gender and health-related attitudes: the role of a macho ... · 238 m. sieverding / gender and...
TRANSCRIPT
Heart Disease: Environment, Stress and GenderG. Weidner et al. (Eds.)lOS Press, 2002
237
Gender and Health-related Attitudes: TheRole of a "Macho" Self-concept
)
Monika SieverdingFreie Universität Berlin, Institut für Arbeits-, Organisations- und Gesundheitspsychologie
Berlin, Germany
Abstract. This article discusses two studies examining the relationship of a"macho" self-concept and health-relevant variables. A macho self-concept wasoperationalized through its similarity to a "Marlboro man" prototype, which hadbeen assessed in a prior study. The first study was conducted with medical studentsand physicians and assessed their motivation to participate in a stress managementcourse in relation to their self-concept. The second study tested the hypothesis that amacho self-concept influences self-ratings ofhealth and physical symptoms amongEast and West German university students. Results ftom both studies support thehypothesis that a macho self-concept is strongly related to variables associated withill health. This association was more pronounced among men than among women.
Keywords: gender roles; health attitudes, health behavior, physical symptoms,self-concept
1. Introduction
Behavioral factors, especial1ythe higher prevalence of negative health behavior in men, areseen as fundamental causes in the etiology of gender differences in health and illness [1,2].In general, men tend to engage in more health-risk behaviors than women, such assmoking, using guns, heavy drinking, using illicit drugs, and reckless driving [3,4,5,6].Complementing this tendency, fewer men than women engage in positive .or preventivehealth behaviors (with the exception of men's greater physical activity). Women showhealthier behaviors than men do across a wide range of activities, such as ftuitconsumption, regular blood pressure check-ups, and health care utilization [2,7].
Gender roles appear tobe very closely related to gender differences in health-related behavior. In her cultural and historical review of gender- and health-relatedbehavior, Waldron conc1uded that "gender differences in specific types of health-relatedbehavior are strongly influenced by the compatibilityof the behavior with general sex rolesand expectations concerning appropriate male and female behavior" [3, p. 204, see alsoWaldron in this volume]. .
The question is how gender roles influence the health-related behavior of a person,because identification with societal gender roles varies considerably among individuals ofthe same sex. In this aitic1e the gender role self-concept is proposed as the mainpsychological mediating variable. The gender role self-concept can be defined as aperson's identification with personal attnDutes that are seen as appropriate for a typicalman or woman in a given society. This gender role self-concept is often operationalized byself-description scales, such as the Personal Attributes Questionnaire [8] or the Bem SexRole Inventory [9]. The similarity ofthe self-concept with a special societal male or femaleprototype is introduced in this article as an alternative and promising way ofoperationalization.
238 M. Sieverding / Gender and Health-Related Attitudes
To explaIDthe altogether more negative health behavior ofmen, identificationwitha traditionally male ''macho'' stereotype, characterized by strength, independence, andwillingness to take risks, is assumed to be particularly relevant. JuSt as :fustand hazardousdriving or high alcohol consumption is seen as ''manly'' [10], preventive behavior such asthe use ofprofessional help might weIl be seen as ''unmanly.'' Similarly,it could be seen as"umnanly" to suffer ftom physical symptoms. In this chapter, two studies are presentedthat investigate the role of a ''macho'' self-concept on (a) the motivation to engage in aspecific type ofpreventive behavior, and on (b) self-rated physicalsymptoms.
2. Study 1: Gender difTerences in preventive health behavior: Is it "unmanly" toparticipate in stress management training?
Preventive health behavior displays substantial gender differences. There are, for example,significant differences in how men and women use medical examinations for theprevention and early detection of illness. As shown in the Health Report for Germany, in1995 48 % (West: 49 %, East: 43 %) ofall women in Germany, but only 14 % ofall menin Germany (West: 15 %, East 10 %) who wereentitled to a fteepreventive examinationfor early cancer detection actually took advantage of it. Between 1985 and 1995 thepercentage of women who participated in the ftee cancer exam climbed steadily,while thepercentage ofmen who participated showed only a slight increase [11].
The situation with measures for health consultation and health promotion is quitesimilar. As mandated by new social welfare legislation, in the late 1980s and early 1990sGerman health insurance providers offered a broad palette of measures to promote goodhealth, especially in the areas of nutrition, movement, non-smoker training, relaxation, andstress management. In 1992, such courses attracted 160,000 individuals insured by oneprovider (Barmer Ersatzkasse); only a minority, however, were men. The share of womenaveraged 86 %. The share of men varied ftom 6 % in nutrition courses to 15 % in courseson movement training and 16 % in stress management training, and peaked at 35 % in non-smoker training [12]. Analyses of participation quotas for other insurance providers invarious German cities yield similarresults [13].
In order to assess the significanceof a macho self-concept for preventive behavior,I selected the example of individual motivation to participate in stress managementtraining [14]. Stress in:fIuencesthe etiology and maintenance of illness in various ways,such as through alterations in health-related behavior or increased physioiogical reactivity[15]. Stress management training is concemed with analyzing the sources of stress,replacing ineffective coping strategies with more effective ones, and learning how toregulate stress-related psycho-physiological agitation, for example, through relaxationexercises. . .
It is necessary here for the individual to admit that he or she needs help, and bewilling to talk about emotions and problems. The classic male stereotype is irreconcilablewith such behavior. Most societies de:6neindependence, achievement, power, and strengthas masculine qualities [16,17]. I thus assumed that a man with a traditionally masculineself-concept (what one could also call a "macho" man) would be less motivated toparticipate in a stress management course than an average man (or even men called"softies" in Germany). The "Marlboro man," a familiar figure ftom movie-theatercommercials (twenty minutes of commercials before a movie is common in Germany) andbillboards, offers a visible and concrete.. embodiment of thetraditional image ofmasculinity.
M. Sieverding I Gender and Health-Related Attitudes 239
2.1 Method
2.1.1 Procedure
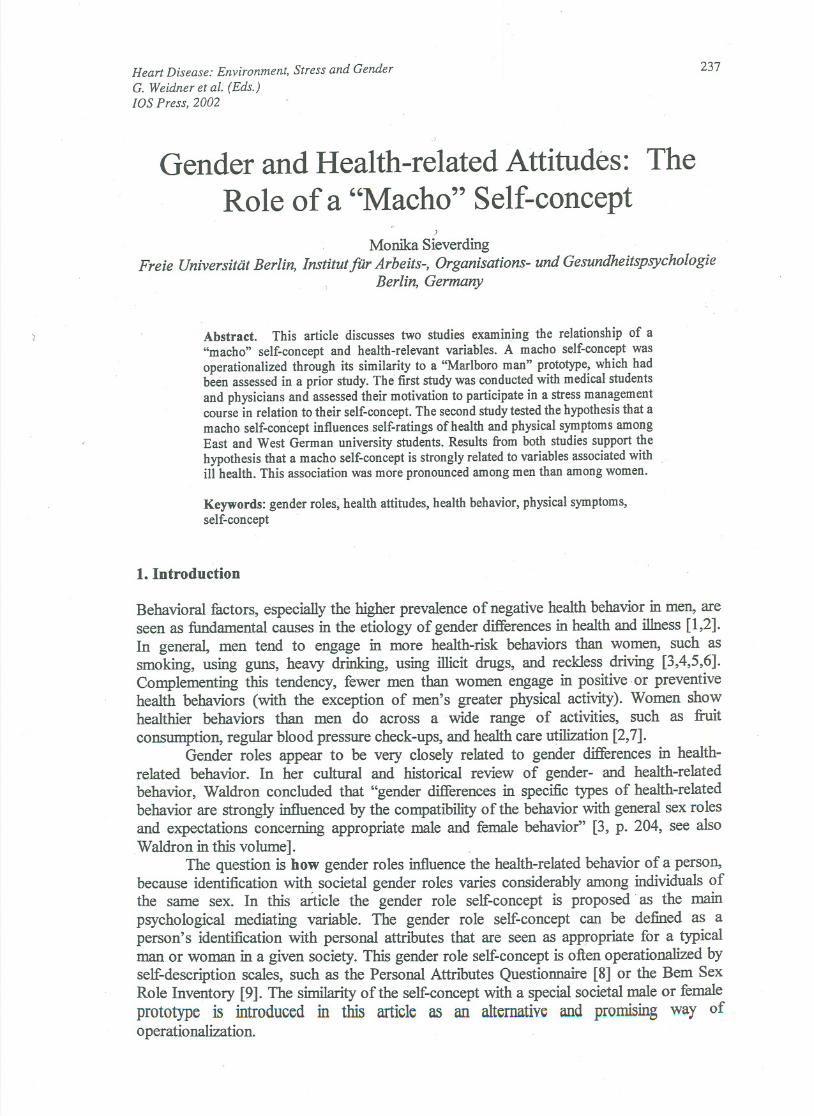
In a previous study, the prototype ofthe ''Marlboro man" was determinedIToma sample ofmale and female participants (N = 68, mean age: M = 28 years, SD = 8) by means of asemaritic differential (see reference 14 for more details). As expected, the "Marlboro man"prototype received high scores for typically masculine traits such as independent, secure,not anxious, self-sufficient, strong, aridmanly(see Figure 1).
independent
tense
dependentinsecurerelaxed
secure
anxious
self-sufficient
not anxious
helpless
weak
healthy
strongsiek
gentlecalm
0
masculine
not cool
feminine
cool
confident
successful
not confident
unsuccessful
6
~Mean Scores
roughdistressed
10
Figure 1. The "Marlboro man" prototype: Results ofthe pre-study
In the main study (N = 161), physicians at a university hospital (male and female,age: M = 37 years, SD = 7) and medical students (age: M = 23 years, SD = 4) were askedto complete a questionnaire on "stress and stress management." They were asked abouttheir usual workweek (in hours) and subjective stress ITequency(in the last year) on an 11-level scale ranging ITom 0 ("almost never") to 10 ("almost always"). Each individualwasalso asked to rate his or her motivation to participate in a stress management course bymeans of an lI-level seale ranging ITom0 (''no, by no means") to 10 (''yes, by all means").Their self-concept was assessed by means of the same semantic differential used in theprevious study. The similarity (or dissimilarity) between self-concept and the "Marlboroman" prototype was determined on the basis ofthe Cronbach and Gleser procedure [18] forcomparmg profiles:
Discrepancy between self-concept (SC) and Marlboro man prototype (MM):2 . 2
D (SC-MM) = L(XiMM- XiSC).
Here the mean scores ITom the pre-study (xiMM)were used to calculate thedifference between self-concept and "Marlboro man." The discrepancy score wascalculated across all pairs of traits with the exception of the pair "masculine- feminine."The inclusion of these traits would have artificially enlarged the gender variation in the2 '
differential scores. The larger the discrepancy sqpre D (SC-MM), the larger thediscrepancy is between self-concept and the ''Marlboro man" prototype. The smaller thediscrepancy score, the greater the similarity is between self-concept and the "Marlboroman" prototype. The similarity ~tween self-concept and the "Marlboro man" stereotype
240 M. Sieverding / Gender and Health-Related Attitudes
(as defined in the pre-study) served to operationalize a "macho" self-concept. (For adetailed description ofthe study see reference 14).
.2.2 Results
The general evaluation modus for the mean-score comparison of the four groups underinvestigation was two-factorial variance analyses with the factors sex andprofessionalstatus (medical students versus physicians). Overall, the participants feIt that they hadfrequently been under stress in the last year (M = 6.4, SD = 2.4). As expected, professionalstatus was significant in both analyses. Physicians reported a higher number of hoursworked per week than didstudents, M = 56.5, SD = 9.1 for physicians versus M = 33.0,SD = 13.0 for students, F(l,149) = 165.6, P < .001. Physicians experienced stress moreoften, M = 6.9, SD = 2.3 versus M = 5.9, SD = 2.4 for students, F(l,155) = 5.4, P < .05.
Sex was not significant for either the number of hours worked per week or forsubjective stress frequency. In motivation for participating in stress management,however,sex turned out to be a significant main effect. Men were elearly less motivated than womento participate in such a course (men: M = 3.9, SD = 3.2; women: M = 5.4, SD = 3.2;F(l,157) = 9.21, P < .01). Sex was also a significant main effect in the discrepancy score
D\SC-MM}; the discrepancy scores were significantly smaller for men (M = 83.2 SD =51.7) than for women (M = 99.4, SD = 57.4), F(l,155) = 4.2, P < .05. In other words, indescribing their self-concept, men came eloser to the "Marlboro man"than did women.
To check the hypothesis that a self-concept similar to the MM prototype was asignificant predictor of motivation to participate in a stress management course, we used ahierarchical multiple regression analysis to leam if the effects of the variables positivelycorrelated with motivation to artend the course. The sociodemographic variables sex andprofessional status were entered in step 1, and subjective stress frequency in step 2. Thediscrepancy between self-concept and the "Marlboro man" prototype was entered in step 3.In the final step, the two-fold interactions (sex or professional status) were entered with thediscrepancy variable from step 3. The results of this regression analysis are presented inTable 1.
Table 1. Hierarchical regression predicting motivationto participate in stress management training
1. Sociodemographic variables
Sexa
Step Variables
2.
3.
4.
Professional status
Subj. stress :&equency
D2(SC-MM)
Interactions
Sex x D2(SC-MM)
Status x D2(SC-MM)
Note. * p < .05; acodification of sex: 1 = male, 2 = female; for regression, beta and t are at final step.R2reflects increment in R2at time of entry.
R2 Beta
.05
.17 2.2*
< 1
.10 .16 2.1*
.14 .18 2.3*
.17
-.15 -2.0*
-1.8

M. Sieverding / Gender and Health-Related Attitudes 241
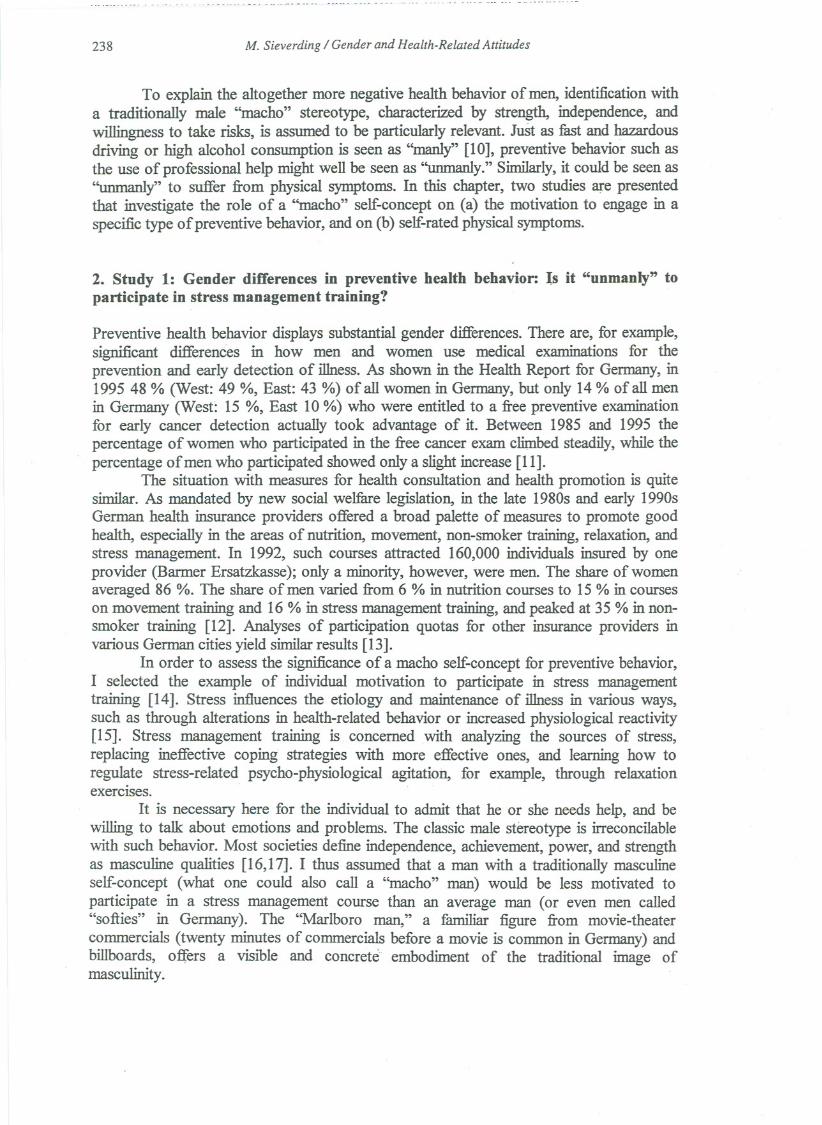
The two sociodemographic variables were able to explain only 5 % of the overallvariance in motivation to participate in a stress management course. The variable.of sexwas the significant predictor. By including the variable of stress frequency, R2 increased to.10. Another significant predictor for explainingthe variance was the discrepancybetweenself-conceptand the "Marlboroman" prototype. The greater this discrepancy- in otherwords, the less the subject's self-concept resembled the MM prototype - the greater themotivation to participate in stress management training. By including the interactions instep 4, the explained variance could be increased further (to R2 = .17). The interactionbetween sex and the discrepancy between self-concept and the "Marlboro man" prototypewas significant;the meaning ofthis interaction is illustrated in Figure 2.
G 8
/I~Men Ifj-Women
similar to dissimilar to"Marlboro Man" "Marlboro Man"
Self.concept
Figure 2. .Motivation to participate in stress management training as a function of the interactionbetween sex and similarity of self-concept to the "Marlboro man" prototype; possible answers from 0("no, by no means") to 10 ("yes, by aII means")
The sampie was divided into two groups (MED = 78) by means of mediandichotomization of the variable discrepancy between s~lf-concept and the MM prototype,D2(SC-MM). The motivation to take a stress management course was dependent only formen on the similarity between self-concept and the MM prototype. Those men whose self-concept resembled the "Marlboro man" (= below average discrepancy scores) expressed aclearly lower motivation than did men whose self-concept was not similarto MM (= aboveaverage discrepancy scores). For women, in contr~st, we find that the discrepancybetweenself-concept and MM did not affect their motivation to take stress management training;motivation was high in both groups (see Figure 2). Separate regression analyses for eachsex confirm this result: the discrepancy between self-concept and the MM prototype was asignificant predictor ofmotivation for men only (men: beta = .31, P < .01; women: beta =.09, P = .47).
Results confirm that the motivation to sign up for a course on stress management isinfluenced by a person's perceived similarity to the "Marlboro man" prototype, but thisresult holds true for male participants only.
Motivation6
5
4
3
2

- --_u -- uc - --- ___H
242 M. Sieverding / Gender and Health-Related Attitudes
3. Study 2: Gender differences in seil-ratings of health and physical symptoms: .
"Marlboro men" do not report sutJering from physical symptoms
Self-ratings of health and physical symptoms are essential factors for assessing health-relevant behavior, such as giving up risk behaviors (quitting smoking) or initiatingpreventive behaviors (using professional help). In terms ofthe gender-specificcomparisonof subjective health, most studies - regardless of where they are conducted - find that menmore ftequently rate their health as ''very good," while womenjudge their health to be "notso good" or "bad." Over the last several years, however, these gendered differencesappearto have become far less pronounced. The majority of men and women are either satisfiedwith their health, or characterize it as good or very good. Depending on the study, thisnumber lies between 75 and 90 % [19]. -
The contrast in reports about physical symptoms is clearer than the gendereddifference in self-ratings of health [20]. One finds a larger number of symptoms amongwomen, regardless of how these are measured. One recent comprehensive review [21]summarized evidence for women's higher rates of physical symptoms ftom three differentresearch bodies: health surveys, studies on symptom reporting, and registration of healthcomplaints by physicians. -
Along with this gender difference, aseries of heaIth surveys in Germany revealedan East-West difference in physical symptoms. After the Wall came down in November,1989, aseries of surveys were conducted to analyze the German health situation bycomparing the responses of East and West residents. Investigations conducted during theyears immediately following 1989 revealed a distinctive pattern in health self-ratings. Thispattern is no longer found in recent studies; see, 'for example, [22]. Not only did EastGerman men assess their health as better overall in comparison to women in East and WestGermany, they also believed it was better than the health of West German men. EastGerman men also reported far fewer physical symptoms and complaints than did WestGerman men.
The studies conducted by the Robert Koch Institute in the early 1990s usedrepresentative sampIes ofEast and West Germans to examine subjective health restrictionsthrough 24 different physical and general symptoms based on the "symptom list" [23]commonly used in Germany. l11e sw::p.score reveals the extent to which an individualfeelsrestricted by physical and general symptoms. It can range ftom 0 to 72 points, whereby 0means that an individual "does not suffer at all" ftom any of the 24 symptoms listed and 72means that an individual "suffers severely" ftom all symptoms.,
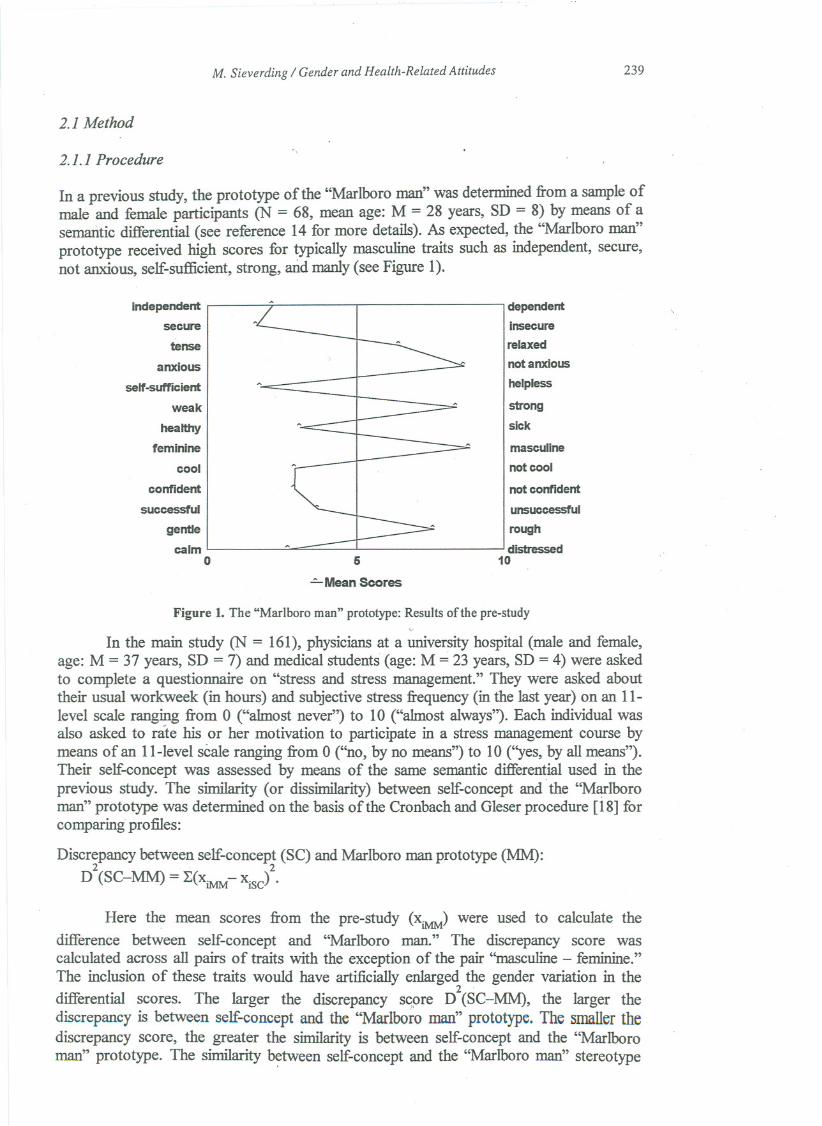
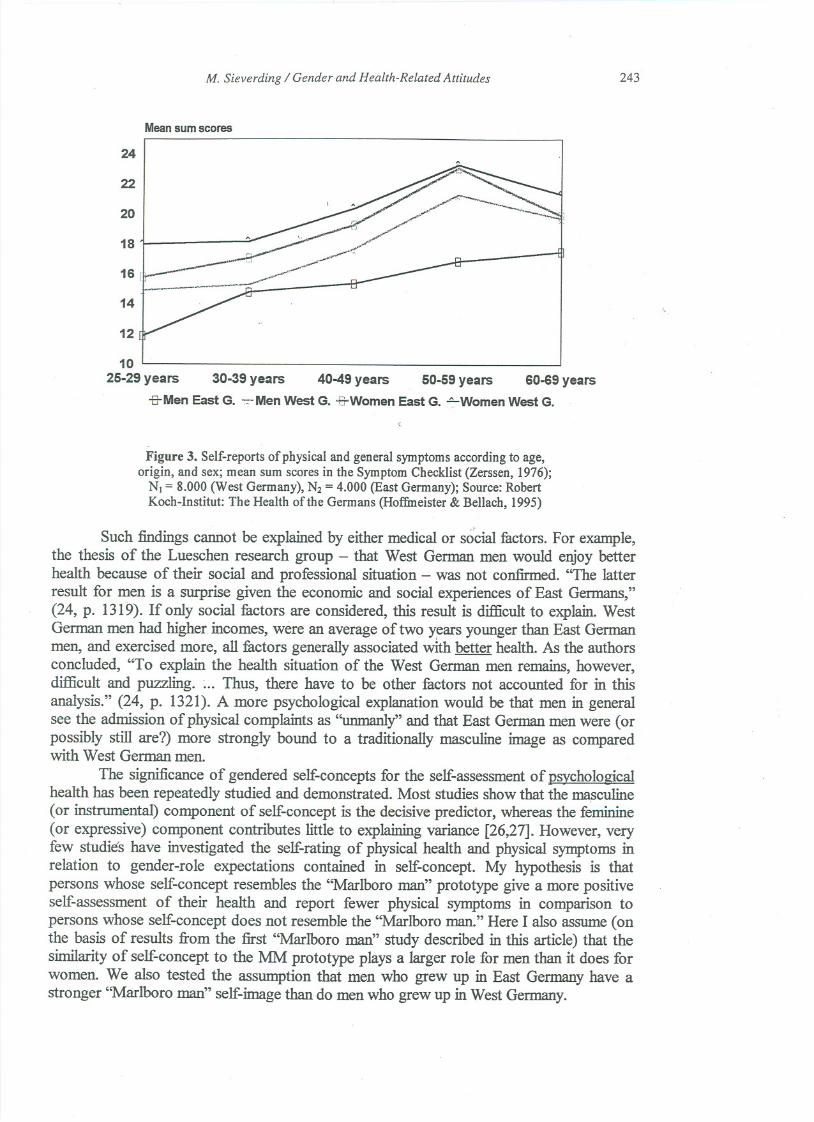
The Robert Koch studies showed that subjective health restriction was related tothree factors: sex, age, and origin (East or West Germany). The ftequency of symptomswas higher among women, older adults, and. West Germans (see Figure 3). Thecomparison of East and West German men is particularly infoImative. Whereas the patternof symptoms among West German men across all age groups resembled that ofwomen inthe sampIe (albeit at a somewhat lower level), the sYD:1ptomcurve among East Germanmen fell clearly below all other groups. Differences between East and West German menin the 30- to 40-year-old group were particularly pronounced. Here the studies foundparalleIs to other East-West comparative surveys [24,25], which also showed that EastGerman men gave a more positive overall assessment oftheir health than did West Germanmen.
M. Sieverding / Gender and Health-Related Attitudes 243
Mean sum scores
24
22
20
18
16,
't14
12
10
25-29 years 30-39 years 40-49 years 50-59 years 60-69 years-B-MenEast G. ~'Men west G. -&Women East G. ~Women West G.
Figure 3. Self-reports of physical and general symptoms according to age,origin, and sex; mean sum scoresin the Symptom Checklist (Zerssen, 1976);
NI = 8.000 (West Germany), N2= 4.000 (East Germany); Source:RobertKoch-Institut: The Health ofthe Germans (Hoffmeister & Bellach, 1995)
Such findings cannot be explained by either medical or social factors. For example,the thesis of the Lueschen research group - that West German men would enjoy betterhealth because of their sodal and professional situation - was not confirmed. "The latterresult for men is a surprise given the economic and social experiences of East Germans,"(24, p. 1319). If only social factors are considered, this result is difficultto explain. WestGerman men had higher incomes, were an average of two years younger than East Germanmen, and exercised more, all factors generally associated with better health. As the authorsconcluded, "To explain the health situation of the West German men remains, however,difficultand puzzling. ~.. Thus, there have to be other factors not accounted for in thisanalysis." (24, p. 1321). A more psychological explanation would be that men in generalsee the admission of physical complaints as "unmanly"and that East German men were (orpossibly still are?) more strongly bound to a traditionally masculine image as comparedwith West German men.
The significance of gendered self-concepts for the self-assessmentof psychologicalhealth has been repeatedly studied and demonstrated. Most studies show that the masculine(or instrumental) component of self-concept is the decisive predictor, whereas the feminine(or expressive) component contributes little to explaining variance [26,27]. However, veryfew studies have investigated the self-rating of physical health and physical symptoms inrelation to gender-role expectations contained in self-concept. My hypothesis is thatpersons whose self-concept resembles the "Marlboro man" prototype give a more positiveself-assessment of their health and report fewer physical symptoms in comparison topersons whose self-concept does not resemble the "Marlboro man." Here I also assume (onthe basis of results ITomthe first "Marlboro man" study described in this artic1e)that thesimilarity of self-concept to the MM prototype plays a larger role for men than it does forwomen. We also tested the assumption that men who grew up in East Germany have astronger "Marlboro man" self-image than do men who grew up in West Germany.

244 M. Sieverding / Gender and Health-Related Attitudes
3.1 Method
3.1.1 SampIes
The sample consisted of 471 German students. Some had grown up in East Germany untilthey entered university (101 men and 121 women), and others had grown up in WestGermany (118 men and 130 women). The participants were studying at variousuniversities in Berlin, Leipzig, and Potsdam. They were between 18 and 34 years old, withan average age ofM = 23 years (SD = 3).
3.1.2 Variables
Self-concept was measured with the semantic differential ITomthe Marlboro 1 study. The
determination of similarity between self-conce~t and the MM prototype :vas Iikewisemeasured on the basis ofthe discrepancy score D (SC-MM).
Participants were asked to rate their overall health on a five-Ievel scale rangingITom0 (''very poor") to 4 (''very good"). The Zersson symptom checklist (23) was used todetermine both general and physical symptoms. This !ist contains 24 symptoms.Participants are asked to rank how much they suffer ITom a particular symptom("severely," "somewhat," ''very little," or "not at all").
3.2 Results
First, sex and country of origin (Bast or West Germany) were checked for significantmaineffects on the variables by means of 2 x 2 ANOVAs. There were no significanteffects onself-rated health. In all foUr groups, the mean scores were relatively high (M = 3.1, SD =.7), as would be expected in a sample of young students. Tbe symptom scores showed asignificant main effect for sex: F(1,468) = 11.7, p <, .01. As shown in numerous studies,
. women participants in this study reported a higher level of symptoms (women: M = 18.6,SD = 9.6; men: M = 15.7, SD = 9.3). In the 2 x 2 ANOVA with sex and.origin as between-
subject factors and the discrepancy score D2(SC-MM) as the dependent variable, asignificantmain effect of sex emerged (women: M = 91.3, SD = 66.4; men: M = 78.4, SD= 51.1); F(1,467) = 5.84, p < .05. Men described themselves as more similar to the"Marlboro man" than women did.
Next, the scores ofthe two male groups were compared by t-tests. The mean scoresfor health and physical symptoms did not differ significantly (t's < I). In contrast, themean discrepancy scores between self-concept and the "Marlboro man" prototype diddiffer significantly: t(217) = 1.98, p < .05. The average discrepancies are significantlylower among East German men (M = 71.1, SD = 44.3) than among West German men (M= 84.7, SD = 55.8). This finding confirms the thesis that the self-concept ofEast Germanmen bears a stronger resemblance to the "Marlboro man" prototype than does the self-concept ofWest German men.
The extent to which the similarity of self-concept to the MM prototype contnoutesto the variance in self-rated health and physical symptoms was analyzed by multiplehierarchical regression analyses. The sociodemographic variables sex, age, and origin wereentered in step 1 (forced entry); the discrepancy scores were entered in step 2. In step 3,interactions ofthe discrepancy scores with the sociodemographic variableswere evaluated.
lIi both self-ratings, the discrepancy score turned out to be the most importantpredictor studied. Here only a small share of the overall variance could be explained withthe variable "self-rated health" (R2 = .06), which is certainly linked to the fact that theoverall variance in responses to this single item variable was very low. The sole significant
M. Sieverding I Gender and Health-Related Attitudes 245
predictor of self-rated health was the discrepancy between self-concept and the MMprototype (Beta = -.22, t = - 4.8, P .001). The greater the sirDiIaritywas between self-conceptandMMprototype,the higherthe ratingwasof one's ownhealth. .
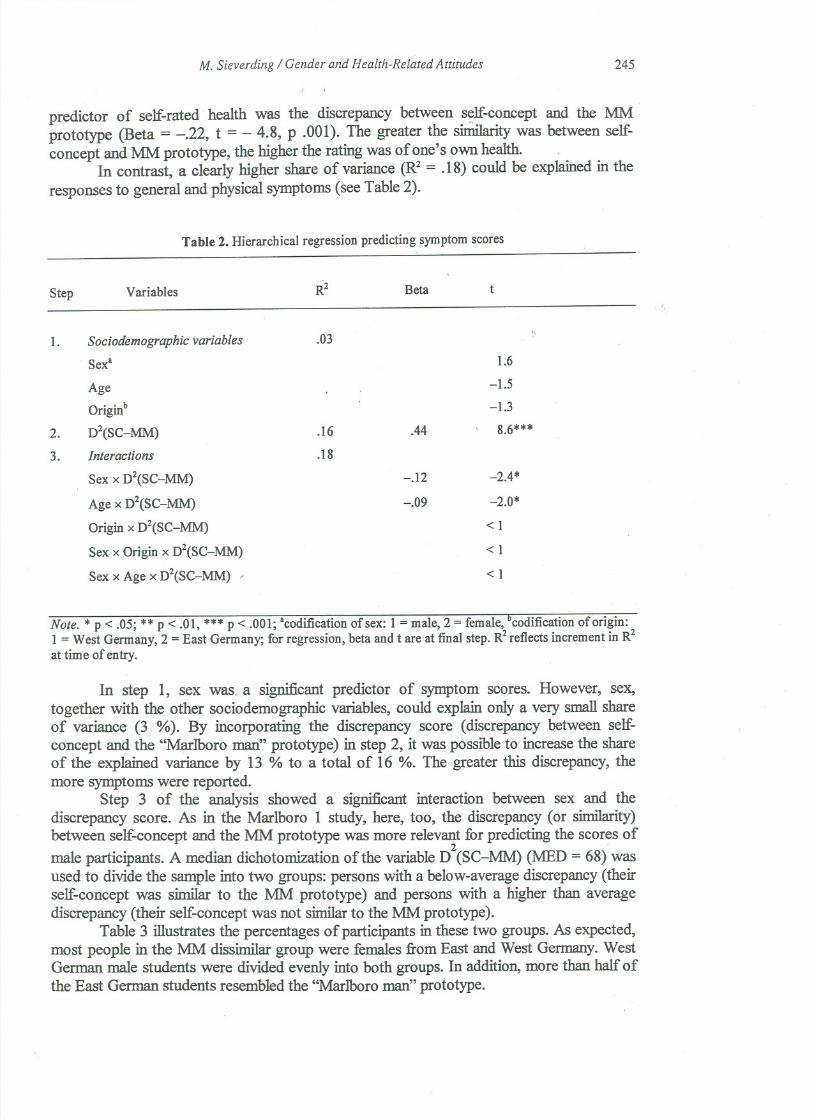
In contrast, a clearly higher share of variance (R2= .18) could be explained in theresponses to general and physical symptoms (see Table 2).
Table 2. Hierarchical regression predicting symptom scores
Step
1.
2.
3.
Note. * p < .05; ** P < .01, *** p < .001; acodificationofsex: 1 =male,2 = female,°codificationoforigin:1 = West Germany, 2 = East Germany; for regression, beta and t are at final step. R2reflects increment in R2at time of entry.
In step 1, sex was, a significant predictor of symptom scores. However, sex,together with the other sociodemographic variables, could explain only a very small shareof variance (3 %). By incorporating the discrepancy score (discrepancy between self-concept and the "Marlboro man" prototype) in step 2, it was possible to increase the shareof the explained variance by 13 % to a total of 16 %. The greater this discrepancy, themore symptoms were reported.
Step 3 of the analysis showed a significant interaction between sex and thediscrepancy score. As in the Marlboro 1 study, here, too, the discrepancy (or similarity)between self-concept and the MM prototype was more relevant for predicting the scores of
male participants. A median dichotomization ofthe variable D2(SC-MM) (J\.1ED= 68) wasused to divide the sampIe into two groups: persons with a below-average discrepancy(theirself-concept was similar to the MM prototype) and persons with a higher than averagediscrepancy (their self-concept was not similarto the MM prototype).
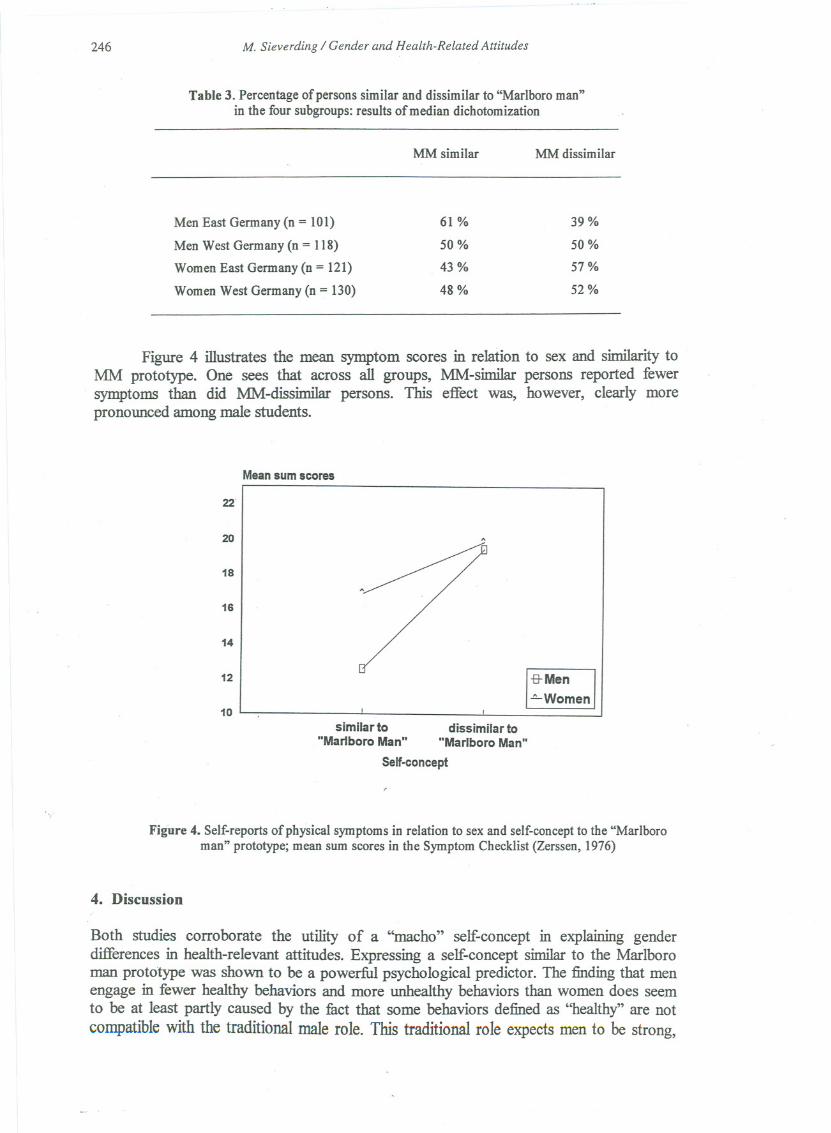
Table 3 illustrates the percentages of participants in these two groups. As expected,most people in theMM dissimilar group were females ftom East and West Gennany. WestGerman male students were divided evenly into both groups. In addition, more than half ofthe East German students resembled the "Marlboro man" prototype.
Variables R2 Beta t
Sociodemographic variables .03
Sexa 1.6
Age -1.5
Originb -1.3
D2(SC-MM) .16 .44 8.6***
Interactions .18
Sex x D2(SC-MM) -.12 -2.4*
Age x D2(SC-MM) -.09 -2.0*
Origin x D2(SC-MM) < 1
Sex x Origin x D2(SC-MM) <1
Sexx Agex D2(SC-MM) /<1
246 M. Sieverding / Gender and Health-Related Attitudes
Table 3. Percentage ofpersons similar and dissimilar to "Marlboro man"in the four subgroups: results of median dichotomization
MM similar MM dissimilar
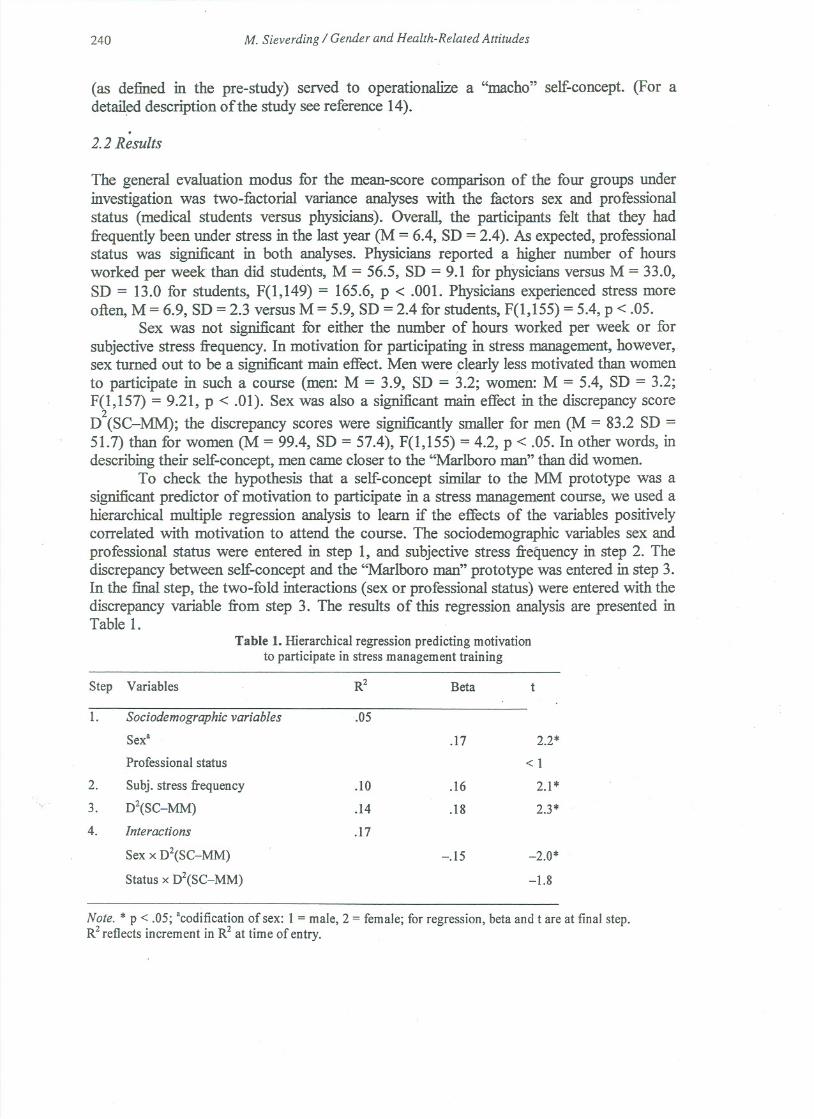
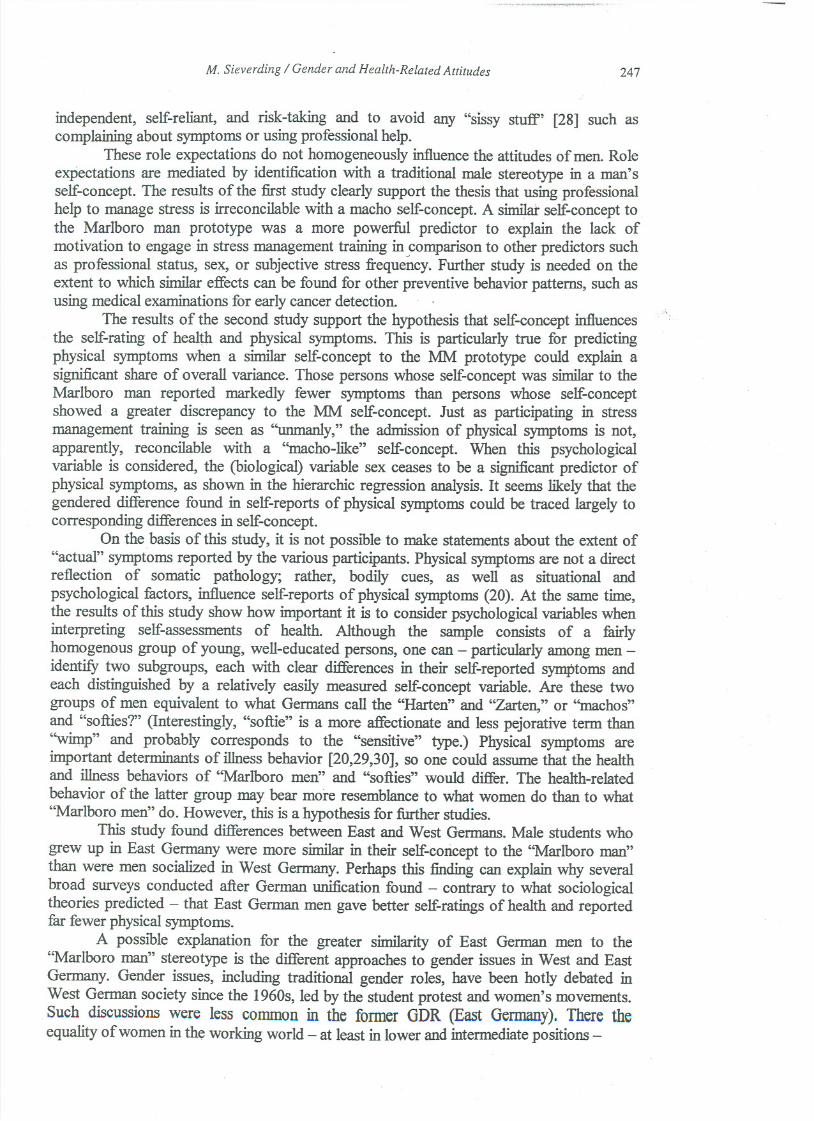
Figure 4 illustrates the mean symptom scores in relation to sex and similarity toMM prototype. One sees that across all groups, MM-similar persons reported fewer
. symptoms than did MM-dissimilar persons. This effect was, however, clearly morepronounced among male students.
Mean sum scores
22
20
.~18
16
-8-Men
~Women
14
12
10similar to dissimilar to
"Marlboro Man" "Marlboro Man"
Self-concept
Figure 4. Self-reports of physical symptoms in relation to sex and self-concept to the "Marlboroman" prototype; mean sum scores in the Symptom Checklist (Zerssen, 1976)
4. Discussion
Both studies corroborate the utility of a "macho" self-concept in explaining genderdifferences in health-relevant attitudes. Expressing a self-concept similar to the Marlboroman prototype was shown to be a powerful psychological predictor. The finding that menengage in fewer healthy behaviors and more unhealthy behaviors than women does seemto be at least partly caused by the fact that some behaviors defined as "healthy" are notcompatible with the traditionaI male role. This traditional rote expects men to be strong,
Men East Germany(n = 101) 61 % 39%
Men West Germany (n = 118) 50% 50%
Women East Germany (n = 121) 43% 57%
Women West Germany (n = 130) 48% 52%
M. Sieverding / Gender and Health-Related Attitudes 247
independent, seIf-reIiant, and risk-taking and to avoid any "sissy stuff' [28] such ascomplainingabout symptoms or using professional help.
These role expectations do not homogeneously influencethe attitudes of men. Roleexpectations are mediated by identification with a traditional male stereotype in a man'sseIf-concept. The results of the first study clearly support the thesis that using professionalhelp to manage stress is irreconcilable with a macho seIf-concept.A similat seIf-concepttothe Marlboro man prototype was a more powerful predictor to explain the lack ofmotivation to engage.in stress management training in comparison to other predictors suchas professional status, sex, or subjective stress frequency. Further study is needed on theextent to which similar effects can be found for other preventive behavior patterns, such asusing medical examinations for early cancer detection. .
The results of the second study support the hypothesis that seIf-concept influencesthe seIf-rating of healt4 and physical symptoms. This is particularly true for predictingphysical symptoms when a similar seIf-concept to the MM prototype could explain asignificant share of overall variance. Those persons whose seIf-concept was similar to theMarlboro man reported markedly fewer symptoms than persons whose seIf-conceptshowed a greater discrepancy to the MM seIf-concept. Just as participating in stressmanagement training is seen as "unmanly," the admission of physical symptoms is not,apparently, reconcilable with a "macho-Iike" seIf-concept. When this psychologicalvariable is considered, the (biological) variable sex ceases to be a significantpredictor ofphysical symptoms, as shown in the hierarchic regression analysis. It seems Iikely that thegendered difference found in seIf-reports of physical symptoms could be traced largely tocorresponding differences in seIf-concept.
On the basis of this study, it is not possible to make statements about the extent of"actual" symptoms reported by the various participants. Physical symptoms are not a directreflection of somatic pathology; rather, bodily cues, as weIl as situational andpsychological factors, influence seIf-reports of physical symptoms (20). At the same time,the results of this study show how important it is to consider psychologicalvariables wheninterpreting seIf-assessments of health. Although the sampleconsists of a fairlyhomogenous group of young, weIl-educated persons, one can - particularly among men -identi:fytwo subgroups, each with clear differences in their seIf-reported symptoms andeach distinguished by a relatively easily measured seIf-concept variable. Are these twogroups of men equivalent to what Germans call the "Harten" and "Zarten," or ''machos''and "softies?" (Interestingly, "softie" is a more affectionate and less pejorative term than"wimp" and probably corresponds to the "sensitive" type.) Physical symptoms areimportant determinants of illness behavior [20,29,30], so one could assume that the healthand illness behaviors of "Marlboro men" and "softies" would differ. The health-relatedbehavior of the latter group may bear more resemblance to what women do than to what"Marlboro men" do. However, this is a hypothesis for further studies.
This study found differences between East and West Germans. Male students whogrew up in East Germany were more similar in their seIf-coriceptto the "Marlboro man"than were men sociaIized in West Germany. Perhaps this finding can explain why severalbroad surveys conducted after German unification found - contrary to what sociologicaltheoriespredicted- that East Germanmen gave better seIf-ratingsof healthand reportedfar fewer physical symptoms.
A possible explanation for the greater similarity of East German men to the"Marlboro man" stereotype is the different approaches to gender issues in West and EastGermany. Gender issues, including traditional gender roles, have been hotly debated inWest German society since the 1960s, led by the student protest and women's movements.Such discussions were less connnon in the former GDR (East Germany). There theequaIity ofwomen in the working world - at least in lower and intermediatepositions-
.,
_u-- ------u -- -- ---
248 M. Sieverding / Gender and Health-Related Attitudes
had been realized to a far greater extent than in West Germany. The GDR promoted thelegally guaranteed equality of men and women, but it did not encourage (and sometimesprohibited) the kind of wide-ranging scholarship on women and feminist literature found inthe West. In West Germany, massive questioning of the traditional ''macho'' role,encouraged largely by women and spanning both the public and private spheres, seems tohave had an impact. Even though West German men continue to admire traditionalmasculine movie idols like Arnold Schwarzenegger and Sylvester Stallone, many menhave apparently emandpated their own self-image ITom such outdated male cliches.However, it is possible that more West German men responded in the study according tosodal expectations and thus presented themselves as less "macho" than they might actuallybe.
Hut how are the results of this study relevant to health and preventive behavior?What does it mean when "Marlboro men" are satisfied with their health and report fewsymptoms? Earlier studies attributed gender differences in self-reports on health andphysical symptoms to the idea that it was more socially acceptable for women to complain.Today the assumption might be that women have a relatively more realistic view oftheirown overall health while men, or at least some men, overestimate their health.
There is disagreement over the extent to which positive illusions might be good forhealth, but most ofthis discussion focused.on psychological and not physical health [31].Others have offered convincing arguments and empirical evidence that an illusionarypsychological health, particularly if it is boot on the defensive denial of stress, can havephysiological costs, which present a risk factor for physical health [32]. An unrealisticallypositive view of one's own physical health and ignoring or not admitting physicalsymptoms could pose a health risk. People who will not admit or accept restrietions ontheir health might assume too many professional or other burdens, and not make choices tomaintain or recover their health, such as taking breaks at work, goingon vacation, oraccessing professional help [33,34]. It is likely that an unrealistically positive view ofone's health also relates to risk behavior. I would surmise that "Marlboro men" tend toconsume higher amounts of alcohol and nicotine, and are more likely to be reckless driversthan the "softies" or ''wimps'' who are often ridiculed.
The "Marlboro man" hypothesis might also help explain the health situation of menin Eastern Europe. It again seems likely that, compared to Western Europe or the UnitedStates, there has been less questioning of traditional macho diches until now. The"Marlboro man" in Eastern Europe probably copes differently with the enormous burdensresulting ITomprofound sodal upheavals than Eastern European women and "softie" men,both in terms of risk behaviors (smoking, alcohol consumption, and reckless driving), andin terms of preventive health behaviors (such as using professional help). In the UnitedStates and, to a lesser extent, in parts ofWestern Europe, a relativelynew body ofresearchon male health is investigating the negative effects of the masculine role on health[17,35,36]. Perhaps for Eastern Europe as wen, questioning the traditional "macho" role isa necessary prerequisite for improving men's health.
" .
Acknowledgement
The author would like to thank Prof. Dr. Dorothee Alfermann for recruiting participants for the second studyITomLeipzig University.
[9]
[10]
[11][12]
[13]
[14]
[15]
[16]
[17]
[18]
[19]
[20][21]
[22]
[23][24]
[25]
[26]
[27]
[28]
M. Sieverding / Gender and Health-Related Attitudes 249
References
[I]
[2]
L.M.Verbrugge, Pathways ofhealth and death. In RD. Apple (ed.), Women,health and medidne inAmerica. New Brunswick, New Jersey: Rutgers University Press. (1990) 41-79. .
D.M. Reddy, R Fleming, and. V.J. Adesso, Gender and health. In S.Maes, H. Leventhal, and M.Johnston (eds.), International Review ofHealth Psychology, Vol. I,Chichester: Wiley. (1992) 3-32.I. Waldron, Gender and health-related behavior. In D.S. Gochman (ed.), Health behavior New York:Plenum. (1988) 193-208.I. Waldron, Changing gender roIes and gender differences in health behavior. In: D.S. Gochman(ed.), Handbook ofHealth Research I: Personal and Sodal Determinants Plenum Press, New York,NY. (1997) 303-328.I. Waldron, Trends in gender differences in coronary heart disease mortality -- Relationships totrends in health-related behavior and changing gender roles. In this volume.RL. Collins, A1cohol consumption, coping, and the gender gap in cardiovascular disease. In thisvolume (2001)A. Steptoe et al., Personality and attitudinal correlates ofhealthy and unhealthy lifestyles in youngadults. Psychology and Health (1994) 331-341.J.T. Spence and RL. Helmreich, Masculinity & femininity. Their psychological dimensions,correlates, & antecedents. Austin: University ofTexas Press. (1978).S.L. Bem, The measurement of psychoIogical androgyny. Journal of Consulting and ClinicalPsychology 42 (1974) 155-162.G. Weidner, C.W. Kohlmann, E. Dotzauer, and L.R Buros, The effectsofacademic stress on healthbehaviors in young adults. Anxiety, Stress, and Coping 9 (1996) 123-133.Statistisches Bundesamt. Gesundheitsbericht fuer Deutschland. Stuttgart: Metzler-Poeschel. (1998).R Meierjürgen and M. Schulte, Routinestatistiken im Gesundheitsrorderungsbereich: Aufgaben -Ziele - erste Ergebnisse. Zeitschrift für Präventivmedizin und Gesundheitsförderung 5 (1993) 61-66.G. Ollenschläger and A. Denecke, Prävention und Gesundheitsförderung als Aufgabe dergesetzlichen Krankenkassen - dargestellt am Beispiel einer Ortskrankenkasse. Gesundheitswesen,56 (1994) 423-429.M. Sieverding, Die Bedeutung von Prototype-Matching fuer präventives Verhalten: Ist dieTeilnahme an Streßbewältigungskursen "unmännlich"? Zeitschrift für Gesundheitspsychologie 5(1997) 272-289.A. Steptoe, The links between stress and iIIness. Journal of Psychosomatic Research 35 (1991).633-644.
J.E. Williams and D.L. Best, Measuring sex stereotypes. A multination study. Beverly Hills: Sage.(1990).F. Leafgren, Being a man can be hazardous to your health: Life-style issues. In D. Moore & F.Leafgren (eds.), Problem solving strategies and interventions for men in conflict Alexandria, VA:American Association for Counseling and Development. (1990) 265-275.L.J. Cronbach and G.C.Gleser, Assessing similarity between profiles. Psychological Bulletin 50(1953) 456-473. .
M. Sieverding, Sind Frauen weniger gesund als Männer? Überprüfung einer verbreiteten Annahmeanhand neuerer Befunde. Kölner Zeitschrift für Soziologie und Sozialpsychologie 50 (1998) 471-489.J.W. Pennebaker, Thepsychology ofphysical symptoms. New York: Springer. (1982).C.M.T.Gijsberg van Wijk, A.M.Kolk, Sex differences in physical symptoms: The contribution ofsymptom perception theory. Sodal Sdence & Medicine 45 (1997) 231-246.U. ElIert and H. Knopf, Zuftiedenheit mit Lebensumstaenden und Gesundheit. Gesundheitswesen,61, Sonderheft 2 (Schwerpunktheft: Bundes-Gesundheitssurvey (1998, 1999).SI45-S150.D. Zerssen,. v. Die Beschwerdenliste. Weinheim: Beltz. (1976).G. Lueschen et al., After unification: Gender and subjective health status in East- and West-Germany. Sodal Science & Medicine 44, 9 (1997) 1313-1323.W. Kirschner, M. Radoschewski, and R Kirschner, § 20 SBG V Gesundheitsfoerderung,Krankheitsverhütung. Untersuchung zur Umsetzung durch die Krankenkassen. St. Augustin:Asgard. (1995).V.S. Helgeson, Relation of agency and communion to well-being: Evidence and potentialexpIanations. Psychological Bulletin 116 (1994) 412-428. .
RE. Whitley, Sex-role orientation and psychological well-being: Two meta-analyses. Sex Roles 12(1985),207-225.
R.C. Brannon, No 'sissy stuff: The stigma of anythingvaguelyfeminine.In D. David& B. Brannon(eds.), Theforty-nine percent majority. Reading, MA: Addison-Wesley. (1976).
[3]
[4]
[5]
[6]
[7]
[8]

250
[29]
[30]
[31]
[32]
[33]
[34]
[35]
[36]
',.
M. Sieverding / Gender and Health-Related Attitudes
R.O. Frost, J.E. Morgenthau, C.K. Riessman, and M. Whalen, Somatic response to stress, physicalsymptoms and heaIth service use: The role of current stress. Behavior Research and Therapy 26(1988) 481-487.C.M.T. Gijsbers van Wijk, H. Huisman, and A.M. Kolk, Sex differences in physical symptoms andiIlness behavior. A heaIth diary study. Social Science & Medicine 49 (1999) 1061-1975.S.E. Taylor, J.D. Brown, Illusion and well-being: A social psychological perspective on mentalhealth. Psychological Bulletin 103 (1988) 193-210.J. Shedler, M. Mayman, and M. Manis, The illusion of mental health. American 0000 Psychologist,48 (1993) 1117-1131.C.W. Kohlmann, G. Weidner, and C.R. Messina, Avoidant coping style and verbal-cardiovascularresponse dissociation. Psychology and Health 11 (I 996) 371-384.T. Toneatto and Y.M. Binik, The body sensation hypothesis: A new contribution to theunderstanding ofpreventive health behavior. Psychology and Health 6 (1992) 1-12.J.B. Harrison, Warning: The male sex role may be dangerous to your heaIth. Journal 01 SocialIssues 34 (I978) 65-86.W.H. Courtenay, Constructions ofmasculinity and their influence on men's well-being: A theory ofgender and health. Social Science & Medicine 50 (2000) 1385-1401.