gonadal hormones: estrogens and androgens synthesis, metabolism, mechanism of action, clinical use...
TRANSCRIPT

GONADAL HORMONES:ESTROGENS AND ANDROGENS
Synthesis, Metabolism, Mechanism of Action, Clinical Use
Rich Minshall, PhDAssociate Professor; Anesthesiology,
Chapter 40. The Gonadal Hormones & Inhibitors
1

Learning Objectives:
Understand the metabolic pathway of testosterone, estrogen and progesterone synthesis and know the drugs that stimulate and inhibit their synthesis
Be familiar with the use and mechanism of action of androgen synthesis and receptor blockers
Be aware of the treatment options for benign prostate hyperplasia and prostate cancer: Finasteride vs Flutamide
Know the symptoms of the menopause period and which symptoms have been shown through clinical trials to benefit from hormone replacement therapy (HRT)
Know the various estrogenic agents that may be used to treat menopausal symptoms: Premarin, Provera; PremPro
Be aware of the protocols and routes of administration of HRT. Understand the rationale for choosing one protocol or route over another.
Explain how a selective estrogen receptor modulator can act as an estrogen agonist in one tissue or cell type while acting as an estrogen antagonist in another tissue or cell type: Tamoxifen vs. Anastrazole

Steroid synthesis
3

The biosynthetic pathwayof the androgens and estrogens
19-carbon precursors are synthesized primarily in the ovaries, testes, and adrenals
4

5
Androgen Receptor Signaling

Control of androgen secretion in males
6
(1) competitive inhibition of LHRH receptors
(2) stimulation (+, pulsatile administration) or inhibition via desensitization of GnRH receptors(–, continuous administration) Lupron: synthetic analog of GnRH,
(3) decreased synthesis of testosterone in the testis; e.g., Ketocanazole, Anastrazole
(4) decreased synthesis of dihydrotestosterone by inhibition of 5a-reductase; e.g., Finesteride
(5) competition for binding to cytosol androgen receptors; e.g., Flutamide
7
Sertoli cells in the testis synthesize and secrete a variety of active proteins, including müllerian duct inhibitory factor, inhibin, and activin.Leydig cells, upon LH stimulation, produce testosterone in the spaces between the seminiferous tubules.
As in the ovary, inhibin and activin appear to be the product of three genes that produce a common a subunit and two b subunits, A and B.Activin, composed of the two b subunits, stimulates pituitary FSH release Inhibins (A and B), which contain the a subunit and one of the b subunits, in conjunction with testosterone and dihydrotestosterone , are responsible for the feedback inhibition of pituitary FSH secretion
Endogenous Mechanism of Feedback Inhibition

8
ANDROGEN REPLACEMENT THERAPY IN MEN:Androgen production falls with age in men and may contribute to the decline in muscle mass, strength, and libido. Hypo-pituitarism.
USED AS PROTEIN ANABOLIC AGENTS
USED AS GROWTH STIMULATORS
ANABOLIC STEROID AND ANDROGEN ABUSE IN SPORTS
ANDROGEN SUPPRESSION THERAPY IN MEN:benign prostatic hyperplasia; prostatic carcinoma
ANDROGEN SUPPRESSION THERAPY IN WOMEN:treatment of hirsutism
Pharmacologic Uses of Androgens

9

10
To replace or augment endogenous androgen secretion in hypogonadal men
Used rather than gonadotropin except when normal spermatogenesis is desired
For hypo-pituitarism, androgens are not added to the treatment regimen until puberty Start with long-acting agents such as testosterone
enanthate or cypionate, 50 mg IM, initially every 4, then every 3, and finally every 2 weeks, with each change taking place at 3-month intervals
The dose is then doubled to 100 mg every 2 weeks until maturation is complete
Finally, the adult replacement dose is 200 mg at 2-week intervals.
Androgen Replacement Therapy

11
Table 40–6 Androgen Preparations for Replacement Therapy.
Drug Route of Administration
Dosage
Methyltestosterone Oral 25–50 mg/d
Sublingual (buccal) 5–10 mg/d
Fluoxymesterone Oral 2–10 mg/dTestosterone enanthate Intramuscular See text
Testosterone cypionate Intramuscular See text
Testosterone Transdermal 2.5–10 mg/d Topical gel (1%) 5–10 g/d
12
Inhibition of Steroid Precursor Conversion to AndrogensKetoconazole-an inhibitor of adrenal and gonadal steroid synthesisAbiraterone- inhibits the 17-hydroxylation of progesterone or pregnenolone to androgensFinasteride- steroid-like orally active inhibitor of 5a-reductase that causes a reduction in dihydrotestosterone levels. Moderately effective in reducing prostate size in men with benign prostatic hyperplasia and is approved for this use in the USA. The dosage is 5 mg/d.Dutasteride- a similar orally active steroid derivative with a slow onset of action and a much longer half-life than finasteride. The dose is 0.5 mg daily.Anastrazole- blocks aromatase and inhibits conversion of androgens to estrogen
Receptor InhibitorsFlutamide- potent anti-androgen that has been used in the treatment of prostatic carcinoma. Although not a steroid, it behaves like a competitive antagonist at the androgen receptor.Cyproterone and cyproterone acetate are effective anti-androgens that inhibit the action of androgens at the target organBicalutamide and nilutamide- potent orally active anti-androgens that can be administered as a single daily dose and are used in patients with metastatic carcinoma of the prostate.Spironolactone- a competitive inhibitor of aldosterone that also competes with dihydrotestosterone for the androgen receptor in target tissues. It also reduces 17-hydroxylase activity, lowering plasma levels of testosterone and androstenedione. It is used in dosages of 50–200 mg/d in the treatment of hirsutism in women and appears to be as effective as finasteride, flutamide, or cyproterone in this condition.GOSSYPOL- cottonseed extract, abandoned as a candidate male contraceptive
Androgen Suppression Therapy

ANDROGEN SUPPRESSION

14
Use of Anti-Androgen Therapy to treat BPH and Prostate Cancer
The glandular cells of the Prostate produce a milky fluid, and during sex the smooth muscles contract and squeeze this fluid into the urethra. Here, it mixes with sperm and other fluids to make semen. Finasteride (Proscar, generic) and dutasteride (Avodart) are drugs used to treat benign prostatic hypertrophy (BPH). They block 5 alpha-reductase, which is the enzyme that converts testosterone to dehydroepiandrosterone (DHEA) that is known to stimulate growth of the prostate.

15
Orchiectomy-surgical removal of the testicles (surgical castration) is the single most effective method of reducing androgens. When combinded with radical prostatectomy, this will delay progression in patients with cancers that have spread only to the pelvic lymph nodes.Orchiectomy increases the risk for osteoporosis
LHRH AgonistsThe primary drugs used for suppressing androgens are LHRH agonists which block the pituitary gland from producing LH that stimulates testosterone production. Leuprolide (Lupron, Leuprogel), goserelin (Zoladex), and buserelin.Side effects: hot flashes and nipple and breast tenderness.
Anti-AndrogensAnti-androgens are drugs used to block the effects of testosterone at the receptor. Flutamide (Eulexin, Drogenil), nilutamide (Nilandron), and bicalutamide (Casodex). Side effect: diarrhea
Treatment of Prostate Cancer

16
Control of ovarian secretion and the
actions of its hormonesIn the follicular phase, the ovary
produces mainly estrogens; In the luteal phase, it produces estrogens and progesterone. SERMs, selective estrogen receptor modulators

Estrogen and Progesterone production
and negative feedback

18
Consider the normal menstrual cycle:
1) Estrogen released from the ovary - increases the expression of estrogen receptors. 2) Estrogen increases the expression of progesterone receptors. 3) Progesterone down regulates the expression of estrogen receptors. 4) With the progesterone-elicited decrease in estrogen receptor numbers - there will be a decrease in the ability of estrogen to stimulate the production of progesterone receptors - in this way - progesterone turns itself off.

19
Estrogen production from progesterone and testosterone
via Aromatase:
Treatment of estrogen-dependent Breast Cancer
withAromatase inhibitors,
Ketocanazole, Anastrazole

20
Estrogen and synthetic analogs

21
Progesterone and synthetic analogs
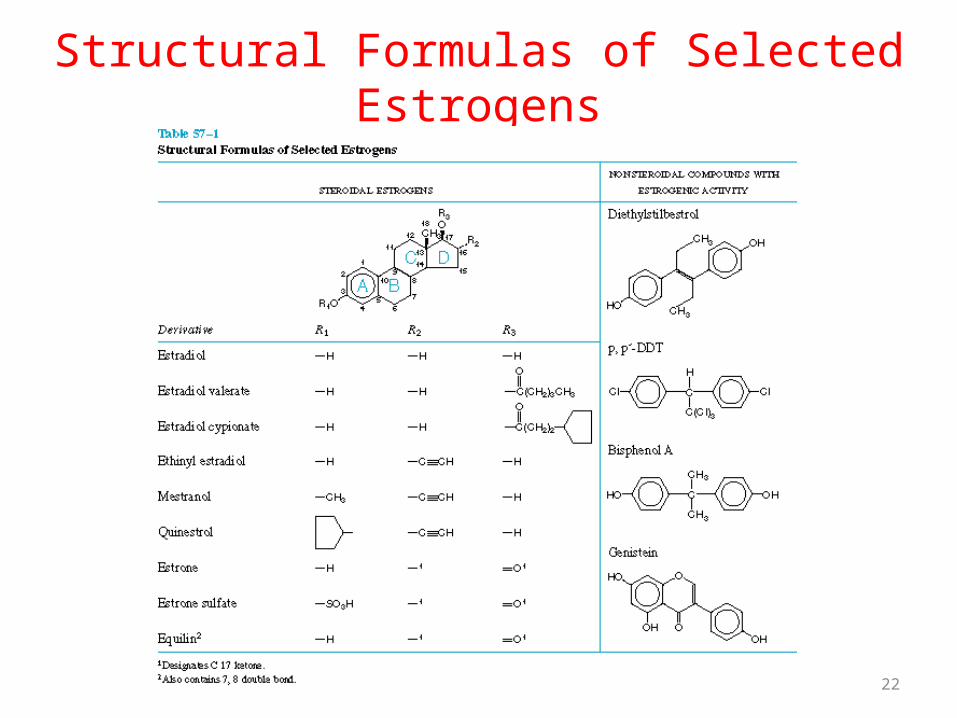
Structural Formulas of Selected Estrogens
22

Estrogen Receptor Isoforms
23

24
Estrogen Receptor Signaling

25
AP-1
Sp1

26
17-estradiol is primarily converted by 17b-hydroxysteroid dehydrogenase to estrone, and converted by 16a-hydroxylation and 17-keto reduction to estriol, which is the major urinary metabolite; sulfate and glucuronide conjugates also are excreted in the urine. Estrone also is converted to the catechol estrogen, or 2-hydroxyestrone which is methylated to 2-methoxyestrone
Elimination of Estrogens

Therapeutic Use and Dose of E2:
• pharmacological considerations for E use in OC and HRT are different because of the dose
• conjugated estrogens for HRT (0.625 mg/day for most women; 1.25 mg in some patients)
• combination oral contraceptives in current use employ 20 to 35 mg/day of ethinyl estradiol
• Conjugated estrogens and ethinyl estradiol differ widely in their oral potencies; for example, a dose of 0.625 mg of conjugated estrogens generally is considered equivalent to 5 to 10 mg of ethinyl estradiol
27

28
Alters liver metabolism
Affects on clotting and fibrinolysis- fibrinogen levels- synthesis of clotting factors (VII, IX, X,
XIII)- plasminogen levels- plasminogen activator inhibitor
Alters metabolism of lipoproteins- HDL- TG- LDL- total cholesterol
Other- increases angiotensinogen and transport
proteins
Physiological Effects of Estrogen

29
Physiological Effects of Estrogen
Alters vascular reactivity (endothelial mediators of contraction and relaxation)
- endothelin-1
- TXA2 receptors
- angiotensin II receptors
- superoxide free radicals
- nitric oxide synthase expression and activity
therefore nitric oxide
30
ANTI-ESTROGENS
• tamoxifen and clomiphene used primarily for treatment of breast cancer and female infertility, respectively
• can produce estrogenic as well as anti-estrogenic effects• competitively block estradiol binding to its receptor; act as
antagonists, agonists, or partial agonists depending upon the context in which they are used

31
Pharmacological Effects:• enlargement of the ovaries• ovulation in many patients with amenorrhea, Stein-
Leventhal syndrome, and dysfunctional bleeding.• Clomiphene is used in conjunction with human
menotropins and CG to induce ovulation• Tamoxifen exhibits anti-estrogenic, estrogenic, or mixed
activity depending upon the species and endpoint measured; inhibits the proliferation of cultured human breast cancer cells, but stimulates proliferation of endometrial cells
• estrogen-like effect to enhance bone density• does not seem to exhibit antiestrogenic effects on
lipoprotein profiles• tamoxifen and clomiphene produce hot flashes in some
women, the expected vasomotor effect

32
Mechanism of Action• Clomiphene and tamoxifen bind ER and prevent binding of E• the drugs and estradiol may interact with overlapping but slightly
different regions of the ligand binding site• depending upon the specific cellular context and gene in question, anti-
estrogen binding may yield a receptor complex that has full, partial, or no intrinsic activity
• best considered as functional competitive receptor antagonists in breast cancer cells and the pituitary
• Clomiphene can stimulate ovulation in women with an intact hypothalamic-pituitary-ovarian axis and adequate endogenous estrogens who have failed to ovulate; opposes the negative feedback of endogenous E resulting in increased gonadotropin secretion and ovulation
• clomiphene increases the amplitude of LH and FSH pulses, without a change in pulse frequency, acting largely at the pituitary level to block inhibitory actions of E on gonadotropin release from the gland and/or is somehow causing the hypothalamus to release larger amounts of GnRH per pulse
• Clomiphene also used in men to stimulate gonadotropin release and enhance spermatogenesis
• the effects of tamoxifen on proliferation of breast cancer cells appear to result largely from estrogen receptor blockade
• mammary tumors that contain ERs show a higher frequency of response to antiestrogens than do tumors without appreciable receptor levels

33
Selective Estrogen Receptor Modulators (SERMs)

34
35
Multiple Outcomes of Raloxifene Evaluation (MORE)
• Double Blind Placebo-Controlled Trial• 7705 PMP women aged 31 to 80 • Raloxifene 60 mg/d or 120 mg/d or placebo• Follow-up for 36 months for efficacy and 40 months for
adverse events• Increased BMD in femoral neck by 2.1% (60 mg) and by 2.4%
(120 mg) • Increased BMD in spine by 2.6% (60 mg) and by 2.7% (120
mg)• Increased risk of VTE (RR=3.1)• Conclusions: Raloxifene increases BMD in spine and femoral
neck and reduces risk of vertebral fracture – but increases risk of venous thromboembolism
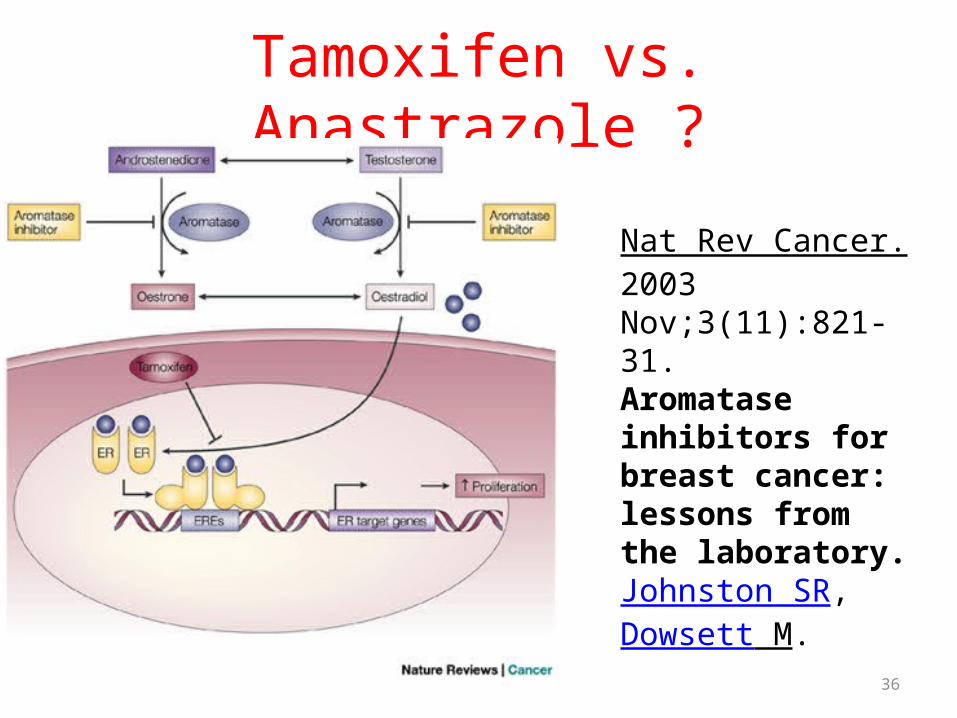
Tamoxifen vs. Anastrazole ?
36
Nat Rev Cancer. 2003 Nov;3(11):821-31.Aromatase inhibitors for breast cancer: lessons from the laboratory.Johnston SR, Dowsett M.
37
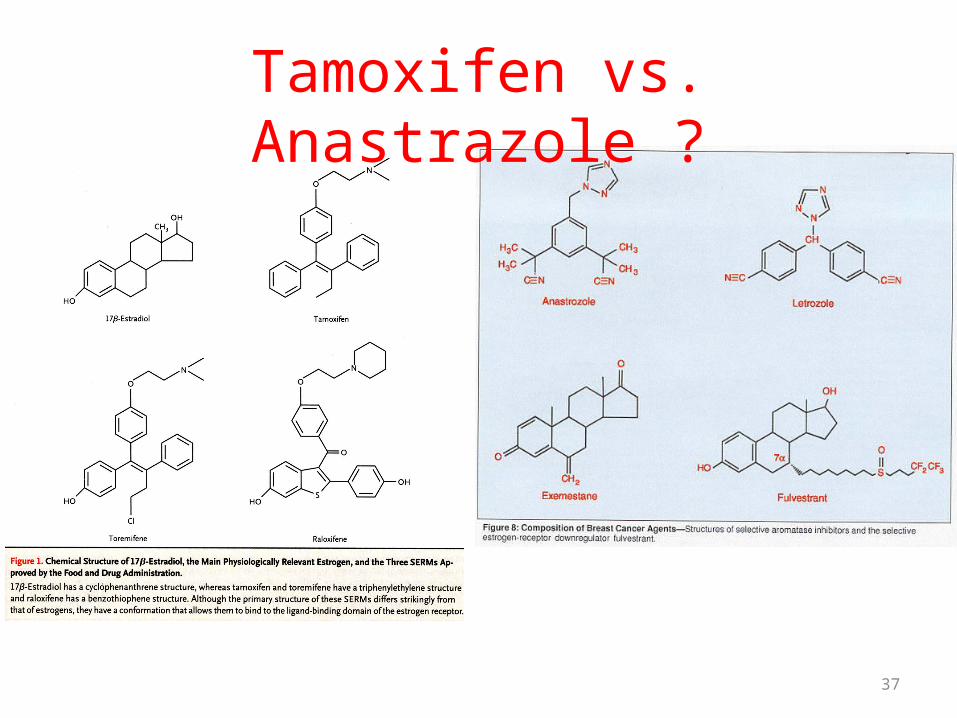
Tamoxifen vs. Anastrazole ?

38
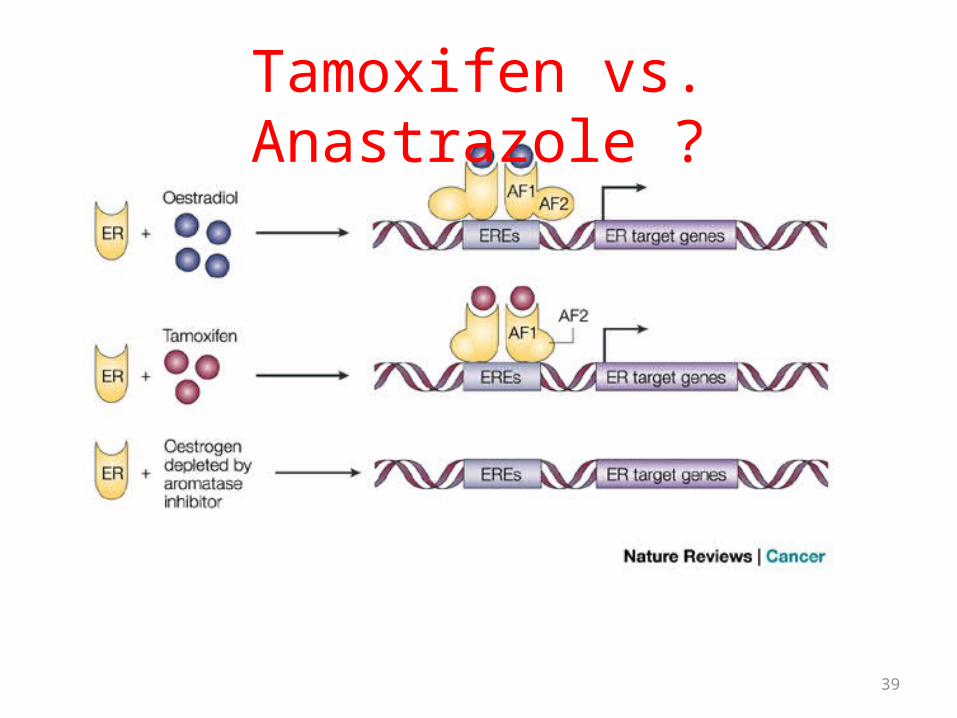
Tamoxifen vs. Anastrazole ?
39
Tamoxifen vs. Anastrazole ?

40

41
Progesterone derivatives

Progesterone Receptor• Progestins are lipophilic and diffuse freely into cells where they bind
to the PR (PR-A and PR-B)
• PRs are ligand-activated nuclear transcription factors that interact with a progesterone response element in target genes to regulate their expression
• PRs are expressed in the female reproductive tract, the mammary gland, the CNS (including the pulse generator in the hypothalamus), and the pituitary
• expression of PRs is induced by estrogens; its presence is a common marker for E action
• A single PR gene yields two forms of the receptor, the so-called A and B forms that arise from two translational start codons; the physiological and pharmacological significance of the two forms is unknown, but may relate to intracellular vs cell surface membrane PR
• progestins enhance differentiation and oppose the actions of E to stimulate cell proliferation by decreasing ER levels, increasing local metabolism of estrogens to less active metabolites, or induction of gene products that blunt cellular responses to estrogenic agents
42

43
Biological Activity of Progestins

Menopause
• Vasomotor instability (hot flashes), night sweats
• Increase incidence of cardiovascular disease
• Osteoporosis• Genitourinary atrophy• Metabolic changes – fat redistribution• Skin changes• Insomnia, fatigue, dysphoria, anxiety• Loss of memory? Susceptibility to
dementia? 44

Menopause TimetableWomen may enter menopause earlier than they realize. Estrogen levels usually drop before menopausal symptoms are seen. Below, the typical
ages for various symptoms.
SYMPTOM AGE -35 40 45 50 55 60 65 70
Dropping estrogen levels
Menstrual irregularity
Mood swings
Loss of concentration
Hot flashes
Vaginal dryness
Last period
Osteoporosis
Heart Disease
45
Sources: “Perimenopause: Preparing for the Change” by Nancy Lee Teaff and Kim Wright (Prima Publishing, 1996); “Perimenopause: Changes in Women’s Health After 35” by Drs. James E. Huston and L. Darlene Lanka (New Harbinger, 1997).

Hormone Replacement Therapy
46
Menopause: cessation of menses; loss of ovarian function leading to a state of permanent amenorrheaOvarian follicle no longer responds to gonadotropin, thus estrogen is not producedLack of negative feedback results in increased levels of gonadotropins (FSH and LH)Amenorrhea lasting 1 year – average age 51.4 years
(2 yrs earlier in smokers)
Climacteric: series of physiologic, endocrinologic and psychologic changes that signify the transition from reproductive to non-reproductive life that spans several years – perimenopausal

Routes and Compounds
• Oral Estrogens– Premarin, Cenestin– Esterified estrogen– Ethinyl estradiol– Estrone sulfate– Micronized estrogen
• Transdermal Estrogens– Less effects on liver –
no first pass effect– Patches, creams
• Vaginal Estrogens– Vaginal creams –
including premarin– Vaginal ring
• Parenteral Estrogens– Estrogen esters
• Progesterones– Medroxyprogesterone
acetate– Norethindrone – etc.– Micronized
progesterone47

Examples of HRT Preparations
• Prempro – continuous combinedPremarin and Provera
Premphase - continuous sequential Premarin 14 days then Premarin plus Provera for next 14 days
• FEMHRT – continuous combined ethinyl estradiol plus norethindrone
• Ortho-Prefest – continuous combined; 6 day cycle – day 1-3 micronized estradiol and day 4-6 micronized estradiol with norgestimate
48

49
Proposed Benefits of HRTCardiovascular• Decreased incidence of cardiovascular disease• Improved lipid profiles• Vasodilatory effects• Antiplatelet activity• Decreased fibrinogen levels• Direct myocardial effects• Antioxidant activity
• Non-Cardiovascuclar• Prevention of bone loss*• Treatment of vasomotor symptoms (hot flashes)*• Prevention of colon cancer• Prevention of Alzheimer’s disease• Prevention of urinary incontinence• Alleviation of sleep disorders
* known effects of estrogen

Reproduced with Permission. Stampfer, M. & Colditz, G. Estrogen replacement therapy and coronary heart disease: A quantitative assessment of the epidemiologic evidence. Preventive Medicine. 1991;20, 47-63.
Hospital Case-Control
50
Pop Case-Control
Prospective Internal
ControlCross-Sectional
Prospective External
Control
All Studies Combined
Prospective Internal
Control andCross Sectional 0 0.5 1
RR
1.5 2
Study Type
Relative Risk for Estrogen Use and Coronary Heart Disease
Physiological and Pharmacological Actions of Estrogen
Developmental Actions: Puberty and secondary sexual characteristics of females growth and development of the vagina, uterus, and fallopian tubes with other hormones cause enlargement of the breasts, promotion of
ductal growth, stromal development, and the accretion of fat; molding body contours, shaping the skeleton, and growth spurt of the long bones
growth of axillary and pubic hair and pigmentation of the genital region; regional pigmentation of the nipples and areolae that occur after the first term of pregnancy
Metabolic Effects of E: blocks bone resorption and increases bone formation increases the level of the hydroxylase that converts vitamin D to 1,25-
dihydroxyvitamin D3 in the kidney slightly elevates serum triglycerides and reduces total serum cholesterol
levels increases HDL levels and decreases LDL values alters bile composition by increasing cholesterol secretion and decreasing
bile acid secretion, leading to increased saturation of bile with cholesterol which may be the basis for increased gallstone formation
decrease slightly fasting levels of glucose and insulin, increase plasma levels of cortisol-binding globulin (CBG or transcortin),
thyroxine-binding globulin (TBG), and sex steroid-binding globulin (SSBG), which binds both androgens and estrogens 51
Physiological and Pharmacological Actions of Progesterone:
Neuroendocrine Actions:• P decreases the frequency of the hypothalamic pulse generator and increases the
amplitude of LH pulsesReproductive Tract:• P released during the luteal phase of the cycle decreases estrogen-driven
endometrial proliferation and leads to the development of a secretory endometrium
• decline in P release from the corpus luteum at the end of the cycle determines onset of menstruation
• P influences the endocervical glands; the abundant watery secretion of the estrogen-stimulated structures is changed to a scant, viscis material, decreasing penetration of the cervix by sperm
• E-induced maturation of the vaginal epithelium is modified toward the condition of pregnancy by P
• P is very important for the maintenance of pregnancy: suppress menstruation and uterine contractility, which led to the use of progestins to prevent threatened abortion. However, such treatment is of questionable benefit because diminished P is rarely the cause of spontaneous abortion
Mammary Gland:• P, acting with E, induces proliferation of the acini of the mammary gland• during the normal menstrual cycle, the mitotic activity in the breast epithelium is
very low in the follicular phase and then peaks in the luteal phase… P triggers a single round of mitotic activity
• in contrast, in the endometrium, proliferation is greatest in the follicular phase due to increasing E and is opposed by P in the second half of the cycle
• hormonal control of proliferation is thus different in breast and endometrium; these cell-specific effects should be kept in mind when interpreting therapeutic and untoward effects of E and P
52

Physiological and Pharmacological Actions of Progesterone:
CNS Effects:• an increase of about 1°F may be noted midway through the normal
menstrual cycle at the time of ovulation• the temperature rise persists for the remainder of the cycle until the onset
of the menstrual, and thus clearly due to P. The mechanism of this effect is unknown
• P increases the ventilatory response of the respiratory centers to carbon dioxide and leads to reduced arterial and alveolar PCO2 in the luteal phase of the menstrual cycle and during pregnancy
• P may have depressant and hypnotic actions, perhaps inducing drowsiness after administration
Metabolic Effects:• P increases basal insulin levels and the rise in insulin after carbohydrate
ingestion• long-term administration of more potent progestins, such as norgestrel,
may decrease glucose tolerance• P stimulates lipoprotein lipase activity and seems to enhance fat
deposition• P and medroxyprogesterone acetate (MPA) cause either no effect or
modest reduction in serum HDL; 19-nor progestins may cause more pronounced decrease in HDL levels, possibly due to androgenic activity. Thus, progestins may diminish the beneficial effects of estrogens on serum lipoprotein profiles in situations where the two agents are given together, such as OCs and HRT.
• P may diminish the effects of aldosterone in the renal tubule and cause a decrease in sodium reabsorption that may increase mineralocorticoid secretion from the adrenal cortex
53

54
Relationship Between Estrogen and Progesterone
1) Estrogen exerts positive feedback on its own activity.
Estrogen stimulates the expression of estrogen receptors. 2) Estrogen must precede progesterone to elicit full
progesterone sensitivity.
Estrogen stimulates the expression of progesterone receptors.
3) Progesterone has anti-estrogenic activity - which helps
to terminate estrogenic activity.
- Progesterone suppresses expression of estrogen receptors.- Progesterone facilitates the metabolism of estradiol to
weaker metabolites.- Progesterone may act as a partial agonist at the estrogen
receptor.