an agreed antibiotic audit, depending on practice priorities, to be
agreed with Medicines Optimisation team
B) Work with your practice PPG to undertake a specific activity in practice to
promote Antibiotics Awareness Day (November) and report this activity at
December/January locality meeting (to be agreed)
C) % Broad spectrum antibiotics - Reduce % broad spectrum antibiotics to less
than England average or by 5% - whichever is the higher (i.e. easier), using 15/16
data as baseline. Maintain if already below this value. Practices to be given their
specific target based on this descriptor (i.e. if England average is 10.5%, a
practice at 17% would reduce to 12%, a practice at 13% would reduce to 10.5%).
Local adjustment to prescribing data may be considered following submission of
practice audits demonstrating appropriateness of prescribing.
D) Items per STAR-PU - Reduce items per Star PU prescribed to less than
EN
C 0
7

Page 5 of 7
England average or by 1-5%, whichever is the lower value, using 15/16 data as
baseline. Maintain if already below this value. Practices to be given their specific
target based on this descriptor. Per bandings below, practice in pink band (10th
decile) - reduce by at least 5%, orange band (8th/9th decile) – reduce by at least
3%, yellow band (6th/7th decile) – reduce by at least 1%. Green band – maintain
2
Referrals
First out-patient referral rate objective
Increase conferral rates using Kinesis by all principles, salaried GPs and GP Registrars
3
Improving quality through Audit in General Practice
Practices to undertake a minimum of 3 audits, 2 of which must be clinical.
Audit findings to be written up, shared within practice teams and re-audited.
Each practice to share the findings of one audit of choice with colleagues at a locality meeting (1 practice presentation per locality meeting)
4
Prevalence and Preventative Work (select 1 from the following)
Run the GRASP-HF audit tool (free) which aims to support practices to interrogate their clinical data enabling them to improve the management and care of patients with heart failure (HF) with left ventricular systolic dysfunction (LVSD). The tool also assists with
EN
C 0
7

Page 6 of 7
case finding activity, helping practices to establish more accurate prevalence rates within the practice population. Practices must submit an end of year report detailing the outcomes of interventions made following the audit Or
% of 65+ who have had their pulse rhythm recorded (looking for AF) as part of the practice based health screening work – to find undiagnosed cases (target screen - 50%) Or
Annual screening of patients 40 years and over with:
o a BMI >30 and/or
o waist size of >80 cm for females; >94 cm for males or >90 cm for South Asian males
7 Funding Based on £2 per head of weighted capitation: the funding will be split across Part 1 and Part 2 as follows: 35.5% for the engagement aspect shared equally between each practice 64.5% for the outcomes section based on list size The outcomes will be monitored at agreed intervals and targeted visits will be made to practices according to progress with the Scheme. These visits will be made by the GP Locality Lead, supported by the Locality Manager and Director of Performance and Primary Care as necessary. All practices will be visited at least once per annum and Action Plans generated as part of this review. Practices will complete an engagement survey in November/December. Achievement will be assessed by a member of the Board of the CCG together with the GP Locality Leads, Locality Manager and Director of Performance and Primary Care. 8 Reporting:
Practice attendance record at Locality meetings, PN meetings, PM meetings and quarterly plenary (Locality Manager to collate and validate).
Practice engagement in Patient Reference Group through attendance record
Prescribing data to be monitored through PACT data and reported monthly through the GP performance dashboard
Outpatient referral rates will be monitored through the GP Performance Dashboard
Kinesis activity to be monitored by SCCG and reported Quarterly to Practices
Practices will present one audit at one locality meeting plus provide summary findings of all 3 audits to SCCG at year end.
Prevalence/Preventative – findings to be reported to CCG at year end (reporting template to be provided)
EN
C 0
7

Page 7 of 7
9 Support offered to the Practices: GP Practices will be supported through the work of Locality GP Leads, Locality Manager, Locality Assistant, PM and PN Locality Leads and Locality Prescribing Leads. 10 Participation: Practices are required to formally sign up to the SES to confirm their commitment to active participation in their Localities, to fulfil the SES requirements. The scheme will be challenging to all Practices through changes to engagement at all levels and changes in referral/prescribing patterns. If a Practice adopts engagement ‘behaviour’ through the year, but, despite this, exceptional circumstances have prevented them from progressing with this scheme, such exceptions will be objectively reviewed by the three GP Locality Leads and a Board member NOTE – On conclusion of the PMS review process the contents of this scheme may be subject to review to ensure Practice engagement with CCG priorities and delivery of constitutional standards.
EN
C 0
7

Report to the Sutton Clinical Commissioning Group
Governing Body
Date of Meeting: 2nd March 2016
Agenda No: 9 Attachments: 08
Title of Document:
Review of Investments and QIPP 16/17
Purpose of Report:
For Approval
Report Authors: Alastair Hughes
Lead Director: Alastair Hughes
Executive Summary:
Our QIPP requirement remains £6.5m. This is unchanged from our Draft Operating Plan submission
of 8 February. Our current plan to deliver this is contained in this paper for approval.
Please note that at the CCG Governing Body meeting on 2 March, we are requesting delegated
authority (granted to the CCG Executive Committee) as required to make decisions on its behalf
relating to 16/17 QIPP scheme approvals and investment reductions (at planned CCG Executive
Committee meetings on 9 March and 30 March).
Please note that decisions may also require Primary Care Committee authorisation as required.
Key sections for particular note (paragraph/page), areas of concern etc: Please note that ‘Additional Identified Savings’ are subject to development and confirmation.
Recommendation(s): To consider and approve the plan to deliver a 2016/17 QIPP programme of £6.5m.
To confirm delegated authority (to the CCG Executive Committee) to make decisions relating to 16/17
QIPP scheme approvals and investment reductions (at planned CCG Executive Committee meetings
on 9 March and 30 March).
Please note that decisions may also require Primary Care Committee authorisation as required.
Committees which have previously discussed/agreed the report: CCG Clinical Strategy Group 24 February 2016
Financial Implications: Please note impact of potential investment reduction decisions on planned 16/17 QIPP scheme
delivery.
Please also note both the non-recurrent and recurrent spend implications of decisions.
Other Implications: Please note the impact of potential investment reduction decisions on ability to deliver strategic
plans.
EN
C 0
8

Page 2 of 4
Equality Impact Assessment: Not Applicable. However please note that investment decisions may relate to improvement schemes
that are subject to impact assessment. Also please note that QIPP schemes are subject to impact
assessment.
Information Privacy Issues: Please treat as commercial in confidence.
Communication Plan: None.
EN
C 0
8

Page 3 of 4
QIPP & Investments Review: Achieving our £6.5m QIPP requirement
Our QIPP requirement remains £6.5m. This is unchanged from our Draft Operating Plan
submission of 8 February. Our current plan to deliver this is shown below, for consideration and
approval.
Please note that we are requesting delegated authority (granted to the CCG Executive Committee)
to make decisions on its behalf relating to 16/17 QIPP scheme approvals and investment
reductions (at planned CCG Executive Committee meetings on 9 March and 30 March). Decisions
may also require Primary Care Committee authorisation as required.
£3.2m Current
planned gross
QIPP
Schemes (approved at CSG on 27 Jan) are being worked up to final PID
approval by Clinical Strategy Group and CCG Executive on 30 March.
See attached.
£1.2m Additional
identified
savings
Potential additional QIPP schemes (see attached): total £0.5m
£0.2m MSK pathway development (planned care) – agreement at
Clinical Strategy Group (24 February) to take this scheme to the next
stage of development.
£0.05m ECI SWL initiative
£0.25m Medicines Optimisation – stretch achievement
Other potential schemes under consideration, also included in the
attached.
A number of additional savings identified by service leaders: total 0.7m
Primary Care
£300k quality premium advance (non-recurrent) £160k LCS (net of new LCSs) conversion to PMS
Mental Health (note: opportunity for savings confirmed possible
within Parity of Esteem required level of spend)
£200k reduction in planned growth (assessment of growth risk containable within Mental Health budget)
CCG Running Costs
£114k CCG IT (£67k part year effect in 16/17): not confirmed until procurement completed
£2.1m Investment
reductions:
All £2.1m
investments
withdrawn.
£1.16m
In view of the considerations above, we are preparing to make
decisions about reducing our investments planned for 16/17 and
beyond. We have identified a maximum of £2.1m of planned
investment (please see attached) which we could cut (other 16/17
investments are committed). Depending on the scale of reduction
required, this may require prioritisation.
All 16/17 investments withdrawn subject to potential re-investment
EN
C 0
8

Page 4 of 4
removed
from 16/17
plans
£0.97m
subject to
potential re-
investment
depending
on CCG
affordability
decisions over the next 6 weeks depending on CCG affordability.
A number of investments to be removed from 16/17 CCG investment plans (total £1.16m): Systems Resilience Funding: £801k Community Mental Health Adults: £200k End-of-Life Care for People with Learning Disabilities: Specialist
nurse post to be recruited and funded from Vanguard: £58k Personal Health Budgets & Complex Pathway Practitioner – PHB
budget provision for 16/17 removed: £100k non-recurrent
8 investments are subject to prioritisation and re-investment decisions over the next 4 weeks depending on CCG affordability (total £0.97m). These are shown in the attached (shaded). Manager Leads to
provide additional information regarding cost, gross saving, activity and alternative funding opportunities. This will help with further prioritisation.
Sufficient time to be allowed for financial affordability to become clearer and additional information to be developed and provided. 24 Feb CSG and Executive Committee decisions ahead of Governing Body approval on 2 March viewed as too soon.
Prioritisation and re-investment decisions to occur on 9 March Executive Committee (note: timetable aligns with QIPP approvals process).
Proposed timetable
24 Feb: CSG (followed by Executive Committee)
2 Mar: CCG Board
4 Mar: Deadline for receipt of additional scheme information to support potential re-
investment decisions
9 Mar: Executive Committee
QIPP & Investments – Prioritisation and re-investment decisions
New QIPP schemes: Cases for Change
30 Mar: CSG and Executive Committee (note Easter)
Overall QIPP Plan Approval including PID Approvals
E
NC
08

16/17 QIPP SCHEMES ORIGINAL SAVINGS TARGETS
NET
SAVINGS (£000s)
Risk Rating
CATEGORY
TYPE PROJ. DESCRIPTION
MANAGER LEAD
CLINICAL LEAD
GROSS SAVINGS (£000s)
Acute
Transformational
Non-elective activity reduction
AH CE
1372
Green
Primary Care Support Model MM CE
Respiratory Pathway (including COPD EoLC)
SG KS
Diabetes Pathway SG KS
Admiral Nurses AD CK
Vanguard CH COS
Enabler – integrated digital care record (IDCR)
SH TBC
Acute Transformational
Paediatrics – ED Nurse Navigator
BD TBC 120 Amber
LTC Transformational
Respiratory and diabetes outpatient scheme
SG KS 48 Amber
Planned Care Transformational
Kinesis Optimisation SR DP 91 Amber
Mental Health Transacti
onal High Cost Placements LF CK 150 Amber
Medicines Management
Transformational
Medicines Management schemes
379.5 Green
MMT practice workstreams ST RS 200
Script switch ST RS 80
Oral Nutritional Supplements
ST RS 80
Medicines optimisation of housebound patients
ST RS 13
Care Homes ST RS 6.5
Medicines Management
Transactional
Prescribing Growth Management
ST RS 1,000 Green
TOTAL
3,160.5

16/17 POTENTIAL QIPP SCHEMES ORIGINAL SAVINGS TARGETS
NET SAVINGS (£000s)
Risk Rating
CATEGORY TYPE PROJECT DESCRIPTION MANAGER
LEAD CLINICAL
LEAD
GROSS SAVINGS (£000s)
Planned Care Transform
ational MSK Pathway Development BD DP
£2m (Right care)
£0.2m Amber
Planned Care Transform
ational GI Pathway Development BD DP
£1m (Right care)
£TBC Red
Planned Care Transactio
nal ECI SWL Initiative SR/TBC DP £0.05m Amber
Planned Care Transform
ational Outpatient Reform AH/SR CE
Pending review of
PwC report
Green
Acute Transform
ational Pathology ES MW 17/18 Red
Meds Mgmt Transform
ational Medicines Optimisation – stretch achievement
ST RS £0.25m Green
TOTAL
£0.5m

16/17 Investments Review Date: 10/02/2016
Wave 1: Investments Approved May 6
A 4Extended Hours/Services in
Primary Care PilotSian Hopkinson
Dr Dino
Pardhanani
Extending opening hours in primary care through two hubs. National expectation / potential directive. SWL CCGs aligned
plan. Risk of impact on Practice confidence in GP Federation if no go.313
£450k recurrent from 17/18.
Pared back from £600k original.
£313k in 16/17 during ramp-up: this figure can be
reduced if delayed start. Can the model be pared
back further and/or delayed?
Expected to contribute to winter pressures in
2016/17 and beyond, ie. reduction in A&E
attendances and consequential NEL admissions.
£450k recurrent TBD TBD Transformation fund?
A 6Better Care Fund Implementation
– Primary Care Support ModelMegan Milmine TBC
Active management of the top 2% of patients most vulnerable, through a model of primary care support and integrated
working.220
£450k in budget. 4/6 nurses recruited. Best model
adds an admin post: total recurrent cost £273k
(saving of £177k on budget). No admin post takes
cost to £231k saving £220k on budget.
NEL QIPP savings scheme: contributing 1.5% to 3.5%
target. 218 reduced admissions equates to £588k
planned savings.
Also an enabler of LTC prevention.
£231k - £273k recurrent £588k recurrent TBD TBD
A 7Systems Resilience Funding –
additional allocationMegan Milmine Dr Chris Elliott
Top-up funding for acute and community schemes to manage impact of winter pressures on performance and quality (incl.
ED, DTOC, NEL, RTT). Please note: currently assumed to be removed from investment plans following Management Team
review on 09/02/2016.
801
£801k (£880k total top-up of which £79k allocated to
mental health) supporting acute & community
schemes over winter.
Acute - mainly ED additional staffing, support staff at
weekends (e.g. portering, diagnostics and therapy
staff). Community spend is on integrated schemes to
support discharges as rapidly and safely as possible
(and admission prevention where possible) from the
acute trust.
Reducing system resilience will increase the risk of
delivery of the following:
• ED 95% target
• DTOC (a 2016/17 BCF target as well)
• NEL admissions
• Ambulance offload delays
• Number of week/weekend discharges
• 18 week targets (cancelled electives due to
emergency flows)
A 9
Systems Resilience Funding –
Allocation to support enhanced
Liaison Psychiatry – St Helier
Adrian DaveyDr Chris Elliott/Dr
Chris Keers
Enhanced liaison psychiatry service to deliver efficient and responsive access to mental health services, accessed via a team
fully integrated into EStH. Please note: removed from review list due to confirmation received (09/02/2016) that funding
confirmed as within baseline for 16/17 block contract with SWLSTG.
0£314k. Funding confirmed as recurrent and within
baseline for 16/17 block contract with SWLSTG.
Benefits
• Patient experience
• 4 and 12 hour breaches
• DToC for people with mental health problems
(including Dementia)
• Early intervention referrals and assessment
performance indicators
A 11Community Mental Health: Older
People & AdultsAdrian Davey Dr Chris Keers
Investment in transformative approach across pathways including assessment and dementia diagnosis. £200k reduction is to
confirm non-investment in Adults (committed for Older People). Please note: confirmed removed from investment plans
following Management Team review on 09/02/2016.
200
£200k budget for Adults - recurrent from 16/17.
(Note: £200k for Older People recruited to, in
baseline for 16/17 block contract with SWLSTG and
not available for review).
£200k investment for Adults to be confirmed
withdrawn from 16/17 budget as not approved - &
subject to potential business case approval during the
year (benefits relate mainly to access and dementia
diagnosis rate).
A 14LTCs - Respiratory and Diabetes
pathways developmentSam Green Karol Selvey Clinically led transformation of priority pathways and the underpinning approach to LTC management and prevention. 150
£90k recurrent (respiratory nursing).
£60k non-recurrent (project management).
NEL QIPP savings scheme:
Respiratory: contributing 1.25% or 181 reduced
admissions equates to £490k savings.
Diabetes: contributing 0.25% or 36 reduced
admissions equates to £98k savings.
£90k recurrent
£60k non-recurrentTBD TBD TBD
A 16CCG Capability, OD and
Succession PlanningJonathan Bates Dr Simon Elliott
Development of our clinical and managerial succession plans, skills, roles and engagement - to enable the CCG to go from
good to great. £77k advance payment (to CSU) required to mitigate non-provision in current budget.
0 (risk of £77k:
see note)£77k cost in 16/17 (of £160k total) not in current
16/17 budget.
An enabler: not direct cost saving.
Risk of impact on staff if curtailed.£77k non-recurrent £0k NA Deliver in-house?
Sub-Total 1,684
Wave 2: Additional Investments Approved October 15
B 5IRIS – Domestic Violence
Programme for Primary CareMary Hopper Anna Cassin
3 year domestic violence and abuse programme for primary care to identify and support victims and their families in
response to unmet local need evidenced in JSNA.51
£51k recurrent for three years. In procurement
(closed 27 Jan). Pull forward opportunity of £153k
for three years in to 15/16 but requires checking with
procurement rules and CFO approval. NICE guidance
awaited Feb 2016. Is there an option to commit to
only 1 year and pay in advance via LBS (in 15/16)?
Benefits
• Impacts the identification and management of
domestic violence for Sutton population. High risk
area of need for Sutton population and women and
children in Sutton. 100's of patients impacted over
three-year period.
• Reduce load on GP practices.
£51k / yr for 3 years TBD TBD TBD
B 6Improving Access to Wound Care
ManagementLou Naidu Karol Selvey
Locality base wound care service to support the work currently being undertaken in general practice: at weekends & bank
holidays, and during the week where capacity/skill mix required.134
£134k recurrent. Specialist nurses identified. Go live
estimated for 1/3/16.
Lou's view is model can not be reduced (e.g. to
£80k).
Alongside quality benefits, we expect cost benefits of
patients not attending for dressings outside of
Primary care (savings at A&E and at The Wilson
expected but not quantified). Patient numbers
relatively high (e.g. complex patients with venous leg
ulcers).
Aligned with Meds Mgmt QIPP (shadow) for 16/17
and Oral Nutritional Supplement reviews (15/16 &
16/17).
£134k recurrent TBD TBD TBD
B 7Patient Education – An Integrated
ApproachLou Naidu Dr Ash Mirza
Community/locality based quarterly education and signposting sessions for selected cohorts of patients and carers: including
living with COPD, dementia, managing health over 75 etc.48
£13k in 15/16 and £27k in 16/17 non-recurrent.
Note: original approved spend was for £48k
recurrent. Any future plans subject to evaluation and
investment proposal.
As an enabler of patient self-management and well-
managed patient/carer decision-making, this can
improve efficiency through appropriate use of health
services. Estimated cost savings to be defined.
£13k 15/16
£27k 16/17
(i.e. 2 years only)
TBD TBD TBD
B 9 CHC: Additional Winter Nurse Jane Pettifer TBCCHC Nurse Assessor based at EStH with the discharge team to support more timely CHC assessment & discharge. Covers
winter pressure & extra nursing home capacity and demand. Post currently filled by agency.50
£50k recurrent. Continuation of role is subject to
evaluation after Winter and approval to make the
post permanent.
Possibility of post not required when review
completed (not assumed).
Benefits relate to CHC and DTOC performance and
management of PHBs. Estimated cost savings to be
defined.
£50k recurrent TBD TBD TBD
B 14End-of-Life Care for People with
Learning DisabilitiesAdrian Davey
Dr Claire
O'Sullivan
A Specialist Nurse post to act as a liaison with: General Practice, Community LD Team, Care Homes and EStH - to identify
demand and develop “Personalised Advanced Care Plans”. Please note: £58k (recurrent) requirement to be sourced from
Vanguard funding, following Management team review on 09/02/2016.
58£58k recurrent. Not recruited. To be funded from
Vanguard.
Addresses skills gap. Significant patient benefits.
Viewed as core to improving 67% dementia diagnosis
rate.
B 16Personal Health Budgets and
Complex Pathway PractitionerSam Green / Jane
PettiferKarol Selvey
Budget provision and Complex Pathway Practitioner (in CHC clinical team) to manage delivery model, information
governance and links with safeguarding and quality including supervision. Please note: £100k for 16/17 (non-recurrent)
currently assumed to be removed from investment plans following Management Team review on 09/02/2016.
100
£150k recurrent (17/18 onwards).
Current funding profile is £70k (15/16), £175k
(16/17) : £150k (17/18 onwards).
The post (16/17) is recruited to and requires £70k -
£75k for 16/17.
Revised proposal is to use £20k (15/16) to fund a
data system and transfer £50k to LBS for 16/17
(instead of originally planned £100k budget for
16/17).
Statutory duty for PHBs from 1st April.
Sub-Total 441
Total 2,125
Ref
Cost Gross saving Activity
Alternative
funding
opportunity?
16/17 Investment ScheduleManager
Lead
Clinician
LeadSummary Description
Potential
Maximum
Reduction 16/17
£000s
Cost of schemePotential gross savings if we invest in
the scheme

Report to the Sutton Clinical Commissioning Group
Governing Body
Date of Meeting: 2nd March 2016
Agenda No: 10 ENCLOSURE: 09
Title of Document:
Operating Plan update including contracting round
Purpose of Report:
For discussion
Report Authors:
Susan Roostan- Director of Commissioning and
Planning
Lead Director:
Susan Roostan - Director of
Commissioning and Planning
Executive Summary: This paper sets out the progress made in relation to the operating plan submission
requirements for NHSE. The commissioning priorities for Sutton CCG 16-17 and the
contracting updates for key areas of commissioned activity for Sutton.
Key sections for particular note (paragraph/page), areas of concern etc.: Operational planning context
Plans to meet constitutional standards for 16-17
Plan on a page showing priority areas for Sutton CCG
Progress made in relation to contracts with local providers
Recommendation(s):
The Governing Body are asked to:
Discuss the content of the report and note progress further updates will be provided prior to final submission in April 2016
Committees which have previously discussed/agreed the report:
Executive Committee – 24th February 2016
Financial Implications:
Financial implications are set out in the finance report from CFO and should be read
in conjunction with this report
EN
C 0
9
Page 1 of 14
Page 2 of 14
Other Implications:
Equality Impact Assessment: (MUST BE COMPLETED)
Please indicate if an Equality Analysis (EA) has been done on this paper No
This paper is for information and as programmes and contracts progress any service
development areas or projects will have separate EA undertaken.
Information Privacy Issues:
Communication Plan:
EN
C 0
9
Page 2 of 14

Page 3 of 14
Introduction
This paper sets out the progress to date in relation to the commissioning and
planning round for 16-17. The paper provides an update on submissions made so far
to NHSE, the timetable for future submissions and the current risks to delivery.
National Context
Delivering the five year forward view was released late December and sets out the
expectations for CCGs for the coming year. The document has been previously
shared with the Executive Committee and Governing Body however it is worth
reiterating the ‘9 Must Do’s’ as set out in the delivery document.
1. Develop a high quality and agreed STP, and subsequently achieve what you determine are your most locally critical milestones for accelerating progress in 2016/17 towards achieving the triple aim as set out in the Forward View.
2. Return the system to aggregate financial balance. This includes secondary care providers delivering efficiency savings through actively engaging with the Lord Carter provider productivity work programme and complying with the maximum total agency spend and hourly rates set out by NHS Improvement. CCGs will additionally be expected to deliver savings by tackling unwarranted variation in demand through implementing the RightCare programme in every locality.
3. Develop and implement a local plan to address the sustainability and quality of general practice, including workforce and workload issues.
4. Get back on track with access standards for A&E and ambulance waits, ensuring more than 95 percent of patients wait no more than four hours in A&E, and that all ambulance trusts respond to 75 percent of Category A calls within eight minutes; including through making progress in implementing the urgent and emergency care review and associated ambulance standard pilots.
5. Improvement against and maintenance of the NHS Constitution standards that more than 92 percent of patients on non-emergency pathways wait no more than 18 weeks from referral to treatment, including offering patient choice.
6. Deliver the NHS Constitution 62 day cancer waiting standard, including by securing adequate diagnostic capacity; continue to deliver the constitutional two week and 31 day cancer standards and make progress in improving one-
EN
C 0
9
Page 3 of 14
Page 4 of 14
year survival rates by delivering a year-on-year improvement in the proportion of cancers diagnosed at stage one and stage two; and reducing the proportion of cancers diagnosed following an emergency admission.
7. Achieve and maintain the two new mental health access standards: more than 50 percent of people experiencing a first episode of psychosis will commence treatment with a NICE approved care package within two weeks of referral; 75 percent of people with common mental health conditions referred to the Improved Access to Psychological Therapies (IAPT) programme will be treated within six weeks of referral, with 95 percent treated within 18 weeks. Continue to meet a dementia diagnosis rate of at least two-thirds of the estimated number of people with dementia.
8. Deliver actions set out in local plans to transform care for people with
learning disabilities, including implementing enhanced community provision, reducing inpatient capacity, and rolling out care and treatment reviews in line with published policy.
9. Develop and implement an affordable plan to make improvements in quality
particularly for organisations in special measures. In addition, providers are
required to participate in the annual publication of avoidable mortality rate by
individual trusts. Local Context
Sutton CCG is working with other CCGs in South West London to develop a
coherent sustainability and transformation plan (STP) for an agreed strategic
planning group (SPG). The SPG is identified as South West London CCGs and
providers but will include a number of other commissioners and providers to reflect
patient flow in and out of London.
The STP will be a 5 year plan.
Individually as CCGs there is a requirement to submit annual operating plans that
support and align delivery of the STP. Sutton has submitted a number of templates
that set out the planned commissioned activity, associated financial summaries,
plans to meet the constitutional standards, operational systems resilience templates
and the updated value proposition associated with the Vanguard programme –
‘Sutton Homes of Care’.
EN
C 0
9
Page 4 of 14

Page 5 of 14
Currently Sutton has not yet submitted Better Care Fund (BCF) plans these are
currently being developed and will be subject to review when BCF guidance is
released.
The submission templates are in the process of being assessed by NHSE and
Sutton is required to attend a stocktake meeting late February to assure the central
team of the validity and achievability of CCG plans.
Constitutional standards
Sutton has a good track record of delivery against most of the key constitutional
standards. However, there have been some areas that continue to challenge the
CCG. These areas are dementia diagnosis, access and recovery targets in
relation to IAPT services and cancer waiting times (62 days specifically).
Dementia diagnosis is currently at 63% and the required standard is 67%. Work
continues to improve in this area and the CCG is wholly committed to deliver this
sustainably for 16-17.
Significant focus has been given to improve access to psychological therapies and
associated recovery using the recently commissioned Uplift Service. I am delighted
to report that the service is meeting both access and recovery in January 16 and it
will be the aim of the CCG and provider of the service to continue this in 16-17.
Cancer 62 days – Epsom and St Helier have delivered the 62 day target for the last
quarter, the CCG will be looking to the Trust to ensure this is maintained. Sutton
CCG has not met the required standard due to a number of breaches for Sutton
patients.
The tables below set out the planned delivery against the constitutional standards for the coming year and the associated commentary. These were submitted to NHSE on
8th February.
The CCG was required to submit its planned trajectories for the delivery of
constitutional standards for 16-17; these are attached for information with additional
notes which highlight where risks to delivery may occur.
Contracting round 16-17
Sutton CCG commissions from a range of providers however there are significant
variances in the size of contracts that Sutton holds locally. The section below sets
out the high value contracts being negotiated and the current status of the
negotiations.
Acute contracts
Sutton is holding productive discussions with Epsom and St Helier University
hospitals NHS Trust regarding a block contract for 2016-2017.
EN
C 0
9
Page 5 of 14

Page 6 of 14
It is likely that for the coming year the expenditure on this contract will take the form
of a block payment to the Trust but will continue to be monitored as if the contract
were cost and volume via payment by results.
The benefits of a block arrangement will allow certainty for the provider in terms of
level of income and for the CCG in relation to expenditure. Whilst the contract will be
monitored in exactly the same way as if it were a cost and volume contract the fixed
nature of the expenditure will allow for further transformational and redesign work to
take place with the Trust and across the system. A memorandum of understanding is
being drafted to support this arrangement and will also support the exiting of such an
arrangement in 17-18. It is anticipated that this will be offered to associates to the
ESH contract. It will be for individual CCGs to determine if this is acceptable to them.
Other acute contracts such as St Georges, Croydon and The Royal Marsden will
remain as cost and volume for the coming year/
Community services
This contract is the first year of a newly commissioned service following procurement
in 2015. As such there is little contractual discussion however there is a significant
amount of work to mobilise the new contract. Although the contract was let to the
incumbent provider the disaggregation from Merton CCG, NHSE and local
authorities is not to be underestimated in terms of complex negotiations for service
lines and staff arrangements to transfer to the newly commissioned service.
The provider is also undergoing significant estates changes to move the service into
Sutton. This may not be fully completed by April 1st although huge progress has been made.
Mental Health
The negotiation for the block arrangement with South West London and St Georges
is being led by Merton CCG.
Initial Cash Envelope has been shared with provider detailing where growth will now
form part of main contract with supporting service specifications, with the exception
of Adult Autism and ADHD, where costs are being reviewed.
The Provider has a number of proposed service developments including
transformation of its Acute Pathway. Sutton currently supports the use of CQUIN to
develop a Psychiatric Decisions Unit to help with admissions avoidance.
Other Business Cases that the provider is looking to CCG’s support are around Post
Traumatic Stress Disorder and Personality Disorder, both of which would be
supported locally but would need revising in light of financial constraints and current
local service model i.e. Sutton Uplift.
EN
C 0
9
Page 6 of 14

Page 7 of 14
A revised set of Key Performance Indicators are currently being considered with
more focus on Access as a measure of quality in line with implementation of the five
year forward view.
Work will continue to negotiate on contracts and submits regular status updates via the CSU team to evidence negotiations are progressing. The deadline for contract
sign off is 31st March 2016.
Susan Roostan
Director of Commissioning & Planning
February 2016
EN
C 0
9
Page 7 of 14

Page 8 of 14
NHS Constitution annual performance and plan
Actuals Plan
Area
Measure
14/15 Year End Position
15/16 Latest Reported Position
Reporting Month
2016/17
Plan
2016/17 National Standard
A&E waits Patients should be admitted, transferred or discharged within 4 hours of their arrival at an A&E department – lead commissioner only
95.1%
95.0%
Jan-16
95%
95%
Cat A Ambulance Calls
Category A calls resulting in an emergency response arriving within 8 minutes - Red 1
67.2%
67.8%
Nov-15
75%
75%
Category A calls resulting in an emergency response arriving within 8 minutes - Red 2
59.7%
63.8%
Nov-15
75%
75%
Category A calls resulting in an ambulance arriving at the scene within 19 minutes
91.7%
92.8%
Nov-15
95%
95%
Referral To Treatment waiting times for non- urgent consultant- led treatment
Patients on incomplete non-emergency pathways (yet to start treatment) should have been waiting no more than 18 weeks from referral
94.4%
92.7%
Nov-15
92%
92%
Diagnostic test waiting times
Patients waiting for a diagnostic test should have been waiting less than 6 weeks from referral
99.4%
99.2%
Nov-15
99%
99%
Mixed Sex Accommodation
Minimise breaches
3
3
Dec-15
0
0
Cancer waits - two- week wait
Maximum two-week wait for first outpatient appointment for patients referred urgently with suspected cancer by a GP
96.7%
95.3%
Nov-15
93%
93%
Maximum two-week wait for first outpatient appointment for patients referred urgently with breast symptoms (where cancer was not initially suspected)
97.7%
96.1%
Nov-15
93%
93%
Cancer waits - 31 days
Maximum one month (31-day) wait from diagnosis to first definitive treatment for all cancers
98.2%
100%
Nov-15
96%
96%
Maximum 31-day wait for subsequent treatment where that treatment is an anti-cancer drug regimen
99.6%
100%
Nov-15
98%
98%
Maximum 31-day wait for subsequent treatment where that treatment is surgery
97.8%
100%
Nov-15
94%
94%
Maximum 31-day wait for subsequent treatment where the treatment is a course of radiotherapy
98.5%
97.2%
Nov-15
94%
94%
EN
C 0
9
Page 8 of 14
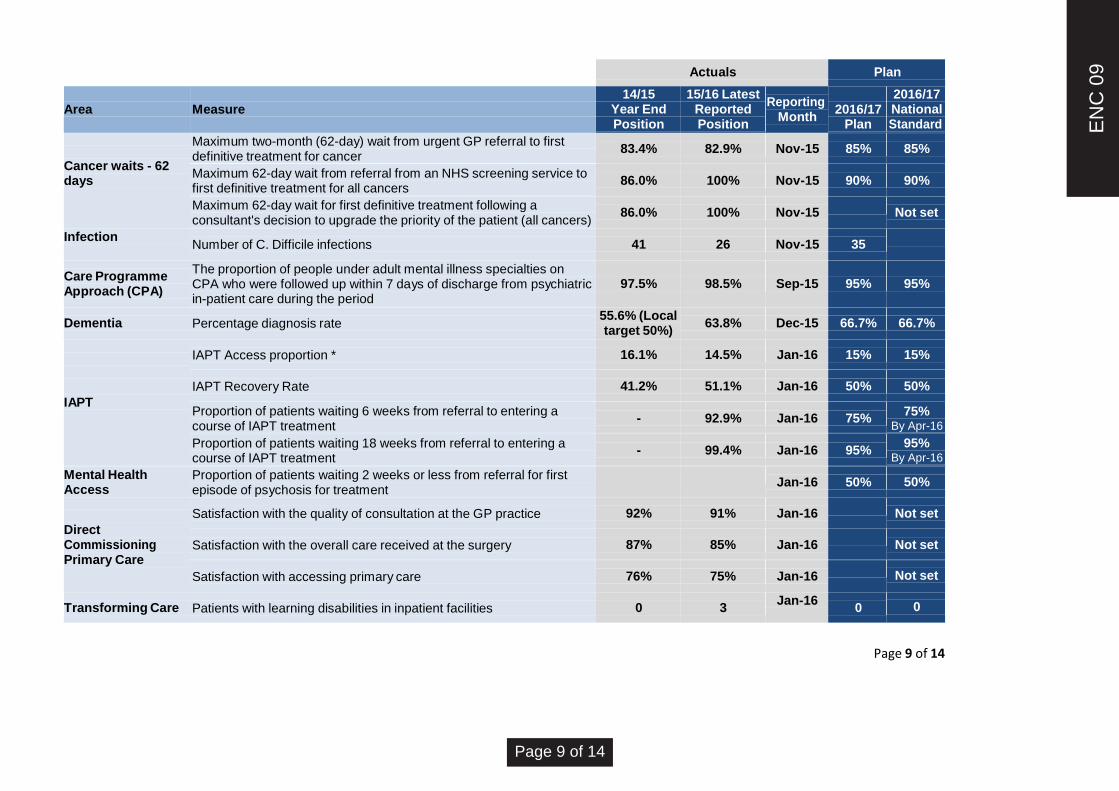
Page 9 of 14
Actuals Plan
Area
Measure
14/15 Year End Position
15/16 Latest Reported Position
Reporting Month
2016/17
Plan
2016/17 National Standard
Cancer waits - 62 days
Maximum two-month (62-day) wait from urgent GP referral to first definitive treatment for cancer
83.4%
82.9%
Nov-15
85%
85%
Maximum 62-day wait from referral from an NHS screening service to first definitive treatment for all cancers
86.0%
100%
Nov-15
90%
90%
Maximum 62-day wait for first definitive treatment following a consultant's decision to upgrade the priority of the patient (all cancers)
86.0%
100%
Nov-15
Not set
Infection
Number of C. Difficile infections
41
26
Nov-15
35
Care Programme Approach (CPA)
The proportion of people under adult mental illness specialties on CPA who were followed up within 7 days of discharge from psychiatric in-patient care during the period
97.5%
98.5%
Sep-15
95%
95%
Dementia
Percentage diagnosis rate 55.6% (Local target 50%)
63.8%
Dec-15
66.7%
66.7%
IAPT
IAPT Access proportion *
16.1%
14.5%
Jan-16
15%
15%
IAPT Recovery Rate
41.2%
51.1%
Jan-16
50%
50%
Proportion of patients waiting 6 weeks from referral to entering a course of IAPT treatment
-
92.9%
Jan-16
75% 75%
By Apr-16
Proportion of patients waiting 18 weeks from referral to entering a course of IAPT treatment
-
99.4%
Jan-16
95% 95%
By Apr-16
Mental Health Access
Proportion of patients waiting 2 weeks or less from referral for first episode of psychosis for treatment
Jan-16
50%
50%
Direct Commissioning Primary Care
Satisfaction with the quality of consultation at the GP practice
92%
91%
Jan-16
Not set
Satisfaction with the overall care received at the surgery
87%
85%
Jan-16
Not set
Satisfaction with accessing primary care
76%
75%
Jan-16
Not set
Transforming Care
Patients with learning disabilities in inpatient facilities
0
3 Jan-16
0
0
EN
C 0
9
Page 9 of 14

Page 10 of 14
Notes on NHS Constitution annual performance and plan - SUTTON CCG
Measure
Forecasting Achievement in 2016/17 where standard has not
been met in 2015/16
Variance to 2016/17 National Standard
Mixed Sex Accommodation There have been three breaches year to date This will be closely monitored and expected to achieve in 16-17
Referral to treatment times for non-urgent
consultant led treatment
Planned levels to exceed the target – close monitoring through the
planned care working group on a monthly basis expected 93%
Maximum two-month (62-day) wait from
urgent GP referral to first definitive treatment
for cancer
ESH have improved their position in relation to performance
against this target however there is still work to be done regarding
IHT and impact this has on Sutton CCG position
Percentage diagnosis rate for dementia Current rate is steadily improving – currently at 63.7%
Planned to achieve early in 2016 – work being undertaken with
practices and additionally work with care homes in the areas to
confirm diagnosis
IAPT Access proportion Currently at 14.5 % with a push to improve before year end to support delivery of access target in 16-17
IAPT Recovery Rate Currently achieving in January 16
This will fluctuate in early months of 16-17 to take account of
increased access to services. Capacity will need to be matched to
demands through marketing work
Cat A Ambulance Calls Awaiting confirmation from host commissioners regarding recovery / improvement plans for LAS
Maximum 31-day wait for subsequent
treatment where that treatment is an anti-
cancer drug regimen
Small cohort numbers – unable to achieve national standard
without showing 100% compliance.
Maximum 31-day wait for subsequent
treatment where that treatment is surgery
Maximum 62-day wait from referral from an
NHS screening service to first definitive
treatment for all cancers
Small numbers in cohort – 4 breaches of standard since April
2015.
Small cohort numbers – unable to achieve national standard
without showing 100% compliance.
Small cohort numbers – unable to achieve national standard
without showing 100% compliance.
EN
C 0
9
Page 10 of 14

Page 11 of 14
NHS Constitution trajectories Area
Measure
Target
2016/17 Plan
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
A&E waits Patients should be admitted, transferred or discharged within 4 hours of their arrival at an A&E department
95%
95%
95%
95%
95%
Cat A Ambulance Calls
Category A calls resulting in an emergency response arriving within 8 minutes – Red 1
75% Waiting plans from LAS commissioners
Category A calls resulting in an emergency response arriving within 8 minutes – Red 2
75%
Category A calls resulting in an ambulance arriving at the scene within 19 minutes
95%
Referral To Treatment waiting times for non-urgent consultant-led treatment
Admitted patients to start treatment within a maximum of 18 weeks from referral
90%
Non-admitted patients to start treatment within a maximum of 18 weeks from referral
95%
Patients on incomplete non-emergency pathways (yet to start treatment) should have been waiting no more than 18 weeks from referral
92%
93%
93%
93%
93%
93%
93%
93%
93%
93%
93%
93%
93%
Diagnostic test waiting times
Patients waiting for a diagnostic test should have been waiting less than 6 weeks from referral
99%
99%
99%
99%
99%
99%
99%
99%
99%
99%
99%
99%
99%
Cancer waits - two-week wait
Maximum two-week wait for first outpatient appointment for patients referred urgently with suspected cancer by a GP
93%
93%
93%
93%
93%
Maximum two-week wait for first outpatient appointment for patients referred urgently with breast symptoms (where cancer was not initially suspected)
93%
93%
93%
93%
93%
Cancer waits - 31 days
Maximum one month (31-day) wait from diagnosis to first definitive treatment for all cancers
96%
96%
96%
96%
96%
EN
C 0
9
Page 11 of 14

Page 12 of 14
Area
Measure
Target
2016/17 Plan
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Maximum 31-day wait for subsequent treatment where that treatment is an anti-cancer drug regimen
98%
98%
98%
98%
98%
Maximum 31-day wait for subsequent treatment where that treatment is surgery
94%
94%
94%
94%
94%
94%
94%
94%
94%
94%
94%
94%
94%
Maximum 31-day wait for subsequent treatment where the treatment is a course of radiotherapy
94%
94%
94%
94%
94%
94%
94%
94%
94%
94%
94%
94%
94%
Cancer waits - 62 days
Maximum two-month (62-day) wait from urgent GP referral to first definitive treatment for cancer
85%
85%
85%
85%
85%
85%
85%
85%
85%
85%
85%
85%
85%
Maximum 62-day wait from referral from an NHS screening service to first definitive treatment for all cancers
90%
90%
90%
90%
90%
90%
90%
90%
90%
90%
90%
90%
90%
Maximum 62-day wait for first definitive treatment following a consultant's decision to upgrade the priority of the patient (all cancers)
Not set
Infection
Number of C. Difficile infections
3
3
3
3
3
3
3
3
3
3
3
2
Dementia
Percentage diagnosis rate (over 65s)
66.7%
66.7%
66.7%
66.7%
66.7%
66.7%
66.7%
66.7%
66.7%
66.7%
66.7%
66.7%
66.7%
IAPT
IAPT Access proportion
15%
15%
15%
15%
15%
IAPT Recovery Rate
50%
50%
50%
50%
50%
Mental Health Access
Proportion of patients waiting 6 weeks from referral to entering a course of IAPT treatment
75% By Apr-16
75%
75%
75%
75%
Proportion of patients waiting 18 weeks from referral to entering a course of IAPT treatment
95% By Apr-16
95%
95%
95%
95%
Direct Commissioning Primary Care
Satisfaction with the quality of consultation at the GP practice
-
92
Satisfaction with the overall care received at the surgery
-
86
EN
C 0
9
Page 12 of 14

Page 13 of 14
Area
Measure
Target
2016/17 Plan
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Satisfaction with accessing primary care
-
76
Transforming Care
2
1
1
1
EN
C 0
9
Page 13 of 14

Sutton CCG continues to iterate the plan on a page which sets out the priority areas for delivery for the CCG. This latest draft is
attached.
Page 14 of 14
EN
C 0
9
Page 14 of 14

Page 1 of 24
Report to the Sutton Clinical Commissioning Group Governing Body
Date of Meeting: 2nd March 2016 Agenda No: 12 ENCLOSURE: 10
Title of Document: Performance and Quality Report
Purpose of Report: For Discussion
Report Authors: Mary Hopper, Director of Quality Siân Hopkinson, Director of Performance & Primary Care
Lead Director: Siân Hopkinson, Director of Performance & Primary Care Mary Hopper, Director of Quality
Executive Summary: This report is to inform and provide assurance to the Governing Body about the performance, quality and safety of service provision commissioned by NHS Sutton CCG. Performance is generally reported up to month 8 (November 2015) unless otherwise stated. Key issues to note are:
Performance against referral to treatment time (RTT) target achieved at aggregate level for every month of 2015/16
Epsom and St Helier Trust met all 6 of 6 Cancer Waiting Time Standards for (M8) November 2015 and met the challenged 62 Day Standard for the second time in 18 months.
Diagnostic test waiting time standard achieved in Month 8
A&E 4 hour wait pressures at Epsom and St Helier and St George’s in Month 8
London Ambulance Service failure to meet response time standards at London level, however improving performance in Sutton
Healthcare Acquired Infection rates are within thresholds for C. Difficile but there have been 2 cases of MRSA for Sutton CCG patients.
Improving Access to Psychological Therapies performance is achieving waiting time standards, but not meeting access or recovery standards
Dementia diagnosis rate has increased to over 63.2% but remains below national target of 66.7%
SWL Sector CCGs’ Contracted Mental Health Performance (Appendix 2). Access for Working Age Adults is not meeting waiting time standards.
GP Out of Hours service is achieving all performance standards up to November 2015 (Appendix 3)
EN
C 1
0
Page 2 of 24
Key sections for particular note (paragraph/page), areas of concern etc: Focus is on the issues highlighted above
Recommendation: The Sutton CCG Governing Body is asked to:
REVIEW the Performance and Quality Report.
Committees which have previously discussed/agreed the report: Executive and Quality Committee
Financial Implications: Activity levels in excess of those contracted will result in unbudgeted expenditure, and failure to meet annual targets for the Quality Premium will reduce the payment to the CCG.
Equality Impact Assessment: The CCG is committed to monitoring the compliance with the Equality duty of the providers from whom we commission services. This is done through the quality and contracting process.
Information Privacy Issues: The information contained in this report is in the public domain.
Communication Plan: This report will be published on the CCG public website as a report to the Governing Body.
Equality Impact Assessment: The CCG is committed to monitoring the compliance with the Equality duty of the providers from whom we commission services. This is done through the quality and contracting process.
Information Privacy Issues: The information contained in this report is in the public domain.
Communication Plan: This report will be published on the CCG public website.
EN
C 1
0

Page 3 of 24
1. Introduction
1.1 Ultimate responsibility for safeguarding the quality of care provided to patients rests with each provider organisation through its Board. However, CCGs, as statutory organisations are required to deliver the best possible services to and
outcomes for, patients within financial allocations. Therefore, Sutton CCG (SCCG) has a statutory duty to secure continuous improvements in the care that we commission and to seek assurance around the quality and safety of those services. This requirement is underpinned by national guidance and locally-determined commissioning intentions.
1.2 For example, the NHS Outcomes Framework forms an essential part of the way in which the Secretary of State for Health holds NHS England to account. Indicators in the NHS Outcomes Framework are grouped around five domains, which set out the high-level national outcomes that the NHS should be aiming to improve. The five domains of the NHS Outcomes Framework are covered by three dimensions against which the quality and safety of services should be measured; they are Effectiveness, Patient Experience and Safety.
1.3 In addition, the CCG’s aim is to provide a continuous focus on improving the quality and safety of services that we commission to give assurance that key benefits are realised for patients.
1.4 This report is to assure the Quality Committee/Executive Committee and the Governing Body that the CCG monitors the performance of the NHS healthcare providers it commissions against the key performance and clinical quality and safety indicators and that those areas of concern or risk to patients are highlighted and addressed. The report presents an overview of quality of care and patient safety matters, with narrative around areas of concern and risk.
1.5 Section One of the report summarises performance against the key areas outlined below and forms the basis of the Local Area Team’s quarterly Assurance meetings:
NHS Constitution
CCG Outcome Framework
1.6 The performance dashboard for Sutton CCG patients (Appendix 1) reflects the formal reporting of the performance position against the goals and core responsibilities of the CCG as outlined in ‘Everyone Counts: planning and
EN
C 1
0

Page 4 of 24
priorities for patients in 2014/15 – 2018/19’ and the ‘CCG Assurance Framework 2015/16’. Matters of concern are addressed throughout this report.
1.7 Section Two of the report provides information about Sutton CCG’s main providers based on each Trust’s performance against a range of quality indicators and reports on all available data at the time of writing the report (01.02.16). This contains national and local data, formal and informal, for all patients (not only Sutton). Detail about key risk areas is within the report by Provider. In this way, any wider concerns around quality and safety leading to potential risk to Sutton CCG patients are addressed.
Risk Management
1.8 Each provider has its own internal governance and risk management processes. Providers own risks relating to contractual requirement are discussed at contract meetings and Clinical Quality Review Group/Monitoring meetings.
1.9 Where inadequacies in provider performance around quality and safety are assessed to be a risk to the CCG as a commissioner of those services, these will be raised on the CCG’s Quality Risk Register or Governing Body Assurance Framework.
2 Executive Summary
2.1. There is a summary of the key concerns at the start of Section One and Section Two.
Section One
1.0 Executive Summary
This report summarises performance against key standards for the year to date, from April 2015 to November 2015 (Month 8) unless otherwise stated. A dashboard of key indicators is attached as Appendix 1. Key performance issues for Sutton CCG’s population are:
Waiting times and waiting lists
o Referral to Treatment (RTT) –Sutton CCG has met this standard for every month of 2015/16, achieving 92.7% at Month 8, against a target of 92%.
o Cancer waits – Sutton CCG has met 8 of the 9 cancer waiting time standards for (M8) November 2015. The CCG did not achieve the 62 Day Urgent Referral Standard, however there was an improvement on M7 performance.
Epsom and St Helier Trust met all 6 cancer waiting time standards for (M8) November 2015 and sustained the 62 Day standard for a second month.
o Diagnostic waits – Sutton CCG achieved the Diagnostic waits target (99%) at Month 8, with performance of 99.2%.
EN
C 1
0

Page 5 of 24
52 week breaches - Sutton CCG had one 52 week wait in the provisional November data that has since been removed in the final data.
A&E Waiting Times
o Epsom and St Helier Trust did not achieve the A&E target in November with performance of 94.4%. The unvalidated figure for December is 93.16%. Year to date performance at 10/2/16 (unvalidated) was just below the standard at 94.96%.
o St George’s Foundation Trust did not achieve the A&E target in November with performance of 89.1%. Commissioners continue to monitor the trust against the actions in the Action Plan.
Ambulance Response Times
o London Ambulance Service (LAS) have not met any of the 3 standards London-wide for response times in 8 minutes and 19 minutes since May 2014 and have an improvement plan in place. It is total London performance that is reported in the dashboard at Appendix 1, however current Sutton only performance for December for 8 minute responses is significantly better:
Target
Sutton only
Ambulance Red 1 8 minute response 75% 88.9%
Ambulance Red 2 8 minute response 75% 68.5%
o Local response times in Sutton continue to improve towards the action plan trajectory, with Red 1 performance now exceeding target for the last 5 months, and the Cat A 19 minute target almost back to plan at 94.4% (target 95%). Commissioners across London continue to monitor progress against the agreed action plan.
Healthcare Acquired Infections (HCAI)
o Sutton CCG had two MRSA cases and five additional Clostridium Difficile cases reported in November. This brings the YTD figure for C. Difficile to 26 against an annual objective of 41 for 2015-16.
Improving Access to Psychological Therapies (IAPT)
o The IAPT service met both the 6 week and 18 week waiting time trajectories in December 2015 (97% & 100% respectively).
o The number of IAPT patients entering treatment fell below the 15% trajectory, at 13% in December 2015.
o The IAPT recovery rate for December was at 42.7%, again falling below the 50% trajectory, but an improvement on the previous month.
o A marketing plan was put in place in November to increase referrals to the IAPT service and subsequently numbers entering treatment.
EN
C 1
0
Page 6 of 24
Dementia
o Sutton’s December 2015 dementia diagnosis rate is 63%.This rate is still currently short of the 66.7% national target.
o This continues to be an area of focus for the CCG, with continued practice coding management, data harmonisation across providers and improving diagnosis rates in our Care Homes.
Community Services
o As of December 2015, Sutton and Merton Community Services (SMCS) achieved the majority of their KPIs. The main areas of non-achievement continue to be access for diabetes education, specialist nursing services, podiatry and children’s therapies.
2.0 Waiting times and waiting lists 2.1 18 Week Referral to Treatment (RTT) 2.1.1 Under the NHS Constitution patients have a right to start consultant-led
treatment within a maximum of 18 weeks. The Planned Care Working Group, chaired by Dr Chris Elliott, monitors Epsom and St Helier’s elective performance, both in terms of activity planned and undertaken, and waiting times, including cancer pathways and diagnostics.
2.1.2 At Month 8 Sutton CCG had 92.7% of patients on incomplete pathways waiting
less than 18 weeks, against a target of 92%. Capacity and pathway issues are monitored and discussed at the Planned Care Working Group.
2.1.3 Additional capacity for 300 patients has been sourced from the independent sector and Epsom and St Helier are offering suitable patients the choice of surgery on earlier dates than if they were to wait for treatment at Epsom or St Helier Hospitals.
2.2 Cancer Waiting Times
2.2.1 62 day standard following GP referral This measure is part of the NHS Constitution and is based on data from the Open Exeter System. The target is for a minimum of 85% of patients to receive first definitive treatment within 62 days of an urgent GP referral for suspected cancer. It should be noted that breaches due to patient choice are included.
2.2.2 The resilience of performance against this standard nationally is of concern to NHS England. Epsom and St Helier Trust (ESHT) are implementing a detailed improvement plan, developed following the visit from the national Intensive Support Team. The Trust’s progress against their plan is monitored by the Planned Care Working Group, chaired by Dr Chris Elliott.
2.2.3 Sutton CCG has not achieved this standard since May 2016 although performance has improved over recent months. In November 82.9% of patients were treated within 62 days against the 85% threshold. There were 7 breaches from 41 Patient Pathways.
EN
C 1
0

Page 7 of 24
2.2.4 Epsom and St Helier as a trust met the 62 Day Standard for a second month. 2.2.5 Specific progress against the action plan has been made as follows:
The new substantive General Manager appointed by the Trust is progressing with the implementation of the delivery plans.
The Trust continues to clear their backlog and is currently implementing remedial action plans.
Epsom and St. Helier continue to work with The Royal Marsden to ensure timely referral of patients requiring tertiary care and initial review of the Urology Pathway.
The Trust has completed capacity and demand modelling for Outpatients, Endoscopy and Radiology.
The Trust has also approved 2 Urology Consultants and an additional SpR Post.
Template biopsy machine is now in situ and the machine is currently being calibrated.
The Trust has secured additional mobile CT scanning capacity and is moving to 7 day working.
The Trust has commenced “straight to test” pathways at both Epsom and St Helier sites for Lower GI patients.
2.3 Diagnostic 6 week wait
2.3.1 The CCG achieved the Diagnostic waits target (99%) in November with
performance of 99.2%. 2.4 52 week breach
2.4.1 Sutton CCG had one 52 week wait in the provisional November data that has
since been removed in the final data. In this instance, the patient had not been waiting 52 weeks or more as there was an error on the system. The error was recognised after reporting the beach and the report has since been amended. South East CSU has requested further information on the error and has asked for further details to provide assurance that there is no risk to a 52 week wait in this instance.
3.0 A&E waiting times 3.1 Epsom and St Helier Hospitals did not achieve the 4 hour standard in
November, with 94.4% performance against the 95% target. The trust met the target on eleven days, but also reported a daily performance below 90% on four occasions.
3.2 St George’s did not achieve the A&E target in November with performance of 89.1%. The provisional and unvalidated position for December is 88.6%.The trust met the 95% target on three days in November, but also reported a daily figure below 90% on fifteen occasions. The trust continues to work through their Action Plan and the CSU and CCGs continue to monitor the trust against the actions in the Action Plan that resulted from the contract query and joint investigation.
EN
C 1
0

Page 8 of 24
4.0 Ambulance response times 4.1 London Ambulance Service (LAS) are failing to meet the Category A targets to
respond to 75% of calls within 8 minutes, with performance for London in December being 72.8% for Red 1 and 65.9% for Red 2, whilst the Sutton performance was better at 88.9% for Red 1 and 68.5% for Red 2.
4.2 Hear and treat activity has reduced over the last 2 months and is now 6.5%
under plan (12.8% London wide), with overall activity 2.8% under plan for Sutton (5% under plan London wide).
4.3 Commissioners across London continue to monitor progress by LAS against
their recovery plan.
5.0 Healthcare Acquired Infections (HCAI) 5.1 Sutton CCG had two MRSA cases reported in November. This case has been
investigated thoroughly and was sent to the NHS England Arbitration Panel for consideration as third party.
5.2 Five additional C. Difficile cases were reported in November. This brings the
YTD total to 26 against an annual objective of 41 for 2015-16. 5.3 Epsom and St Helier have identified 64 cases of Clostridium Difficile trustwide
YTD. Of these cases 23 have been trust apportioned against an objective of 39 cases. A review of all cases reported in Quarter one and two by the CCG did not identify any lapses in care. Of these 64 cases, 18 have been identified as Sutton CCG patients.
5.3 Minimising HCAIs remains a high priority for the CCG and is routinely discussed
at Clinical Quality Review Group (CQRG) meetings.
6.0 Improving Access to Psychological Therapies (IAPT) 6.1 The number of patients entering treatment during December 2015 was at 13% of need, below the 15% National trajectory. 6.2 The percentage reaching recovery in December 2015 was 42.7%, an improvement on November but still short of the 50% trajectory. 6.3 97% of patients referred to the IAPT service entered treatment within 6 weeks of
referral and 100% within 18 weeks of referral during December 2015, meeting the national targets of 75% and 95% respectively.
6.4 An investment has been made (Nov 15) in marketing the IAPT service to boost
referral numbers and subsequent entering treatment rates. This forms part of the wider IAPT recovery plan.
7.0 Dementia Diagnosis 7.1 Sutton’s December 2015 dementia diagnosis rate is at 63.2%.
EN
C 1
0

Page 9 of 24
7.2 This rate is still currently short of the 66.7% national target and will continue to be an area of focus for the CCG in 2015/16.
7.3 There is significant focus within Sutton on improving dementia care. In particular there is continued targeted focus with those practices with the lowest reported rates of diagnosis and work in progress to increase diagnosis rates in care homes.
8.0 Child and Adolescent Mental Health Services (CAMHS) Performance 8.1 South West London (SWL) CCGs issued a contract query notice in relation to the South West London and St George’s Mental Health Trust performance
against the 8 week target for CAMHS assessments, particularly around long waits for ASD/ADHD assessment. An action plan is in place to address this issue.
8.2 Sutton has seen an improved Q3 performance position in terms of increased efficiency and increased assessments undertaken. Wait time for access to
CAMHS was 3.7 weeks with 91% of referrals seen within 8 weeks. 94 % of young people referred to CAMHS for an urgent appointment were seen within 7 days (1 child was outside this timeframe due to parents being unable to bring the child to the first available appointment) and 100 % of young people referred to CAMHS as an emergency were seen within 24 hours. Waiting times for ASD/ADHD assessment have improved but remain significantly outside the 8week target with only 22% of referrals being seen within 8 weeks and average wait times of 16.9 weeks.
9.0 Mental Health Contract
9.1 A dashboard of SWL Sector CCGs’ Contracted Mental Health Performance is attached as Appendix 2.
9.2 Exceptions: Access
Sutton remains behind target against one of the Access Targets:
Access to services 1 - Adult Community Mental Health Teams (CMHTs): Percentage of patients that were assessed within 28 calendar days of referral (Non-Urgent Referrals) - with performance of 73% against the 80% Target. This is an improvement from 62% in the previous month. This deterioration is due to data migration following the implementation of the new Sutton Uplift Service. This has been addressed by the provider and both monthly and cumulative performance is expected to continue to improve.
Access to services 1 - Older People’s CMHTs: Percentage of patients that were assessed within 28 calendar days of referral (Non-Urgent Referrals) - with a performance of 80% against the 70% Target. This is a significant improvement on the previous month.
EN
C 1
0

Page 10 of 24
10.0 Community Services
10.1 Achievement of Key Performance Indicators (KPIs) As of December 2015, Sutton and Merton Community Services (SMCS) achieved the majority of their KPIs. The main areas of non-achievement continue to be access for diabetes education, specialist nursing services, podiatry and children’s therapies.
10.2 SMCS have undertaken a demand and capacity review for DESMOND education sessions for patients with diabetes. There have been increased referrals to DESMOND in addition to staffing gaps. New staff is now in post and are able to support the service following completion of their DESMOND educator course in early October. The following action plan is in place and continues to monitor KPI performance and progress:
A full review of alternatives to DESMOND education sessions (including an alternative to a class-based session) to offer more choice and better access;
Additional Saturday half day sessions for DESMOND available at The Nelson Centre to reduce waiting times;
Skill mix review to inform staff required to deliver DESMOND programme.
10.3 The following action plan is in place for all specialist nursing services: diabetes; heart failure and respiratory:
Demand-and-capacity modelling;
Additional diabetes clinics now in place;
Text confirmation/reminder service to reduce DNA / cancellation rates;
Recruitment to vacancies – heart failure specialist nurse in post September; respiratory specialist nurse in January.
10.4 Routine access to podiatry services is improving with 79% of Sutton patients
being seen within 30 days and should achieve the waiting time target by Q4.
10.5 Waiting times to access the falls prevention service have now improved following the challenge incurred by the change to the pathway, which now accepts referrals direct from London Ambulance Service. Additional short term investment is now in place to address the backlog whilst undertaking a service review to identify sustained additional capacity requirements. 84% of Sutton referrals for urgent home response were seen within 2 weeks and 100% of Sutton patients attended a falls class within 10 weeks of referral.
10.6 Access to children’s therapies is improving following additional investment within the service and should achieve waiting time target by Quarter 4. All children’s therapy services except occupational therapy are now 18 week compliant.
10.7 Improvement in delivery of the Musculoskeletal (MSK) service and outpatient physiotherapy is being sustained with 96% of physiotherapy referrals seen within 6 weeks.
EN
C 1
0

Page 11 of 24
11.0 GP Out of Hours
11.1 The GP Out of Hours service, provided by SELDOC, have achieved every national quality standard for every month of 2015/16 up to November. See dashboard at Appendix 3.
EN
C 1
0

Page 12 of 24
Section Two
Executive Summary
1. Executive Summary
1.1 This section of the report provides information about Sutton CCG’s main providers based on each Trust’s performance against a range of quality indicators and reports on all available data at the time of writing the report. This contains national and local data, formal and informal, for all patients (not only Sutton). Detail about key risk areas is within the report by Provider. In this way, any wider concerns around quality and safety within individual providers that may lead to potential risk to Sutton CCG patients are addressed. In addition, it gives an opportunity for organisational performance against a number of quality metrics to be benchmarked against similar providers.
2. Epsom and St Helier University Hospitals NHS Trust (ESH) 2.2 Health Care Associated Infection (HCAI)
2.21 MRSA
There were no MRSA cases reported in September. A case was reported in November in a Merton resident. After a thorough investigation this was sent to the NHSE arbitration panel for consideration of 3rd party assignment. The panel reviewed the case and have finally assigned the case to the Trust. The source of the infection was a long-standing wound. This brings the total number of Trust assigned MRSA Bacteraemias to 3 and includes 2 previous cases identified as contaminants.
2.22 C. Difficile
There were 4 Trust apportioned cases of C. Difficile reported in September, bringing the Trust’s position to 15 against the internal trajectory of 17. There have been 23 reported trust cases of Clostridium difficile against the annual objective of 39 cases. A review of cases in both Quarter 1 and Quarter 2 have not identified any lapses in care.
2.23 Epsom and St Helier Hospital are one of thirty Trusts who have been asked to participate in a 90 day NHS infection prevention and control collaborative improvement programme supported by the NHS Trust Development Authority. The aim of the programme is to deliver an improved experience and clinical outcomes for patients through the delivery of best practice pathways in IPC, whilst also seeking to measure, monitor and reduce the cost of care by having a zero tolerance to avoidable infections. The programme will be launched on the 9th March 2016.
2.3 Key Issues Discussed at Clinical Quality Review Group (CQRG)
EN
C 1
0
Page 13 of 24
2.31 Enhanced Discharge Communication for GPs
The Trust circulated a template detailing the changes to hospital discharge summaries for Acute Kidney Infection and Dementia in line with the national CQUINs requirements. It was noted that the additional follow-up information section “Renal function to be monitored by GP with regular tests” was not sufficiently clear for GPs. Trust confirmed this is also accompanied by a narrative providing further details as to the nature and regularity of tests to be performed. The group noted the changes and felt that the success of the enhanced discharge summaries should be best monitored through a sample audit involving both the Trust and primary care for greater triangulation.
2.32 Pressure Ulcer Management update
The Trust submitted a revised paper to provide commissioners with appropriate assurance around their current management of category 3 and 4 pressure ulcers in light of the recent changes to the NHSE SI Reporting Framework, key ones being the six conditions that a pressure ulcer has to meet in order to be reported as an SI.
Since the changes to the guidance in March 2015, the Trust has been working hard to maintain the same strong focus on pressure ulcers assessment, capturing, reporting and prevention. The paper detailing the current processes through which the Trust assures itself of the appropriate management of pressure ulcers was summarised to the group as follows:
• All patients who enter the hospital are assessed for pressure ulcers within 6 hours of admission, this target is met for 96-98% of patients.
• pressure ulcers not noted on admission are declared as hospital acquired if noted within 72 hours of admission and reported to Datix.
• There is ongoing liaison with tissue viability nurses from Central Surrey Health, Merton and Sutton to ensure the accuracy of the data captured.
• In August 2015 ESTH started to capture via Datix patients admitted with multiple sites of Pressure Ulcer damage. For the majority of these patients, the primary sites of pressure damage are the heel and sacrum; this is consistent with national figures.
• All category 2 pressure ulcers have a mini RCA carried out, including treatment to date, documentation completed and timeline for completion and pathways in place for the patient. The results of the RCA are then fed back to the Head of Nursing and ward managers to ensure the recommendations can be implemented as soon as possible. The Trust reported ongoing difficulties in capturing category 2 pressure ulcers.
• All admitted category 3 pressure ulcers trigger a prima fascia meeting , where all the patient notes from the first 72 hours of admission are being reviewed and further discussed with the Director of Nursing and ward managers in a subsequent meeting that is convened in the next 72 hours.
• In terms of scrutiny at patient safety forums, there is a monthly pressure ulcer report that forms part of the CQAC agenda.
EN
C 1
0
Page 14 of 24
Trust highlighted that the main issue they are encountering is the high number of patients presenting with pressure ulcers acquired prior to admission and the difficulty in tracing the pressure ulcer back to the original setting of occurrence. This issue highlighted the need for an integrated pressure ulcers reporting and alert system between the Trust and community services. Both Sutton and Surrey Downs commissioners agreed to support the Trust in developing this system and facilitate engagement from all the relevant agencies.
2.34 November Stroke Audit review
The outcome of the November Stroke Audit review carried out at ESTH was circulated for information to the group.
It was noted that Trust was compliant with most of the Stroke standards, with key areas of non-compliance being: 90% of patients stay spent on a stroke unit and 90% of patient repatriated within 24 hours. An action plan is being developed following the visit.
2.35 Older People/Dementia update
Trust presented their new model of care for patients with Dementia currently being piloted in C2. The need for this model emerged from a qualitative audit carried out by Dementia Care Matters which identified a number of areas for the Trust to focus on, including staff awareness and the patient environment.
• C2 features a number of improvements, creating a more therapeutic environment to help people with dementia feel less disoriented and confused, such as patients’ beds having pictures of their favourite flowers.
• To prevent this from being a long-stay ward, there is a set of admission criteria in place, one being that it is only for patients with an established diagnosis of dementia and who have a high risk of falls.
• In terms of discharge planning from the ward, this will be supported by the SWOOP team in addition to the ward therapists.
• A set of KPIs measuring patient outcomes has also been put in place for this model.
• Trust confirmed there have been some previous issues regarding consultant cover for this ward. These have been resolved in the short term whilst alternatives to ensure suitable cover in the long term are explored.
2.36 CQC update
Work continues following the informal visit feedback, however the Trust are still awaiting the final report from the visit in November.
2.37 Cancer 62 day
The Trust met the standard for the third month in a row (October 87.4%; 86.6% November), and achieved 86% in December. The SWL pathway ‘switches’ for
EN
C 1
0
Page 15 of 24
Urology (MRI & TRUS biopsy) and Lower GI (straight to test) have been implemented to support the 62 cancer waits.
SWL performance has been compliant in meeting the 62 day urgent referral standard in November and December. The new guidance on the 62 day cancer breach reallocation process has been rolled out in shadow form. It focuses on referring trusts processing a referral by day 42 and receiving trusts, providing treatment within 20 days. The new process will make delivery challenging for pathways involving more than 2 providers, where the delay occurs with the middle provider.
The Systems Leadership forum has had bi weekly meetings with providers and CCGs.
Regular teleconferences are held with the Trust and weekly review of cancer PTLs, to understand ‘shared pathways’ and movement on waiting lists/backlog for both 62 days and 104 days by speciality.
2.371 Prostate Follow up Project:
A Prostate Steering group jointly set up with the Trust’s Urology team is looking at replicating a best practice model implemented by Croydon CCG. This involves a follow-up service in the community to be set up to manage prostate cancer patients. A specification has been reviewed by the Clinical Strategy group, and partner CCGs have been invited to share the learning from the Croydon model.
To support work on early detection, Sutton CCG’s cancer team have linked up with Health Specialist Advisors from SWL’s Bowel Cancer Screening Hub have presented to the Pharmacy forum to promote screening tools in Sutton which can be used by community pharmacists to highlight symptoms.
2.372 Practice Visits:
Our Macmillan GP in partnership with the CRUK Facilitator have been busy visiting Sutton practices to discuss Cancer Screening and Early Diagnosis with GPs and the members of the primary health care team.
Data available from the Public Health England’s Cancer commissioning toolkit summarises practice profiles which detail the number of TWR referrals made, conversions to cancer, performance data on Breast, Bowel and Cervical screening – this allows practices to benchmark themselves to the CCG and England mean. It also allows practices to reflect on the areas that could be improved e.g. two referral rates for suspected cancer vs conversion rates, screening statistics versus the England Standard rates.
Visits have also triggered discussions around TWR processes within the practice and use of available tools, such as SEA template (Significant Event Analysis recommended by RCGP) which can be used to reflect and report on significant events in practice and discuss actions that can be put in within the Practice following the significant event. Safety netting methods during consultations have also been discussed within the Practice team and how these can be improved (e.g. electronic alerts for non-responders; checking current contact details before referring patients; using a ‘task list’ on EMIS and maintaining a TWR register/ log to follow up on patients who can potentially be
EN
C 1
0

Page 16 of 24
lost in the system; SEA templates help practices with CQC visits and GP appraisals, and encourage teams to nurture a culture of continued ‘learning and improving’)
Visits have also provided an opportunity to share information with practices such as the LCA’s Patient Information Leaflet (PILS); ‘Straight to Scope’ which the CCG has linked in with the trust to support them on one of the stratified pathways we need to focus on under the cancer commissioning intentions. Practices have also been given the Rapid Referral guidance toolkit produced by Macmillan which summarises the NICE referral guidelines for suspected cancer; which aims to provide GPs with practical support and guidance in the light of the new NICE guidance published in 2015 and the new PAN London electronic forms for suspected cancer due to come out in Spring 2016.
Practices have been notified about the new FIT pilot for bowel screening and encouraged to continue to raise awareness around cancer (smoking cessation) screening (posters and flyers have been made available by CRUK).
A follow-up email is then sent to the Practice visited summarising the discussions during the practice visits and attaching electronic links for the toolkits discussed as well as other electronic links that the GPs may find useful during that daily practice to improve early detection of cancers and cancer screening rates.
Sutton CCG has also opted to be one of three CCG’s pilot sites for the Cancer Care Review (led by TCST) to plan for the survivorship or ‘Living with or Beyond’ cancer agenda, as part of the holistic pathway for patients post discharge.
2.4 Serious Incidents Requiring Investigation and Never Events
The Trust has reported two never events year to date. The Trust has undertaken a number of learning events to share the findings of the first investigation and have been proactively working with the CCG to find opportunities to do this with external partners as well as within the Trust.
3. Sutton and Merton Community Services (SMCS)
3.1 Commissioning for Quality and Innovation (CQUIN)
SMCS achieved all CQUINs in Q3 2015/16; the prevention of admissions CQUIN sets to decrease emergency admissions to hospital for patients under the care of SMCS. This includes people living within residential homes (who are on the SMCS caseload) and on the Integrated Locality Teams (ILT) caseload. This will be measured by the rate of emergency admissions for patients known to community services (ILT) in 2015/16 (Q2 to Q4) as compared to the rate in 2014/15 (Q2 to Q4) Another CQUIN is to improve the care of venous leg ulcers percentage of ulcers that have healed. The final CQUIN supports wellness and promotion of self-care in patients with long term conditions and aims to empower and educate patients to take control of their own health needs and administer their own medication, where appropriate, leading to greater independence.
EN
C 1
0

Page 17 of 24
3.2 Care Quality Commission (CQC)
SMCS is currently compliant in all standards that have been inspected. This service has not been inspected yet.
3.3 Serious Incidents Requiring Investigation and Never Events.
SMCS has not reported any Never Events or any Serious Incidents excluding pressure ulcers in April-Dec 2015/16. 40 SMCS attributable acquired category 3 and 4 pressure ulcers (SIs) were reported April-Dec 2015/16
3.4 Achievement of KPIs
As of December 2015 SMCS achieved the majority of contract KPIs. The main areas of non-achievement remain access for diabetes education, specialist nursing services, podiatry and children’s therapies.
SMCS have undertaken a demand and capacity and skill mix review for diabetes education sessions; additional clinical staff are now trained and in post delivering additional capacity including Saturday sessions. A full review of alternatives to the current DESMOND education programme will be complete by November 2015 which will include alternative to a class-based session to offer more choice and improve access.
An action plan is in place for all specialist nursing services; diabetes; heart failure and respiratory which includes demand and capacity modelling and text confirmation /reminder service to reduce DNA/cancellation rates. Additional diabetes clinics are now in place and recruitment to vacancies has been successful with heart failure specialist nurse in post September and respiratory specialist nurse due in January.
Routine access to podiatry services is improving with 79% of patients being seen within 30 days and SMCS should achieve the 90% waiting time target by Q4.
Waiting times to access the falls prevention service have now improved following the challenge incurred by the change to the pathway, which now accepts referrals direct from London Ambulance Service. Additional short term investment is now in place to address the backlog whilst undertaking a service review to identify sustained additional capacity requirements. 84% of Sutton referrals for urgent home response were seen within 2 weeks and 100% of Sutton patients attended a falls class within 10 weeks of referral.
Access to children’s therapies is improving following additional investment within the service and should achieve waiting time target by Quarter 4. All children’s therapy services except occupational therapy are now 18 week compliant.
Improvement in delivery of the musculoskeletal service and outpatient physiotherapy is being sustained with 96% of physiotherapy referrals seen within 6 weeks.
EN
C 1
0

Page 18 of 24
4. South West London and St George’s Mental Health NHS Trust (SWL&StG)
4.1 Secondary Care
As at period 9 (December) Sutton services are performing well against the majority of performance/quality indicators set within the contract arrangements with the trust. The exception being Access for Working Age Adults:
The fall in performance for Access to services for Working Age Adults relates to the implementation of the new Sutton Uplift services. This was due to administrative systems changes and the trust has assured the CCG that this will show a significant improvement from October/November.
In respect to Access to services for Older People: This area has seen a significant improvement in performance over the past 3 months with a rise from 59% of patients being assessed within 28 days in November to an 80% rate in December against 70% target. With the increase in dementia diagnosis referrals the CCG has committed significant investment in this area to increase the capacity of the Memory Assessment Service. The trust has assured the CCG that this performance is now sustainable.
South West London (SWL) CCGs issued a contract query notice in relation to the South West London and St George’s Mental Health Trust performance against the 8 week target for CAMHS assessments, particularly around long waits for ASD/ADHD assessment. An action plan is in place to address this issue.
Sutton has seen an improved Q3 performance position in terms of increased efficiency and increased assessments undertaken. Wait time for access to CAMHS was 3.7 weeks with 91% of referrals seen within 8 weeks. 94 % of young people referred to CAMHS for an urgent appointment were seen within 7 days (1 child was outside this timeframe due to parents being unable to bring the child to the first available appointment) and 100 % of young people referred to CAMHS as an emergency were seen within 24 hours. Waiting times for ASD/ADHD assessment have improved but remain significantly outside the 8 week target with only 22% of referrals being seen within 8 weeks and average wait times of 16.9 weeks.
4.2 Primary Care
The new Primary Mental Health Care service (Sutton Uplift) started in July 2015. This service looks to bring together all aspects of mental healthcare including a Single Point of Access and a Wellbeing Arena, and the service contains the Improving Access to Psychological Therapies (IAPT) service.
The IAPT performance targets remain high profile and an area the service is currently underachieving. The service is committed to achieving the core IAPT targets of 15% Access and 50% Recovery. The service has produced significant performance assurance through action plans and regular meetings.
5.0 Organisational Quality Responsibilities
EN
C 1
0

Page 19 of 24
5.1 Safeguarding Adults and Children
Policies and Guidance: Both the adult and the children safeguarding policies have been reviewed. Final draft of the reviewed Safeguarding Children policy was ratified at the September 2015 Governing Body. The Safeguarding Adult Policy was ratified at the January 2016 Board. The publication of the Pan London Adult Safeguarding Guidance has now been finalised, and was formally launched on 9th February 2016. Organisations are expected to be compliant by April 1st. The Intercollegiate Guidance for Safeguarding Adults was brought out in December 2015 in draft format for consultation until 29th December. There is no date currently for final release.
In January 2015 the first Safeguarding Assurance Committee met and agreed a Safeguarding Assurance Strategy for 2015/16 and the action plan for the strategy has been reviewed at subsequent committees. The Committee will meet a minimum of quarterly and report into the Quality Committee. The last meeting was on December 10th 2015.
Significant Meetings/Information: Sutton LSCB met on 11th February 2016. The Sutton Safeguarding Adult Board (SSAB) met on 19th January 2016. Feedback from these meetings has been disseminated to the CCG through staff workshops and to member practices through dedicated education sessions.
NHSE London and SCCG met to complete a deep dive audit on 12th November 2015. The designated professionals and executive lead for safeguarding attended the meeting. Feedback on the deep dive is anticipated from NHS England during week commencing 15th February 2016.
5.2 Safeguarding Adults
The Sutton Safeguarding Adults Board (SSAB) has a Quality and Performance sub group which is chaired by the CCGs Director of Quality. The group has now completed on the development of a safeguarding assurance dashboard for partners to complete and a peer audit tool to quality assure on case work. It is anticipated that a pan London dashboard will however be formulated to replace the CCGs own by year end. The SSAB also has a Safeguarding Adult Review (SAR) sub group which is co-chaired by the CCGs Designated Adult Safeguarding Manager – this considers cases where abuse or neglect has occurred but where inter-agency working could be improved in order to prevent a recurrence. A SAR policy, formulated by the sub-group, was approved by the SSAB in January 2016.
The appropriate levels of safeguarding adults (and safeguarding children) and mental capacity training was last delivered to all CCG staff still requiring this on January 25th 2016. Training will now be delivered on a rolling 6 monthly basis to ensure staff are able to receive this mandatory training in a timely manner. Safeguarding Adult Level 3+ training will be delivered by an external trainer, “St Thomas Training” who was successful during the recent CCG/LBS tender process, to CHC staff and members of the Medicines Optimisation Team who have patient contact. A programme will run 2 days a month throughout 2016.
Prevent: The CCG is required by NHS England to provide a quarterly return on the Prevent Strategy. The return includes information on training and policy for the CCG and confirmation of assurance that its statutory health providers are meeting their responsibilities in this area. Awareness training was provided to
EN
C 1
0

Page 20 of 24
GP Safeguarding Adult Leads at the GP Forum in July 2015. CCG staff have also received awareness training, delivered at a staff forum in May and again in January 2016 – this will be now repeated every 6 months. The more comprehensive "WRAP3" for practitioners has now been delivered to staff and managers at the CCG mental health commissioned 12 bedded recovery service, as well as the Forensic Mental Health Hostel in York Road and to community staff at St Raphaels. It has also been offered to a further forensic hostel provision on Sutton Common Road. The Safer Sutton Partnership’s Prevent Lead, has now successfully co-ordinated the Channel Panel and these are running monthly. The CCGs DASM attends to represent the health economy. Two whole day events are due to take place in early March, with a half day focus on children and half day focus on adults.
Mental Capacity & DoLS: Awareness training on MCA and DoLs for CCG staff took place again as planned in January. St Thomas Training have commenced providing 2 days a month of MCA and DoLs training to anyone in Sutton services, including care home, and NHS staff and this will continue until March 2017. Additional hours were retained by the CCG to offer to the NHS acute and community providers and to the Vanguard programme, in order to meet their specific needs. To date these have been taken up by both Royal Marsden and St Raphael’s Hospice.
The second GP Safeguarding Adult Leads Forum was held in November and concentrated on Mental Capacity. A repeat session was delivered for CCG clinicians and other practice staff. Feedback received has informed that this was very well received by those attendees who responded to the on-line questionnaire, and that the next GP leads forum, in June, should concentrate on Advance Decision and Best Interest Decision making.
5.3 Safeguarding Children
The current children Serious Case Reviews (SCRs) have all been to the LSCB and one is awaiting a publication date. Assurance work is in place through the CCG Safeguarding Assurance Strategy and the LSCB Case review Sub Group to monitor and seek assurance on action plans for providers and our own internal action plans. The LSCB has a Case Review Sub Group which leads on this function and the designated professionals will be able to monitor actions through this forum and report on the CCG’s progress with action plans.
Looked after Children during quarter 1, 2 and 3 the timeliness of health assessments for looked after children has not been optimal. An improvement plan with children’s social and providers has been implemented. All parties are meeting regularly through a LAC health working group and performance calls to ensure that health assessments are being undertaken within timeframes. The performance has begun to improve and support from the newly appointed Designated Nurse for Looked after Children who is regularly escalating delays with social care and commissioned providers.
On 14th January 2016 Ofsted and other inspectorates announced Joint Targeted Area Inspections (JTAI) of arrangements and services for children in need of help and protection in local authority areas in England. These inspections are undertaken by Ofsted, the Care Quality Commission (CQC), Her Majesty’s Inspectorate of Constabulary (HMIC) and Her Majesty’s Inspectorate of Probation (HMI Probation). These inspections are to be themed with the first theme being Child Sexual Exploitation. Safeguarding leads and
EN
C 1
0

Page 21 of 24
named professionals in current health providers have been asked to collate information in preparation for this themed inspection.
The designated nurse for safeguarding children has piloted a safeguarding children dashboard and assurance report presented at the LSCB Quality Assurance Group and to commissioners both in the CCG and public health for scrutiny. The report is due six monthly and will be reviewed at the Safeguarding Assurance Committee and the LSCB Quality Assurance group.
6. Winterbourne View Concordat: Assuring transformation of care for NHS funded patients
The CCG and the Local Authority must be able to assure people with learning disability and those on the Autistic Spectrum Disorder, their families and carers, the wider public and the Department of Health that our commitments in the Winterbourne View Concordat action plan are delivered.
The NHS Commissioning Board’s objective is to ensure that CCGs work with local authorities to ensure that vulnerable people, particularly those with learning disabilities and autism, receive safe, appropriate, high quality care. The presumption should always be that services are local and that people remain in their communities.
We continue to assure the Governing Body that person-centred, community- based services are in place to meet the needs of any local people in this vulnerable group; to limit problems arising, manage any problems that do arise, and prevent future institutional admissions. At the time of writing there are two people with a learning disability from Sutton are currently placed in a hospital registered service which is meeting their specific needs. These placements are being monitored closely via Care & Treatment Reviews, CPA meetings and the Mental Health Act Tribunal alongside care plans and planned discharge dates. There is work underway to discharge one person by the 31st March 2016.
7.0 CCG Quality – internal
7.1 Risk Management
The Quality Risk Register will be brought to the Quality Committee each month, to provide the organisational context plus narrative to support assurance on risks around quality and safety.
The Risk Register enables the Committee to focus on the areas of highest risk and assists the quality team to prioritise its work across all CCG commissioned services. A pro-active approach is taken by the Quality Committee to identify new risks as they arise. It is also anticipated that new risks may be identified through discussion at Quality Committee meetings.
We have recently undertaken a refresh of the Quality Risk Register and have ensured that the Board Assurance Framework is also accurate. 8.0 PALS and Complaints From December the 1st Sutton CCG will be responding to CCG complaints rather than using the service provided by the South Commissioning Support Unit.
EN
C 1
0

Page 22 of 24
Appendix 1: CCG Performance Dashboard
EN
C 1
0

Page 23 of 24
Appendix 2: Sutton CCG Contracted Mental Health Performance (December 2015)
EN
C 1
0

Page 24 of 24
Appendix 3: GP Out of Hours (SELDOC) Performance
EN
C 1
0

Report to the Sutton Clinical Commissioning Group
Governing Body
Date of Meeting: 2nd March 2016
Agenda No: 13 ENCLOSURE: 11
Title of Document: Financial Year 2015/16
Finance report, M10
Purpose of Report:
For Discussion
Report Authors:
Geoff Price, CFO
Lead Director:
Geoff Price, CFO
EN
C 1
1

Page 2 of 3
Executive Summary: Summary
NHS Sutton CCG is forecast to meet all its financial targets for the Year 2015/16.
Report
The CCG reported the M10 position to NHSE on 09 February 16.
Key Financials
The CCG is reporting on plan year to date ( the 10 months ended 31 January 16 ) and full year
forecast. This report uses month 08 prescribing and month 09 acute data as the basis for M10
reporting.
In terms of the full year forecast , overall the CCG is reporting meeting plan for both program and
running costs for year to date and full year forecast. Note that running costs are shown as ‘
underspent ‘ because the quality premium funding is received as a running cost allocation but the
expenditure is charged to program costs.
Salient matters are :
A full year forecast overspend on continuing health care costs of £3.4 million
Overall acute spend is forecast to be in line with contracts. A year end agreement was reached with ESH and SWLEOC in December 15.
A full year forecast overspend on Mental health and Learning Disability services of £700k mainly due to high cost placements.
A full year forecast underspend on prescribing of £275k
Overall QIPP savings targets are being met
All other commissioned services on plan.
The net overspend of £3.8 m is covered by reserves.
Surplus/(Deficit)
£000
Running costs
£000
Plan YTD 1830 3654
Actual YTD 1830 3387
Full year plan 2340 4385
Full year forecast 2340 4063
EN
C 1
1
Page 3 of 3
The summary income and expenditure account is shown in appendix A.
Sutton CCG reviews and monitors its financial position on an ongoing basis by reviewing a range of
outcomes dependent on underlying assumptions and forecasts. The CCG is focusing on maintaining
and improving performance, in particular RTT ( waiting times ) for patients. The Governing Body will
be aware that the CCG has invested to support the RTT target and will be taking other measures that
facilitate risk reduction in 201617.
The CCG balance sheet position is satisfactory in terms of levels of debtors, creditors and cash with all
KPIs being met. The better payment practice code re payment of suppliers is being met.
Recommendation(s): The Governing Body is asked to:
NOTE the report.
Financial Implications:
The CCG is meeting its financial plan year to date and is forecast to do so for the full year.
Other Implications:
None
EN
C 1
1
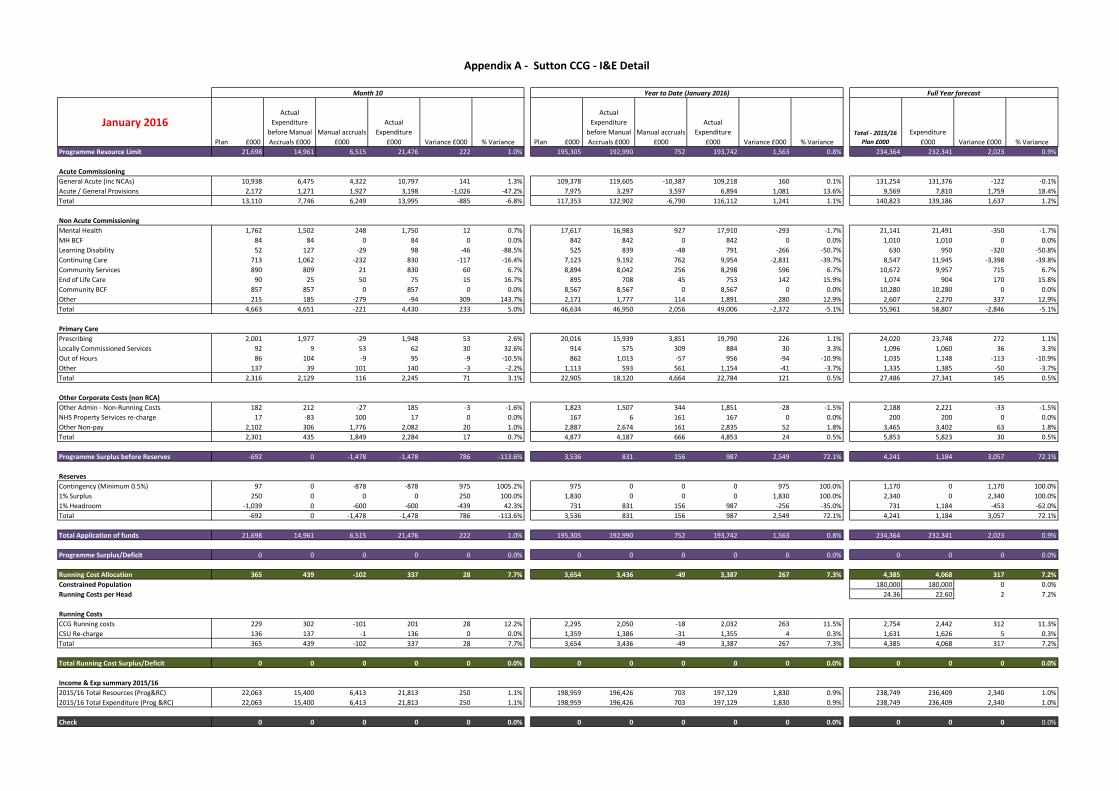
January 2016
Plan £000
Actual
Expenditure
before Manual
Accruals £000
Manual accruals
£000
Actual
Expenditure
£000 Variance £000 % Variance Plan £000
Actual
Expenditure
before Manual
Accruals £000
Manual accruals
£000
Actual
Expenditure
£000 Variance £000 % VarianceTotal - 2015/16
Plan £000
Expenditure
£000 Variance £000 % Variance
Programme Resource Limit 21,698 14,961 6,515 21,476 222 1.0% 195,305 192,990 752 193,742 1,563 0.8% 234,364 232,341 2,023 0.9%
Acute Commissioning
General Acute (inc NCAs) 10,938 6,475 4,322 10,797 141 1.3% 109,378 119,605 -10,387 109,218 160 0.1% 131,254 131,376 -122 -0.1%
Acute / General Provisions 2,172 1,271 1,927 3,198 -1,026 -47.2% 7,975 3,297 3,597 6,894 1,081 13.6% 9,569 7,810 1,759 18.4%
Total 13,110 7,746 6,249 13,995 -885 -6.8% 117,353 122,902 -6,790 116,112 1,241 1.1% 140,823 139,186 1,637 1.2%
Non Acute Commissioning
Mental Health 1,762 1,502 248 1,750 12 0.7% 17,617 16,983 927 17,910 -293 -1.7% 21,141 21,491 -350 -1.7%
MH BCF 84 84 0 84 0 0.0% 842 842 0 842 0 0.0% 1,010 1,010 0 0.0%
Learning Disability 52 127 -29 98 -46 -88.5% 525 839 -48 791 -266 -50.7% 630 950 -320 -50.8%
Continuing Care 713 1,062 -232 830 -117 -16.4% 7,123 9,192 762 9,954 -2,831 -39.7% 8,547 11,945 -3,398 -39.8%
Community Services 890 809 21 830 60 6.7% 8,894 8,042 256 8,298 596 6.7% 10,672 9,957 715 6.7%
End of Life Care 90 25 50 75 15 16.7% 895 708 45 753 142 15.9% 1,074 904 170 15.8%
Community BCF 857 857 0 857 0 0.0% 8,567 8,567 0 8,567 0 0.0% 10,280 10,280 0 0.0%
Other 215 185 -279 -94 309 143.7% 2,171 1,777 114 1,891 280 12.9% 2,607 2,270 337 12.9%
Total 4,663 4,651 -221 4,430 233 5.0% 46,634 46,950 2,056 49,006 -2,372 -5.1% 55,961 58,807 -2,846 -5.1%
Primary Care
Prescribing 2,001 1,977 -29 1,948 53 2.6% 20,016 15,939 3,851 19,790 226 1.1% 24,020 23,748 272 1.1%
Locally Commissioned Services 92 9 53 62 30 32.6% 914 575 309 884 30 3.3% 1,096 1,060 36 3.3%
Out of Hours 86 104 -9 95 -9 -10.5% 862 1,013 -57 956 -94 -10.9% 1,035 1,148 -113 -10.9%
Other 137 39 101 140 -3 -2.2% 1,113 593 561 1,154 -41 -3.7% 1,335 1,385 -50 -3.7%
Total 2,316 2,129 116 2,245 71 3.1% 22,905 18,120 4,664 22,784 121 0.5% 27,486 27,341 145 0.5%
Other Corporate Costs (non RCA)
Other Admin - Non-Running Costs 182 212 -27 185 -3 -1.6% 1,823 1,507 344 1,851 -28 -1.5% 2,188 2,221 -33 -1.5%
NHS Property Services re-charge 17 -83 100 17 0 0.0% 167 6 161 167 0 0.0% 200 200 0 0.0%
Other Non-pay 2,102 306 1,776 2,082 20 1.0% 2,887 2,674 161 2,835 52 1.8% 3,465 3,402 63 1.8%
Total 2,301 435 1,849 2,284 17 0.7% 4,877 4,187 666 4,853 24 0.5% 5,853 5,823 30 0.5%
Programme Surplus before Reserves -692 0 -1,478 -1,478 786 -113.6% 3,536 831 156 987 2,549 72.1% 4,241 1,184 3,057 72.1%
Reserves
Contingency (Minimum 0.5%) 97 0 -878 -878 975 1005.2% 975 0 0 0 975 100.0% 1,170 0 1,170 100.0%
1% Surplus 250 0 0 0 250 100.0% 1,830 0 0 0 1,830 100.0% 2,340 0 2,340 100.0%
1% Headroom -1,039 0 -600 -600 -439 42.3% 731 831 156 987 -256 -35.0% 731 1,184 -453 -62.0%
Total -692 0 -1,478 -1,478 786 -113.6% 3,536 831 156 987 2,549 72.1% 4,241 1,184 3,057 72.1%
Total Application of funds 21,698 14,961 6,515 21,476 222 1.0% 195,305 192,990 752 193,742 1,563 0.8% 234,364 232,341 2,023 0.9%
Programme Surplus/Deficit 0 0 0 0 0 0.0% 0 0 0 0 0 0.0% 0 0 0 0.0%
Running Cost Allocation 365 439 -102 337 28 7.7% 3,654 3,436 -49 3,387 267 7.3% 4,385 4,068 317 7.2%
Constrained Population 180,000 180,000 0 0.0%
Running Costs per Head 24.36 22.60 2 7.2%
Running Costs
CCG Running costs 229 302 -101 201 28 12.2% 2,295 2,050 -18 2,032 263 11.5% 2,754 2,442 312 11.3%
CSU Re-charge 136 137 -1 136 0 0.0% 1,359 1,386 -31 1,355 4 0.3% 1,631 1,626 5 0.3%
Total 365 439 -102 337 28 7.7% 3,654 3,436 -49 3,387 267 7.3% 4,385 4,068 317 7.2%
Total Running Cost Surplus/Deficit 0 0 0 0 0 0.0% 0 0 0 0 0 0.0% 0 0 0 0.0%
Income & Exp summary 2015/16
2015/16 Total Resources (Prog&RC) 22,063 15,400 6,413 21,813 250 1.1% 198,959 196,426 703 197,129 1,830 0.9% 238,749 236,409 2,340 1.0%
2015/16 Total Expenditure (Prog &RC) 22,063 15,400 6,413 21,813 250 1.1% 198,959 196,426 703 197,129 1,830 0.9% 238,749 236,409 2,340 1.0%
Check 0 0 0 0 0 0.0% 0 0 0 0 0 0.0% 0 0 0 0.0%
Appendix A - Sutton CCG - I&E Detail
Full Year forecastMonth 10 Year to Date (January 2016)

Report to the Sutton Clinical Commissioning Group
Governing Body
Date of Meeting: 2nd March 2016
Agenda No: 14 ENCLOSURE: 12
Title of Document:
QIPP M9 2015/16 Board Report
Purpose of Report:
For Discussion
Report Authors:
Alastair Hughes
Lead Director:
Alastair Hughes
Executive Summary: The Sutton CCG Governing Body is requested to note the contents of the report and flag any items for discussion by exception. The current (M9) forecast outturn is 99.9% of the net target. This represents no change in the year end position as forecast at M8. Our year-to-date achievement is slightly ahead of plan (101%) at M9. Although many schemes are performing on plan (BCF and LTC schemes) or above plan (medicines management), the majority of urgent and planned care schemes remain behind plan and at risk - and we have risk-assessed and adjusted forecast final outturn savings for these schemes accordingly. Although there is potential opportunity in the BCF workstream we are not assuming this will be realised at this stage due to the potential impact of winter.
Key sections for particular note (paragraph/page), areas of concern etc: Please refer in particular to sections 4.2 (Urgent Care) and 4.3 (Planned Care).
Recommendation(s):
The Sutton CCG Governing Body is requested to note the contents of the report and
flag any aspects for review and discussion by exception.
Committees which have previously discussed/agreed the report:
Sutton CCG Executive Committee on 24 February 2016. The Clinical Strategy Group
meets monthly and reviews QIPP delivery performance bi-monthly (next scheduled
for 30 March).
Financial Implications:
None
Other Implications:
None
EN
C 1
2

Page 2 of 2
Equality Impact Assessment:
NA
Information Privacy Issues:
Commercial in confidence.
Communication Plan:
NA
EN
C 1
2

1
QIPP REPORT FOR MONTH 9 (December) – 2015/16
1. Recommendations The Sutton Governing Body is requested to note the contents of the report and flag any items for discussion by exception. The current (M9) forecast outturn is 99.9% of the net target. This represents no change in the year end position as forecast at M8. Our year-to-date achievement is slightly ahead of plan (101%) at M9. Although many schemes are performing on plan (BCF and LTC schemes) or above plan (medicines management), the majority of urgent and planned care schemes remain behind plan and at risk - and we have risk-assessed and adjusted forecast final outturn savings for these schemes accordingly. Although there is potential opportunity in the BCF workstream we are not assuming this will be realised at this stage due to the potential impact of winter. 2. Introduction & background
The CCG has a gross QIPP target of £5.0M and net target (after costs) of £4.24M for 2015/16. Schemes to the value of £6.04M were identified by April 2015. These schemes are then risk rated on a monthly basis to ensure projected savings targets are achievable. The current (M9) forecast outturn is £4.55M (gross) and £4.235M (net) which is 99.9% of the £4.238M net target at year end. Net figures are reported to NHS England, and will therefore be reported here in order to ensure consistency. Please note - this is slightly higher than the original QIPP target set for the year due to the introduction of new schemes and several schemes which are delivering beyond expected targets for the year. This also mitigates several schemes which are behind plan and at risk.
3. Summary
The charts below shows the breakdown of the 2015/16 QIPP by work stream with the expected
savings to be generated by each work stream area (Fig 1); and the current performance against plan at
M9 (Fig 2).
Fig 1
Fig 2
Urgent Care £115
LTC, EOL £317
Planned Care £470
Medicines Management
£1,152
BCF £1,395
OOH Recharge
£100
Transactional £689
0
0 0
QIPP Planned Net Savings Target by Workstream 2015/6 (£000)
£-
£500
£1,000
£1,500
£2,000
£2,500
£3,000
£3,500
£4,000
QIPP Performance vs Annual Plan (£000)
Planned Savings
YTD Target
Actual
savings

2
4. Overview of key QIPP areas achievement year to date
The sections below detail YTD achievement by project for each work stream.
4.1. Long Term Conditions, including BCF. YTD achievement £1,217k vs £1,202k plan. Annual
plan £1,712k
The long term conditions work stream includes:
1. Better Care Fund (BCF) reduction in non-elective admissions. Annual plan £1,395
2. Respiratory Pathway redesign. Annual plan £207k (starting July)
3. End of Life – care homes schemes. Annual plan £80k
4. COPD health coaching programme. Annual plan £30k
BCF: on plan. YTD achievement of £975k to plan
The BCF work on non-elective admissions utilises SUS data to determine the impact of the BCF
schemes on admission rates. Whilst delivery of the cost saving associated with the BCF target
of a 3.5% reduction in acute non-elective admissions is currently above target (despite a year-
on-year increase in month 8 activity) - we are mitigating the risk of potential overspends
during the winter months by reporting this trajectory currently as ‘on plan’ with YTD delivery
of £975k savings.
Respiratory: above plan. YTD achievement of £171k vs £144k plan
Implementation of priority pathway developments are underway. These include:
Pilot set up with St Helier and community services working together to improve discharge
of appropriate patients from acute to community services
Primary care training set up for up to 20 clinicians to access the Diploma programme in
Asthma (Education for Health) in April and August 2016
Further training sessions planned by our St Helier Consultant
Next pathway development workshop planned with the Respiratory Clinical Reference
Group later in February
End of Life: on plan. YTD achievement of £59k to plan
This includes End of Life Care Nurses and a LAS scheme to reduce call outs, conveyances and
admissions to St Helier as part of the Vanguard work in Sutton.
COPD health coaching: behind plan. YTD achievement of £12k vs £21k plan. No change in
previously reduced forecast final outturn to £12k
This scheme finished in July 2015. Key learning covers the consenting process, targeting of
appropriate patients and review of secondary care and primary care data for completeness.

3
4.2. Urgent Care – Rapid Access Doctor: behind plan and at risk. YTD achievement of £30k vs
£70k plan. Annual plan £115k (starting October). No change in previously reduced forecast
FOT (Final Out Turn) to £50k.
In summary, activity is increasing and conveyance rates are still low. However, the pilot is still not making the planned savings (note costs shared across SWL as part of the collaborative roll-out) so there is some improvement but not enough. Amongst a number of further mitigating actions is a plan to better match capacity to demand by reducing the number of cars to 2 and change operating hours from 15/2/16.
Rapid Access Doctor – mobile GP taking green ambulance calls directly from LAS. The wider-scale roll-out (part of the SWL out of hospital initiative) includes different planning assumptions from our 14/15 pilot. The 2014/15 pilot ran from 3pm-3am on Fridays, Saturdays and Sundays as well as Bank Holidays during the height of winter pressures – early December to mid-February. In contrast the wider 2015/16 pilot is running from 1pm-1am Monday-Sundays. Referrals to the service have been low in the first weeks of operation: 27% of anticipated levels. There have been very few referrals to the service from the LAS Clinical Hub. Notwithstanding operational challenges of providing this service at scale, there is a possible lack of incentive for LAS to support the initiative as it results in a reduction in activity and associated income. The figures are below: Planning assumptions for the pilot were 7 referrals per car per shift to achieve savings. Therefore, with the go live
dates of the cars the following activity would be expected:
Planned activity by car October November December January Total
Sutton & Merton car (go live 19/10/15)
91 210 217 217 735
Wandsworth car (go live 2/11/15) 0 203 217 217 637
Kingston & Richmond car (go live 16/10/15)
0 105 217 217 539
Total 91 518 651 651 1911
Referrals to the service have increased but still remain at 39% of planned levels (January activity).
Actual activity by car October November December January Total
Sutton & Merton car (go live 19/10/15)
23 67 93 116 299
Wandsworth car (go live 2/11/15) 0 48 66 55 169
Kingston & Richmond car (go live 16/10/15)
0 22 51 69 142
Total 23 137 210 255 610
There have been very few referrals to the service from the LAS Clinical Hub. A summary of referrals by source and
CCG for October - January is as follows:
Activity by CCG Total Referral from LAS Clinical Hub
Referral from LAS Ambulance Crew
Sutton & Merton car 299 17 282
Wandsworth car 169 6 163
Kingston & Richmond car 142 12 130
Total 610 35 (5.7%) 575 (94.3%)
Conveyances to hospital following a visit by the Rapid Access Doctor have been lower than expected at 9%
compared to the predicted levels of 25%. Only 10 Sutton CCG patients have been conveyed to hospital, a

4
conveyance rate of 3%. This is a marked improvement on the 2014/15 pilot in which 23% of patients seen by the
Rapid Access Doctor were then referred onto A&E.
Conveyances to Hospital by Car October November December January Total
Sutton & Merton car (go live 19/10/15)
1 3 8 6 18
Wandsworth car (go live 2/11/15) 0 4 8 5 17
Kingston & Richmond car (go live 16/10/15)
0 1 6 13 20
Total 1 8 22 24 55 (9%)
Further mitigating actions to increase referrals to the Rapid Access Doctor and also better match capacity with demand are as follows:
Expand to green LAS dispositions via 111 (re-triaged patients). Referrals are now
being accepted from NHS 111.
Geographic working by LAS clinician in the clinical hub so there is now a team for
South West London. Discussions are taking place to pilot a dedicated clinician to
review SWL calls and refer onto the Rapid Access Doctor.
Reduction in number of cars from 3 to 2 with effect from Monday 15 February and
change in operating hours from 1pm-1am to 11am-11pm.
Savings to date (M9, December) for Sutton CCG are £29,519 (please note that savings have not been recalculated to take into consideration the lower than predicted conveyance rates). Costs-to-date are now shared via the wider SWL roll-out and our contribution to-date is £64,192.
4.3. Planned Care. YTD achievement of £97k vs £320k plan. Annual Plan £470k
The planned care workstream includes:
1. Walk in, Walk out Hernia service. Annual plan £110k
2. Kinesis consultant advice. Annual plan £100k
3. Direct Access diagnostics. Annual plan £200k (starting September)
4. Gynaecology pathway ‘one stop clinic’. Annual plan £60k (starting July)
5. ‘GP Access’ triage scheme. Annual plan £0k, £40k opportunity (starting September)
Walk in, Walk out Hernia service: behind plan and at risk. YTD achievement of £19k vs £68k
plan. No change in previously reduced forecast FOT to £30k based on continuance of
current lower levels of referrals (and associated savings) than planned.
A review meeting occurred 13 January with the provider to discuss promoting the hernia
service to localities to increase numbers. Referral form to be revised; referrals will be received
into the service via NHS net. Presenting to Localities in March.
Kinesis consultant advice: slightly behind plan. YTD achievement of £65k vs £70k plan. No
change to forecast FOT of £100k.
From April to November there were 299 saved acute referrals. This represents continued
usage of the system. There is a drive to improve uptake by promoting Kinesis to Localities in
the New Year with a next Steering Group to review development in March. Presentation to
Joint Localities 23rd Feb.

5
Direct access diagnostics: behind plan and at risk. £0k vs £140k plan. No change in
previously reduced forecast FOT to £50k.
The Trust went live on 4 January with MRI Brain and CT Pancreas in line with NICE guidance for
suspected cancer and communications sent to GPs highlighting the relevant clinical
information required when making a request/referral via the Dart System. We held a meeting
with the Trust on 2nd February: baseline work has been completed following demand &
capacity workshops (to be submitted to the CCG at the end of February) to help with planning;
a steering group is looking at ways to maximise usage of Kinesis to expedite referrals (e.g.
“further imaging needed” which often comes up on radiology reports for lung).
Gynaecology pathway ‘one stop clinic’: behind plan. YTD achievement of £10k vs £42k plan.
No change in previously reduced forecast FOT to £40k.
The new one stop clinic for gynaecology went live on 29th July at the Jubilee Health Centre. It
is a consultant-led (EStH outreach) clinic with clinics running alternate weeks (9 slots: 5 new
and 4 follow-up capacity). Clinics are now set to run weekly from 1st February. The Service is
getting busier and booking into mid April. Appetite to look at delivering Urogynae service.
‘GP Access’ triage scheme: YTD achievement of £3k vs £0k plan and at risk.
Four initial practice meetings for this pilot resulted in no initial take-up (all large practices with
list sizes between 8500 and 13500). We are working with the Clinical Lead to stimulate uptake
and Carshalton Fields signed up in early October.
4.4. Medicines Management. YTD achievement of £1,053k vs £864k plan. Annual Plan £1,152k
The medicines management work stream includes:
1. Practice workstreams. Annual plan £200k
2. Budgetary adjustments. Annual plan £782k
3. Domiciliary pharmacist for Medicines Use Reviews. Annual plan £55k (starting August)
4. Dietician for Oral Nutritional Supplement reviews. Annual plan £60k
5. Care Homes pharmacist. Annual plan £55k (starting August)
6. Script Switch. Annual plan £0k
Practice workstreams: above plan. YTD achievement of £224k vs £149k plan. No change to
previously increased forecast FOT of £230k
Please note that 0.9 wte pharmacist has been lost from the team due to a one year
secondment to care homes pharmacist role from August 2015. 0.4wte capacity has been
backfilled but 0.5 wte remains vacant. Although this represents a risk to delivery of the
revised plan, conversations are underway to secure remainder of backfill. Note that the CCG
has been given notice of termination of the rivaroxaban rebate, agreed in July, at the end of
December 2015. This will be replaced with a reduction in list price.
Prescribing growth management: on plan. YTD achievement of £590k to plan
Domiciliary pharmacist for Medicines Use Reviews: behind plan. YTD achievement of (£19k)
vs £40k plan. No change in previously reduced forecast FOT of (£25k)
Delays in starting this piece of work have occurred due to recruitment and resolution of data
collection and information governance issues. The first domiciliary review only concluded in

6
January 2016 and we do not expect net savings benefits to be realised until FY 2016. Please
note that underperformance due to delays in implementation of domiciliary visits has been
reflected by increased delivery of savings from practice workstreams.
Dietician for Oral Nutritional Supplement reviews: above plan. YTD achievement of £196k
vs £45k plan. No change in previously increased forecast FOT of £223k
Current focus of this scheme is on obtaining agreement of ‘Cows milk protein allergy
guidelines’ to support appropriate prescribing and reduction of waste in primary care. Note
that the CCG has been given notice of termination of the Nutricia rebate, agreed in 14/15, at
the end of December 2015. This will be replaced with a reduction in list price.
Please note that we have extended and made substantive the post during 15/16 along with
increasing the target.
Care Homes pharmacist: behind plan. YTD achievement of (£21k) vs £40k plan. No change
in previously reduced forecast FOT of (£17k)
Recruitment issues have meant that this pharmacist was not in post until August 2015,
delaying the start of this piece of work. Medications reviews have started in the six
phase1/wave1 nursing homes. Alignment of the workplan with Vanguard priorities may
reduce the quantifiable savings over the year and the forecast has been amended, however
intangible savings are also being recorded. We do not expect net savings benefits to be
realised until FY 2016.
Scriptswitch: above plan. YTD achievement of £83k to £0k plan
Scriptswitch continues to represent value for money. The profile will undergo a full review in
Q4 to ensure that messages are up to date and ensure continued relevance to prescribers to
maximise the savings made from the software.

Report to the Sutton Clinical Commissioning Group
Governing Body
Date of Meeting: 2nd March 2016
Agenda No: 15 ENCLOSURE: 13
Title of Document:
Board Assurance Framework
Purpose of Report:
For Review
Report Authors:
Terri Burns, Corporate Affairs Principal
Associate, SECSU
Lead Director:
Geoff Price, Chief Financial Officer
Executive Summary: No risks have been escalated to or from the Governing Body Assurance Framework this month. Risks have recently been received by all risk holders. Risk 1020 regarding Continuing Health Care has been reduced from significant to high. No other risks have changed.
Key sections for particular note (paragraph/page), areas of concern etc: Escalation of risks from the corporate risk register to the Board Assurance Framework No risks have been added to the BAF this month. De-escalation of risks from the Board Assurance Framework to the corporate risk register No risks have been removed from the BAF to the corporate risk register.
Recommendation(s):
The Governing Body are asked to:
• NOTE the Board Assurance Framework
• REVIEW and make comment ( if any ) on content of BAF
Committees which have previously discussed/agreed the report:
N/A
EN
C 1
3

Page 2 of 2
Financial Implications:
As per risk 531
Other Implications:
N/A
Equality Impact Assessment:
N/A
Information Privacy Issues:
As per Freedom of Information Act 2000.
Communication Plan:
Publish in public Governing Body papers for March 2016.
EN
C 1
3

Governing Body Assurance Framework Summary February 2016
Corporate Objectives Principal risks to achievement of objectives Initial Score
Current Score
Target Risk
Score
Date of last
review
Change since
previous review
C L C L
Objective 1: Ensure patients are at the heart of decision making, working in partnership with individuals, patient representative groups, families and carers to deliver high quality, accessible services that tackle inequalities and respond to personal need.
534 If engagement with CCG practices inadequate, then there is a risk of a disconnection between the GB and the broader membership
4x3=12 4x2=8 4x2=8 Feb 2016
913 If the CCG does not adequately listen or act on the patient and public voice, the CCG will not meet the national guidance on Transforming Participation in Health and Care and will not commission services in line with patients' needs and expectations
4x3=12 3x1=3 2x1=2 Nov 2015
Objective 2: Commission high quality cohesive health services for the population of Sutton through joint working between health and social care organisations ensuring patients’ physical, mental and social wellbeing needs are met.
528 If quality measurements do not provide sufficient assurance of good quality care as a result of transitional reporting processes there is a risk the CCG may unaware of poor quality care within providers as highlighted by the Francis Report
5x3=15 3x2=6 3x2=6 Nov 2015
530 If the CCG fails to commission adequate commissioning support due to the maturity of the commissioning support market then there may be a risk that the CCG does not fulfil all of its statutory commissioning functions
4x3=12 4x4=16 4x1=4 Feb 2016
664 If the CCG fails to reach agreement on hospital configuration across South London, as a result of the SWL Collaborative Commissioning Strategic Plan being supported, this may mean the CCG is unable to deliver its 5 year strategic plan
5x3=15 5x4=20 4x2=8 Feb 2016
677 If Sutton urgent care services are unable to provide sufficient capacity to meet patient demand, this may result in providers failing to meet key quality and performance commissioning expectations
4x4=16 4x3=12 4x2=8 Nov 2015
805 If providers do not meet national and local quality and performance standards, then the CCG population does not have constitutional pledges honoured by providers e.g. Cancer Targets, RTT, HCAIs
5x4=20 4x4=16 4x2=8 Feb 2016
912 If the CCG does not realise the financial benefits of the BCF programme, then savings will not be available for investment elsewhere in the heath economy and the CCG may not be able to deliver its 5 year strategy in full
4x4=16 3x3=9 3x2=6 Nov 2015
1019 Implications of Primary Care Commissioning as a new area of responsibility with capacity, capability, resources and conflict of interest issues
4x4=16 4x4=16 2x4=8 Feb 2016
1020 Continuing Health Care service brought back in house from SECSU - significant legacy issues and financial challenges
4x4=16 4x3=12 3x3=9 Feb 2016
Objective 3: Maintain an efficient and financially stable, local healthcare system by improving primary care and community services and working closely with secondary care to deliver integrated services that bring healthcare into the community.
529 If the CCG's QIPP programmes do not achieve all planned objectives due to the demand for services and complexity of healthcare reconfiguration then there is a risk that the CCG may not be able to realise its cost savings and financial balance
5x4=20 4x2=8 4x2=8 Dec 2015
531 If costs for commissioned services exceed the resources available then there may be a risk of non-delivery of financial targets of 1% surplus
5x4=20 4x2=8 4x2=8 Feb 2016
Objective 4: Work with the local authority to develop an integrated commissioning framework that supports single, pooled budget for health and social care services with planned and agreed delivery across a range of areas.
803 If the CCG does not align 5 year forward view, Better Care Fund programmes and the Out of Hospital Strategy, as a result of conflicting perspectives, the CCG may fail to develop a locally owned and credible Strategic Plan
4x3=12 4x3=12 3x2=6 Feb 2016

Governing Body Assurance Framework Summary February 2016
The top risks currently facing Sutton CCG, by risk score are:
664 If the CCG fails to reach agreement on hospital configuration across South London, as a result of the SWL Collaborative
Commissioning Strategic Plan being supported, this may mean the CCG is unable to finalise its 5 year strategic plan
805 If providers do not meet national and local quality and performance standards, then the CCG population does not have
constitutional pledges honoured by providers e.g. Cancer Targets, RTT, HCAIs
530 If the CCG fails to commission adequate commissioning support due to the maturity of the commissioning support market then
there may be a risk that the CCG does not fulfil all of its statutory commissioning functions
1019 Implications of Primary Care Commissioning as a new area of responsibility with capacity, capability, resources and conflict of
interest issues

Report to the Sutton Clinical Commissioning Group
Governing Body
Date of Meeting: 2nd March 2016
Agenda No: 16 ENCLOSURE: 14
Title of Document: Approved minutes of Committees of the
Sutton CCG Governing Body
Purpose of Report:
For Note
Report Authors:
As per details on each attachment
Lead Director:
As per details on each attachment
Executive Summary: The following minutes are attached for the Governing Body to note:
Executive Committee: 16.12.15, 13.01.16, 27.01.16, 10.02.16
Finance Committee: 18.11.15, 16.12.15
Quality Committee: 19.11.15, 17.12.15
SWL Joint Committee for Primary Care: 12.11.15
Recommendation(s):
The Governing Body are asked to:
NOTE the minutes.
EN
C 1
4

MINUTES OF THE SUTTON CLINICAL COMMISSIONING GROUP
EXECUTIVE COMMITTEE MEETING
Wednesday 16th December 2015, 2.30pm - 3.30pm Meeting Room 1, Priory Crescent
Present
Jonathan Bates JB Chief Operating Officer, Sutton CCG
Dr Chris Elliott CE Chief Clinical Officer / GP - Benhill & Belmont Surgery (Chair)
Dr Simon Elliott SE QIPP Lead-Medicines Management
Sian Hopkinson SH Director of Performance & Primary Care
Dr Senthooran Kathirgama Kanthan
SK Sutton & Cheam Locality Lead
Geoffrey Price GPr Chief Finance Officer, Sutton CCG
Dr Farhan Rabbani FR Wallington Locality Lead
Sue Roostan SR Director of Commissioning and Planning
Dr Roshni Scott RS QIPP Lead-Medicines Management
Karol Selvey KS QIPP Lead / Nurse Practitioner & Partner - Dr Grice & Partners
Dr Mark Wells MW QIPP Lead-Acute Contracts / GP - Wrythe Green Surgery
In Attendance
Louise Naidu LN Locality Manager, Sutton CCG
Jane Walker JW Head of Corporate Governance, Sutton CCG
Apologies
Dr Chris Keers CK QIPP Lead-Mental Health / GP - Wrythe Green Surgery
Dr Dino Pardhanani DP QIPP Lead-LCCs & Service Redesign / GP - Mulgrave Road Surgery
Dr Ash Mirza AM Carshalton Locality Lead / GP - Faccini House Surgery
ACTION
Welcome & Introduction
1. Welcome and Apologies CE welcomed members to the meeting and apologies of absence are noted above.
2. Declarations of Interest The Register of Interest was agreed as a correct and accurate record.
3. To approve the minutes of the Executive Committee meeting held on 9 December 2015 The minutes of the meeting held on 9 December 2015 were approved as accurate records.
4. Matters arising not on the agenda & review of action log from previous meeting The action log was updated and would be submitted to the next meeting of the Executive Committee.
EN
C 1
4a 1
6.12
.15
Page 2 of 7
IAPT Performance
SR reported that as at the 16 December 2016, performance in
relation to the Access target had improved and was now on track to
meet the National Target. There were still however issues in relation
to communications from the Trust and sustaining performance.
Performance in relation to the Recovery target was still poor.
Adrian Davey was in the process of arranging a meeting with
managers from the service to understand what more was required to
improve performance especially around the issue of marketing.
RTT
JB reported that the CCG were still awaiting further information from
ESHT prior to presenting a further paper on delivering referral to
treatment times to the Executive Committee.
JB agreed to chase the Trust for the information and bring back a
report to the Executive Committee early in the New Year.
AD
JB
Items for Decision
5. Sutton CCG Estates Strategy
GP introduced the final draft Estates Strategy which was required to
be submitted to NHSE by the end of December 2015.
GP confirmed that an earlier draft had been submitted to the
Executive Committee on the 25th November and to the Board
Seminar on 2nd December 2015. Comments received following both
these meetings had now been incorporated into the draft together
with the primary care sections being expanded and updated.
GP highlighted the fact that bids for capital development 2016/17
would now be to the Primary Care Transformation Fund. NHSE had
written to CCGs, included at Appendix 2.1 of the draft strategy,
Primary Care Transformation Fund - Approach to Funding 2016 to
2019 setting out the proposals for primary care estates development
which would require CCG sign off and financial support. It was need
that the CCG did not take delegation until April 2016 and would need
time to digest primary care premises proposals.
It was noted that the development of an integrated NHS Estates
Strategy for South West London was expected to be completed
during 2016.
GP requested any further comments to be made direct to himself
prior to submission at the end of December 2015.
ALL
EN
C 1
4a 1
6.12
.15

Page 3 of 7
The Executive Committee APPROVED the draft estates strategy
for submission to NHSE.
Items for Discussion
6. 2016/17 GP Practice Engagement Scheme
FR presented a discussion paper on the GP practice engagement
scheme supporting clinical commissioning for 2016/17.
Following on from the success of the 2015/16 GP engagement
scheme, the planning for the 2016/17 scheme was well underway. A
draft scheme was being proposed which preserves the many positive
aspects of the previous scheme whilst expanding it to include
additional, yet achievable, measurable, quality and cost effective
outcomes as detailed within the paper.
Funding would be made available to each practice to support
engagement in clinical commissioning through Localities and on
delivery of outcomes.
FR stated that to ensure engagement with the proposed scheme for
2016/17 the localities team have actively pursued feedback about
the current scheme via a number of meetings and events including
the Sutton CCG away day and locality meetings. Colleagues from
Sutton CCG had been involved in discussions to ensure that Sutton
CCG’s organisational objectives and priorities were incorporated into
any proposal moving forward.
FR highlighted the requirements of the proposed scheme which was
detailed within the paper and included the criteria for both:
- Engagement with locality meetings, practice manager and
practice nurse forums etc.
- Practice based engagement - outcomes
It was noted that further detail was to be provided for the Prescribing
practice based engagement outcome working with community
pharmacists to deliver Medicines use reviews.
Executive Committee members felt it was important to include areas
within the constitutional standards to the outcomes e.g. Dementia
and IAPT Access and include a compulsory component for those
practices currently not achieving targets.
GP stated there would be a need to look at cost pressures before
funding of the scheme could be agreed.
LN stated that there would be a need to review the proposal if funded
ST
EN
C 1
4a 1
6.12
.15
Page 4 of 7
was not increased from 2015/16 as the requirements had increased.
LN agreed to circulate the success rates for this year across
localities to Executive Committee members.
The Executive Committee DISCUSSED the content of the Sutton
GP engagement scheme 2016/17 to enable financial modelling
and reporting requirements to be developed.
LN
7. Commissioning Intentions 2016/17 - Plan on a Page SR presented the draft plan on a page to support the operating arrangement for 2016/17. The content of the plan is derived from discussions with clinicians, patient reference groups, lead managers and the CCG away day held in October 2015. SR confirmed that the plan includes three additional areas:
- Children’s services - Primary Care commissioning - Sutton Homes of care
SR confirmed that the plan would be reviewed and amended following the release of planning guidance and once the CCG receives its financial allocation. The plan had been simplified from previous years and did not currently reflect the CCG’s vision as this was currently being refreshed to reflect the ambition of the CCG and would be added once shared and signed off. The Executive Committee noted the draft Plan on a Page and that it was subject to change once planning guidance was issued.
8. Performance Report SH presented the month 6 report to inform and provide assurance to the Executive Committee about the performance, quality and safety of service provision commissioned by NHS Sutton CCG. SH highlighted the following key areas:
- Performance against referral to treatment time (RTT) target achieved at aggregate level for every month of 2015/2016, achieving 92.6% at month 6, against a target of 92%
- Cancer waiting times and continued pressure on 62 day wait standards and progress against action plan at Epsom and St Helier Trust and meeting the 85% target in October
- London Ambulance Service failure to meet response time standards at London level, however improving performance in Sutton
EN
C 1
4a 1
6.12
.15

Page 5 of 7
- GP Out of Hours service continues to achieve all performance standards
It was noted that the Quality report would be discussed and reviewed at the Quality Committee scheduled for 17th December 2015. The Executive Committee NOTED and REVIEWED the Performance Report.
Standard Items
9. Finance Report - Month 8 GP presented the finance report at month 8. The CCG was reporting on plan year to date (the 8 months ended 30 N0vember 15) and full year forecast. The report uses month 06 prescribing and month 7 acute data as the basis for month 8 reporting. GP stated that overall the CCG was reporting meeting plan for both program and running costs, however there was:
- A full year forecast overspend on continuing health care costs of £3.1m, an increase on the M07 position of £2.8 m overspend. This is a very significant overspend and a result of continuing work on CHC since the transfer of the service from the SECSU. Action is being taken to ensure complete and accurate reporting; completing clinical reviews and managing the services for this cohort of patients better.
- A full year forecast underspend on acute contracts of £200k. This is an adverse movement of £900k from M07 due largely to a change in the ESH and SWLEOC forecast given a significant increase in activity in M07 and discussions with the Trust on likely future activity levels. The CCG is keen to see RTT performance improve and is supportive of this activity trajectory. Overall an acute overspend of £200K is just 0.2% from contract value.
- A full year forecast overspend on Mental health and Learning Disability services of £700k mainly due to high cost placements ( M07; £700k ).
- A full year forecast underspend on prescribing of £300k (M07; £350k).
- Overall QIPP savings targets are being met.
All other commissioned services were on plan with the net overspend of £3.3m being covered by reserves. The Executive Committee NOTED the report.
10. Board Assurance Framework GP presented the BAF and asking Executive Committee members to note the ratings for both risks 530 and 805, as detailed within the
EN
C 1
4a 1
6.12
.15

Page 6 of 7
report, have been increased, from high to very high, to reflect recent developments in relation to SECSU and performance against constitutional pledges respectively. The report also includes newly developed risks proposed for addition to the Governing Body Assurance Framework. These relate to Primary Care Commissioning and Continuing Health Care. The Executive Committee NOTED and REVIEWED the BAF.
11. QIPP Report – Month 7 The Executive Committee received the QIPP report at month 7. The current month 7 forecast outturn was 100.4% of the net target at year end. This was a slight reduction in the position at month 6, 104%. Although many schemes were performing on plan or above plan, the majority of urgent or planned care schemes were behind and at risk. These had been assessed and the forecast final outturn savings adjusted for these schemes. It was noted that the Clinical Strategy Group met monthly to review QIPP performance on a bi-monthly basis. The Executive Committee NOTED the report.
For Information
12. IT Procurement Update The Executive Committee received a report, for information only, on the SWL IT Collaborative Working Group membership, the IT Lead Provider Framework Procurement timeline and the proposed membership of the Sutton CCG IT Project Board. The Executive Committee NOTED the report and the formation of a Sutton CCG IT Programme Board.
13. Continuing Health Care Update As previously agreed, the Executive Committee received a regular update on the continuing health care service and provides details of progress and risks since the service was returned from the CSU. It was noted that a further update would be presented to the Governing Body meeting on 6th January 2015. The Executive Committee NOTED the report.
14. Business Cases – Two Additional 15/16 Investments Following the refresh of the investment plan in October 2015, the Management Team considered that a small amount of Non-Recurrent funding could be allocated for further investment in 2015/16.
EN
C 1
4a 1
6.12
.15

Page 7 of 7
A number of business cases were received and two had been approved for investment this year by the Management Team and attached for information by the Executive Committee:
1. Social Prescribing (£39k non-recurrent) 2. Childrens Domestic Violence Advocacy and Support (£35k
non-recurrent) The Executive Committee NOTED the two business cases.
Any Other Business
11. Any Other Business CE thanked Dr Simon Elliott for all his work, both as the Medicines Management Lead and his contribution to the Executive Committee following his decision to step-down from this role as of the end of December 2015.
12. Date of Next Meeting Wednesday 13th January 2016, 1.00pm-3.00pm, Meeting Room 1, Priory Crescent
EN
C 1
4a 1
6.12
.15

MINUTES OF THE SUTTON CLINICAL COMMISSIONING GROUP
EXECUTIVE COMMITTEE MEETING
Wednesday 13th January 2016, 1.00pm - 3.00pm Meeting Room 1, Priory Crescent
Present
Jonathan Bates JB Chief Operating Officer, Sutton CCG
Dr Chris Elliott CE Chief Clinical Officer / GP - Benhill & Belmont Surgery (Chair)
Dr Senthooran Kathirgama Kanthan
SK Sutton & Cheam Locality Lead
Dr Chris Keers CK QIPP Lead-Mental Health / GP - Wrythe Green Surgery
Dr Ash Mirza AM Carshalton Locality Lead / GP - Faccini House Surgery
Dr Dino Pardhanani DP QIPP Lead-LCCs & Service Redesign / GP - Mulgrave Road Surgery
Geoffrey Price GPr Chief Finance Officer, Sutton CCG
Dr Roshni Scott RS QIPP Lead-Medicines Management
Karol Selvey KS QIPP Lead / Nurse Practitioner & Partner - Dr Grice & Partners
Dr Mark Wells MW QIPP Lead-Acute Contracts / GP - Wrythe Green Surgery
In Attendance
Rob Grove RG South London CSU
Brendan Hudson BH Chair, Sutton CCG
Frankie Lynch FL South London CSU
Sarah Taylor ST Head of Medicines Optimisation
Koruthu Varghese KV Project Manager, Sutton CCG (Item 5)
Jane Walker JW Head of Corporate Governance, Sutton CCG
Apologies
Sian Hopkinson SH Director of Performance & Primary Care
Dr Farhan Rabbani FR Wallington Locality Lead
Sue Roostan SR Director of Commissioning and Planning
ACTION
Welcome & Introduction
1. Welcome and Apologies CE welcomed members to the meeting and apologies of absence are noted above.
2. Declarations of Interest The Register of Interest was agreed as a correct and accurate record.
3. To approve the minutes of the Executive Committee meeting held on 16 December 2015 The minutes of the meeting held on 16 December 2015 were approved as accurate records.
EN
C 1
4a 1
3.01
.16

Page 2 of 7
4. Matters arising not on the agenda & review of action log from previous meeting The action log was updated and would be submitted to the next meeting of the Executive Committee. IAPT Performance
Adrian Davey had arranged to meet with Dawn Chamberlain,
Director of Operations at SWL & ST Georges MH NHS Trust to
discuss the service to understand what more was required to
improve performance.
RTT
JB stated that at the SCCG Governing Body meeting held on 6
January 2016, it was agreed to explore the possibility of improving
18 week referral to treatment times at Epsom and St Helier Trust
(ESTH). It was also agreed in principle that this would be funded up
to a maximum of £1M.
Subsequently in order for ESTH to improve performance additional
activity with the independent sector would be commissioned at both
Ashtead & St Anthony’s Hospitals at an approximate value of £850K.
JB stated that this will improve the SCCGs resilience for meeting the
RTT constitutional standard.
Items for Decision
5. CCG IT Service Specification
Koruthu Varghese attended the meeting and presented a paper on
the Service Specification and key performance indicators for CCG
Corporate ICT Services.
KV stated Sutton CCG were preparing for the collaborative
procurement of ICT services with Wandsworth and Merton, aiming to
start the process in January 2016 for a contract being awarded in
April and a go-live date of August 2016. Since writing the paper,
Richmond had decided not to be included as part of the
collaboration.
KV confirmed that only Sutton and Merton CCGs were planning to
procure corporate ICT services from the same provider and in the
same procurement lot as GP ICT services.
The Executive Committee reviewed the Service Specification
and Key Performance Indicators and AGREED that any further
amendments would be approved by the Chief Operating Officer
and Director of Performance and Primary Care.
EN
C 1
4a 1
3.01
.16
Page 3 of 7
Items for Discussion
6. High Performing Team Survey
Frankie Lynch and Rob Groves from SLCSU attended the meeting
and carried out a High-Performing Leadership Team Survey with the
Executive Committee members as part of the Organisational
Development work the CCG had commissioned the SLCSU to
undertake.
FL informed the Executive Committee that the same survey had
been completed by the Management Team and the results would be
collated and shared in due course.
FL (SCU)
7. 2016/17 Planning Guidance and Allocations
Allocation & 2016/17 Financial Planning
GP informed the Executive Committee that CCGs had been informed
of their allocations for 16/17 and future years late afternoon 11
January.
GP confirmed that Sutton CCG had received 3.05% growth for 16/17
which was significantly less than expected and below the average
for London. The reasons for this are complex but appear to be the
result of changes to the allocation formula, projected population
growth, and the new 'place based' system which appears to
take into account primary care and specialised commissioning
allocations. This area is complex and it will take time to understand
( if one can ). It is very unlikely that allocations will change from these
published.
GP noted that program ( health spending ) allocation growth at
3.05% for 1617 is below the average for England ( 3.85% ) and the
average for London ( 3.95% ).
The primary care allocation growth ( with delegated commissioning )
at 3.4% is also below the London average of 4.8%. This is because
Sutton is deemed to be over ‘target ‘ for primary care funding ( some
7% in 1617 ).
Running costs allocations were roughly flat over the 5 year planning
period.
This had important implications for 16/17 budgeting as the current
financial model indicated a QIPP requirement of £7 million (based on
the current assumptions in the model). In addition this level of QIPP
did not generate a general reserve. GP stated that while the CCG is
currently working on its 5 year financial plan, it is clear some
measures are necessary now. He stated that in his view investments
agreed in 2015/16 that had not been started should be paused for
review amongst a number of other measures ( listed below ). GP
EN
C 1
4a 1
3.01
.16

Page 4 of 7
also said seeking agreement of a block contract with ESTH in
2016/17 would help mitigate risk.
DP raised concern with regards to pausing all investments that had
not been started for review of affordability. Even though he accepted
in principle, DP raised concerns re the work that had already taken
place on a number of schemes and the people currently working on
projects.
GP acknowledged this but felt all investments had to be paused; one
could not be selected at this stage. This would be for around 2
months to allow review and for a number of uncertainties that effect
financial planning being bottomed out.
Following discussion GP set out the following principles and asked
for Executive Committee agreement to them:
As far as possible and permissible, expenditure will be incurred in 2015/16 to support 2016/17.
As normal, budget meeting will be held with budget holders to help refine budgets but with the clear aim of reducing cost where possible. Budgets holders will be required to sign up to final budgets.
All new investment not started will be paused pending review of affordability. This is likely to take around 2 months to end March 2016.
The CCG will seek to maximise QIPP saving opportunities. QIPP savings must be real (risk rated) and credible and included in contracts or budgets as applicable. There can be no ‘unidentified ‘ savings requirement in the final CCG budget.
Primary care premises development (for which CCGs now underwrite revenue consequences) are on hold until affordability can be properly assessed (as well as non -financial matters).
A block contract (a generic term for various forms of block contract) will be sought with the main acute provider to mitigate financial risk in 16/17.
The Executive Committee noted the update and AGREED the principles detailed above. 2016/17 Planning Guidance JB presented the 2016/17 Planning Guidance Delivering the Forward View 2016/17-2020/21 included within the papers together with the first draft SCCG plan on a page. JB highlighted the following key points to note:
Key focus of the guidance was that all systems were required to submit sustainability and transformation plan that are
EN
C 1
4a 1
3.01
.16

Page 5 of 7
system wide i.e. SW London
One year organisational plans would be required although these would need to complement the transformation plans and triangulate across the system
‘Nine must dos’ for delivery in 16/17
The Executive Committee NOTED the first draft plan on a page and discussed the new planning guidance taking account of the potential impact for Sutton CCG.
8. Primary Care Commissioning - Due Diligence Report GP presented the outcome of the financial due diligence in relation to Primary Care Full Delegation. This had been requested by Sutton CCG to help the Governing Body to consider the financial risks associated with the proposed transfer of responsibilities for the management of primary care contracts from NHS England. The review concluded that there was a level of financial risk to the
CCG in taking on Level 3 delegated commissioning responsibility.
The level of risk is related to the budget setting process, QIPP
requirements and the historic approach to accruing for costs at a GP
Practice level. A number of recommendations have been made in
this document to help the CCG mitigate these risks.
In addition, these risks needed to be considered in the context of the
opportunities that Level 3 delegated commissioning may provide,
such as the scope for improved system-wide financial management
is significant and should be weighed up against the likely short-term
financial challenge that the CCG will inherit if they decide to proceed
with Level 3 delegation.
The second component of due diligence, relating to legal matters,
was not yet available.
The GP Plenary will have access to this information prior to its
meeting on 11 February 2016 and it would be shared with Governing
Body Members when it becomes available.
GP confirmed that the Governing Body at the meeting on 6
January 2016, considered the points set out in the paper and agreed to recommend to the Plenary that the CCG continue with its
application but ask NHSE to indemnify the CCG for past rent review
gaps.
JB agreed to discuss with CE and SH what documentation should be
shared with practices and how the CCG can ensure practices are
well informed prior to the Plenary.
The Executive Committee NOTED the report.
JB
EN
C 1
4a 1
3.01
.16
Page 6 of 7
9. Performance Update JB gave a verbal update on performance and tabled a sheet showing the 7 ‘must do’ constitutional standards showing the likely outturn 2015/16 and the current trend in relation to SCCG. JB stressed that it was important to establish whether there was anything more the CCG could do to achieve these targets and asked Executive Committee members to feedback. Members felt that the dementia target was achievable with systematic support and commitment from the practices. A request was made for the analytical support to practices to be reinvigorated, for care homes to review all patients on their caseload and for older people’s psychiatrist caseloads to be cross-checked with practice registers.
SR
Standard Items
10. Feedback from Localities The Localities Leads gave a brief updated and highlighted the following key points:
Practice visits had now been completed
The joint locality workshop had been well received by practices
Wandle Valley practice had now closed, This was causing problems with surrounding practices due to high numbers of patients wanting to register.
11. Finance Report GP gave a verbal finance update at month 9 confirming that the CCG
was reporting on plan year to date and full year forecast.
For Information
12. Approved minutes: The Executive Committee noted the following minutes:
Primary Care Steering Group - 12 Nov, 9 Dec 2015
Planned Care Working Group - 19 Nov 2015
Urgent Care Working Group - 20 Oct, 24 Nov 2015
Management Team Action Notes - Dec 2015
Any Other Business
13. Any Other Business CE informed the Executive Committee that Sutton CCG were asked by the CQC to present to their Inspectors on the work that the CCG have been doing in providing support to the two practices in ‘Special Measures’. The presentation was really well received by the CQC followed by a lively Q&A session.
14. Date of Next Meeting Wednesday 27th January 2016, 2.30pm-3.30pm, Meeting Room 1, Priory Crescent
EN
C 1
4a 1
3.01
.16

Page 7 of 7
EN
C 1
4a 1
3.01
.16

MINUTES OF THE SUTTON CLINICAL COMMISSIONING GROUP
EXECUTIVE COMMITTEE MEETING
Wednesday 27th January 2016, 1.45pm - 3.15pm Meeting Room 1, Priory Crescent
Present
Jonathan Bates JB Chief Operating Officer, Sutton CCG
Dr Chris Elliott CE Chief Clinical Officer / GP - Benhill & Belmont Surgery (Chair)
Dr Senthooran Kathirgama Kanthan
SK Sutton & Cheam Locality Lead
Dr Chris Keers CK QIPP Lead-Mental Health / GP - Wrythe Green Surgery
Dr Ash Mirza AM Carshalton Locality Lead / GP - Faccini House Surgery
Dr Dino Pardhanani DP QIPP Lead-LCCs & Service Redesign / GP - Mulgrave Road Surgery
Geoffrey Price GPr Chief Finance Officer, Sutton CCG
Dr Farhan Rabbani FR Wallington Locality Lead
Sue Roostan SR Director of Commissioning and Planning
Dr Roshni Scott RS QIPP Lead-Medicines Management
Karol Selvey KS QIPP Lead / Nurse Practitioner & Partner - Dr Grice & Partners
Dr Mark Wells MW QIPP Lead-Acute Contracts / GP - Wrythe Green Surgery
In Attendance
Alastair Hughes AH Director of Service Transformation
Sam Green SG Service Redesign Manager
Bernadette Devine BD Business Resilience & Service Redesign Manager
Sarah Taylor ST Head of Medicines Optimisation
Emma Stapleton ES Service Redesign & Business Resilience Manager
Jane Walker JW Head of Corporate Governance, Sutton CCG
Apologies
Sian Hopkinson SH Director of Performance & Primary Care
ACTION
ITEMS FOR DISCUSSION
CSG 1.
Financial Planning Finance Update 2015/16 GP updated the Executive Committee on the financial position at month 9. The CCG was reporting on plan year to date ( the 9 months ended 31
December 15 ) and full year forecast. This report uses month 07
prescribing and month 08 acute data as the basis for M09 reporting.
In terms of the full year forecast, overall the CCG is reporting meeting
plan for both program and running costs for year to date and full year
forecast.
Key items to note included :
EN
C 1
4a 2
7.01
.16

Page 2 of 7
A full year forecast overspend on continuing health care costs of £3.2 million
Overall acute spend is forecast to be in line with contracts. A year end agreement was reached with ESH and SWLEOC in December 15.
A full year forecast overspend on Mental health and Learning Disability services of £700k mainly due to high cost placements.
A full year forecast underspend on prescribing of £250k
Overall QIPP savings targets are being met
All other commissioned services on plan.
The net overspend of £3.3 m was covered by reserves.
The CCG has been informed of its 2015/16 Charge Exempt Overseas
Visitor allocation which corrects the shortfall in allocation received in
201415 following CCG representations on this matter.
Financial Planning 2016/17 GP gave an update and presented a report on the financial position facing the CCG and principles going forward. Given the financial challenges facing the CCG in 2016/17 and beyond,
the following principles were agreed by the Executive at its meeting on
13 January :
As far as possible and permissible , expenditure will be incurred in 2015/16 to support 2016/17
As normal, budget meeting will be held with budget holders to help refine budgets but with the clear aim of reducing cost where possible. Budgets holders will be required to sign up to final budgets.
All new investment not started will be paused pending review of affordability. This is likely to take around 2 months.
The CCG will seek to maximise QIPP saving opportunities. QIPP savings must be real (risk rated) and credible and included in contracts or budgets as applicable. There can be no ‘unidentified’ savings requirement in the final CCG budget.
Given the QIPP ‘ask ‘ is around £6.5m ( the position moves as current uncertainties become clearer ) , and some £3.3m has so far been identified, the challenge of identifying the balance with credible risk rated schemes is a significant challenge. Consequently it is recognised that it is very likely that certain investments schemes will need to be paused.
Seek external funding where possible for transformational schemes (for example for GP extended hours from the centrally held transformation ‘fund’ )
Primary care premises development ( for which CCGs now underwrite revenue consequences ) are on hold until affordability can be properly assessed ( as well as non -financial matters )
A block contract ( a generic term for various forms of block contract ) will be sought with the main acute provider.
EN
C 1
4a 2
7.01
.16

Page 3 of 7
GP stated that at the CCG Finance Committee meeting on 20 January,
these principles were unanimously endorsed.
In terms of on-going work GP confirmed the following:
Agreement of Acute SLA’s for 2016/17. In particular constructive
discussions on a ‘block contract ‘ with Epsom & St Helier NHS
Trust have started.
A strong focus on 2016/17 QIPP savings programme
development. This includes a review, with CCG clinicians, of the
latest RightCare data packs and priority opportunities for
improved outcomes and reduced cost.
2015/16 Investment review – of new investment approved in
2015/16, some £0.8m to 2.3m has been assessed as available
for immediate review as it is not committed, not statutory, and
able to be unwound. These are difficult decisions.
Assessment of parity of esteem investment.
Clarity on use of the 1% Non-recurrent reserve.
The impact of Vanguard costs and funding.
The financial position of the BCF
Active management and review of continuing healthcare
services
Ongoing review of the named client budgets to ensure a robust
recurrent baseline together with growth control.
The impact of delegated primary care commissioning.
The impact of specialist commissioning transfers
Other service cost areas , such as the impact of the 111 / OOH
procurement
A review of organisational capacity and capability to identify that
known areas of risk, both financial and performance, are
adequately addressed.
SPG collective planning.
CSG 2.
Review of Investments 16/17 AH presented a review of 2016/17 investments and QIPP. AH stated that there was a need to identify £3.2m of potential savings (in order to achieve the net savings requirement of £6.5m on top of the current QIPP plan of £3.3m gross). It was noted that this figure was highly dependent on the CCGs financial strategy. 3 sources:
1. 16/17 investments review 2. Additional QIPP schemes 3. Challenging service leaders to identify savings
E
NC
14a
27.
01.1
6

Page 4 of 7
In order to achieve a strong financial plan aligned with the strategic plans for 16/17, there was a need to achieve the best mix of decisions across the above three areas (also noting dependencies). The Executive Committee were asked to review the information and identify any particular ideas for additional QIPP schemes that should be considered. For areas to challenge service leaders had been asked to identify savings, the Executive Committee were also asked to consider the areas identified and the scale of the ‘challenge’. AH confirmed that further work would continue over the next couple of weeks with a further report being submitted to the Executive Committee scheduled for the 10th February 2016 on 2016/17 QIPP Plans and (Dis) Investment Plans. GP stated that whilst further QIPP savings should continue be sought, he did not feel that a further £3.2m of savings could be found and that , unfortunately , savings from pausing investments would need to be at the higher end of the range ie at £2.3m.
Welcome & Introduction
1. Welcome and Apologies CE welcomed members to the meeting and apologies of absence are noted above.
2. Declarations of Interest The Register of Interest was agreed as a correct and accurate record.
3. To approve the minutes of the Executive Committee meeting held on 13th January 2016 The minutes of the meeting held on 13th January 2016 were approved as accurate records.
4. Matters arising not on the agenda & review of action log from previous meeting The action log was updated and would be submitted to the next meeting of the Executive Committee. IAPT Performance
Adrian Davey had arranged to meet with Dawn Chamberlain, Director of
Operations at SWL & ST Georges MH NHS Trust on Monday 1 February
2016, to discuss the service to understand what more was required to
improve performance.
EN
C 1
4a 2
7.01
.16
Page 5 of 7
Items for Discussion
5. Primary Care Legal Due Diligence
JB presented the final legal due diligence full report and executive
summary for South West London CCGs completed by Capsticks.
It was noted that the main report was private and confidential, with only
the executive summary being sent to members of the Plenary prior to the
meeting on 11th February 2016.
The report sets out a number of key issues and action points relating to
the following areas:
Primary Medical Contracts
Performance Management
Legacy Issues
Breach and CQC
GP Survey
Delegation Agreement
Delivery of Full QIPP Requirement
Joint Working – Governance
Conflicts of Interest Management
The Executive Committee noted the content of the report and
agreed to recommend to the Plenary of member practices that
Sutton CCG proceeds with its application for delegated
commissioning of primary medical services.
6. Quality Premium 14/15 JB presented the report on the Quality Premium Achievement for 2014/15. The CCG had received its funding award for achievement against the Quality Premium indicators for 2014/15. The award was £307,000 out of a possible £910,000. Indicators achieved were:
Access to IAPT (15% of estimated prevalence), Value15%
Improvement in Friends and Family Test in hospital, Value 15%
Improvement in Hospital Reported Medication Errors, Value 15%
So achievement was 45% of the total value, however this was reduced
by 25% for failure to meet Ambulance response times.
Indicators that were not achieved were:
Reducing Potential Years Life Lost (15%)
Reduction in Avoidable emergency admissions (25%)
Improvement in GP Out of Hours patient experience (15%)
EN
C 1
4a 2
7.01
.16
Page 6 of 7
JB stated that given the CCG’s challenging financial position, the quality
premium funding be used to finance the CCG’s primary care
engagement scheme.
The Executive Committee noted the report and agreed to commit
the financial resource to funding the primary care engagement
scheme, approved by the Governing Body/Primary Care Committee.
7. Executive Committee Forward Plan Following previous discussions at the Executive Committee CE
confirmed that he would like to review three aspects of effective meeting
content and management.
The first was the development of succinct coversheets that point the
reader towards critical components of the report which was currently
being discussed and development by the Management Team.
The second was to develop a regular cycle of feedback from clinical
members of the Executive Committee. This would ensure on an annual
basis, as a minimum, all clinical leads had a 30 minute slot on the
agenda to feedback key issues and outcomes from their area of work
and to highlight challenges and opportunities to the wider group.
The third was to develop a forward plan for the Executive Committee. An
initial draft for the remaining months of 15/16 was circulated with the
agenda. Once the format was agreed, the proposal would be to develop
a forward plan for the entirety of 2016. The forward plan would obviously
be more subject to change in later months of 2016 and would require
input from Executive Committee members, nonetheless it would provide
a guide for the Executive to ensure they are appropriately focussed.
It was agreed to include the forward plan on all future agendas of the
Executive Committee, for information.
The Executive Committee noted the paper and agreed the proposed way forward.
CE
JW
Standard Items
8. Finance Report – Month 9 As per item CSG 1 above.
9. Board Assurance Framework
GP introduced the BAF and stated that there had been no significant
changes to the BAF since the last meeting of the Executive Committee.
GP confirmed that the Implications of Primary Care Commissioning as a
new area of responsibility was now included on the BAF.
The Executive Committee noted the BAF.
EN
C 1
4a 2
7.01
.16
Page 7 of 7
10. QIPP Report – Month 8 The Executive Committee noted the contents of the report. It was noted that the current (M8) forecast outturn is 99.9% of the net target. This represents almost no change in the year end position as forecast at M7 (100.4%). The year-to-date achievement is ahead of plan (107%) at M8, an improvement on M7 (104%). Although many schemes are performing on plan (BCF and LTC schemes) or above plan (medicines management), the majority of urgent and planned care schemes remain behind plan and at risk - and we have risk-assessed and adjusted forecast final outturn savings for these schemes accordingly. Although there is potential opportunity in the BCF workstream we are not assuming this will be realised at this stage due to the potential impact of winter. The Executive Committee noted the report.
For Information
11. Report on Weekend Discharge Pilot events – Saturday 25th July and 3rd October 2015 (Super Saturday) The Executive Committee received and noted the report for information.
12. Cancer Education Event – 1 December 2015 The Executive Committee received and noted the report for information.
Any Other Business
13. Any Other Business
14. Date of Next Meeting Wednesday 10th February 2016, 1.00pm-3.00pm, Meeting Room 1, Priory Crescent
EN
C 1
4a 2
7.01
.16

MINUTES OF THE SUTTON CLINICAL COMMISSIONING GROUP
EXECUTIVE COMMITTEE MEETING
Wednesday 10th February 2016, 1.00pm - 3.00pm Meeting Room 1, Priory Crescent
Present
Dr Chris Elliott CE Chief Clinical Officer / GP - Benhill & Belmont Surgery (Chair)
Dr Senthooran Kathirgama Kanthan
SK Sutton & Cheam Locality Lead
Dr Ash Mirza AM Carshalton Locality Lead / GP - Faccini House Surgery
Dr Dino Pardhanani DP QIPP Lead-LCCs & Service Redesign / GP - Mulgrave Road Surgery
Geoffrey Price GPr Chief Finance Officer, Sutton CCG
Dr Farhan Rabbani FR Wallington Locality Lead
Sue Roostan SR Director of Commissioning and Planning, Sutton CCG
Sian Hopkinson SH Director of Performance and Primary Care, Sutton CCG
Karol Selvey KS QIPP Lead / Nurse Practitioner & Partner - Dr Grice & Partners
Dr Roshni Scott RS QIPP Lead-Medicines Management (Arrived at 2pm)
Dr Chris Keers CK QIPP Lead-Mental Health / GP - Wrythe Green Surgery
Dr Mark Wells MW QIPP Lead-Acute Contracts / GP - Wrythe Green Surgery
In Attendance
Alastair Hughes AH Director of Service Transformation
Apologies
Jonathan Bates JB Chief Operating Officer, Sutton CCG
Jane Walker JW Head of Corporate Governance, Sutton CCG
ACTION
Welcome & Introduction
1. Welcome and Apologies CE welcomed members to the meeting and apologies of absence are noted above.
2. Declarations of Interest The Register of Interest was agreed as a correct and accurate record.
3. To approve the minutes of the Executive Committee meeting held on 27th January 2016 The minutes of the meeting held on 27th January 2016 were approved as an accurate record.
4. Matters arising not on the agenda & review of action log from previous meeting The action log was updated and would be submitted to the next meeting of the Executive Committee.
EN
C 1
4a 1
0.02
.16

Page 2 of 5
ACTION
Items for Presentation and Discussion
5. Report from Clinical Lead (area to be defined by CCO) CE asked for this item to be deferred until April 2016 for work developments.
CE
Items for Discussion
6. 2016/17 First Draft Operating Plan Submission
SR gave a verbal update that the operating plan template submissions to
NHSE took place on 8th February. Feedback from NHSE is not expected
on 29 February, but key lines of enquiry will be supplied by 29 February
with feedback required by 2 March. All operating plans have to
triangulate with the provider plans. In addition, there will be a
submission for cancer relating to the constitutional standards.
GP reported the financial plan and commentary were submitted on
Monday 8th February where £3.2m was identified for QIPP. Sutton CCG
is required to allocate a 1% surplus, other CCGs are predicting either a
deficit or breakeven which will require further discussion with NHSE.
It was noted the next submissions to NHSE are12 February and 2
March.
The Executive Committee NOTED the verbal synopsis and
requested a further update be provided at March’s Executive.
7. 2016/17 Contract Negotiations SR gave a verbal update that contract negotiations had commenced with
Epsom & St Helier as the host, Royal Marsden Hospital, SWL & St
George’s Mental Health Trust and Royal Marsden for the Community
Services.
The main spend is with ESHT and discussions took place last Friday with
a further meeting scheduled for Monday 15 February on block contracts
for 2016/17. The block contracts will be managed in the same way as a
cost and volume contract, and contracts exiting a block arrangement will
be required to return to PBR - therefore overperformance will cause risks
in 2017-18. It was noted the block arrangements will be made available
to associates and the signing of contracts is scheduled for the end of
February.
GP reiterated that Sutton CCG has set aside sufficient funds for the
block contracts.
The CCG has issued a Contract Query Notice to SWL & St George’s MH
Trust in relation to performance against access into IAPT and recovery
rates. Both elements are provided as part of the Uplift.
On 1 February, an Uplift meeting was held with Sutton CCG and SWL &
EN
C 1
4a 1
0.02
.16

Page 3 of 5
ACTION
St George’s MH Trust where access was the main focus. SWL & St
George’s MH Trust have provided an action plan and further meetings to
be scheduled to assure the CCG delivery of the service and that
standards are being met going forward.
The Executive Committee NOTED the verbal update.
8. 2016/17 QIPP Plans & (Dis) Investment Plans AH tabled the documentation on QIPP schemes and investment plans.
This was covered in detail at the Management Team where the emerging
thinking of achieving the gaps were identified in the following three
areas: :
1. Additional QIPP schemes - through reviewing other SWL CCG
QIPP schemes, the EStH transformation plans and NHSE Right
Care data pack which requires additional clinical input and
guidance
2. Challenging service leaders to identify possible savings in
specified areas
3. 2016/17 investments review
The Executive Committee DISCUSSED the tabled plans and agreed that further clarification is required on how to assess the schemes in order to address the gaps.
9. Outcome of Functionally Integrated 111 OOHs Procurement FR being a member of the SELDOC Board was asked to leave the room due to conflict of interest. SR informed members following the procurement process the standstill period has been extended to respond to questions raised. A further update will be provided in due course.
SR
10. Outcome of SWL Primary Care Joint Committee CE said the general consensus from SWL Joint Committee is primary care carries a certain amount of risk. Undoubtedly, delivery of primary care will be best served via the CCGs. In 2016/17, CCGs are expected to take on board primary care; however those CCGs who are not taking delegation will remain in a shadow year, but advised to undertake this for 2017/18. Following this, if still no uptake primary care will return under the umbrella of NHSE. CE went on to say that the CCGs who opt for delegated primary care commissioning will no longer be participants of the SWL Primary Care Joint Committee. Sutton CCG will therefore no longer be a member of the Joint Committee which will be an Advisory Forum going forward.
EN
C 1
4a 1
0.02
.16

Page 4 of 5
ACTION
Standard Items
11. Feedback from Localities The Localities Leads gave a brief update and highlighted the following key points:
Sutton & Cheam Locality met on 20th January which JB attended. Discussions did take place on due diligence, but noted majority of the GPs were not in receipt of the report at that time
Wallington had nothing to report
On 26th January, Carshalton Locality members were presented with the Urgent Care dashboard
o Plenary - full attendance expected
The next Joint Locality Workshop is scheduled for 23rd February
12. Finance Update 2015/16 (M10)
GP gave a verbal finance update on Month 10 confirming the CCG was
reporting on plan year to date and will deliver the required surplus for
2015-16.
For Information
13. Approved minutes The Executive Committee received and noted the minutes for information.
14. Executive Committee - Forward Plan 2016/17 The Executive Committee received and noted the plan for information.
Any Other Business
15. Any Other Business CE informed members that he had attended the Audit Committee on 4th February, where the Internal Auditors raised there is no central register being maintained to ensure individual Conflicts of Interests are being consistently reported across all Groups/Committee. CE said a Quarterly Review with the National Care Model Team (Vanguard) was taking place today at Strawberry Lodge Conference Centre. Mary Hopper to advise as to when an update would be provided to the Executive Committee. CE reiterated the Plenary scheduled for 11 February is an important meeting and the expectation is for representation from each of the practices. SH stated a Plenary agenda item for discussion will be the PMS Review, focussing on commissioning intentions for primary care. SH informed members that Shotfield and Beddington practices will merge on 1st July 2016. It was noted the CCG 360 degree assessments will be disseminated to stakeholders today.
FM
EN
C 1
4a 1
0.02
.16

Page 5 of 5
ACTION
16. Date of Next Meeting Wednesday 24th February 2016, 2.30pm-3.30pm, Meeting Room 1, Priory Crescent
EN
C 1
4a 1
0.02
.16

Attachment 1
SUTTON CLINICAL COMMISSIONING GROUP DRAFT MINUTES OF A MEETING OF THE FINANCE COMMITTEE Wednesday 18 November 2015 Present : Dr Brendan Hudson ( Chair )
Paul Sarfaty, ( lay member, governance and audit ) Les Ross, ( lay member, secondary care consultant ) In attendance: Geoff Price, CFO 1. Apologies and minutes of the meeting of 21 October.
Apologies received from Jonathan Bates. The minutes confirmed as a correct record.
Matters arising Report on continuing health care spend Mr Price presented the report prepared by the Director responsible for CHC. This set out the financial position and planned actions to achieve a complete and accurate database of CHC patients and ensure that all clinical reviews are up to date. This report has also gone to the CCG Executive Committee. Having taken CHC ‘in house’ from September and reviewed the QA database, the CCG have found that it is incomplete and inaccurate, so much so that the CCG has had to substantially revise its 1516 CHC forecast spend which had relied on the database to this point. The CCG is now forecasting a £2.8 million overspend on a budget of £6.7m, an overspend of 40%. This is around £1m higher than previous forecast at M06 of £1.75m. The potential range of forecast overspend was around £2.5m to £3.1 m. There is significant work to do to put the database right and frustration and irritation at the position the CCG has inherited. The CCG is considering its response to the SECSU and Mr Bates, COO, will be writing to SECSU on the matter. The COO has put in place fortnightly reports from the CHC manager on progress with the action plan. The Committee noted its concern at the forecast overspend, noted the actions being taken and asked that the CCG Executive continued to monitor the position.
EN
C 1
4b 1
8.11
.15

Mr Price additionally informed the Committee that the SECSU was facing significant financial challenges and was unlikely to continue in the long term in its current form. This presented a risk to the CCG though NHSE had stated that no changes would be made until the 1617 planning round was complete. Options re forecast financial position. Covered under item 2.
2. Financial Report M07
GP presented the report. The CCG reported the M07 position to NHSE on 10 November. Key Financials
The CCG is reporting on plan year to date ( the 7 months ended 31 October 15 ) and full year forecast. This report uses month 05 prescribing and month 06 acute data as the basis for M06. In terms of the full year forecast
Overall the CCG is reporting meeting plan for both program and running costs,
however there is
o A full year forecast overspend on continuing health care costs of £2.8m (M06 - £1.75m ). This is a very significant overspend and a report on this matter went to the CCG Executive on 11 November and is included on this Finance Committee agenda.
o A full year forecast underspend on acute contracts of £1.1 m 700k ( M06; £700k ). The underspend is mainly at St Georges, the Royal Marsden and SWLEOC. The main ESH contract is forecast on contract.
o A full year forecast overspend on Mental health and Learning Disability services of £700k mainly due to high cost placements ( M06; £500k ). These are being reviewed by the MH commissioner.
o A full year forecast underspend on prescribing of £350k ( M06; £250k ). o Overall QIPP savings targets are being met
All other commissioned services on plan.
Surplus/(Deficit) £000
Running costs £000
Plan YTD 1086 2379
Actual YTD 1086 2379
Full year plan 2340 4078
Full year forecast 2340 4078
EN
C 1
4b 1
8.11
.15

The net overspend of £2 m is covered by reserves. The summary income and expenditure account is shown in appendix A. The summary acute provider position is shown in appendix B. Sutton CCG reviews and monitors it’s financial position on an ongoing basis by reviewing a range of outcomes dependent on underlying assumptions and forecasts. Mr Price noted that the CCG had recently had its ‘ stocktake ‘ meeting with NHSE(L). This had gone well overall with NHSE mainly seeking assurance on performance. On the finance side, NHSE were content with the CCG’ s position. NHSE did note the cash support that the CCG had given to Epson St Helier ( from July to November ) stating that the TDA should have provided such support. The CCG had responded that that support was not in place, and given the Trust’s cash position and the risks that posed to patient care, the CCG had taken the decision at the time to provide support. The Committee reviewed the potential forecast outturn position ( appendix C ). It reiterated its view on priorities ( per minutes of October meeting ). In summary the CCG should ensure that performance ( waiting times for treatment in the main ) is maintained.
The balance sheet position is satisfactory in terms of levels of debtors, creditors and cash with all KPIs being met. The better payment practice code re payment of suppliers is being met.
Action : options re financial position to be discussed on ongoing basis
3. Charitable Funds
There were no items to report. The next meeting is on 22 February 2016..
4. Any Other Business There was no other business. The next meeting is Wednesday 16 December at 9am.
EN
C 1
4b 1
8.11
.15

Attachment 1
SUTTON CLINICAL COMMISSIONING GROUP DRAFT MINUTES OF A MEETING OF THE FINANCE COMMITTEE Wednesday 16 December 2015 Present : Dr Brendan Hudson ( Chair )
Paul Sarfaty, ( lay member, governance and audit ) Les Ross, ( lay member, secondary care consultant ) In attendance: Geoff Price, CFO 1. Apologies and minutes of the meeting of 18 November.
Apologies received from Jonathan Bates. The minutes confirmed as a correct record.
Matters arising None that are not on the agenda.
2. Financial Report M08
GP presented the report. The CCG reported the M08 position to NHSE on 09 December. Key Financials
The CCG is reporting on plan year to date ( the 8 months ended 30 November 15 ) and full year forecast. This report uses month 06 prescribing and month 07 acute data as the basis for M08 reporting.
Surplus/(Deficit) £000
Running costs £000
Plan YTD 1332 2719
Actual YTD 1332 2719
Full year plan 2340 4078
Full year forecast 2340 4078
EN
C 1
4b 1
6.12
.15

In terms of the full year forecast
Overall the CCG is reporting meeting plan for both program and running
costs, however there is
o A full year forecast overspend on continuing health care costs of £3.1m, an increase on the M07 position of £2.8 m overspend. This is a very significant overspend and a result of continuing work on CHC since the transfer of the service from the SECSU. A fortnightly update on progress in establishing a sound system of reporting is provided to the COO. This spend also has significant implications for 1617 budgeting.
o A full year forecast underspend on acute contracts of £200k, just 0.2% from contract value. This is an adverse movement of £900k from M07 due largely to a change in the ESH and SWLEOC forecast given a significant recorded increase in activity in M07 and the Trust’s assertion that this will continue. The CCG is keen to see RTT performance improve and is generally supportive of this activity trajectory. The CCG forecast overspend on the ESH contract is £400k ( 0.4% ) and SWLEOC £300k ( 5%) . There are underspends on other acute contracts, mainly St Georges and the Royal Marsden.
o A full year forecast overspend on Mental health and Learning Disability services of £700k mainly due to high cost placements ( M07; £700k ).
o A full year forecast underspend on prescribing of £300k ( M07; £350k ).
o Overall QIPP savings targets are being met All other commissioned services on plan. The net overspend of £3.3 m is covered by reserves. The summary income and expenditure account is shown in appendix A. The summary acute provider position is shown in appendix B. Sutton CCG reviews and monitors its financial position on an ongoing basis by reviewing a range of outcomes dependent on underlying assumptions and forecasts. Appendix C gives the forecast outturn under various scenarios. The Committee reviewed the potential forecast outturn position. It reiterated its view on priorities ( per minutes of November meeting ). In summary the CCG should ensure that performance ( for example, waiting times for treatment ) is maintained as first priority.
EN
C 1
4b 1
6.12
.15

The CCG has received very outline proposals from Epsom ST Helier NHS Trust for various schemes. The CCG is supportive of transformation schemes that deliver costs savings for ESH Trust whilst maintaining or indeed improving the quality and safety of services to patients. Of course these would need to be affordable to the CCG, subject to appropriate assurance of the credibility and deliverability of the scheme presented and subject to other priorities. The CCG balance sheet position is satisfactory in terms of levels of debtors, creditors and cash with all KPIs being met. The better payment practice code re payment of suppliers is being met.
Action : options re financial position to be discussed on ongoing basis
3. Charitable Funds
There were no items to report. The next meeting is on 22 February 2016..
4. Any Other Business There was no other business. The next meeting is 20 January 2016. Action : options re financial position to be discussed on ongoing basis
EN
C 1
4b 1
6.12
.15

MINUTES OF THE SUTTON CLINICAL COMMISSIONING GROUP
QUALITY COMMITTEE MEETING
Thursday 19th November 2015 2.00pm - 4.00pm at Priory Crescent
Present
Sally Brearley SB Chair, Quality Committee, Sutton CCG
Mary Hopper MH Director of Quality, Sutton CCG
Dr Chris Elliott CE Chief Clinical Officer, Sutton CCG
Mary McKenna MM Independent Nurse Governing Body Member
Les Ross LR Secondary Care Consultant, Governing Board Member
In Attendance
Sarah Taylor ST Head of Medicines Optimisation
Clare Ridsdill-Smith CRS Public Health
Viccie Nelson VN Vanguard Programme Lead
Carolyn Moore CM IPC Specialist
Claire Symons CS Designated Adult Safeguarding Manager
Mustapha Haruna MHa Information Governance - CSU
Subodh Rusdharry SR Joint Health Commissioning Manager
Andrea Merry AM PA to Operations Team
Apologies
Dr Jonathan Cockbain JC Clinical Lead
Hilary Smith HS Vice Chair Sutton CCG Patient Reference Group
Jonathan Bates JB Chief Operating Officer
Karol Selvey KS Clinical Lead, Community & LTC
Geoff Price GP Chief Finance Officer
Dr Roshni Scott RS Clinical Lead, Prescribing
Annette Brown AB Healthwatch
Jane Walker JW Head of Corporate Governance
1. Welcome & Introduction ACTION
1.1
Welcome and Apologies SB welcomed all to the meeting and introductions were made around the table. Apologies were noted as above.
1.2
Declarations of Interest The Quality Committee approved the Register of Declared Interests as a full, accurate and current statement of all interests held and there were no amendments noted.
EN
C14
c 19
.11.
15

Page 2 of 8
2. For Review/Discussion
2.1
Medicines Management ST presented the Medicines Optimisation Team’s 14/15 Annual Report to the Committee which sets out the key activities and achievements of the team as well as providing a summary of identified and implemented savings during the past year. ST apologised for the fact that Appendix 3 was missing from report and advised that she would email the document to the Committee after the meeting. Action: ST ST updated that meeting as to the key issues to note which include:-
The Medicines Optimisation Team has expanded to include the new role of Dietician. This new role supports practices by ensuring cost-effective prescribing of products such as baby mile and sip feeds.
The prescribing budget position currently stands at an underspend of £400k with work ongoing around hospital only and specialist medicines.
Work has been undertaken to ensure that appropriate governance regulations are in place in additional to sourcing as cost effective prescribing products as possible.
All practices have an allocated pharmacist who work with them to provide guidance and prescribing support
Scriptswitch was installed in all practices in 2014/15, which provides locally authored messages and recommendations to the prescriber at the point of prescribing
The Medicines Optimisation Team continues with their involvement with the individual funding request process. This work will now be extended to include ECIs and IVF requests. All requests are given full consideration with the involvement of the CCG, Public Health, GPs and pharmacy representation, thus making it easier to identify trends and enables consistency in decision making.
With regard to PbR drugs, work has involved invoice reconciliation and validation which has resulted in savings in terms of credits back to the CCG.
ST
EN
C14
c 19
.11.
15

Page 3 of 8
2.2
The Committee noted the Medicines Optimisation Team Annual Report for 2014/15.
Learning Disabilities
SR updated the meeting as to the current position around learning disabilities and advised that there are currently three LD individuals in hospital, one being an NHS patient and two who are in private facilities.
SR stated that NHS England has issued an update which states that patients who need a hospital admission are required to receive a Care and Treatment Review. SR explained that the aim of exercise is to review if there are any other options available for patients in a community setting with a view to reducing admissions and lengths of stay.
SR advised that each CTR is attended by a Clinical Expert, a register of which is kept by NHS England. MH queried if there is a standard agreement in place between NHS England and Commissioners. SR stated that an agreement has been set out by NHS England and he will find out further information and report back. Action: SR
SR stated that a risk register is in place to ensure that patients’ needs and level of support are captured which would include social work as well as psychiatric intervention. MH commented that the Committee should be sighted on the risk register month to month and asked if it could be presented on a regular basis to the meeting. Action: SR to take forward.
CS expressed concern around the possibility that other local authorities would be able to place inappropriately in Sutton, for example for patients coming through A & E. MH advised that it was important to track information to highlight any patterns or trends such as inappropriate placements and asked SR to create a schedule of Care and Treatment reviews to be presented at future meetings. Action: SR
Information Governance
MHa presented the Information Governance report and Terms of Reference for the IG Steering Group to the meeting for information and advised that the report highlights the work undertaken by the IG Steering Group in Quarters 1 and 2.
MHa stated that key points to note are:-
Following the Continuing Healthcare Team moving to Sutton CCG, work has been ongoing to ensure that the team continue to work in a safe haven environment due to the amount of confidential data handled by the team.
MHa told the meeting that there is an issue around infection control and specifically differing perceptions as to certain roles and whether these roles would have access to identifiable
SR
SR
SR
EN
C14
c 19
.11.
15

Page 4 of 8
information. LR advised that there are still issues regarding the understanding of information assets and highlighted the fact that the LMC has challenged infection control. It was agreed that LR would discuss with MH outside of the meeting. Action LR/MHa
MHa drew the Committee’s attention to the fact that as the CHC team has now been brought ‘in house’, the CCG will now be receiving subject access requests from members of the public.
The Committee noted the Information Governance report and Terms of Reference for the IG Steering Group.
LR/MHa
3. For Approval
3.1
Draft minutes of meeting held on 15th October 2015 The minutes of the last meeting dated 15th October 2015 were agreed as a true record.
3.2
Action log Annual report for both Adults and Childrens’ Safeguarding to be submitted to a future meeting of the Quality Committee – item on the agenda as an update. ESTH to be invited to a future meeting of the Quality Committee to talk through their complaints process – MH advised that the backlog of complaints had not yet been cleared. However, new staff are now in place who are working towards getting the level of complaints back on track. ‘Other’ providers to be included in future report to the Quality Committee – MH advised that a meeting is scheduled with Sharron Bawden at the end of November which will initially start to ‘sketch out’ any new contracts. To be brought back to January Quality Committee. Action: MH Adult Diabetic data to be raised at ESTH CQRG – MH confirmed that this item is now included on the CQRG agenda. CE to raise directly with St Helier the recommendation with regards to an ICE pod. MH confirmed that an ICE pod funded by the CCG will be going into St Helier. Care Home Nurses to be invited to the practice nurse forum – MH confirmed that Karol Selvey and the Vanguard team have been working closely with care homes regarding revalidation work. It was noted that all actions have been completed.
MH
EN
C14
c 19
.11.
15

Page 5 of 8
3.3 3.4
Quality Risk Register MH presented the Risk Register to the meeting and confirmed that no changes had been made since the last meeting. MH advised that it should be noted that Continuing Health Care will be added to the register going forward. SB questioned if the risk register picked up the learning disabilities issues already discussed at this meeting. MH advised that she would review the register and report back. The Quality Committee approved the Quality Risk Register. Children’s’ Safeguarding Annual Report CS presented the Children’s Safeguarding Annual Report in Anna Cassin’s absence who had sent her apologies to today’s meeting CS advised that the report sets out the CCG’s responsibilities with regard to children’s’ safeguarding, the actions taken to achieve their responsibilities and priorities and issues for the coming year. CS stated that key points to note include:-
It should be noted that Sutton is reporting a higher number of children subject to safeguarding plans in addition to higher incidences of domestic violence compared to other Boroughs.
In 2014/15 there were 15 cases reviewed of sudden unexpected deaths in children with 2 cases going through to completion.
The team has been strengthened by the inclusion of a Looked After Children nurse role and the new postholder will be starting at the CCG in January.
There are likely to be three sets of inspections due to take place at SCCG within the next 12 months which include an Ofsted inspection and a CQC inspection.
Going forward the CCG will be supporting a business case submitted by IRIS (Identification and Referral to Improve Safety) and Anna Cassin and CS will be meeting to discuss transition planning.
Sutton CCG participated in a NHS England deep dive audit regarding safeguarding arrangements already in place and it was felt that the exercise went well. The result of the exercise
MH
EN
C14
c 19
.11.
15

Page 6 of 8
will be communicated to the CCG by the end of the year.
The Quality Committee approved the Safeguarding Children Annual Report for 2014/15.
CS advised that he Adult Safeguarding Policy and Annual Report will be
presented to the next meeting. Action CS
CS
4. Standing Items
4.1 4.1 4.2
Never Events / Serious Incidents MH advised that Epsom & St Helier reported a Never Event at the last CQRG meeting.
MH further advised that a second Never Event involving in a private hospital has been picked up through the Epsom & St Helier emergency route. The hospital is undertaking an investigation and has demonstrated that they are keen to investigate how this event occurred. MH confirmed that the incident will be reported through the STEIS process.
Safeguarding
This item has been already discussed earlier in the agenda.
Intermediate Care/Continuing Healthcare
JP gave a verbal update to the meeting on the current position and issues regarding Intermediate Care and Continuing Healthcare.
JP advised that key points to note include:-
The recruitment process for the Continuing Healthcare Team has now been completed. JP highlighted the fact that database cleansing had not been carried out by the CSU, therefore a bid has been submitted for additional admin staff to cleanse the system. Following this exercise, the CCG will be able to claw back funds for residents who have received funding but who do not fall under Sutton CCG.
Provider contract letters have been sent to Crossways and Bridge House and JP has visited both homes to discuss implementation and mobilisation plans.
JP reported that Bridge House currently only has 4 en-suite rooms. As SCCG has contracted for 10m the home will be undertaking building work to address this. It is anticipated that by March 2016 the ground floor of Bridge House will be solely for the use intermediate care.
Crossways will be reducing their beds from 16 to 8 and a block contract will be introduced as from the 8th December
EN
C14
c 19
.11.
15

Page 7 of 8
4.4 4.5
JP advised that the infection control policy will need to be reviewed with the view to developing a policy across all care homes.
Infection Control
CM updated the meeting regarding infection control and advised that key points to note are:-
CM advised that Epsom & St Helier have reported that there have been 18 Cdiff cases this year. CM further advised that Quarters 1 and 2 did not identify any lapses in care.
SCCG will be looking at processes in place to review cases which will feed into trajectories for next year.
The outbreak of MRSA on A3 at St Helier is now over and as noted earlier in the meeting, funding for an ICE pod has been agreed.
A norovirus outbreak has been reported on C4 at St Helier which has affected 9 patients and 10 staff. It has been agreed that a wash-up meeting is needed as it is felt that this outbreak was avoidable.
CM has been working with care homes in an effort to increase flu vaccinations amongst health care workers. CM advised that as a result of discussions with NHS England, it has been agreed that flu vaccines will be provided free of charge for health workers in care homes.
Vanguard – Sutton Homes of Care
VN updated the meeting as to ongoing work of the Vanguard Team which includes:-
The pilot of the new care model was launched on the 26th October. The launch outlined the new improvements in care for the elderly which are being put in place which include skill development for care home staff and the creation of the Care Co-ordinator role.
The Health Forums are continuing and are now being held on a monthly basis with the next Forum dedicated solely to the launch of the ‘Red Bag’.
There has been ongoing joint working with both Epson & St Helier and Community Services to agree and establish pathways.
The Vanguard Team have recently held an awayday to discuss and develop thinking around rolling out the Vanguard project to other care homes.
4.5 CQRG Approved Minutes and Feedback
EN
C14
c 19
.11.
15

Page 8 of 8
a) Epsom & St Helier – 8th October 2015
The Committee noted the minutes and no comments were made.
b) Sutton & Merton Community Services – 22nd September 2015
The Committee noted the minutes and no comments were made.
c) SWLStG Approved Action Points
The Committee noted the approved action points and no comments were made.
d) St Georges – 19th August and 16th September 2015
The Committee noted the minutes and no comments were made.
4.6 Forward Plan The Committee noted the Forward Plan which as agreed at the last meeting had been updated to the end of the year.
5. Any Other Business
5.1 5.2
CE stated that following the pre-planned CQC visit at Epsom & St Helier last week some immediate actions had taken place. CE further advised that an update will be given to next month’s Board Seminar. Date of Next Meeting The next meeting of the Quality Committee will take place on Thursday, 17th December 2015, 2.00 p.m. – 4.00 p.m. at Priory Crescent
EN
C14
c 19
.11.
15
MINUTES OF THE SUTTON CLINICAL COMMISSIONING GROUP
QUALITY COMMITTEE MEETING
Thursday 17th December 2015 2.00pm - 4.00pm at Priory Crescent
Present
Sally Brearley SB Chair, Quality Committee, Sutton CCG
Mary Hopper MH Director of Quality, Sutton CCG
Dr Chris Elliott CE Chief Clinical Officer, Sutton CCG
Mary McKenna MM Independent Nurse Governing Body Member
Jonathan Bates JB Chief Operating Officer, Sutton CCG
Les Ross LR Secondary Care Consultant, Governing Board Member
Dr Roshni Scott RS Clinical Prescribing Lead
Hilary Smith HS Sutton CCG Patient Reference Group
Anna Cassin AC Head of Safeguarding/Designated Nurse Safeguarding
Children
Annette Brown AB Healthwatch
In Attendance
Clare Ridsdill-Smith
CRS Public Health
Yasmin Mahmood YM Senior Associate, Equality & Diversity - CSU
Carolyn Moore CM IPC Specialist
Adrian Davey AD Commissioning Manager – Mental Health
Amy Pepper AP Admiral Nurse
Viccie Nelson VN Vanguard Team
Andrea Merry AM PA to Operations Team
Apologies
Dr Jonathan Cockbain
JC Clinical Lead
Dr Simon Elliott SE Clinical Lead, Prescribing
Karol Selvey KS Clinical Lead, Community & LTC
Claire Symons CS Designated Safeguarding Adult and MCA Lead
Jane Walker JW Head of Corporate Governance
1. Welcome & Introduction ACTION
1.1
Welcome and Apologies SB welcomed all to the meeting and introductions were made around the table. Apologies were noted as above.
1.2
Declarations of Interest
EN
C 1
4c 1
7.12
.15

Page 2 of 10
It was noted that Hilary Smith should read PRG representative and not Vice Chair – JW to amend the Register of Declared Interests. Subject to the above amendment, the Quality Committee approved the Register of Declared Interests as a full, accurate and current statement of all interests held.
JW
2. For Review/Discussion
2.1
Quality and Performance Report
MH presented the quality and performance report to the
Committee and advised that it has previously been discussed at
the Executive Meeting.
MH further advised that key points to note within the report are:-
The CQC report following the inspection of Epsom & St
Helier in November is expected to be published in
March 2016.
LAS Londonwide response times continue to be a
concern, however performance has improved within
Sutton.
A considerable amount of work has been undertaken by
AC and Claire Symons in terms of reviewing of policies,
delivery of adult and children’s safeguarding training and
Prevent training.
MH advised that as from the 1st December, the
complaints service has been taken ‘in-house’ and all
complaints are now being acknowledged and responded
to by the CCG. MH further advised that a number of
complaints previously received via the Commissioning
Support Unit have been regarding continuing healthcare
issues and as this service has also been brought back
to the CCG, the process will be much easier to manage.
The meeting discussed the quality and performance report and
following a lengthy discussion, the following questions were
raised:-
LS commented on the community service dashboard,
specifically the children’s’ therapies 30 day target
statistics which was reporting as ‘red’ on both Sutton and
Merton figures. LS queried that once the outcome of the
procurement process has been put in place will the CCG
continue to receive the same level of staff investment in
Sutton. JB confirmed that Sutton would receive the
same level of investment and advised that he has met
with Carol Lambe to discuss resources to support the
children’s therapy service. It was noted that going
forward Merton CCG statistics should be removed from
EN
C 1
4c 1
7.12
.15
Page 3 of 10
2.2 2.3 2.4
the report.
With regard to the Primary Mental Health Care Service
(Sutton Uplift), SB asked what the IAPT target of 15%
access meant. AD explained that the 15% target refers
to those service users who enter into psychological
therapy.
It was agreed that JB and MH would meet to discuss the report
prior to its presentation at the January Governing Board
meeting. Action: JB/MH
The meeting noted the Quality and Performance Report.
CQC Visit to Epsom & St Helier – Update CE updated the meeting regarding the CQC visit to Epsom & St Helier and advised that a formal written report has yet to be received from the CQC. CE advised that as highlighted in the previous Quality Committee meeting, the main area of concern is access to critical care from the general wards at St Helier. . CE stated that there is no evidence that patient care has suffered and the CCG will continue to monitor the measures which have put in place to address the issue. With regard to the recent Urgent Care Review, CE advised that no issues have been highlighted at St Helier, however staffing levels have been raised as an area of concern at Epsom Hospital. Transforming Care – December Position
AD updated the meeting as to the Transforming Care
December position and advised that the CCG is asked to
provide a report on planned discharge dates on a fortnightly
basis. AD advised that going forward a monthly return on dates
will be presented to the Quality Committee.
AD advised that there are three individuals who are currently in
an inpatient setting. AD further advised that the first patient has
an anticipated planned discharge date for the end of January,
the second patient has no discharge date planned and there
are no details regarding the CTR available as yet. The third
patient is due for discharge in the next six weeks; a placement
has been found and is currently being worked up.
AD suggested that a rag rating approach may be appropriate
for internal reporting purposes.
The Committee noted the Transforming Care December
position.
Admiral Nurse Report
JB/MH
EN
C 1
4c 1
7.12
.15

Page 4 of 10
AD updated the meeting as to the background to the Admiral
Nurse service and advised that the decision was made 18
months ago through the transforming care budget to
commission a single Admiral Nurse. AD advised that the CCG
has agreed to invest further monies and the nursing posts have
now increased to four which are linked to GP localities in the
Borough.
AP introduced herself to Committee and presented the Admiral
Service end of year report to the meeting.
AP advised that key issues to note within the report are:-
The top three referrers are Social Services, the Carers
Centre and the Community Mental Health Team. It
should be noted that there are very few referrals from
Primary Care and GPs and work is ongoing around
promoting the service in these areas.
The age of referrals and gender statistics are in line with
national data.
Ethnicity statistics highlight the fact that 14% of carers
were from a BME background.
The average Quality of Life measure for adult carers sits
within the low range.
There has been an increase in the ‘support for caring’
measure which reflects the impact the service is having
on service users.
JB asked what is the timeline for recruitment to the
additional nursing posts? AP advised that there is one
more post to recruit to which has taken longer than
anticipated; an advert for the post will be going out in
January.
Plans are in place for setting up a dedicated email
address for direct referrals to the Admiral Nursing team.
LS asked if the colours used in the pie charts could be
changed to make them stand out within the report. AP
advised that the colours used are standard within
Dementia UK, however she will feed back the request
for a more user friendly presentation.
The Quality Committee thanked AP for the report which was
noted by the meeting.
3. For Approval
3.1
Draft minutes of meeting held on 19th November 2015 The minutes of the last meeting dated 19th November 2015 were agreed as a true record.
EN
C 1
4c 1
7.12
.15
Page 5 of 10
3.2 3.3 3.4
Action log Learning Disabilities – actions regarding NHS England agreement, risk register and schedule of Care and Treatment reviews – MH advised that she will be meeting with Adrian Davey, Claire Symons and Subodh Rusdharry in the New Year to discuss how the CCG can assure themselves in terms learning disabilities/mental health issues going forward, the outcome of which will be reported on at this meeting. Other providers to be included in future report to the Quality Committee – to be brought to the January meeting. Adult Safeguarding Policy and Annual Report to be presented to the next meeting – item on the agenda for approval. Quality Risk Register MH presented the Quality Risk Register to the meeting and advised that the risk of the Continuing Health Care service being brought back in house from the CSU had been added. MH advised that a risk has been highlighted due to the fact that the data cleanse process had not been carried out by the CSU as had been originally agreed and therefore additional staff have been recruited to undertake this procedure. AC updated the meeting on another additional risk added which is namely around information sharing for GPs, specifically the issue which has arisen due to the social care team not informing GP practices of children who are subject to plans or reviews. The Quality Committee approved the Quality Risk Register. Equality and Diversity – Public Sector Equality Duty Annual Report and Workforce Equality Standard Report YM presented the Public Sector Equality Duty Annual Report and Workforce Equality Standard report to the Committee. YM advised that the annual equality report highlights the progress made at Sutton CCG regarding equality and diversity responsibilities over the past year and is due for publication by the 31st January 2016 YM explained the background to the Workforce Race Equality Standard report and advised that the standard acts as a benchmarking tool to monitor the progress of race equality within Sutton CCG. The tool sets out nine workforce race equality metric indicators and the CCG is required to
EN
C 1
4c 1
7.12
.15

Page 6 of 10
demonstrate that the organisation is following these standards as well as ensuring that their providers are also implementing the same. YM advised that she is aiming to look at four key providers in the New Year who hold large contracts with the CCG. JB queried whether the information provided within the report was correct and specifically highlighted the statement that the majority of BME staff are at VSM level. JB also queried the statistic that 66.7% of board members are women. YM stated that the information had been provided by the HR at the Commissioning Support Unit. The Committee agreed that they were unable to approve the report at today’s meeting due to the incorrect information contained within it. SB advised that due to time constraints and the fact that the report is due to be presented at the next Board Meeting in January, she suggested delegation of authority to JB and MH to review the document prior to presentation at the Board. Action: JB/MH/AC The Quality Committee agreed that they were content to delegate authority to JB/MH and AC to approve the revised version of the report.
JB/MH/AC
3.5
Adult Safeguarding Annual Report AC presented the Adult’s Safeguarding Annual Report and Adult Safeguarding CCG Policy for approval in Claire Symon’s absence who had sent her apologies to today’s meeting AC advised that the annual report has been written retrospectively for 14/15 and that CS has summarised within it the key governance arrangements as well as highlighting any changes in legislation. AC stated that key points to note include:-
The establishment of the SSAB Sub Groups to carry out functions identified by the SSAB. Two new sub-groups have been set up which are namely the Safeguarding Adults Review and Serious Case Review and the Communication and Community Engagement group. The Serious Case Review Group is co-chaired by Claire Symons.
A deep dive audit was carried out by NHS England in November which covered both adult and child safeguarding.
EN
C 1
4c 1
7.12
.15

Page 7 of 10
3.6
There were seven fatalities attributable to substance misuse between October 2013 and February 2014. JB asked if this trend had continued into 15/16 and if any lessons had been learnt from those fatalities. AD advised that the trend has been continuing and that it has been agreed with the local authority that a learning group would be established and a workshop has been arranged in January to discuss the joining up of services around substance misuse and mental health issues.
Adult Safeguarding CCG Policy AC presented the Adult Safeguarding CCG Policy to the Committee for approval and advised that Claire Symons has re-drafted the policy to incorporate the Care Act and Prevent requirements. AC asked the Committee to review and to forward her any comments regarding any inaccuracies in the policy prior to presentation to the Governing Body. Action All Prevent Policy AC presented the Prevent policy to the Committee for approval. LR queried the mandatory Prevent Awareness training for Sutton CCG staff as the majority of staff rarely has patient contact. AC advised that the training is a requirement as commissioners, that the Prevent policy is understood by staff to enable them to ensure that providers are complying with the requirements of the contract. The Quality Committee approved the Adult Safeguarding Annual Report, Adult Safeguarding CCG Policy and the Prevent Policy Sutton CCG Complaints Policy MH presented the Sutton CCG Complaints Policy to the
meeting and asked the Committee to forward her any
comments.
The Quality Committee noted the Sutton CCG Complaints
Policy.
All
4. Standing Items
EN
C 1
4c 1
7.12
.15
Page 8 of 10
4.1 4.2 4.3 4.4
Never Events / Serious Incidents
MH advised that no Never Events or Serious Incidents have been reported this month.
Safeguarding - Update
This item has been already discussed earlier in the agenda.
Intermediate Care/Continuing Healthcare
JP gave a verbal update to the meeting on the current position and issues regarding Intermediate Care and Continuing Healthcare.
JP advised that key points to note include:-
Care contracts have now gone live as of the 4th December.
There are now 8 contract beds provide at Crossways and 4 spot beds have been purchased.
At the present time, Bridge House can only supply 2 rooms; however an additional 6 rooms are in the process of adaptation to include en-suite facilities. Work is ongoing around the intermediate care unit on the ground floor and the top floor will solely be for the use of dementia and challenging behaviour residents.
There have been quality issues highlighted as robust policies are not currently in place as standard in care homes and this issue will be picked up through Vanguard team. Policies to be put in place include tissue viability, infection control and business continuity.
Cleansing of the database is currently ongoing and hopefully this will be completed by the end of December.
JP advised that it should be noted that there are still ongoing IT issues and a lack of desk space for the CHC team.
Infection Control CM updated the meeting regarding infection control and advised that key points to note are:-
There have been 2 cases MRSA cases assigned to SCCG in November. CM advised that one of these cases is regarding the dialysis line of a renal patient which has been referred to arbitration as a safeguarding
EN
C 1
4c 1
7.12
.15
Page 9 of 10
4.5
issue has been identified.
52% of staff have been given the flu vaccinations to date, however work is still ongoing to increase this figure.
There have been 26 cdiff cases at the Royal Marsden, however it is acknowledged that more tests are undertaken on patients, therefore they are more susceptible to infections.
A3 ward has seen another three cases reported with clarification awaited as to the strain of the virus. It has been noted that hand hygiene is a cause of concern within the ward. CM reported that the ICE pod has yet to be installed.
There will be an external review of infection control planned at the Trust following concerns highlighted around the recent CQC inspection.
Antibiotic prescribing has also been highlighted as an cause of concern as there is evidence that on-ward audits are not been undertaken efficiently. CM and Sarah Taylor will be meeting with the antibiotic pharmacist in the New Year to discuss.
CM advised that patient hand hygiene is another area of concern, whereby hand wipes are often handed out to patients but checks are not made to ensure they are used before meals.
CM drew the meeting’s attention to the National data capture system which was updated in October. CM advised that the system is not user-friendly and is constantly crashing and she has asked that this concern be fed up to Public Health England.
Vanguard – Sutton Homes of Care
VN updated the meeting as to ongoing work of the Vanguard Team and advised of the following:-
The ‘Red Bag’ initiative was launched at the most recent Care Home Forum at which there were approximately 40 people in attendance.
A training package and video has been produced to introduce the ‘Red Bag’ scheme. VN to forward the link to the Quality Committee.
VN
EN
C 1
4c 1
7.12
.15

Page 10 of 10
4.6 4.7
VN advised that she had attended an event with Christine Harger in Nottingham with all 6 care home vanguard sites to discuss sharing of information. It has been agreed that all 6 vanguards will visit each site and the Sutton CCG visit in planned for January.
CQRG Approved Minutes and Feedback
a) Epsom & St Helier – 5th November 2015
The Committee noted the minutes and no comments were made.
b) Sutton & Merton Community Services – 27th October 2015
The Committee noted the minutes and not comments were made.
c) SWLStG Approved Action Points
The Committee noted the approved action points and no comments were made
d) St George’s
The Committee noted the minutes and no comments were made.
Forward Plan
It was agreed that due to time constraints all would read the forward plan with any comments back to MH.
5. Any Other Business
5.1 5.2
CE advised that Dr Simon Elliott is retiring from his post as Medicines Management Clinical Lead and passed on his thanks for his work and input into the Quality Committee. CE also expressed his thanks to Mary McKenna for her input and work regarding the Quality Committee. Date of Next Meeting The next meeting of the Quality Committee will take place on Thursday, 21st January 2016, 2.00 p.m. – 4.00 p.m. at Priory Crescent
EN
C 1
4c 1
7.12
.15
Croydon, Kingston, Merton, Richmond, Sutton, Wandsworth CCGs and NHS England
PAPER 02
Page 1 of 8
MINUTES (draft) Members in attendance
Name Organisation Designation
Carol Varlaam Wandsworth CCG Lay Member (Committee Chair)
Graham Mackenzie Wandsworth CCG Chief Officer
Dr Nicola Jones Wandsworth CCG Chair
Dr Chris Elliott
(arrived at 17:22pm)
Sutton CCG Chief Officer
Tonia Michaelides Kingston CCG Chief Officer
Dr Naz Jivani Kingston CCG Chair
Kathryn Magson Richmond CCG Chief Officer
Dr Graham Lewis Richmond CCG Chair
Bob Armitage Richmond CCG Lay Member
Paula Swann Croydon CCG Chief Officer
Dr Tony Brzezicki Croydon CCG Chair
Adam Doyle Merton CCG Chief Officer
Peter Derrick Merton CCG Lay Member
David Sturgeon NHS England Head of Primary Care South London
Attendees
Name Organisation Designation
William Cunningham Davis NHS England Head of Primary Care South London
Nora Simon NHS England Assistant Head Primary Care Commissioning
Omid Gilanshah NHS England Assistant Head Primary Care Commissioning
Richard Jeffery NHS England Director of Financial Management, London Region
Dr Julius Parker Surrey and Sussex LMCs Representative
Dr Amer Salim Merton, Sutton & Wandsworth LMC
Representative
Julie Freeman London Wide LMC Representative
Cllr Ruth Dombey Sutton CCG Health and Wellbeing Board Representative
Cllr Christine Percival Richmond CCG Health & Wellbeing Board Representative
Cllr Julie Pickering Kingston CCG Health and Wellbeing Board Representative
Jamie Gillespie Wandsworth CCG Healthwatch Representative
Dave Curtis Merton CCG Healthwatch Representative
South West London Primary Care Joint Committee Meeting in public
Thursday 12th November 2015 17:00pm – 19:00pm,
Big Hall, Drake House, 44 St Georges Road, Wimbledon,
London SW19 4ED
EN
C 1
4d 1
2.11
.15

Croydon, Kingston, Merton, Richmond, Sutton, Wandsworth CCGs and NHS England
PAPER 02
Page 2 of 8
SWL Collaborative Programme Team
Name Organisation Designation
Joanne Devlin SWL Collaborative Interim AD Out of Hospital and
Primary Care
Gurvinder Chana SWL Collaborative Governance Lead
Kasia Gaj SWL Collaborative Strategic Manager Primary Care
Clare Wilson SWL Collaborative Senior Strategy Manager
Members of the public
Name Organisation Designation
Kalsoom Bibi Qureshi
Greta Ruffino
Paul
Apologies
Name Organisation Designation
Dr Andrew Murray Merton CCG Chair
Dr Brendan Hudson Sutton CCG Chair
Sally Brearley Sutton CCG Lay Member
Helen Pernelet Croydon CCG Lay Member
David Knowles Kingston CCG Lay Member
Mike Sexton Croydon CCG Chief Finance Officer
Hardev Virdee Wandsworth CCG Chief Finance Officer
Matthew Trainer NHS England Area Director South London
Dr Jane Fryer NHS England Medical Director South London
Pete Flavell Sutton CCG Healthwatch Representative
Steve Hardisty Kingston CCG Healthwatch Representative
Charlie Ladyman Croydon CCG Healthwatch Representative
Paul Pegden-Smith Richmond CCG Healthwatch Representative
Cllr Maggie Mansell Croydon CCG Health & Wellbeing Board Representative
Cllr Jim Maddan Wandsworth CCG Health & Wellbeing Board Representative
Cllr Caroline Cooper-Marbiah Merton CCG Health and Wellbeing Board Representative
Dr Marek Jarzembowski London wide LMCs Representative
EN
C 1
4d 1
2.11
.15

Croydon, Kingston, Merton, Richmond, Sutton, Wandsworth CCGs and NHS England
PAPER 02
Page 3 of 8
Item Title Action
1 Declarations of Interest – Carol Varlaam
No new declarations of interest were declared.
2 Welcome, Introductions and Apologies – Carol Varlaam
The chair welcomed the attendees and noted the apologies.
3 Minutes of the Joint Committee meeting held on 09.07.2015 – Carol Varlaam
The minutes of the last meeting were APPROVED as an accurate record of the meeting.
4 Action log from meeting held on 03.09.2015 – Carol Varlaam
The action log was reviewed and the outstanding action is on the agenda.
5 Matters arising not on the agenda – Carol Varlaam
None
ITEMS for DECISION
6 Terms of Reference and Memorandum of Understanding (for APPROVAL) – Graham Mackenzie
The SWL Primary Care Joint Committee ToR and MoU were updated following the agreement on the establishment of the working groups supporting the Joint Committee and approval of the working group membership at the last Joint Committee 03.09.2015. The three working groups supporting the Joint Committee are:
Quality, Prevention and Innovation Working Group
Capital and Estates Working Group
Finance and Contracting Working Group The Terms of Reference for the Joint Committee have incorporated the approved ToR’s for each working group into the annex, in accordance with section 23 of the Terms of Reference. The Memorandum of Understand has incorporated the agreed membership for these working groups into the annex. It was noted that Healthwatch representation and LMC representation is included on to the MoU and not the individual working group memberships. The Joint Committee APPROVED the ToR and MoU subject to the addition of Healthwatch and LMC representation being included onto the membership for each working group.
Gurvinder Chana
7 Contractual Changes: Tudor Drive (Kingston) Surgery (for APPROVAL) – David Sturgeon / William Cunningham Davis
David Sturgeon explained that the providers of the contract a Tudor Drive surgery have handed back their contract to NHS England with a termination date of 31st December 2015. NHS England have engaged with the local population, stakeholders and providers and together with Kingston CCG, they recommend that the 2,547 patients registered should be dispersed and patients be advised to register at an alternative local practice.
EN
C 1
4d 1
2.11
.15

Croydon, Kingston, Merton, Richmond, Sutton, Wandsworth CCGs and NHS England
PAPER 02
Page 4 of 8
The patient consultation ran from the 24 September 2015 to the 25 October 2015. NHS England received 428 (17%) responses from the 2,547 patients registered at the practice.
234 (9%) supporting re-procurement of the service
174 (7%) supporting dispersal
20 (1%) reporting no preference
2119 (83%) of patients did not respond, with those who did respond presenting a mixed view. The overwhelming majority of patients are unmoved by the service re-provision.
NHS England and Kingston Clinical Commissioning Group are seeking approval from the Joint Committee to proceed with the recommendation outlined in the paper to disperse the registered list at Tudor Drive Surgery upon contract termination.
Dr Julius Parker said that on behalf of Surrey and Sussex LMC, no negative comments have been reported from patients or public
NHS England and Kingston CCG APPROVED the decision to disperse the registered list at Tudor Drive Surgery.
8 Contractual Changes: Wandle Valley (Sutton) Health (for APPROVAL) – David Sturgeon / William Cunningham Davis
David Sturgeon provided a brief summary on the position with The Wandle Valley Health Centre. He explained that the contractors, AT Medics, notified NHS England Primary Care team in writing on 23 July 2015 of their intent to end their contract to provide primary medical services from that practice. It was noted that NHS England and NHS Sutton CCG have worked together on this issue, engaged with the registered patients, stakeholders including Healthwatch, the Local Medical Committee and the local MP and councillors, to ensure continuity of care for the patients registered at the Health Centre. As part of this engagement, there was a month-long patient consultation; this included writing to all registered patients, holding two drop-in patient events at the practice, and seeking opinions by post, phone, email and web-survey. NHS England carried out a patient consultation exercise which ran from the 21s September 2015 to the 16 October 2015. They received responses from 24% (450) of the 1,914 patients registered at the practice:
361 (19%) supported re-procurement of the service
74 (4%) supported dispersal, and
15 (1%) reported no preference
1,464 (76%) of patients did not respond, so although those who did respond were opposed to dispersal, the majority of patients did not express any preference.
NHS England and Sutton CCG APPROVED the decision to disperse the registered list at Wandle Valley Health.
9 Operating Model (for APPROVAL) – David Sturgeon
David Sturgeon presented the Operating Model to the Joint Committee. He explained that the Operating Model has been developed by NHS England (London), with extensive consultation with CCGs and SPGs through the Co-Commissioning Next Steps Working Group, chaired by David Sturgeon. There were a number of comments and feedback which was received and incorporated into this document.
EN
C 1
4d 1
2.11
.15

Croydon, Kingston, Merton, Richmond, Sutton, Wandsworth CCGs and NHS England
PAPER 02
Page 5 of 8
Members of the Joint Committee asked if it is possible to see a tracked change version of the Operating Model to see what changes and where these have been made.
NHS England will submit a tracked change version and the committee agreed to send around any comments to Graham Mackenzie (SPG Lead for SWL) within two weeks from the date the model is circulated. It was also agreed that if no comments are received within two weeks, then it will be assumed that the Joint Committee for SWL approve the Operating Model.
Gurvinder Chana
ITEMS for DISCUSSION
10 Personal Medical Services Update – David Sturgeon
David Sturgeon presented the latest slide deck setting out an analysis of the existing PMS contracts in SWL. He explained that a baseline and analysis of finances, current service premium and KPI that are contractualised as part of the current PMS contracts in included. The current position of the review is that engagement with each individual CCG is now beginning to take place. Carol Varlaam asked if these dates are already in the diaries and David said that confirmed dates are not in the CCG diaries as yet, but the sharing of information with the CCGs has begun. Graham Mackenzie confirmed that following the Chief Officers Group meeting, it was agreed in principle that although most of the work around PMS review will be carried out in local CCG groups, the Primary Care Quality, Prevention and Innovation Working Group will be oversee the whole process and provide feedback to this committee. Naz Jivani provided an update on Kingston position regarding PMS. He said that KCCG are still having discussions around the definitions of the investment elements of the PMS savings. He said that a lot of clarity and consistency is needed around these definitions across SWL. It was noted that the six CCG Chairs wrote a letter to NHS England asking for a substantial extension regarding the PMS review. Graham Mackenzie said that a written response has not been received; however there has been some dialogue around the potential of a three month extension. On behalf of the six CCGs, he explained that this is not enough time and therefore the CCGs will just continue with the work. The Joint Committee NOTED the paper.
11 Due Diligence Work Update – Graham Mackenzie / Mike Sexton
It was noted that five of the six CCGs have submitted their applications for move to level 3 delegations. Graham Mackenzie explained that all five submissions are subject to the completion of successful due diligence piece of work. He explained that the due diligence work is aiming to ensure that the CCGs are sighted on any contractual or financial risks that may be present in terms of taking on delegation. Two organisations have been commissioned to do this work; Capsticks for the legal review and RSM (formally Baker Tilly) for the financial work. They are due to report in the middle of December, in time for CCG Governing Bodies. Adam Doyle confirmed that Merton CCG have submitted their application and are keen to progress with delegation. However he highlighted how important the outcome of the due diligence is for each CCG and everyone needs to be clear of the consequences of the outcome. Chris Elliott supported Adam’s comment and said that CCG allocations for next year are not available as yet, so CCGs need to be sure that they can afford to take
EN
C 1
4d 1
2.11
.15

Croydon, Kingston, Merton, Richmond, Sutton, Wandsworth CCGs and NHS England
PAPER 02
Page 6 of 8
over these budgets following delegation. David Sturgeon acknowledged that NHS England have received all five applications have been received and the process of approval has begun, subject to a series of conditions. Budget allocations are due to be discussed at the National Board on 17th December 2015. The Joint Committee NOTED the update on the due diligence work.
12 Planning for London Stocktake visit 18.11.2015 – Graham Mackenzie
Graham Mackenzie informed the Joint Committee that NHS England are conducting a stock take review of progress with the delivery of primary care transformation in each of the strategic planning group areas in London. The six CCGs have been working with the collaborative team to put together a slide pack. The Executive summary was tabled at the meeting. Graham explained that the key lines of enquiry that have been asked by NHS England involve four main areas:
SWL strategy and our overall progress against the strategy How ready we are on the commissioning side of primary care transformation Provider side development – in terms of local practices Finances and other enablers to resource this piece of work
Slide 5 is a snapshot of progress and intended aims and objectives year by year up to 2019 against the main London specifications for General Practice, around access, coordinated care and proactive care. Nicola Jones said that discussions around the content of these slides have taken place amongst the CCG Chairs and their feedback has been incorporated accordingly. Naz Jivani said that there has been a bit of a pushback from Kingston CCG Council of Members around the 17 standards. They felt that when they were developed, they were appropriate but at this time, because of workforce, developments in primary care etc, they need a bit of tweeking to be able to represent what the current situation is. In essence the 17 standards should be adhered to but there are certain aspects around the wording of these standards; e.g. everyone needs to see a GP etc. Graham highlighted that one of the things SWL will be challenged on is the degree of consistency versus the variation and what is more tolerable to us across SWL. Carol Varlaam asked what is the expected range of outcomes from this stock take review. Graham said that it is a developmental piece of work, so the outputs will essentially highlight areas of challenge, successes, lessons learnt etc. The Joint Committee ACCEPTED and NOTED the planning for the Stocktake visit.
13 Finance Report Month 6 – Richard Jeffrey
Richard Jeffrey presented the month 6 finance report. He explained that the overall financial position for South West London GP Primary Medical services is showing an overspend of £652k against issued budgets for the 6 months ending 30th September 2015. This position is after the release of £1,029k non-recurrent 2014/15 accruals write backs. The overspend is largely due to unachieved planned QIPP savings. The year to date position comprises net overspends after QIPP on PMS £268k, GMS £231k, APMS £61k with a slight overspend on other. The gap between the QIPP target (£2.7m) and the recurrent QIPP opportunity continues to be the single biggest risk facing primary care budgets. NHS England has received a joint response from all CCGs regarding CCGs and NHSE collaborating to deliver transformation QIPP through primary care.
EN
C 1
4d 1
2.11
.15

Croydon, Kingston, Merton, Richmond, Sutton, Wandsworth CCGs and NHS England
PAPER 02
Page 7 of 8
It was noted that although a due diligence engagement has been commissioned to review financial and legal risks of delegated commissioning, any CCG considering taking on full delegation from 2016/17 must do so in the full knowledge of the current recurrent funding gap of £2.7m in GP primary care budgets.
Peter Derrick made a comment about QIPP and said that the success of the route that NHS England is embarking does not make him confident. He expressed that SWL are not making the QIPP targets and NHS England are making up the balance even then with some one-off non continuing savings. He said that he fears if this expectation is carried forward into 16/17; then SWL will be in a serious position in the first year of delegated primary care.
Richard explained that there will always be a QIPP ask for all of primary care for16/17; however in terms of the amount carried forward for this year because of the non-recurrent measures made, there will be some recurrent impact to some of those schemes.
Naz Jivani commented that there is a lot of pressure on primary care; QIPP initially was introduced to try and look at quality, prevention and innovation and we are still focusing on productivity and savings.
Tony Brzezicki said that it will be interesting to see the outcome of the due diligence work as there may even be a possibility that CCGs cannot actually take on their ambition of delegated commissioning.
The Joint Committee NOTED the contents of report.
ITEMS FOR NOTING / INFORMATION
14 Report back from Joint Committee Working Groups
Finance and Contracting Working Group (Mike Sexton) NOTED
Capital and Estates Forum (Hardev Virdee) NOTED
Quality, Prevention and Innovation Working Group (Dr Nicola Jones) The summary from the first meeting was NOTED and Nicola Jones explained that the focus for this working group until April 2016 is PMS review and also looking at how quality is monitored in reporting across SWL.
15 Contractual Changes – action log (to NOTE) – NHS England
NOTED
16 Open Space / Questions from the public – Members of the public
None
17 Any Other Business - All
None
The meeting closed at 18:20pm
EN
C 1
4d 1
2.11
.15

Croydon, Kingston, Merton, Richmond, Sutton, Wandsworth CCGs and NHS England
PAPER 02
Page 8 of 8
Date and Venue of next meetings
14th January 2016 14:00pm – 17:00pm 120 The Broadway, Wimbledon, SW19 1RH E
NC
14d
12.
11.1
5