g schmidt septic shock management
TRANSCRIPT
Official reprint from UpToDate® www.uptodate.com
©2012 UpToDate®
Print | Back
Management of severe sepsis and septic shock in adults Authors
Gregory A Schmidt, MD
Jess Mandel, MD
Section Editors
Polly E Parsons, MD
Daniel J Sexton, MD
Deputy Editor
Kevin C Wilson, MD
Disclosures
All topics are updated as new evidence becomes available and our peer review process is
complete.
Literature review current through: Feb 2012. | This topic last updated: Oct 25, 2011.
INTRODUCTION — Sepsis is a clinical syndrome characterized by systemic inflammation
due to infection. There is a continuum of severity ranging from sepsis to severe sepsis and
septic shock. Over 750,000 cases of sepsis occur in the United States each year, resulting in
approximately 200,000 fatalities [1]. Even with optimal treatment, mortality due to severe
sepsis or septic shock is approximately 40 percent and can exceed 50 percent in the sickest
patients [2-5].
Numerous interventions exist that decrease mortality due to sepsis. In this topic review, the
management of severe sepsis and septic shock is discussed. Definitions, diagnosis,
pathophysiology, and investigational therapies are reviewed separately. (See "Sepsis and
the systemic inflammatory response syndrome: Definitions, epidemiology, and
prognosis" and "Pathophysiology of sepsis" and "Investigational and ineffective therapies for
sepsis".)
THERAPEUTIC PRIORITIES — Therapeutic priorities for patients with severe sepsis or
septic shock include:
Early initiation of supportive care to correct physiologic abnormalities, such as
hypoxemia and hypotension [6-9].
Distinguishing sepsis from systemic inflammatory response syndrome (SIRS) (table
1 and table 2) because, if an infection exists, it must be identified and treated as
soon as possible (table 3). This may require a surgical procedure (eg, drainage), as
well as appropriate antibiotics.
EARLY MANAGEMENT — The first priority in any patient with severe sepsis or septic shock
is stabilization of their airway and breathing. Next, perfusion to the peripheral tissues should
be restored [7,10].
Stabilize respiration — Supplemental oxygen should be supplied to all patients with sepsis
and oxygenation should be monitored continuously with pulse oximetry. Intubation and
mechanical ventilation may be required to support the increased work of breathing that
typically accompanies sepsis, or for airway protection since encephalopathy and a depressed
level of consciousness frequently complicate sepsis [11,12].
Sedative and induction agents (eg, etomidate) used to intubate patients with severe sepsis
or septic shock are discussed separately. Other aspects of intubation and mechanical
ventilation are similarly described elsewhere. (See "Sedation or induction agents for rapid
sequence intubation in adults" and "Advanced emergency airway management in
adults" and "Rapid sequence intubation in adults" and "The decision to intubate" and "The
difficult airway in adults".)
Chest radiographs and arterial blood analysis should be obtained following initial
stabilization. These studies are used in combination with other clinical parameters to
diagnose acute lung injury (ALI) or acute respiratory distress syndrome (ARDS), which
frequently complicate sepsis. (See "Acute respiratory distress syndrome: Definition; clinical
features; and diagnosis" and "Mechanical ventilation in acute respiratory distress
syndrome".)
Assess perfusion — Once the patient's respiratory status has been stabilized, the
adequacy of perfusion should be assessed. Hypotension is the most common indicator that
perfusion is inadequate. Therefore, it is important that the blood pressure be assessed early
and often. An arterial catheter may be inserted if blood pressure is labile or restoration of
arterial perfusion pressures is expected to be a protracted process, because a
sphygmomanometer may be unreliable in hypotensive patients [8]. Attempts to insert an
arterial line should not be allowed to delay the prompt management of shock. (See "Arterial
catheterization techniques for invasive monitoring".)
Critical hypoperfusion can also occur in the absence of hypotension, especially during early
sepsis. Thus, clinical evidence of impaired perfusion should be sought in all patients with
sepsis.
Common signs of hypoperfusion include cool, vasoconstricted skin due to redirection of
blood flow to core organs (although warm, flushed skin may be present in the early phases
of sepsis), obtundation or restlessness, oliguria or anuria, and lactic acidosis. These findings
may be modified by preexisting disease or medications. As an example, elderly patients,
diabetic patients, and patients who take beta-blockers may not exhibit an appropriate
tachycardia as blood pressure falls. Patients with chronic hypertension may develop critical
hypoperfusion at a higher blood pressure than healthy patients (ie, relative hypotension).
Catheters — After initial assessment, a central venous catheter (CVC) should be inserted in
most patients with severe sepsis or septic shock. A CVC can be used to infuse intravenous
fluids, infuse medications, infuse blood products, and draw blood. In addition, it can be used
for hemodynamic monitoring by measuring the central venous pressure (CVP) and the
central venous oxyhemoglobin saturation (ScvO2). In one clinical trial, treatment of septic
shock guided by the ScvO2 reduced mortality [13]. (See "Indications for and complications
of central venous catheters".)
We believe that pulmonary artery catheters (PACs) should not be used in the routine
management of patients with severe sepsis or septic shock. PACs can measure the
pulmonary artery occlusion pressure (PAOP) and mixed venous oxyhemoglobin saturation
(SvO2). In theory, this may be helpful to guide circulatory resuscitation. However, the PAOP
has proven to be a poor predictor of fluid responsiveness in sepsis and the SvO2 is similar
to the ScvO2, which can be obtained from a CVC [14,15]. PACs increase complications and
have not been shown to improve outcome [16-18]. (See "Pulmonary artery catheterization:
Indications and complications".)
Respiratory changes in the radial artery pulse pressure, aortic blood flow peak velocity, and
brachial artery blood flow velocity are considered dynamic hemodynamic measures,
whereas CVP and PAOP are considered static hemodynamic measures [19,20]. There is
increasing evidence that dynamic measures are more accurate predictors of fluid
responsiveness than static measures, as long as the patients are in sinus rhythm and
passively ventilated with a sufficient tidal volume [14,21,22]. For actively breathing patients
or those with irregular cardiac rhythms, an increase in the cardiac output in response to a
passive leg-raising maneuver (measured by echocardiography, arterial pulse waveform
analysis, or pulmonary artery catheterization) is a sensitive and specific predictor of fluid
responsiveness [23]. It seems likely that dynamic measures will become more common and
be used to identify patients who are likely to increase organ perfusion in response to
intravenous fluids.
Restore perfusion — Once it has been established that hypoperfusion exists, early
restoration of perfusion is necessary to prevent or limit multiple organ dysfunction, as well
as reduce mortality. Hypoperfusion results from loss of plasma volume into the interstitial
space, decreased vascular tone, and myocardial depression. The increase in the cardiac
output that is necessary to compensate for the diminished vascular tone may be limited by
the myocardial depression.

Central or mixed venous oxyhemoglobin saturation — Resuscitation of the circulation
should target a central or mixed venous oxyhemoglobin saturation (ScvO2 or SvO2,
respectively) of ≥70 percent [7,13]. Other common goals include a central venous pressure
(CVP) 8 to 12 mmHg, a mean arterial pressure (MAP) ≥65 mmHg, and a urine output ≥0.5
mL/kg per hour, although these targets have not been well studied.
Many clinicians prefer to use dynamic indices (eg, radial pulse pressure, aortic blood flow
peak velocity, brachial artery blood flow velocity, or passive leg raising) to guide fluid
resuscitation rather than static hemodynamic measures (ie, CVP, pulmonary artery
occlusion pressure) [19,20].
The focus on the ScvO2 derives from a clinical trial in which 263 patients with severe sepsis
or septic shock were randomly assigned to therapy targeting a ScvO2 ≥70 percent, or
conventional therapy that did not target a ScvO2 [13]. Both groups initiated therapy within
six hours of presentation and targeted the same CVP, MAP, and urine output. Mortality was
lower in the group that targeted a ScvO2 ≥70 percent (31 versus 47 percent). This
approach is known as "early goal-directed therapy" (ie, administered within the first six
hours of presentation).
Earlier studies of critically ill patients that used similar targets (SvO2 ≥70 percent) found no
mortality benefit [24]. This might be because these studies were not conducted during the
crucial initial hours. This is supported by a systemic review that compared resuscitation
targeting specific physiologic endpoints to standard resuscitation [25]. In a meta-analysis of
randomized trials initiated within 24 hours of the onset of sepsis (6 trials, 740 patients),
resuscitation targeting specific physiologic endpoints improved mortality compared to
standard resuscitation (39 versus 57 percent, odds ratio 0.50, 95% CI 0.37-0.69). In
contrast, a meta-analysis of randomized trials initiated more than 24 hours after the onset
of sepsis (3 trials, 261 patients) found that resuscitation targeting specific physiologic
endpoints did not improve mortality (64 versus 58 percent for standard resuscitation, odds
ratio 1.16, 95% CI 0.60-2.22).
Lactate clearance — Lactate clearance has been evaluated as a potential substitute for
ScvO2 as the target of resuscitation. A trial randomly assigned 300 patients with severe
sepsis to undergo resuscitation targeting either a lactate clearance ≥10 percent or an ScvO2
≥70 percent (other than these targets, the resuscitation protocols were identical) [26].
There was no difference in hospital mortality, length of stay, ventilator-free days, or
incidence of multiorgan failure, suggesting that lactate clearance criteria may be an
acceptable alternative to ScvO2 criteria.
In our practice, we adhere to the principles of early goal-directed therapy; that is, we
initiate early aggressive therapy in order to restore perfusion. We prefer to target an ScvO2
≥70 percent because it is the more extensively studied resuscitation goal, although a lactate
clearance ≥10 percent appears to be a reasonable alternative if ScvO2 monitoring is
unavailable.
We consider the numeric goals for CVP, MAP, and urine output to be guidelines and always
consider additional clinical signs of hypoperfusion when assessing the patient's response to
a therapy and need for more of a therapy.
Intravenous fluids — Relative intravascular hypovolemia is typical and may be severe. As
an example, early goal-directed therapy required a mean infusion volume of approximately
five liters within the initial six hours of therapy in the trial described above [13]. As a result,
rapid, large volume infusions of intravenous fluids are indicated as initial therapy for severe
sepsis or septic shock, unless there is coexisting clinical or radiographic evidence of heart
failure.
Fluid therapy should be administered in well-defined (eg, 500 mL), rapidly infused boluses
[8,9]. Volume status, tissue perfusion, blood pressure, and the presence or absence of
pulmonary edema must be assessed before and after each bolus. Intravenous fluid
challenges can be repeated until blood pressure is acceptable, tissue perfusion is
acceptable, pulmonary edema ensues, or fluid fails to augment perfusion.
Careful monitoring is essential in this approach because patients with sepsis typically
develop noncardiogenic pulmonary edema (ie, ALI, ARDS). In patients with ALI or ARDS
who are hemodynamically resuscitated, a liberal approach to intravenous fluid
administration prolongs the duration of mechanical ventilation, compared to a more
restrictive approach that typically requires large doses of furosemide [27]. Thus, while the
early, aggressive fluid therapy is appropriate in severe sepsis and septic shock, fluids may
be unhelpful or harmful when the circulation is no longer fluid-responsive. (See "Supportive
care and oxygenation in acute respiratory distress syndrome", section on 'Fluid
management'.)
Clinical trials have failed to consistently demonstrate a difference between colloid and
crystalloid in the treatment of septic shock [28,29]. In the saline versus albumin fluid
evaluation (SAFE) trial, 6997 critically ill patients were randomly assigned to receive 4
percent albumin or normal saline for up to 28 days [30]. There were no differences between
groups for any endpoint, including the primary endpoint, mortality. Among the patients with
severe sepsis (18 percent of the total group), there were also no differences in outcome.

Another randomized trial compared pentastarch (a colloid) to modified Ringer's lactate (a
crystalloid) in patients with severe sepsis — the Efficacy of Volume Substitution and Insulin
Therapy in Severe Sepsis (VISEP) trial [31]. There was no difference in 28-day mortality,
but the trial was stopped early because there was a trend toward increased 90-day
mortality among patients who received pentastarch.
In our clinical practice, we generally use crystalloid because of the higher cost of colloid. We
believe that giving a sufficient quantity of intravenous fluids rapidly and targeting
appropriate goals is more important than the type of fluid chosen.
Vasopressors — Vasopressors are second line agents in the treatment of severe sepsis and
septic shock; we prefer intravenous fluids as long as they increase perfusion without
seriously impairing gas exchange [32]. However, intravenous vasopressors are useful in
patients who remain hypotensive despite adequate fluid resuscitation or who develop
cardiogenic pulmonary edema.
In severe septic shock, there is no definitive evidence of the superiority of one vasopressor
over another (table 4). We prefer to use norepinephrine in most patients [7,33]. However,
we find phenylephrine (a pure alpha-adrenergic agonist) to be useful when tachycardia or
arrhythmias preclude the use of agents with beta-adrenergic activity. Choosing a
vasopressor agent is discussed in greater detail elsewhere. (See "Use of vasopressors and
inotropes", section on 'Choice of agent in septic shock'.)
Additional therapies — When the ScvO2 remains <70 percent after optimization of
intravenous fluid and vasopressor therapy, it is reasonable to consider additional therapies,
such as inotropic therapy or red blood cell transfusion.
Inotropic therapy — For patients who have myocardial dysfunction, a trial of
inotropic therapy is warranted if ScvO2 remains <70 percent after all of the
interventions discussed above [7,8,13,34,35]. Inotropic therapy should not be used
to increase the cardiac index to supranormal levels [7]. Dobutamine is the usual
inotropic agent. At low doses, dobutamine may cause the blood pressure to decrease
because it can dilate the systemic arteries. However, as the dose is increased, blood
pressure usually rises because cardiac output increases out of proportion to the fall
in vascular resistance.
Red blood cell transfusions — Early goal-directed therapy aggressively utilizes red
blood cell transfusions to raise the ScvO2. In the trial discussed above, nearly 70
percent of patients in the early goal-directed therapy group received transfusions,
compared to 45 percent in the conventional therapy group [13]. However, other data
support a more cautious approach to transfusion in critically ill patients [36]. (See
"Use of blood products in the critically ill", section on 'Red blood cells'.) There are
several possible explanations for the conflicting data:
Outcome may be related to when a red blood cell transfusion is given. Transfusions
administered as part of early goal-directed therapy were given early in the course of
illness, whereas studies that support a more cautious approach typically gave
transfusions later in the course of illness.
The apparent benefit of red blood cell transfusions may be due to other
interventions. In other words, red blood cell transfusion was just one of several
interventions during early goal-directed therapy and it is possible that the benefit
was due to one or more of the other interventions, not the red blood cell transfusion
per se.
Ongoing management — There are two possible outcomes following the interventions
described above:
Despite aggressive therapy, the patient may have persistent hypoperfusion and
progressive organ failure. This should prompt reassessment of the adequacy of the
above therapies, antimicrobial regimen, and control of the septic focus, as well as
the accuracy of the diagnosis and the possibility that unexpected complications or
coexisting problems have intervened (eg, pneumothorax following CVC insertion).
The patient may have responded to the above interventions with restored perfusion
and a ScvO2 greater than 70 percent. Such patients should continue to have their
clinical and laboratory parameters followed closely. These include blood pressure,
arterial lactate, urine output, creatinine, platelet count, Glasgow coma scale score,
serum bilirubin, liver enzymes, oxygenation (ie, arterial oxygen tension or
oxyhemoglobin saturation), and gut function (table 5). Gastric tonometry may also
be helpful, if available. Reevaluation is indicated if any of these parameters worsen
or fail to improve.
In early sepsis, most lactate is probably a byproduct of anaerobic metabolism due to organ
hypoperfusion. Supporting this view, early goal-directed therapy decreases lactate levels
faster than conventional therapy [13]. After the restoration of perfusion, however, lactate is
probably due to causes other than anaerobic metabolism and further increasing oxygen
delivery to the peripheral tissues is unlikely to decrease its levels [37]. As a result, lactate
values are generally unhelpful following restoration of perfusion, with one exception — a
rising lactate level should prompt reevaluation of perfusion (see "Arterial and mixed venous
blood gases in lactic acidosis").
It would be ideal if hypoxia could be detected for individual organs, because tests that
combine output from many organs (eg, arterial lactate) may obscure the presence of
significant ischemia in an individual organ [38]. Gastric tonometry indirectly measures
perfusion to the gut by estimating the gastric mucosal PCO2. It can be used to detect gut
hypoxia by calculating the gastric to arterial PCO2 gap [39,40]. But, gastric tonometry is
not widely available and it is uncertain whether it can successfully guide therapy. Additional
studies and clinical experience are needed.
CONTROL OF THE SEPTIC FOCUS — Prompt identification and treatment of the primary
site or sites of infection are essential [41-43]. This is the primary therapeutic intervention,
with most other interventions being purely supportive.
Identification of the septic focus — A careful history and physical examination may yield
clues to the source of sepsis and help guide microbiologic evaluation (table 6). As an
example, sepsis arising after trauma or surgery is often due to infection at the site of injury
or surgery. The presence of a urinary or vascular catheter increases the chances that these
are the source of sepsis.
Gram stain of material from sites of possible infection may give early clues to the etiology of
infection while cultures are incubating. As examples, urine should be routinely Gram stained
and cultured, sputum should be examined in a patient with a productive cough, and an
intra-abdominal collection in a postoperative patient should be percutaneously sampled
under ultrasound or radiologic guidance.
Blood should be taken from two distinct venipuncture sites and inoculated into standard
blood culture media. (See "Blood cultures for the detection of bacteremia".)
There is no single test that immediately confirms the diagnosis of severe sepsis or septic
shock. However, several laboratory tests, all of which are still investigational, have been
studied as diagnostic markers of active bacterial infection [6]:
Elevated serum procalcitonin levels are associated with bacterial infection and sepsis
[44-46]. Despite this, a meta-analysis of 18 studies found that procalcitonin
distinguished sepsis from nonseptic systemic inflammation poorly (sensitivity of 71
percent and specificity of 71 percent) [45] and another meta-analysis of six trials
(four in patients with sepsis and two in patients with other infections) found that
using clinical algorithms based upon procalcitonin levels did not affect mortality [47].
The plasma concentration of soluble TREM-1 (triggering receptor expressed on
myeloid cells), a member of the immunoglobulin superfamily that is specifically
upregulated in the presence of bacterial products, is increased in patients with sepsis

[48-50]. In a small trial, increased TREM-1 levels were both sensitive and specific for
the diagnosis of bacterial sepsis (96 and 89 percent, respectively) [48]. Serial
monitoring of TREM-1 may also provide prognostic information in patients with
established sepsis [49,50].
Evaluation of the clinical usefulness of both procalcitonin and TREM-1 is still in its earliest
stages and should be considered preliminary. Until additional clinical investigations have
been performed, we do not suggest the routine use of either.
Eradication of infection — Effective treatment of the active infection is essential to the
successful treatment of severe sepsis and septic shock. Source control (physical measures
undertaken to eradicate a focus of infection and eliminate or treat ongoing microbial
proliferation and infection) should be undertaken since undrained foci of infection may not
respond to antibiotics alone (table 3). As examples, potentially infected foreign bodies (eg,
vascular access devices) should be removed when possible, and abscesses should undergo
percutaneous or surgical drainage. Some patients require extensive soft tissue debridement
or amputation; in severe cases, fulminant Clostridium difficile-associated colitis may
necessitate colectomy [51].
Antimicrobial regimen — Intravenous antibiotic therapy should be initiated immediately
after obtaining appropriate cultures, since early initiation of antibiotic therapy is associated
with lower mortality [52]. The choice of antibiotics can be complex and should consider the
patient's history (eg, recent antibiotics received [53]), comorbidities, clinical context (eg,
community- or hospital-acquired), Gram stain data, and local resistance patterns [7,54,55].
Poor outcomes are associated with inadequate or inappropriate antimicrobial therapy (ie,
treatment with antibiotics to which the pathogen was later shown to be resistant in vitro)
[56-62]. They are also associated with delays in initiating antimicrobial therapy, even short
delays (eg, an hour).
A prospective cohort study of 2124 patients demonstrated that inappropriate
antibiotic selection was surprisingly common (32 percent) [59]. Mortality was
markedly increased in these patients compared to those who had received
appropriate antibiotics (34 versus 18 percent).
A retrospective analysis of 2731 patients with septic shock demonstrated that the
time to initiation of appropriate antimicrobial therapy was the strongest predictor of
mortality [60].
When the potential pathogen or infection source is not immediately obvious, we favor
broad-spectrum antibiotic coverage directed against both gram-positive and gram-negative
bacteria. Few guidelines exist for the initial selection of empiric antibiotics in severe sepsis
or septic shock. In our practice, if Pseudomonas is an unlikely pathogen, we favor
combining vancomycin with one of the following:
Cephalosporin, 3rd generation (eg, ceftriaxone or cefotaxime), or
Beta-lactam/beta-lactamase inhibitor (eg, piperacillin-tazobactam, ticarcillin-
clavulanate), or
Carbapenem (eg, imipenem or meropenem)
Alternatively, if Pseudomonas is a possible pathogen, we favor combining vancomycin with
two of the following (see "Treatment of Pseudomonas aeruginosa infections"):
Antipseudomonal cephalosporin (eg, ceftazidime, cefepime), or
Antipseudomonal carbapenem (eg, imipenem, meropenem), or
Antipseudomonal beta-lactam/beta-lactamase inhibitor (eg, piperacillin-tazobactam,
ticarcillin-clavulanate), or
Fluoroquinolone with good anti-pseudomonal activity (eg, ciprofloxacin), or
Aminoglycoside (eg, gentamicin, amikacin), or
Monobactam (eg, aztreonam)
Selection of two agents from the same class, for example, two beta-lactams, should be
avoided. We emphasize the importance of considering local susceptibility patterns when
choosing an empiric antibiotic regimen.
Staphylococcus aureus is associated with significant morbidity if not treated early in the
course of infection [63]. There is growing recognition that methicillin-resistant S. aureus
(MRSA) is a cause of sepsis not only in hospitalized patients, but also in community dwelling
individuals without recent hospitalization [64,65]. Many of these staphylococci have the
Panton-Valentine leukocidin virulence factor, which causes severe, necrotizing infections
[66]. For these reasons, we recommend that severely ill patients presenting with sepsis of
unclear etiology be treated with intravenous vancomycin (adjusted for renal function) until
the possibility of MRSA sepsis has been excluded. Linezolid is a reasonable alternative if
there are contraindications to vancomycin.
After culture results and antimicrobial susceptibility data return, we recommend that
therapy be pathogen- and susceptibility-directed, even if there has been clinical
improvement while on the initial antimicrobial regimen. Gram-negative pathogens have
historically been covered with two agents from different antibiotic classes. However, several
clinical trials and two meta-analyses have failed to demonstrate superior overall efficacy of
combination therapy compared to monotherapy with a third generation cephalosporin or a
carbapenem [59,67-71]. Furthermore, one meta-analysis found double coverage was
associated with an increased incidence of adverse events [70,71]. For this reason, we
recommend use of a single agent with proven efficacy and the least possible toxicity, except
in patients who are either neutropenic or whose severe sepsis is due to a known or
suspected Pseudomonas infection [7,69]. (See "Pseudomonas aeruginosa bacteremia and
endocarditis" and "Treatment of Pseudomonas aeruginosa infections".)
Regardless of the antibiotic regimen selected, patients should be observed closely for
toxicity, evidence of response, and the development of nosocomial superinfection [72]. The
duration of therapy is typically 7 to 10 days, although longer courses may be appropriate in
patients who have a slow clinical response, an undrainable focus of infection, or
immunologic deficiencies [7]. In patients who are neutropenic, antibiotic treatment should
continue until the neutropenia has resolved. In non-neutropenic patients in whom infection
is thoroughly excluded, antibiotics should be discontinued to minimize colonization or
infection with drug-resistant microorganisms and superinfection with other pathogens.
ADDITIONAL THERAPIES
Glucocorticoids — Glucocorticoids have long been investigated as therapeutic agents in
sepsis because the pathogenesis of sepsis involves an intense and potentially deleterious
host inflammatory response. This topic is discussed in detail separately. (See "Corticosteroid
therapy in septic shock".)
Nutrition — There is consensus that nutritional support improves nutritional outcomes in
critically ill patients, such as body weight and mid-arm muscle mass. However, it is
uncertain whether nutritional support improves important clinical outcomes (eg, duration of
mechanical ventilation, length of stay, mortality), or when nutritional support should be
initiated. This topic is reviewed in detail elsewhere. (See "Nutrition support in critically ill
patients: An overview".)
Intensive insulin therapy — Hyperglycemia and insulin resistance are common in
critically ill patients, independent of a history of diabetes mellitus [73]. As a result, intensive
glycemic control has been studied and a body of evidence has accumulated. This topic is
discussed separately. (See "Glycemic control and intensive insulin therapy in critical
illness".)
Protocols — Sepsis treatment protocols may improve outcome [74-76]. This was illustrated
by an observational cohort study of 120 patients with septic shock [76]. Implementation of
a standardized hospital order set was associated with greater likelihood that the initial
antibiotic regimen targeted the culprit microorganism (87 versus 72 percent), shorter
hospital stay (9 versus 12 days), and lower 28-day mortality (30 versus 48 percent),
compared to historical controls. It is impossible to determine which component or
components of the protocol conferred the benefit.
INFORMATION FOR PATIENTS — UpToDate offers two types of patient education
materials, “The Basics” and “Beyond the Basics.” The Basics patient education pieces are
written in plain language, at the 5th to 6th grade reading level, and they answer the four or
five key questions a patient might have about a given condition. These articles are best for
patients who want a general overview and who prefer short, easy-to-read materials. Beyond
the Basics patient education pieces are longer, more sophisticated, and more detailed.
These articles are written at the 10th to 12th grade reading level and are best for patients
who want in-depth information and are comfortable with some medical jargon.
Here are the patient education articles that are relevant to this topic. We encourage you to
print or e-mail these topics to your patients. (You can also locate patient education articles
on a variety of subjects by searching on “patient info” and the keyword(s) of interest.)
Basics topic (see "Patient information: Sepsis (The Basics)")
SUMMARY AND RECOMMENDATIONS
Sepsis is a clinical syndrome characterized by systemic inflammation and widespread
tissue injury due to infection. There is a continuum of illness severity ranging from
sepsis to severe sepsis and septic shock. When infection is absent, the clinical
syndrome is termed systemic inflammatory response syndrome (SIRS). (See
'Introduction' above.)
Initial management is aimed at securing the airway and correcting hypoxemia.
Intubation and mechanical ventilation may be required. (See 'Stabilize
respiration' above.)
Once the patient's respiratory status has been stabilized, the adequacy of perfusion
should be assessed. Hypotension is the most common indicator that perfusion is
inadequate. However, critical hypoperfusion can also occur in the absence of
hypotension, especially during early sepsis. Common signs of hypoperfusion include
cool, vasoconstricted skin due to redirection of blood flow to core organs (although
warm, flushed skin may be present in the early phases of sepsis), obtundation or
restlessness, oliguria or anuria, and lactic acidosis. (See 'Assess perfusion' above.)
Once it has been established that hypoperfusion exists, early restoration of perfusion
is necessary to prevent or limit multiple organ dysfunction, as well as reduce
mortality. Tissue perfusion should be promptly restored using intravenous fluids,
vasopressors, inotropes, and, possibly, red blood cell transfusions. We recommend
that patients be managed with therapy aimed at achieving a central (or mixed)
venous oxygen saturation ≥70 percent within six hours of presentation (Grade 1B).
(See 'Restore perfusion' above.)
We recommend boluses of intravenous fluids as first-line therapy in patients who
demonstrate impaired perfusion (Grade 1B). Fluid boluses are repeated until blood
pressure and tissue perfusion are acceptable, pulmonary edema ensues, or there is
no further response. These parameters should be assessed before and after each
fluid bolus. There are no data to support preferential administration of crystalloid or
colloid. (See 'Intravenous fluids' above.)
We recommend vasopressors for patients who remain hypotensive following
intravascular volume repletion (Grade 1B). Although there is no definitive evidence
of the superiority of one vasopressor over another, we suggest beginning with
norepinephrine (Grade 2C). (See 'Vasopressors' above.)
For patients whose ScvO2 remains <70 percent after intravenous fluid and
vasopressor therapy, it is reasonable to administer additional therapies, including
blood transfusions or inotropic therapy. (See 'Additional therapies' above.)
Prompt identification and treatment of the site of infection are essential. Sputum and
urine should be collected for gram stain and culture. Intra-abdominal fluid collections
should be percutaneously sampled. Blood should be taken from two distinct
venipuncture sites and from indwelling vascular access devices and cultured
aerobically and anaerobically. (See 'Identification of the septic focus' above.)
Antibiotics should be administered immediately after appropriate cultures have been
obtained. We recommend empiric broad spectrum antibiotics when a definite source
of infection can not be identified (Grade 1B). (See 'Antimicrobial regimen' above.)
Potentially infected vascular access devices should be removed (if possible),
abscesses should be drained, and extensive soft tissue infections should be debrided
or amputated (table 3). (See 'Eradication of infection' above.)
Glucocorticoid therapy, nutritional support, and glucose control are additional issues
that are important in the management of patients with severe sepsis or septic shock.
Each is discussed separately. (See "Corticosteroid therapy in septic shock" and
"Nutrition support in critically ill patients: An overview" and "Glycemic control and
intensive insulin therapy in critical illness".)
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
1. Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United
States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001;
29:1303.
2. Bernard GR, Wheeler AP, Russell JA, et al. The effects of ibuprofen on the physiology and
survival of patients with sepsis. The Ibuprofen in Sepsis Study Group. N Engl J Med 1997;
336:912.
3. McCloskey RV, Straube RC, Sanders C, et al. Treatment of septic shock with human
monoclonal antibody HA-1A. A randomized, double-blind, placebo-controlled trial. CHESS
Trial Study Group. Ann Intern Med 1994; 121:1.
4. Zeni F, Freeman B, Natanson C. Anti-inflammatory therapies to treat sepsis and septic
shock: a reassessment. Crit Care Med 1997; 25:1095.
5. Sasse KC, Nauenberg E, Long A, et al. Long-term survival after intensive care unit
admission with sepsis. Crit Care Med 1995; 23:1040.
6. Annane D, Bellissant E, Cavaillon JM. Septic shock. Lancet 2005; 365:63.
7. Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Campaign: international guidelines
for management of severe sepsis and septic shock: 2008. Crit Care Med 2008; 36:296.
8. Hollenberg SM, Ahrens TS, Annane D, et al. Practice parameters for hemodynamic support
of sepsis in adult patients: 2004 update. Crit Care Med 2004; 32:1928.
9. Practice parameters for hemodynamic support of sepsis in adult patients in sepsis. Task
Force of the American College of Critical Care Medicine, Society of Critical Care Medicine.
Crit Care Med 1999; 27:639.
10. Sessler CN, Perry JC, Varney KL. Management of severe sepsis and septic shock. Curr Opin
Crit Care 2004; 10:354.
11. Luce JM. Pathogenesis and management of septic shock. Chest 1987; 91:883.
12. Ghosh S, Latimer RD, Gray BM, et al. Endotoxin-induced organ injury. Crit Care Med 1993;
21:S19.
13. Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe
sepsis and septic shock. N Engl J Med 2001; 345:1368.
14. Michard F, Boussat S, Chemla D, et al. Relation between respiratory changes in arterial
pulse pressure and fluid responsiveness in septic patients with acute circulatory failure. Am
J Respir Crit Care Med 2000; 162:134.
15. Walley KR. Use of central venous oxygen saturation to guide therapy. Am J Respir Crit Care
Med 2011; 184:514.
16. Harvey S, Harrison DA, Singer M, et al. Assessment of the clinical effectiveness of
pulmonary artery catheters in management of patients in intensive care (PAC-Man): a
randomised controlled trial. Lancet 2005; 366:472.
17. Richard C, Warszawski J, Anguel N, et al. Early use of the pulmonary artery catheter and
outcomes in patients with shock and acute respiratory distress syndrome: a randomized
controlled trial. JAMA 2003; 290:2713.
18. National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS)
Clinical Trials Network, Wheeler AP, Bernard GR, et al. Pulmonary-artery versus central
venous catheter to guide treatment of acute lung injury. N Engl J Med 2006; 354:2213.
19. Brennan JM, Blair JE, Hampole C, et al. Radial artery pulse pressure variation correlates with
brachial artery peak velocity variation in ventilated subjects when measured by internal
medicine residents using hand-carried ultrasound devices. Chest 2007; 131:1301.
20. Eikermann M, Magder S, Malhotra A. Is brachial artery peak velocity variation ready for
prime time? Chest 2007; 131:1279.
21. Monnet X, Rienzo M, Osman D, et al. Esophageal Doppler monitoring predicts fluid
responsiveness in critically ill ventilated patients. Intensive Care Med 2005; 31:1195.
22. Reuter DA, Bayerlein J, Goepfert MS, et al. Influence of tidal volume on left ventricular
stroke volume variation measured by pulse contour analysis in mechanically ventilated
patients. Intensive Care Med 2003; 29:476.
23. Cavallaro F, Sandroni C, Marano C, et al. Diagnostic accuracy of passive leg raising for
prediction of fluid responsiveness in adults: systematic review and meta-analysis of clinical
studies. Intensive Care Med 2010; 36:1475.
24. Gattinoni L, Brazzi L, Pelosi P, et al. A trial of goal-oriented hemodynamic therapy in
critically ill patients. SvO2 Collaborative Group. N Engl J Med 1995; 333:1025.
25. Jones AE, Brown MD, Trzeciak S, et al. The effect of a quantitative resuscitation strategy on
mortality in patients with sepsis: a meta-analysis. Crit Care Med 2008; 36:2734.
26. Jones AE, Shapiro NI, Trzeciak S, et al. Lactate clearance vs central venous oxygen
saturation as goals of early sepsis therapy: a randomized clinical trial. JAMA 2010; 303:739.
27. National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS)
Clinical Trials Network, Wiedemann HP, Wheeler AP, et al. Comparison of two fluid-
management strategies in acute lung injury. N Engl J Med 2006; 354:2564.
28. Wilkes MM, Navickis RJ. Patient survival after human albumin administration. A meta-
analysis of randomized, controlled trials. Ann Intern Med 2001; 135:149.
29. Choi PT, Yip G, Quinonez LG, Cook DJ. Crystalloids vs. colloids in fluid resuscitation: a
systematic review. Crit Care Med 1999; 27:200.
30. Finfer S, Bellomo R, Boyce N, et al. A comparison of albumin and saline for fluid
resuscitation in the intensive care unit. N Engl J Med 2004; 350:2247.
31. Brunkhorst FM, Engel C, Bloos F, et al. Intensive insulin therapy and pentastarch
resuscitation in severe sepsis. N Engl J Med 2008; 358:125.
32. Reinhart K, Bloos F, Spies C. Vasoactive drug therapy in sepsis. In: Clinical Trials for the
treatment of sepsis, Sibbald WJ, Vincent JL (Eds), Springer Verlag, Berlin 1995. p.207.
33. De Backer D, Biston P, Devriendt J, et al. Comparison of dopamine and norepinephrine in
the treatment of shock. N Engl J Med 2010; 362:779.
34. Rhodes A, Bennett ED. Early goal-directed therapy: an evidence-based review. Crit Care
Med 2004; 32:S448.
35. Bersten AD, Hersch M, Cheung H, et al. The effect of various sympathomimetics on the
regional circulations in hyperdynamic sepsis. Surgery 1992; 112:549.
36. Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial
of transfusion requirements in critical care. Transfusion Requirements in Critical Care
Investigators, Canadian Critical Care Trials Group. N Engl J Med 1999; 340:409.
37. Forsythe SM, Schmidt GA. Sodium bicarbonate for the treatment of lactic acidosis. Chest
2000; 117:260.
38. Third European Consensus Conference in Intensive Care Medicine. Tissue hypoxia: How to
detect, how to correct, how to prevent. Société de Réanimation de Langue Française. The
American Thoracic Society. European Society of Intensive Care Medicine. Am J Respir Crit
Care Med 1996; 154:1573.
39. Gutierrez G, Palizas F, Doglio G, et al. Gastric intramucosal pH as a therapeutic index of
tissue oxygenation in critically ill patients. Lancet 1992; 339:195.
40. Poeze M, Solberg BC, Greve JW, Ramsay G. Monitoring global volume-related hemodynamic
or regional variables after initial resuscitation: What is a better predictor of outcome in
critically ill septic patients? Crit Care Med 2005; 33:2494.
41. Rangel-Frausto MS, Pittet D, Costigan M, et al. The natural history of the systemic
inflammatory response syndrome (SIRS). A prospective study. JAMA 1995; 273:117.
42. Brun-Buisson C, Doyon F, Carlet J, et al. Incidence, risk factors, and outcome of severe
sepsis and septic shock in adults. A multicenter prospective study in intensive care units.
French ICU Group for Severe Sepsis. JAMA 1995; 274:968.
43. Wheeler AP, Bernard GR. Treating patients with severe sepsis. N Engl J Med 1999; 340:207.
44. Clec'h C, Fosse JP, Karoubi P, et al. Differential diagnostic value of procalcitonin in surgical
and medical patients with septic shock. Crit Care Med 2006; 34:102.
45. Tang BM, Eslick GD, Craig JC, McLean AS. Accuracy of procalcitonin for sepsis diagnosis in
critically ill patients: systematic review and meta-analysis. Lancet Infect Dis 2007; 7:210.
46. Ruiz-Alvarez MJ, García-Valdecasas S, De Pablo R, et al. Diagnostic efficacy and prognostic
value of serum procalcitonin concentration in patients with suspected sepsis. J Intensive
Care Med 2009; 24:63.
47. Schuetz P, Chiappa V, Briel M, Greenwald JL. Procalcitonin algorithms for antibiotic therapy
decisions: a systematic review of randomized controlled trials and recommendations for
clinical algorithms. Arch Intern Med 2011; 171:1322.
48. Gibot S, Kolopp-Sarda MN, Béné MC, et al. Plasma level of a triggering receptor expressed
on myeloid cells-1: its diagnostic accuracy in patients with suspected sepsis. Ann Intern Med
2004; 141:9.
49. Gibot S, Cravoisy A, Kolopp-Sarda MN, et al. Time-course of sTREM (soluble triggering
receptor expressed on myeloid cells)-1, procalcitonin, and C-reactive protein plasma
concentrations during sepsis. Crit Care Med 2005; 33:792.
50. Gibot S, Le Renard PE, Bollaert PE, et al. Surface triggering receptor expressed on myeloid
cells 1 expression patterns in septic shock. Intensive Care Med 2005; 31:594.
51. Seder CW, Villalba MR Jr, Robbins J, et al. Early colectomy may be associated with improved
survival in fulminant Clostridium difficile colitis: an 8-year experience. Am J Surg 2009;
197:302.
52. Gaieski DF, Mikkelsen ME, Band RA, et al. Impact of time to antibiotics on survival in
patients with severe sepsis or septic shock in whom early goal-directed therapy was
initiated in the emergency department. Crit Care Med 2010; 38:1045.
53. Johnson MT, Reichley R, Hoppe-Bauer J, et al. Impact of previous antibiotic therapy on
outcome of Gram-negative severe sepsis. Crit Care Med 2011; 39:1859.
54. Verhoef J, Hustinx WM, Frasa H, Hoepelman AI. Issues in the adjunct therapy of severe
sepsis. J Antimicrob Chemother 1996; 38:167.
55. Sibbald WJ, Vincent JL. Round table conference on clinical trials for the treatment of sepsis.
Crit Care Med 1995; 23:394.
56. Garnacho-Montero J, Garcia-Garmendia JL, Barrero-Almodovar A, et al. Impact of adequate
empirical antibiotic therapy on the outcome of patients admitted to the intensive care unit
with sepsis. Crit Care Med 2003; 31:2742.
57. Ibrahim EH, Sherman G, Ward S, et al. The influence of inadequate antimicrobial treatment
of bloodstream infections on patient outcomes in the ICU setting. Chest 2000; 118:146.
58. Harbarth S, Garbino J, Pugin J, et al. Inappropriate initial antimicrobial therapy and its effect
on survival in a clinical trial of immunomodulating therapy for severe sepsis. Am J Med
2003; 115:529.
59. Leibovici L, Paul M, Poznanski O, et al. Monotherapy versus beta-lactam-aminoglycoside
combination treatment for gram-negative bacteremia: a prospective, observational study.
Antimicrob Agents Chemother 1997; 41:1127.
60. Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective
antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care
Med 2006; 34:1589.
61. Schramm GE, Johnson JA, Doherty JA, et al. Methicillin-resistant Staphylococcus aureus
sterile-site infection: The importance of appropriate initial antimicrobial treatment. Crit Care
Med 2006; 34:2069.
62. Kumar A, Ellis P, Arabi Y, et al. Initiation of inappropriate antimicrobial therapy results in a
fivefold reduction of survival in human septic shock. Chest 2009; 136:1237.
63. McDonald JR, Friedman ND, Stout JE, et al. Risk factors for ineffective therapy in patients
with bloodstream infection. Arch Intern Med 2005; 165:308.
64. Miller LG, Perdreau-Remington F, Rieg G, et al. Necrotizing fasciitis caused by community-
associated methicillin-resistant Staphylococcus aureus in Los Angeles. N Engl J Med 2005;
352:1445.
65. Fridkin SK, Hageman JC, Morrison M, et al. Methicillin-resistant Staphylococcus aureus
disease in three communities. N Engl J Med 2005; 352:1436.
66. Francis JS, Doherty MC, Lopatin U, et al. Severe community-onset pneumonia in healthy
adults caused by methicillin-resistant Staphylococcus aureus carrying the Panton-Valentine
leukocidin genes. Clin Infect Dis 2005; 40:100.
67. Rubinstein E, Lode H, Grassi C. Ceftazidime monotherapy vs. ceftriaxone/tobramycin for
serious hospital-acquired gram-negative infections. Antibiotic Study Group. Clin Infect Dis
1995; 20:1217.
68. Cometta A, Calandra T, Gaya H, et al. Monotherapy with meropenem versus combination
therapy with ceftazidime plus amikacin as empiric therapy for fever in granulocytopenic
patients with cancer. The International Antimicrobial Therapy Cooperative Group of the
European Organization for Research and Treatment of Cancer and the Gruppo Italiano
Malattie Ematologiche Maligne dell'Adulto Infection Program. Antimicrob Agents Chemother
1996; 40:1108.
69. Safdar N, Handelsman J, Maki DG. Does combination antimicrobial therapy reduce mortality
in Gram-negative bacteraemia? A meta-analysis. Lancet Infect Dis 2004; 4:519.
70. Paul M, Benuri-Silbiger I, Soares-Weiser K, Leibovici L. Beta lactam monotherapy versus
beta lactam-aminoglycoside combination therapy for sepsis in immunocompetent patients:
systematic review and meta-analysis of randomised trials. BMJ 2004; 328:668.
71. Paul M, Silbiger I, Grozinsky S, et al. Beta lactam antibiotic monotherapy versus beta
lactam-aminoglycoside antibiotic combination therapy for sepsis. Cochrane Database Syst
Rev 2006; :CD003344.
72. Marshall J, Lowry S. Evaluation of the adequacy of source control. In: Clinical Trials for the
treatment of sepsis, Sibbald WJ, Vincent JL (Eds), Springer Verlag, Berlin 1995. p.329.
73. McCowen KC, Malhotra A, Bistrian BR. Stress-induced hyperglycemia. Crit Care Clin 2001;
17:107.
74. Kortgen A, Niederprüm P, Bauer M. Implementation of an evidence-based "standard
operating procedure" and outcome in septic shock. Crit Care Med 2006; 34:943.
75. Shapiro NI, Howell MD, Talmor D, et al. Implementation and outcomes of the Multiple
Urgent Sepsis Therapies (MUST) protocol. Crit Care Med 2006; 34:1025.
76. Micek ST, Roubinian N, Heuring T, et al. Before-after study of a standardized hospital order set for the management of septic shock. Crit Care Med 2006; 34:2707.
Topic 1613 Version 11.0
GRAPHICS

Definitions of systemic inflammatory response syndrome (SIRS) and different degrees of severity of sepsis
Condition Description
Systemic inflammatory response syndrome
Two or more of the following conditions: temperature >38.5°C or <35.0°C; heart rate of >90 beats/min; respiratory rate of >20 breaths/min or PaCO2 of <32 mm Hg; and WBC count of >12,000 cells/mL, <4000 cells/mL, or >10 percent immature (band) forms
Sepsis SIRS in response to documented infection (culture or Gram stain of blood, sputum, urine, or normally sterile body fluid positive for pathogenic
microorganism; or focus of infection identified by visual inspection, eg, ruptured bowel with free air or bowel contents found in abdomen at surgery, wound with purulent discharge)
Severe sepsis Sepsis and at least one of the following signs of organ hypoperfusion or organ dysfunction: areas of mottled skin; capillary refilling of ≥3 s; urinary output of <0.5 mL/kg for at least 1 h or renal replacement therapy; lactate >2 mmol/L; abrupt change in mental status or abnormal EEG findings; platelet count of <100,000 cells/mL or disseminated intravascular coagulation; acute lung injury/ARDS; and cardiac dysfunction (echocardiography)
Septic shock Severe sepsis and one of the following conditions: systemic mean BP of <60 mm Hg (<80 mm Hg if previous hypertension) after 20 to 30 mL/kg starch or
40 to 60 mL/kg saline solution, or PCWP between 12 and 20 mm Hg; and need for dopamine of >5 mcg/kg/min, or norepinephrine or epinephrine of <0.25 mcg/kg/min to maintain mean BP at >60 mm Hg (80 mm Hg if previous hypertension)
Refractory septic shock
Need for dopamine at >15 mcg/kg/min, or norepinephrine or epinephrine at >0.25 mcg/kg/min to maintain mean BP at >60 mm Hg (80 mm Hg if previous hypertension)
WBC count: white blood cell count; BP: blood pressure. Data from: Annane, D, Bellissant, E, Cavaillon, JM. Septic shock. Lancet 2005; 365:63.
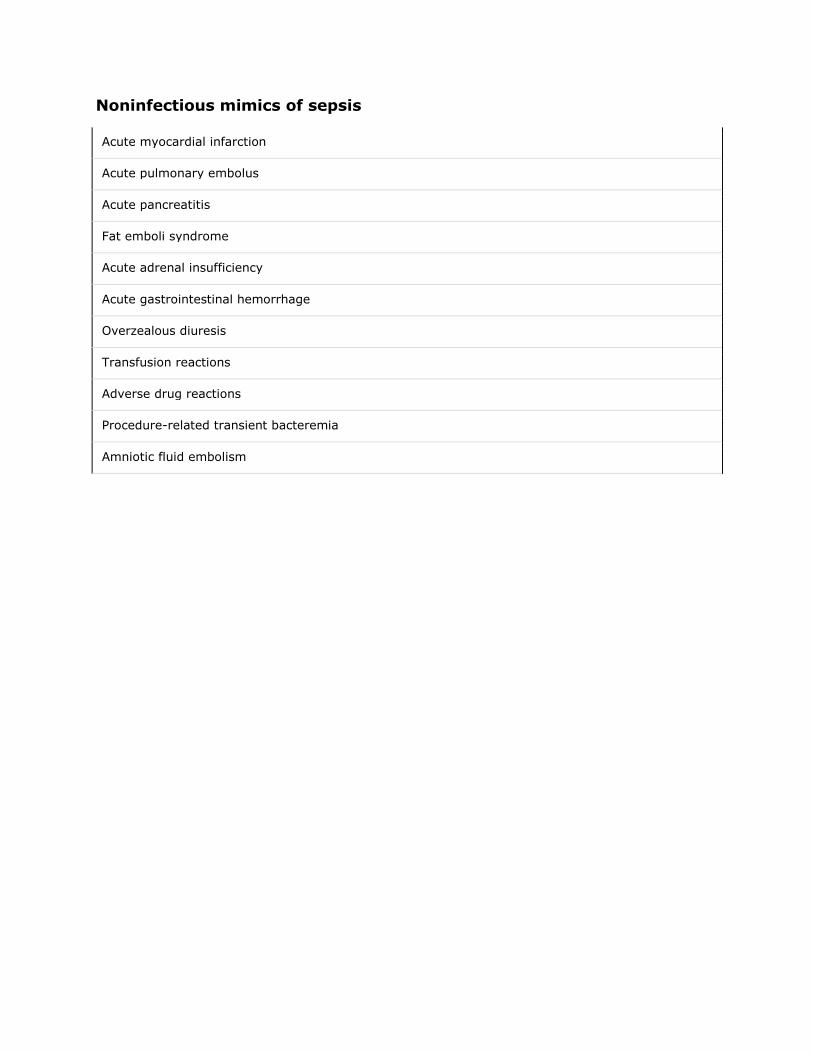
Noninfectious mimics of sepsis
Acute myocardial infarction
Acute pulmonary embolus
Acute pancreatitis
Fat emboli syndrome
Acute adrenal insufficiency
Acute gastrointestinal hemorrhage
Overzealous diuresis
Transfusion reactions
Adverse drug reactions
Procedure-related transient bacteremia
Amniotic fluid embolism

Adapted from Cuhna, BA, Crit Care Clin 1998; 14:1
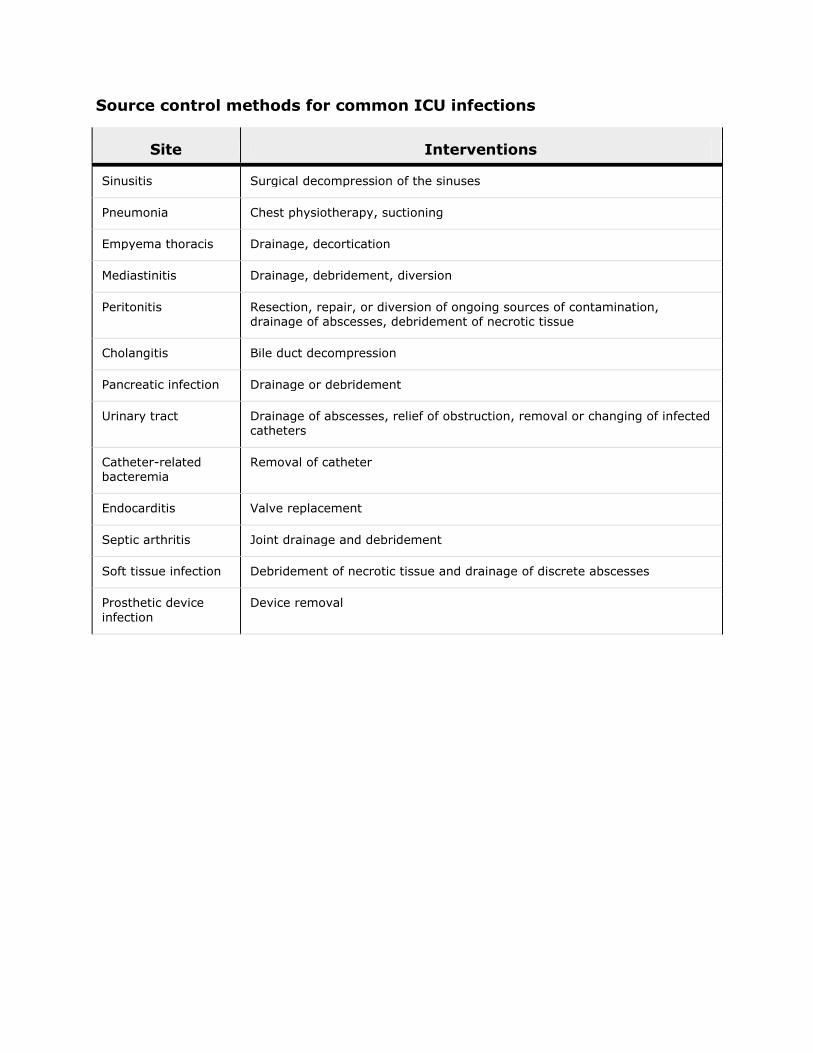
Source control methods for common ICU infections
Site Interventions
Sinusitis Surgical decompression of the sinuses
Pneumonia Chest physiotherapy, suctioning
Empyema thoracis Drainage, decortication
Mediastinitis Drainage, debridement, diversion
Peritonitis Resection, repair, or diversion of ongoing sources of contamination, drainage of abscesses, debridement of necrotic tissue
Cholangitis Bile duct decompression
Pancreatic infection Drainage or debridement
Urinary tract Drainage of abscesses, relief of obstruction, removal or changing of infected catheters
Catheter-related bacteremia
Removal of catheter
Endocarditis Valve replacement
Septic arthritis Joint drainage and debridement
Soft tissue infection Debridement of necrotic tissue and drainage of discrete abscesses
Prosthetic device
infection
Device removal
Adapted from Marshall, JC, Lowry, SF. Evaluation of the adequacy of source control. In: Sibbald, WJ, Vincent, JL, Clinical Trials for the Treatment of Sepsis. Springer-Verlag, Berlin, 1995 p 329.
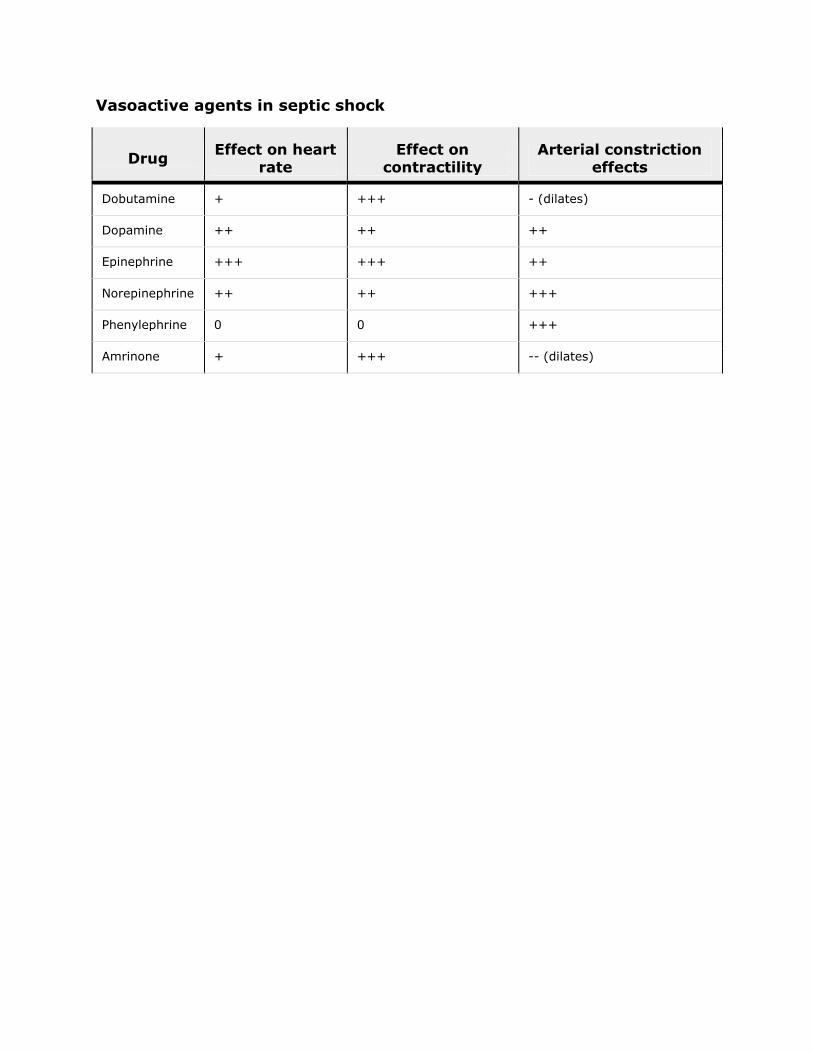
Vasoactive agents in septic shock
Drug Effect on heart
rate Effect on
contractility Arterial constriction
effects
Dobutamine + +++ - (dilates)
Dopamine ++ ++ ++
Epinephrine +++ +++ ++
Norepinephrine ++ ++ +++
Phenylephrine 0 0 +++
Amrinone + +++ -- (dilates)
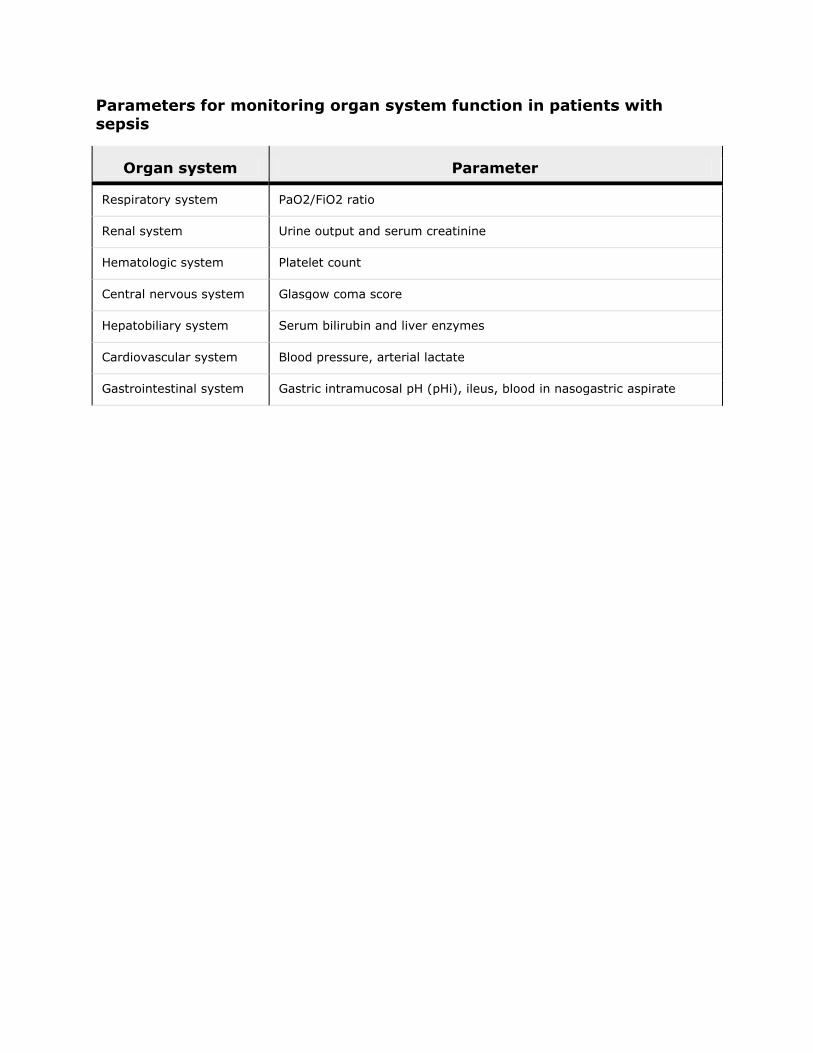
Parameters for monitoring organ system function in patients with sepsis
Organ system Parameter
Respiratory system PaO2/FiO2 ratio
Renal system Urine output and serum creatinine
Hematologic system Platelet count
Central nervous system Glasgow coma score
Hepatobiliary system Serum bilirubin and liver enzymes
Cardiovascular system Blood pressure, arterial lactate
Gastrointestinal system Gastric intramucosal pH (pHi), ileus, blood in nasogastric aspirate
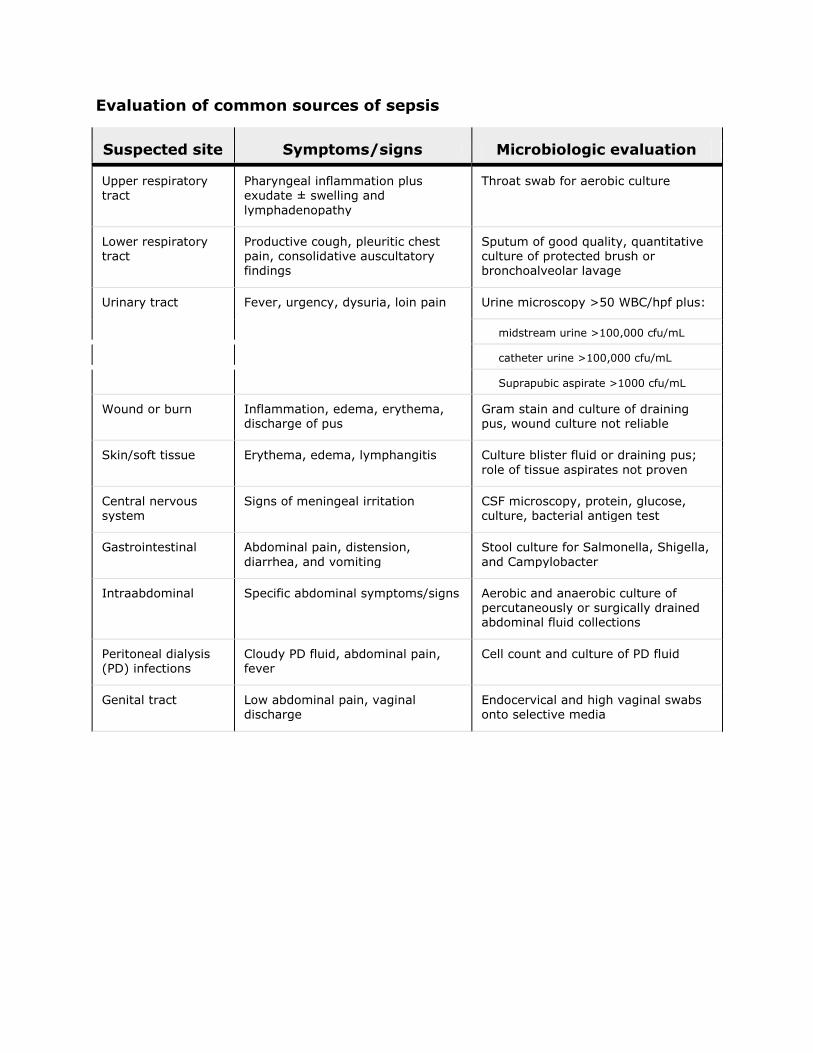
Evaluation of common sources of sepsis
Suspected site Symptoms/signs Microbiologic evaluation
Upper respiratory tract
Pharyngeal inflammation plus exudate ± swelling and
lymphadenopathy
Throat swab for aerobic culture
Lower respiratory tract
Productive cough, pleuritic chest pain, consolidative auscultatory findings
Sputum of good quality, quantitative culture of protected brush or bronchoalveolar lavage
Urinary tract Fever, urgency, dysuria, loin pain Urine microscopy >50 WBC/hpf plus:
midstream urine >100,000 cfu/mL
catheter urine >100,000 cfu/mL
Suprapubic aspirate >1000 cfu/mL
Wound or burn Inflammation, edema, erythema, discharge of pus
Gram stain and culture of draining pus, wound culture not reliable
Skin/soft tissue Erythema, edema, lymphangitis Culture blister fluid or draining pus;
role of tissue aspirates not proven
Central nervous system
Signs of meningeal irritation CSF microscopy, protein, glucose, culture, bacterial antigen test
Gastrointestinal Abdominal pain, distension,
diarrhea, and vomiting
Stool culture for Salmonella, Shigella,
and Campylobacter
Intraabdominal Specific abdominal symptoms/signs Aerobic and anaerobic culture of percutaneously or surgically drained abdominal fluid collections
Peritoneal dialysis (PD) infections
Cloudy PD fluid, abdominal pain, fever
Cell count and culture of PD fluid
Genital tract Low abdominal pain, vaginal discharge
Endocervical and high vaginal swabs onto selective media
Adapted from Cohen, J, Microbiologic requirements for studies of sepsis. In: Sibbald, WJ, Vincent, JL (eds), Clinical Trials for the Treatment of Sepsis, Springer-Verlag, Berlin, 1995, p 73.
© 2012 UpToDate, Inc. All rights reserved. | Subscription and License Agreement |Release: 20.3 - C20.4 Licensed to: UpToDate Individual Web - Elena Copaciu |Support Tag: [ecapp0505p.utd.com-92.55.145.242-67D204B38A-6.14-178237618] | Your UpToDate subscription will expire in 24 day(s). Click here to renew.
Print Options
Text
References
Graphics