futrue health threats initiative report january 9, 2017 (1)
TRANSCRIPT
Future Health Threat s In it iat ive
An Integrated Approach to Public Health Security
Bibliothèque Solvay, 9 January, 2017
With Support of Praesens Fund

Future Health Threat s In it iat ive
An Integrated Approach to Public Health Security
Bibliothèque Solvay, 9 January, 2017
With Support of Praesens Fund

Future Health Threats Initiative 5
The Praesens Fund is an entity whose purpose is to improve world health by providing in situ disease surveillance through quality molecular diagnostics to social environments in need, irrespective of location and means. The scope of our mission embraces discrete situations in the world in which a measurable impact can be achieved. The fund operates within the frame of the King Baudouin Foundation.
The Fund, created by biotech entrepreneur Rudi Pauwels has the aim of raising philanthropic funds to provide and promote the use of molecular diagnostics in resource-poor settings as well as to improve rapid response capabilities and surveillance in areas regularly affected by epidemic and endemic diseases. The name of the Fund therefore reflects the notion of “present here at the present time to improve health”.
The steering committee that manages the Praesens Fund is composed of: Prof. dr. Peter Piot, Mr. Luc Tayart de Borms and Dr. Rudi Pauwels.
IntroductionWe believe no community is too remote to help.”

Future Health Threats Initiative 7
Recommendations .............................................................................9
Four recommendations resulting from the 9, January
symposium
Program Outline ................................................................................. 10
Chairmen & Speakers Biographies .............................................. 13
Analysis .................................................................................................21
Jill Bellamy, UN Counter Terrorism Task Force/Biodefence
consultant provides background and a deeper analysis of
Future Health Threats
Future Health Threats Initiative Working Group ...................43
Summary of Speaker Discussions ..............................................45
Lessons Learned ...............................................................................46
Quotes ....................................................................................................49
Praesens Fund Mission Statement ..............................................51
Contents
Future Health Threats Initiative 9
Four Recommendations following the Praesen’s Fund Future Health Threats Initiative Symposium, 9, January, 2017
1. Implement a strategy to coordinate international level response to emergency disease outbreaks.
2. Collaboration among international public health institutions must address increasing laboratory surge
capacity as a key component for containing future infectious disease and emergency disease outbreaks.
3. Rapid response requires investment in sustainable technologies and grass root initiatives, to create and maintain a public health infrastructure in the weakest states.
4. Increasing cross-sector partnerships: public-private collaborations and civil-military interoperability will
support efforts to rapidly respond to outbreaks of emergency disease and increase capabilities of the
global health community.
The Future Health Threats Initiative will work, throughout 2017, to translate these recommendations into actionable results via a FHTI Working Group project comprised of international experts in public health and emergency disease response.
Recommendations
Future Health Threats Initiative, Bibliothèque Solvay,
Brussels, Belgium, 9 January 2017
Future Health Threats Initiative 11
Program
Registration and Welcome
Keynote Prof. Dr. Piot: Are we ready for the next big epidemic?
Mr. De Brouwer (DG ECHO): Ebola and the European Medical Corps
Mr. Jean-Louis De Bouwer, Director of Operations, the European Commission’s Humanitarian Aid and Civil Protection Department (ECHO)
Coffee Break
Dr. Rudi Pauwels: Expanding rapid molecular diagnostic field capabilities during disease outbreaksMobile Unit Revealed
Reception and Walking Dinner
Registration and Welcome Coffee
Symposium Opening: Welcome Speech by Dr. Pauwels and Prof. Dr. Piot
Panel One: Laboratory Surge Capacity: A vital tool in emergency disease containment
Prof. dr. Guido van der Groen, former Head of the Virology Unit of the Institute of Tropical Medicine, Antwerp
Prof. dr. Kevin Ariën, Unit of Virology, Institute of Tropical Medicine, Antwerp
Ms. Hilde De Clerck, Mobile implementation officer, Médecins Sans Frontières, Belgique
Dr. Tim Brooks, Clinical Services Director, RIPL, Public Health England
Mr. Conor Elliott, Director of Programmes, GOAL
Coffee Break
Panel Two: Developing a Rapid Reaction Force to Counter Emerging and Re-emerging Disease Outbreaks
Ms. Dorinda Vandecauter, Belgian Defense, Teamleader B-Fast Guinea Mission
Dr. Jessica Vanhomwegen, Head of the Viral Identification Team, Laboratory for UrgentResponse to Biological Threats, Institute Pasteur
Mr. Loic Lallemand Zeller, Head of Unit Emergency Response Coordination Centre, The European Commission’s Humanitarian Aid and Civil Protection Department (ECHO)
Prof. dr. Marion Koopmans, Head of the Viroscience Department, Erasmus MC, The Netherlands
Dr. Daniel Reynders, Head of the International Relations Unit, the Belgian Federal Public Service (FPS) of Health, Food Chain Safety and Environment
Discussion and Wrap up
Luncheon
•
•
•
•
•
•
•
•
•
•
•
09:30 - 10:00
10:00 - 10:15
10:15 - 11:30
11:30 - 11:45
11:45 - 12:45
12:45 - 13:00
13:00 - 14:15
14:00 - 14:15
14:15 - 14:45
14:45 - 15:00
15:00 - 15:15
15:15 - 19:00
17:00 - 19:00
The program was chaired by Dr. Rudi Pauwels,
biotech entrepreneur and founder of the Praesens Fund
and Dr. Jill Bellamy, United Nations Counter-Terrorism Task Force
Future Health Threats Initiative, Solvay Library, Brussels, Belgium, 9 January 2017

Future Health Threats Initiative 13
ChairmenPROF. DR. PETER PIOT
Peter Piot is the Director of the London School of Hygiene and Tropical Medicine and a Professor of Global Health. In 2009-2010 he was the Director of the Institute for Global Health at Imperial College, London. He was the founding Executive Director of UNAIDS and Under Secretary-General of the United Nations from 1995 until 2008, and was an Associate Director of the Global Programme on AIDS of WHO. Under his leadership UNAIDS became the chief advocate for worldwide action against AIDS, also spearheading UN reform by bringing together 10 UN system organizations. He has a medical degree from the University of Ghent (1974), and a PhD in Microbiology from the University of Antwerp (1980). In 1976 he co-discovered the Ebola virus in Zaire while working at the Institute of Tropical Medicine in Antwerp, Belgium, and led research on HIV/AIDS, sexually transmitted diseases and women’s health, mostly in sub-Saharan Africa. He was a professor of microbiology, and of public health at the Institute of Tropical Medicine, Antwerp, the Free University of Brussels, and the University of Nairobi, was a Senior Fellow at the University of Washington, a Scholar in Residence at the Ford Foundation, and a Senior Fellow at the Bill & Melinda Gates Foundation. He has received numerous scientific and civic awards including an honorary doctorate from seven universities, the Canada Gairdner Global Health Award, Robert Koch Gold medal, Prix International INSERM, Paris (2015). He was a 2014 TIME Person of the Year (The Ebola Fighters), and received the Prince Mahidol Award for Public Health. He has published over 580 scientific articles and 17 books, including his memoir ‘No Time to Lose’ in 2012 (WW Norton), translated into French, Dutch, Japanese and Korean, and ‘AIDS between science and politics’ in 2015 (Columbia University Press).

Future Health Threats Initiative 15
PROF. DR. GUIDO VAN DER GROEN
Guido van der Groen is emeritus professor of virology and former head of the Unit of Microbiology of the Institute for Tropical Medicine in Antwerp. He is a co-discoverer of the Ebola Zaire virus in 1976. During 1977 - 1981, he trained to work in high security labs (HSL) in the US, knowledge allowing him to build, at ITM, the smallest and cheapest HSL on earth. In 1980, he actively contributed to the eradication of smallpox, and discovered the existence of Hantaviruses in Belgium and many other countries, while working on Ebola in the HSLs of Fort Detrick. Between 1982 and 2002, he actively participated in the worldwide fight against AIDS, under the impulse of his colleague Peter Piot. Between 2003 and 2008, he was Professor Molecular Targets in infected cells in AIDS research at the Free University of Brussels (VUB).
PROF. DR. KEVIN ARIËN
Kevin K. Ariën obtained his PhD in 2005 from the Universiteit Antwerpen on HIV replicative fitness. After a 1-year intermezzo in pharmaceutical industry with Tibotec-Virco, he started postdoctoral research in 2006 in the lab of Prof. Dr. Bruno Verhasselt at the Universiteit Gent, studying various molecular and immunological aspects of the HIV accessory protein Nef. In late 2009, Kevin returned to the ITM to study HIV sexual transmission and prevention through topical microbicides. In June 2014, he was appointed head of ITM’s Virology Unit, director of the Virus BSL3 facility and Professor of Virology. In the context of the 2013-2016 Ebola epidemic in West Africa, the Unit developed Ebola virus diagnostic testing at ITM, as part of the National Reference Center for Tropical Infectious Diseases. His current research efforts on tropical viruses focus on the development of new diagnostic tests for the simultaneous detection of a wide variety of epidemiologically relevant arboviruses and haemorrhagic fever viruses, in the context of a VLAIO innovation mandate. Kevin serves as scientific adviser to the National Ebola Coordinator and as a technical expert for HIV, Ebola and Zika diagnostics to the World Health Organisation.
DR. RUDI PAUWELS
Rudi Pauwels, PhD (M), is the Chief Executive Officer of Biocartis and founded the company in 2007. As a pharmaceutical scientist (1960, Belgium), he belonged to the first group of HIV/AIDS researchers who, shortly after the discovery of HIV in 1983-1984, started the efforts to find new treatments for HIV (AIDS). For nearly 3 decades, he mainly focused on the search and development of anti-HIV drugs, a number of which have been approved and introduced in the clinic while generating several billion USD revenue and the development of diagnostic technologies and products that address the needs in this new era of high precision, more personalized medicine. His research as well as his entrepreneurial career is driven by medical needs and the passion to advance medicine while holding a strong belief in the value of a multidisciplinary: scientific, technological and clinical approach to solve the key pharmaceutical and diagnostic challenges. In 2004 he expanded his areas of interest into micro- and nanotechnology and went on a 3-year sabbatical at the Swiss Federal Institute of Technology-EPFL (Lausanne, Switzerland), one of the leading research centres in this emerging field. Mr. Pauwels received several awards for excelling and inspiring in medical innovations and technologies. In 2012, he and Biocartis received the Global Technology Pioneer Award from the World Economic Forum (Davos, Switzerland). Mr. Pauwels received an honorary Doctorate Degree from the University of Ghent in 2013. In 2016, he was received as Honorary Speaker at the Distinguished Technopreneur Speaker (DTS) Forum in Singapore, for excelling and inspiring in innovative value creation and unleashing the potential of technological innovation. In July 2016, he was honoured with the noble title ‘Commandeur in de Leopoldsorde’ by the King of Belgium. He is (co)-author of more than 150 papers in peer-reviewed journals and is the recipient of several awards for his scientific and entrepreneurial accomplishments. Mr. Pauwels holds a PhD in Pharmaceutical Sciences from the Katholieke Universiteit Leuven, Belgium.
Speakers

Future Health Threats Initiative 17
CONOR ELLIOTT
With 17 years professional experience in humanitarian and development assistance around the world, Conor is currently responsible for ensuring the effective delivery of humanitarian and development programmes in a range of conflict, post conflict, fragile states and stable development environments in 18 countries around the work. For 5 years Conor has been the Director of Programmes and Operations at GOAL, an international humanitarian organisation. Conor has directed GOAL’s response in crises such as Syria, Iraq, South Sudan, and Ebola in West Africa amongst others. Conor also directs GOAL’s Humanitarian Response Unit which is a rapid response surge team deployed to meet immediate needs in the aftermath of a sudden onset disaster. In recent years GOALs surge team has responded in Yemen, Philippines (Yolanda), Syria, South Sudan, Myanmar, and Nepal among others. In earlier positons with GOAL Conor has lead rapid response teams on deployment in Darfur, Niger, Philippines, Somalia, South Sudan and Malawi.
DORINDA VAN DE CAUTER
Dorinda’s military career started in the Royal Military Academy in 2002. She studied Social and Military Sciences until 2006. In 2008 she became a Platoon Commander of Leopoard 1 (tanks, cavalry), a second commander of a company in 2010, instructor of tactics and heavy weapon system in 2012. In 2015 she was also in charge of a bachelor year in the Royal Military Academy. From December 2014 until February 2015, she was the team leader of the B-Fast Mission in Guinea during the Ebola outbreak.
DR. JESSICA VANHOMWEGEN
Dr. Jessica Vanhomwegen is the head of the Viral Identification Group within the Laboratory for Urgent Response to Biological Threats at Institut Pasteur, Paris. Her main research interests include the diagnosis and surveillance of emerging and epidemic-prone pathogens, with a particular focus on the detection and characterization of a wide array of viral pathogens, including arboviruses and viral hemorrhagic fevers. Dr. Vanhomwegen has served on numerous outbreak investigation taskforces to respond rapidly to and support local investigation and control of infectious disease outbreaks.
MR. LOIC LALLEMAND-ZELLER
M. Loic Lallemand-Zeller works as Acting Head of the Emergency Response Coordination center in DG ECHO, European Commission; he was previously posted at the Delegation of the European Union to the United Nations in New York, where he served as the First Counsellor and Head of Humanitarian Team for the European Union. Previously, M. Lallemand-Zeller held various positions at the European Commission such as in the Near East Unit and Middle East Peace Process or as a Desk Officer for the relations with India. He also worked for various Delegations around the world such as the Head of Political and Economic Section in Damascus, Syria or in other cities including Bangkok, Mexico/La Havana.
DR. TIM BROOKS
Dr. Tim Brooks CBE is Head of the Rare and Imported Pathogens Laboratory (RIPL) at Public Health England, based at Porton Down in the UK. RIPL is a WHO collaborating laboratory for High Consequence Pathogens, and provides diagnostic and clinical advice for a wide range of unusual bacterial and viral pathogens. Tim Brooks is one of the leading partners in the national Imported Fever Service, which combines the clinical skills of the Liverpool and London Tropical Infectious Disease Hospitals with RIPL laboratory services. His research interests range from environmental detection of micro-organisms and clinical diagnostics, through aerobiology and decontamination, to disease pathogenesis and work for the European Space Agency. He led the PHE Ebola laboratories in Sierra Leone during the 2015 outbreak, and latterly in the surveillance phase in 2016.
HILDE DE CLERCK
Hilde De Clerck is a medical doctor working for Médecins Sans Frontières – Operational Centre Brussels. She went on several long-term missions: post-earthquake Pakistan (2006); health center conflict zone Ivory Coast (2007); chronic diseases (diabetes, hypertension and HIV, TB) Cambodia (2008); Lassa fever care (pediatric hospital) Sierra Leone (2013-2014). She currently holds the position of Mobile Implementation Officer Viral Hemorrhagic Fevers at Médecins Sans Frontières and spends most of her time as a technical referent in the field. Over the last 10 year, she intervened in 6 different Ebola/Marburg outbreaks and in the last Ebola outbreak she continuously did fieldwork from March 2014 until September 2014.

Future Health Threats Initiative 19
JEAN-LOUIS DE BROUWER
Jean-Louis De Brouwer, a Belgian, is Director for Europe, Eastern Neighbourhood and Middle East as of July 2016, in the European Commission’s Directorate-General for European Civil Protection and Humanitarian Aid Operations (ECHO). He joined ECHO in November 2012 as Director of Operations in the European Commission’s Humanitarian Aid and Civil Protection department, having previously been Director in charge of the coordination of employment politics in the Commission’s department for Employment and Social Affairs. Prior to that, he spent 18 years in the Justice and Home Affairs department, specialising in migration and asylum questions, latterly as Director in charge of border and visa issues. Before joining the European Commission, Mr. De Brouwer worked in the Belgian civil service (Ministry of Economic Affairs and Ministry of Home Affairs).
DR. DANIEL REYNDERS
Dr. Daniel Reynders currently holds the position of Head of the International Relations and Public Health Emergencies Unit at the Belgian Federal Public Service (FPS) of Health, Food Chain Safety and Environment. He is also WHO’s International Health Regulations Focal Point for Belgium (IHR) and National Focal Point for the Early Warning and Response System (EWRS) of the European Commission. He is Chair of the ECDC Management Board and Belgium’s representative to the Health Security Committee (European Council and Commission). He played a role in several health crises: during the recent Ebola Crisis as Deputy National Coordinator Ebola, the H1N1 pandemic management, both nationally (as deputy Interministerial Commissioner Influenza) and internationally, implemented a Health Vigilance Unit within the Directorate-General for Primary Health Care and Crisis Management at the Belgian FPS of Health. He also Served in Africa and Asia as public health officer for around 15 years.
PROF. DR. MARION KOOPMANS
Dr. Marion Koopmans (DVM, PhD) is head of the Viroscience department at the Erasmus MC in Rotterdam. Her responsibilities include reference diagnostics, syndromic surveillance and emergency preparedness for viral diseases, including research aimed at improving the response capacity of a public health lab. Her research interests focus enteric viruses, food-borne infections, emerging disease preparedness, and infections at the human-animal interface, with a particular focus on unraveling mechanisms underlying possible emergence of new health threats and optimizing the early detection and response. She has authored over 250 papers in peer reviewed journals. She also acts as the National microbiology focal point for the ECDC, being a senior microbiologist with excellent knowledge of the organization of microbiology and its applications in the public health arena in the country.
Future Health Threats Initiative 21
Historic Background
“The worst possible fears were confirmed in June or July (2014), that this was very different from ’76, [] context is extremely important. There had been civil war, a lack of trust, breakdown of health services because of civil war and dictatorship in Guinea. Most professionals had left the country. In Liberia there were 51 registered medical doctors and four of those worked for the ministry of health, so 47 for a population of 4.5 million. These are countries in reconstruction after civil war, still very fragile politically and with traditional beliefs in the causation of disease – it’s not pathogens but witchcraft.” 3 Prof. dr. Peter Piot
Introduction
On the 9th of January, 2017, Praesens’ Fund, supported by the King Boudewijn Foundation, convened its first meeting at the Bibliothèque Solvay in Brussels, to launch the Future Health Threats Initiative (FHTI). The Founder of Praesens Fund, Dr. Rudi Pauwels, opened the first session on laboratory capacity building, with an introduction covering his experience in the field and introducing the background to the founding of Praesens Fund. Following upon his highly insightful introduction, Keynote for the event Prof. dr. Peter Piot, the co-discoverer of Ebola virus, presented his distinguished experience on the discovery of Ebola virus, emerging and re-emerging disease and the future risk to global public health.
Dr. Jill Bellamy, appointed adviser to the United Nations Counter Terrorism Task Force, launched the program and debate with introductory remarks for FHTI expert group speakers. With a focus on best practices for countering emergency disease outbreaks and review of international collaborative efforts to contain public health threats, the meeting brought together experts from various international health institutes, academia, the medical defence community, NGO’s and private industry.
The concept of the program and idea to convene an expert group, developed from the general observation, that while public health is now considered by many nations to be a national security issue, and while the international community, brings considerable and highly advanced technical means to counter emergency health events to the table, coordination, which lies at the core of containment, remains an international challenge.
1 Peter Piot: the veteran scientist who helped to raise the alarm over Ebola, Boseley, S., The Guardian, 25, December, 2014. URL: https://www.theguardian.com/world/2014/dec/25/peter-piot-scientist-ebola-congo2 Joel G. Breman et al. Discovery and Description of Ebola Zaire Virus in 1976 and Relevance to the West African Epidemic During 2013–2016. The Journal of Infectious Diseases, June 2016 DOI: 10.1093/infdis/jiw207
3 Peter Piot: the veteran scientist who helped to raise the alarm over Ebola, Boseley, S., The Guardian, 25, December, 2014. URL: https://www.theguardian.com/world/2014/dec/25/peter-piot-scientist-ebola-congo
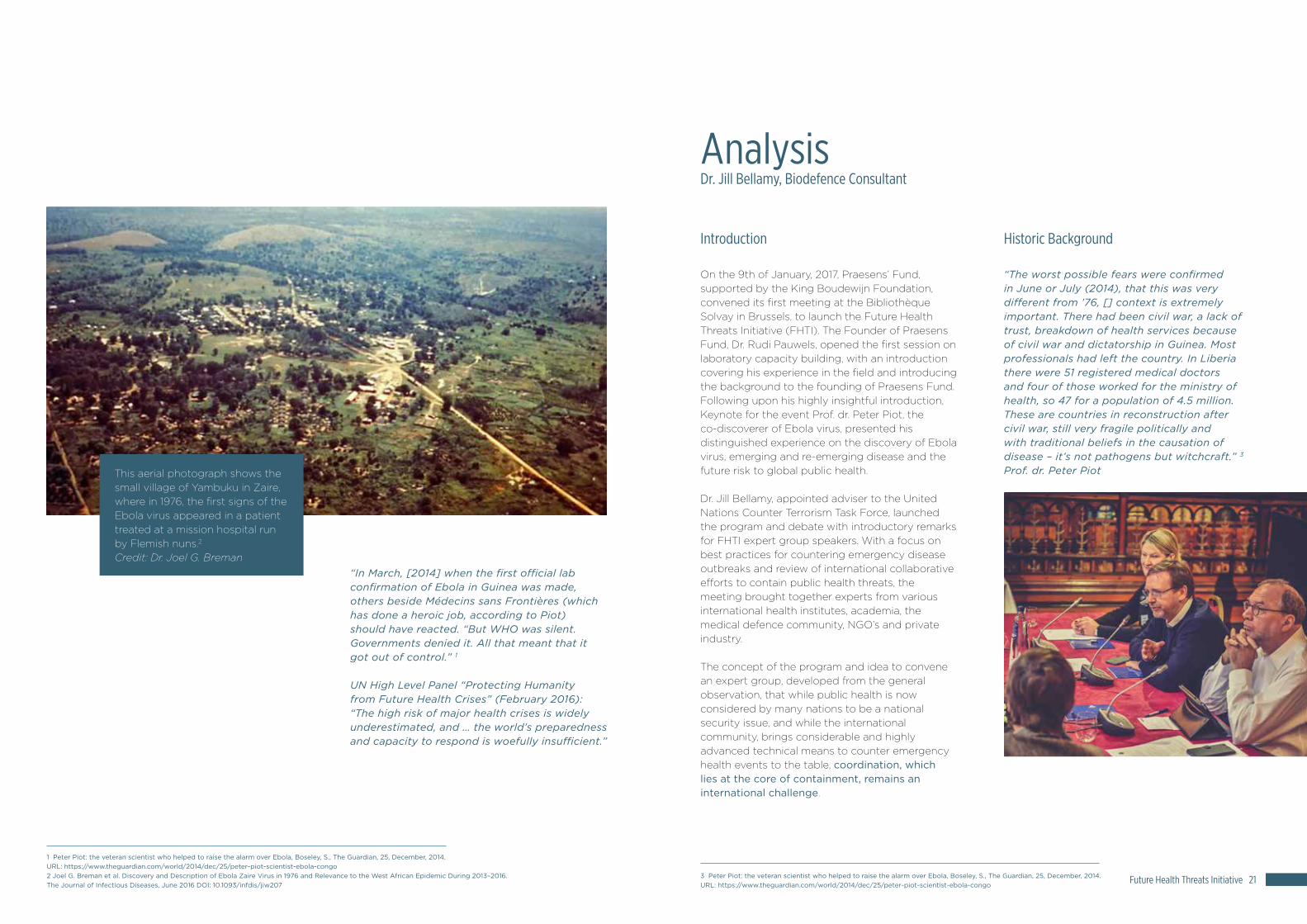
This aerial photograph shows the small village of Yambuku in Zaire, where in 1976, the first signs of the Ebola virus appeared in a patient treated at a mission hospital run by Flemish nuns.2 Credit: Dr. Joel G. Breman
Analysis Dr. Jill Bellamy, Biodefence Consultant
“In March, [2014] when the first official lab confirmation of Ebola in Guinea was made, others beside Médecins sans Frontières (which has done a heroic job, according to Piot) should have reacted. “But WHO was silent. Governments denied it. All that meant that it got out of control.” 1
UN High Level Panel “Protecting Humanity from Future Health Crises” (February 2016): “The high risk of major health crises is widely underestimated, and … the world’s preparedness and capacity to respond is woefully insufficient.”

Future Health Threats Initiative 23
Although advances in science and technology currently provide the global public health community with unprecedented capabilities to counter emerging and re-emerging infectious disease and the epidemics and pandemics these diseases often spawn; we continue to experience emergency disease outbreaks for which response is less than robust. We must consider, given our current technical capacity to effectively respond, why the international public health community continues to struggle to counter emergency disease events.
Responding to emergency disease events, whether natural or deliberate, involves a set of resources and proscribed activities, which must be in place to rapidly counter and contain such events. The primary activities involved including: preparedness, identification, containment and response, require coordination at the international level, as well as the diagnostic tools and mobile capability to address such emergencies. Gaps in coordination and lack of noted resources will likely affect the outcome of the event. In considering one of the more recent threats to global public health, the 2013-2016, Ebola virus (EBV) outbreak in West Africa, we must assess why governments, with the means to respond effectively, encountered obstacles early on.
A review of the very first outbreak of Ebola virus4, co-discovered by Prof. dr. Peter Piot, Director of the London School of Hygiene and Tropical Medicine, in Yambuku, Zaire (currently Democratic Republic of Congo), may provide answers to this critical question. In 1976, two simultaneous outbreaks (one in Nzara, South Sudan and one in Yambuku, near the Ebola River)5 of an unknown disease swept through the population in Yambuku, Zaire.
“On 28 September 1976, just prior to her death, a blood specimen was again collected from the sick nun from Yambuku by Jacques Courteille, a Belgian physician working at Ngaliema Hospital in Kinshasa. He reported that she had a 5-day febrile, hemorrhagic illness, possibly yellow fever. The sample arrived in a broken vial at the Institute of Tropical Medicine (ITM; Antwerp, Belgium) on 29 September, followed by a postmortem liver specimen a day later. These specimens were inoculated into Vero cells and analyzed by Guido van der Groen, René Delgadillo, and Peter Piot in the microbiology department directed by Stefaan Pattyn [3]; a cytopathic effect was observed. When a Marburg-like virus was observed by electron microscopist Wim Jacob, the World Health Organization (WHO; Geneva, Switzerland) was notified: the ITM team was told by Paul Brès of the WHO to send all specimens immediately to the Microbiological Research Establishment (MRE; Porton Down, United Kingdom), arriving on 5 October. Some materials were forwarded to the Centers for Disease Control and Prevention (CDC; Atlanta, Georgia), arriving on 11 October and 13 October; both laboratories had maximum containment for highly pathogenic viruses. The ITM retained some specimens in Antwerp.” 6
The Institute of Tropical Medicine in Antwerp, Belgium was the first to receive blood samples drawn from a patient who’d succumbed to the unknown illness.7 The virus appeared to resemble Marburg virus, a hemorrhagic fever virus discovered several years prior, but under observation was a novel virus. The virus was morphologically similar to Marburg virus, but immunologically distinct. It was named Ebola virus.8
Containment of this Viral Hemorrhagic Fever, would depend on rapid identification. As noted, samples were sent to the US Centre for Disease Control and Prevention in Atlanta, Georgia and to Porton Down, the UK’s premier military laboratory, both of whom had the necessary protective labo-ratories to work on highly pathogenic viruses. The ability of the teams to quickly identify a novel virus impacted its successful containment. It’s prudent to recall, at this time, no internet existed, epidemio-logical traceback was conducted with hand written notations, and barrier technology in the field was largely limited to basic protective equipment (gloves, masks, soap) and the use of quarantine.
Dr. Joel Breman of the Fogarty International Center at the National Institutes of Health, released a report highlighting lessons learned from the smaller, more quickly contained 1976 outbreak.9 He noted “We found it essential to have a group able to lead efforts overall, to organize and coordinate with others and form partnerships with community leaders. For instance, we delegated a scientist to do serology, a communications officer, a physician managing the clinical care and I was in charge of epidemiology and surveillance. For every step, it’s important to ensure transparency and to communicate extensively about what’s going on. Then you need infrastructure for the teams to carry out effective logistics, transport and identification of patients.” 10
Peter Piot’s notes in 1976: Many people were interviewed and detailed notes were taken during the investigation.
4 Ebola virus is an aggressive pathogen that causes a highly lethal hemorrhagic fever syndrome in humans and nonhuman primates. First recognized near the Ebola River valley during an outbreak in Zaire in 1976 (6, 20), outbreaks have occurred in Africa in the ensuing 27 years, with mortality rates ranging from 50 to 90% (26, 28). Outbreaks have been identified yearly for the past 3 years in central Africa, the most recent of which continues in the Republic of the Congo, with more than 125 fatalities to date according to the World Health Organization (http://www.who.int/csr/don/2003_05_07/en/, accessed 7 May 2003). The natural host for Ebola virus is unknown, so it has not been possible to implement programs to control or eliminate viral reservoirs of transmission to human populations. The rapid progression of Ebola virus infection has further complicated the control of this disease, affording little opportunity to develop acquired immunity. Nancy Sullivan, Zhi-Yong Yang, and Gary J. Nabel, Ebola Virus Pathogenesis: Implications for Vaccines and Therapies, Journal of Virology. 2003 Sep; 77(18): 9733–9737. doi: 10.1128/JVI.77.18.9733-9737.20035 Ebola Virus Disease Fact Sheet, World Health Organization, updated January, 2016. URL: http://www.who.int/mediacentre/factsheets/fs103/en/6 Joel G. Breman et al. Discovery and Description of Ebola Zaire Virus in 1976 and Relevance to the West African Epidemic During 2013–2016. The Journal of Infectious Diseases, June 2016 DOI: 10.1093/infdis/jiw207 7 Joel G. Breman et al. Discovery and Description of Ebola Zaire Virus in 1976 and Relevance to the West African Epidemic During 2013–2016. The Journal of Infectious Diseases, June 2016 DOI: 10.1093/infdis/jiw207 8 Ebola Hemorrhagic Fever Virus in Zaire,1976, Bull World Health Organ. 1978; 56(2): 271–293. URL: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2395567/
9 Joel G. Breman et al. Discovery and Description of Ebola Zaire Virus in 1976 and Relevance to the West African Epidemic During 2013–2016. The Journal of Infectious Diseases, June 2016 DOI: 10.1093/infdis/jiw20710 Fogarty International Center, “Lessons learned from 1976 Ebola outbreak: Q and A with Fogarty Scientist Emeritus Dr Joel Breman”, November / December 2014 | Volume 13, Issue 6. URL: https://www.fic.nih.gov/News/GlobalHealthMatters/november-december-2014/Pages/ebola-outbreak-1976-africa-joel-breman.aspx

Future Health Threats Initiative 25
warned the Ebola outbreak was a public health emergency and advised the following:
• The Ebola outbreak in West Africa constitutes an ‘extraordinary event’ and a public health risk to other States;
• The possible consequences of further international spread are particularly serious in view of the virulence of the virus, the intensive community and health facility transmission patterns, and the weak health systems in the currently affected and most at-risk countries;
• A coordinated international response is deemed essential to stop and reverse the international spread of Ebola. 12
Given the number of international agencies involved and existing advanced technology, the question remains: why was the international public health community not better prepared? Why after decades of modeling emergency disease outbreaks, training at the national and international public health institutional level, possessing technologies developed specifically for containing pandemic disease and the robust capacity of national reference laboratories, was the containment effort less then optimal? The answer to this can be found within evaluation of the response itself. Given the lack of public health resources in the area, poor infrastructure, delayed reporting, gaps in the structure of the response and the inability to coordinate among organizations, NGO’s, the defence sector, at an international level, combined to adversely impact the outcome of this outbreak.
“[a]lthough the laboratory processing time for PCR testing can be under 6 hours, the time between sample collection and receiving the result has often been much longer during the epidemic, owing to limited laboratory capacity and logistical infrastructure8. This has been a crucial issue, because delays in testing lead to longer hospital stays for patients, increasing both bed demand and the likelihood of nosocomial transmission (a major issue in Ebola outbreaks9). At the peak of the epidemic in Sierra Leone (between October and November 2014) there were reports of delays in test results of up to 1 week.” 13
In contrast to the previously limited outbreaks of Ebola in central Africa, what has been called the worst Ebola outbreak in history, challenged the international emergency response efforts, specifically in its ability to mount and sustain a coordinated response with adequate hospital and laboratory surge capacity. Rapid identification critically defines the difference between containment and epidemic, response and the potential for increased mortality. Identification and diagnostic capability remains a hallmark of public health security, it forms the very foundation of laboratory surge capacity. During the 2013 to 2016 outbreak that capacity was severally tested.
The ability of most clinics and existing hospitals to ramp up surge capacity was largely lacking. Where earlier outbreaks of Ebola benefited from timely identification, the scale of the 2013 outbreak seemingly caught the global health community by surprise. A concern, as advanced technology existed which could provide far more sensitive and rapid test results. Such technologies are a definitive advantage to containing epidemics. Teams working on the 2013-2016 Ebola outbreak in West Africa, unfortunately faced challenges at both the technological level as well as the coordination level, which ultimately impacted mortality rates. Given the history and lessons of previous Ebola outbreaks, the struggle to contain the West African outbreak is concerning.
The Ebola Outbreak of 2013-2016
“The unprecedented scale of the 2014–2015 West African Ebola epidemic, posed major challenges for delivering rapid diagnosis - an essential component of controlling Ebola epidemics, given the non-specific nature of early clinical symptoms.” 11
The scale of the 2013-2016, West African Ebola outbreak outstripped all previous outbreaks and largely took the international public health community by surprise. The World Health Organization issued a number of defining points, noted as inhibiting the response. In comparison to the first recorded outbreak of EBV, a number of quite basic issues arose. In August, 2014, the WHO
Abbreviations: CDC, Centers for Disease Control and Prevention; CPE, cytopathic effect; ELISA, enzyme-linked immunosorbent assay; ETUs, Ebola treatment units; IFA, immunofluorescence antibody; RT-PCR, reverse transcription–polymerase chain reaction; WHO, World Health Organization.
Event 1976 Democratic Republic of the Congo (Formerly, Zaire)
2013–2016 Guinea, Sierra Leone, Liberia
Deaths/cases, proportion (%)
280/318 (88) 11 310/28 616 (39); as of 31 March 2016
Time first case from onset to international alert
Approximately 5 wk (26 August–28 September 1976)
Guinea, >12 wk (26 December 2013–22 March 2014)
International Commission convened 18 October: approximately 8 wk
WHO emergency declared 8 August 2014: >32 wk
Local containment Hospital closed 30 September; isolation and rapid burial
Difficult; some families and communities initially uncooperative; health services overwhelmed
Quarantine imposed Effective in rural and urban settings Initially ineffective; community mutiny, rural and urban areas
Spread to urban sites Transmission chain to 2 persons in Kinshasa
Rapid spread from forest to multiple urban sites; followed transport routes
International spread None Elsewhere in Africa/Europe/United States
Incubation range; quarantine period
2–21 d; 42-d quarantine 21 d; use as maximum 42-d quarantine
Viral load and presence
CPE/qualitative-quantitative (1 laboratory, CDC)
RT-PCR, qualitative (44 laboratories in the field)
Serological IFA (rapid diagnosis in field) ELISA (delayed results)
Plasmapheresis collection and effect
Started early, uncertain effect No improvement in survival
Treated other diseases services
Yes Yes in ETUs: variable, health services overwhelmed
Sequelae Not studied Ophthalmologic, neurological, psychological; semen and eye with virus; sexual transmission
Research Limited epidemiology, virology, ecology Extensive: immunotherapy, drugs, vaccines, transmission, personal protection
Key Points Tying the 1976 Ebola Virus Outbreak to the 2013–2016 Epidemic 14
14 Joel G. Breman, David L. Heymann, Graham Lloyd, Joseph B. McCormick, Malonga Miatudila, Frederick A. Murphy, Jean-Jacques Muyembé-Tamfun, Peter Piot, Jean-François Ruppol, Pierre Sureau, Guido van der Groen, Karl M. Johnson; Discovery and Description of Ebola Zaire Virus in 1976 and Relevance to the West African Epidemic During 2013–2016. J Infect Dis 2016; 214 (suppl_3): S93-S101. doi: 10.1093/infdis/jiw207
11 Nouvellet, P., Garske, T., Mills, H. L., Nedjati-Gilani, G., Hinsley, W., Blake, I. M., … Ferguson, N. M. (2015). The role of rapid diagnostics in managing Ebola epidemics. Nature, 528(7580), S109–S116. http://doi.org/10.1038/nature1604112 Barriers to the Rapid Containment of the Ebola Outbreak, WHO, Ebola Situation Assessment, 11 August, 2014. URL: http://www.who.int/csr/disease/ebola/overview-august-2014/en/13 Pathmanathan I, et al. Rapid assessment of Ebola infection prevention and control needs — six districts, Sierra Leone, October 2014. Morb Mortal Wkly Rep. 2014;63:1172–1174.

Future Health Threats Initiative 27
Launching a massive containment effort in remote areas, often with primitive logistical infrastructure and few public health resources, demands a very specific set of approaches and assets; coordination of such assets, however, is key. During the 2013-2016 outbreak, the early responsibility of which largely fell on Médecins Sans Frontières (MSF), few resources existed in country to contain what would later be called the worst Ebola outbreak in history. Hospitals, clinics, treatment centers and units, hospital staff, laboratories and lab staff, were swiftly overwhelmed. Additionally, collecting samples in remote areas, with little or no transportation infrastructure, delayed diagnostic efforts.
By May 8, 2016, the WHO, reported a total of 28,616 suspected cases and 11,310 deaths.15 Basic issues which would not inhibit a response in states with developed public health infrastructures and robust logistical resources, became a major issue in rural areas and those states recovering from several years of civil war. The core issues effecting the 2013-2016 Ebola outbreak include (but are not limited too) the following:
• Transportation of samples was very early on, an obstacle to rapid diagnosis, which likely cost lives as suspected cases were held in triage areas with confirmed cases;
• Limited capacity to conduct rapid, sensitive, molecular diagnostics, in the field;
• Lack of trained health personnel;• Lack of laboratory surge capacity, for those in
country labs processing samples;• Local customs;• Suspicion of aid workers and hospitals
(initial lack of community outreach and crisis communication);
• Inability to develop streamline communication and disease surveillance networks;
• Inability to coordinate the response effort among numerous sectors and existing government level networks;
• Ineffective mobility to rural areas where Ebola was present.
In the 2013–2016 epidemic, 44 diagnostic laboratories working in 3 countries, used reverse transcription–polymerase chain reaction providing qualitative results.16 Critically, lack of infrastructure,
which inhibited samples being quickly received and analyzed and the type of diagnostics available, impacted the mission. Technical means were available, but logistics and critical collaboration, left a serious gap in coordination of the international response. Diagnostics play a critical role in all disease outbreaks, but none more so than those with the potential to become epidemics and pandemics. Laboratory surge capacity is highly dependent upon medical diagnostic capabilities, resources, training and the staff this requires. While the 2013 outbreak of Ebola, which swept through West Africa is historically, considered the worst outbreak to date, emerging and re-emerging infectious disease continues to pose a risk to global public health security. Unfortunately, the gaps which inhibited an early robust response, to greater and lesser degrees, still exist, even after focused international attention and significant financial investment by stakeholders to curb such shortcomings.
Laboratory Surge Capacity: The Weakest Link?
“Laboratory technicians will need to diagnose between 1,000 and 10,000 cases per day, he said. “So, you need a lot of these kits and today it is not possible to do that” in the mobile labs, even with considerable expertise.” 17 Pierre Formenty, WHO
Laboratory ‘surge capacity,’ includes the ability to deal with a rapid upsurge in demand for diagnostic analysis, such as that occurring during an epidemic, pandemic or bio-terrorist incident where mass casualties require immediate and substantial assistance. On August 11, 2014, the World Health Organization (WHO) issued an Ebola Situation Assessment.
The statement noted: “The outbreak of Ebola virus disease in West Africa continues to evolve in alarming ways, with no immediate end in sight. [ ] Many barriers stand in the way of rapid containment. The recent surge in the number of cases has stretched all capacities to the breaking point. Supplies of personal protective equipment and disinfectants are inadequate. The outbreak continues to outstrip diagnostic capacity, delaying the confirmation or exclusion of cases and impeding contact tracing. Diagnostic capacity is especially important as the early symptoms of Ebola virus disease mimic those of many other diseases commonly seen in this region, including malaria, typhoid fever, and Lassa fever.” 18
Historically, epidemics and pandemics have outstripped laboratory surge capacity in the states and regions where they occur. Often, public health emergencies are zoonotic. Laboratory surge capacity is an important aspect of controlling animal disease outbreaks which have the potential to emerge quickly and spread to human populations. With the exception of variola major (smallpox), all Center for Disease Control and Prevention, Category A listed pathogens are zoonotic. Several CDC Category B and C, as well as those listed pathogens on European and International reportable disease lists are zoonotic as well. Generally, those diseases with the ability to impact economic interests and public health are prioritized within national reporting system and OIE (World Organization for Animal Health).
15 Ebola Data and Statistics, Situation Summary, WHO, 11, May, 2016. URL: http://apps.who.int/gho/data/view.ebola-sitrep.ebola-summary-latest?lang=en16 Joel G. Breman, David L. Heymann, Graham Lloyd, Joseph B. McCormick, Malonga Miatudila, Frederick A. Murphy, Jean-Jacques Muyembé-Tamfun, Peter Piot, Jean-François Ruppol, Pierre Sureau, Guido van der Groen, Karl M. Johnson; Discovery and Description of Ebola Zaire Virus in 1976 and Relevance to the West African Epidemic During 2013–2016. J Infect Dis 2016; 214 (suppl_3): S93-S101. doi: 10.1093/infdis/jiw207
17 WHO Pushes for Rapid, Safe Ebola Diagnostic Tests, Schlein, L., VOA. 18, November, 2014. URL: http://www.voanews.com/a/who-pushes-for-rapid-safe-ebola-diagnostic-tests/2525269.html 18 Barriers to rapid containment of the Ebola outbreak, Ebola Situation Assessment, 11 August, 2014. URL: http://www.who.int/csr/disease/ebola/overview-august-2014/en/

Future Health Threats Initiative 29
While other highly infectious (in some instances non-communicable) diseases are carried by insects, the importance of identification and differentiation, at first instance, requires substantial commitment to zoonotic disease surveillance. The concept of one-health has been considered for several years and is largely accepted as the gold standard for countering the emergence and re-emergence of highly pathogenic infectious disease.
“Diagnostic laboratories are an essential component of animal disease surveillance systems. To understand the occurrence of disease in populations, surveillance systems rely on random or targeted surveys using three approaches: clinical, serological and virological surveillance.” 19 “The importance of sensitivity and specificity estimates in the design and interpretation of statistically based surveys and risk analysis is fundamental to establish appropriate disease control and prevention strategies.” 20
For over a decade major concern over avian influenza and other respiratory viruses, has witnessed significant funding from all sectors (civilian and military), across the globe. Zoonosis is a major concern with regard to public health preparedness. Should a major pandemic occur, the surge training of laboratory personnel and the diagnostics required to contain a global pandemic are simply not available. Training of personnel in technical procedures for diagnostics is both time consuming and often times not possible in a field situation. In addition to this remote outbreaks make on-site diagnostics a challenge at best. Rapid test kits, which may be useful in some instances, can lack sensitivity which then requires further testing at increased costs. Quick and reliable diagnostics for fixed and mobile laboratories is highly desirable to public health laboratories, animal disease surveillance networks, NGO’s and the military.
A number of diagnostic tests were used during the West African outbreak. To a greater or lesser degree this was useful in containing the outbreak and breaking the transmission chain, however, many of the diagnostics in the field required highly trained personnel, stable electricity sources, and temperature controlled environments. Additionally, the time required to run hundreds of tests simultaneously was simply not feasible under existing conditions. Delays, which initially ran into several days, undoubtedly increase transmission rates within Ebola Treatment Centers and Units. Lack of coordination among responding sectors and a lack of surge capacity, initially added a considerable burden to the overall effort to contain Ebola.
Future epidemics and pandemics will require a far more agile, coordinated and streamlined response. Assets which provide such advantages, must be rapidly deployed and remain until the public health emergency is contained. Coordinating these efforts and these assets is a priority for all public health security stakeholders. Ultimately, increasing laboratory surge capacity by developing those tools and assets which remain in country and contribute to strengthening the public health infrastructure in country, will benefit global public health security. Addressing disease surveillance in a more comprehensive ‘one health’ approach will increase our ability to swiftly and successfully respond in future emergency disease situations.
19 Zepeda, C., The role of diagnostic laboratories in support of animal disease surveillance systems (abstract), Dev Biol (Basel). 2007;128:139-43.Pubmed, NCBI. URL: https://www.ncbi.nlm.nih.gov/pubmed/1808493920 Zepeda, C., The role of diagnostic laboratories in support of animal disease surveillance systems (abstract), Dev Biol (Basel). 2007;128:139-43.Pubmed, NCBI. URL: https://www.ncbi.nlm.nih.gov/pubmed/18084939

Future Health Threats Initiative 31

Future Health Threats Initiative 33
Emerging infectious disease: the threat of large scale public transmission
“A recent study led by the University of Cambridge identified 20 known infectious diseases that have re-emerged or spread geographically, including dengue, chikungunya, typhoid, West Nile, artemisinin-resistant malaria and the plague. 5 Other known threats – such as influenza (i.e. H1N1 Swine Flu), MERS-CoV, and Ebola – continue to raise fears, especially when they take hold in densely populated areas and when treatment and prevention measures are not necessarily available. Even when known infectious diseases can be mitigated by existing treatments or vaccines, we face the risk of emerging resistant strains, mutating viruses, or a pandemic that is so large it renders response supplies inadequate.” 21
Emerging infectious diseases (EID), pose significant public health security risks. These risks may be amplified given a variety of factors, which include, urbanization, modern air travel, mass gathering events (i.e. the Olympics and the Hajj), dense industrial animal husbandry, inadequate public health infrastructure and low or absent herd immunity. Each of these factors may contribute toward increasing the likelihood an emerging infectious disease will go global.
In 2012, Middle East Respiratory Syndrome coronavirus (MERS-CoV) was newly identified in a Saudi Arabian patient.22 The second time (after severe acute respiratory syndrome coronavirus, SARS-CoV), in the Twenty First century, that a coronavirus emerged as a new lethal zoonotic pathogen in humans.23 From April 2012 and as of 15 July 2016, 1,782 cases of MERS-CoV, including 680 deaths, have been reported by 27 countries worldwide.24 Most of the cases have been reported from Middle East; Saudi Arabia (1105 cases & 479 deaths), United Arab Emirates, Qatar, Jordan,
Oman, Kuwait, Egypt, Yemen, Lebanon, South Korea, Philippines, Thailand and Iran.25 ”So far, cases of MERS-CoV have been linked through travel to or residence in countries in and near the Arabian Peninsula.”26 The capabilities required for prevention, in the first instance, require establishing a rapid diagnostic capacity which can be easily and swiftly deployed. In addition to ease of use, the ability to process hundreds of samples a day during an outbreak is an essential component of response. To date, resources which would allow for such a deployment are largely lacking in regions which could best utilize and benefit from this technology.
“Infectious diseases, which are among the leading causes of death worldwide, do not confine themselves to national borders. Their capacity to spread rapidly across geographies – jeopardizing social and economic security as well as challenging human health and well-being – is amplified by ever-growing globalization, increased trade and travel, the rise in urbanization, and changes in the environment, behaviour and society. Some threats, such as influenza, are known. Others are not. Unknown just a few decades ago, HIV/AIDS has killed more than 30 million people from all socio-economic backgrounds. What might be the next HIV/AIDS, and are we sufficiently prepared for its arrival?” 27
One of the main lessons learned from nearly all transmissible diseases outbreaks is that disease does not discriminate and does not recognize national boundaries. In the case of SARS-CoV, an outbreak in 2003 affected twenty-six nations, resulting in more than 8,000 cases. Although most cases of human to human transmission occurred in a hospital setting, the absence of adequate infectious disease control practices likely lead to an increase in transmission.
As zoonotic transboundary diseases28 pose an ever-greater threat to global public health security, increasingly the need to develop both sentinel and passive monitoring of such zoonotic and epizonotic diseases is becoming a crucial factor in preventing pandemics. In the case of MERS-CoV, the main reservoir is dromedary camels. Results of a study, published in a paper which appeared in Science entitled: “Co-circulation of three camel coronavirus species and recombination of MERS-CoVs in Saudi Arabia,” identified MERS-CoV species and a human CoV 229E related lineage co-circulating at high prevalence, with frequent co-infections in the upper respiratory tract of dromedary camels.29 Given concerns over human to human transmission and transmission in hospital setting, such as occurred in the 2015 outbreak of MERS-CoV in South Korea, the risk of MERS-CoV transmission in mass gatherings and concerns over future epidemics is well justified.
“The annual Hajj in the Kingdom of Saudi Arabia is the largest recurring single mass gathering in the world. Every year more than 10 million pilgrims attend the annual Hajj and Umrah. Attendees assemble in confined areas for several days. People with a wide range of age, health, susceptibility to illness, and hygiene sophistication come in close contact, creating an enormous public health challenge. Controlling respiratory infections at the Hajj requires surveillance, rapid diagnostic testing, and containment strategies. Although the Hajj is without equal, other mass gatherings can generate similar hazards. The geographic colocalization of the Zika virus epidemic and the 2016 Summer Olympic Games in Brazil is a current example of great concern. The potential of international mass gatherings for local and global calamity calls for greater global attention and research.”30
21 “Global Disease Outbreaks”, World Economic Forum, Global Risks Report, 2016. URL: http://reports.weforum.org/global-risks-2016/global-disease-outbreaks/22 Alimuddin Zumla, Abdulaziz N. Alagaili, Matthew Cotten and Esam I. Azhar, “Infectious diseases epidemic threats and mass gatherings: refocusing global attention on the continuing spread of the Middle East Respiratory syndrome coronavirus (MERS-CoV)”, BMC Medicine, 201614:132 DOI: 10.1186/s12916-016-0686-3 23 Alimuddin Zumla, Abdulaziz N. Alagaili, Matthew Cotten and Esam I. Azhar, “Infectious diseases epidemic threats and mass gatherings: refocusing global attention on the continuing spread of the Middle East Respiratory syndrome coronavirus (MERS-CoV)”, BMC Medicine, 201614:132 DOI: 10.1186/s12916-016-0686-3 24 Alimuddin Zumla, Abdulaziz N. Alagaili, Matthew Cotten and Esam I. Azhar, “Infectious diseases epidemic threats and mass gatherings: refocusing global attention on the continuing spread of the Middle East Respiratory syndrome coronavirus (MERS-CoV)”, BMC Medicine, 201614:132 DOI: 10.1186/s12916-016-0686-3 25 Alimuddin Zumla, Abdulaziz N. Alagaili, Matthew Cotten and Esam I. Azhar, “Infectious diseases epidemic threats and mass gatherings: refocusing global attention on the continuing spread of the Middle East Respiratory syndrome coronavirus (MERS-CoV)”, BMC Medicine, 201614:132 DOI: 10.1186/s12916-016-0686-3 26 Advisory on the Prevention and Control of Middle East Respiratory Syndrome Corona Virus (MERS-CoV) during upcoming Umrah & Haj, National Institute of Health, Islamabad Ministry of National Health Services, Regulation and Coordination, July, 2016. URL: http://www.nih.org.pk/files/Newsletter/Advisory%20on%20MERS-CoV%20during%20upcoming%20Umrah%20Hajj%202016.pdf27 “Global Disease Outbreaks”, World Economic Forum, Global Risks Report, 2016. URL: http://reports.weforum.org/global-risks-2016/global-disease-outbreaks/
28 Transboundary animal diseases are highly contagious epidemic diseases that can spread extremely rapidly, irrespective of national borders. They cause high rates of death and disease in animals, thereby having serious socio-economic and sometimes public health consequences while constituting a constant threat to the livelihoods of livestock farmers. Globalization, land encroachment and climate change contribute to outbreaks of such animal diseases – some transmissible to humans – as brucellosis, bovine tuberculosis, parasitic illnesses, anthrax, bovine spongiform encephalopathy (BSE) and certain strains of influenza viruses. High-impact animal diseases such as foot-and-mouth disease, peste des petits ruminants, classical or African swine fevers, while not directly affecting human health, do affect food and nutrition security and livestock production and trade. Transboundary Animal Diseases, FAO in Emergencies. URL: http://www.fao.org/emergencies/emergency-types/transboundary-animal-diseases/en/29 Jamal S. M. Sabir, Tommy T.-Y. Lam, Mohamed M. M. Ahmed, Lifeng Li, Yongyi Shen, Salah E. M. Abo-Aba, Muhammad I. Qureshi, Mohamed Abu-Zeid, Yu Zhang, Mohammad A. Khiyami, Njud S. Alharbi Nahid H. Hajrah Meshaal J. Sabir, Mohammed H. Z. Mutwakil, Saleh A. Kabli, Faten A. S.Alsulaimany, Abdullah Y. Obaid, Boping Zhou, David K. Smith4, Edward C. Holmes, Huachen Zhu, Yi Guan, “Co-circulation of three camel coronavirus species and recombination of MERS-CoVs in Saudi Arabia”, Science 17 Dec 2015:DOI: 10.1126/science.aac860830 Jaffar, A. Tawfiq, Philippe Gautret, Samir Benkouiten, Ziad A. Memish, Mass Gatherings and the Spread of Respiratory Infections. Lessons from the Hajj. Annals of the American Thoracic Society 13:11, 2106-2106. 10, November, 2016. DOI: http://dx.doi.org/10.1513/AnnalsATS.201511-772FR
Mass gatherings, ports of entry, as well as major transportation hubs, such as airports and train stations, could well be vectors of transmission beyond borders; it’s often the pace (of disease transmission), not the space (region or geographic zone), that counts in containing highly infectious and communicable disease. Early identification is critical to containment and ultimately one of the clear factors between stopping an epidemic before it becomes a pandemic. Emerging diseases often occur in geographically remote locations or locations which witness a sudden upsurge in population density. Preparedness, coordination and the ability to rapidly upscale technology platforms will likely determine the outcome.
Emerging diseases often occur in geographically remote locations or locations which witness a sudden upsurge in population density. Preparedness, coordination and the ability to rapidly upscale technology platforms will likely determine the outcome.

Future Health Threats Initiative 35
Epidemic intelligence platforms: a critical link in outbreak surveillance
“Of the 46 countries in the World Health Organization (WHO) African region (AFRO), 43 are implementing Integrated Disease Surveillance and Response (IDSR) guidelines to improve their abilities to detect, confirm, and respond to high-priority communicable and noncommunicable diseases. IDSR provides a framework for strengthening the surveillance, response, and laboratory core capacities required by the revised International Health Regulations [IHR (2005)]. In turn, IHR obligations can serve as a driving force to sustain national commitments to IDSR strategies. The ability to report potential public health events of international concern according to IHR (2005) relies on early warning systems founded in national surveillance capacities.” 31
During an emergency disease outbreak, the vital role of disease surveillance, diagnostics and connectivity cannot be overstated. Several international disease surveillance networks exist. In addition to human disease surveillance, as mentioned above, it is critical we consider animal disease surveillance networks, as zoonosis is a major concern in current and future pandemic planning.
“The majority of avian outbreaks in Southeast Asia have been attributed to the movement of poultry and poultry products (Chen et al., 2006; Rosenthal, 2006). Similarly, international trade and travel will play a major role in transmission in human outbreaks, and frequent and widespread travel will make it difficult to contain any pandemic in humans. Even if trade and travel are severely restricted in order to limit human transmission, migratory birds will likely spread the disease by infecting birds on other continents (Normile, 2006).” 32
The threat posed by a highly infectious disease outbreak, capable of developing into a pandemic, haunts the international public health community; in fact, it has done so for centuries. Smallpox, the Spanish Flu, Ebola, SARS-CoV, HIV, MERS-CoV, all hold a place of considerable historic reference among public health specialists. Preparedness and response are currently less impeded by technical hurdles, but more strongly related to gaps in capacity, infrastructure and coordination.
A multitude of international health organizations, NGO’s and institutes exist to monitor emerging and re-emerging disease outbreaks and coordinate preparedness for potential epidemics and pandemics. The major public health organizations and intuitions involved in surveillance include: The World Health Organization (Global Outbreak and Response Network, GOARN), US Centers for Disease Control and Prevention, the UK Public Health Laboratory Service, the French Pasteur Institutes, the European Union, the United States Task Force on Emerging Communicable Diseases the global network of schools of public health and the Training in Epidemiology and Public Health Intervention Network (TEPHINET). 33
Most of these sites are or will become part of the WHO Collaborating Centre network. This network, along with the WHO Regional Offices, WHO country representatives and other WHO and UNAIDS reporting sites, contributes to global surveillance along with reporting networks of other United Nations agencies such as UNHCR and UNICEF. 34
31 Kasolo, F., Yoti, Z., Bakyaita, N., Gaturuku, P., Katz, R., Fischer, J. E., & Perry, H. N. (2013). IDSR as a Platform for Implementing IHR in African Countries. Biosecurity and Bioterrorism: Biodefense Strategy, Practice, and Science, 11(3), 163–169. http://doi.org/10.1089/bsp.2013.003232 Gostin, Lawrence, O., J.D., and Benjamin E. Burkman, J.D., M.P.H., Preparing for Pandemic Influenza: Legal and Ethical Challenges, National Center for Biotechnology Information, National Academies Press, 2007. URL: https://www.ncbi.nlm.nih.gov/books/NBK54163/33 World Health Organization, Global Infectious Disease Surveillance, Fact sheet No. 200. URL: http://www.who.int/mediacentre/factsheets/fs200/en/34 World Health Organization, Global Infectious Disease Surveillance, Fact sheet No. 200. URL: http://www.who.int/mediacentre/factsheets/fs200/en/
African Field Epidemiology Network
Agence régionale de santé, Pays de la Loire, France
Agence régionale de santé, Rhône-Alpes, France
Agence régionale de santé, Île-de-France, France
Association pour le développement de l’épidémiologie de terrain
Australasian College for Infection Prevention and Control
Australian Response ARM Network
Bernhard Nocht Institute for Tropical Medicine
Bundeswehr Institute of Microbiology
Burnet Institute for Medical Research and Public Health
Caribbean Public Health Agency
Center for Disease Control, Iran
Center for Infection and Immunity, Mailman School of Public Health of Columbia University
Centers for Disease Control and Prevention, USA
Centre de Coopération Internationale en Recherche Agronomique pour le développement
Centre International de Recherches Médicales de Franceville
Chinese Center for Disease Control and Prevention, China
Communicable Disease Control Directorat, Western Australia
Croatian National Institute of Public Health
Department of Public Health, Osaka City University Faculty of Medicine, Japan
Department of Tropical Medicine, Tulane School of Public Health and Tropical Medicine
Department of Virology, Tohoku University, School of Medicine
Division of Tuberculosis and Infectious Disease Control, Ministry of Health, Labour and Welfare
Eastern Mediterranean Public Health Network
École des hautes études en santé publique
Epicentre research and epidemiology
European Programme for Intervention Epidemiology Training, Alumni Network
Etablissement de Préparation et de Réponse aux Urgences Sanitaires
European Centre for Disease Prevention and Control
European Mobile Laboratory Consortium
European Network for Diagnostics of Imported Viral Diseases, Robert Koch Institute
European Programme for Intervention Epidemiology Training
European Virus Archive
Faculty of Health Sciences, Curtin University of Technology
Federal Ministry of Health, Sudan
Federal Public Service, Health, Food Chain Safety and Environment
Field Epidemiology Training Program, Malaysia
Field Epidemiology Training Program, Mongolia
Field Epidemiology Training Program, Egypt
French Health Agency for the Indian Ocean
German Armed Forces Medical Service, Ministry of Defence
Health Protection Surveillance Centre
Hokkaido University Research Center for Zoonosis Control, Japan
Institut de Santé Publique d’Épidémiologie et de Développement
Institut de Veille Sanitaire
Institut Pasteur, Lyon, France
Institut Pasteur, Dakar, Senegal
Institut Pasteur International
Institute of Microbiology and Immunology, Faculty of Medicine, University of Ljubljana
Institute of Tropical Medicine
Institute of Tropical Medicine, Nagasaki University
Instituto de Salud Carlos III
Instituto Nacional de Enfermedades Virales Humanas
International Epidemiological Association
International Federation of Red Cross and Red Crescent Societies
International Medical Center of Japan
IS Global, Barcelona
Korea Centres for Disease Control and Prevention
Laboratory Inserm Jean Merieux
London School of Hygiene and Tropical Medicine, UK
Médecins Sans Frontières, Belgium
Médecins Sans Frontières, France
Médecins Sans Frontières
Médecins Sans Frontières, Spain
Medecins Sans Frontieres, Switzerland
Ministry of Public Health, Lebanon
Ministry of Health, Brazil
MRC Centre for Outbreak Analysis and Modelling, Imperial College London
Museum national d histoire naturelle
National Center for Epidemiological Surveillance and Disease Control, Ministry of Health
National Center for Global Health and Medicine, Japan
National Centre for Epidemiology and Population Health, Australian National University
National Institute for Communicable Diseases, South Africa
National Institute for Infectious Diseases Lazzaro Spallanzani
National Institute of Infectious Diseases
National University of Singapore
Norwegian Institute of Public Health
New South Wwales Ministry of Health
Office of Health Protection, Department of Health and Ageing, DOHA
Ontario Medical Association
Ontario Ministry of Health
Osaka University
Pasteur Institute of Iran
PathWest Laboratory Medicine
Public Health Agency of Canada
Public Health England
Robert Koch Institut
Royal Perth Hospital
Ryerson University
Save the Children International
School of Public Health and Community Medicine, University of New South Wales
Shizuoka Cancer Center Hospital
Spiez Laboratory, Federal Office for Civil Protection
Statens Serum Institut
Tan Tock Seng Hospital
The International Rescue Committee
The University of the West Indies
Training Programmes in Epidemiology and Public Health Interventions Network
U.S. Army Medical Research Institute of Infectious Diseases
United Nations Childrens Fund
United Nations Food and Agriculture Organization
United Nations High Commission for Refugees
University Hospital Düsseldorf
University Hospital Limerick
University Hospital of Heidelberg
University Hospital of South Manchester
University of Geneva
University of Nebraska Medical Center
University of Texas Medical Branch
United Nations Office for Project Services
Vancouver Coastal Health
WHO Emerging and Dangerous Pathogens Laboratory Network
WHO Global Infection Prevention and Control Network
WHO Virtual Interdisciplinary Advisory Group on Mass Gathering
World Organisation for Animal Health
GOARN partners responding to the Ebola outbreak 2014-2015 35
35 World Health Organization, Partners: Global Outbreak Alert and Response Network (GOARN), Emergency preparedness, response. URL: http://www.who.int/csr/disease/ebola/partners/en/

Future Health Threats Initiative 37
International military medical networks, such as the United States Department of Defense Global Emerging Infections System (DoD-GEIS), NATO’s Deployment Health Surveillance Capability (DHSC), developed by the French Army and code named, ASTER is an outbreak reporting system utilized by all NATO Member States, private clinics, individual scientists and public health practitioners complete the network of formal information sources.36 While disease surveillance networks are extensive, coordination among the various stakeholders and real time data analysis has proven challenging.
Advanced, highly integrated, epidemiology data analysis technology, which will enable government or private sector stakeholders to monitor outbreaks in real-time with a substantial traceback capability is currently under development. Using smart phones and tablets, this technology can be utilized to create a war room for monitoring in real time outbreaks of disease. Moreover, it is designed to enable users in report in resource poor areas in order to build and maintain a data profile for identifying hotspots. Such a network could be utilized to provide nations with real time data sets in country, allowing ownership of data and provide a platform for greater coordination among the established global health institutes and surveillance programs, which currently exist.
Future pandemic preparedness planning must certainly incorporate a range of technologies and support a more highly integrated response network. Emerging and disruptive technologies37 have the ability to change how we respond to emergency disease. Future outbreaks will likely require such technologies be utilized in the field. Often, such technologies are developed by government or defence industry sectors, with the goal of providing support to civil-military operations which may fall outside traditional missions. Government and defence sector investment in disruptive technologies has a lengthy history. One example of government funding and investment is the United States Burr Bill I and II, which eventually lead to ‘Bioshield’ legislation, following the US anthrax attacks. This committed government investment
in technologies, often deemed risky by traditional corporations and guaranteed procurement. This type of public-private investment is the future of technology enterprises which will develop assets for countering major outbreaks of disease.
Civil defence and civil protection While the Additional Protocol I to the Geneva Conventions of 1949 (AP I) lists the tasks that define “Civil Defence”. There is no internationally agreed definition of civil defence or civil protection actors in terms of how they operate, what is their mandate or nature of the relationship with military or security forces of their countries. While in some countries and regions, these terms may have developed distinct meanings; these terms are sometimes used interchangeably. This lack of clarity is reflected in the Additional Protocol 1 itself and is replicated in the interagency guidance on civil-military coordination. While the English version of the AP I and the Oslo Guidelines refer to “military and civil defence assets” and defines for the purpose of the guidance civil defence as “any organization that, under the control of a Government perform the functions enumerated in paragraph 61 of Additional Protocol 1 to the Geneva Conventions of 1949…,” the French language versions of the AP I and Oslo Guidelines use the term “protection civile” in the place of “civil defence” throughout. In the absence of any clear and internationally agreed definition it is critical to recognize that civil defence and civil protection actors are deployed in support of an agenda of the government to which they belong. The way in which humanitarian actors coordinate with civil defence and civil protection actors in a specific setting, depends on the specific nature of the civil defence and civil protection actors in that setting. It may be appropriate to include some of these actors in the humanitarian coordination mechanism itself, while in others the approach to coordination may more closely resemble the approach to coordination with military actors. In light of this lack of clarity, this paper will employ the phrase “civil defence and civil protection” throughout. 38
36 World Health Organization, Global Infectious Disease Surveillance, Fact sheet No. 200. URL: http://www.who.int/mediacentre/factsheets/fs200/en/ 37 A “disruptive technology” is one that displaces an established technology and shakes up the industry, or a ground-breaking product that creates a completely new industry. “According to Harvard Business School Professor, Clayton M. Christianson, large companies work with sustaining technologies. He states, [] its not unusual for a big corporation to dismiss the value of a disruptive technology because it does not reinforce current corporate goals, only to be blindsided as the technology matures, gains a larger audience and market share and threatens the status quo.” Whatis.techtarget.com/definition/disruptive-technology38 Global Health Cluster - Position Paper Civil-military coordination during humanitarian health action 2 Provisional version – February 2011. URL: http://www.who.int/hac/global_health_cluster/about/policy_strategy/ghc_position_paper_civil_military_coord_2_feb2011.pdf

Future Health Threats Initiative 39
Civil Military Collaboration in Natural and Deliberate Disease Containment
“Six months into the worst Ebola epidemic in history, the world is losing the battle to contain it,” said Dr. Liu. “Leaders are failing to come to grips with this transnational threat. The WHO announcement on August 8 that epidemic constituted a ‘public health emergency of international concern’ has not led to decisive action, and states have essentially joined a global coalition of inaction,” she said.
Many countries possess biological threat response mechanisms. They can deploy trained civilian or military medical teams in a matter of days, in an organized fashion, and with a chain of command to assure high standards of safety and efficiency to support the affected countries.39
The role of civil-military collaboration to counter public health threats has changed over the past decade. Traditionally, military involvement in health and or humanitarian disasters has been considered a “last resort” type of collaboration by both the defence community as well as NGO’s. As many nations now consider public health security an aspect of their national security posture, such collaboration is occurring with more frequency. It should however be noted the defence community traditionally perceived involvement with humanitarian and public health security issues, as possibly diverting its primary mission. The NGO community has been equally hesitant and perhaps for good reason, as health security is a privacy concern, not only for individuals but the state as well.
“This issue crystallizes many of the concerns of the national security community, including potentially weakening the traditional military agenda by widening the spectrum of security threats, removing the discussion of policy issues from the biomedical and public health practitioners and placing it in the hands of the diplomats, the military and possibly even the intelligence community, and focusing attention on the needs of the economically and militarily stronger countries and not on global health.” 40
During the 2013-2016 West African Ebola outbreak, military participation, primarily involved logistic assets and was deemed necessary to bring the epidemic under control. Unconventional public health threats, with a conventional security profile, such as the US anthrax attack in 2001, involved military and security assets primarily for investigation and forensic analysis. However, this spawned significant government investment in what would be considered civil-military stockpiles and medical assets. These medical assets, while an essential part of force health protection, can be designated for civilian/humanitarian aid and relief, with specific regard to natural disasters and disease outbreak. The role of the military in humanitarian relief and civil-military collaboration remains a sensitive issue.
Historic outbreaks of infectious and communicable disease, such as the 1972 outbreak of variola major (smallpox) in Yugoslavia, involved the military in a nationwide quarantine. Sensitivities and concerns related to the role of the military in securing public health remains contentious. It’s likely future pandemics may well require increased cooperation between the civilian and military medical communities. Many times, the military has the resources and logistical expertise to reduce the burden on the civilian sector during emergency health related events.
NATO, as well as all European Union Member State national defence structures, has a medical command, primarily tasked with force health protection. NATO’s resources, extensive training and ability to rapidly deploy, bring considerable assets to an emergency disease event. In the event of an unconventional deliberate release of a highly infectious and or communicable disease, the military is likely to be called upon for their considerable expertise in decontamination and forensics. It is to the benefit of both civilian and defence communities to coordinate efforts should a mass casualty emergency or major pandemic occur. Since 2011, NATO (COMEDS) has run Vigorous Warrior, a bi-annual exercise, solely for medical military personnel.
While the role of the military in civilian and humanitarian health emergencies may augment available resources, a report by the Global Health Cluster, led by WHO, noted the following key points:
• There is a marked difference in the requirements for civil-military coordination of responses to natural disasters that occur in a peaceful environment and those that occur in the midst of complex emergencies.
• Humanitarian actions should be guided by humanitarian principles and a proper assessment of the impact and evolution of the crisis and the corresponding needs of the population.
• Humanitarian actions should not be used to advance security and/or political agendas.
• In complex emergencies, military forces and humanitarian actors have different agendas, strategies, tactics, mandates and accountability frameworks.
• Internationally deployed military forces involved in peace operations or disaster response should provide direct or indirect health assistance to civilians only as a last resort, i.e. in the absence of any comparable civilian alternative and to meet the critical needs of the affected population.
• Health services provided by military actors must be in line with the assessed needs of the affected population.
• All actors – civilian and military – involved in the provision of health services should follow the national government’s health priorities and plans. In complex emergencies, national health plans must be complemented by health information from areas that may not be under the control of the government, as well as by work plans prepared by the international humanitarian community.
• Humanitarians must constantly review the evolution of the crisis and, when necessary, adapt civil-military coordination modalities to emerging conflict dynamics and new roles played by the military.
• Maintaining humanitarian identity is paramount. Humanitarian actors should be aware of the perceptions of stakeholders and how different degrees of civil-military coordination may change local perceptions of their impartiality.41
While civil military operations to contain disease, and support public health security will likely remain a controversial issue, support for joint training in preparation for future collaboration, would serve to ensure preparedness, particularly among multi-national forces and the civilian sector.
39 Global Bio-disaster Response Urgently Needed in Ebola Fight, Medecins sans Frontieres, 2, September, 2014. URL: http://www.doctorswithoutborders.org/news-stories/press-release/global-bio-disaster-response-urgently-needed-ebola-fight40 National Security and Public Health—Why the Controversy?” OECD Insights, 23, July, 2010. URL: http://oecdinsights.org/2010/07/23/national-security-and-public-health-why-the-controversy/
41 The Global Health Cluster, under the leadership of the World Health Organization, is made up of more than 30 international humanitarian health organizations that have been working together over the past four years to build partnerships and mutual understanding and to develop common approaches to humanitarian health action. Global Health Cluster - Position Paper Civil-military coordination during humanitarian health action 2 Provisional version – February 2011. URL: http://www.who.int/hac/global_health_cluster/about/policy_strategy/ghc_position_paper_civil_military_coord_2_feb2011.pdf

Future Health Threats Initiative 41
Conclusion
“In terms of sheer drama, the emergence of the severe acute respiratory syndrome (SARS) rivaled the most exotic Michael Crichton thriller. A novel viral strain spread in “wet markets” from an obscure animal to food handlers; through a rural province in southern China; to Hong Kong, by way of an ill Chinese physician who had traveled to attend a wedding; and in one night at a Hong Kong hotel, from that man to at least 12 other people. These 12 returned to their five home countries and created multiple chains of transmission that, over the course of the next four months, led to more than 8000 cases of SARS, resulting in almost 800 deaths in 27 countries, representing every continent.” 42
Emerging and re-emerging diseases, be this, Zika, Yellow Fever, Ebola, Malaria, Dengue, will continue to outpace the global public health community, until that time when coordination and the investment in research and technologies to counter pandemics is considered both a national and international priority. Community level response, international level coordination and disruptive technologies form the critical assets of mounting a successful response.
Médecins Sans Frontières, who made an outstanding contribution, sounded the alarm over Ebola very early on. Unfortunately, even though several international public health organizations have participated in previous outbreaks (HIV, SARS, VHF’s, Avian Influenza), this alarm largely fell on deaf ears. Beyond lessons learned, the public health community and military medical community must develop a framework for streamlined collaboration and engagement before emergency disease outbreaks burn through communities. Creating such a framework, will augment current assets in much the same way vaccinating a society against infectious disease creates herd immunity. Planning, preparedness and cooperation on all levels of public health, including national institutes, reference laboratories (including veterinary) and international health organizations is essential to our ability to prepare for future pandemics. A concept that has gained momentum over the past few years as a global strategy for expanding collaborations in all sectors of health care (animals, humans and the environment) is that of “One Health.”43 Within this concept national and regional health sectors prioritize surveillance systems and enhance diagnostics regarding emerging pathogens.
“Highly pathogenic influenza A (H5N1) has captured the close attention of policy makers who regard pandemic influenza as a national security threat. The virus is endemic in bird populations in Southeast Asia, with serious outbreaks also having now occurred in Africa, Europe, and the Middle East (WHO, 2006a, 2007a). Modeling4suggests that the infection will eventually affect the entire globe through transmission mechanisms involving both birds and humans (Longini et al., 2005). 44
42 Weinstein, Robert, A., Planning for Epidemics: The Lessons of SARS, n engl j med 350;23, 3, June, 2004. URL: http://www.mintie.com/assets/img/education/Planning%20for%20Epidemics%20-%20the%20lessons%20of%20SARS.pdf43 Giulia Rabozzi, Luigi Bonizzi, Eleonora Crespi, Chiara Somaruga, Maryam Sokooti, Ramin Tabibi, Francesca Vellere, Gabri Brambilla, Claudio Colosio, Emerging Zoonosis: The “One Health Approach”, Saf Health Work. 2012 Mar; 3(1): 77–83. Published online 2012 Mar 8. doi: 10.5491/SHAW.2012.3.1.77 PMCID: PMC343092544 Gostin, Lawrence, O., J.D., and Benjamin E. Burkman, J.D., M.P.H., Preparing for Pandemic Influenza: Legal and Ethical Challenges, National Center for Biotechnology Information, National Academies Press, 2007. URL: https://www.ncbi.nlm.nih.gov/books/NBK54163/
A scientist separates blood from plasma cells to isolate
any Ebola RNA to test for the virus at the European
Mobile Laboratory in Gueckedou, Guinea.45
Developing sustainable public health infrastructures in nations with few resources is critical to global public health security. Ensuring these nations have the resources in country to fight the next outbreak is a vital component of preparedness. Ensuring we can rapidly respond, with appropriate technology is critical to outcome success.
As worrying as the history of Ebola and other infectious disease (HIV, SARS, Malaria, Dengue etc.) has been, experts warn far worse pandemics lay ahead and the international community may be unprepared for the scale of such public health emergencies. Clearly coordinating our efforts to prepare for humanitarian and potential national security crisis, must be placed higher on the agenda of global stakeholders.
45 Schlein, Lisa, “WHO Pushes for Rapid, Safe Ebola Diagnostic Tests”,18, Nov. 2014, VOA Science and Health, 18, Nov. 2014. URL: http://www.voanews.com/a/who-pushes-for-rapid-safe-ebola-diagnostic-tests/2525269.html

Future Health Threats Initiative 43
“The international community must not miss the chance to bolster that response capability. One thing is for sure – we will have other epidemics. Certainly, pandemic flu is going to come at some time.” 45
Peter Piot
Beyond the advanced technology currently available to contain highly pathogenic outbreaks of disease, one of the primary factors impacting a successful response is coordination and collaboration between global public and private health partners. It is hoped the Future Health Threats Initiative will be a first step in supporting public-private health coordination to prepare for future health threats. As FHTI consolidates its Expert Working Group, core considerations of the group will include:
• Exchanging best practices for coordinating the response;
• Contributing to the development of a sustainable public health infrastructure in resource poor countries
• Acquiring advanced laboratory technology;• Establishing robust integrated disease
surveillance systems;
The Future Health Threats Initiative looks forward to a productive year and intends to hold quarterly meetings to review progress and promote collaboration among international public health institutions, private organizations, NGO’s as well as the military medical community.
Future Health Threats Initiative Working Group

Future Health Threats Initiative 45
The Future Health Threats Initiative brought together international experts in infectious disease, policy and decision makers and the members of the defence community to share their experience in emergency disease containment. Core points of speaker’s main observations with regard to preparing for emergency disease outbreaks and laboratory surge capacity, included the following:
• Overall working conditions in the field in resource-limited settings make good clinical practices difficult to achieve (e.g. tent set-ups, electricity cuts, hot and humid climate, unhygienic)
• Healthcare workers are under pressure to release rapid and accurate results
• Short turnaround time for diagnosis is critical to containment: long waiting times for diagnosis at ETC increased the likelihood that transmission between non-EVD infected patents and those with EVD would occur
• Siloed response to outbreaks, very slow funding mechanisms
• Lack of coordination of efforts, competing priorities
• Lack of standard operating procedures• Inequality in healthcare systems• Poor prediction capabilities• Regional surveillance effort was rejected because
it was regional and ‘only’ a pilot program, which is a lost opportunity
• The lack of field-applicable technologies that counter the technical challenges (e.g. sample preparation), their current availability is limited
• The 2014 Ebola outbreak made medicines available to resource-limited settings and very solid scientific clinical research was conducted: vaccines and treatments trials, established a new model for research in preparation for the next pandemic
Summary of Speaker Discussions

Future Health Threats Initiative 47
Cross-sectoral Collaboration
• Build upon collective experience and know- how from 2013-2016 Ebola outbreak to ensure we respond faster and more effectively to next epidemic or pandemic;
• Understand the value of public-private partnerships
• Understand the significant role for the private sector at both an international and local level;
• Consider strengthening civil-military collaboration (e.g. B-Fast and B-Life), an uncommon collaboration with noted challenges which still proved successful during Ebola crisis;
Training & Communication
• The need for better training and information/communication for military prior to deployment is needed;
• Better coordination among noted existing lab networks to enable these networks to work together and reduce competition;
• Timely sharing of data and samples during epidemics, as well as shared training and logistics to reduce duplication;
• Human resources are essential for efficient performance (retain qualified personnel who can quickly deploy to outbreak zones);
• Train local people in dealing with future outbreaks, so they can independently counter emergency disease outbreaks and reduce dependence on external medical staff;
• Encourage and support sustainable local medical health care capacity;
Community Engagement
• Given the distrust and fear towards strangers, it is crucial to build confidence and acceptance in the new health system to achieve local engagement;
• Understand the local culture, their customs and beliefs in order to conduct successful work;
Lessons Learned • Understand the environment and ecosystem that
surrounds laboratory surge capacity;• Communication with the local community and
being transparent about field work is key to community engagement;
• Legacy is crucial: what do we leave behind? Did we achieve anything in long-term response capacity?
Funding
• Reconsider traditional donor funding models (big donors funding the big NGO’s), need to invest in smaller NGO’s that conduct preparatory work;
• Need for structural funding for local capacity building;
• Pair traditional testing (biochemistry, hematology etc.) with Dx for infectious diseases;
Observations on Industry Solutions
• Early action and mobilization needs to occur to avoid further transmission of disease; higher chances of survival and reduction in overall mortality, with early diagnosis;
• The geographic scope of pathogens can change and this needs to be translated in Dx;
• Investing in R&D despite the lack of market incentives will support efforts to counter future epidemics and pandemics.
• Genetic sequencing is very useful;• The need for sensitive, rapid and integrated Dx
tests to detect a wide variety of (re-)emerging pathogens; preferably syndromic test panels that target 20-30 diseases simultaneously that have similar profiles, defining the exact disease agent is key;
• Less random testing, more syndromic, differential Dx;
• Need for comprehensive and sustainable technologies that local people can use and afford in the long-term;
• Isothermal amplification, as an alternative to PCR, especially valuable in minimally equipped field and mobile lab environments, valid equivalent in terms of clinical performances and delivers results which are quicker and require lower energy needs;
• The need for multi-sample capacities and multiplex assays, broad spectrum tools for differential diagnosis, that have a high throughput;
• Ideally, structural lab capacity: routine clinical and public health Dx should be embedded in local health systems in combination with emerging infectious diseases preparedness support;
• Added value of a mobile lab: early threat detection, key to identifying new cases, in the absence of local capacity, provides a fully independent solution for remote accessibility;

Future Health Threats Initiative 49
Mobile lab requirements:
✔ Truly mobile : rapidly deployable in resource-limited settings, expanding the reach of a fixed site
✔ Field applicable : sufficiently robust to resist tough field conditions, test operationability in rural areas
✔Ability to link the diagnostic results in real-time with patient data = Diagnostic Grid
✔ Deployment plan: logistics, transport, customs
✔ Cheaper than fixed labs✔Wastemanagement procedures✔Fully autonomous and off-the-grid
Existing response initiatives
• European Commission DG ECHO’s among first responders to provide humanitarian funding. The Emergency Response Coordination Centre and its civic protection mechanism can be activated by any affected country, and will provide assistance, coordination and logistics to the field;
• Post-Ebola: European Medical Corps, aims to provide a rapid European response to emergencies with health consequences both inside and outside Europe;
• Weakness: based on voluntary offers from the participating member states to be made available for future deployment, no guarantee of what will be provided (mobile labs, medical air evacuation, emergency medical teams etc.), need increased commitments, for support and assets. Working on a better coordination with WHO, ECDC;
• Institut Pasteur CIBU : Cellule d’Intervention Biologique d’Urgence : response to biological emergencies : epidemiological or bio-terrorist attacks to conduct risk assessments followed by possible interventions and capacity building (sampling, Dx, biosafety);
• CEPI : launched at World Economic Forum in Davos, coalition for epidemiological preparedness and innovation, organizations and foundations joining forces to provide financial incentives to develop vaccines.
QuotesProf. dr. Piot (London School of Hygiene and Tropical Medicine)
“Until today, we do not seem to have learned from disease outbreaks in the past, we reinvent the wheel every time, which is highly inefficient to say the least. Will Ebola change the game? We do not want 11.000 people to have died in vein, we need to show we’ve learned something.”
Conor Elliott (GOAL):
“Building networks of high capacity partners is the most important lesson learned. You cannot be an expert in everything, you need to bring the expertise with you. ”
Prof. dr. Koopmans (Erasmus University):
“During emerging disease outbreaks, interaction between the clinical and public health research purposes is needed. ”
Dr. Daniël Reynders (Belgian Ministry of Health):
“Detection and surveillance are not sustainable without strengthening the local health systems. ”
Hilde De Clerck (MSF):
“A transversal approach is essential in outbreak control, we need glue between the different pillars. ”
Jean-Louis De Brouwer (European Commission, DG ECHO):
“The time has come to align the resources: the scientific expertise and experience together with the political commitment and goodwill.
Future Health Threats Initiative 51
Praesens Mobile Lab aims to take the full power of the traditional diagnostic lab to a site in immediate need, enabling more rapid access to sample testing in the most remote areas and real-time results that are critical in making faster and more accurate medical decisions. Beyond its mandates and capacities, the international community bears the responsibility for intervening during a humanitarian health crisis and helping the most vulnerable communities. We believe cross-sectoral cooperation is a critical component for successful preparedness and response to emergency infectious disease outbreaks.
We believe in accelerated molecular (PCR based) diagnostics that detect a wide range of pathogens through any type of clinical sample, anywhere and anytime. Discover our integrated solutions that address the increasing need for greater laboratory capacity in the field and rapid and highly precise diagnostics and surveillance on-site. In case of an outbreak, our all-terrain vehicles can be rapidly deployed by boat or cargo aircraft to any part of the world. All laboratory equipment is seamlessly integrated into the Mobile Lab. Because there is no need of transporting samples to far away centralized national reference laboratories, no installation time and only some minimal training required, this all dramatically reduces the time and cost of molecular diagnostics. The configuration is customizable according to the location of deployment, the duration of the mission, the type of crisis and the scale of the intervention.
Praesens Fund Mission Statement

Future Health Threats Initiative 53
IdyllaTM stand-alone
IdyllaTM in a box
Mobile lab
• Scalable throughput depending on the context, up to 8 instruments per console
• Low power consumption• No cold chain for cartridges• System operates up to 30°C (validated);
conditions can be extended up to 40°C (tested)
• Low shipping costs• Allowed checked-in luggage in flight• No setup time• No unpacking of the instrument, fully operational
in the ruggedized case• Ruggedized case for remote environments
• All terrain vehicle and fully operational mobile laboratory
• Idylla systems integrated on board• Deployable in the most remote environments • No setup time• Extremely mobile: location depending
on testing needs; no fixed location• Fully autonomous: equipped with generator and
lithium batteries
Integrated & Scalable Solutions
Mobile Lab: bringing the new standard for molecular diagnostic testing to the field

Future Health Threats Initiative 55
Interior highlights
Idylla™ instruments • Modular configuration (up to 8 instruments)
allows a maximum throughput of 96 samples/day*
• Idylla™ instruments accept any possible Idylla™ test cartridge
• Idylla™ test cartridges have all the necessary reagents on-board, blood samples do not require manual intervention prior to sample loading
Idylla™ Console (touchscreen-based) installed in isolatorThree simple steps: • Scan or type in the sample ID • Scan the test cartridge • Load the sample in the test cartridge
Closed, under-pressured biosafety isolator for handling all classes of infectious pathogens• H2O2 decontamination system
Biohazard waste container safely connected to the inside of the isolator
Storage cabinets• For lab equipment,
protective gear and consumables
Lab fridgePreserving the (inactivated) samples
Lab climatization• The lab room is kept at controlled
temperature even in hot (up to 54°C) and humid environments.
Infectious disease assays On Market
IFV-RSV Panel CE - IVD
Ebola
Respiratory MP
Syndromic Panels: -Tropical Fever Flavivirus Panel
- Hemorrhagic Tropical Fever Panel
Viral Load Assays: HIV, HBV and HCV
MeningitisMERS
Prototypes Pipeline
EUA granted by U.S. FDA
Multidrug Resistance Panel

Future Health Threats Initiative 57
Secured sample hatch• External entry port to bring
infectious samples directly in into the isolator
• Badge access for doors, authorized personnel only
Telecommunication system• Permanent connectivity possible by
using rooftop mounted cellular and satellite network connection
• Worldwide secured satellite communication system between the on-field mobile lab and the external world
Disease surveillance gridComplementary technology for epidemiological
mapping that uses the real-time molecular diagnostic data generated by the Idylla™ systems
to capture the evolution of emerging disease outbreaks.
Silent generator and lithium batteries• Powerful generator and
state-of-the-art lithium-ion batteries on board to guarantee full operational autonomy
Biocartis aims to provide direct access to personalized medicine for patients worldwide by developing fully integrated, broadly applicable molecular diagnostics. Biocartis’ MDx Idylla™ platform, launched in September 2014, is a fully automated sample-to-result, real-time Polymerase Chain Reaction system that offers accurate, highly reliable molecular information from virtually any biological sample in virtually any setting. Biocartis is developing and marketing a rapidly expanding test menu addressing key unmet clinical needs in oncology and infectious diseases. These areas represent respectively the fastest growing and largest segments of the MDx market worldwide. Today, Biocartis has seven oncology tests and two infectious disease tests on the market. For more information: www.biocartis.com.
The Praesens Fund is an entity whose purpose is to improve world health by providing in situ disease surveillance through quality molecular diagnostics to social environments in need, irrespective of location and means. The scope of its mission embraces discrete situations in the world in which a measurable impact can be achieved. The fund operates within the frame of the King Baudouin Foundation. The Fund has the aim of raising philanthropic funds to provide and promote the use of molecular diagnostics in resource-poor settings as well as to improve rapid response capabilities and surveillance in areas regularly affected by epidemic and endemic diseases. For more information: https://www.kbs-frb.be
Biocartis trademark and logo are trademarks belonging to Biocartis and are used and registered in Europe. Idylla™ is a registered trademark in the United States and other countries. Idylla™ trademark and logo are used trademarks belonging to Biocartis. Mobile lab is under development and not yet commercially available. Please be aware that some of the features presented in this document are subject to change in the final commercial product.
Biocartis NVGeneraal de Wittelaan 11 B32800 Mechelen - BelgiumT +32 15 632 888www.biocartis.com [email protected]
Praesens [email protected]
Exterior highlights
Certificate Number10506-1507-1002
www.climatepartner.com

Future Health Threats Initiative 59

CONTACTAurélie CappuynsPraesens Fund [email protected]