glucocorticoid-induced osteoporosis (gio) nguyen thy khue, md, phd department of endocrinology,...
TRANSCRIPT
Glucocorticoid-Induced Osteoporosis (GIO)
Nguyen Thy Khue, MD, PhD
Department of Endocrinology,
HoChiMinh City University of Medicine and Pharmacy
Epidemiology of GIO
• Prevalence of oral glucocorticoid use ~1% of the adult population1
2.5% in individuals aged 70-79
• Up to 350,000 individuals in UK at risk of fractures due to glucocorticoid use
(Van Staa TP et al, 2000)

GC in developing countries
• Prevalence: unknown.
• Glucocorticoid can be purchased over the counter.
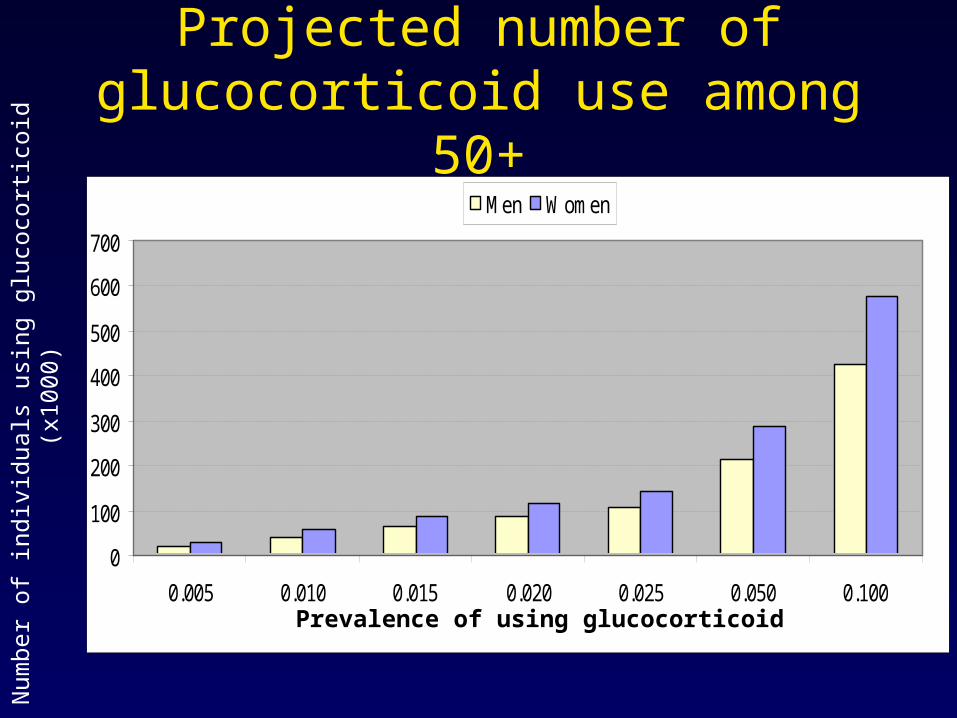
Projected number of glucocorticoid use among 50+
0
100
200
300
400
500
600
700
0.005 0.010 0.015 0.020 0.025 0.050 0.100
Men Women
Prevalence of using glucocorticoid Num
ber
of in
divi
dual
s us
ing
gluc
ocor
ticoi
d (
x100
0)

Mechanism of Corticosteroid Induced Osteoporosis
(Segal L G et al. 1997)D1202
Osteoporosis
Osteoblastbone
formation
PTH?
Effects ongrowth hormones& growth factors
gastrointestinalcalcium absorption
urinary calciumexcretion
calcium
Corticosteroids
osteoclastbone resorption
Sex hormone effects: adrenal androgens
oestrogen
testosterone
musclemass
-6.0%
-5.0%
-4.0%
-3.0%
-2.0%
-1.0%
0.0%
3 6 9 12
*
*
*
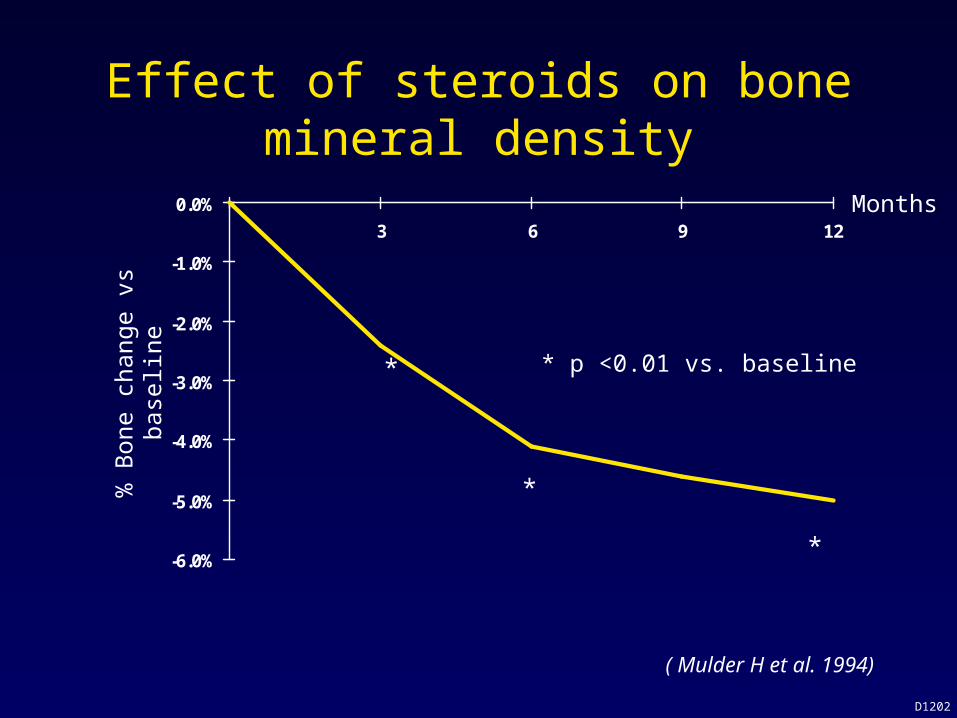
* p <0.01 vs. baseline
Effect of steroids on bone mineral density%
Bon
e ch
ange
vs
base
line
( Mulder H et al. 1994)
D1202
Months
Factors associated with fracture risk with GC Rx
• Age• BMD
– Initial & subsequent to GC Rx.– Postmenopausal women – highest risk.
• Glucorticoid dose: cumulative & mean daily dose.
• Duration of exposure.• Underlying diseases.

Fracture type and the use of Glucocorticoid
Fracture type Gender Corticosteroid use
Prior fracture
Any fracture M 1.7 (1.1–2.5) 1.7 (1.4–2.1 )
F 1.4 (1.2–1.6) 1.7 (1.6–1.9)
Osteoporotic
fracture
M 2.2 (1.4–3.3) 1.7 (1.4–2.1)
F 1.4 (1.2–1.7) 1.7 (1.6–1.9)
Hip fracture M 2.6 (0.9–7.5) 1.7 (1.0–2.9)
F 2.1 (1.4–3.1) 1.7 (1.3–2.1)
(Kanis JA, et al, 2004)
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
0.020 0.025 0.050 0.100
Men Women
0
500
1000
1500
2000
2500
3000
0.020 0.025 0.050 0.100
Men Women
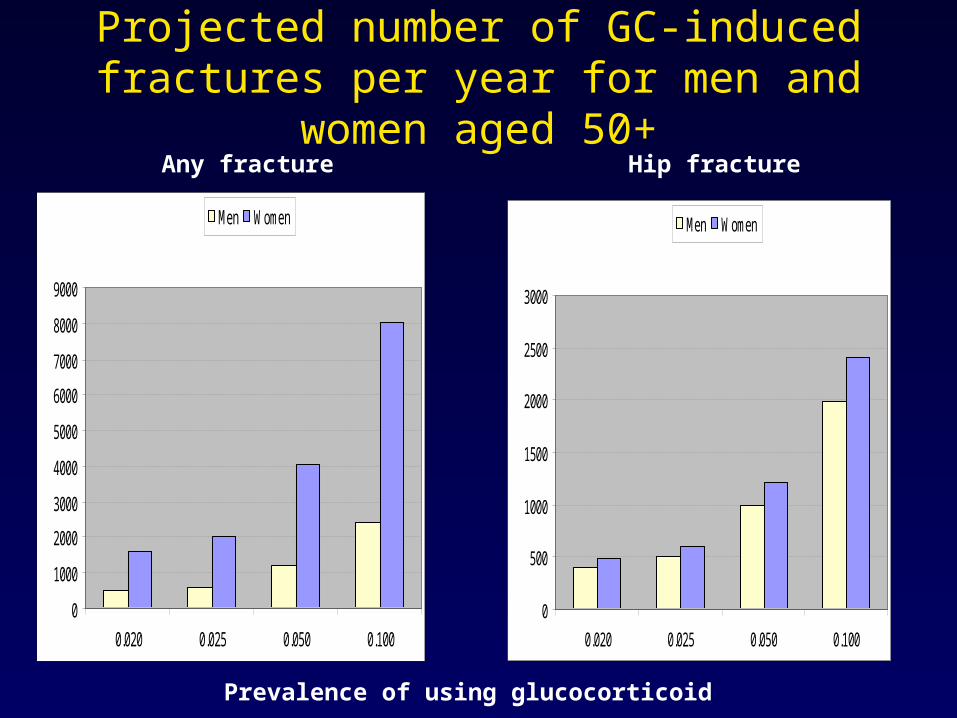
Projected number of GC-induced fractures per year for men and women aged 50+
Prevalence of using glucocorticoid
Any fracture Hip fracture

Incidence of non-vertebral fractures (per 100 p-yrs) in women
(van Staa et al, 2000)
0
1
2
3
4
5
6
7
8Control< 2.5mg
2.5-7.5mg>7.5 mg
18-34 35-44 45-54 55-64 65-74 75-84 > 85
Age (years)
244.235 oral GC users244.235 controls58.6% female
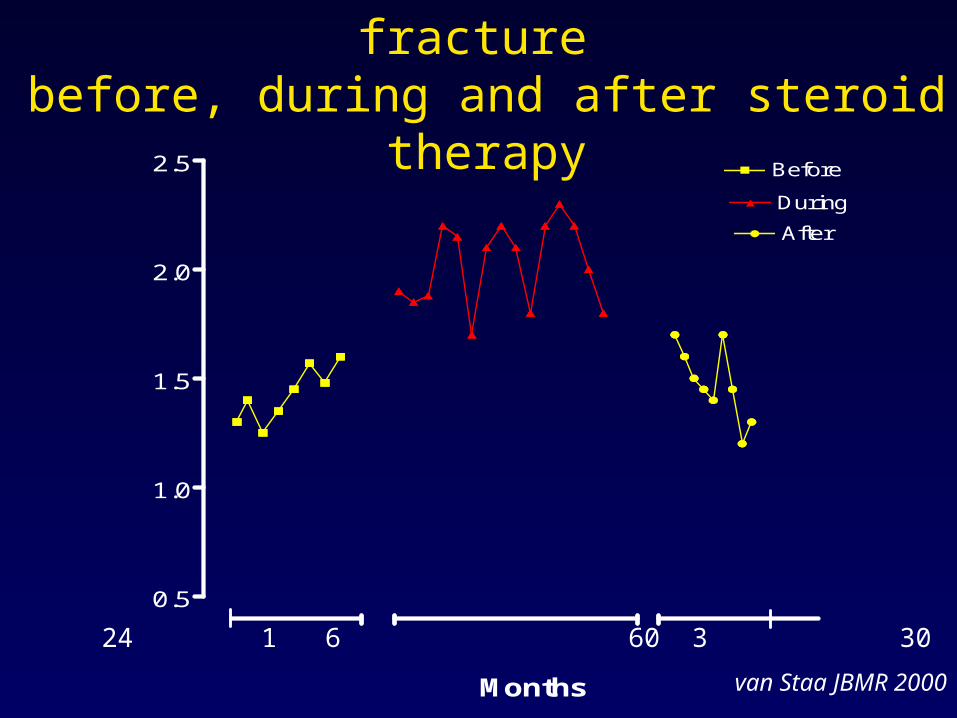
Incidence of non-vertebral fracture before, during and after steroid therapy
0.5
1.0
1.5
2.0
2.5 Before
During
After
Months
24 1 6 60 3 30
van Staa JBMR 2000

3 to 6months
Time 3 to 6months
Bone Strength
Steroid therapy
A + B C D + E
A = osteocyte apoptosis C = accumulation of D = fast repair of defectsB = fast bone loss unrepaired defects E = restoration of osteocytes
(Manolagas et al, 2000)
Treatment of GIO
• Primary prevention– Most rapid bone loss within 1st 6 – 12 months
of Rx
• Secondary prevention
Prevention of Glucocorticoid -induced bone loss
• Use lowest dose GC possible.
• Minimise lifestyle risk factors: quit smoking.
• Individualised exercise programmes.
• Drug Rx.
Drug treatment of osteoporosis
• Anti-resorptives:– Bisphosphonates– HRT/SERMS– Calcitonin
• Anabolics:– Teriparatide– Strontium ranelate
• Calcium & Vitamin D for all patients


GC doses ~ Prednisone >5mg/d for > 3 mo
Additional Risk Factors
· Postmenopausal
· Male > 50 y
· Low weight
· Prior fracture
· High dose of prednisone (>10mg/day)
· Underlying disease with rapid bone loss
. Immobilized due to underlying disease
. Low calcium intake
· Family history of osteoporosis
CLINICALPRESENTATION
BMD
MANAGEMENT
(Sambrook PN)
Calcium and vitamin DRepeat BMD in 12 months if GC therapy ongoing.
T-scores ≥ –1.0
Therapy to prevent bone loss
First line:
Oral or IV bisphosphonates
Adjunctive or 2nd line therapy: Calcium and vitamin D
- 2.5 <T-scores
≤ –1.5
Consider
T-scores ≤ –2.5
Commence
Cost of treatment
• Bisphosphonates (alendronate): $280 per patient/year
• Individuals age 50+ using GC: ~ 1M (based on 10% of prevalence of using GC)
• Number of fractured cases reduced: 5240
• Treatment cost for prevention of one fracture: 53,579 USD
Summary
• Glucocorticoids widely used in clinical practice.
• >7.5mg/day Pednisone for >3-6 m of therapy, but no absolute cutoff below which GC treatment safe.
Summary
• Rapid bone loss (3-6 months) early prevention.
• Consideration for prevention:– fracture risk assessment – Effect of underlying disease – Effect of GC and other drugs on skeleton
• Bisphosphonates the mainstay of therapy.
