glaucoma update 2016 - california optometric glaucoma update.pdf · glaucoma update 2016 michael...
TRANSCRIPT

Glaucoma Update 2016
Michael Chaglasian, OD 1
Glaucoma Update:New Tools and Treatment Options
Michael Chaglasian, OD, FAAOChief of Staff, Illinois Eye Institute
Associate Professor, Illinois College of Optometry
Disclosure
• Michael Chaglasian, O.D. is a paid advisor, consultant or researcher for the following commercial/industry groups:
– Allergan, Alcon Labs, Bauch+Lomb, Carl Zeiss Meditec, Topcon Medical, Heidelberg Engineering, Reichert
Ocular Hypertension
• What is this condition?
• Who has OHTN?
• What are the risk factors?
• Who should be treated for OHTN?
• Is treatment beneficial?
• How should these patients be followed?
Ocular hypertension is a condition in which the following criteria are met:
• An intraocular pressure greater than 21 mm Hg in one or both eyes, as measured by applanationtonometry on 2 or more occasions
• Absence of glaucomatous defects on visual‐field testing
• Normal appearance of the optic disc and nerve fiber layer
• Anatomically normal, open angles on gonioscopy• Absence of ocular conditions contributing to the elevation of pressure, such as narrow angles, neovascular conditions, and uveitis
www. http://ohts.wustl.edu/index.html
Ocular Hypertension
119 million people in US over age 40 (Census 2000)
4%‐8% of people in the United States over age 40 (4.8 – 9.5 million people) have OHT
The number of affected people will increase with the aging of the population
Managing this large group of people is associated with substantial costs for examinations, tests and treatment
www. http://ohts.wustl.edu/index.html
CASE AC
• 53 year old
• Myopia, no sig. medical history
• No family history glaucoma
• GAT= 27 OD 25 OS
• Gonioscopy= Open to CB 3600 OU
CASE AC:IOP 27 OD; 25 OS
Visual Fields Treat or Observe?

Glaucoma Update 2016
Michael Chaglasian, OD 2
Risk Assessment in Clinical PracticeGlaucoma Risk Factors
Evidence Based Age:
– Most commonly occurs after age 60 (risk increases with age)
– Earlier in those with a Family History
Race: – African, Hispanic, Asian
Family history– First degree relatives (OR 2.9; Tielsch et al)
Elevated Intraocular pressure
Other ocular factors:– Thin central corneal thickness, narrow angles, increased cup:disc
ratio, exfoliation
Systemic factors:– Low Perfusion Pressure, hypotension
Genetic factors:
The Ocular HypertensionTreatment Study
Does Treatment of Ocular Hypertension Prevent POAG?
Investigator Protective
Graham no
Norskov no
Levine no
David et al. no
Chisholm no
Schulzer et al. no
Heijl et al. no
Kamal et al. no
Miglior et al. no
Investigator Protective
Becker & Morton yes
Shin et al. yes
Kitizawa yes
Epstein et al. yes
Kass et al. yes
Limitations of previous studies: Varying endpoints
Limited treatment regimens
Small sample size
March 2010
Ocular Hypertension Treatment Study (OHTS)Primary Goals
Evaluate the safety and efficacy of topical ocular hypotensive medication in delaying or preventing the development of POAG in individuals with elevated IOP
Identify baseline demographic andclinical factors that predict whichparticipants will develop POAG
Kass, et al. 2002
The OHTS Entry Criteria
Age 40 - 80
Normal visual fields Humphrey 30-2
Normal optic discs
Untreated IOP: 24 to 32 mm Hg in one eye
21 to 32 mm Hg in fellow eye
Kass, et al. 2002
June, 2002
Primary POAG Endpoints*Log Rank P-value <0.001, Hazard Ratio 0.40, 95% CI (0.27, 0.59)
*through 8 Nov 2001
Pro
port
ion
PO
AG
Medication Observation
Months
Medication reduced incidence of POAG in OHT participants by more than 50% at 5 years from 9.5% in the Observation Group to 4.4% in the Medication Group.
Baseline Predictive Factors for the Development of POAG
Age
IOP
Vertical C/D Ratio
PSD
CCT
OHTS/EGPS,2007
Pachymetry

Glaucoma Update 2016
Michael Chaglasian, OD 3
POAG Endpoints by Central Corneal Thickness and Baseline IOP (mmHg) in Observation Group*
OHTS Data
Baseline IOP (mmHg)
Central Corneal Thickness (microns)
* through 8 Nov 2001
< 23.75
>23.75 to < 25.75
>25.75
< 555 >555 to < 588 >588
17% 9% 2%
12% 10% 7%
36% 13% 6%
Risk Factors
Self-identified race not significant predictor of POAG in a multivariate model.
Race not significant when central corneal thickness and baseline cup-disc ratio included.
Age Decade OHTS
EGPS
DIGS
OHTS-EGPS
IOP (mm Hg) OHTS
EGPS
DIGS
OHTS-EGPS
CCT (40 µm decrease) OHTS
EGPS
DIGS
OHTS-EGPS
PSD (per 0.2 dB increase) OHTS
EGPS
DIGS
OHTS-EGPS
Vertical CD ratio OHTS
EGPS
DIGS
OHTS-EGPS
Multivariate Hazard Ratios for Predictors of POAG OHTS Observation group, EGPS Placebo group, DIGS and OHTS/EGPS
OHTS/EGPS 2007
How to Manage OHTN?
OHTS/EGPS, 2007
Using the OHTS/EGPS Prediction Model for the Development of POAG
Available on web free of charge
http://ohts.wustl.edu/risk
OHTS / EGPS Risk Calculator
http://ohts.wustl.edu/risk/calculator.html
Pachymetry: 3 Outcomes
Thin: <555 µ High Risk
Average: 555-588 µ No change in Risk
Thick: >588 µ Low Risk
The predictions derived using these methods are designed to aid, but not to replace clinical judgment.
Risk Calculator Limitations
A number of factors described as predictive in previous studies either did not add to the explanatory power of the OHTS–EGPS pooled model or were not assessed in this study. These include:
1. Disc Hemorrhages2. Ocular Perfusion Pressure3. Family History of glaucoma4. Ocular Perfusion Pressure5. Life Expectancy:
much higher lifetime risk for younger pts
Why Not Treat Everyone?
Costs of Therapy:– Monetary costs
» Number Needed to Treat from OHTS = 20
» Overall impact to healthcare system and to the patient personally
– Side Effects» Minor for most but should not be ignored
– Quality of Life Costs

Glaucoma Update 2016
Michael Chaglasian, OD 4
How to Incorporate Information From OHTS Into
Clinical Practice?
March 2010
Managing OHTN
Most OHT patients are at low risk. Many low risk OHT patients can be followed without medication.
Delaying treatment for 7.5 years resulted in only a small absolute increase in POAG in low risk participants.
Starting treatment of POAG at diagnosis has no major negative effect on prognosis over 5 years.
March 2010
High risk OHT patients may benefit from more frequent examinations and early
treatment taking into consideration:
Patient age Health status Life expectancy Personal
preference
Follow these Patients More Closely– Frequent VFs
» 10-2
– OCTs
– ONH examination
March 2010
Taking Glaucoma risk assessment to the next level:
THE ROLE OF CORNEAL HYSTERESIS
Ocular Response Analyzer
(Reichert)
Michael Chaglasian, ODIllinois Eye Institute Illinois College of [email protected] 1. Glass DH et al. Invest Ophthalmol Vis Sci. 2008;49:3919‐3926.
2. Wells AP et al. Invest Ophthalmol Vis Sci. 2008;49:3262‐32683. Taylor DA et al. Corneal Biomechanics. In: Copeland RA Jr., Afshari NA, eds.: Copeland and Afshari’s Principles and Practice of
Cornea. Two Volume Cornea Textbook. Jaypee Brothers. 2012:148‐157.
Section 1: Introduction to Corneal HysteresisBioengineering of the Eye: Emerging Concepts
Viscoelastic tissue with complex, interconnected microstructure1
Geometrical attributes are not a surrogate for biomechanical properties1
• eg: CCT does not describe viscoelasticity
The eye appears to be a mechanical structural continuum2
• Tissue properties may provide additional diagnostic information3
37
©2002 Park et al. Invest OphthalmolVis Sci.
1. Vincent J. Basic elasticity and viscoelasticity. In: Vincent J, ed. Structural Biomaterials. 3rd ed. Princeton, NJ: Princeton University Press; 2012:1‐28.
2. PubMed Search for “hysteresis” on October 3, 2014 returned 7696 results. 3. Hjortdal JO1. On the biomechanical properties of the cornea with particular reference to refractive surgery. Acta Ophthalmol Scand Suppl.
1998;(225):1‐23.
Section 1: Introduction to Corneal HysteresisHysteresis: Not a New Concept
A measurement that characterizes response to application and removal of force (load/unload)1
• Found in materials or systems that do not instantly follow forces applied to them but react slowly, or dissipate a portion of the applied energy 1
More than 7500 papers published on hysteresis in a variety of medical fields2
• Various tissues and structures (tendon, lung, arteries, etc)
• The importance of Corneal visco‐elasticity had been discussed and explored (EX‐VIVO)prior to the ORA3
39
Classic “Hysteresis Loop”Sir James Alfred Ewing Identified the phenomenonof hysteresis and coined theterm in 1890
Hysteresis Property:“More like a Shock Absorberand NOT just a Coil Spring”
1. Luce DA. J Cataract Refract Surg. 2005;31:156‐162.2. Dupps WJ Jr. J Cataract Refract Surg. 2007;33:1499‐1501.3. Glass DH et al. Invest Ophthalmol Vis Sci. 2008;49:3919‐3926.
Section 1: Introduction to Corneal Hysteresis What is Corneal Hysteresis (CH)
The only in‐vivo measurement of corneal/ocular biomechanics• CH specifically refers to the output
of the measurement process performed by the Ocular Response Analyzer (ORA)1,2
Corneal Hysteresis reflects the ability of the corneal tissue to dissipate energy 1
• Function of viscoelastic damping2
• Not a characterization of stiffness3
Provides insight into ocular properties that were not previously understood or conceived of
40
Ocular Response Analyzer measurement signal
David Luce, PhDInvented the concept of Corneal Hysteresis
CCT is a geometrical attribute. CH is a tissue property. CCT is NOT a surrogate for corneal biomechanical (ie: bending / strength) properties. The relationship between CCT and CH is weak and non‐linear, especially when pathological eyes are included.
CCT vs. CH - 184 normal eyes
Section 1: Introduction to Corneal Hysteresis CH: Not a surrogate for other parameters (slide a)
Data courtesy New England College of Optometry
Section 1: Introduction to Corneal Hysteresis CH: Average Values in Normal Subjects
1. Fontes BM J Refract Surg. 2008 Nov;24(9):941-5. 2. Carbonaro. The Heritability of Corneal Hysteresis and Ocular Pulse Amplitude A Twin Study doi:10.1016/j.ophtha.2008.02.0113. Lam A. Et Al. Optom Vis Sci. 2007 Sep;84(9):909-144. Kamiya Et Al. J Refract Surg. 2009 Oct;25(10):888-935. Ortiz Et Al. J Cataract Refract Surg. 2007 Aug;33(8):1371-56. John Et. Al. 2007 Spring;39(1):9-14
CH Values in Normals around the world N CH*
Brazil1 105 10.1 ± 1.8
UK2272 pairs 10.2 ± 1.2
China3125 10.9 ± 1.5
Japan4204 10.2 ± 1.3
Spain5 88 10.8 ± 1.5
USA6 44 10.5 ± 1.2
*CH units are mmHg
Glaucoma Update 2016
Michael Chaglasian, OD 5
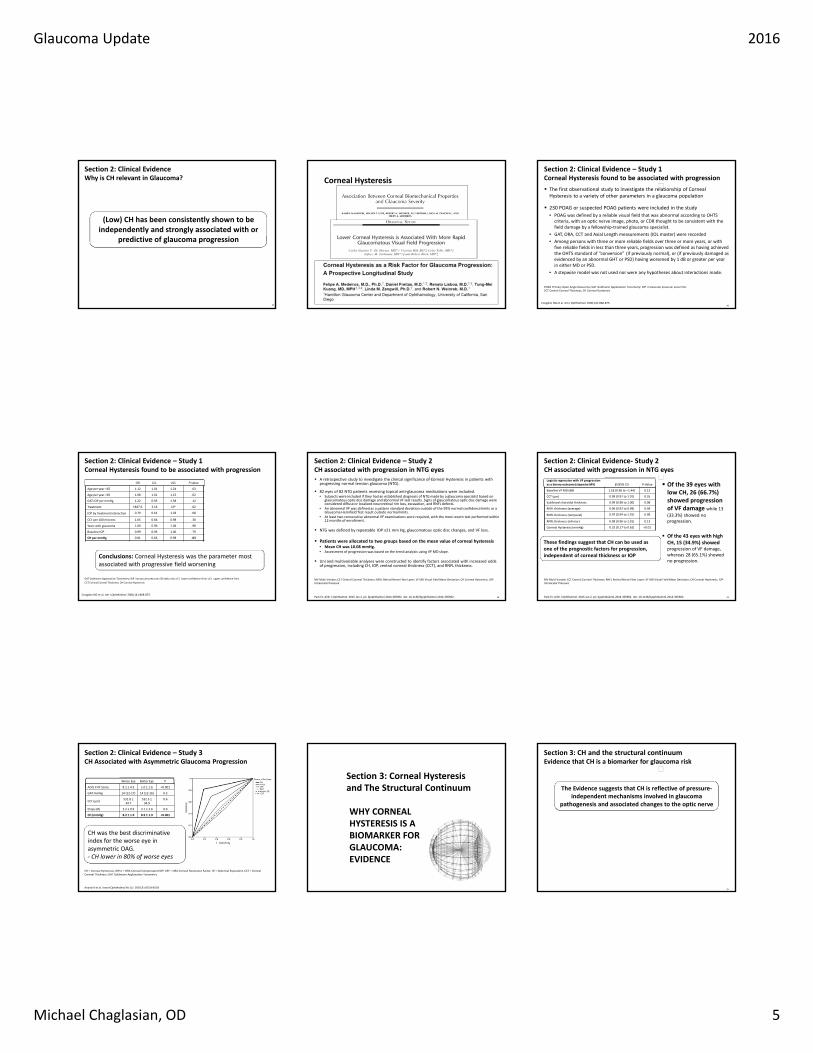
Section 2: Clinical EvidenceWhy is CH relevant in Glaucoma?
44
(Low) CH has been consistently shown to be independently and strongly associated with or
predictive of glaucoma progression
Corneal Hysteresis
Section 2: Clinical Evidence – Study 1Corneal Hysteresis found to be associated with progression
The first observational study to investigate the relationship of Corneal Hysteresis to a variety of other parameters in a glaucoma population
230 POAG or suspected POAG patients were included in the study
• POAG was defined by a reliable visual field that was abnormal according to OHTS criteria, with an optic nerve image, photo, or CDR thought to be consistent with the field damage by a fellowship‐trained glaucoma specialist.
• GAT, ORA, CCT and Axial Length measurements (IOL master) were recorded
• Among persons with three or more reliable fields over three or more years, or with five reliable fields in less than three years, progression was defined as having achieved the OHTS standard of “conversion” (if previously normal), or (if previously damaged as evidenced by an abnormal GHT or PSD) having worsened by 1 dB or greater per year in either MD or PSD.
• A stepwise model was not used nor were any hypotheses about interactions made.
46
POAG Primary Open Angle Glaucoma; GAT Goldmann Applanation Tonometry; IOP intraocular pressure; ence limit.CCT Central Corneal Thickness; CH Corneal Hysteresis,
Congdon NG et al. Am J Ophthalmol. 2006;141:868‐875.
Congdon NG et al. Am J Ophthalmol. 2006;141:868‐875.
Conclusions: Corneal Hysteresis was the parameter most associated with progressive field worsening
GAT Goldmann Applanation Tonometry; IOP intraocular pressure; OR odds ratio; LCL lower confidence limit; UCL upper confidence limit.
CCT Central Corneal Thickness; CH Corneal Hysteresis
OR LCL UCL P‐value
Age per year <65 1.12 1.01 1.24 .03
Age per year >65 1.08 1.01 1.15 .02
GAT IOP per mmHg 1.22 0.95 1.58 .12
Treatment 1847.6 3.16 106 .02
IOP by treatment interaction 0.79 0.61 1.03 .08
CCT per 100 microns 1.65 0.66 0.98 .30
Years with glaucoma 1.00 0.96 1.04 .98
Baseline IOP 0.99 0.93 1.06 .79
CH per mmHg 0.81 0.66 0.98 .03
Section 2: Clinical Evidence – Study 1Corneal Hysteresis found to be associated with progression
Section 2: Clinical Evidence – Study 2CH associated with progression in NTG eyes
48
A retrospective study to investigate the clinical significance of Corneal Hysteresis in patients with progressing normal tension glaucoma (NTG).
82 eyes of 82 NTG patients receiving topical anti‐glaucoma medications were included. • Subjects were included if they had an established diagnosis of NTG made by a glaucoma specialist based on
glaucomatous optic disc damage and abnormal VF test results. Signs of glaucomatous optic disc damage were considered diffuse or localized neuroretinal rim loss, excavation, and RNFL defects.
• An abnormal VF was defined as a pattern standard deviation outside of the 95% normal confidence limits or a Glaucoma Hemifield Test result outside normal limits.
• At least two consecutive abnormal VF examinations were required, with the most recent test performed within 12 months of enrollment.
NTG was defined by repeatable IOP ≤21 mm Hg, glaucomatous optic disc changes, and VF loss.
Patients were allocated to two groups based on the mean value of corneal hysteresis• Mean CH was 10.08 mmHg. • Assessment of progression was based on the trend analysis using VF MD slope.
Uni and multivariable analyses were constructed to identify factors associated with increased odds of progression, including CH, IOP, central corneal thickness (CCT), and RNFL thickness.
Park Et. Al Br J Ophthalmol. 2015 Jan 2. pii: bjophthalmol‐2014‐305962. doi: 10.1136/bjophthalmol‐2014‐305962.
MV Multi‐Variate; CCT Central Corneal Thickness; RNFL Retinal Nerve Fiber Layer; VF MD Visual Field Mean Deviation; CH Corneal Hysteresis, IOP Intraocular Pressure
Park Et. Al Br J Ophthalmol. 2015 Jan 2. pii: bjophthalmol‐2014‐305962. doi: 10.1136/bjophthalmol‐2014‐305962.
Section 2: Clinical Evidence‐ Study 2 CH associated with progression in NTG eyes
49
MV Multi‐Variate; CCT Central Corneal Thickness; RNFL Retinal Nerve Fiber Layer; VF MD Visual Field Mean Deviation; CH Corneal Hysteresis, IOP Intraocular Pressure
Logistic regression with VF progression as a binary outcome (stepwise MV) β (95% CI) P‐Value
Baseline VF MD (dB) 1.18 (0.96 to –1.44) 0.12
CCT (μm) 0.99 (0.97 to 1.01) 0.35
Subfoveal choroidal thickness 0.99 (0.98 to 1.00) 0.08
RNFL thickness (average) 0.96 (0.92 to 0.99) 0.04
RNFL thickness (temporal) 0.97 (0.94 to 1.01) 0.09
RNFL thickness (inferior) 0.98 (0.96 to 1.01) 0.13
Corneal Hysteresis (mmHg) 0.32 (0.17 to 0.62) <0.01
Of the 39 eyes with low CH, 26 (66.7%) showed progression of VF damage while 13 (33.3%) showed no progression.
Of the 43 eyes with high CH, 15 (34.9%) showed progression of VF damage, whereas 28 (65.1%) showed no progression.
These findings suggest that CH can be used as one of the prognostic factors for progression, independent of corneal thickness or IOP
CH was the best discriminative index for the worse eye in asymmetric OAG.‐ CH lower in 80% of worse eyes
Section 2: Clinical Evidence – Study 3 CH Associated with Asymmetric Glaucoma Progression
Worse Eye Better Eye P
AGIS II VF Score 8.1 ± 4.3 1.0 ± 1.6 <0.001
GAT mmHg 14 (12‐17) 14 (12‐16) 0.3
CCT (μm)531.8 ±34.7
532.3 ±34.9
0.6
Drops (#) 2.2 ± 0.9 2.1 ± 2.6 0.9
CH (mmHg) 8.2 ± 1.9 8.9 ± 1.9 <0.001
CH = Corneal Hysteresis, IOPcc = ORA Corneal Compensated IOP, CRF = ORA Corneal Resistance Factor, SE = Spherical Equivalent, CCT = Central Corneal Thickness; GAT Goldmann Applanation Tonometry
Anand A et al. Invest Ophthalmol Vis Sci. 2010;51:6514‐6518
WHY CORNEAL HYSTERESIS IS A BIOMARKER FOR GLAUCOMA: EVIDENCE
Section 3: Corneal Hysteresis and The Structural Continuum
Section 3: CH and the structural continuum Evidence that CH is a biomarker for glaucoma risk
55
The Evidence suggests that CH is reflective of pressure‐independent mechanisms involved in glaucoma
pathogenesis and associated changes to the optic nerve

Glaucoma Update 2016
Michael Chaglasian, OD 6
Section 3: CH and the structural continuum Conclusion based on evidence in the literature
58
The eye is a mechanical structural continuum
The Evidence suggests that CH is reflective of overall ocular tissue properties
CH appears is related to pressure‐independent mechanisms involved in glaucoma pathogenesis and
associated changes to the optic nerve
2002: Clinical research with ORA commences
2005: The 1st generation ORA was made commercially available
2012: Generation II ORA was launched
3rd Generation “ORA G3” introduced September 2015
Measures:
• Corneal Hysteresis (CH)
• Goldmann‐correlated IOP (IOPg)
• Corneal compensated IOP (IOPCC)
Section 4: Ocular Response Analyzer TechnologyThe instrument
59
Patient positioning Measurement Screen
Section 4: Ocular Response Analyzer TechnologyThe instrument
Corneal Compensated IOP: An IOP measurement that is less influenced by corneal properties than Goldmann or other tonometers. This value is closer to the “true pressure” and has been shown to be a better indicator of glaucoma than Goldmann. Matches GAT on average, so numerical “Scale” is the same
Corneal Hysteresis: An indication of corneal biomechanical properties that has been show to be independently predictive of future glaucoma progression. Reimbursable under CPT 92145.Typical average value is 10.5. Typical Range is 8‐14. Low is bad
IOPg: A Goldmann‐correlated IOP measurement for reference purposes so that clinicians can appreciate what a Goldmann would read simultaneously with the IOPcc value above.
Waveform Score: A signal analysis algorithm that rates the “quality” of the measurement signal on a scale of 0‐10. The higher the value, the more reliable the IOP and CH values are. 6‐10 is excellent. 4‐5 is not so good. 3 or below is poor.
Section 4: Ocular Response Analyzer TechnologyInterpretation of measurement values Spectral Domain: Many Options Spectral Domain: Many Options
Still Valuable: But Perhaps Limited Future
(I am unaware of any timelines)
GDx
Stratus
Cirrus SD OCT
• Glaucoma Applications:
– RNFL
– Optic Disc
– Ganglion Cell Analysis
• Retinal Application:
– Not Covered here
73
Cirrus
Printout

Glaucoma Update 2016
Michael Chaglasian, OD 7
How to “Read” a Printout
• FIRST!: Signal Strength
– A KEY indicator of image quality
– Should be 7/10 or higher on Cirrus
– DO NOT interpret poor quality scan as “red” disease
• Well centered image
• No evidence of movement artifact
• Review Plots and Displays
– Thickness Map and Deviation Map
– Quadrant and Sector Plots
– TSNIT and Optic Nerve B‐Scan Tomograms
76 77
Glaucoma – RNFL Thickness AnalysisThe RNFL thickness map shows
the patterns and thickness of the nerve fiber layer within the 6mm x 6mm cube
• The RNFL deviation map is overlaid on the OCT fundus image to illustrate precisely where RNFL thickness deviates from a normal range
Glaucoma – RNFL Thickness Analysis
A TSNIT (temporal-superior-nasal-inferior-temporal) circle, with a radius of 1.73mm, is established around the disc The LSO fundus image is shown with an OCT fundus
overlay. The red circle indicates the location of the RNFL TNSIT circle
Normative Data: Glaucoma
• Average RNFL Thickness
• RNFL Symmetry
• Rim Area
• Disc Area
• Average C/D Ratio
• Vertical C/D Ratio
• Cup Volume
Distribution of Normals:Color coded indication of normative data
comparison for RNFL and ONH.
• The thickest 5% fall in the white area.
• 90% of measurements fall in the green area.
• The thinnest 5% fall in the yellow area or below.
• The thinnest 1% of fall in the red area.
• Measurements in red are considered outside normal limits.
• ONH values will be shown in gray when the disc area does not match with normative data.
Zeiss: Cirrus OCT Printouts Cirrus: Ganglion Cell Analysis
• Measures thickness for the sum of the ganglion cell layer and inner plexiform layer (GCL + IPL layers) using data from the Macular 200 x 200 or 512 x 128 cube scan patterns.
Carl Zeiss Meditec, Inc Cirrus 6.0 Speaker Slide Set CIR.3992 Rev B 01/2012
SecondScan Obtained
– Ganglion Cell Layer
– Inner Plexiform Layer
– Theory that the RNFL is too variable and notimportant in macular assessment
2 Layers
Ganglion Cell Analysis ‐ Zeiss

Glaucoma Update 2016
Michael Chaglasian, OD 8
Anatomy:Ganglion Cell Layer and IPL Cirrus: Ganglion Cell Analysis
The analysis contains:
• Data for both eyes (OU)
• Thickness Map –
– shows thickness measurements of the GCL + IPL in the 6mm by6mm cube and contains an
elliptical annulus centered about the fovea.
• Deviation Maps –
– shows a comparison of GCL + IPL
– thickness to normative data.
• Thickness table –
– shows average and minimum thickness within the elliptical annulus.
Macular/Ganglion Cell Analysis for Glaucoma: Key Points
• Is a “complement” to traditional RNFL scans
• Has a large number of false positives.
• Should NOT be used as the sole basis of a diagnosis for glaucoma.
• Not proven to make an earlier diagnosis.
“The thought that these devices can diagnose glaucoma in the absence of corroborating clinical evidence is, in my opinion, the most common (and potentially dangerous) misunderstanding.
The limited normative databases against which scans are compared can never cover the remarkably varied appearance and structure of the optic nerve we encounter in normal individuals.”
James Brandt, MD
What are practitioners' most common misunderstandings of imaging technology? Red Disease! Read a Printout Summary
• Image Quality
• Step by step to review most plots.
• RNFL and Optic Nerve
• Localized vs. Diffuse
• Normative Data
• Red Disease
99
Glaucoma Case
EXAMPLESCASE MZ
IOP in high teens
CCT= 560
CASE CM
38 yo
GAT= 22 OD 25 OS

Glaucoma Update 2016
Michael Chaglasian, OD 9
Visual Field Testing
Remains an essential exam component.
In fact, indications for more frequent testing on patients.
Central Field Loss is Important
Understanding if there is central visual field loss (within 10° of fixation) is important for the patient• Decreased reading speed and errors• Altered driving ability – reading signs• Increased risk of falls
Peripheral visual field loss• Asymptomatic (unless bilateral and severe)• Does not impact function as significantly
Central Visual Fields and Glaucoma
Recent papers have suggested that the 24-2 test pattern has limited ability to detect central field defects• 50% of retinal ganglion cells are found within 4.5mm
of fovea
• Macula region comprises only 10% of overall visual field area though it is responsible for 60% of area of visual cortex
• Damage to central 100 associated with diminished contrast sensitivity, reduced reading ability
10-2 and 24-2The Central Field in Glaucoma
Does the 24-2 detect functional vision loss in the central 100 in all cases?• Points in test grid are 60 apart in a grid pattern
Is there a role for a complementary test such as the 10-2 in which 55 points are placed in a 100
area that are 20 apart?• Will this detect small scotomas that fall between the
cracks?
Is glaucoma a disease that involves the macula region early in the condition?
Use 24-2 mostly
24-2 tests 54 points 30-2 = 76 points
For severe loss: 10-2 or size V
Spacing: 24-2 and 30-2 every 6 degrees
Spacing: 10-2 every 2 degrees
30-2 24-2
10-2
Key Information on the Single Field Analysis Printout:
1. Demographics• Testing Conditions
2. Reliability Indices• FL, FP, FN
• Gaze Tracking
3. Total Deviation
Pattern Deviation4. Glaucoma Hemifield
Test (GHT)
5. Global Indices• VFI, MD, PSD

Glaucoma Update 2016
Michael Chaglasian, OD 10
Reliability Indices: Fixation Losses
• Checks the blind spot• Over 20-25% Suggests
Compromised test
• However, many artifactually high results BS not located
Head Tilt
High FP
Gaze Tracking
Gaze Tracking
The Field Analyzer Primer: Effective Perimetry fourth editionAnders Heijl, Vincent Michael Patella, Boel Bengtsson
2012 Carl Zeiss Meditec
Reliability Indices: False Positives
• Most important index
• Rates of 10-15% or higher indicate significantly compromised results
Total Deviation Probability Plots
Symbols used to show % of normal pts with a sensitivity that low or lower
For example, 0.5% symbol indicates that less than 0.5% of normal subjects will have sensitivity that low
132
Pattern Deviation Plots
Shows sensitivity losses after an adjustment has been made to remove any generalized depression.
Highlights only significant localizedvisual field loss
Uses decibels and probability symbols like total deviation plots
Comparing Total and Pattern Deviation
TD• Uniformaly abnormal
PD• Clear
Some scattered points may still show
Assessment:• Cataract
Global Indices
VFI• Visual Field Index
MD• Mean Deviation
PSD • Pattern Standerd
Deviation
Visual Field Index (VFI)
Recently developed staging index, designed to be less affected by cataract (vs. MD)
VFI is approximately 100% in normal fields and approaches 0% in perimetrically blind fields.
More usefully for progression analysis
72%
Mean Deviation (MD)
Shows how much on average the whole field departs from age-normal values.
Is sensitive for generalized depression and very large localized defects
Range=• 0 to -30-35 dB
-4.6dB

Glaucoma Update 2016
Michael Chaglasian, OD 11
Glaucoma Hemifield Test: GHT
The Field Analyzer Primer: Effective Perimetry fourth editionAnders Heijl, Vincent Michael Patella, Boel Bengtsson
2012 Carl Zeiss Meditec
Glaucoma Hemifield Test:
Plain language classification of test results:
1. Outside Normal limitsEarly Localized Defect
2. Borderline (localized defect)
3. Generalized Depression of Sensitivity
4. Abnormally High Sensitivity (high FP)
5. Within Normal Limits
Early Glaucoma Defects
• Arcuate Defects
• Paracentral Defects
• Nasal Steps
Look for a cluster of 2-3+ adjacent defects (P< 1%, P< 0.5%) on the Patten Deviation Plot (must also be on the Total Deviation Plot)
CASE WS
65 yo Patient
POAG:– OD worse than OS
Pre Tx IOP : 32 OD; 24 OS
Currently: 22 OD; 21 OS
ONHs and VFs =>
Functional Assessments for Glaucoma: Standard Visual Field Tests
• Is disease present ?
• How bad is it ?
• Is it getting worse?
Factors Affecting the Measurement of Progression
1. Difficulty in detecting change in a chronic, slowly progressive disease
2. Patients are usually treated so it is difficult to establish the natural history of progression
3. Normal test-retest variability vs. progression
1.1
Baseline exams.
• Establishes initial visual field status.
VFI Rate of Progression Analysis.
• Trend Analysis of patients
overall visual field history
Today’s Visual Field. • Complete report of
current visual field exam
including PD, VFI,
progression analysis and
GPA Alert.
Glaucoma Progression Analysis
1.1
Central points weighted more heavily than those on periphery
Reduces cataract contribution to the measurement of VF loss
“ B”has more damaged central points and lower VFI than“A”.
A B
VFI = 90% VFI = 81%
Visual Field Index (VFI)
1.1
The VFI Bar• historical and
projected VFI loss
Loss to date
Projected future loss100%
HFA GPA VFI Summary

Glaucoma Update 2016
Michael Chaglasian, OD 12
1.1
•Event analysis (GPA alert) indicates “Likely Progression”.
•Slope is nearly flat and the confidence interval is narrow.
•Patient is 75 years old.
EXAMPLE Rate of Progression
Caprioli J. AJO 2008
Most OAG patients will
not be impaired.
Even worstAGIS group had modest
change
Worst group lost3 decibels in 8 years
= 0.4 dB/yearAGIS 7. Am J Ophthal2000;130:429 - 440
OAG patients should be subdivided into (at least) 2 groups
stable cases = 0.1 dB/yearprogressive cases
0.9 dB/year “catastrophic”
Collab Normal Tenstion Glau Study. Am J Ophthalmol 2000Katz et al. Ophthalmology 1997;104:1017Heijl A, Bengtsson B, Hyman L, Leske MC. EMGT. Ophthalmology.
2009;116:2271-6
How Often to Repeat VFs?
At 1 field per year,
>10 years to detect average progression
At 3 fields per year, find average in 4 years, catastrophic in 2 years.
Chauhan et al BJO 2011
How many fields per year ?And when ?
For the new glaucoma patient with real field loss
Consider doing 3 fields in first year and one every 6 months the next year
At a total of 5 in 2 years, good identification of the catastrophically worsening patient
Then scale back to 1 per year
Many already known to be generally stable don’t need this intensity
VF Testing Guidelines= 3/yr!Prostaglandin Analogs
LumiganLumigan
TRAVATAN Z
Xalatan

Glaucoma Update 2016
Michael Chaglasian, OD 13
Travatan Z: Non BAK optionUnique Ionic Buffer
SystemTMPolyolsBorate Zinc
When TRAVATAN® Z solution comes in contact with the positively charged ions in the tear film, the ionic buffered preservative system becomes inactive, providing a solution that is safe and gentle on the eye.
Travoprost: Sustained IOP Lowering
Clinical Ophthalmology 2012:6 525–531
Lumigan 0.01% The Only:Preservative Free PGA
Zioptan
A Preservative Free prostaglandin analog– Introduced in 2003
– Tafluprost 0.015%
– Single use vial delivery
Same PGA side effects:– Iris/Periorbital Pigmenation,
Hyperemia, Deepening Orbital Sulcus, etc.
http://www.zioptan.com/zioptan/consumer/secure/index.html
Small Switch Study (2010)
Conclusion: Preservative-free tafluprost
was better tolerated than the commercially available formulation of latanoprost
Patients (n=158) who were recruited to the study because exhibiting symptoms ⁄ signs of ocular surface side-effects.
The drugs appeared to have equal IOP reducing effect.
Generic Ophthalmics
Prostaglandins– Latanoprost– Travoprost– Bitmatoprost 0.03%
Alpha Agonist– Brimonidine 0.2,
0.15%
CAI– Dorzolamide 2%
Beta Blockers– Timolol– Levobunolol
Fixed Combination– Dorzolamide/timolol
80% of all Rxs
“In 2010 alone, the use of FDA-approved generics saved $158 billion, an average of $3 billion every week.”
Latanoprost Generic
March 2011
Multiple Suppliers– Including Pfizer/Greenstone and
Falcon
Glaucoma Update 2016
Michael Chaglasian, OD 14
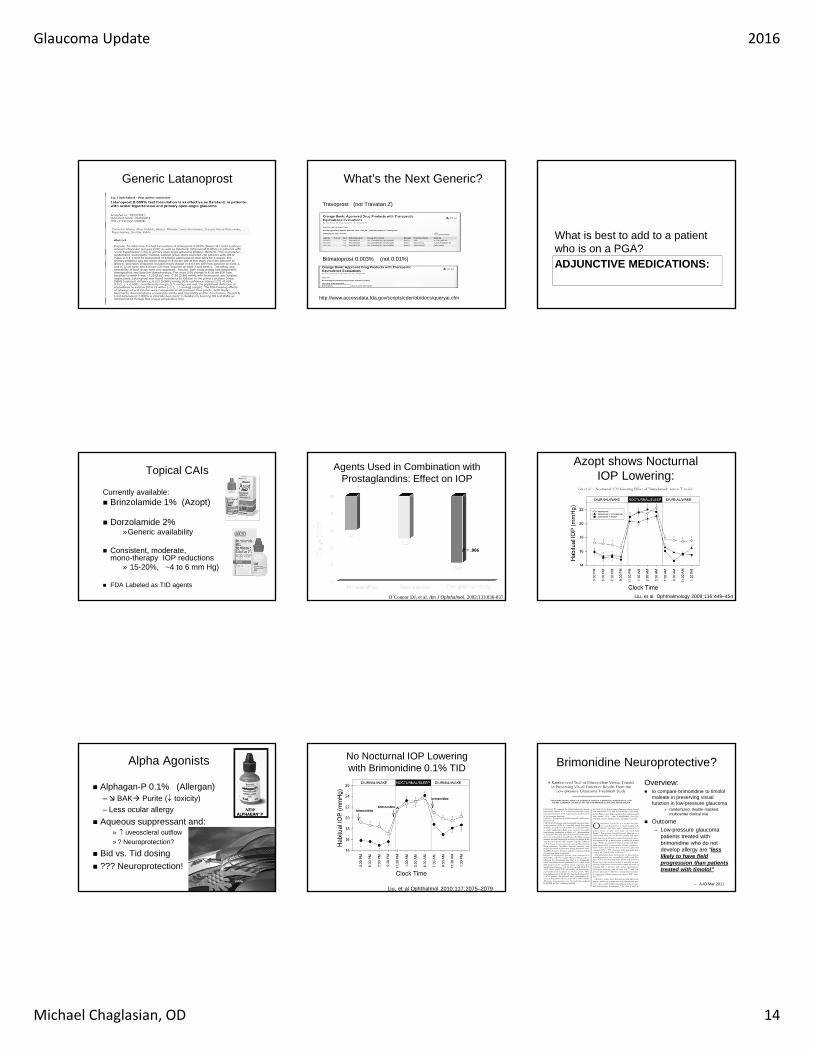
Generic Latanoprost What’s the Next Generic?
Travoprost (not Travatan Z)
Bitmatoprost 0.003% (not 0.01%)
http://www.accessdata.fda.gov/scripts/cder/ob/docs/queryai.cfm
ADJUNCTIVE MEDICATIONS:
What is best to add to a patient who is on a PGA?
Topical CAIs
Currently available: Brinzolamide 1% (Azopt)
Dorzolamide 2%»Generic availability
Consistent, moderate, mono-therapy IOP reductions
» 15-20%, ~4 to 6 mm Hg)
FDA Labeled as TID agents
Agents Used in Combination with Prostaglandins: Effect on IOP
O’Connor DJ, et al. Am J Ophthalmol. 2002;133:836-837.
P = .006
Azopt shows NocturnalIOP Lowering:
Liu, et al Ophthalmology 2009;116:449–454
Alpha Agonists
Alphagan-P 0.1% (Allergan) – BAK Purite ( toxicity)
– Less ocular allergy
Aqueous suppressant and:» uveoscleral outflow
» ? Neuroprotection?
Bid vs. Tid dosing
??? Neuroprotection!
No Nocturnal IOP Lowering with Brimonidine 0.1% TID
Liu, et al Ophthalmol 2010;117:2075–2079
Brimonidine Neuroprotective?
Overview: to compare brimonidine to timolol
maleate in preserving visual function in low-pressure glaucoma
» randomized, double-masked, multicenter clinical trial
Outcome– Low-pressure glaucoma
patients treated with brimonidine who do not develop allergy are “less likely to have field progression than patients treated with timolol”
– AJO Mar 2011

Glaucoma Update 2016
Michael Chaglasian, OD 15
Issues with Data/Conclusions
Failure rate of beta blockers– much higher than our collective clinical experience:
EMGT, OHTS
– Extrapolating the Kaplan-Meier survival graph to 5 years would predict a 100% progression rate for the patients taking timolol
Side effect rate of brimonidine– ~30 % drop out due to side effects (0.2%)
Degree of IOP lowering in treatment groups– Approximately the same between the 2 drugs
Generic Brimonidine
0.2%– Risk of increased allergy
0.15% (expensive and hard to find)
Generic Timolol
No Night-time IOP lowering effect. Many glaucoma specialists have shifted away from using timolol by itself.
Advantages of Fixed Combinations
Dosing—1 drop vs 2 drops
Convenience
Potential to improve compliance1
No risk of washout from second drug2
– Washout impedes absorption, thereby reducing efficacy3
Possible cost savings– Only 1 copay
1. Razeghinejad et al. Expert Opin Pharmacother. 2010; 2. Choudhri et al. Am J Ophthalmol. 2000.; .3 Khouri. Drugs Aging. 2007.
Timolol Fixed Combinations
Cosopt®
– Dorzolamide hydrochloride/timolol maleate solution
Generic dorzolamide / timololmaleate ophthalmic solution
Fixed Combination: Combigan
Combigan (Allergan)– Brimonidine 0.2%
and timolol 0.5%
– BID dosing
Less allergy than brimonidine alone– timololo is a buffer
Cosopt PF (Akorn)
dorzolamide HCL - timololmaleate 2%/0.5%
Preservative Free
BID dosing
25-30% IOP reduction when used as monotherapy
Role:– COPD and other beta
blocker contraindications
Similar indications for OSD patients where BAK toxicity is a concer
http://akorn.com/prod_detail.php?ndc=17478-604-30
Cosopt PF
MG13241SK
Delivers 21-35% IOP-lowering efficacy1-3
Only fixed-combination without a beta blocker1-3
SIMBRINZA™ Suspension (Brinzolamide/Brimonidine)
Additional 1-3 mm Hg IOP-lowering compared to the individual components1-3
Adverse events profile consistent with those of its individual components1-3
Creates new treatment possibilities for lowering IOP
1. Katz G, et al. Three‐Month Randomized Trial of Fixed‐Combination Brinzolamide 1%/Brimonidine 0.2%. JAMA Oph. 2013.2. Nguyen QH, et al. Phase 3 Randomized 3‐Month Trial With an Ongoing 3‐Month Safety Extension of Fixed‐Combination
Brinzolamide 1%/Brimonidine 0.2%. J Ocul Pharmacol Ther. 2013;29:290‐7.3. SIMBRINZA™ Suspension Package Insert.
210

Glaucoma Update 2016
Michael Chaglasian, OD 16
MG13241SK
1. SIMBRINZA™ Suspension Package Insert. 2. Katz G, et al. Three‐Month Randomized Trial of Fixed‐Combination Brinzolamide 1%/Brimonidine 0.2%. JAMA Oph. 2013.3. Nguyen QH, et al. Phase 3 Randomized 3‐Month Trial With an Ongoing 3‐Month Safety Extension of Fixed‐Combination
Brinzolamide 1%/Brimonidine 0.2%. J Ocul Pharmacol Ther. 2013;29:290‐7.
SIMBRINZA™ Suspension is a fixed-combination that is beta blocker-free2,3
Brimonidine
Brinzolamide
Brinzolamide
SIMBRINZA™ Suspension Has Two Active Compounds with Complementary MOAs1
+
=
SIMBRINZA™ Suspension
211
New and Upcoming Meds
Vesneo
Vesneo
Latanoprostene bunod 0.024%– Nitric oxide donating PGA
– Thus a “dual” action PGA
Adds improved outflow through the trabecular meshwork by inhibiting actomyosin contractility in TM cells and relaxing/opening the meshwork– Trials (vs timolol) show IOP reduction of 7.5 –
9.1 mmHg
Approved! Bausch+Lomb Summer 2016
Rho Kinase Inhibitors
“ROCK” Inhibitors: family of protein kinases– The enzyme and the pathway play a critical role
in regulating the contractile tone of smooth muscle
– Research in the last decade has identified ROCK as an important mediator of aqueous outflow through the trabecular meshwork
» lowers resistance to aqueous outflow in the trabecular meshwork
– potential of restoring normal TM function
– No other medication works in this fashion
Roclatan (Arie)
Rho Kinase Inhibitors (Arie)
Rhopressa: “triple action”– Reduces aqueous production– Increase TM outflow– Decreases episcleral venous pressure (inc.
outflow)
Phase 3 Trial 2015– Did not meet primary endpoints
» But did meet in patients with lower IOP» FDA allowing to re-submit
– Hyperemia is an issue:» Noted in 35%, though 85% reported as mild
Rho Kinase Inhibitors (Arie)
Roclatan– Rhopressa and latanoprost (quadruple
action!)
– Phase 2 Trials Completed w/ 35% IOP lowering
» Exceeded latanoprost by up to 3 mmHg
» Hyperemia 40%
Trabodenoson (Inotek)

Glaucoma Update 2016
Michael Chaglasian, OD 17
Trabodenoson
A selective adenosine mimetic (novel)– Adenosine A1 receptors in the TM
– Upregulates proteases (MM-2) which digest and remove hydrolyzed proteins that clog the TM
– Thus improving/restoring normal TM outflow
Phase 2 Trials Completed: (dosing, concentration)
– QD dosing; alone or in combo w/PGA
– No ocular side effects
– Significantly Lowered IOP
Phase 3 trials are enrolling (Inotek)
The Helios Insert
http://forsightvision5.com/products/helios-insert/
OTX-TP
Sustained release travoprost Intra-canalicular depot
– Punctal plug delivery system
– 3 Month Release time period
Ocular Therapeutix– Phase 2 Clinical Trials underway
Ocular Therapeutix Ocular Therapeutix
224
http://www.sec.gov/Archives/edgar/data/850693/000119312514254394/d750005dex992.htm
Michael Chaglasian, OD, FAAOIllinois Eye Institute
Illinois College of [email protected]
• 57 yo, W, F
• ‐7.50 Myopia
• Good Medical Health
• CCT= 562, 571
• GAT: 19‐23 / 18‐23mmHg– Pre‐Treatment 26/31; 12 months ago
• Current Meds:– PGA qhs OU
– Fixed Combination OU
• Target IOP OD:– ≤ 12 mmHg
• Is this patient a candidate for laser procedure?
• Is this patient a candidate for surgical procedure?
• What are the Pros and Cons?
• What are facts about the pros and cons?

Glaucoma Update 2016
Michael Chaglasian, OD 18
1. Is SLT more effective (IOP reduction) than ALT?
2. Is SLT better than medical therapy?
3. Is SLT repeatable?
4. Do topical medications affect SLT?
5. How good is SLT on maximal topical therapy?
6. Does SLT work on nocturnal IOP elevation?
7. Does SLT work after cataract surgery?
8. Cost effectiveness vs. medical therapy?
• Conclusions:
– Laser trabeculoplasty is successful in lowering intraocular pressure for patients with open angle glaucoma.
– At this time, there is no literature establishing the superiority of any particular form of laser trabeculoplasty.
• Conclusions:
– IOP reduction was similar in both arms after 9 to 12‐months follow‐up.
– These results support the option of SLT as a safe and effective initial therapy in open‐angle glaucoma or ocular hypertension.
– SLT may be the best or most preferred treatment option for some patients
• Conclusions:
– “We found that a repeat 360‐degree SLT provided additional IOP reduction, which was not as marked as that with the first treatment (≥20%)”
• Overall, poorly studied.
• Generally yes, to a very modest extent (~2 mmHg)
• 45 eyes/25 subjects
• Avg 28 m post 1st Tx
@ 24 m
• 29% > 20% IOP lowering
• 39% > 15% lowering
• Repeat Tx was less effective than initial
• Conclusions: • Topical medications do not
adversely, nor favorably, affect SLT success.
• Success rate of 67% at 6 months.
• Factors: – Pigmentation of the anterior
chamber angle, class of antiglaucoma medications, diabetes, sex, corneal thickness, pseudophakia, diagnosis, washout of eye drops, and previous argon laser trabeculoplastytreatment are not associated with SLT treatment efficacy.
SLT with ≥ 3 mmHg Reduction
NonResponders
Responders
70%
30%
• Conclusions:
– SLT response was delayed in pseudophakiccompared to phakicpatients,
– while the long‐term effectiveness of SLT is the same in both groups.

Glaucoma Update 2016
Michael Chaglasian, OD 19
• Results: – There were no significant differences in the IOP‐lowering effects between the two methods at any time point during the follow‐up period (12m)
– Mean IOP reduction:• 75% subjects ≥ 15% dec.from base.
• Approx. 3‐4 mmHg
• Conclusions:
• Prostaglandin analogs and LTP are both cost‐effective options for the management of newly diagnosed mild open‐angle glaucoma.
• Assuming optimal medication adherence, PGAs confer greater value compared with LTP.
• However, when assuming more realistic levels of medication adherence (making them 25% less effective)
• Then at current prices for PGAs ($330/yr), LTP may be a more cost‐effective alternative.
• Cataract Extraction
– Generally only appropriate for early stage OHTN glaucoma that is not progressing (or ACG)
– Much less effect for moderate glaucoma
– Can reduce use of topical medications
– Is not long lasting.
Data from OHTS:
• ~ 3‐4 mmHg lower
• mean of ‐16% lower
• ~ 36 months (at least)
Traditional filtering or glaucoma drainage devices remain the surgery of choice for patients with advanced
glaucoma.
• Trabeculectomy with anti‐metabolite (MMC)– Bleb forming procedure
• Risk of bleb leak related complications
– Long established procedure with vast experience
• Glaucoma Drainage Device– External reservoir,
moderately invasive • Baerveldt, Ahmed
– Typical role is following failed procedures
• E‐Shunt– Stainless steel implant into angle
– still is a bleb forming procedure
– Generally good outcomes, about on par with standard trabeculectomy
– Fewer complications
MIGSMicro Invasive Glaucoma SurgeryWhy?• An unmet need for surgical intervention for
mild to moderate glaucoma patients with coexisting cataract.
• MIGS combined with cataract surgery will have an increasing role in managing these patients
• MIGS–Micro Invasive Glaucoma Surgery
• Emerging category of devices and procedures– Alternative to multiple medications
– Often combined with cataract extraction
– Differing definitions and can be grouped into two categories
1. Schlemm’s canal (Trabectome ‐ NeoMedix; iStent ‐ Glaukos)
2. Supraciliary space (none FDA‐approved, Cypass – Transcend; Supra – Glaukos both in trials)
3. Subconjunctival space
(none FDA‐approved, Aquesys XEN)
4. Intra‐Canalicular( Hydrus MicroShunt)