goldschmidt gmmg heidelberg 2013 korr kw · hd-1:treatment plan time va(i)d, until cr or plateau,...
TRANSCRIPT

27. April 2013
German-SpeakingMyeloma Multicenter Group
Hartmut Goldschmidt

Priv.-Doz. Serke, Professor HuhnPriv.-Doz. Martin, Professor HoelzerDr. Goldschmidt, Professor HaasHD1 1995
Dr. Cremer, Prof. Ho„Triple MMM“ 2000
Front-Line Trials of the GMMGHD1 Trial: Tandem-Transplantation 1996 – 1998 (Phase II, n=151)
HD2 Trial: Single- versus Double-Transplantation (Phase III, n=480) 1998 – 2001
HD3 Trial: Tandem-Transplantation (Germany) plus/minus Thalidomide (Phase III, GMMG n=550, HOVON n=500) 2001 – 2004
HO65/HD4 Trial: VAD vs. PAD, Transplantation, maintenance Thalidomide vs. Bortezomib (Phase III, GMMG n=399, HOVON=434) 2005-2008
MM5 Trial: VCD vs. Pad, Standard-intensification, consolidation / maintenance Lenalidomid, maintenance 2a vs. until CR (Phase III, n=504, Start II/2010; Extension n=100 Start 6/2013)
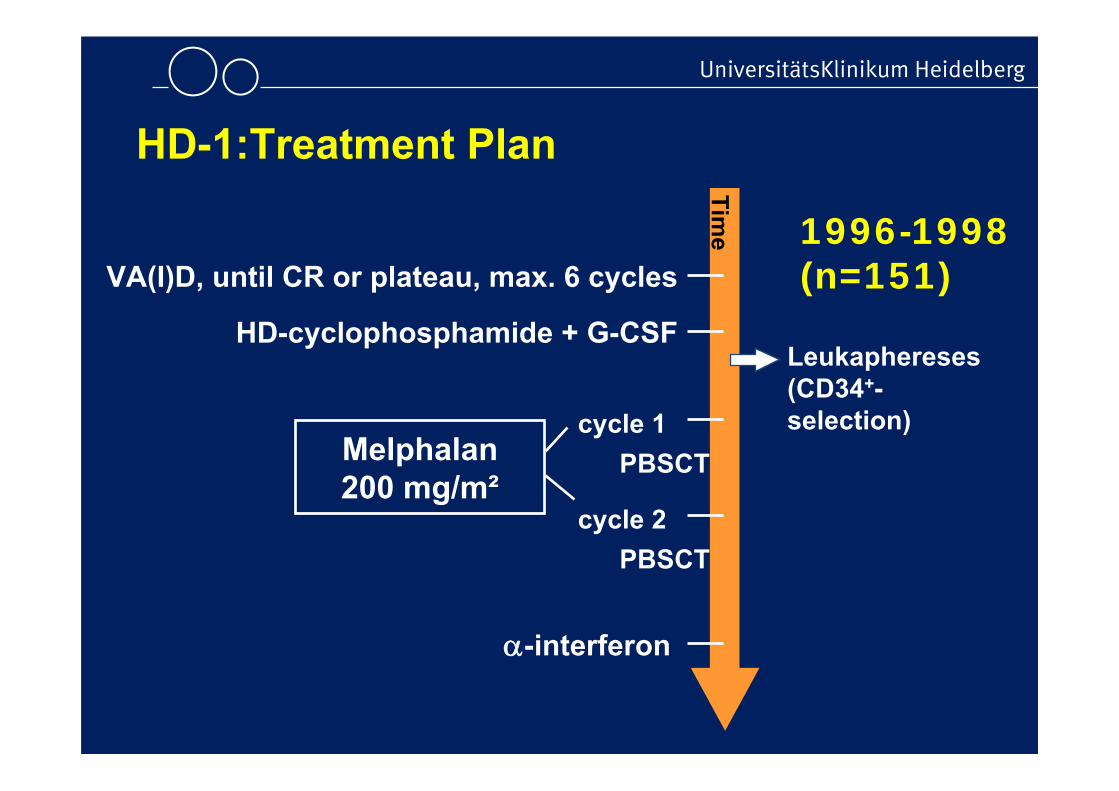
HD-1:Treatment Plan
Time
VA(I)D, until CR or plateau, max. 6 cycles
HD-cyclophosphamide + G-CSF
Melphalan200 mg/m²
cycle 1
cycle 2
PBSCT
PBSCT
Leukaphereses(CD34+-selection)
-interferon
1996-1998(n=151)
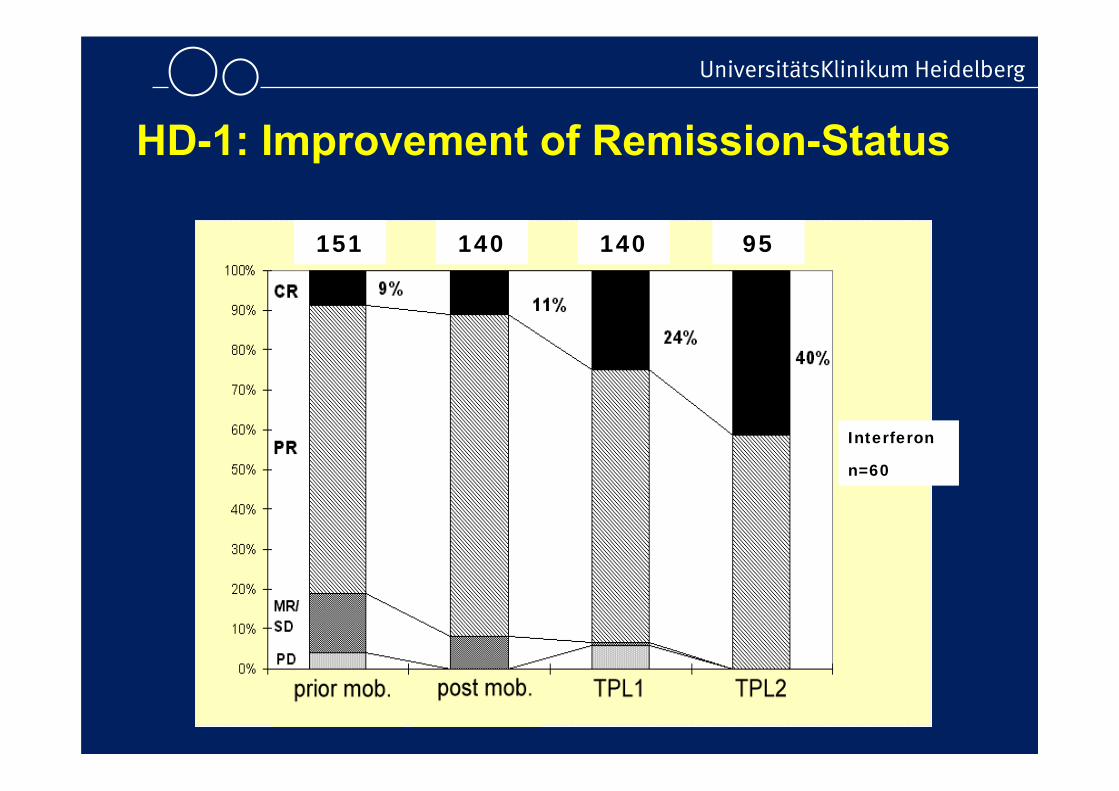
HD-1: Improvement of Remission-Status
151 140 140 95
Interferon
n=60

GMMG-HD2 Trial: Single versus Double Autologous Stem CellTransplantation for Newly Diagnosed Multiple Myeloma
• 385 pts < 65 yrs (recruited 1998-2002), 358 pts evaluable
• Treatment– 3-6 cycles of VAD-like induction– Randomization: single ASCT versus double ASCT
• Results– No significant difference for PFS between two treatment arms (P=0.36) – Only ~ 51% of pts received intended double ASCT arm
• Conclusions– Data do not support double HDT as standard frontline treatment in general– Role of double HDT in the era of new drugs is under investigation
Goldschmidt et al. IMW 2013 (Abstract P-216), poster presentation

GMMG-HD2 Trial

GMMG-HD2 Trial - Patient baselinecharacteristics

GMMG-HD2 TrialConsort Diagram

GMMG-HD2 Trial
Analysis 08/12
Intention to treat Per ProtocolITT
Progression Free Survival

GMMG-HD2 Trial
Analysis 08/12
PPIntention to treat Per Protocol
Overall Survival

Mobilisation & Leukapheresis
Randomisation
MM Stage II oder III, Age 18-65
CAD
3 x VAD
CAD
3 x AD
MEL 200 + PBSCT
MEL 200 + PBSCT
MEL 200 + PBSCT
MEL 200 + PBSCT
Thal
idom
ide
-Interferon9 Mio. U/Week
Allogeneic Tx2Gy + FludaraEBMT-study
Del13 / B2MG >3 mg/l, HLA-sib Donor
HD3/HOVON50-Studie 2001-2004

C
umul
ativ
e pe
rcen
tage
0 2 4 6
0
5
10
15
20
25
VAD
AD+thal
months At risk:
VAD 201 194 191 187 AD+thal 211 197 187 185
Logrank P=.15
VAD 201 11 AD+thal 211 19
N O
Minnema et al., Leukemia, 2004
ArmA: DVT 8 (4%)Arm B: DVT 16 (8%)Arm B + LMWH: 12 (6%)
HOVON 50/GMMG-HD3: Safety analysis
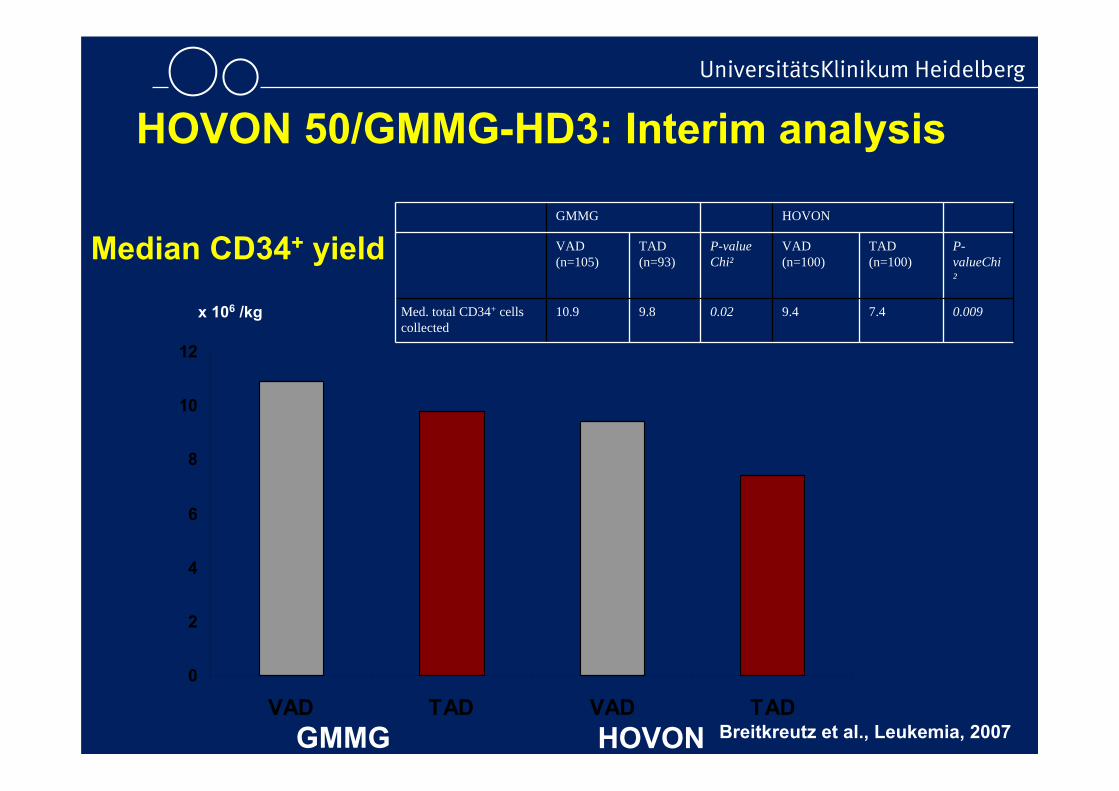
Median CD34+ yield
HOVON 50/GMMG-HD3: Interim analysis
0
2
4
6
8
10
12
VAD TAD VAD TADGMMG HOVON
GMMG HOVON
VAD (n=105)
TAD (n=93)
P-valueChi²
VAD (n=100)
TAD (n=100)
P-valueChi²
Med. total CD34+ cellscollected
10.9 9.8 0.02 9.4 7.4 0.009x 106 /kg
Breitkreutz et al., Leukemia, 2007

EFS
p = 0.012p = 0.73
Gesamtpopulation

OS
p = 0.70p = 0.42
Gesamtpopulation

Randomization
MM Stage II or III, Age 18–65
CAD + GCSF
3 x VAD
CAD + GCSF
3 x PAD
MEL 200 + PBSCT
In GMMG 2nd MEL 200 +
PBSCT
MEL 200 + PBSCT
In GMMG 2nd MEL 200 +
PBSCT
Thalidomide50 mg/day for2 yearsmaintenance
AllogeneicTx
Bortezomib1.3 mg/m2 / 2 weeksfor 2 yearsmaintenance
HOVON 65 MM / GMMG-HD4 Trial
Bortezomib 1.3 mg/m2
Doxorubicin 9 mg/m2
Dexamethasone 40 mg HDD
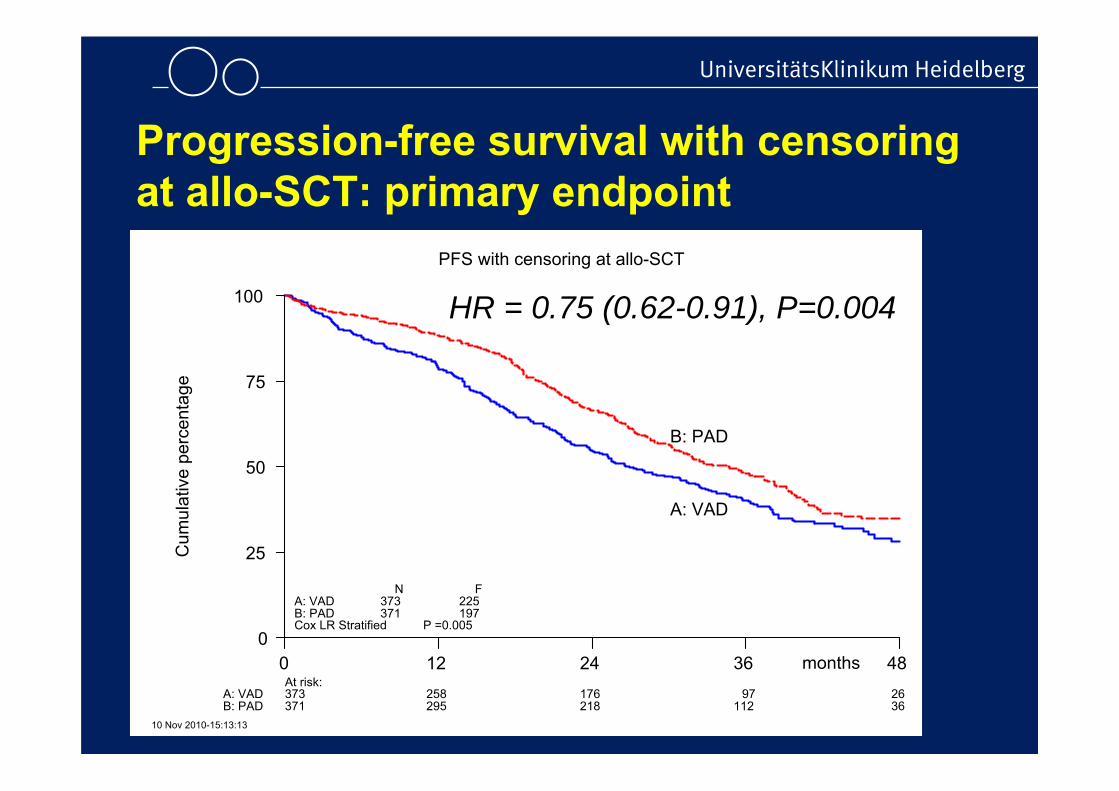
Progression-free survival with censoringat allo-SCT: primary endpoint
A: VADB: PADCox LR Stratified
N373371
F225197
P =0.005
A: VADB: PAD
10 Nov 2010-15:13:13
At risk:373371
258295
176218
97
112
2636
A: VAD
B: PAD
0
25
50
75
100
months0 12 24 36 48
Cum
ulat
ive
perc
enta
ge
PFS with censoring at allo-SCT
HR = 0.75 (0.62-0.91), P=0.004

PFS (allo censored) OS
t HR p t HR p
Arm 0.74 .002 Arm 0.70 .013
WHO 1.22 .005 WHO 1.49 <.001
IgA 1.62 .002 IgA 1.82 .01
IgG 1.33 .041 IgG 1.71 .008
LDH 1.25 .10 LDH 1.59 .006
ISS 1.25 .001 ISS 1.47 <.001
13q- 1.43 .001 13q- 1.62 .002
SG 0.81 .039 SG 0.73 .031
Multivariate Cox regression analysis

A;cr<=176A;cr>176B;cr<=176B;cr>176Logrank
N32844
33634
D89318310
P <.001
A;cr<=176
A;cr>176B;cr<=176
B;cr>176
24 Nov 2010-11:21:42
At risk:3284433634
29128
30728
26920
28025
16310
17615
A;cr<=176
A;cr>176
B;cr<=176
B;cr>176
0
25
50
75
100
months0 12 24 36
Cum
ulat
ive
perc
enta
ge
Overall survival
C. Scheid et al., ASH 2010 / EBMT 2011
HO65/HD4: Impact of kidney function

Analysis of HOVON/GMMG trial (German centres)
PFS OS
Neben et al. Blood 2012;119(4):940-8.
Impact of intensive therapy in high-riskdisease

„Standard für die Induktionstherapie war bislang VAD, so dass der Ersatz der ohnehin nicht sehr wirksamen Substanz Vincristin durch Bortezomib entsprechend dem GMMG/HOVON-Protokoll als neuer Standard für die Induktionstherapie anzusehen ist. Dies entspricht auch der Bewertung der deutschen Studien-gruppe GMMG.“
MDK Gutachten Prof. Heyll, August 2009
PAD (Vel/Dex) zur Erstlinienbehandlung vonPatienten mit multiplen Myelom


611 540 441 272 135 43534 441 364 206 101 36
Number at risk
0 12 24 36 48 60Months
Del(17p) and t(4;14) negative*0
2550
7510
0
B-based ASCT(s)Non-B-based ASCT(s)
B-based ASCT(s)
Non-B-based ASCT(s)
P=0.0101
50
41
HR 0.79 (0.67-0.95) p=0.010
172 144 112 59 28 9150 112 71 33 15 5
Number at risk
0 12 24 36 48 60Months
Del(17p) and/or t(4;14) positive*
025
5075
100
B-based ASCT(s)Non-B-based ASCT(s)
B-based ASCT(s)
Non-B-based ASCT(s)P=0.0002
35
23
HR 0.58 (0.44-0.76) p=0.000
* Regardless of presence or absence of del(13q)
PFS according to B-based and non-B-based ASCT(s) within subgroups with or without cytogenetic abnormalities
Bortezomib-based versusnon-bortezomib-based inductionprior to ASCT in multiple myeloma:meta-analysis of phase 3 trials
Pieter Sonneveld,1 Hartmut Goldschmidt,2 Laura Rosiñol,3 Joan Bladé,3Juan José Lahuerta,4 Michele Cavo,5 Paola Tacchetti,5 Elena Zamagni,5
Michel Attal,6 Henk M. Lokhorst,7 Avinash Desai,8 Andrew Cakana,9 Kevin Liu,10 Helgi van de Velde,11 Dixie-Lee Esseltine,12
Philippe Moreau13
1Department of Hematology, Erasmus Medical Center, Rotterdam, the Netherlands; 2University Hospital of Heidelberg, Heidelberg, Germany; 3Hematology Department, Hospital Clinic de Barcelona, IDIBAPS,
Barcelona, Spain; 4Servicio de Hematología, Hospital Universitario 12 de Octubre, Madrid, Spain; 5Istituto di Ematologia Seràgnoli, Università degli Studi di Bologna, Bologna, Italy; 6Department of
Hematology, Hopital Purpan, Toulouse, France; 7Utrecht Medical Center, Utrecht, the Netherlands; 8Janssen Global Services, Raritan, NJ, USA; 9Janssen Research & Development, High Wycombe, UK; 10Janssen Research & Development, Raritan, NJ, USA; 11Janssen Research & Development, Beerse, Belgium; 12Millennium: The Takeda Oncology Company, Cambridge, MA, USA; 13University Hospital,
Nantes, France

1. Harousseau JL, et al. J Clin Oncol 2010;28:4621-9. 3. Rosiñol L, et al. Blood 2012;120:1589-96.2. Sonneveld P, et al. J Clin Oncol 2012;30:2946-55. 4. Cavo M, et al. Lancet 2010;376:2075-85.
• Bortezomib-based regimens compared to non-bortezomib-based previous standards of care as induction therapy prior to ASCT ina total of 4 multicenter, cooperative group phase 3 studies1–4
Study 1º endpoint Bortezomib-based regimen Non-bortezomib-based regimen
IFM 2005-01 Post-induction CR+nCR rate
Bortezomib-dexamethasone(N=240)
Vincristine-doxorubicin-dexamethasone (VAD, N=242)
HOVON-65/ GMMG-HD4
PFS Bortezomib-doxorubicin-dexamethasone (PAD, N=413)
VAD(N=414)
PETHEMA GEM05MENOS65*
Post-induction and post-ASCT CR rate
Bortezomib-thalidomide-dexamethasone (VTD, N=130)
Thalidomide-dexamethasone(TD, N=127)
GIMEMAMM-BO2005
Post-induction CR+nCR rate
VTD(N=241)
TD(N=239)
*Study included a third induction arm, comprising VBMCP/VBAD followed by bortezomib
Background

OR for post-transplant CR+nCR rate similar across studies
• With inclusion of study-level data from GIMEMA MM-BO2005, the pooled OR remained similar (1.96) to that for the integrated analysis
Non-bortezomib-basedBortezomib-based
Study Odds ratio (95% CI) N CR/nCR (%) N CR/nCR (%) P-value
HOVON-65/GMMG-HD4 2.02 (1.46, 2.79) 408 82 (20) 409 136 (33) <0.0001
IFM 2005-01 1.99 (1.34, 2.96) 238 56 (24) 236 90 (38) 0.0006
PETHEMA GEM05MENOS65 2.31 (1.40, 3.83) 126 44 (35) 130 72 (55) 0.0010
Pooled (fixed effect) 2.05 (1.64, 2.56) 772 182 (24) 775 298 (39) <0.0001
Heterogeneity I2 = 0%Q = 0.25 with df = 2
GIMEMA MM-BO2005 1.75 (1.22, 2.52) 238 98 (41) 236 130 (55) 0.0025
Pooled (fixed effect) 1.96 (1.62, 2.37) 1010 280 (28) 1011 428 (42) <0.0001
Heterogeneity I2 = 0%Q = 0.82 with df = 3
Favor non-bortezomib-based treatment Favor bortezomib-based treatment
Odds ratio and 95% CI (log scale)
0.2 0.5 1 2 5

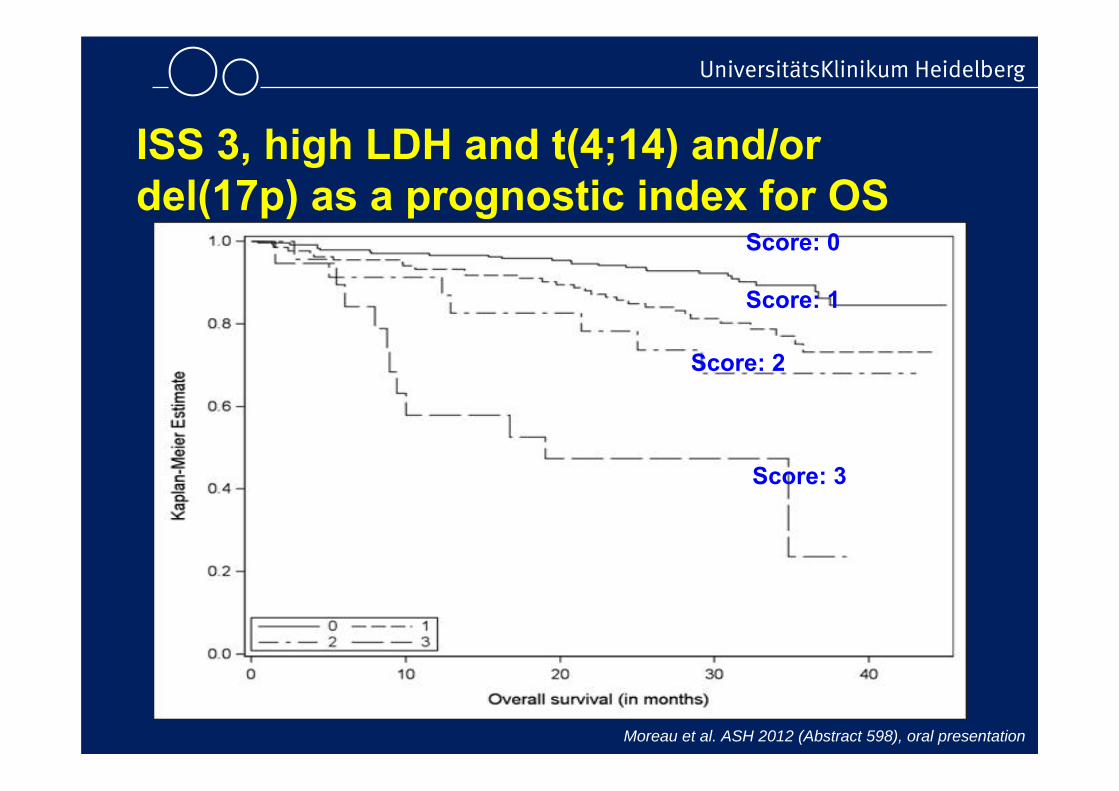
ISS 3, high LDH and t(4;14) and/or del(17p) as a prognostic index for OS
Score Definition % of overall population Outcome
0 Absence of adverse factors (neither high LDH, nor ISS 3, nor t(4;14) and /or del(17p)) 57% 3-year OS: 89%
1 Presence of only 1 adverse factor (either high LDH or ISS 3 or t(4;14) and/or del(17p)) 32% 3-year OS: 73%
2 Presence of high LDH plus ISS 3 in the absence of t(4;14) and /or del(17p) 6% 3-year OS: 68%
3 Presence of t(4;14) and/or del(17p) in addition to either ISS 3 or high LDH 5%
Median OS: 19 mos
3-year OS: 24%
Moreau et al. ASH 2012 (Abstract 598), oral presentation
ISS 3, high LDH and t(4;14) and/or del(17p) as a prognostic index for OS
Score: 0
Score: 1
Score: 2
Score: 3
Moreau et al. ASH 2012 (Abstract 598), oral presentation

Scoring system
Score GIMEMA
N = 399
IFM
N = 405
Pethema
N = 381
HOVON /GMMGN = 416
Total
N = 16010 232
(58%)234
(58%)236
(62%)201
(48%)903
(56%)
1 134(34%)
128(32%)
110(29%)
143(34%)
515(32%)
2 8(2%)
23(6%)
16(4%)
21(5%)
68(4%)
3 25(6%)
20(5%)
19(5%)
51(12%)
115(7%)

24181260
1,0
,8
,6
,4
,2
0,0
3
2
1
0
2-year Overall survival (OS) according to « scoring system »in 850 patients receiving bortezomib-based induction
OS 1
0.8
0.6
0.4
0.2
06 12 18 24 months
93%86%
73%
52%
P < 0.0001

Cereblon Expression in HOVON-65/GMMG-HD4
Broyl A, et al. Blood. 2013;121:624-7.
48
1.0
0.8
0.6
0.4
0.2
0.00 12 24 36
Prog
ress
ion
free
sur
viva
l
Months
p = 0.009
> median< median
42 31 13 430 19 4 0
A
1.0
0.8
0.6
0.4
0.2
0.00 12 24 36
Prog
ress
ion
free
sur
viva
l
Months
p = 0.18
> median< median
38 19 3 239 33 10 4
C
48
1.0
0.8
0.6
0.4
0.2
0.00 12 24 36
Ove
rall
surv
ival
Months
p = 0.81
> median< median
42 35 15 847 43 25 10
D
48
–2
60
1.0
0.8
0.6
0.4
0.2
0.00 12 24 36
Ove
rall
surv
ival
Months
p = 0.13
> median< median
48 38 18 940 31 16 6
B
48
11
60
A-B: thal-treated, C-D: bort-treated

symptomatic MM 1st line treatment
18-70a
3 x PAd
Lenalidomide
for 2 years
CAD + leukapheresis
3 x VCD
HDM + TPL
2. HDM + TPL (if no nCR/CR)
2 x Lenalidomide
Randomization
Lenalidomide
for 2 years
Lenalidomideif no CR
Lenalidomideif no CR
A1 B1 A2 B2
A1 + B1 A2 + B2
1) 1)
MM5-Trial
Flowsheet 31.03.20111) High Risk Patients, optional in Phase II trial
Standard intensificationaccording to local protocol(GMMG standard)

Amendment – seit 02/2012→ subkutane Applikation von Bortezomib
Moreau et al., Lancet Oncol., 2011:
- Bessere Verträglichkeit (PNP-Rate ↓)
- Vergleichbare Response-Raten
Umstellung in MM5
von i.v. zu s.c.-Applikation
- Gleiche Dosis, Injektionsvolumen ↓

GMMG-ReLApsE study
1) stem cell collection only if no useable stem cells are available from earlier mobilization2) Lenalidomide maintenance therapy 10mg/dayR-Lenalidomide, D-Dexamethasone, HD Mel-high dose Melphalan
relapsed Multiple Myeloma (1.-3. relapse)age 18-70 years
relapse ≥12 months after high dose therapy
Randomization
3x RD
Cyclophosphamide + G-CSF + stem cell collection 1)
Cyclophosphamide + G-CSF + stem cell collection 1)
RD until progression/ relapse
HD Mel 200mg/m²+ autologous transplantation
R-maintenance 2)
until progression/ relapse
3x RD

OS GMMG-HD2 vs HD3/HD4
years since first HDM
OS
Pro
babi
lity
0 1 2 3 4 5 6 7 8
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Overall Survival ITT
HD2HD3/HD4
GMMG-HD2, -HD3, -HD4 – Beteiligte Kliniken und Praxen

Assoziierte Prüfzentren in hämatologischen Studien• Hinweis auf Publikation im Ärzteblatt
Schurich, B., Bertsch, U., Hügle-Dörr, B.: Deutsches Ärzteblatt, Jg. 110, Heft 5, Seite 176 -177, 01. Februar 2013

Altenkirchen / StrehlAschaffenburg/WelslauBaden-Baden / StaigerBad Honnef / ForstbauerBad Kreuznach / SchulzBad Mergentheim / HartungBerlin / KieweBerlin / Ilona BlauBerlin Seestraße/ SchmittelBochum / NückelBonn / KoBonn / VerbeekBonn-Beuel / ForstbauerBraunschweig / PiesBuchholz / SchiederCelle / MarquardCoburg / LambertiDarmstadt / KojouharoffDortmund / LathanDuisburg / Selbach, AnhufErfurt / WenigerEschweiler / StaibFrankfurt / BollingFrankf.NW-KH / WeidmannFrankfurt Maingau KH/ Böck
Frankfurt / Prof. ChowFrechen / SchulzGießen / Schließer Hamburg / Engel (HOPA)HH-Schnelsen /Müller-HagenHH-Lerchenfeld / WolffHanau / FauthHanau Klinikum / ImmenschuhHeidelberg / Karcher/FuxiusHeilbronn / KoniczekHeilbronn / Martens (SLK)Hennigsdorf/SpeidelIdar-Oberstein / RoemerKaiserslautern / ReebKarlsruhe / ProcacciantiKoblenz / Thomalla (InVO)Köln / ReiserKöln / SchmitzKöln-Holweide / SchulteKöln / MVZ WeihrauchKronach / StauchLandshut / Vehling-KaiserLebach / KremersLüneburg / GoldmannMainz / Papesch
Mannheim / HenselMarburg / BalserNeunkirchen / SchmidtNürtingen / GolfOberhausen / SteinigerOffenbach / BöckOstfildern Paracelsus / AbelePforzheim / DencaussePinneberg / LeonhardPirmasens / ScheuerSiegburg / FronhoffsSiegen / KlumpSingen / FietzSpeyer / Franz-WernerStuttgart / DenzlingerTrier / GrundheberTrier / Kirchen (Brüder-KH)Trier / RendenbachTrier / Mahlberg (Mutterh.)Troisdorf / ForstbauerViersen / ReiterWendlingen / EckertWesterstede / JanssenWolfsburg / Gabrysiak

First patient in:
26.07.2010
Last patient in:
11.10.2012
n=504 Patienten
Rekrutierung MM5
geplantregistriert
Soll: ca. 7 Pat./Monat (erste 6 Monate)
Soll: ca. 15 Pat./Monat (ab Monat 7)
MM5 – Rekrutierung (11.10.2012)

To do 2013• Fokus auf Relapse
• Extension MM 5 (LKP Goldschmidt)
• Benda-Borte-Pred. (LKP Knauf)
• Poma responseadaptiert plus Cyclo (LKP Weisel)
• MM6 Protokoll (Start 2/14)
• Tumorzell-Mob (Start multizentrisch 4/14)

GMMG - Study group meeting