gastroenterology revision lecture
TRANSCRIPT
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 1/49
Gastroenterology
Ammad Mahmood
GUMSA Revision Lectures
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 2/49
Contents
• Peptic ulcer disease
• Coeliac disease• Alcoholic liver disease
• Obstructive jaundice
• Hepatitis
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 3/49
Peptic Ulcer Disease
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 4/49
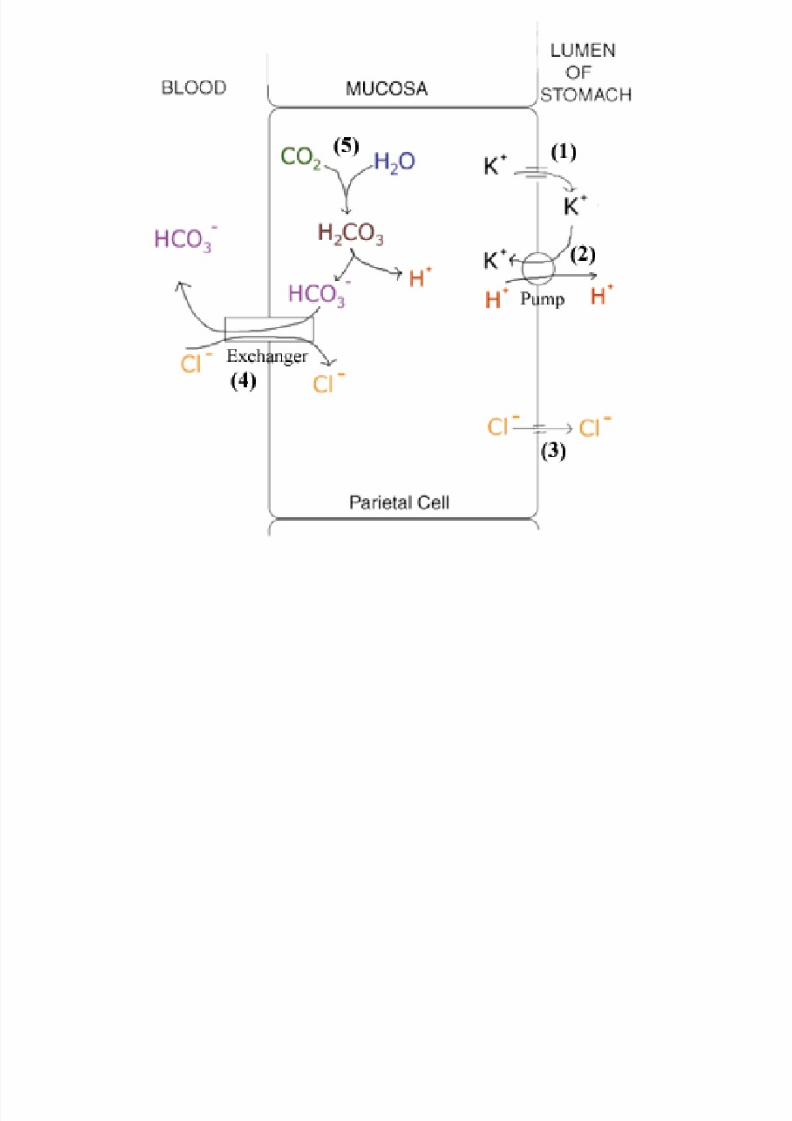
Gastric Acid Production
• Parietal cells produce hydrocholoric acid which: – Destroys microorganisms – Activates enzymes eg pepsinogen – Helps in digestion by breaking down and coagulating proteins
and by combining with calcium and iron to produce salts
• H+ ions are produced by dissociation of H2O andpumped into the stomach by H+ /K+ exchangers
• The OH-
ions combine with H2CO3 to produce H2O andHCO3- which is pumped into the blood by HCO3
- /Cl- exchangers
• The Cl- ions are pumped into the stomach with the K+
brought in by the H+
/K+
exchanger or move by diffusion
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 5/49
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 6/49
Control of Acid Secretion
• At rest the H+ /K+ exchangers are held in intracellularvesicles – stimulus to produce acid causes them to befused with the membrane which throws the membraneinto folds called secretory canaliculi increasing thesurface area for secretion
• Stimuli to produce acid include: – Acetylcholine – increases acid production – Histamine – increases acid production
– Gastrin – increases acid production
– Prostaglandin E2 – decreases acid production – Somatostatin – decreases gastrin release
• All of these function by having an effect on proteinkinases, through Ca2+ levels or G-proteins, which control
the activity of the H+
/K+
exchangers
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 7/49
Helicobacter Pylori
• Gram –ve rod bacteria, spread person to person, verycommon (90% in developing world, %=age in developedworld)
• Produces urease, an enzyme which produces ammoniafrom urea allowing it to survive in very acidicenvironments
• Using flagella it moves to the alkaline mucus layer in thestomach, irritating the gastric epithelium and causing aninflammatory reaction in this area (gastritis)
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 8/49
Peptic ulcers• A break in the epithelium of the stomach or duodenum caused by an
imbalance between gastric acid production and mucosal resistance
• Around 80% located in duodenum, 20% in stomach
• Causes
– H Pylori infection – NSAIDs – Zollinger Ellison syndrome – Post surgery – Smoking
• Ulcers are large (2-10cm), round, with perpindicular walls and asmooth base which can extend through to the muscularis externa orfurther
• They contain fibrin deposition and layers of granulation and scartissue
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 9/49
Peptic ulcers
• Duodenal ulcers – Ammonia released by H Pylori in the stomach causes increased
gastrin production which causes excessive acid production
– Excess acid causes damage to the duodenal mucosa and canlead to ulceration or gastric metaplasia
– Acid also precipitates the bile salts in the duodenum which wouldnormally have stopped infection
– The islands of gastric mucosa can be infected by H Pylori furtherworsening the problem
• Gastric ulcers – Epithelial damage and destruction of the protective alkaline
mucus barrier leads to ulceration
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 10/49
Clinical features
• Epigastric pain – worse at night and before meals
• Nausea, vomiting, dyspepsia
• Anorexia, weight loss
• Can be asymptomatic before complications
• Complications – Perforation – causes peritonitis
– Penetration – ulcer enters adjacent organ
– Haemorrhage – ulcer erodes into a blood vessel and bleeds – causes haemetemesis and melaena
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 11/49
Investigations
• Diagnosis of H Pylori infection – 14C urea breath test – 14C is ingested and if H Pylori is present it
will break urea down to ammonia and CO2. If 14C is detected ina breath test it is positive
– Serology for antibodies
– Stool test using immunoassays – Rapid urease/CLO test – Gastric biopsy added to solution
containing urea and pH indicator, if ammonia is produced pH willincrease
– Biopsy culture and histology
• Endoscopy – Carried out for over 55s or those with ‘alarm symptoms’
(dysphagia, weight loss, anorexia)
– Gastric ulcers are always biopsied
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 12/49
Treatment
• H Pylori infection is treated with eradication triple therapy – Proton pump inhibitor – omeprazole
– Antibiotics – clarithromycin + amoxicillin or metronidazole
• Drugs for treatment of dyspepsia
• Management of complications – Surgery for perforation or massive bleeds – may require partial
gastrectomy – Bleeding ulcers can be injected with adrenaline endoscopically
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 13/49
Management of Dyspepsia
• Dyspepsia refers to any disorder related togastric acid• Drugs used include:
– Proton pump inhibitors eg omeprazole – inhibit H+/K+pumps, effective as it works regardless of the stimulusfor acid secretion
– Antacids eg calcium carbonate – buffer acid andincrease pH
– H2 receptor antagonists eg ranitidine – antagonisehistamine to reduce acid production
– Anticholinergics eg atropine – reduce acid productionbut have too many side effects
– Synthetic prostaglandins eg misoprostol – reduceacid production and increase mucus and bicarbonateproduction
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 14/49
Coeliac Disease
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 15/49
Coeliac disease
• Abnormal reaction to gluten in the diet leading tomalabsorption
• 1 in 2000 prevalence in the UK, higher in Western
Ireland
• Aetiology not fully understood but a component of glutencalled gliadin is believed to stimulate enterocytes tomount an inflammatory reaction
• Other factors include: – Genetics – related to the HLA B8 antigen which is also involved
in the condition dermatitis herpetiformis – Environmental – a factor such as a viral infection may explain
the variable age of onset
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 16/49
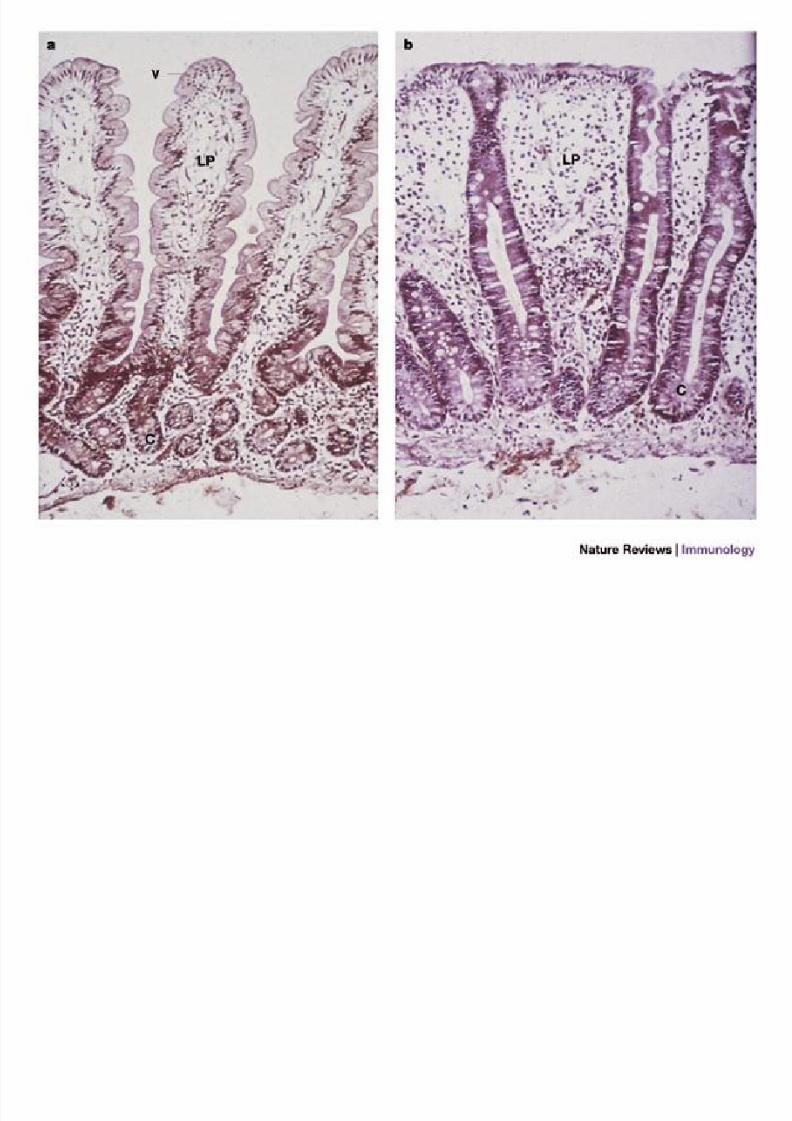
Pathology
• Primarily affects the proximal SI around the jejunum
• Epithelial cell loss accelerates to the point where cellproliferation in the crypts is unable to maintain a normal
amount of functioning cells
• This leads to the classical histological findings of subtotalvillous atrophy and crypt hyperplasia
• The immature cells which populate the brush bordercannot absorb as efficiently and hormone secretion isalso impaired
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 17/49

8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 18/49
Clinical Features
• Can present at any age but most commonis women in their 40s
• Symptoms are variable and non-specific: – Malnutrition and weight loss
– Anaemia
– Fatigue and malaise – GI symptoms – steatorrhoea, diarrhoea,
bloating, discomfort/pain
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 19/49
Investigations
• Jejunal biopsy – ‘Gold standard’, obtained by endoscopy
• Antibodies – IgA endomysial antibodies (IgA EMA)
– Tissue transglutaminase antibodies
• Blood tests – Macrocytic anaemia due to folate deficiency
– Iron deficiency

8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 20/49
Management
• Gluten free diet – Substitute wheat, rye and barley for rice, maize, soya, some oats
• Vitamin and mineral supplementation
• Compliance to gluten free diet can be assessed bytesting antibodies at 4-6 weeks following start of diet
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 21/49
Obstructive Jaundice
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 22/49
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 23/49
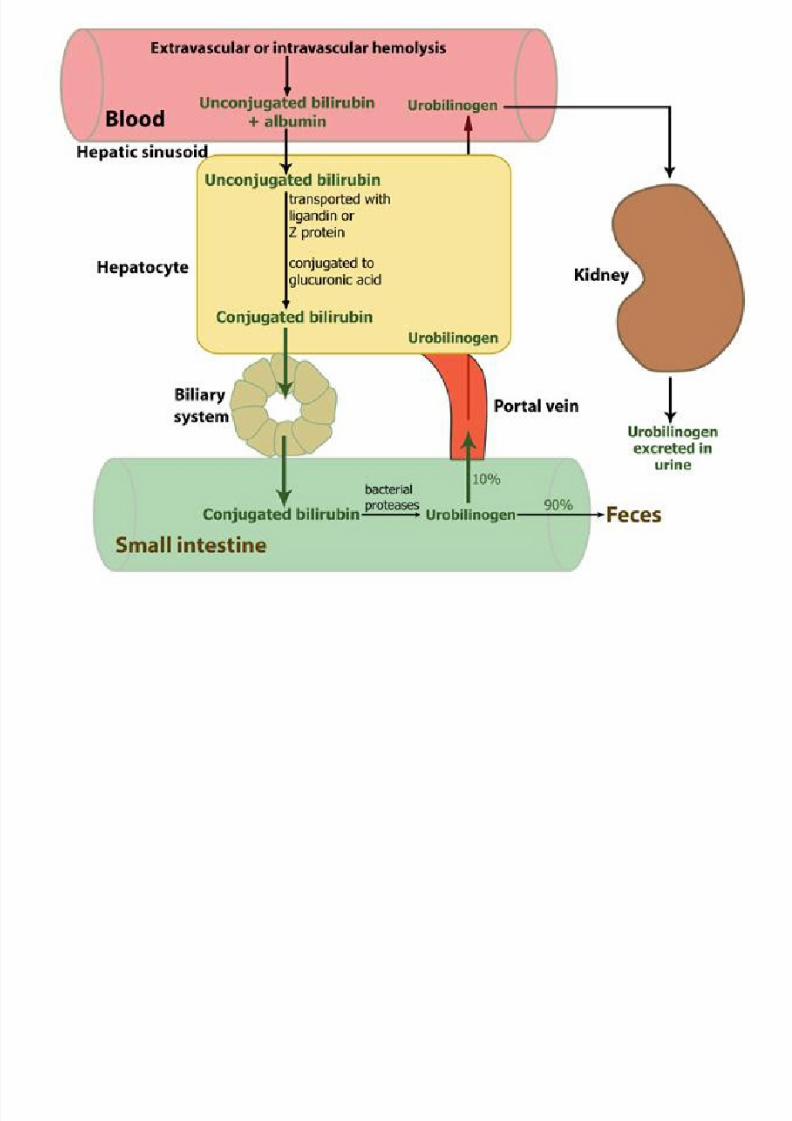
Jaundice
• Caused by hyperbilirubinaemia• Symptoms
– Yellow discolouration of the skin and sclera due to cutaneousdeposition of bilirubin
– Pruritus
– Pale stools (absence of stercobilin) and dark urine (excretion ofconjugated bilirubin) in obstructive jaundice
• Causes divided into: – Pre-hepatic – unconjugated hyperbilirubinaemia usually due to
haemolysis
– Hepatic – mixed hyperbilirubinaemia, variety of causes, due tohepatocellular damage – Post-hepatic – conjugated hyperbilirubinaemia due to blockage
of the biliary tree – gallstones or pancreatic tumours
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 24/49
Gallstones (Cholelithiasis)
• Types of stones: – Cholestrol – large yellow stones – 20% – Bile Pigment – small black irregular – 5% – Mixed – 75%
• Typical patient – fair, fat, fertile
• Depending on anatomical site gallstones have differenteffects:
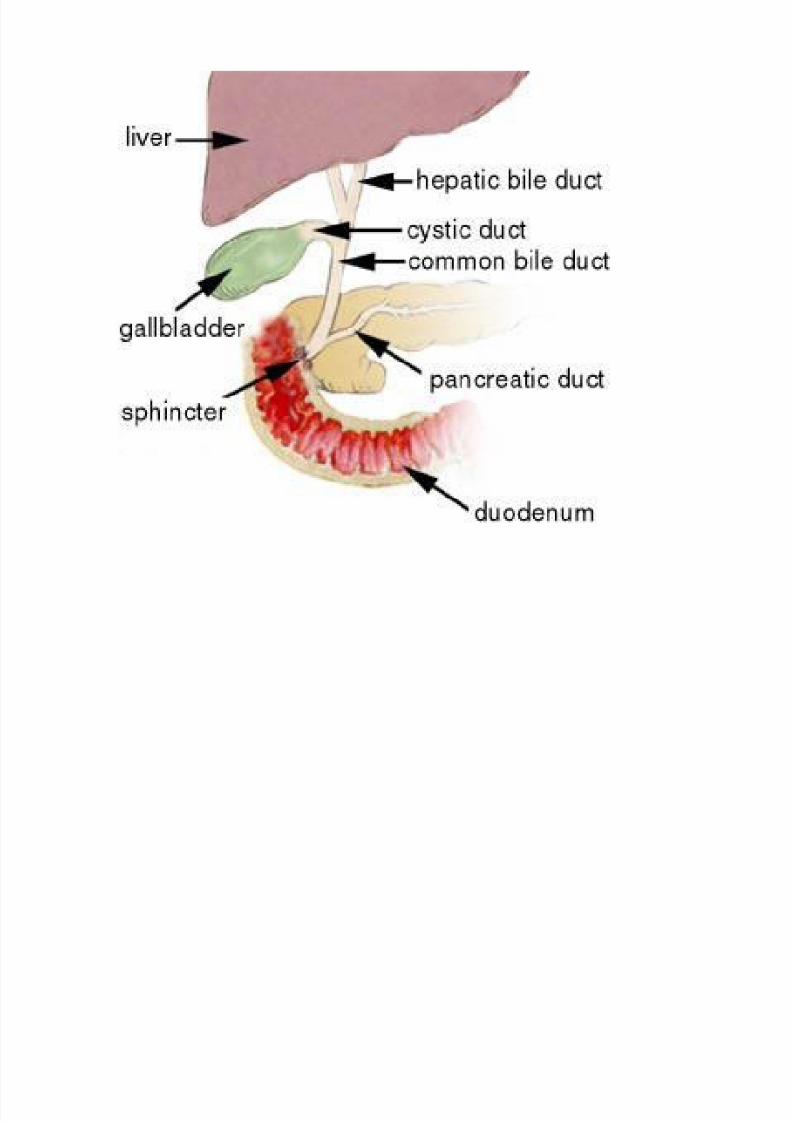
– Silent – Impaction in Hartmann’s pouch/cystic duct – biliary colic, acutecholecystitis
– Impaction in CBD – choledocholithiasis, ascending cholangitis – Gallstone ileus – Pancreatitis
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 25/49
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 26/49
Gallstones
• Biliary colic – Impaction at Hartmann’s pouch which the gallbladder tries to
contract against
– Causes RUQ colicky pain for 2-3 hours after eating which canradiate to right shoulder, patient characteristically lies still
– Not systemically unwell, not jaundiced
• Acute cholecystitis – Prolonged impaction at Hartmann’s pouch/cystic duct causing
the gallbladder to be irritated as it fills with concentrated bile.Becomes infected and fills with pus
– Persisting RUQ pain + fever
– Chronically can lead to a fibrosed gallbladder and chroniccholecystitis
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 27/49
Gallstones
• Choledocholithiasis – Impaction in the CBD
– Causes RUQ pain + jaundice
– If obstruction is not relieved the pressure can causeliver damage
• Ascending cholangitis
– Infection behind an impacted CBD stone – Causes RUQ pain + jaundice + fever (Charcot’s triad)
– High morbidity and mortality
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 28/49
Investigations
• Ultrasound – Gallstones – Thickened gallbladder surrounded by fluid – CBD dilation
• AXR – 10% of gallstones are radio-opaque
• MRCP – Specialised MRI scanner to image biliary tree and pancreas
• ERCP – Endoscopic retrograde cholangiopancreatography – An endoscope with a side view camera to visualise sphincter of Oddi – Diagnostic and therapeutic eg sphincterotomy, stone retrieval
• Bloods – LFTs, coagulation screen for procedures

8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 29/49
Management
• Depends on which pathology is present
• Measures include – Analgesia eg morphine – Antibiotics (eg amoxicillin, gentamicin, metronidazole)
and rest – Removal of stone by ERCP or rarely using lithotripsy – Cholecystectomy either within 72h or after 6 weeks
after the inflammation has settled
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 30/49
Alcoholic Liver Disease

8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 31/49
Alcohol Metabolism
• ADH – alcohol dehydrogenase• ALDH – aldehyde dehydrogenase
• CYP2E1 – an enzyme which is part of the microsomal ethanoloxidising system (MEOS)
• High levels of acetaldehyde and its derivatives in the geneticallysusceptible are hepatotoxic
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 32/49
Alcoholic Liver Disease
• Fatty liver – Excess fat deposition in the liver, reversible – Occurs in 50% of heavy drinkers – Causes derangement of LFTs but normal coagulation – Few symptoms, no encephalopathy – Also occurs without alcohol – non-alcohol steatohepatitis, occurs in
metabolic syndrome
• Acute hepatitis – Occurs in 40% of heavy drinkers – More deranged LFTs, prolonged clotting time
– Moderate symptoms, encephalopathy possible
• Cirrhosis – Severe alcohol abuse – Features of chronic liver disease eg encephalopathy, portal
hypertension
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 33/49
Clinical Features
• Some clinical features are common to chronic liverdisease due to any cause and some are specific toalcohol excess
• Chronic alcohol abuse leads to: – Neural damage due to the thiamine deficiency and alcohol
neurotoxicity. This leads to cortical and cerebellar atrophyresulting in reduced cognition and cerebellar ataxia
– Thiamine deficiency leads to Wernicke Korsakoff syndromewhich involves Wernicke’s encephalopathy in the early stagesand eventually causes Korsakoff psychosis
• Classically presents with confusion, gait ataxia and mild nystagmus• Immediate memory recall retained but have anterograde and
retrograde amnesia, display confabulation
– Peripheral neuropathy – Psychiatric problems
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 34/49
Chronic Liver Disease
• Ascites - Excess fluid in the peritoneal cavity due to: – Reduced albumin and oncotic pressure – Portal hypertension leading to transudation of fluid into
peritoneal cavity – Peripheral vasodilation leading to water retention by kidneys
• Portal hypertension – The normally low pressure in the portal system is elevated due
to back pressure caused by liver cirrhosis – Blood finds alternative pathways to the systemic circulation
which bypass the liver leading to portosystemic shunting anddistension of these vessels eg oesophageal varices – Thus the protective first pass metabolism of the liver is lost – Oesophageal varices have a tendency to rupture and with
concurrent coagulopathy this can be fatal
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 35/49
Chronic Liver Disease
• Hepatic encephalopathy – Portosystemic shunting leads to blood which has not been
detoxified reaching the brain
– Neurotoxins such as ammonia, FFA, excess GABA cause neuraldamage
– Patients are irritable, confused and disorientated, can lead tocoma
– Signs include fetor herpeticus and asterixis
• Other features: – Jaundice
– Coagulopathy
– Proximal muscle weakness
– Hepatorenal syndrome
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 36/49
Management
• Investigations – Bloods – FBC, U+E, LFTs, coagulation – Imaging – liver ultrasound, CT scan
• Detox – thiamine and benzodiazepines
• Alcohol abstinence – psychiatric input, antabuse drugseg disulfiram
• Liver cirrhosis is incurable and requires transplant
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 37/49
Viral Hepatitis
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 38/49
Hepatitis
• Hepatitis is inflammation of the liver and hasmany causes
• Viral causes include: –
Hepatitis A to E – EBV
– CMV
– Yellow fever
– Herpes Simplex
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 39/49
Hepatitis A
• Most common but least serious type• ssRNA hepatovirus• Spreads by faecal oral route, infects liver via gut, shed in faeces for
2 weeks before and 1 week after onset of symptoms• 90% of children in developing countries infected by 5 years
• Clinical features – Non specific symptoms eg nausea, malaise – Some may develop jaundice – Severe disease leading to liver failure rare
• Investigations – LFTs – marked increase in transaminases
– IgM indicates acute infection (IgG indicates previous infection)• No specific treatment, most recover by 3-6 weeks• Vaccine recommended for travellers etc, inactivated virus which
gives immunity for 1 year or 10 years with a booster. IgG treatmentprovides protection quickly for 3-4 months
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 40/49
Hepatitis B
• dsDNA virus with three important antigens: – HBsAg – surface antigen surrounding virus core – HBcAg – core antigen surrounding DNA – HBe – secreted by core, appears on hepatocyte surface, targetted by
immune system
• Spread by blood (eg blood products, needles, tattoos), sexualintercourse and vertical transmission from mother to child
• Infected 2bn people worldwide with 300m carriers – low prevalencein the Western world
• The majority of cases involve a mild or subclinical transient infectionhence which requires no treatment
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 41/49
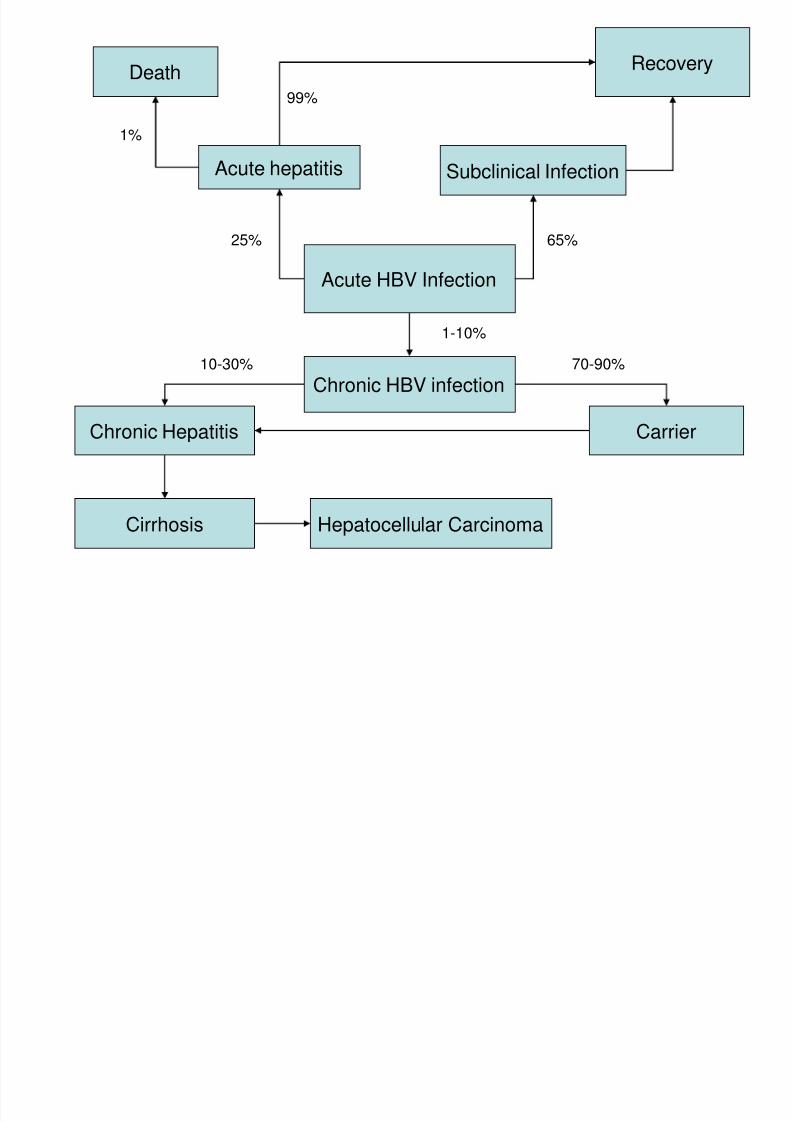
Acute HBV Infection
Acute hepatitis Subclinical Infection
RecoveryDeath
Chronic HBV infection
CarrierChronic Hepatitis
Cirrhosis Hepatocellular Carcinoma
1%
99%
10-30% 70-90%
25% 65%
1-10%
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 42/49
Reaction to HBV infection
• The immune response is made by cytotoxic T cells – thetype of response depends on the type of T cell
• Th1 responses (IL-2, gamma interferon) lead toclearance of the virus
• Th2 reponses (IL-4,5,6,10,13) lead to chronic infection• A poor cell mediated response eg in children is more
likely to lead to carrier status but adults are more likely tosuffer liver damage
• Chronic infection goes through two stages: – Replicative stage – virus is replicated, patient is highly infectious
– Integrative phase – viral DNA is integrated into host DNA andtranscribed with it, inflammation decreases but cirrhosis andcancer more likely

8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 43/49
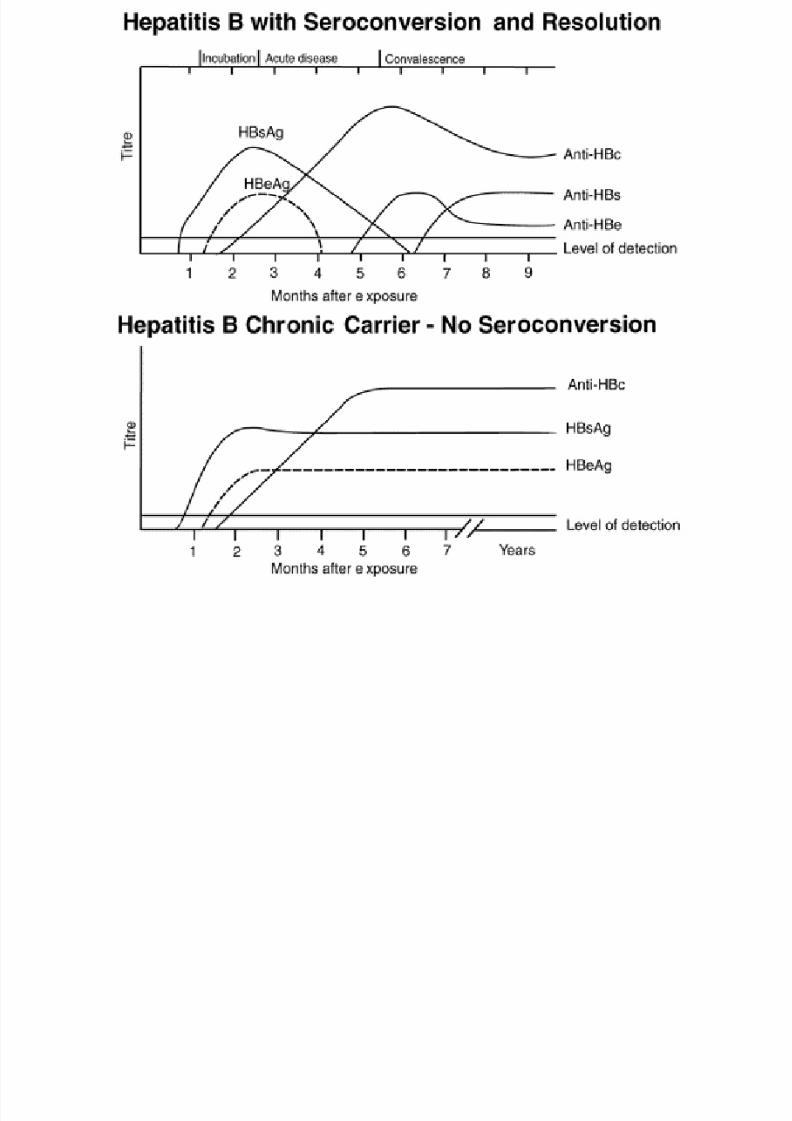
Investigations• A number of viral antigens and host antibodies can be
detected to monitor the state and course of HBVinfection: – HBsAg – surface antigen is present in acute infection but rapidly
cleared, persistence beyond 6 months indicates chronic infection – Anti-HBs – appears a few weeks after clearance of HBsAg,
indicates immunity
– Anti-HBc – appears in symptomatic infection, persists followingany infection
– Anti-HBc IgM – appears in symptomatic acute or highly infectivechronic infection, disappears over 6-9 months
– HBeAg – appears in acute infection but generally cleared,persists in highly infective carriers
– Anti-HBe – only detected in low infectivity carriers
• LFTs would show hepatitis
• Imaging eg US or CT and biopsy in chronic infection
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 44/49

8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 45/49
Treatment
• Interferon – Bind to host ribosomes and prevent translation of viral mRNA – Pegylated interferon α2a (pegylated means it is conjugated and stays in
circulation longer) – Clear HBeAg in 40% of patients – Severe side effects eg fever, headache, malaise, depression, diarrhoea,
hair loss, infection
• Antivirals – Nucleoside or nucleotide analogues which inhibit enzymes involved in
viral replication eg reverse transcriptase or DNA polymerase – Lamivudine used – reverse transcriptase inhibitor
• Vaccination – Active immunisation using the HBsAg antigen – In the UK it is administered to high risk groups – Passive immunisation can be given using HBV antibodies – Post exposure prophylaxis with both active and passive immunisation
should be given to people exposed to HBV eg needle stick injuries
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 46/49
Hepatitis C
• ssRNA flavivirus spread through blood, blood products,needles, tattooing etc
• Sexual or vertical transmission is less likely than HBV
• Identified in 1989, has infected around 240m peopleworldwide
• The course of illness also depends the immuneresponse mounted but progression to chronic illness ismuch more likely than HBV
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 47/49
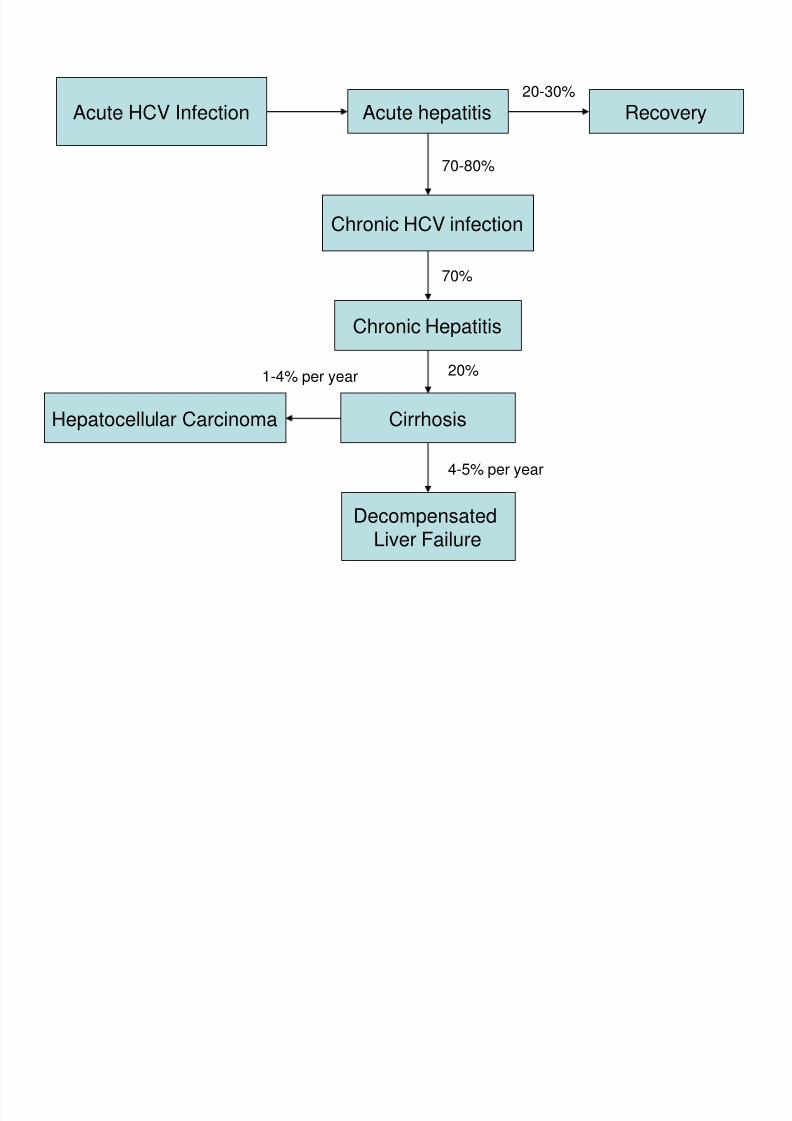
Acute HCV Infection Acute hepatitis
Chronic HCV infection
Recovery
Chronic Hepatitis
CirrhosisHepatocellular Carcinoma
70%
20-30%
70-80%
20%1-4% per year
DecompensatedLiver Failure
4-5% per year
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 48/49
Management
• Investigations – Anti-HCV antibodies, HCV DNA and viral load – LFTs – Imaging and biopsy in chronic infection
• Treatment (similar to HBV) – Pegylated interferon α2b – Ribavirin – viral DNA polymerase inhibitor
– No vaccine
8/2/2019 Gastroenterology Revision Lecture
http://slidepdf.com/reader/full/gastroenterology-revision-lecture 49/49
Questions?