goals of pulp therapy allowing the child to masticate with comfort. allowing the tooth to remain...
TRANSCRIPT



Goals of pulp therapy
Allowing the child to masticate with comfort.
Allowing the tooth to remain in the mouth in a nonpathogenic state.
Maintenance of tooth space and arch length.
Prevention of speech abnormalities.
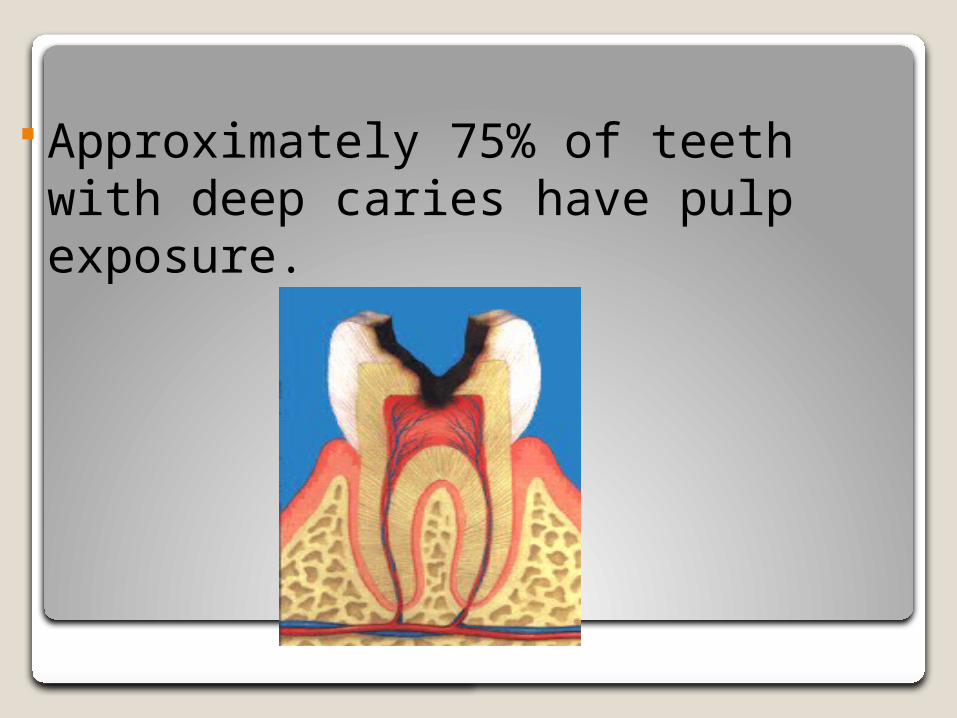
Approximately 75% of teeth with deep caries have pulp exposure.

Why is it important to for the pedodontist to conserve pulpally involved teeth?

premature extraction of pulpally involved teeth leads to loss of space
and subsequent problems concerning the development of occlusion in the permanent dentition.
Factors influencing success of pulp therapy:
Speed of carious attack.Depth of bacterial penetration into the
pulpal tissue.Type and amount of pulpal hemorrhage.The extent of pulp inflammation.Pulp age (mature and immature teeth)

Young dental pulp has a high degree of cellularity and vascularity.
Young pulp is ready for procedures concerned with the preservation of pulp vitality e.g.: indirect pulp capping and pulpotomy.

Evaluation of pulp vitality

Preoperative diagnosis is important and dictates the type of treatment to be carried out.
Accurate determination of the extent of pulp inflammation cannot be made short of histological examination.
Correlation between clinical symptoms and histological features is poor in exposed primary pulp.
Diagnostic considerations

Factors to be considered before clinical and radiographic evaluation for pulp therapy:
1. The length of time the tooth to be retained.
2. The restorability of the tooth.3. The status of the remaining
dentition.4. The patient and parent cooperation
(attendance for periodic evaluation).

5.Physical condition of the patient:Success of pulp therapy depends on the absence of systemic disturbances.

1)Endodontic treatment in patient with cardiac disorders can expose the patient to the risk of subacute bacterial endocarditis.
2)Chronic illness, such as diabetes, nephritis, leukemia, tumors or any condition that causes depression of granulocytes and leucocytes counts are contraindicated for pulp therapy to avoid the possibility of acute infection.

Diagnostic information
History of painMobilitySensitivity to percussionCharacter of exposure siteEvaluation of hemorrhage at exposure siteRadiographic picture
History of pain
A negative history of pain is not a reliable sign to diagnose the pulp status of primary teeth.
Children are often unable to recall the experience of pain they have short attention span.
Varying degree of pulp degeneration are seen without any history of pain.
The nerve element diminishes with time as the tooth approaches shedding.

Children with rampant caries have experienced pain since their early years and probably had no other experience and can recall only dental pain. Symptoms could be misleading because of their apprehension.History is sometimes misleading due to parental influence.

characteristics of pain
It includes type of pain, duration, frequency, and provoking factors.
Sensitivity to thermal stimuli indicates vital pulp.
Pain relationship to pulp status Type and duration of pain provide a clue
as to:Whether the pulp inflammation is
mild chronic necrotic changes
Type of pain provoked or spontaneousDuration intermittent or continuous

Provoked pain : is temporary sensitivity to thermal changes in a deep carious lesion
or Pain associated with eating.or sensitivity to sweets The Provoked pain is usually reversible and disappears with removal of stimulus.
Type of pain
Pain associated with eating:History of momentary pain associated
with eating and disappears with removal of the stimulus indicates that there is only a thin layer of remaining dentine between the carious lesion and the pulp.

The Pain is probably due to:Pressure on the dentine floorChemical irritation of foodThermal irritation.
The pain probably indicates:No actual exposureReversible pulp statusA tooth that is good candidate for indirect
pulp capping or if accidentally exposed may be a good candidate for direct pulp capping or pulpotomy.
Spontaneous or unprovoked pain:
The pain is unprovoked and nocturnal; it awakes the child during night sleeps.
It is an acute continuous throbbing painIt is often an indication of a hyperemic pulp a
widespread inflammation of the pulp extending throughout the radicular part (irreversible).
characteristics of pain:
Duration of pain:Temporary pain indicates reversible
pulpitis due to exposure of dentine to oral environmental factors due to leaking restoration or frank cavitations.
Persistent pain indicates widespread pulpitis.
Clinical implication of pain Reversible pulpitis: Pain provoked by thermal, chemical or mechanical irritants & is reduced or eliminated when the stimulus is removed.
Chronic pulpitis: intermittent dull aching pain.
Irreversible wide spreading pulpitis:
A history of spontaneous throbbing pain, particularly at night and keep the child awake, indicates extensive inflammation of the pulp.
This contraindicates vital pulp therapy.The tooth is indicated for extraction or
RCT.

Diagnostic clinical signs and symptoms.

I Visual examination
1.Caries, trauma, missing or fractured restoration

2.Gingival swelling, fistulas tract, tenderness or enlargement of lymph nodes are signs of necrotic pulp with acute or chronic abscess formation.

3.Discoloration and loss of translucency of teeth are indications of pulp degeneration.

II- Manipulation
Sensitivity to vertical percussion. Abnormal tooth mobility
associated with pain. Both are signs of advanced pulp
inflammation that proceeded deep apically to involve the periodontal ligament.

II- Manipulation
• Older children undergo normal exfoliation mobility which should be
substantiated radiographically.• Sensitivity to percussion may also
be related to high restorations.

III-Pulp Vitality Tests
Vitality tests are of little value for children. The use of this type of stimulation might
cause loss of the child’s cooperation.

There are 2 types of vitality test:
1-Electrical pulp test.
2-Thermal pulp test.

Electric Pulp Test It is done by applying an electric
impulses on the mid-buccal dry tooth surface under test.
The result obtained from the tooth in question is compared to the contra lateral sound tooth.
The test indicates vitality condition not the degree of pulp pathological condition.

The difference may be :
Immediate rapid response indicating pulp hyperemia
Delay or no response indicating a non vital tooth pulp.
The test does not give reliable evidence of the degree of pulp inflammation in children.
False positive results may be due to :
1- Excessive fear in young children.2- liquefaction of the radicular pulp tissues.3- Stimulation of the gingiva or periodontal ligament.4-contact with a vital tooth through metal crown or space maintainer.5- A single vital canal in association with non vital canals.
False negative results may be due to:
Near exfoliation time due to reduced pulp neural element.
Post traumatic temporary parathesia.
Serial post trauma testing are needed to reveal progress of pulp health.

Thermal pulp test
It is done by applying :- hot items or cold items
HOT ITEMS
Hot gutta percha sticks on a moist or Vaseline coated tooth surface (mid buccal).
COLD ITEMS
Cotton pellet socked with ethylchloride.
Ice stick in an anesthetic carpule.

Normal teeth respond to thermal changes, especially to cold, with pain that disappears when the stimulus is removed.

Persistence of pain, after removal of the stimulus, whether it is cold or heat, is indication of irreversible pulpitis.
Exposure site
It is important in diagnosing the extent of inflammation in an exposed pulp:
If during the removal of the last bits of caries, the pulp was exposed while the periphery of exposure shows sound dentine and there is little or no hemorrhage, there is a possibility that the exposure is mechanical and the pulp shows no or limited inflammation at the exposure site.

If during the removal of the last bits of carious dentine with a spoon excavator, a large pod of caries was removed exposing the pulp and the periphery of the exposure still shows carious dentine, the tooth must be diagnosed as pathologically exposed with a pulp in an advanced stage of degeneration.

Exposure size
a true carious exposure is always accompanied with pulpal inflammation.
A pinpoint carious exposure may have varying degrees of pulpal inflammation (minimal, extensive to total necrosis)
A massive exposure always causes a widespread inflammation or necrosis and the tooth is therefore not suitable for any form of vital pulp therapy except in young permanent teeth with incomplete root development.
IV Radiographic interpretation:
A recent periapical or bitewing x-ray film must be available.
Check the following:
Presence of succedanous toothRoot resorptionThe depth of caries; carious lesions near the
pulp require some types of pulp protection or treatment.
Deep restorations close to a pulp horn.Successful or failing previous pulpotomy or
pulpectomy.
The proximity of carious lesion to the pulp cannot be determined from a radiograph.
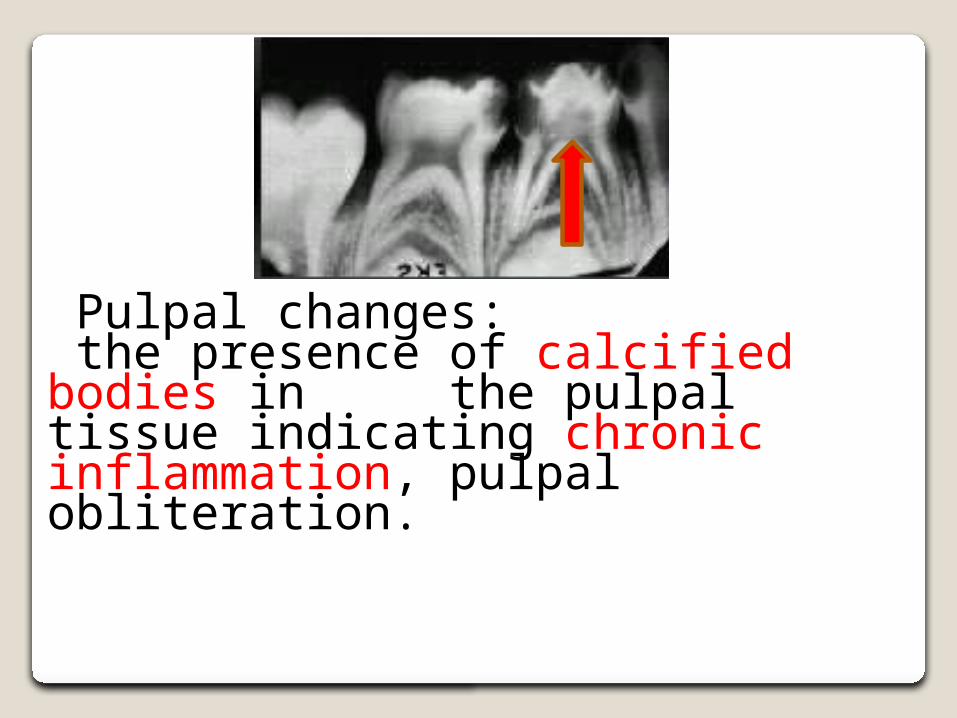
Pulpal changes: the presence of calcified bodies in the pulpal tissue indicating chronic inflammation, pulpal obliteration.

The supporting structures
The integrity of the lamina dura. Widening of periodontal space.
periapical rarefactions.

Bifurcation radiolucencies caused by degenerative breakdown of the pulp and spread of infection into bone.
Treatment: if the tooth is mobile, extraction if bone resorption is minimum, RCT
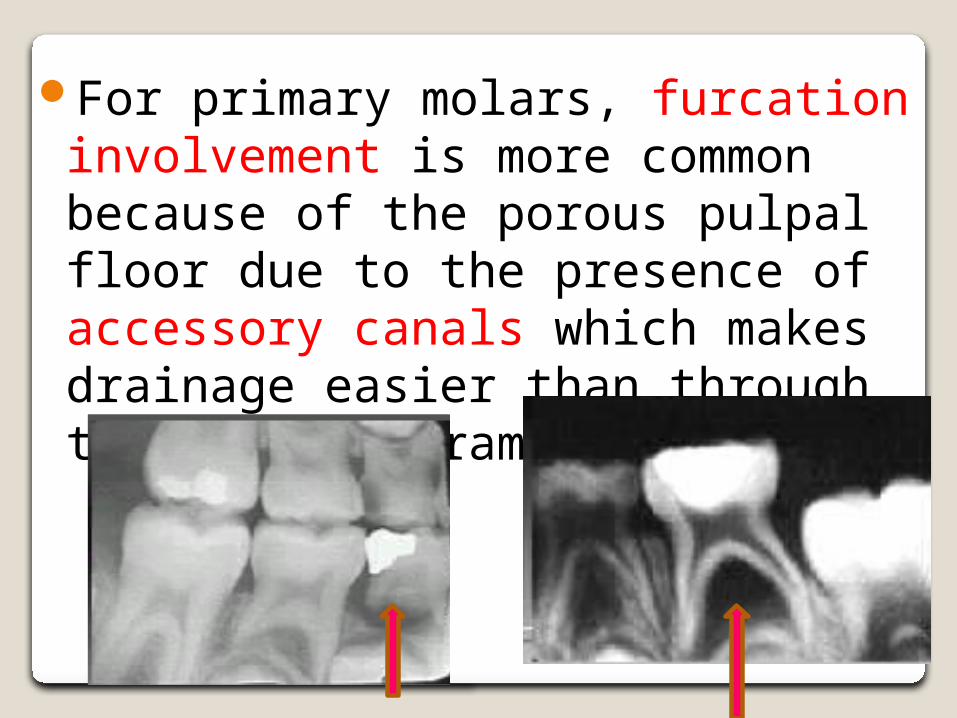
For primary molars, furcation involvement is more common because of the porous pulpal floor due to the presence of accessory canals which makes drainage easier than through the apical foramina.

Pathologic external root resorption caused by pulpal degeneration and inflammation of supporting structure.Treatment: Pulpectomy or extraction
Internal root resorption caused by chronic inflammation or exposure treated by calcium hydroxide.Treatment:If severe pulpotomy is contraindicated.Extraction is recommended
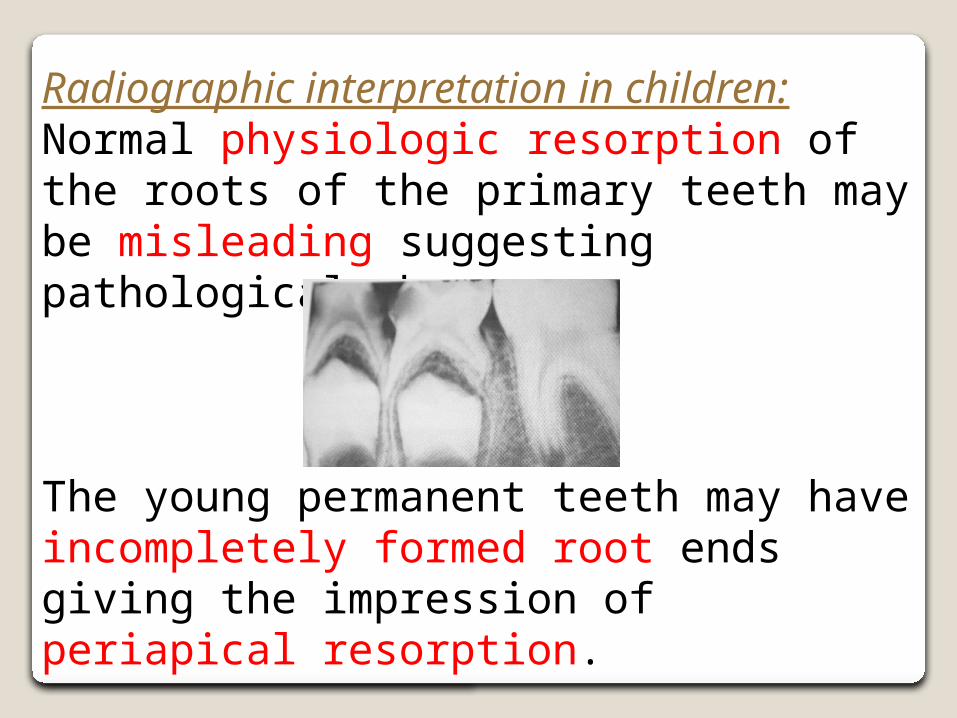
Radiographic interpretation in children:Normal physiologic resorption of the roots of the primary teeth may be misleading suggesting pathological changes.
The young permanent teeth may have incompletely formed root ends giving the impression of periapical resorption.
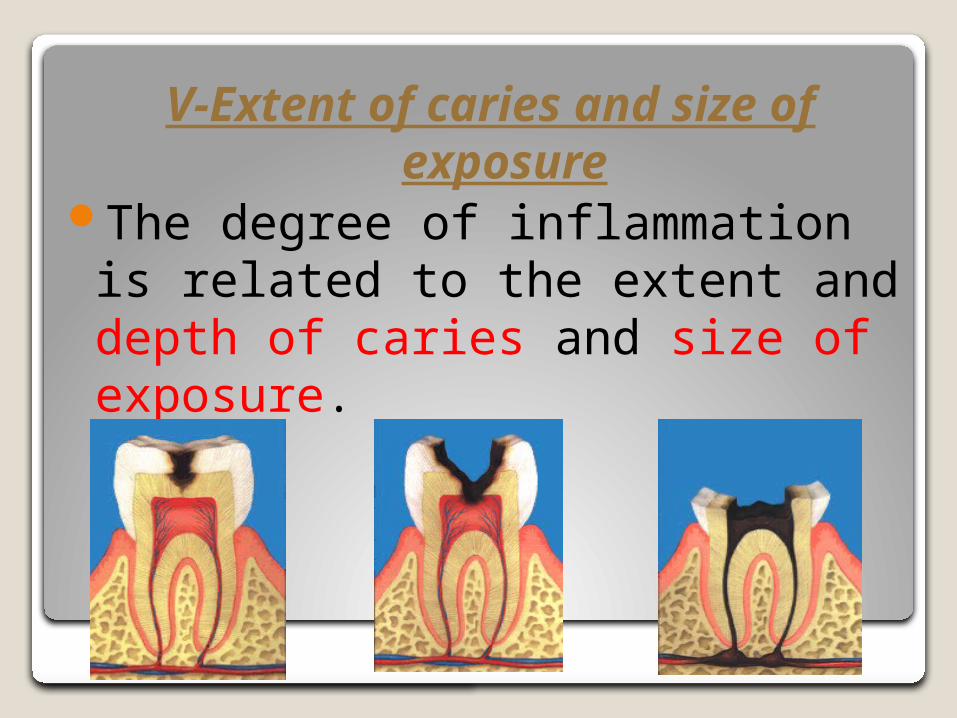
V-Extent of caries and size of exposure
The degree of inflammation is related to the extent and depth of caries and size of exposure.

VI-Character of hemorrhage:
Bleeding that can be easily arrested with moistened cotton pellets is an indication of pulp vitality.
Profuse Bleeding Highly inflamed pulp.
No Bleeding Degenerating pulp.
The presence of Pus Non vital necrotic pulp.
Clinical implication of hemorrhage:


The most difficult aspect of pulp therapy is to determine the health of the pulp or its stage of inflammation.
Pulp treatment procedures can be classified into two categories
1.Conservative: which includes approaches that aim at maintaining pulp vitality (vital pulp therapy).
2.Radical: including pulpectomy and root canal filling (non vital pulp therapy).
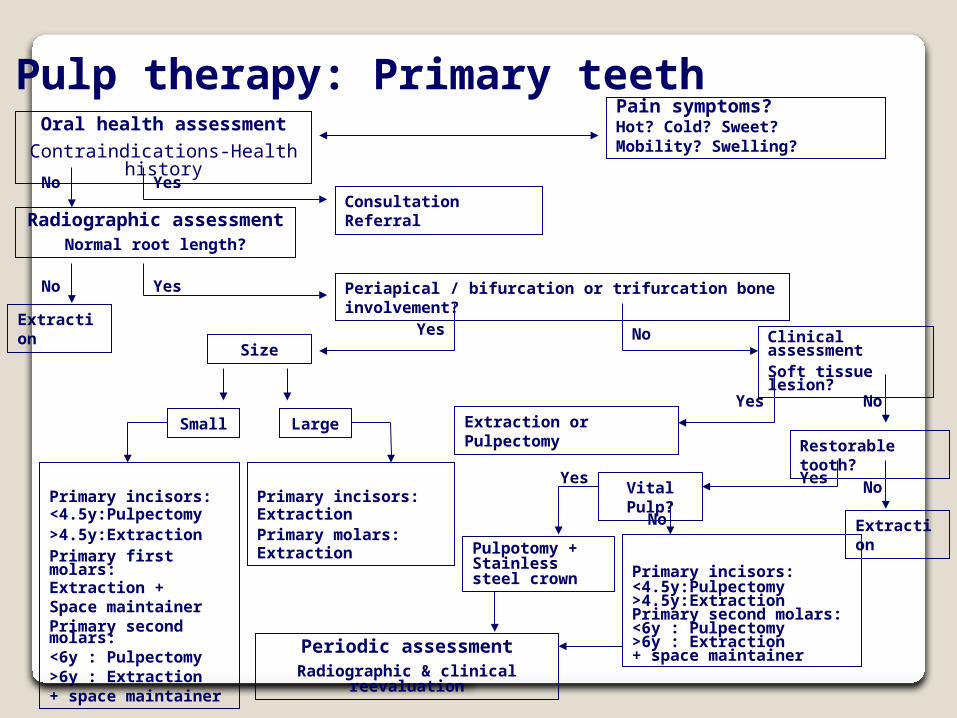
Oral health assessment
Contraindications-Health history
Pain symptoms?Hot? Cold? Sweet? Mobility? Swelling?
Radiographic assessmentNormal root length?
Yes
Consultation Referral
Extraction or Pulpectomy
Clinical assessmentSoft tissue lesion?
No
No Yes
Periapical / bifurcation or trifurcation bone involvement?
ExtractionYes No
Size
Small Large
Primary incisors:<4.5y:Pulpectomy>4.5y:ExtractionPrimary first molars:Extraction +Space maintainerPrimary second molars:<6y : Pulpectomy>6y : Extraction+ space maintainer
Primary incisors:ExtractionPrimary molars:Extraction
Yes
Restorable tooth?
No
No
Extraction
YesVital Pulp?
Primary incisors:<4.5y:Pulpectomy>4.5y:ExtractionPrimary second molars:<6y : Pulpectomy>6y : Extraction+ space maintainer
No
Yes
Pulpotomy + Stainless steel crown
Periodic assessmentRadiographic & clinical reevaluation
Pulp therapy: Primary teeth

Oral health assessment
Contraindications-Health history
Pain symptoms?Hot? Cold? Sweet? Mobility? Swelling?
Radiographic assessmentPossible carious exposure
Yes
Consultation Referral
No
No Yes
Periapical pathosis
Routine operative procedure or small mechanical exposure Ca(OH)2 + restoration
Yes
Pulp therapy: Permanent teeth
Open Apex?
Yes
No
No
Clinical Assessment Carious lesion- Possible exposure?
Apexification Root canal therapy
Root canal therapy
Yes No
Restorable tooth? Routine operative procedure Ca(OH)2 + restoration
Yes
No
Extraction space maintainer
Indirect pulp therapy:Remove deep cariesNo pulp exposure!Ca(OH)2 + interimRestorative material + restoration
Periodic assessmentRadiographic & clinical reevaluation