go with the flow: the development of a rescue ecls program · technology to a tertiary-care...
TRANSCRIPT

Go with the Flow: The Development of a Rescue
ECLS Program
Tanya Spence RN MNClinical Nurse Specialist PICU
tanya spence@ahs ca

ObjectivesAlberta Children’s Hospital (ACH)What is it?
– Brief review of Extracorporeal Life Support (ECLS) – Introduce the equipment and techniques used to provide
safe, effective ECLS
What does it mean for our hospital?– Introduction of our rescue ECLS program– How it came to be, what its introduction entailed and
what patients have participated in our program to date
*We have permission to include patient pictures throughout this talk.

What exactly is ECLS?■ Extra Corporeal Life Support = ECLS
■ A therapy for patients with acute life-threatening reversiblerespiratory or cardiac failure who are not responding to maximal ventilatory, medical and surgical treatment
■ It is a temporary lung and/or heart support system which can be used on newborns, children and adults
■ Modified form of cardio-pulmonary bypass
■ ECLS is their one last chance to survive

What exactly is ECLS?
ECLS = ECMO V-A ECLS – heart and lung supportV-V ECLS – lung support only
ECPRPlacing a patient on ECLS when they are
actively undergoing CPR

Veno-Arterial ECLS (VA)
ECLS
Blood taken from systemic venous system
(deoxygenated, venous blood)
Blood returned to systemic arterial system
(oxygenated, arterial blood)

Veno-Venous ECLS
ECLS
Blood returned to systemic venous system
(oxygenated, arterial blood)
Blood taken from systemic venous system (deoxygenated, venous blood)

The ECLS circuit
Venous line drains to a pump
Pump generates a Blood Pressure and sends blue blood to an oxygenator
Red (oxygenated) blood is returned to the patient

Who requires ECLS?
In general 4 reasons to cannulate:
– Bridge to recovery *– Bridge to transplant– Bridge to Ventricular Assist Device (VAD)– Bridge to decision **important for families

Why are we unique?
ACH is a non-cardiac children’s hospital which means no pediatric cardiac surgeons or perfusionists
ACH is a free standing children’s hospital therefore no easy access to adult CV team
General surgeons cannulate
OR/surgery are not in house 24/7
Requirement to maintain competency for a high risk low volume life saving procedure
*Only rescue program we can find internationally
Sister program is at the Stollery Children’s Hospital in Edmonton

Why an ELCS program?■ Upon review of cases, it was determined that
some children passed away in Calgary that would have had ECLS as an option in other centres.
■ Kids with – Congenital heart disease– Myocarditis– Sepsis– Other (sand aspiration!!)
■ We estimated 8-10 cases per year
Lets be honest, this was not on our list BUT it has been one of the indications for ECLS!
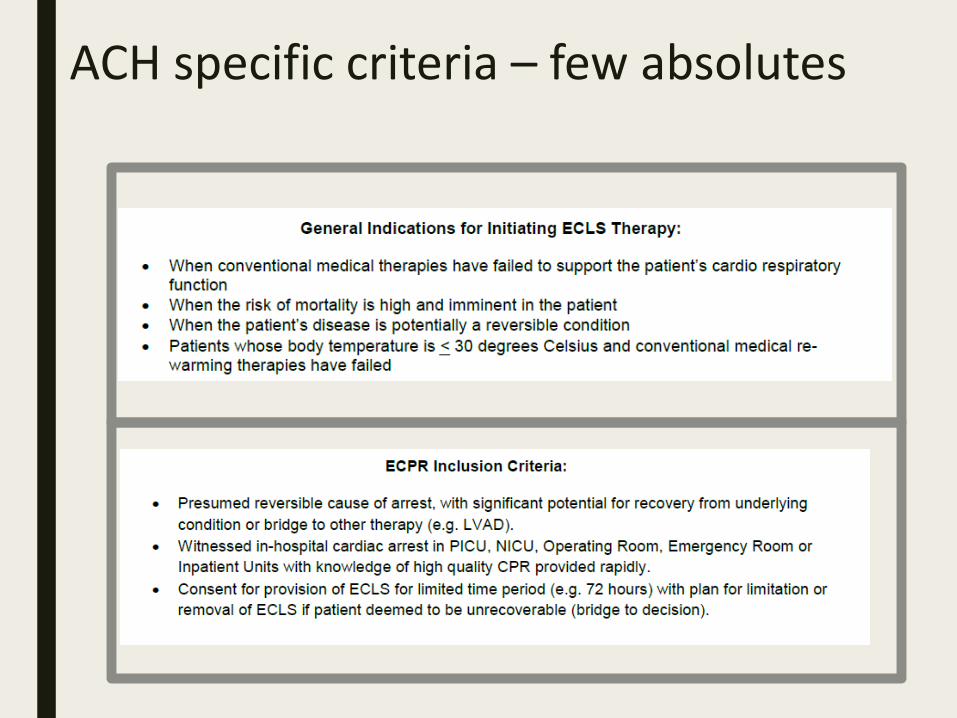
ACH specific criteria – few absolutes

ECPR AHA/PALS Guidelines“E-CPR may be beneficial for infants and children with cardiac arrest if they have heart disease amenable to recovery or transplantation and the arrest occurs in a highly supervised environment such as an ICU with existing clinical protocols and available expertise and equipment to rapidly initiate”
There is insufficient evidence for any specific threshold for CPR duration beyond which survival with ECPR is unlikely.
ECLS Program Live Oct 2011

“The institution of ECLS in any hospital requires commitmentat all levels of administration and practice, specialized equipment and supplies, carefully defined clinical protocols, and training in the animal laboratory.”
Setting up the Program
An Introduction to Extracorporeal Life Support
Joseph B. Zwischenberger, MD and Robert H. Bartlett, MDhttp://www.med.umich.edu/ecmo/about/what.html

ECLS/ ECPR: who is involved?Expert team■ PICU MD■ Bedside RN + RT
– Manage patient■ General surgeon■ Perfusionist (adult)■ ECLS specialist
– Prepare and initiate ECLS■ Cardiology
Support team■ OR nurses
■ Blood bank
■ X-ray techs
• Unique partnership with adult perfusionists• Transfer to Stollery within 24 hours

Educational Curriculum
Didactic / Hands on Training– ECLS Specialists get a 4 day intensive
training course and annual educationAnimal / Wet labs
– Using sheep and pig modelsECLS / ECPR Simulations
– Run in situ – PICU/OR/ER/Inpatient unitsDebrief Sessions

Simulation – Our Foundation
Pt blood volume reservoir
Low fidelity cannulation doll
Pt monitor
Hidden highfidelity doll



So many checklists!

Practice makes perfect…

Team ‘buy in’ is so important

EVALUATING THE INTRODUCTION OF EXTRACORPOREAL LIFE SUPPORT TECHNOLOGY TO A TERTIARY-CARE PEDIATRIC INSTITUTION: SMOOTHING THE LEARNING CURVE THROUGH INTER-PROFESSIONAL SIMULATION TRAINING
Carlos F. Sánchez-Glanville MD,, Jaime Blackwood MD, Mary Brindle MD, Tanya Drews MD, Steve Menzies CPC, Tanya Spence RN, Steven Lopushinsky MD.
CAPS edition of Journal of Pediatric Surgery May 2015

Staged implementation approach■ PICU 2011
■ PICU ECPR 2012
■ ED 2013
■ OR 2014
■ NICU 2016
■ Inpatient units 2017
* All children at ACH now have the same access to ECLS

Comprehensive QI program
■ A debrief is held for all cases at ACH
■ If ECPR then the CPR feedback is reviewed
■ Joint case review sessions with the Stollery Children’s Hospital
■ Development of a long term follow up program in partnership with the neuro critical care program.
Our data 2011-201896 total activations of the ECLS team
49 activations did not result in cannulation for various reasons
47 patients have been cannulated– 40 patients for VA (11 patients classified as ECPR)– 7 patients for VV

Our indicationsVA■ 36 for VA
– ECPR 11– CHD 3– Myocarditis 4– Cardiomyopathy 2– Cardiogenic shock 3– Other 13
■ 4 VV to VA– Viral pneumonia 2– Hantavirus 1– ARDS 1
VV■ 7 VV
– Sand aspiration 1– Viral pneumonia 2– Bacterial pneumonia 1– Respiratory Failure 3
Ages range from 34 weeks to 17 years

11 year old boy– Sand Aspiration Fernie BC– Digging hole at bottom of sand dune, sand dune
collapsed. Immersed for 5 mins before dad able to dig him out.
– Intubated and transported by STARS. Difficult to oxygenate and ventilate.
– Direct admit to PICU

– Cannulated for VV ECLS due to severe hypoxemia and hypercarbia
– ENT thereafter able to scope and clear airway (ACH and Stollery)
– Decannulated day 3, extubated day 6, D/C home back to baseline day 12
Sand Bronchogram!

4.4 kg 1 month old babe– Presented to Lethbridge in shock– Intubated and transported by Pediatric transport
team and STARS.– Babe unstable throughout transport with
refractory tachycardia/arrhythmia, hypotension, poor perfusion, continued when arrived at ACH.
– ECLS page send within 30 mins of arrival– Cannulated for VA ECLS due to refractory
cardiogenic shock (secondary to arrhythmia)– Decannulated day 3 (after established rhythm
control), discharged home after 15 days no major sequalae

13 year old 42 kg boy– Admitted to Lethbridge with pneumonia– Transported on NIV by Pediatric transport team
via fixed wing– Immediately intubated on arrival to ACH PICU
and placed on HFOV. Unable to oxygenate or ventilate.
– Cannulated for VV, converted to VA ECLS b/c of worsening hemodynamic instability
– Diagnosis = Hantavirus!

5 year old boy– Fell from 4 feet and pulled a 50lb object onto chest– Initially very stable - EMS to ACH – Deteriorated shortly after arrival to ACH, intubated
and ventilated, quickly needed HFOV. – Initial echo: mildly concerning RV dilation and
↓function– Repeat echo: large apical VSD with large L to R shunt,
progressive dilation of RV and poor biventricular function.

Cannulated for VA ECLSTransferred to Stollery where he had definitive surgery (closed VSD)Discharged home POD 9 back to baseline

Our outcomes
■ 42/47 pts were transferred to Stollery– Two withdrawn b/c severe neuro injury– Two withdrawn b/c inability to achieve flows– One cannula dislodged, unable to place again
■ Overall 35/47 survivors(74%)■ 11 patients (25%) ECPR
– 5/11 survived (45%)As a rescue ECLS program we currently
cannulate children here at ACH, thereafter our partner program (Stollery Children’s Hospital) retrieve the cannulated patients and transport
them to Edmonton to complete their run.
Extracorporeal Life Support Organization (ELSO)
■ International consortium of health care professionals and scientists
■ Primary mission of the Organization is to maintain a registry of the use of extracorporeal life support in active ELSO centers.

To put this in perspective ■ The survival rate for children to be discharged home
who have received ECLS is between 41% and 57% according to ELSO
■ ACH has a current survival rate for children being discharged home of 74% (all comers), 45% (ECPR)
July 2018 report

– ECLS is a complex life saving therapy that is constantly evolving
– Low volume high risk procedure for our institution that requires constant skill maintenance
– These patients have no other options– We are good at it! And argue others internationally
should adopt a similar model
Conclusions
Special thanks to the Alberta Children’s Hospital Foundation and our community

Logan, 1 day oldPulmonary Hypertension
Benicio, 2 years oldRespiratory Failure
Liam, 18 months oldPulmonary Hypertensive Crisis
Payton, 3 years old Sepsis
Madison 21 months oldRespiratory Failure