gingival recession associated with predisposing factors...
TRANSCRIPT

134
IntroductionGingival recession has been defined as a displace-ment of gingival margin apically from the cemen-to-enamel junction (CEJ), leading to root-surfaceexposure, which may cause poor aesthetics, dentinehypersensitivity, plaque retention, gingival bleed-ing, susceptibility for root caries and fear of toothloss [1-3]. A denuded root surface frequentlyresults from a combination of predisposing andtriggering/aggravating factors. Predisposing factorsincluded bone dehiscence, insufficiency of widthand/or thickness of keratinised gingiva, tooth mal-position and high fraenal attachment. The trigger-ing/aggravating factors may include: traumatic
tooth-brushing, non-carious cervical lesions (abra-sion, abfraction, erosion, resorption), inflammation(dental plaque, calculus, gingivitis, periodontitis),iatrogenic factors (inappropriate fixed prostheses,poorly designed partial dentures, operative proce-dures, orthodontic treatment, traumatic occlusion)and diverse factors (age, gender, piercing, chewingstick trauma) [3,4]. A high prevalence of gingivalrecession has been reported in America (63%-89%)[5-7], Europe (25%-84%) [8-13] and Australia(71%) [14] but a lower prevalence has been foundin Africa (28%) [15,16] and Asia (15%) [17].However, the extent of root-surface exposure washigher in Africa (18%-51%) [15,16] and America
Gingival Recession Associated With Predisposing Factors in YoungVietnamese: A Pilot Study
Tung Nguyen-Hieu1, Bao-Dan Ha-Thi2, Hang Do-Thu2, Hoa Tran-Giao3
1PhD, DDS.* † 2MSc, DDS.* 3DDS.**Department of Periodontology, Faculty of Odonto-Stomatology, University of Medicine and Pharmacy, Ho Chi MinhCity, Vietnam.†Unité de Recherche sur les Maladies Infectieuses et Tropicales Emergentes, UM 63, CNRS 7278, IRD 198, INSERM1095, Aix-Marseille Université, Marseille, France.
Corresponding author: Tung Nguyen-Hieu, Unité de Recherche sur les Maladies Infectieuses et Tropicales Emergentes,Faculté de Médecine, Aix-Marseille Université, 27 boulevard Jean Moulin, 13005 Marseille, France; e-mail :[email protected]
AbstractAims: Several studies have shown a large diversity in the prevalence, extent and severity of gingival recession as wellas controversial conclusions of its associated factors. Therefore, the aim of this pilot study was to evaluate gingival reces-sion with predisposing factors in young Vietnamese.Methods: A cross-sectional study using clinical examination was performed in 120 dental students. Oral hygiene status,tooth malposition and fraenal attachment were recorded. The width of keratinised gingiva was measured after mucosastaining with Lugol’s iodine solution. Measurements of gingival recession were performed on labial tooth surfaces. Chi-square test, t-test and Pearson’s correlation were used for data analysis.Results: The prevalence of gingival recession was 72.5% of the studied population. The extent of affected teeth was11.1% of the examined teeth. The proportion of root-surface exposure was statistically higher (P<0.05) in the maxilla(12.5%) than in the mandible (9.6%). Premolars and right canines were the teeth most frequently and most seriouslyassociated with gingival recession, respectively. There was a strong negative correlation between narrow width of kera-tinised gingiva and gingival recession (P<0.001). The recession was statistically associated with tooth malposition(P<0.001) but it was not related to high fraenal attachment and gender.Conclusions: A high prevalence of gingival recession was found in Vietnamese dental students. Gingival recession wasassociated with narrow width of keratinised gingiva, tooth malposition and maxillary teeth. Further studies performed inlarger populations with more extended age groups are needed to confirm these findings.
Key Words: Gingival Recession, Prevalence, Severity, Extent, Tooth Malposition, Fraenal Attachment, KeratinisedGingiva

135
OHDM - Vol. 11 - No. 3 - September, 2012
(38%-44%) [5-7] than in Europe (5%-17%) [8-13],Australia (4.6%) [14] and Asia (2%) [17]. Thereare limited published data concerning the preva-lence, extent, and severity, as well as associatedfactors of gingival recession in Asia [16,18].Furthermore, conclusions of the associationbetween gingival recession and predisposing fac-tors including width of keratinised gingiva [12],fraenum attachment [13,18] and tooth malposition[15,18,19] are still controversial [20]. Although theaetiology of root-surface exposure is multifactorial,determining the influence of predisposing factorshas an important role in management of gingivalrecession such as increasing keratinised tissue,fraenectomy or orthodontic treatment.
AimThe aim of this pilot study was to measure gingivalrecession in a population of 19-25 year-old dentalstudents for preliminary assessment of the preva-lence, extent, severity of gingival recession and itspredisposing factors including width of keratinisedgingiva, tooth malposition and fraenal attachmentin Vietnamese young adults.
Methods
Target populationA cross-sectional study using a clinical examina-tion was performed in a population of 120 dentalstudents of University of Medicine and Pharmacyof Ho Chi Minh City in Vietnam. These subjectswere randomly selected from about 600 students ofFaculty of Odonto-Stomatology. Briefly, 80-120dental students from every class were classifiedinto ten groups of 8-12 students, from which twogroups were randomly selected. A total of 12groups including 120 students from six classesagreed to participate in this study after reading theresearch objectives and signing a consent form.Only 19-25 year-old students, non-smoking andthose having more than 24 teeth (excluding thirdmolars) were included. Students with a history oforthodontic or periodontal treatment were exclud-ed. The type of toothbrush (soft, medium or hard)used by the students was recorded.
Clinical examination and measurementsAll clinical examinations were performed by twoperiodontists (B-D H-T and H D-T) who had previ-ously calibrated by recording all clinical measure-ments to be used in the study on ten dental students.
They obtained a kappa index of agreement of morethan 0.8. Oral hygiene status was evaluated bySimplified Oral Hygiene Index (OHI-S) [21].Labial surfaces of upper first molars and lingualsurfaces of lower first molars (sometimes secondmolars because of first molar loss) and the labialsurfaces of upper right and lower left central inci-sors were assessed for debris and calculus accumu-lations. The OHI-S has two components includingthe Simplified Debris Index (DI-S) and theSimplified Calculus Index (CI-S), which are basedon numerical determinations representing theamount of debris and calculus found on the select-ed tooth surfaces. Each of these indices has scoresfrom 0-3 corresponding with an absence of softdebris/calculus, their amount covering one-third,two-thirds, and more than two-thirds of the exam-ined tooth surface, respectively.
All excluded sites including absent teeth, toothroots and tooth-supported fixed prostheses (crownsand bridges) were noted. Tooth malpositionsincluding overeruption, rotation and othermalalignment were also recorded. The position ofthe CEJ was determined by visual observation andthe "slight scratch" of a periodontal probe on thecervical tooth area in a cervico-occlusal direction.If there were non-carious cervical (wear) lesions orcervical restorations, the position of the CEJ wasconsidered as corresponding with that of adjacentteeth. Gingival recession was evaluated by using amillimetre-graduated periodontal probe to measurefrom the free gingival margin to the CEJ at the siteof maximum gingival recession on the labial sur-face of each tooth (excluding third molars). In orderto localise the mucogingival junction (MGJ), boththe gingiva and buccal mucosa were rinsed withwater, dried and then stained with 3% Lugol'siodine solution (3 g of elemental iodine and 6 gpotassium iodine in 300 mL sterile water) by usinga cotton swab. After two minutes, highly kera-tinised epithelium did not retain the Lugol's iodinesolution while buccal mucosa was stained a red-brown colour. The width of keratinised gingiva ofeach tooth (excluding third molars and previouslyexcluded sites) was measured by using a millime-tre-graduated periodontal probe from MGJ to freegingival margin with 1.0 mm precision. Fraenalattachments were also assessed according to thePlacek et al. (1974) classification [22] in whichfour levels of labial fraenal attachments are mucos-al, gingival, papillary and papillary penetrating.After clinical examination, participants were given

136
OHDM - Vol. 11 - No. 3 - September, 2012
oral hygiene instruction and advice on how to con-trol the progression of gingival recession as well assuggestions for appropriate treatment.
Data analysisFor assessing the oral hygiene status, OHI-S valuewas calculated and classified from 0-1.2 for goodstatus, 1.3-3.0 for medium status and 3.1-6.0 forpoor status. Values of DI-S and CI-S were com-bined to obtain OHI-S value as follows: DI-S =(total scores of debris)/(total number of tooth sur-faces with debris), CI-S = (total scores of calcu-lus)/(total number of tooth surfaces with calculus)and OHI-S = (DI-S + CI-S) [21]. Descriptive statis-tics and the chi-square test were carried out to char-acterise the prevalence, extent, severity of gingivalrecession, and the predisposing factors. In thisstudy, the prevalence of gingival recession was thepercentage of patients with at least one gingivalrecession in the studied population, the extent wasthe percentage of teeth associated with root-surfaceexposure in examined teeth, and the severity wasthe level of apical migration of marginal gingivafrom the CEJ. The Student's t-test was used to com-pare keratinised gingiva widths between teeth withand without root-surface exposure. The correlationbetween keratinised tissue and gingival recessionwas assessed by Pearson's correlation coefficient.These statistical analyses were independently per-formed by a specialist using statistical software(Statistical Package for the Social Sciences, version15.0; SPSS Inc, Chicago, USA). Differences wereconsidered statistically significant when the P-value was <0.05.
Results
Prevalence, extent and severity of gingival reces-sionThe study group comprised 60 males and 60females with mean age of 22.3±2.0 years. Ninety-six (80%) subjects had a good status of oral hygieneaccording to the OHI-S value and 116 (97%) sub-jects used soft/medium toothbrushes. The preva-lence of gingival recession (at least one tooth withdenuded root surface >1.0 mm) was 87/120(72.5%). This prevalence was slightly higher infemales (45/60, 75%) than in males (42/60, 70%)but this difference was not statistically significant.
Among a total of 3269 examined teeth (1634teeth in the maxilla and 1635 teeth in themandible), there were 362 teeth (11.1%) with gin-
gival recession. The proportion of root denudationwas statistically higher (chi-square test, P<0.05) inthe maxilla (205/1634, 12.5%) than in the mandible(157/1635, 9.6%). Furthermore, teeth most fre-quently associated with gingival recession were theleft first molar (35/116, 30.2%) and the right firstpremolar (31/114, 27.2%) in the maxilla and theright second premolar (24/113, 21.2%) and left firstpremolar (25/119, 21%) in the mandible (Figure 1).In the maxilla, a decreasing degree of root-surfaceexposure was observed as follows: premolars(84/205, 41%) > molars (74/205, 36.1%) > canines(34/205, 16.6%) > incisors (13/205, 6.3%). In themandible, this was found as follow: premolars(90/157, 57.3%) > molars (37/157, 23.6%) > inci-sors (18/157, 11.5%) > canines (12/157, 7.6%).
Students with gingival recession had meanmeasurements of denuded root surface from 1.0-1.9mm in both maxilla and mandible. The most seri-ous gingival recession was detected at upper rightcanines (1.9±1.2 mm) and lower right canines(1.9±1.3 mm) (Figure 2).
Predisposing factors associated with gingivalrecessionOverall, the width of keratinised gingiva was moreimportant in the regions of incisors and molars andless important in the regions of canines and premo-lars. Teeth with gingival recession had a greaterreduced width of keratinised gingiva than non-affected teeth. In particular, these differences werestatistically significant in all premolars (t-test,P<0.05) and right canines (t-test, P<0.01) of boththe maxilla and the mandible (Figure 3). A nega-tive correlation was also found between the fre-quency of root-surface exposure and width of kera-tinised gingiva (Pearson's correlation, r=-0.33,P<0.001). A narrow width of keratinised gingiva(<2 mm according to classification of Maynard andWilson, 1980) [23] was observed in 388 (11.9%) ofthe teeth. Teeth with a narrow width of keratinisedgingiva had a higher prevalence of gingival reces-sion (111/388, 28.6%) than teeth with a broadwidth of attached gingiva (251/2881, 8.7%) andthis difference was statistically significant (chi-square test, P<0.001) (Table 1). Gingival/papillaryattachments of fraenal (types II, III and IV accord-ing to classification of Placek et al. (1974) [22])were only detected at 64 (1.9%) teeth. Teeth withthese high fraenal attachments had a lower frequen-cy of denuded root surface (3/64, 4.7%) than teethwithout this feature (359/3205, 11.2%) but this dif-

137
OHDM - Vol. 11 - No. 3 - September, 2012
Figure 1. Extent of gingi-val recessions in the max-
illa and the mandible.
Figure 3. Width of kera-tinised gingiva betweenteeth with and without
gingival recession.(t-test:**:P<0.01; *:P<0.05)
Figure 2. Severity of gin-gival recession in the max-
illa and the mandible

OHDM - Vol. 11 - No. 3 - September, 2012
ference was not statistically significant (chi-squaretest, P>0.05). The proportion of malpositionedteeth was 313/3269 (9.6%), of which dental rota-tion (117/3269, 3.6%) and labial declination(67/3269, 2%) were most frequently found.Malaligned teeth had a higher prevalence of gingi-val recession (64/313, 20.4%) than normally posi-tioned teeth (298/2956, 10.1%) and this differencewas statistically significant (chi-square test,P<0.001) (Table 1). Of the 362 teeth associatedwith root-surface exposure, 111 (30.7%) teeth hada narrow width of keratinised gingiva, 64 (17.7%)teeth were related to dental malpositions, only 3(0.8%) teeth were associated with high fraenalattachments, and 219 (60.5%) teeth were still non-identified aetiology.
DiscussionIn this study, 19-25 year-old students were includ-ed because their permanent dentition was relativelycomplete and the occurrence of gingival recessionhad previously been detected in this age group.Only subjects without triggering/aggravating fac-tors (smoking, orthodontic/periodontitis treatment,periodontal surgery, and fixed prostheses) of gingi-val recession were selected to assess the influenceof predisposing factors. The reasons for theseexclusions were that gingival recession might berelated to young adults having orthodontic treat-ment [17,24]. Moreover, periodontitis is a bacterialinfection and inflammation, leading to bonedestruction along with an apical migration of junc-tional epithelium. Periodontal surgery-includingthe opened flap associated with root surfacedebridement and the apically repositioned flap foreliminating pockets-can also lead to root-surfaceexposure [3]. Although gingival recession is morefrequently observed in smokers than in non-smok-ers [7,10,13], the risk of gingival recession attribut-able to smoking is still controversial [17,25].
Because poor crown margins can be a factor inattachment loss and gingival recession [26], siteswith fixed prostheses were also excluded. Althoughseveral studies have indicated that dental plaque,gingival inflammation and calculus were signifi-cantly associated with root-surface exposure[7,10,16,18,19], gingival recession more frequentlyoccurred in patients having good rather than poororal hygiene [2,27]. The oral hygiene of dental stu-dents who took part in the current study was evalu-ated by using OHI-S, which may be suitable forsubsequent studies assessing oral hygiene and gin-gival recession in wider populations of non-dentalstudents. In this pilot study, the majority of dentalstudents had a good level of oral hygiene and theiruse of soft/medium toothbrushes suggested thatthey had high awareness of the need for good oralhealth. Therefore, the orodental status of these den-tal students almost certainly differs from that ofyoung adults in the overall Vietnamese population.This is a limitation of the study in that the resultscannot safely be generalised to all Vietnameseyoung people. However, these preliminary resultscan be used as reference for further studies in alarger population with wider age groups.
A review of the literature from 1982 to 2011on the prevalence, extent, severity and associatedfactors of gingival recession is summarised inTable 2. Studies targeting 15-32 year-old subjects[8,9,12,14,17,18] or this age group in a large popu-lation [6,7,11] showed 29%-76% subjects wereassociated with at least one root-surface exposure>1 mm and an extent of from 2%-18% of teeth. Inthe current study, gingival recession was detectedin 72.5% of Vietnamese dental students with thesame age range. Indeed, this high prevalence wassimilar to that reported in France (76%) [12], Italy(64%) [8], Brazil (64%-77%) [6,7]. The extent ofaffected teeth in the current study (11.1%) was alsoin agreement with previous studies in France
138
Table 1. Correlations between gingival recessions and predisposing factors
Predisposing factors Number of teeth (%) P*Without recession With recession
Normal width of keratinised gingiva (> 2 mm) 2630 (91.3%) 251 (8.7%) <0.001Narrow width of keratinised gingiva (< 2 mm) 277 (71.4%) 111 (28.6%)No fraenum/normal fraenal attachments 2846 (88.8%) 359 (11.2%) >0.05Gingival/papillary fraenal attachments 61 (95.3%) 3 (4.7%)Normal position teeth 2658 (89.9%) 298 (10.1%) <0.001Tooth malposition 249 (79.6%) 64 (20.4%)
* Chi-square test

139
OHDM - Vol. 11 - No. 3 - September, 2012
Authors Year Population Prevalence (% Extent (% teeth Associated Non-associatedStudy Country [males/females] subjects with GR) with GR) Severity factors factors
Years of age (mean) Examined surfaces Most frequent teethTenenbaum 1982 100 dental students 76/100 (76%) 320/2725 (11.7%) - Attached Oral hygieneCross-sectional France [68/32] Male = female First premolars gingiva status, fraenum
19-26 (21.7) Labial (r = -0.201, attachmentP<0.05)
Khocht et al. 1993 182 subjects (63%) - - Age, tooth -Cross-sectional USA 18-65 Male > female brushing
frequencySerino et al. 1994 225 subjects (25%) 1373/5168 (26.6%) - Age, loss of GingivalCross-sectional Sweden 18-65 18-29 years: (44%) 18-29 years: (7%) approximal inflammationand longitudinal Labial Upper first molars attachment
and premolars (multiple regression model,P<0.01)
Van Palenstein 1998 575 subjects Labial and lingual 20-34 years: (18%) Most Calculus -Helderman et al. Tanzania [350/225] 35-44 years: (31%) serious: (PearsonCross-sectional 20-64 45-64 years: (51%) lingual correlation,
surface of P<0.05), agelower
incisorsChecchi et al. 1999 55 dental students (64%) Left side (55%) - Tooth-brushing Age, Cross-sectional Italy [29/26] Male < female > right side (45%) (multiple gender
19-26 Labial Premolars regression model, P<0.05)
Arowojolu 2000 491 subjects 137/491 (27.7%) - - ToothCross-sectional Nigeria [259/232] malalignment, -
16-82 chewing sticktrauma, traumatic tooth-brushing, calculus
Dodwad 2001 1200 GR patients Labial Mandibular Classification Tooth-brushingCross-sectional India [804/396] anterior of Miller: method and -
15-24 teeth I (86.2%), tooth-brush type,II (11.8%), plaque andIII (1.8%), gingivalIV (0.6%) inflammation,
malaligned teeth (chi-square test, P<0.001), fraenal pull
Marini et al. 2004 380 subjects 338/380 (89%) 3526/9379 (38%) Classification Age -Cross-sectional Brazil [146/234] 20-29 years: (64%) 20-29 years: (13.9%) of Miller:
> 20 Labial and lingual Mandible > Maxilla I (59.2%),Mandibular central II (2.8%),incisors III (32.5%),
IV (5.6%)Susin et al. 2004 1586 subjects (83.4%) (43.5%) GR > 3 mm Cigarette smoking, Gender, race,Cross-sectional Brazil [719/867] 20-29 years: (76.5%) 20-29 years: 18.1% (51.6 %), supragingival dental visits,
14-103 Male = female Mandibular GR > 3 mm calculus (Wald socio-economic(37.9 ± 13.3) Labial and lingual incisors (22 %) test, P<0.05 and status
relative risk ratio, P<0.05), age (P<0.01)
Kozlowska et al. 2005 455 medical students 134/455 (29.4%) (5.1%) - Age, tooth-brush -Cross-sectional Poland 18-32 Male < female Premolars and and tooth-brushing,
Labial lower canines and female genderincisors (multiple
regression model, P<0.05)
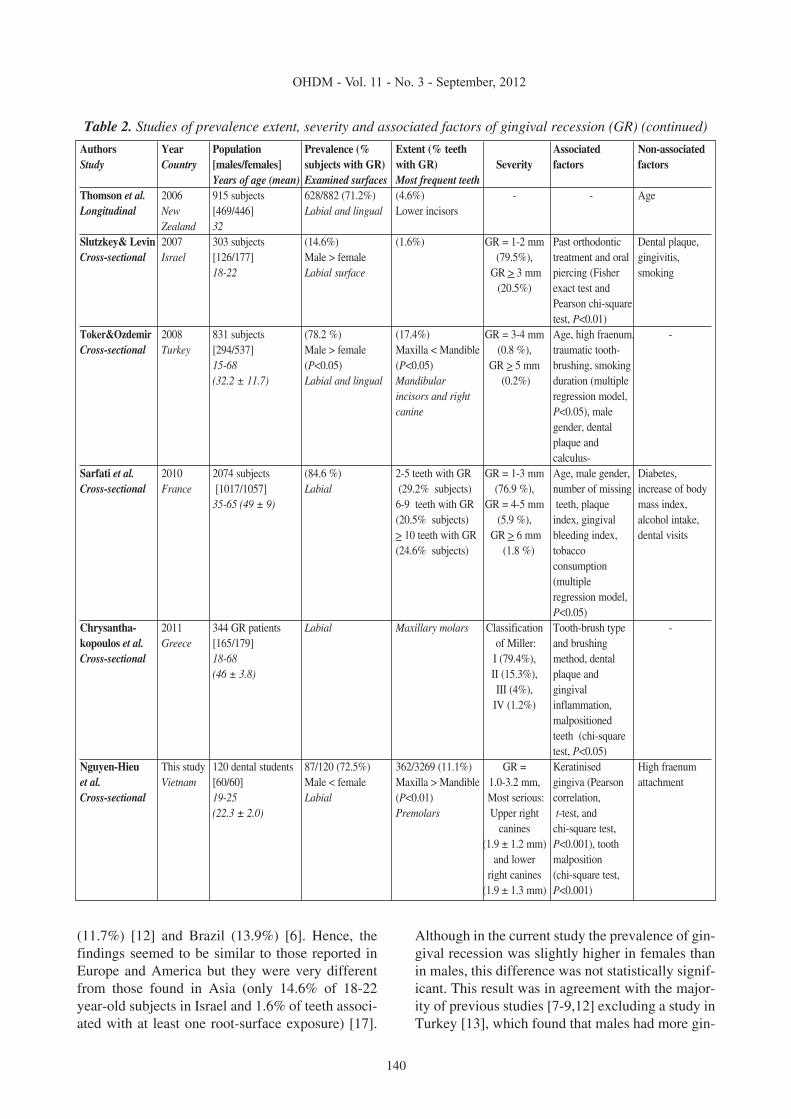
Table 2. Studies of prevalence extent, severity and associated factors of gingival recession (GR) (continued over)
140
OHDM - Vol. 11 - No. 3 - September, 2012
(11.7%) [12] and Brazil (13.9%) [6]. Hence, thefindings seemed to be similar to those reported inEurope and America but they were very differentfrom those found in Asia (only 14.6% of 18-22year-old subjects in Israel and 1.6% of teeth associ-ated with at least one root-surface exposure) [17].
Although in the current study the prevalence of gin-gival recession was slightly higher in females thanin males, this difference was not statistically signif-icant. This result was in agreement with the major-ity of previous studies [7-9,12] excluding a study inTurkey [13], which found that males had more gin-
Authors Year Population Prevalence (% Extent (% teeth Associated Non-associatedStudy Country [males/females] subjects with GR) with GR) Severity factors factors
Years of age (mean) Examined surfaces Most frequent teethThomson et al. 2006 915 subjects 628/882 (71.2%) (4.6%) - - AgeLongitudinal New [469/446] Labial and lingual Lower incisors
Zealand 32Slutzkey& Levin 2007 303 subjects (14.6%) (1.6%) GR = 1-2 mm Past orthodontic Dental plaque,Cross-sectional Israel [126/177] Male > female (79.5%), treatment and oral gingivitis,
18-22 Labial surface GR > 3 mm piercing (Fisher smoking(20.5%) exact test and
Pearson chi-squaretest, P<0.01)
Toker&Ozdemir 2008 831 subjects (78.2 %) (17.4%) GR = 3-4 mm Age, high fraenum, -Cross-sectional Turkey [294/537] Male > female Maxilla < Mandible (0.8 %), traumatic tooth-
15-68 (P<0.05) (P<0.05) GR > 5 mm brushing, smoking(32.2 ± 11.7) Labial and lingual Mandibular (0.2%) duration (multiple
incisors and right regression model,canine P<0.05), male
gender, dental plaque and calculus-
Sarfati et al. 2010 2074 subjects (84.6 %) 2-5 teeth with GR GR = 1-3 mm Age, male gender, Diabetes,Cross-sectional France [1017/1057] Labial (29.2% subjects) (76.9 %), number of missing increase of body
35-65 (49 ± 9) 6-9 teeth with GR GR = 4-5 mm teeth, plaque mass index,(20.5% subjects) (5.9 %), index, gingival alcohol intake,> 10 teeth with GR GR > 6 mm bleeding index, dental visits(24.6% subjects) (1.8 %) tobacco
consumption (multiple regression model, P<0.05)
Chrysantha- 2011 344 GR patients Labial Maxillary molars Classification Tooth-brush type -kopoulos et al. Greece [165/179] of Miller: and brushingCross-sectional 18-68 I (79.4%), method, dental
(46 ± 3.8) II (15.3%), plaque andIII (4%), gingival
IV (1.2%) inflammation,malpositioned teeth (chi-square test, P<0.05)
Nguyen-Hieu This study 120 dental students 87/120 (72.5%) 362/3269 (11.1%) GR = Keratinised High fraenumet al. Vietnam [60/60] Male < female Maxilla > Mandible 1.0-3.2 mm, gingiva (Pearson attachmentCross-sectional 19-25 Labial (P<0.01) Most serious: correlation,
(22.3 ± 2.0) Premolars Upper right t-test, andcanines chi-square test,
(1.9 ± 1.2 mm) P<0.001), toothand lower malposition
right canines (chi-square test,(1.9 ± 1.3 mm) P<0.001)
Table 2. Studies of prevalence extent, severity and associated factors of gingival recession (GR) (continued)

gival recession than females. Moreover, the propor-tion of affected teeth in the current study was statis-tically higher in the maxilla than in the mandiblewhereas two previous studies [6,13] reported anopposite finding. This contradiction could beexplained by the assessment of gingival recessionof both labial and lingual tooth surfaces in thesetwo studies. Indeed, the frequent accumulation ofcalculus on the lingual surface of lower incisorsincreased the proportion of root-surface exposurein mandible [7,13,16]. Therefore, teeth most fre-quently associated with gingival recession also var-ied according to which tooth surfaces were exam-ined. Studies assessing both labial and lingual sur-faces have usually found that the most frequentlyaffected teeth were mandibular incisors [6,7,13,14,16] whereas studies assessing only labial sur-faces have suggested premolars or upper firstmolars as most frequently associated with gingivalrecession [8,9,11,12,19]. Accordingly, maxillaryand mandibular premolars were most frequentlyassociated with gingival recession in the currentstudy. The narrowest width of keratinised gingivawas also found in premolar regions. Moreover, thestudy of Joshipura et al. (1994) suggested that gin-gival recession might be due to tooth-brushingforce in premolars or debris/calculus accumulationin molars [28]. A significant negative correlationhas also been found between gingival recession anddental plaque [29]. However, the role of calculus asan aetiological factor or consequence of gingivalrecession is disputed [6].
Although many studies have confirmed theinfluence of toothbrush type, tooth-brushingmethod and tooth-brushing frequency on the inci-dence of gingival recession [5,8,9,13,18,19], a sys-tematic review by Rajapakse et al. (2007) conclud-ed that data to support or refute this relation wereinconclusive [30]. The highest level of evidenceleading to this conclusion was presented in just oneabstract of an industry-sponsored randomised con-trolled clinical trial and after presentation at a sci-entific conference, this full trial had not been pub-lished [31]. Interestingly, in the current study it wasobserved that the most serious gingival recessionwas found in right canines of both the maxilla andthe mandible. According to the evaluation of root-surface exposure in left- and right-handed adults,Tezel et al. (2001) suggested the relationshipbetween gingival recession and the hand used intooth-brushing. In right-handed subjects, denudedroot surfaces were frequently detected in premolar
and canine regions of upper right and lower rightarches. A similar result was also observed in left-handed subjects: gingival recession was usuallydetected in their upper left and lower left arches[32]. The majority of Vietnamese dental studentswere right-handed, used soft/medium toothbrushesand had a good level of oral hygiene. This suggest-ed a correlation between gingival recession andtooth-brushing. Moreover, because of the transi-tional site between anterior and posterior teeth, thespecific position of canines in dental arch couldmake them more susceptible to traumatic tooth-brushing. Although subjects with periodontitis, orthose who had undergone or had periodontal sur-gery, orthodontics, fixed prostheses and smokingwere excluded from this study, other triggering/aggravating factors including traumatic tooth-brushing and non-carious cervical lesions (abra-sion, erosion) may be risks for bias. Indeed, tooth-brushing and an acidic diet are probably related toboth tooth wear and dentine hypersensitivity andmay be associated with gingival recession that istermed "healthy recession" [1]. Traumatic tooth-brushing can cause superficial damage of the gingi-va usually termed "gingival abrasions". However,the relevance of this phenomenon to gingival reces-sion remains unclear [33]. Nevertheless it is clearthat toothbrush abrasion may cause wear at theCEJ, resulting in the destruction of the supportingperiodontium and leading to gingival recession[34].
Localising the MGJ was facilitated by mucosastaining with 3% Lugol's iodine solution. Indeed,Lugol staining has been widely used to detectmalignant changes in the cervix uteri and theoesophagus [35], and recently has been used todetect epithelial dysplasia in oral mucosa [36]. Thisstaining produced a red-brown colour based on thereaction of iodine with glycogen granules of oralmucosa whereas content glycogen was inverselyrelated to degree of keratosis, leading to keratinisedgingiva unstained with Lugol's iodine solution[35,36]. This iodine solution has also been used tomeasure the width of keratinised gingiva in previ-ous studies [20,37]. Lang and Löe (1972) foundthat in areas with less than 2 mm of keratinised gin-giva, inflammation persisted in spite of effectiveoral hygiene and they suggested that at least 2 mmof keratinised gingiva was necessary to maintaingingival health [37]. Only one longitudinal studyhas demonstrated that in patients maintaining prop-er plaque control, lack of an adequate zone of
141
OHDM - Vol. 11 - No. 3 - September, 2012

142
OHDM - Vol. 11 - No. 3 - September, 2012
attached gingiva did not result in the increased inci-dence of gingival recession [20] whereas severalcross-sectional studies have confirmed a correla-tion between the decreased width of keratinised/attached gingiva and soft-tissue recession [12,38].In the current cross-sectional study, statistical testsshowed a strong negative correlation between thelack of keratinised gingiva and root-surface exposurein subjects with good oral hygiene. Additionally,teeth with narrow width of keratinised gingiva hada statistically higher prevalence of gingival reces-sion than teeth without. However, it cannot be con-cluded from these findings that a narrow width ofkeratinised gingiva was a cause or a consequenceof gingival recession. Further longitudinal studiesare required to investigate this question.
Malaligned teeth had a statistically higher pro-portion of root-surface exposure than those in anormal position. This finding was in accordancewith previous studies [15,18,19]. It was seen thattooth malposition, including rotation and lingualinclination, was usually associated with soft debrisretention and calculus because of difficult accessduring tooth-brushing. Labially inclined teeth wereoften susceptible to traumatic tooth-brushing andappeared to be more susceptible to non-carious cer-vical lesions. Furthermore, if a tooth erupts close tothe MGJ, there is probably very little or no kera-tinised gingiva labially and then gingival recessioncan occur [3].
In the current study, no correlation was foundbetween high fraenal attachment and root-surfaceexposure. This finding was similar to that from astudy in France which also showed a low propor-tion (3%) of affected teeth with high fraenal attach-ments [12]. However, high fraenal attachmentshave been reported as significantly associated withgingival recession in two previous studies [13,18].It has been suggested that gingival/papillary fraenalattachments could impede access for plaqueremoval [13] and that fraenal pull due to lack ofattached gingival is also a factor causing gingivalrecession [18]. Although the fraenal attachment hasbeen reported as influencing plaque accumulationand gingivitis [39], in well-motivated individualswith good oral hygiene (such as the dental studentswho took part in the current study) this influencingfactor for gingival recession can be reduced oreliminated. A key finding in the current study wasthat 60.5% of teeth related to gingival recession did
not appear to be associated with predisposing fac-tors. Therefore, further studies will be needed toinvestigate the issue further.
ConclusionsThis pilot study performed in a small population ofdental students with high awareness of dental caremay not be representative of the whole populationof the Vietnamese young adults. However, somepreliminary conclusions may be drawn:
• A high prevalence of gingival recession(72.5%) was found in 19-25 year-oldVietnamese dental students with 11.1%extent of affected teeth.
• The proportion of root-surface exposurewas statistically higher in the maxilla(12.5%) than in the mandible (9.6%).
• Premolars were most frequently associatedwith gingival recession and right canineswere the most severely affected teeth.
• There was a strong negative correlationbetween a narrow width of keratinised gin-giva and soft-tissue recessions.
• Root-surface exposure was statisticallyassociated with tooth malposition.
• Gingival recession was not associated withhigh fraenal attachment and gender.
Further studies performed in a larger popula-tion of non-dental students with more extended agegroups are required to confirm these findings.
AcknowledgementsThe authors would like to thank Dr. Trong-HungHoang (Department of Community Dentistry,Faculty of Odonto-Stomatology, University ofMedicine and Pharmacy of Ho Chi Minh City,Vietnam) for the statistical analysis.
Author contributions• T N-H and B-D H-T conceived and
designed the study.• B-D H-T and H D-T performed the clinical
examinations.• T N-H and H T-G wrote the paper.
Conflict of interest and source of fundingThe authors declare that they have no conflicts
of interest and no funding source.

143
OHDM - Vol. 11 - No. 3 - September, 2012
References1. Addy M. Tooth brushing, tooth wear and dentine
hypersensitivity: are they associated? International DentalJournal. 2005; 55: 261-267.
2. Kassab MM, Cohen RE. The etiology and prevalenceof gingival recession. Journal of the American DentalAssociation. 2003; 134: 220-225.
3. Tugnait A, Clerehugh V. Gingival recession: its signif-icance and management. Journal of Dentistry. 2001; 29: 381-394.
4. Borghetti A, Monnet-Corti V. Récessions gingivales[Gingival recession]. In: Borghetti A, Monnet-Corti V, editors.Chirurgie plastique parodontale [Periodontal PlasticSurgery]. 2nd ed. Rueil-Malmaison, France: Editions CDP;2008: p. 77-95. French
5. Khocht A, Simon G, Person P, Denepitiya JL. Gingivalrecession in relation to history of hard toothbrush use. Journalof Periodontology. 1993; 64: 900-905.
6. Marini MG, Greghi SL, Passanezi E, Sant’ana AC.Gingival recession: prevalence, extension and severity inadults. Journal of Applied Oral Science. 2004; 12: 250-255.
7. Susin C, Haas AN, Oppermann RV, Haugejorden O,Albandar JM. Gingival recession: epidemiology and risk indi-cators in a representative urban Brazilian population. Journalof Periodontology. 2004; 75: 1377-1386.
8. Checchi L, Daprile G, Gatto MR, Pelliccioni GA.Gingival recession and toothbrushing in an Italian School ofDentistry: a pilot study. Journal of Clinical Periodontology.1999; 26: 276-280.
9. Kozlowska M, Wawrzyn-Sobczak K, Karczewski JK,Stokowska W. The oral cavity hygiene as the basic element ofthe gingival recession prophylaxis. Roczniki AkademiiMedycznej w Bialymstoku. 2005; 50 Suppl 1: 234-237.
10. Sarfati A, Bourgeois D, Katsahian S, Mora F,Bouchard P. Risk assessment for buccal gingival recessiondefects in an adult population. Journal of Periodontology.2010; 81: 1419-1425.
11. Serino G, Wennstrom JL, Lindhe J, Eneroth L. Theprevalence and distribution of gingival recession in subjectswith a high standard of oral hygiene. Journal of ClinicalPeriodontology. 1994; 21: 57-63.
12. Tenenbaum H. A clinical study comparing the widthof attached gingiva and the prevalence of gingival recessions.Journal of Clinical Periodontology. 1982; 9: 86-92.
13. Toker H, Ozdemir H. Gingival recession: epidemiol-ogy and risk indicators in a university dental hospital inTurkey. International Journal of Dental Hygiene. 2009; 7: 115-120.
14. Thomson WM, Broadbent JM, Poulton R, Beck JD.Changes in periodontal disease experience from 26 to 32 yearsof age in a birth cohort. Journal of Periodontology. 2006; 77:947-954.
15. Arowojolu MO. Gingival recession at the UniversityCollege Hospital, Ibadan: prevalence and effect of some aetio-logical factors. African Journal of Medicine and MedicalSciences. 2000; 29: 259-263.
16. van Palenstein Helderman WH, Lembariti BS, vander Weijden GA, van ‘t Hof MA. Gingival recession and itsassociation with calculus in subjects deprived of prophylacticdental care. Journal of Clinical Periodontology. 1998; 25: 106-111.
17. Slutzkey S, Levin L. Gingival recession in youngadults: occurrence, severity, and relationship to past orthodon-
tic treatment and oral piercing. American Journal ofOrthodontic and Dentofacial Orthopedics. 2008; 134: 652-656.
18. Dodwad V. Aetiology and severity of gingival reces-sion among young individuals in Belgaum district in India.Annals of the Dental University of Malaya. 2001; 8: 1-6.
19. Chrysanthakopoulos NA. Aetiology and severity ofgingival recession in an adult population sample in Greece.Dental Research Journal (Isfahan). 2011; 8: 64-70.
20. Wennstrom JL. Lack of association between width ofattached gingiva and development of soft tissue recession. A 5-year longitudinal study. Journal of Clinical Periodontology.1987; 14: 181-184.
21. Greene JC, Vermillion JR. The Simplified OralHygiene Index. Journal of the American Dental Associaiton.1964; 68: 7-13.
22. Placek M, Skach M, Mrklas L. [Problems with the lipfrenulum in parodontology. I. Classification and epidemiologyof tendons of the lip frenulum]. Ceskoslovenská Stomatologie.1974; 74: 385-391.
23. Maynard JG, Wilson RD. Diagnosis and managementof mucogingival problems in children. Dental Clinics of NorthAmerica. 1980; 24: 683-703.
24. Closs LQ, Grehs B, Raveli DB, Rosing CK.Occurrence, extension, and severity of gingival margin alter-ations after orthodontic treatment. World Journal ofOrthodontics. 2008; 9: e1-e6.
25. Muller HP, Stadermann S, Heinecke A. Gingivalrecession in smokers and non-smokers with minimal periodon-tal disease. Journal of Clinical Periodontology. 2002; 29: 129-136.
26. Koke U, Sander C, Heinecke A, Muller HP. A possi-ble influence of gingival dimensions on attachment loss andgingival recession following placement of artificial crowns.International Journal of Periodontics and RestorativeDentistry. 2003; 23: 439-445.
27. Daprile G, Gatto MR, Checchi L. The evolution ofbuccal gingival recessions in a student population: a 5-year fol-low-up. Journal of Periodontology. 2007; 78: 611-614.
28. Joshipura KJ, Kent RL, DePaola PF. Gingival reces-sion: intra-oral distribution and associated factors. Journal ofPeriodontology. 1994; 65: 864-871.
29. Addy M, Mostafa P, Newcombe RG. Dentine hyper-sensitivity: the distribution of recession, sensitivity and plaque.Journal of Dentistry. 1987; 15: 242-248.
30. Rajapakse PS, McCracken GI, Gwynnett E, SteenND, Guentsch A, Heasman PA. Does tooth brushing influencethe development and progression of non-inflammatory gingivalrecession? A systematic review. Journal of ClinicalPeriodontology. 2007; 34: 1046-1061.
31. Matthews DC. No good evidence to link toothbrush-ing trauma to gingival recession. Evidence-Based Dentistry.2008; 9: 49.
32. Tezel A, Canakci V, Cicek Y, Demir T. Evaluation ofgingival recession in left- and right-handed adults.International Journal of Neuroscience. 2001; 110: 135-146.
33. Addy M, Hunter ML. Can tooth brushing damageyour health? Effects on oral and dental tissues. InternationalDental Journal. 2003; 53 Suppl 3: 177-186.
34. Litonjua LA, Andreana S, Bush PJ, Cohen RE.Toothbrushing and gingival recession. International DentalJournal. 2003; 53: 67-72.

144
OHDM - Vol. 11 - No. 3 - September, 2012
35. Ohta K, Ogawa I, Ono S, Taki M, Mizuta K,Miyauchi M, et al. Histopathological evaluation includingcytokeratin 13 and Ki-67 in the border between Lugol-stainedand -unstained areas. Oncology Reports. 2010; 24: 9-14.
36. Umeda M, Shigeta T, Takahashi H, Minamikawa T,Komatsubara H, Oguni A, et al. Clinical evaluation of Lugol’siodine staining in the treatment of stage I-II squamous cell car-cinoma of the tongue. International Journal of OralMaxillofacial Surgery. 2011; 40: 593-596.
37. Lang NP, Loe H. The relationship between the width
of keratinized gingiva and gingival health. Journal ofPeriodontology. 1972; 43: 623-627.
38. Goutoudi P, Koidis PT, Konstantinidis A. Gingivalrecession: a cross-sectional clinical investigation. EuropeanJournal of Prosthodontic and Restorative Dentistry. 1997; 5:57-61.
39. Addy M, Dummer PM, Hunter ML, Kingdon A,Shaw WC. A study of the association of fraenal attachment, lipcoverage, and vestibular depth with plaque and gingivitis.Journal of Periodontology. 1987; 58: 752-757.