function of the integumentary system · function of the integumentary system protection temperature...
TRANSCRIPT

Page 96 – 97 & 126 -138
FUNCTION OF THE INTEGUMENTARY SYSTEM
Protection
Temperature regulation - the skin has an abundant blood supply, which is primarily for temperature regulation. For example, when we become hot, the blood supply rushes to the skin surface and heat is lost through radiation.
The skin also regulates temperature by perspiration, when we perspire heat is lost through evaporation.
Sensory input- the skin has millions of nerve endings, which allow us to respond to the sensations of pain, heat and cold.
Excretion of water and waste products
Manufacture of vitamin D.
NORMAL CHANGES ASSOCIATED WITH AGEING:
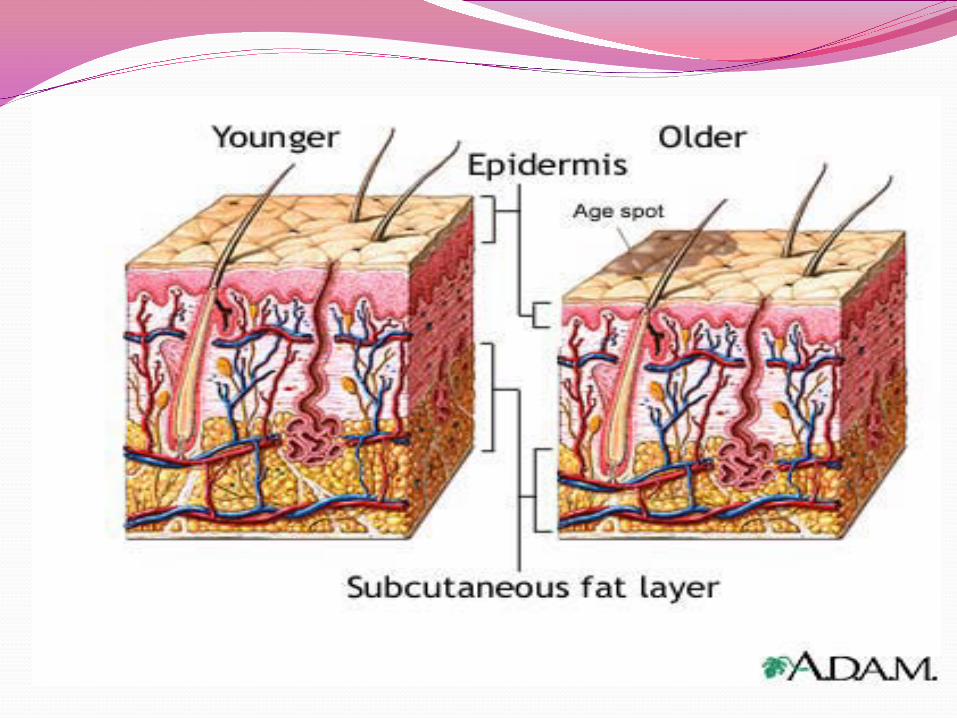
The changes in the appearance and function of the skin reflect the continual ageing process more than any other organ system.
Normal changes: Thinning of the skin layers, decreased strength and
elasticity, decreased vascularity and delayed healing. The epidermis shows a generalised thinning with
advancing age (although there may be some thickening in sun exposed areas) and appears thinner, paler and more translucent.

The dermis contains a large percentage of collagen fibres.
Skin thickens
Decreased vascularity of the dermis and vascular fragility
These factors lead to a slower rate of repair resulting in a higher incidence of pressure ulcers and slower healing of damaged skin.
Decreased vascularity and circulation in the dermis and subcutaneous layer also affects subcutaneous drug absorption, slowing the absorption rate and prolonging the half-life of the drug.
Fat in the subcutaneous layer decreases, arms and legs appear thinner.
Skin becomes folded, lined and wrinkled and has a diminished ability to maintain body temperature and homeostasis.
the secretions of the sebaceous and sweat glands tend to diminish
hair becomes thinner and greyer, and nails become thicker, more brittle and hard with diminished growth rates
Appearance of senile purpura, cherry angiomas, venous stasis, and venous lakes

COMMON HEALTH PROBLEMS AND MANAGEMENT
More than 90% of older people have a skin disorder.
Usually associated with disorders such as diabetes, gout, malignancies, hereditary, stress, neurological disorders, liver disease, muscle weakness, vascular and metabolic disorders, toxic reactions to drugs and obesity
Skin Lesions
Lesions such as keratosis and skin cancers are common. Senile purpura is related to the loss of subcutaneous tissue
Management: Most these lesions cause little discomfort, although skin
cancers need to be treated

Pruritus: Pruritus can occur without a rash and internal causes
should be investigated. However, excessive dryness is the most common cause of itching in the older person
Management: Pruritus can be relived by restricting the amount of
bathing. By applying lubricants and if necessary the administration of drugs such as antihistamines or steroids

Eczema/Dermatitis Eczema is a term often interchanged with the term
dermatitis. Eczema is characterised by round patches of inflammation that are reddened, scaly and extremely itchy
Management: Avoidance of drying agents, use of steroid cream for
inflammation and antihistamines to stop the itching

Stasis Dermatitis associated with leg ulcers
Leg ulcers are common in the older person, and the resulting oedema causes an eczematous reaction
Management:
The leg ulcer needs to be treated by diagnosing the type of ulcer i.e. venous or arterial.
Venous ulcers are much more common that arterial and are treated by application of compression

Herpes Zoster Herpes zoster is also known as shingles, caused by the virus that causes chicken pox and is common
in older people. Presenting problems include: burning pain followed by a papular rash that becomes
oedematous then vesicular and pustular. The skin is permanently scarred and there may be chronic
pain at the site
Management Treatment is usually the administration of an antifungal
agent, and analgesics

Herpes zoster
Psoriasis Psoriasis is usually hereditary and presents as bright
red macules or patches covered with silvery scales
Management A good healthy lifestyle , stress management and
topical medications such as corticosteroids and tar preparations

PSORIASIS

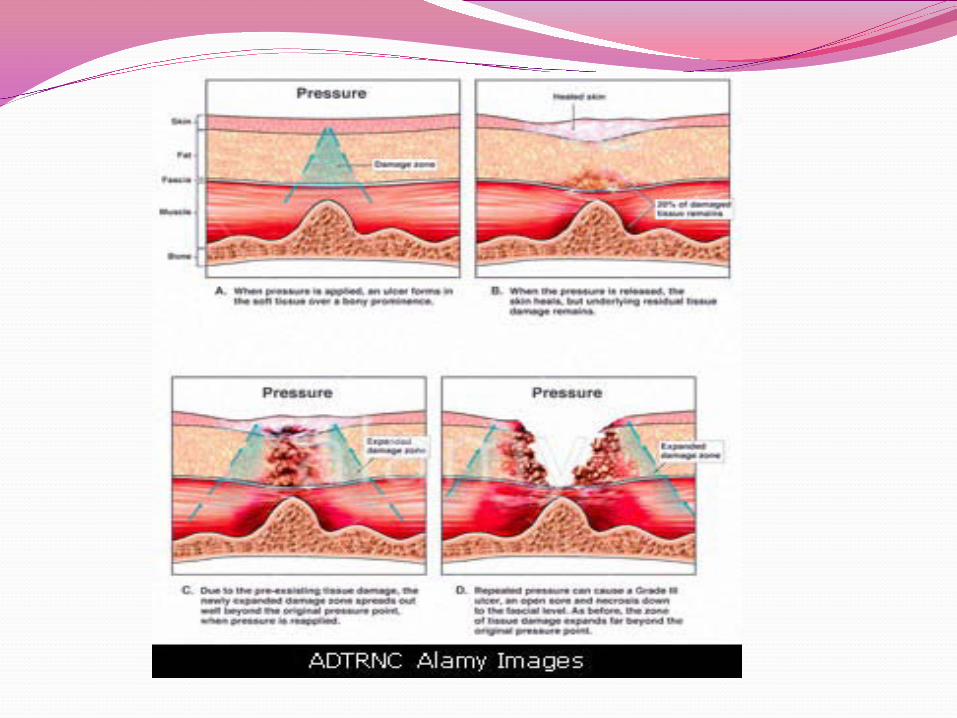
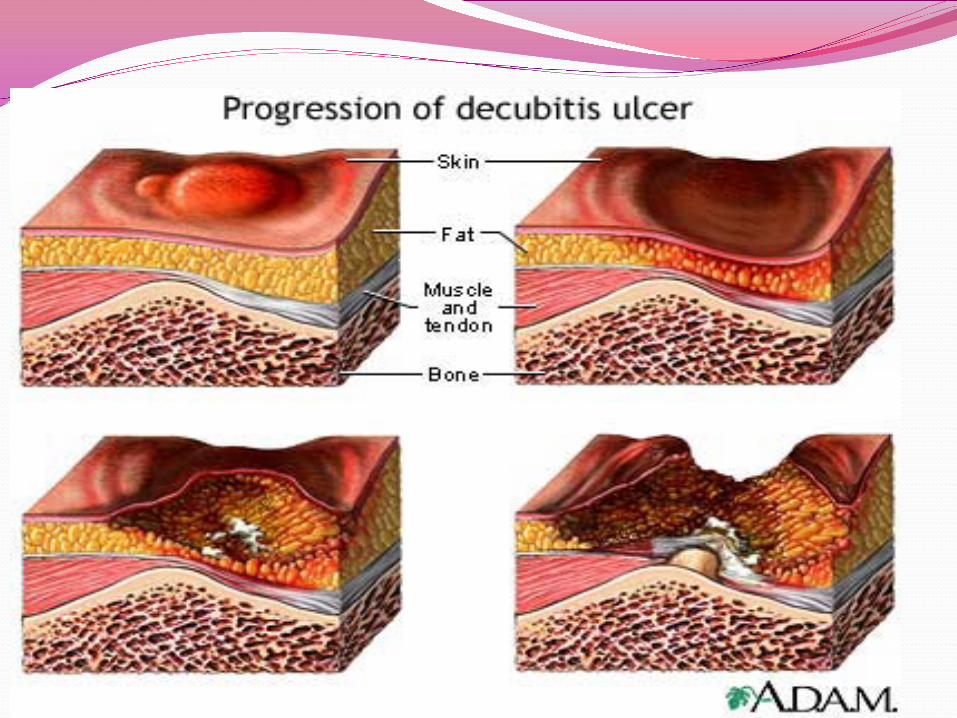
Pressure Ulcers A pressure ulcer is damage to the skin caused by
pressure, shearing forces or friction, or a combination of any of these
Common sites: 95 % of all pressure ulcers develop over bony
prominences on the lower half of the body. 67% of the ulcers occur around the hips and buttocks, 29% on the lower limbs


INTRINSIC EXTRINSCICPoor nutritionAdvancing ageInfection and pyrexiaImmobility - lack of spontaneous movements, repositioningIncreased moistureNeurological/SensoryfactorsVascular factors e.g. diabetes, arteriosclerosis
Prolonged pressure ii. Shearing iii. Friction
Skin Integritye.g. rubbing/massaging theskin

Stages of development Stage I: area of skin becomes red which does not return to
normal colour with relief of pressureStage II: epidermis breaks or a blister is present surrounding area is reddened.
Stage III: breakdown in epidermis through the dermis exudate is present, it may be serous or purulent.

Stage IV breakdown extends into subcutaneous tissue, muscle
and bone exudate is usually present (serous or purulent) sinuses and widely undermined areas may be present.
Some scales include a Stage V infective necrosis destruction of muscle occurs rapidly.

Products & devices to assist with prevention: Any older person who suffers from immobility is at risk of
developing a pressure ulcer. An assessment tool is required i.e Braden, Norton, Waterlow
Strategies used:
Low risk: turning schedule correct lifting
Medium risk: pressure reduction devices
High risk: pressure relief devices
Shearing and Friction A shearing force may occur when a person is pulled
upward in a bed or when in a sitting position, and slides downward.
Shearing forces account for a high incidence of sacral
Friction can be defined as the force of two surfaces moving across one another e.g. an abrasion
It occurs during the movement of persons, during spastic movements, during agitation, or from prosthetic devices or supports
Pressure reduction/relieving devices:
Pressure reducing equipment (static): Pressure reducing equipment is defined as
equipment which “reduces tissue interface pressure as compared to a standard hospital mattress, but does not consistently maintain tissue interface pressure below capillary closing pressure”

This equipment is non-powered, with no moving parts and reduces pressure at the ‘at risk’ sites by distributing an individuals weight more evenly e.g. mattress overlays filled with foam, water, fibre or gel.
This equipment MUST also be accompanied with a turning regime.
To be effective they must be used as per manufacturers instructions (life expectancy, laundering etc)

Pressure relieving equipment (dynamic):
Pressure relieving equipment is defined as those that “constantly maintain tissue interface pressure below capillary closing pressure”
It is equipment, which uses energy or physical force in motion and requires access to a power supply.
This equipment relieves pressure at the ‘at risk’ sites e.g. on a cyclic basis. Every 5-10 minutes an inflated cell (bed width) will deflate and a corresponding deflated cell will inflate.
Other devices/products
seat pads/cushions e.g. foam, gel and fluid
The importance of considering seating needs cannot be stressed strongly enough.
Pressure area care is often overlooked when the individual is seating in a chair, yet it must be considered as part of the overall management.

LEFT HEEL

COMPETENCY-Personal Care - showering, dressing, grooming and shavingMAINTAINING HYGIENE - Bathing We need to wash regularity for a variety of reasons:
It is necessary to establish when a resident preferences for personal hygiene. Why?
Personal hygiene refers to the measures taken to keep an individual’s skin, hair, nails, mouth, nose, eyes and ears clean.
What should you observe when assisting a resident with personal hygiene?

Methods of bathing Bathing Showering Bed bathing/sponging
Safety precautions
Actions for competency in hygiene – bathing
Offer a bedpan or urinal prior to commencing. Promote comfort during procedure
Completely rinse off soap. Residual soap can lead to drying, cracking and itching of the skin.
Dry skin thoroughly (by patting). Prevent skin excoriation.

MAINTAINING HYGIENE – Hair care
What is the importance of brushing, combing and shampooing the hair?
Brushing and combing To stimulate scalp circulation, remove dead skin cells,
distribute natural oils (i.e. sebum) and remove tangles in hair.
Shampooing To remove excess sebum and prevent odour
What important observation can be made when performing hair care?
Texture including dryness, brittleness or fragility, patches of hair loss
Presence of sores on the scalp Infestations of the hair/scalp Excessive flaking of scalp (dandruff)
MAINTAINING HYGIENE - Nail Care
Nails are easier to trim and clean right after they are soaked because they are softer.
Clippers should be used rather the scissors as they are less likely to cause damage.
Caution should be used to prevent damage to the surrounding skin. Nursing assistants should not cut the nails of residents who:
Nails check:
Shape, thickness, texture, colour and length Tissue around nails for: dryness, breaks in the
skin, inflammation, paronychia (infection)
What observations can be made?
Diabetes mellitus Circulatory problems

MAINTAINING HYGIENE – Eye Care
Three (3) indications for eye care: To remove eye discharge and /or crusts. To soothe the eye of individuals with sensitive or
diseased eyes Prior to the instillation of eye drops/ointment
Observations that can be made: Redness or conjunctiva or adjacent tissues Crusting on the eyelashes Any complaints of discomfort or difficulty seeing.
(Others: inability of eyes to move simultaneously, presence of artificial eye, contact lenses).
How do you minimise the risk of cross infection?
Swab from inner to outer canthus of eye
Position on affected side
Use each swab once


MAINTAINING HYGIENE – Mouth Care
Define the following terms: Halitosis Sordes Gingivitis Glossitis Stomatitis
A resident may require mouth care if they are:
Nil by Mouth
Dyspnoea which results in mouth breathing
Oxygen therapy
Unconscious individual
For an individual with a naso-gastric/PEG tube
When teeth cleaning, it is important to: Use circular motions to clean teeth and massage
gums. Use soft toothbrush small enough to reach all
surfaces. Rinse adequately, floss teeth.
When cleaning dentures: Use warm water. Handle carefully; use gauze PRN for firmer grip. Provide mouth care prior to replacing dentures.
Moisten dentures to facilitate easier insertion.
When a resident is unconscious, then the followingprecautions should be used:
Use minimal amount of fluid. Correct positioning, head to side, chin slightly
down. Use tongue depressor to keep mouth open.
Use sponge holding forceps to secure swabs.
BED MAKING
Reasons for bed making.
When linen is soiled
As part of sponging an individual in bed
When an individual goes to theatre
To maintain comfort
After an individual is discharged
When making beds there are a number of principlesto be considered
Reduce the risk of the spread of micro-organisms.
Wash hands before and after bed making
Do not shake linen
Do not hold linen against the nurse’s uniform
Do not put linen on the floor,
Do not put linen on another patient’s bed

Promote comfort and safety, and reduce the risk of complications (e.g. pressure sores and contractures).
Ensure there are no wrinkles or crumbs in the bed Use a toe pleat if indicated (e.g. for those on bed
rest or with reduced mobility) Make sure bed brakes are used Maintain body mechanics (for nurse) Raise the bed to the appropriate height Avoid unnecessary bending, twisting or stretching
Move with smooth, even actions, avoid jerking movements
Conserve time and energy. Gather all linen and equipment prior to
commencing If only one nurse, make one side of the bed and
then the other Use two nurses if possible and work as a mirror
image
Situations when the bedrails should be raised.
Babies and young children
Confused individuals
Unconscious individuals
When one nurse is making an occupied bed