gallbladder, the big picture
TRANSCRIPT

Gallbladder
By: Krystle Rolle Bobby Korah
& Oladapo Samson

Anatomy of GallbladderThe gall bladder is
located in the junction of the right ninth costal cartilage and lateral border of the rectus abdominis .
It is a pear shaped sac lying on the inferior surface of the liver in a fossa between the right and quadrate lobes with a capacity of about 30 to 50 mL.

Anatomy of GallbladderThe gallbladder is in direct
contact to the superior part of the duodenum and transverse colon.
The gall bladder has three parts the neck which tapers into the narrow cystic duct which connects with the common duct.
Body: contacts the visceral surface of the liver the transverse colon and superior part of the duodenum
Fundus: The wide end of the organ projects 1-2 cm from the inferior border of the liver.

Anatomy of GallbladderThe cystic duct (3-4 cm long) connects the neck of the
gallbladder to the common hepatic duct .The spiral fold helps keep the cystic duct open ;thus bile
can easily be diverted into the gallbladder when the distal end of the bile duct is closed by the sphincter of the bile duct.
The spiral fold also offers additional resistance to sudden dumping of bile when the sphincters are closed, and intra-abdominal pressure is suddenly increased, as during a sneeze or cough.
The cystic duct passes between the layers of the lesser omentum, usually parallel to the common hepatic duct, which it joins to form the bile duct.

Blood Supply of the Gall BladderThe cystic artery,
supplying the gallbladder and cystic duct commonly arises from the right hepatic artery.

CYSTOHEPATIC TRIANGLE OF CALOT
In the angle between the common hepatic duct and the cystic duct cystohepatic triangle (of Calot) which is formed by the visceral surface of the liver superiorly, the cystic duct inferior-laterally and the common hepatic duct medially.

Variations to the Cystic ArteryVariations occur in the
origin and course of the cystic artery .
In approximately 12% of cases, the right hepatic artery arises from the superior mesenteric artery.
The cystic artery usually arises from the right hepatic artery, but other origins are possible.
The cystic artery may pass posterior (75%) or anterior (24%) to the common hepatic duct.

Venous Drainage of the GallbladderThe cystic veins, draining the neck of the
gallbladder and cystic duct, enter the liver directly or drain through the portal vein to the liver, after joining the veins draining the hepatic ducts and upper bile duct.
The veins from the fundus and body of the gallbladder pass directly into the visceral surface of the liver and drain into the hepatic sinusoids.
Because this is drainage from one capillary (sinusoidal) bed to another, it constitutes an addition (parallel) portal system.

Lymphatic Drainage of Gallbladder
The lymphatic drainage of the gallbladder is to the hepatic lymph nodes often through cystic lymph nodes located near the neck of the gallbladder.
Efferent lymphatic vessels from these nodes pass to the celiac lymph nodes.

Nerve SupplyThe nerves to the gallbladder and cystic duct pass
along the cystic artery from the celiac nerve plexus (sympathetic and visceral afferent [pain] fibers), the vagus nerve (parasympathetic), and the right phrenic nerve (actually somatic afferent fibers).
Parasympathetic stimulation causes contractions of the gallbladder and relaxation of the sphincters at the hepatopancreatic ampulla.
However, these responses are generally stimulated by the hormone cholecystokinin (CCK), produced by the duodenal walls (in response to the arrival of a fatty meal) and circulated through the blood stream

FunctionsGall bladder
It stores BileIt concentrates bileEjects bile into lumen
BileEmulsify dietary lipidsFormation of micelles with products of lipid
digestion.

BILEBile is produced at a rate of 500–1500 mL/d by
the hepatocytes and the cells of the ductsThe organic constituents of bile are bile salts
(50%), bile pigments such as phospholipids (40%), cholesterol (4%), and bilirubin (2%) Bile also contains electrolytes and water.
Bile acids are conjugated with amino acids , glycine or taurine to form bile salts.
Bilirubin , a yellow- colored byproduct is the major bile pigment.

Secretion and enterohepatic circulation of bile salts

CHOLELITHIASIS
Presence of one or more calculi (gallstones) in the gallbladder.

Incidence and EpidemiologyIn the United States, about 20 million
people (10-20% of adults) have gallstones.Every year 1-3% of people develop
gallstones and about 1-3% of people become symptomatic.
Prevalence of cholesterol cholelithiasis in other Western cultures is similar to that of the United States, but it appears to be somewhat lower in Asia and Africa.
Prevalence is highest in people of northern European descent and in Hispanic populations
Women are more likely to develop cholesterol gallstones than men, especially during their reproductive years, when the incidence is 2-3 times than that in men.

Risk factorsCholesterol stones:
Obesity, age <50Estrogens: female, multiparity, OCPsEthnicity: Caucasian > blackTerminal ileal resection or disease (Crohn’s
Disease)Impaired gallbladder emptying: starvation, DM
type 1Rapid weight loss: rapid cholesterol mobilization
and biliary stasis Pigment stones :
Chronic (contains calcium bilirubinate):CirrhosisChronic hemolysisBiliary stasis (strictures, dilation, biliary infection)

PathophysiologyBiliary sludge is often a precursor of
gallstones. It consists of Ca++ bilirubinate (a polymer of bilirubin), cholesterol microcrystals, and mucin.
Sludge develops during gallbladder stasis, as occurs during pregnancy.
Most sludge is asymptomatic or disappears when the primary condition resolves.
Alternatively, sludge can evolve into gallstones and migrate into the biliary tract, obstructing the ducts and leading to biliary colic, cholangitis, or pancreatitis.

PathophysiologyThree types of stones, cholesterol,
pigment, mixed.Formation of each types is caused
by crystallization of bile.Cholesterol stones most common.Impaired motility can predispose to
stones.Pigment stones (15%) are from
calcium bilirubinate. Diseases that increase RBC destruction will cause these. Also in cirrhotic patients, parasitic infections.

PathophysiologyCholesterol stones – vary in color from light
yellow to dark green or brown and are oval in shape, 2-3 cm in length, often having a tiny dark central spot.
Pigmented stones – are small dark stones made of bilirubin and calcium salts that are found in the bile
Mixed stones – calcium carbonate, palmitate phosphate, bilirubin and other bile pigments. Because of their calcium content, they are often radiographically visible.

4 Stages of CholelithiasisGallstone disease may be thought of as
having the following 4 stages:The lithogenic state, in which
conditions favor gallstone formationAsymptomatic gallstonesSymptomatic gallstones,
characterized by episodes of biliary colic
Complicated cholelithiasis

Symptoms and signs80% of gallstones are asymptomatic. The
remainder have symptoms ranging from biliary-type pain (biliary colic) to cholecytitis to life-threatening cholangitis. Biliary colic is the most common symptom.
RUQ (Right Upper Quadrant) pain which may radiate to the back – described as colicky, but more often is dull and constant.
Nausea & Vomiting, fever and chills do not occur.
Other symptoms include dyspepsia, flatulence, food intolerance, particularly to fats, and some alteration in bowel frequency.
Restlessness

Biliary colic
Biliary colic is pain associated with irritation of the viscera secondary to cholecystitis and gallstones.
Unlike renal colic, the phrase 'biliary colic' refers to the actual cholelithiasis.
Although it is frequently described as a colic, the pain is steady, starts rapidly, becomes intense and lasts at least 30 minutes and up to several hours.

CHOLECYCTITIS
A common condition that results from inflammatory, infections, metabolic, neoplastic and congenital disorders
It is the inflammation of gallbladder that occurs most commonly because of an obstruction of the cystic duct from cholelithiasis.
Acute acalculous cholecystitis – cholecystitis without stones. It accounts for 5-10% of cholecystectomies done for acute cholecystitis
Acute calculous cholecystitis – cholecystitis with stones. It accounts for 90-95%.

CHOLECYCTITISAcute cholecystitis is inflammation of the
gallbladder that develops over hours, usually because a gallstone obstucts the cystic duct.
Symptoms include RUQ pain and tenderness, sometimes accompanied by fever (usually low grade), chills, nausea, and vomiting.
Most patients have had prior attacks of biliary colic or acute cholecystitis.
Pain lasts longer (i.e. >6hr) than in biliary colic and more severe.
Acute cholecystitis begins to subside in 2 to 3 days and resolves within 1 week in 85% of patients.

CHOLECYCTITISChronic cholecystitis is long-standing
gallbladder inflammation almost always due to gallstones.
Chronic cholecystitis almost always results from gallstones and prior episodes of acute cholecystitis (even if mild). Damage ranges from a modest infiltrate of chronic inflammatory cells to a fibrotic, shrunken gallbladder. Extensive calcification due to fibrosis is called porcelain gallbladder.
Gallstones intermittently obstruct the cystic duct and so cause recurrent biliary colic. Such episodes of pain are not necessarily accompanied by overt gallbladder inflammation; the extent of inflammation does not correlate with the intensity or frequency of biliary colic. Upper abdominal tenderness may be present, but usually fever is not. Fever suggests acute cholecystitis.

Physical findings:Fever, tachycardia, and
hypotension; alert you to more serious infections, including cholangitis, cholecystitis.
Murphy’s sign - it is performed by asking the patient to breathe out and then gently placing the hand below the costal margin on the right side at the mid-clavicular line (the approximate location of the gallbladder). The patient is then instructed to inspire (breathe in). Normally, during inspiration, the abdominal contents are pushed downward as the diaphragm moves down (and lungs expand). If the patient stops breathing in (as the gallbladder is tender and, in moving downward, comes in contact with the examiner's fingers) and winces with a 'catch' in breath, the test is considered positive


Physical findings:
Lepenet’s symptom – tenderness is revealed by a light tapping of the right hypochondrium with flexed fingers on inspiration.
Kehr’s symptom – tenderness in the zone of gallbladder (Kehr’s point) especially evident on inspiration)
Mussi’s sign – detects pain by pressing a point of the phrenic nerve between peduncles of the right sternocleidomastoid muscle.
Gausman’s symptom – light tapping of the right hypochondrium with breath holding on deep inspiration (inflated abdomen) – tenderness on inspiration suggests chronic cholecystitis, and on expiration – a likelihood of pyloro-duodenal pathology.

Differentials Abdominal Aorta AneurysmAppendicitisCholangitis, cholelithiasisDiverticulitisGastroenteritisHepatitisInflammatory Bowel DiseaseMyocardial InfarctionPancreatitis, renal colic, pneumonia

CHOLECYCTITIS - complicationPerforationEmpyema – pus in the gallbladderGangrene Mirizzi’s syndrome – rarely, a gallstone
becomes impacted in the cystic duct or Hartman’s pouch and compresses and obstructs the common bile duct, causing cholestasis.
Gallstone pancreatitis: Gallstones pass from the gallbladder into the biliary tract and block the pancreatic duct.
Cholecystoenteric fistula: Infrequently, a large stone erodes the gallbladder wall, creating a fistula into the small bowel (or elsewhere in the abdominal cavity); the stone may pass freely or obstruct the small bowel (gallstone ileus).

CHOLEDOCHOLITHIASIS Is the presence of stones in bile ducts; the
stones can form in the gallbladder or in the ducts themselves. These stones cause biliary colic, biliary obstruction, gallstone pancreatitis, or cholangitis (bile duct infection and inflammation).
Stones may be described as:Primary stones (usually brown pigment stones),
which form in the bile ductsSecondary stones (usually cholesterol), which
form in the gallbladder but migrate to the bile ducts
Residual stones, which are missed at the time of cholecystectomy (evident < 3 years later)
Recurrent stones, which develop in the ducts > 3 years after surgery.

CHOLEDOCHOLITHIASIS Essentials for diagnosis:
Biliary painJaundiceEpisodic cholangitisGallstones in gallbladder or previous
cholecystectomySigns:
Patient may be icteric and toxic, with high fever and chills, or may appear to be perfectly healthy.
A palpable gallbladder is unusual in patients with obstructive jaundice.
Dark-tea coloured urine.

Acute Biliary PancreatitisGallstones are the most
common cause of acute pancreatitis (AP), a potentially life-threatening condition, worldwide.
accounting for at least one half of the 4.8-24.2 cases of pancreatitis per 100,000 people that occur in Western countries. About 80,000 cases occur in the USA; 17 per 100,000 new cases.

Etiology? ?Unknown ?? - But Gender and Stone size may
be risk factors.Suggested possible initiating events in gallstone
pancreatitis include the reflux of bile into the pancreatic duct due to transient obstruction of the ampulla during passage of gallstones.
The risk of developing acute pancreatitis in patients with gallstones is greater in men; however, more women develop this disorder since gallstones occur with increased frequency in women.

Prevailing Theory of PathogenesisCommon Channel Theory
sterile bile does not result in pancreatitis. However, infected bile is capable of activating pancreatic enzymes leading to auto digestion of the gland.
reflux of infected bile into the pancreas activating a cascade of proteolytic enzymes, and obstruction of pancreatic duct causing acinar disruption from raised pressure.
Results in leakage of pancreatic enzymes into pancreatic and peripancreatic tissue.

History/PESevere epigastric pain
radiating to the backGrey Turner’s sign
Flank discolorationCullen’s sign
Periumbilical discolorationNausea, vomiting, weakness, fever, shock

Clues for DifferentialsPrior History of Biliary ColicRule out other causes of acute Pancreatitis
Heavy alcohol consumptionMedicationsGenetic diseasesInfectious agentsPostoperative statesEndoscopic procedure involving pancreatic and
bile ducts and other types of injury to pancreas.

Ampula of Vater

InvestigationsIn patients with suspected gallstone
complications, blood work should include:CBC with differentialsLFT – Liver Function TestAmylase and lipase.
Abdominal Ultra Sound – sensitivity and specificity are 95%. It also accurately detects sludge.
Endoscopic Ultra Sound accurately detects small stones (<3mm) and may be needed if other tests are ambiguous.
CT, MRI – though accurate but are not cost effective.

LabsSerological inflammatory markers
Serum amylaseelevated in at least 75% of cases of acute pancreatitis
and remains elevated for 5-10 days in most patients. However, amylase lacks specificity.
Serum lipaseSerum lipase has a longer half life than amylase and
therefore tends to remain elevated for longer. Using a cut-off of three times the upper limit of normal,
the sensitivity of serum lipase for pancreatitis approaches 90% in patients presenting with abdominal pain.
Calcium

InvestigationsUltra Sound
Should be considered for initial investigationCan show enlarged pancreas with
StrandingAbscessHemorrhageNecrosisPseudocyst
The sensitivity of this study in detecting pancreatitis is 62 to 95 percent. However, in 35 percent of cases, the pancreas is obscured secondary to bowel gas.

Imaging studies: Ultra Sound
→ denotes gallstones
► denotes the acoustic shadow due to absence of reflected sound waves behind the gallstone
→→
►

Investigations cont.Computed Tomography (CT) scan
provides the best imaging of the pancreas and surrounding structures.
useful when other diagnostic studies are: Inconclusivewhen the patient has severe symptomswhen fever is present in the face of persistent leukocytosis that suggests secondary
infection.findings in pancreatitis may show inflammation
characterized by diffuse or segmental enlargement of the pancreas, with irregular contour and obliteration of peri-pancreatic fat, necrosis or a pseudocyst.

CT scanContrast-enhanced
axial computed tomographic section of the upper abdomen showing peri-pancreatic and retroperitoneal edema (large arrows) and stranding. The pancreas itself (small rrow) appears relatively normal.

CTContrast-enhanced
axial computed tomographic section of the upper abdomen showing peripancreatic and retroperitoneal edema. Large non-enhancing areas of necrosis are visible in the body and neck of the pancreas (arrows).

CT
Contrast-enhanced axial computed tomographic section of the upper abdomen showing a well-defined fluid collection in the retroperitoneum (arrow) just below the level of the pancreas.

Investigations cont.Early Endoscopic Retrograde
Cholangiopancreatography (ERCP)It is primarily indicated in patients with severe
disease who are suspected of having biliary obstruction.The endoscope travels orally into the stomach,
through the pylorus into the duodenum where the ampulla of Vater (the opening of the common bile duct and pancreatic duct) exists. The sphincter of Oddi is a muscular valve that controls the
opening of the ampulla.Through the endoscope, the surgeon can see the inside of
the stomach and duodenum, and inject dyes into the ducts in the biliary tree and pancreas so they can be further visualized on X-rays.
A cholecstectomy should be done upon successful removal of the gallstones from the bile ducts.

ERCP
Fluoroscopic image of common bile duct stone seen at the time of ERCP.
The stone is impacted in the distal common bile duct.
A nasobiliary tube has been inserted.
ERCP
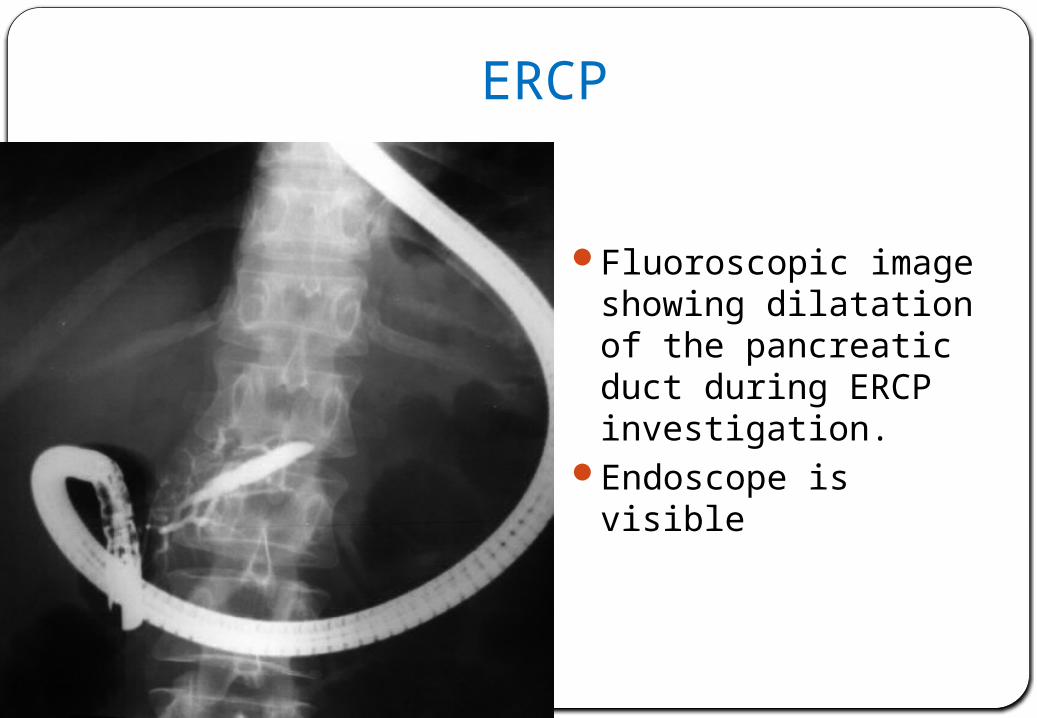
Fluoroscopic image showing dilatation of the pancreatic duct during ERCP investigation.
Endoscope is visible

HIDA SCANA HIDA scan
(hepatobiliary iminodiacetic acid scan) is radiodiagnostic procedure that helps track the production and flow of bile from the liver to the small intestine.
It uses a radioactive chemical, or tracer, that helps highlight certain organs on the scan. The gallbladder should be visualized between 1 – 4 hours.
It has been found to be up to 95% accurate in diagnosing acute cholecystitis.

HIDA SCAN
Normal Abnormal

TreatmentLaparoscopic cholecystectomy with
preoperative endoscopic common bile duct clearance is recommended as a treatment of choice for acute biliary pancreatitis.
Supportive care:IV fluids/electrolyte replacementAnalgesiaBowel restNG suction Nutritional support Oxygen

TreatmentSymptomatic
Laparoscopic cholecystectomy for symptomatic stones
Open cholecystectomy, which involves a large abdominal incision and direct exploration, is safe and effective. Its overall mortality rate is about 0.1% when done electively during a period free of complications.
AsymptomaticFor patients who decline surgery, or are at high
risk of surgical complications, but want to remove asymptomatic stones; these gallstones can sometimes be dissolved by ingesting bile acids orally for many months.

Prognosis85-90% are mild and self-limiting10-15% are severe
Which require ICU admissionMortality may approach 50% in severe cases
Acute pancreatitis is a potentially fatal disease with an overall mortality of 2 - 7% despite aggressive intervention.
The outcome of acute pancreatitis is determined by two factors which reflect the severity of the illness: organ failure and pancreatic necrosis.
About half of the deaths in patients with acute pancreatitis occur within the first one/two weeks and are mainly attributable to multiple organ dysfunction syndromes. When not treated, the risk of recurrence in gallstone pancreatitis ranges from 32 to 61%.
At least one study has shown that patients with severe biliary pancreatitis show a reduction in morbidity and mortality with early (less than 24 hours) ERCP.

Case 1 :
46 year old female patient presents with RUQ pain, jaundice, acholic stools, dark tea-colored urine, no fevers
Known history of cholelithiasisExam: unremarkableWBC 8,000 per μl; Total Bilirubin is 8mg/dl,
increased AST/ALT , negative for Hepatitis B & C
Ultrasound: Gallstones, Common Bile Duct stone, dilated Common Bile Duct > 1cm
CHOLEDOCHOLITHIASIS

Case 2 A 47-year-old man presents to the emergency room with sudden
onset of severe upper abdominal pain with vomiting. The pain is focused in the epigastrium with radiation to the back. Serum amylase levels are 2000 U/L.
Which of the following are the most commonly encountered predisposing factors for this patient‘s condition?
A. Alcohol use and gallstones B. Helicobacter pylori infection and excess gastric acid secretion C. Hepatitis B infection and iron overload D. Obesity and high serum cholesterol E. Stress and cigarette use
The correct answer is A. The clinical scenario is typical of acute pancreatitis. The overwhelmingly most important contributing factors for development of acute pancreatitis are gallstones (particularly small ones) and alcohol abuse.