ftre-sa= surgery great and technical
TRANSCRIPT

The Japanese Society of Pediatric Surgeons (JSPS)
NII-Electronic Library Service
The JapaneseSociety of Pediatric Surgeons{JSPS)
ll,jhpt".:,S em36-gl I'- 2000.fti2n
'mek:Esu
- ag 36A H Zs 4sve Slili,1\ tsrvmifi ll
ftre-sA=
23
Surgery forPhysiologic,Transpositionand Technical
Tom R, KarL MD.', Andrew D.
of the Great ArteriesConsiderations
Cochrane,FRACS,
: Anatomic,
Christian PR. Brizard, MD.
" Victroian Paediatric Clardiac Surgicai Unit, Ro.val C7tiidren"s Hospital,
Melbourne, Austtulia
Abstract
The outcome of transposition surgery has been
revolutionized during the past two decades with the
arterial switch operation. Impertant contributions to
this strategy have come from Europe. the USA, Japan,
South America, and Australia. This paper will serve as
an update on some issues relating to the arterial
switch operation, including perioperative support,
pustoperative management, and surgical strategies for
various anatomic subgroups. In this review we analyse
indications, techniques, and outcome for various TGA
subsets, including patients with intact ventricular
septum beyond 21 days of age, intramural coronary
arteries, aortic arch obstruction, the Taussig Bing
anomaly, discordant (corrected) transposition, TGA
with LVOTO, and univentricular hearts with TGA and
SAS.
Abbreviations Used in This Manuscript
ASO l arterial switch operation
AV : atrioventricular
CPB :eardiopulmonarybypass
DORV : double outlet right ventricle
IMCA : intramurat coronary artery
IVS : intact ventricu!ar septum
LA :left atrium
' Adress reprinet requests to : Tom R. KarL M,D. Victorian
Paediatric Cardiac Surgical (Jnit, Royal Children's Hospital,
F]emington Road, Parkville. 3052, Melbourne, AtJSTRALIA,
( 43
LVLVOTOPARVSASTGATVUVHVSD
For the
speciattions,
but
physioLogy and the relative immatumty of the lungs
and the airway. Neonates are known to have a lower
tolerance for the side effects of CPB. There are also
some unique postoperative problems such as necrotiz-
ing enterocolitis and lntraventricular haemorrhage
which occur only rarely even in older infants.
There are a number of cardiac lesions that may
require neonatal repalr, and one of the most impor-
tant and interesting for the cardiac surgeon is TGA.
This lesion presents the surgeon with a unique oppor-
tunity to transform a lethal heart lesion into one with
an excellent long term prognosis. Furthermore this is
usually accomplished within the first week or two of
life. As such. transposition is now the prototype for
neonatal cardiac surgeons.
The ASO has evolved to become the treatment of
)
: left ventricle
: left ventricular outfiew traet obstruction
: pulmonary artery
: right ventricle
: subaortic stenosis
: transposition of the great arteries
: tricuspid valve
: univentricular heart
: ventricular septal defect
lntreduction
paediatric cardiac surgeon, neonates are a
group. This is due not just to size considera-
also to the presence of a dynamic foetal
The Japanese Society of Pediatric Surgeons (JSPS)
NII-Electronic Library Service
The JapaneseSociety of Pediatric Surgeons {JSPS)
24
choice for most forms of TGA, and success with this
operation has become a standard by which paediatric
cardiac surgical units are judged. This is apprepriate,
since without expertise in neonatal anaesthetic
mangagement, perfusion, intensive care, cardiology,
and surgery, consistently good results are impessible
to achieve. Results of the arterial switch operation are
excellent in many centers werldwide these days. and
they surpass results achieved in the era of atrial
repair, especially for the more complex anatomic
subsets, StilL there are a number of anatomic subsets
that continue to present a challenge to the medical
and surgical team.
Surgical Anatomy of TGA
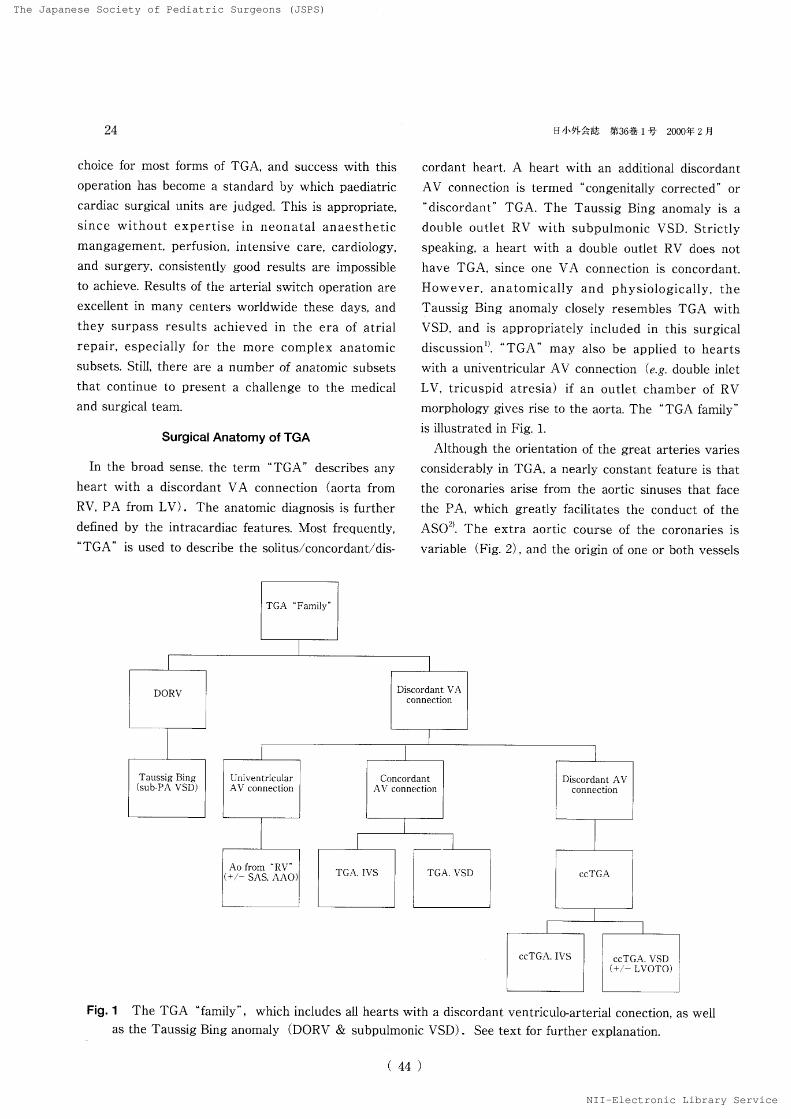
In the broad sense, thc term "TGA"
describes anyheart with a discordant VA connection (aorta fromRV, PA from LV). The anatomic diagnosis is further
defined by the intracardiac features. Most frequently,"TGA"
is used to describe the solituslconcordant/dis-
DORV
TaussigBing(sub-PAVSD)
TGA"Famity'
DtlheF.nL'i,-.. ig36ts1:- 2ooO{F2fi
cordant heart, A heart with an additional discordantAV connection is termed
"congenitally
eorrected" or
"discorclant"
TGA. The Taussig Bing anomaly is a
double outlet RV with subputmonic VSD. Strictly
speaking, a heart with a double outlet RV does net
have TGA, since one VA connection is concordant.
However, anatomically and physiologically, the
Taussig Bing anomaly closely resembles TGA with
VSD, and is appropriately included in this surgical
discussionii. "TGA'-
may also be applied to hearts
with a univentricular AV connection (e.g, double inletLV, tricuspid atresia) if an outlet chamber of RV
morphology gives rise to the aorta. The `'TGA
family"
is illustrated in Fig..].
Although the orientation of the great arteries varies
considerably in TGA, a nearLy constant feature is that
the coronaries arise from the aortic sinuses that face
the PA, which greatly facilitates the conduct of the
AS02). The extra aortic course of the coronaries is
variable (Fig. 2) , and the origin of one or both vessels
UlliventriculflrAV connection
Ao from 'RV'
{..,- SAS, AAO}
rDistordant
AV connection
ccTGA
ccTGA.IVS , ccTGA. L'SD
C+.,- LVOTO)
Fig. 1 The TGA "family",
which includes all hearts with a discordant ventriculo-arterial cenection,
as the Taussig Bing anomaly (DORV & subpulmonic VSD). See text for further explanation,
(44)
NII-Electronic
as well

The Japanese Society of Pediatric Surgeons (JSPS)
NII-Electronic Library Service
The JapaneseSociety ofPediatric Surgeons {JSPS)
H ,JieFkl-Lig36ts 1 t'2ouoelzH
S{Left h
A
g}
25
Leiden lLCx-2R Leiden lL-2RCx . c. Leiden lCx-2LR
YacoubA YacoubD
'
RCA
x
llS<D LAD LAD
B C
P
R
,
L
RCA RCA
LeidenlR-2LCx LeidenlLR-2Cx
Yacoub E
Fig. 2 The Leiden classification of eoronary anatomy in TGA. The right hand of an observer standing
in the non-corenary sinus (facing the coronary ostia) points to sinus 1, the left hand to sinus 2, The
most common pattern is ILCX, 2R. Corresponding Yacoub nomenclative in included where
appropnate.
may rarely be intramural and stenotic posing special
problems for the surgeon during AS03)`),
Diagnosis of TGA
The diagnosis of TGA colud be considered in any
cyanotic newborn, but ECG, CXR, and physical
examination are not diagnositc. 2D echocardiography
usually provides rapid and complete non-invasive
diagnosis, and in the neonate, cardiac catheterisation is
rarely necessary. A weak area in imaging is the
proximal coronary arteries, which may be difficult to
accurately describe with echocardiography or angiog-
(45
raphy`). Prenatal echo diagnosis of TGA is new
possible as well, although knowing what to do with the
information remains problematic5).
Physiolegy and Natural History
The central physielogic problem is arterial
haemoglobin desaturation. the severity of which varies
with the degree of communication between the
parallel systemic and pulmonary circulations. The
neonatal presentation varies from that of a healthy
appearing baby to complete cardiovascular collapse,
At the worst end of the clinical spectrum are those
>
NII-Electronic

The Japanese Society of Pediatric Surgeons (JSPS)
NII-Electronic Library Service
TheJapaneseSociety of Pediatric Surgeons {JSPS)
26
babies with a rest.rictive ASD and,'or aortic areh
obstruction, who are uften profoundly hypoxaemic und
acidotic.
The natural history of all forms of TGA is extremely
unfavourable, and without some form of palliative or
definitive surgery, most neonates would not survive
infancy. In nearly all cases, the initial resuscitation
efforts sheuld include balloon atrial septostomy.
irrespective of surgical plan.
Timing of operation is criticai. especially for babies
with TGA. IVS, In ext,rauterine life, the puln]onary
vascutar resistance drops from its foetal (systemic)
level to a nermal postnatal level within 2 weeks. This
decline will be accempanied by an involution of LV'
mass, unless a PDA. VSD, or LVOTO is present to
maintain the LV pressure at systemic levels. The
optimal time for ASO is therefore wihtin the first 2
weeks of life, if one is to avoid the preblem of a
"deconditioned" LV, "rhich may conLribute to low
cardiac output postoperativelyfi}. Infanrs wlth TGA and
arch obstructien (as weH as other PGE-1 dependent
patients) usuatly require operation within the first
few days of life7) In TGA. VSI). elective operation can
usually be carried out at 1-3 months of age, if the
clinical condition remains stable.
Surgery for TGA
The goal of transposition surgery is to restore a
series circulation with a feur chambered heart, using
the left ventricle and the systemic circuit in the right
ventricle and the pulmonary circuit. The left ventricle
is more suited for pressure work fer a number oi
reasons, The conus portion is minimal, and the left
ventricle is mostly sinus morphology. The left
ventricle was the original pump in evolution, and has a
dual coronary and conduction system and a more
compact myocardium than the right vcntricle. The
mitra] valve is a better design than the tricuspid valve
for high pressure work, since the papillary muscles
arise trom the free wall rather than the septum.
The ASO has emerged as the preeedure of choice
for most babies with TGA, The technical modification
employed at the RCH is a hybrid of techniques
proposed by Jatene, Lecompte, Quaegebeur, Mee, a]d
(
['IilxV"・ftStV・,'t,' ee36ts 1 ;]- LOoo# 2 H
others2)S)'iO). The proccdure is technically demanding,
but logical ancl reproducible. We briefly describe the
ASO technique herein.
With the heart arrested, the aorta and PA are
transected just above the commissures <Fig, 3). The
coronaries are excised with a large cuff of sinus tissue,
and medially based reetangular fiaps are cut into the
facing sinuses of the PA. The mobilised coronaries are
translecated and sutured in place with running 8,,'O
potypropylcne. We employ the Lecompte manoeuvre
in nearyl all cases, ineluding those with side by side
great vessetsD)]iL The neoaortic anastomosis is
completed by gathering tissue on the proximal side to
match the vessel sizes. At this point the VSD, if
present, is closed with pledgett.ed mat,tress sutures
A, v""
iK
Fig.
46 )
rkRCA
BPANeoaorta)
/
Neopulmenarya. .X#ila-
3 The ASO technique used at the RCH. We
employ medially based rectangular flaps in the
ncoaortic sinuses for coronary translocation. Theflaps decrease the are of rotation and prevent
tension on the anastomosis. Neopul-monary sinus
defects are repaired with large autulogous
pericardial patches, extended posteriorly.
'E /
/. ・At.ttT.-.'"r'l-.t't="t'.. t.'--
e.-'-..T=-t.''tt7?ttttt? ).'
/t ' i'NeoaorLa
'
NII-Electronic

The Japanese Society of Pediatric Surgeons (JSPS)
NII-Electronic Library Service
TheJapaneseSociety of Pediatric Surgeons {JSPS)
H4lib'Vkth ut36ts 1 ny- 2ooe4f zn
and a Dacron patch. The ASD is closed directly. and
the heart is deaired. With the aortic clamp efL the
neopulmonary sinus defects are repaired with
individual autologous pericardial patches. extended
posteriorly to lenghten the PA. The neopulmonary
anastomosis is completed, and the patient is warmed
to 37℃ , then separated from CPB. LA and PA lines
and a peritoneal dialysis catheter are used in most
cases.
Perioperative Support Systems
There are a number of problems related to cardiG
pulmonary bypass for ASO in neonates. They include
the prirning volume, the wide range of flows, the
extremes of temperature. duration of the procedure,
and dinthesis toward capillary leak syndreme and
bleeding,
For our CPB strategy we employ a fresh heparin-
ised blood prime, and a hollow fiber or membrane
oxygenator2). Citrate preseved blood (CPD) imposes a
pon-physiologic osmolar load due to glucose, and low
rnetabolism of citrate may occur due to hypothermia
and reduced hepatic perfusion and function, Newborns
are especially at risk due to altered calcium
'rnetabolism and a decreased capaeity to rnetabolise
'citrate, We therefore believe that fresh heparinized
blood is a superior physiologic solution for prirning the
CPB circuit. No citrate is added to the heparinized
unit, resulting in better in vivo preservatiun of 2, 3-
DPG, red cells, and labi!e coagulation factors.
AIpha stat pH strategy is fQllowed for ceeling to 26'
28℃, In most cases. full flow CPB (150 ml!kg) is used
for the entire operation, with aortic and bicaval 'cannulation, and left heart venting through the ASD.
We have employed cold crystalloid cardioplegia
solution and topical cold saline fpr myocardial
protection, although many units use sanguineous
cardioplegia with good resuLts. Various cardieplegia
solutions have been shown to have similar results in
neonatal cardiac surgery, However, equally important
to the content is the way in which it is delivered. For
antegrade cardioplegia in the arterial switch operation
it is critically important to maintain a physioiogic
aortic root pressure. in order to avoid poor distribution
(47
27
of cardioplegia(low pressure), or myocaridial oedema
(high pressure). Haemostasis is important in neonatal cardiac
surgery, especially for the ASO. We currently employ
aprotinin for all ASO. Aprotinin is a polyvalent
enzyme inhibitor and modulator of the coagulation and
infiammatory responses. It attenuates the release of
some pro infiammatory cytokines after bypass (TNF
a , interleuken 1, interleuken 6) . Aprotinin is known to
prevent coagulation, fibrinolysis, and platelet activation
during and/or after CPB, and haemostatic benefit has
been documented in numerous ctinical studies. The
disadvantage is that aprotinin is a basic polypeptide of
bovine origin with antigenic properties. Re-exposure
should therefore be avoided within 6 months of
uriginal exposure, to avoid the risk of anaphylaxis. Our
usual aprotinin dose is 10,OOO KIU!kg for loading, and
hourly during CPB. Higher doses of aprotinin (30,OOOKIUfkg) therefore may be associated with better
suppression ef the inflarnmatory response.
Control of fluid accumulation is a critical peint for
safe cenduct of the arterial switch operation. We
employ modified ultrafiltration following CPB as well
as peritoneal dialysis postoperatively. We also use
continuous AV haemofiltratien during CPB, Our
modified ultrafiltration circuit is shown in Fig. 4. 0ver
Ao cannulaM.
U, F, circuit for neonatesvenous
cannula
Fig. 4 Modified ultrafiltration circuit employed at the
Royal Children's Hospital. The priming volume
can usally be removed over a 20 minute period,
with predictable haemodynamic improvement.
)
NII-Electronic
The Japanese Society of Pediatric Surgeons (JSPS)
NII-Electronic Library Service
TheJapaneseSociety of Pediatric Surgeons {JSPS)
28
an average time of 20 minutes we are usuatly able to
remove the entire priming volume, resulting in signifi-
eant haernoconcentration. During this time we gener-
ally see improvement in systolic and diastolic function
which occurs more rapidly than would be expected
without the use of medified ultrafiltration, There may
also be a reduction in fluid retention, weight gain, and
transfusion requirements. Modified ultrafiltration has
been shown to attenuate the brain injury associated
with prolonged circulatory arrest times. There is a]so
a predictable reduction in pulmonary artery pressure
which takes place coneurrent to appearance of
endothelin 1 in the uttrafiltrate.
The peritoneal catheter is equally important for
neonatal cardiac surgery. This catheter is placed
routinely at the time of arterial switch operation, and
is left on free drainage for abdominal decompression.
For periods of reduced urine output or hypercal-
caemia, isotonic or hypertonic dialysate 10mLlkg (30minute exchange cycles) is used. We also employ cold
dia]ysis for core cooling for rhe treatment of postoper-
ative hypothermia, especially when associated with
arrhythmias.
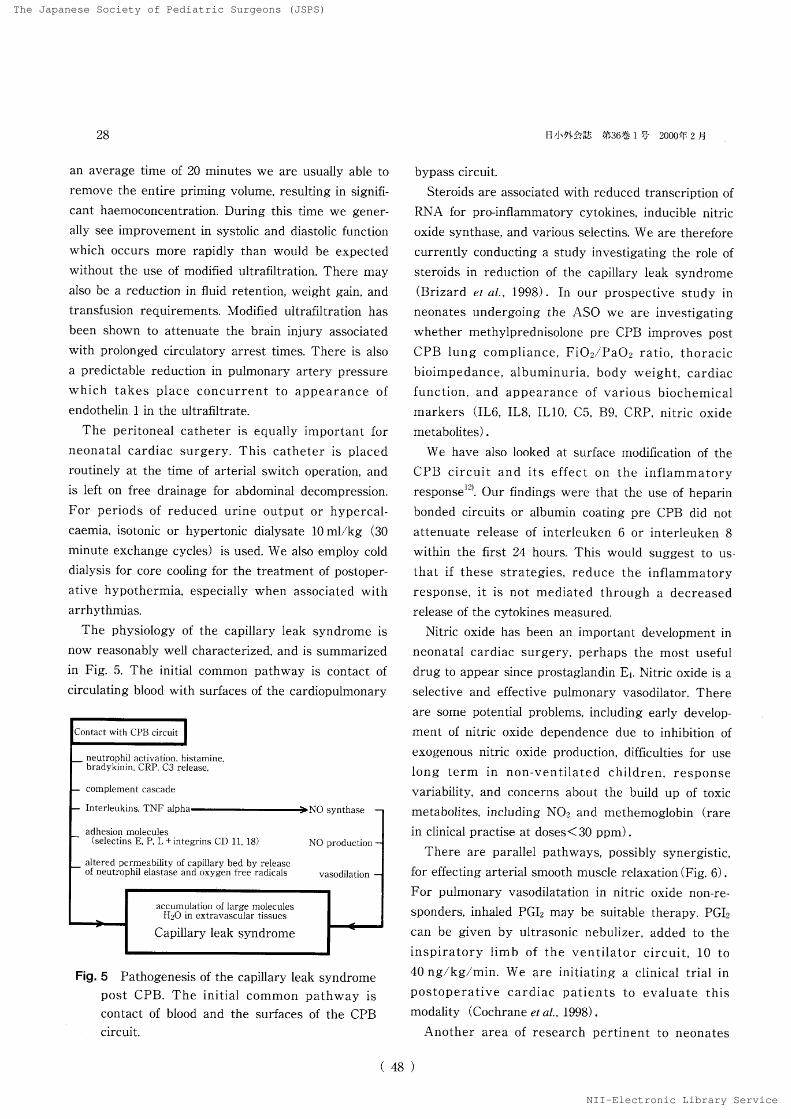
The physiology of the capillary leak syndrome isnow reasonably well characterized, and is summarized
in Fig. 5. The initial common pathway is contact of
circulating blood with surfaces of the cardiopulmonary
Fig. 5 Pathogenesis of the capillary Leak syndrome
post CPB. The initial cemmon pathway is
contact of blood and the surfaces of the CPB circuit.
( 48
n,JiP"kE',l ac36ts 1 Fi 2oooff 2 N
bypass circuit.
Steroids are associated with reduced transcription of
RNA for pro-inflammatory cytokines, inducible nitric
oxide synthase, and various selectins, We are therefore
currently cenducting a study investigating the role of
steroids in reduction af the capillary leak syndrome
(Brizard et ai., 1998). In our prespective study in
neonates undergoing the ASO we are investigating
whether methylprednisolone pre CPB improves postCPB tung eompliance. Fi021Pa02 ratio, thoracic
bioimpedance, albuminuria, body weight, cardiac
function, and appearance of various biochemical
markers (IL6, IL8, ILIO. C5, B9, CRP. nitric oxide
metabolites).
We have also looked at surface modification of the
CPB cireuit and its effect on the inflammatory
responseiZ). Our findings were that the use of heparin
bonded circuits or albumin coating pre CPB did not
attenuate release of interleuken 6 or interleuken 8
within the first 24 hours. This would suggest to us・
that if these strategies, reduce the inflamrnatory
response, it is not mediated through a decreased
release of the cytokines measured.
Nitric oxide has been an important development in
neonatal cardiac surgery, perhaps the most useful
drug to appear since prostaglandin Ei, Nitric oxide is a
selective and effective pulmonary vasodilator. There
are some potential problems, including early develop-
rnent of nitric oxide dependence due to inhibition of
exogenous nitric oxide production, clienculties for use
long term in non-ventilated children, respense
variabMty, and concerns about the build up of toxic
metabelites, including N02 and rnethemoglobin (rare
in clinical practise at doses<30 ppm).
There are parallet pathways, possibly synergistic,
for effecting arterial smooth muscle relaxation (Fig, 6) .
For pulmonary vasodilatation in nitric oxide non-re-
sponders, inhaled PGIz may be suitable therapy. PGI2
can be given by uttrasonic nebulizer, added to the
inspiratory limb of the ventilator circuit, 10 to
40 ngfkg/'min. We are initiating a clinical trial in
postoperative cardiac patients to evaluate this
modality (CochraneetaL 1998).
Another area of research pertinent to neonates
)
NII-Electronic

The Japanese Society of Pediatric Surgeons (JSPS)
NII-Electronic Library Service
The JapaneseSociety of Pediatric Surgeons {JSPS)
N,IHPFft-ar as36ts1・ry 2000ff2fi
L-arginine
arachidonic acid
Fig.
1 ll
.8
.6
.4
2
o
o NO ocGMP
(lliiiiil})
O PG-12 =>cAM
6 Parallel pathways for relaxation of arterioLar
smooth muscle, both relevant for control of PHT
in neonates post CPB. There may be a therapeutic
role for both nitric oxide and prostaeyelin (PG I2).
29
Table 1 Parameters studied for prediction of major
adverse events post CPB. Only MAP index and serum
lactative hact signifi-cant predictive value. From i
Duke T, Butt W, South M, Karl TR. Early markers of
major adverse events in children after cardiac
operations, J Thorac Cardiovasc Surg, l14:1042-
1052, 1997.
Predicting major adverse events (admission to ICU)
Variable Event NocventOdds ratiop
Prebability {log-iikelihood)
MAP index
Hean rate
CtD02SV02Base
deficit
Lactate(mmolU)
GastricpHi
DC027be-core
temp
109
98
3.45619,4
48.9-2.4
3
Z26 15.4
3.f
12S104
4.22470
61.7-O.4
2,2
7,31 12.9
3.2
O.96O.97e.7O.96O.95O.841.36O,64e,96O,98O.03O.12O.25O,09O,12O.J4O.03O.2O.3e.
84
e 2 4 6 8 10 Lactate in mmoVl
Fig. 7 Probability of a major adverse event following
open heart surgery, based on serum lactate levels
in the ICU. Serum lactate at 4 hours had
singificant predictive value for adverse events.
From1Duke T, Butt W, South M, Karl TR. Eary
markers of major adverse events in children after
cardiac operations. J Thorac Cardiovasc Surg.
114 : 1042-1052, 1997.
undergeing the ASO is prediciton of major adverse
events after cardiac operationsi3). Such events include
cardiac arrest, need for emergency chest opening.
sepsis, multiorgan failure and death, We know that
hypotension may be a late and unre!iable sign, and
that measurement of cardiac output is invasive,
dithcult, expensive and unreliable in neonates, Table 1
summarizes the parameters examined in predicting
major adverse everits in our patients during their ICU
stay, Figure 7 shows a predicted probability of major
adverse events following cardiac surgery based on the
serum lactate level at 4 h. There is a strong cerrela-
(49
tion, which was not found with the other parameters
examined. The unanswered question is whether
treatment of elevated lactate in isolation can prevent
the development of a major adverse event,
Special Problems
A number of anatomic and physiologic TGA subsets
require special consideration, and are discussed
herein :
1 . The older baby with TGA. IVS
Beyond 2 weeks of age, LV involution has usually
begun, and concerns are therefore raised regarding
postoperative centractility. An early ASO study using
pooled CHHS data suggested that the risk of ASO
increased beyond 7 days of agei4}, This result !ed many
centres to adopt a 2 stage approach for children
beyond 2'3 weeks of age. especialLy those with
subnormal calculated LV mass or wali thicknessiS)', We
know that post-natal myocardial growth is character-
ized by an early hyperplastic phase of myocytes and
capillaries, followed by myocyte hypertrophy only.
Pressure overload induces hypoplasia, hypertrophy
and angiogenesis in neonates but only rnyocyte hyper-
)
NII-Electronic

The Japanese Society of Pediatric Surgeons (JSPS)
NII-Electronic Library Service
The JapaneseSociety of Pediatric Surgeons {JSPS)
30
trophy tater on. Therefore the capacity and rapidity of
LV hypertrophy may decrease dramatlcally with
increasing age of the patient. Rapid LV hypertrophy
has been doeumented in the early postoperative
period6). We have therefore taken the appreach of
offering a primary ASO to all children up to 8 weeks
of age, <and selectively to older children us we]1)
irrespective gf LV pressure, geemetry or massE),
Infants with TGA.IVS presenting between 8 weeks
and 6 mont,hs of age are best treated with a two stage
Aso strategy6)i5)i6). The capacity of the LV to respond
to a pressure load with hypertrephy in this age group
makes rapid retraining (<2 weeks) possible, The
first stage is transsternal PA band placement,
accompanled by a 4 rrim PTFE innominate to right PA
sh'u'ht to maintain oxygenation, Tennporary low cardiac
output follewing this procedure is common, but within
7'10 days the LV pressure and mass will usually be
adequate to allow ASO without severe low cardiac
output postoperatively. Within this time frame,
adhesions are generally llot too troublesome at
resternotomy, and ASO (with simple debanding and
shunt.division) can be performed as described above.
In older patients, a more pro]onged period of LV
conditioning is usually requiredii). Fortunately, sueh
patients are unusual in today's practise.
1)he left ventricular assist device provides
postoperative support for rapid retraining of the LV in
patients with borderline function after the ASO due to
preoperative deconditioning. Looking at 53 infants and
children who required ventricular assist device
support in our unit (alg diagnostic groups), those
with TGA or ALCAPA syndrome had the best overall
survival probability of 0.91 (CL O.59J1.0).
2. Coronary artery abnormalities
We would consider virtually all coronary artery
variations to be potentially suitable for ASO, although
some are more problematic than others from n
technical point of veiw. In ()ur experience with over
400 ASO, only 1 patient was considered unsuitable by
virtue of coronary anatomy (a premature infant with
bilateral intramural branching of a single coronary,
coursing between Ao and PA). IMCA was noted in
(50
H,]sptftas bl36tsle 2000ny2H
Fig. 8 Intramural left coronary artery shown in cross
sectional echocardiogram. The proximal left
coronary courses within the aortic walL The ostium
is eccentrically placed and frequently stenotie. This
pattern is seen in about 5% of cases of TGA, and
creates technical problems for excision,
(a) (b) (1c1)
(d) (e>
Fig. 9 Teehnique mobi!ization and translecation of an
IMCA. The posterior aortic commissure is
detached (a)to provide sinus tissue for eoronary
excision {b). The ostium is cutback to enlarge
and move it laterally (c), The commissure is
resuspended from the pericardial patch <d e),
5% of infants undergoing ASO in our institute <Fig.
8). The natural history of IMCA in TGA is unknown,
but there is an association of this type of coronary
anatorny with sudden death in concordant hearts.
In tnfants with IMCA, the arterial switch technique
must be modified4). Following aortic transection, an
IMCA should be suspeeted if there is an eccentrically
)
NII-Electronic

The Japanese Society of Pediatric Surgeons (JSPS)
NII-Electronic Library Service
The JapaneseSociety of Pediatric Surgeons {JSPS)
nilhSSkts ee36msle 2000ijt- 2n
placed, small, or apparently single ostium er a vessel
arising atop a valve commissure. To mobilise and
translocate this type of vessel safely, the posterior
aortic valve commissure must be detached (Fig. 9).
The ostium is then cut back to enlarge it and move it
laterally. The coronaries are excised as a large cuff
which can be divided and translocated as described
above. This technique leaves a single large defect in
the neopulmonary artery which can be repaired with
one pericardial patch, The commissure can then be
resuspended to the patch with interrupted sutures to
reconstruct the neopulmonary valve. The operation
may then be completed as described above.
3 . TGA with LVOTO
LVOTO is found in 20% of infants with TGA, and is
often considered a contraindication to ASO, In such
patients, alternate strategies can be employed, but the
longterm results may be less satisfactory than those of
the ASO. A minority of patients may have a
resectable type of LVOTO, such as accessory AV
valve or endocardial cushion tissue, fibrous subvalvar
membranes, and anornaldus rnuscle bundlesi8}. The
final decision regarding resectability must often be
made intraoperatively. Resection is performed via the
transected PA, combined with exposure through the
tricuspid valve if necessary. Structures at risk during
resection include the ,neoaortic valve, coronary
branches, and the cenduction tissue. Sustained relief of
obstrvction can be expected in preperly selected
cases.
4 . TGA with aortic arch ob$truction
Aortic arch obstruction. rare in TGA.IVS,
complicates 7'10% of cases of TGA.VSD and Taussig
Bing anomalyii). The obstruction is mest commonly a
discrete coarctation with a hypoplastic transverse arch
and isthmusi9)20), A compLete interruption is more likely
to occur in the UVH with TGA and SASMZi'. For all
types of TGA with arch obstruction, closure of the
ductus can precipitate profound cardiovascular
collapse in the neonate. The risk of necrotising
enterocolitis and intraventricular haemorrhage is also
increased as compared to other forms of TGA. Most
(51
31
patients with TGA and arch obstruction should have a
one stage neonatal repair via median sternotomy7)2b,
For arch repair, two arterial periusion cannulas are
placed, one in the ascending aorta .and the ether in the
ductus, which is proximally ligated. The patient is
cooled to 18℃. the circulation is arrested, and snares
are placed to occlude the head vessels, Selective
myocardial perfusion has been employed in some
patients, The descending aorta is transected justbeyond the duct insertion and anastomosed to the
ascending aorta at the base of the innominate artery.
The arterial switch is then cpmpleted as described
above.
5. TheTaussig Bing Anomaty
Defining this entity has created more problems for
the anatomist than for the surgeon. Certainly there is
some overlap between DORV with uncomitted VSD,
Taussig Bing anomaly, and TGA with VSD. For
surgical purposes, however. the key question in DORV
is whether or not the LV can be directly connected te
the aorta via an intraventricular tunnel, or whether
the LV can be more directly connected to the PA.
There are a nurnber of operatiens which have been
employed for this latter situation. including atrial level
and intraventricular repairs wlthout ASO. Our strong
preference, however, is ASO, performed within the
first three months ef Lifei2). The surgeon should be
aware that Taussig Bi4g hearts are more Likely to
have atypical coronary anatomy, side by side great
vessels, and aortic arch obstruction than are other
TGA variants. ASO is performed as for TGA,VSD,
with a transatrial approach for placement of a LV-PA
baffle, Exposure through the tricuspid valve ls usually
quite adequate. and pledgetted individual sutures can
be placed around the subpulmonic conus and through
the septal TV leaflet. A large Dacron patch is used for
septation, in order to achieve an unobstructed
pathway to the neoaorta, which has a biventricular
origin, overriding the VSD. The neopulmonary artery
anastomesis can be constructed on a branch PA,
closing a portion of distal main PA. to compensate for
a side by side vessel position. In an occasional patient
PA reeonstruction may be performed better without
)
NII-Electronic
The Japanese Society of Pediatric Surgeons (JSPS)
NII-Electronic Library Service
The JapaneseSociety of Pediatric Surgeons {JSPS)
32
the use of the Lecompte manoeuver]2).
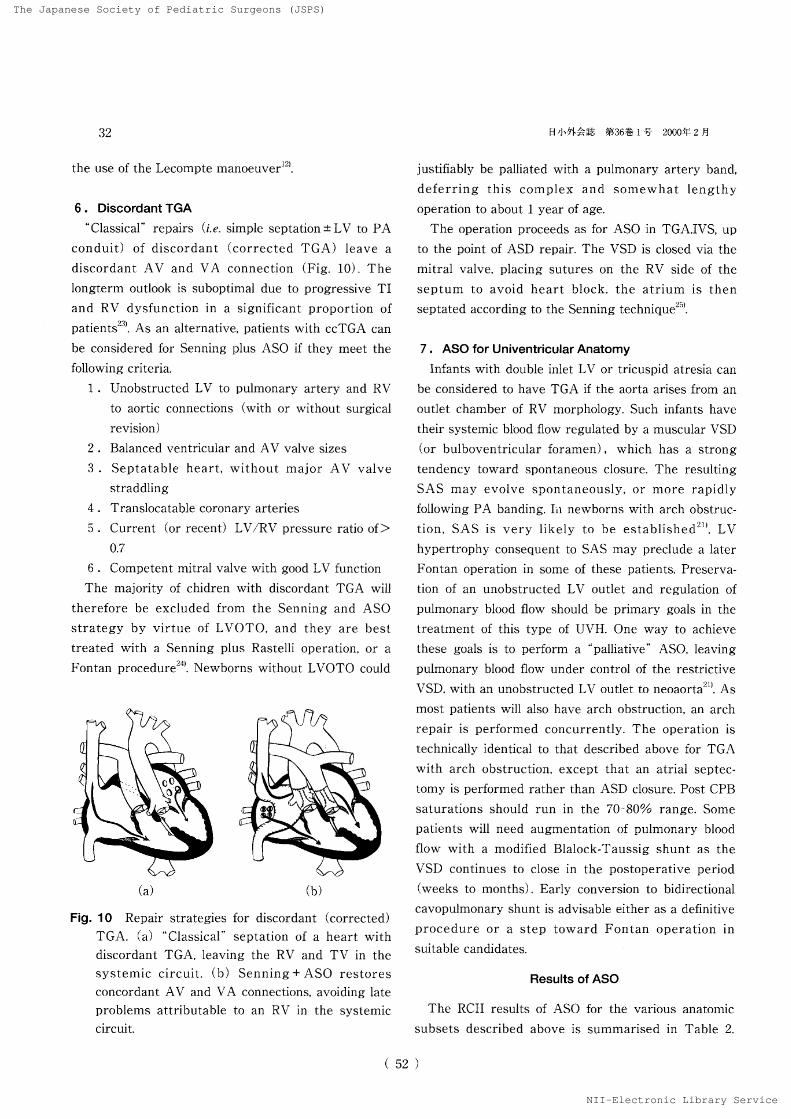
6. DiscordantTGA
"Classical"
repairs (i.e. simple septation ± LXr to PA
conduit) of discordant (corrected TGA) leave a
discordant AV ancl VA connection (Fig. 10). Thelongterm outlook is suboptirnai due to progressive TI
and RV dysfunction in a significant proportion of
patientsL'3L As an alternative, patients with ccTGA can
be considered for Senning plus ASO if they meet the
follewing criteria.
1 . Unobstructed LV to pulmonary artery and RV
te aortic connections (with or without surgical
revision)
2 . Balanced ventricular and AV valve sizes
3 . Septatable heart, without majer AV valve
straddling
4 . Transiocatable coronary arteries
5 . Current <or recent) LVfRIv' pressure ratio of>
O,7
6 . Competent mitral valve with good LV' function
The majority of chidren with diseordant TGA will
thereiore be excluded frem the Senning and ASO
strategy by virtue of LVOTO, and they are best
treated with a Senning plus Rastelli operation, or a
Fontan procedure24). Newborns without LVOTO coutd
¢
ooegl
・ oo
Y
(a) (b)
Fig.10 Repair strategies for discordant (eorrected) TGA. (a)
"Classical" septation of a heart with
discordant TGA, leaving the RXJ and TV in the
systemic circuit, (b) Senning+ASO restores
concordant AV and VA connections, aveiding tate
problems attributable to an RV in the systemic
circuit.
(52
HJJx・ptkE't[ ca36ts1 ny- 2000f2H
justifiabty be palliated with a pulmonary artery band,
deferring this eomplex and somewhat lengthy
eperation to about 1 year of age.
The operation proceeds as fbr ASO in TGA,IVS, up
to the point of ASD repair. The VSD is closed via the
mitral valve, placing sutures en the RV side of the
septum to avoid heart block. the atrium is then
septat,ed according te the Senning technique25}.
7. ASOforUniventricularAnatomy
Infants with double inlet LV or tricuspid atresia can
be considered to have TGA if the aorta arises from an
outlet chamber of RV morphology. Such infants have
their systemic blood flow regulated by a muscular VSD
(or bulboventricular foramen), which has a strong
tendency toward spontaneous elosure. The resulting
SAS may evolve spontaneously, or more rapidly
following PA banding. In newborns with arch obstruc-
t,ion, SAS is very like]y to be established2i). LV
hypertrophy consequent to SAS may preclude a later
Fontan operation in some of these patients, Preserva-
tion of an unobstructed LV' outlet and regulation of
pulmonary blood flow should be primary goals in the
treatment of this type of UVH. One way to achieve
these goals is to perform a "palliative"
ASO. Ieaving
pulmonary btood flow under control of the restrictive
VSD, with an unobstructed LV outlet to neoaortaL'i). As
most patients will also have arch obstruction, an arch
repair is perforrned concurrently. The operation is
technically identical to that described above for TGA
with arch obstruction, except that an atrial septec-
tomy is performed rather than ASD closure. Post CPB
saturations should run in the 70'80% range. Some
patients will need augmentation ef pulmonary blood
flew with a modified Blalock-Taussig shunt as the
VSD centinues to close in the postoperative period
(weeks to rnonths). Early conversion to bidireetiunal
cavopulmonary shunt is advisable either as a definitive
procedure or a step toward Fontan operation in
suitabre candidates.
Results of ASO
The RCII results of ASO for the various anatomic
subsets described above is surnmarised in TabLe 2.
)
NII-Electronic Mbrary

The Japanese Society of Pediatric Surgeons (JSPS)
NII-Electronic Library Service
The JapaneseSociety of Pediatric Surgeons {JSPS)
u,]wlftde ng36-g1e 2ooorp2H
The lowest risk group consists of babies with TGA.
IVS operated upon within the first 3 weeks of life. The
risk of primary ASO for infants in the 3'8 week age
range compares favourably to that of a two stage
approach with PAB prus shunt (Table 3), although
we don't have a large experience with the latter
strategy in our own unit. This risk also compares
favourably with that of many other open heart
procedures, especially those performed in neonates.
The risk has been higher for the mere compLex TGA
subset7)i2)2V. Intramural coronary artery has not been
an independent risk factor for operative mortallty,
whether considered against non-IMCA patients as a
group, or within the various anatomic subsets (Table4a, b) 4)en).
Long term follow up of our own TGA patiellts (>
Table 2 RCH results of the ASO for various anatomic
groups. The highest risk group comprised infants with
uni-ventricular anatemy. Arterial Switch Outcome in
413 Cases (to December 1997)
95 % confidenceHospitalmortality intervals
33
1000 patient years) has shown that most children
have experieneed normal growth and development
with a good quality of life following ASO, We have
hand no late deaths in patients undergoing ASO for
TGA. IVS or TGA. VSD,
The operative risk of ASO for 27 infants with Taus-
sig Bing anomaly was 7% (CL=1-23%) and, in our
exprience, not increased for patients requiring cencur-
rent aortic arch obstruction (p := 1.0)i2). Actuarial survial
and freedom from reoperation at 72 months were
likewise similar (p>O.05). All survivors are in NYHA
classIata rnean jla time of 54 (+1-36) months, and
all are in sinus rhythmi2]. The risk of ASO for Taussig
Bing anomaly also compares very favourably to
alternate surgical strategies used for similar patients.
The experience with Senning+ASO for discordant
TGA is limited. Fourteen patients have had the
operation performed since July, 198922). Age and
Operation type
TGA,IVS
TGA,VSD
TaussigBing
Double switch
DILV-SASConversion
2r222 ( O.9%)5X121 ( 4,1%)21 30 (6.6 %)lt 14 (7 %)31 12 <25 %)
2t !9 (le.5%)
O- 3%1-
9%1-22
%O-34 %S-S7 %1-33%
Table 4a,b Outcome of ASO in the presence of IMCA.
(a) The risk of ASO stratified according to coronary
anatomy, There was no signMcant risk increment for
[MCA vs ILCX-RR. the most cornmon (and
technically most straightforward) variant. (b) ASO
risk stratified by coronary anatomy within anatemic
subgroups. Once again, we could not demonstrate a
risk increment fbr IMCA.
(a) Risk ofASO Stratified by Coronaiy Anatomy
Coronary type n Risk (95%CL) p
Table 3 Outcome for babies with TGA and intact ventri-
cular septum operated after day 21. Although the risk is
higher in older babies with intact septum, primary ASO
compares favourably to a 2 stage approach up to 8
weeks of age.
ASO after day 21 1 Outcome
iLdr2RIL2RCxSingleintramurat
ILR2CxInvertedOther
Group
21969332e
17
17
7
swI9 (2.3%, 1- 5%)lt 69 (1.5 %, O- 8%)
31 33 (9 %,2-24 %)
cr 20( O-17 %)
Of 17( O-19 %)lf l7 (5,8%,O-29 %)Ol 7( O-41 %)
LJ
1
Mortalityrisk 95%CL p
T6A.IVS
(<21 days)
TGA.IVS
(>21 days)>21 days, low pLV>21 days, high pLV
O/191 O- 2%
21 24 (8.3%) 1-27% O.Ol
U19 (5,2%) O-26% O.09
IX 5 <20 %) 1-72% O.02
<b) ASO Risk Stratified by Coronary & Intracardiac
Anatomy
Anatomy non-IMCA IMCA p
IVS 1 % <O-3%) Ot14 (O-23 %) 1
VSDtDORV 4.8%(2-10%) O16(O-46%) 1
Total 2.6% (1-5%) Of20 (O-17%) 1
(53)

The Japanese Society of Pediatric Surgeons (JSPS)
NII-Electronic Library Service
TheJapaneseSociety of Pediatric Surgeons {JSPS)
34
weight medians were 12 months (O.5-120) and 8.2 kg
(3.2J3.4). AII but one patient had a left ventricular te
right ventricular pressure ratio>O,7, due to a large
ventricular septal defect (+!-previous PA band),
severe congestive heart failure frorn RV dysfunction
and tricuspid insufficiency, or pulmonary artery band
for left ventricular retraining. At Ieast 10 patients had
strong contraindications to laclassical"
repair, including
right ventricular hypoplasia (n=2) moderate to
severe RV dysfunction, (n=5) and/or moderate to
severe tricuspid insufficiency (n=9). There was one
hospital death, occurring in a neonate (7%, CL=O-
34%). Actuarial survival beyond 10 months is 81%
(CL=42-95%), currently with 389 patient months
total fellow-up time. The median grade of tricuspid
insufficieficy fell from 3,/4 preoperatively to 1,i4 post-
operatively (p=.O03), Right ventricutar function is
normal in 1IA2 current survivors, a!t but one of whom
are in NYHA calss 1 or 2. 0ne child required revision
of the Senning baffle.
26 of our first 413 ASO paticnts had some form of
anatomic LVOTO, due to uccessory endocardial
cushion,!AV valve tissue, iibromuscular subpulmonic
obstruction, or anomalous muscle bands]S). Actuarial
survival at 5 and 10 years following ASO and LVOTO
resection was similar C97 vs 92%p>O.05) to the rnain
ASO cohort, but there was a higher probability of
reoperation (p<O.O05). The preoperative LV-PA
gradient was not a good predictor of resectabilityi8).
For infants with UV'H, TGA, and SAS, ASO as
palliative treatment has carried an operative risk
which is high but competitive with other treatment
strategies (e.g. Norwood operation, PA band+/rV'SD
enlargement, cardiac transplantation)2[). Although ASO
has been highly effective for permanent relief of SAS
In our patients, ultimate suitability for further
operations has been limited ln some cases by I'A
distortion related to the use of the Lecompte
manoeuvre. Of 12 neonates so treat.ed, 7 of 8 Iong-term
survivors have had a bidirectional cavopulmonary
shunt and 5 of these have progressed to a Fontan
operation (over 400 patient months follow up), The
best treatment strategy for this difficult TGA subset
remains undecided although the Damus connection
(54
il4ieFftax ca36#1・e 2000qi2H
Cwith MBTS) is currently our favoured approach,
reserving the technically more complex ASO for
selected patients,
The ASO in biventricular hearts with TGA comes
very close to being both a complete anatomic and
physiologic correction. The mujority of patients (>
95%) after ASO, at teast those with the less eomplex
variants, have normal resting LV function. Segmental
perfusion abnormalities may occasionally be seeen on
Tc 99 scuns at rest but they tend to improve with
exercise. These defects are not predicted by ECG or
echo. LV end systolic wall stress/fibre shortening
vetocity has been relative]y normaL suggesting that
contractility is not impaired. Importantly, these results
are significantly better than the best published data
concerning atrial level repairs!'7)'35). The presence of an
IDvTCA at operation has not been associated with late
death, or with ischaemic features on ECG or echocar-
diography`)ZO), Routine angiographic surveillance of
postoperative ASO patients in our own institution has
failed to reveal any coronary anastomotic problems
{irrespective of coronary anatomy and translocation
technique). We are initiating a study to assess the
ability of MRI to image coronary post ASO (Karl et al.,
1999).
The most frequent indication for reoperation has
been supravalvar putmonary stenosis (8 patients in our
series). but this complication has been nearly eliminated
by the use ol our current PA recenstruction techniques
(see technique section) .
Following ASO, there has been a tendency for great
vessel (anastomotic) diameter to be smaller than that
of controls, and for the neoaortic root to be larger.
Reported risk factors for neoaortic root enlargement
include the presence of neoaortic insufficiency, a
previous PAB, and switch conversion followirig atrial ttt tt /tttrepalr.
Concerns have been raised about a6rLic insufficiency,
which develops in abeut 10% ef patients following the
ASO. This has been at,tributed to progressive dilation
of the neopulmonary annulus, a phenomenon that has
aLso been reported in other conditions in which the
pulmonary valve is used in the systemic circulatlon.
We lookcd at our own patients at a mean follow up of
)
NII-Electronic Mbrary

The Japanese Society of Pediatric Surgeons (JSPS)
NII-Electronic Library Service
TheJapanese Society of Pediatric Surgeons {JSPS)
H ,JiSF ft:-S S36g 1 t 2000f 2 fi
105 months. calculating the echocardiographic diam-
eter of the ・neoaortic annulus and neopulmonary
annulus (Fig, 11). We found that the neoaortic
annulus was significantly Larger than predicted (meanZ score 2,59 ± 2.7). However if the regression was
performed against a normal pulmonary annulus, the
mean Z score fell to O.87± 1.35. This difference was
highly significant (p=O,OOOI). In a multivariate
analysis neither age at operation, weight at operation,
follow up interval, nor type of intracardiac anatomy
were predictive of the Z score, The median grade of
aortic insufficiency in these patients was O (range O-2)
and was not related to the annular Z score using
either the aorta or the pulmonary artery as a controL
These data suggest that the neoaorta does not dilate
abnormally but rather grows as a normal pulmonary
valve. The mechanism of the insufficiency may lie
elsewhere.
Although ASO results are now exceilent in most
large centres when only operative mortality is
considered, concerns have been-raised regarding long-
term neurodevelopmental outcome36)37}, There are a
number of CPB strategies available for the ASO. We
have preferred full fiow with moderate hypothermia
for most operations. Circulatory arrest is unnecessary
for most ASO. and has been associated with some sub-
Neoaortic diameter following ASO
62 patients, 105 (84-180) months flu
Z SCORE {annulus diameter) 8
6
4
2
o-2-4
p-,Oop1
Fig. tl Neoaortic diameter a'fter ASO. Regression
against normal aortic controls suggests 'dilation,
but using normal PA control values the mean Z
score is significantly lower.
( 55
35
optimal correlates of neurological outcome. Children
who have been subjected to circulatory arrest for ASO
were found to have developmental index scores that
were lower (at 1 year) than children operated with
low flow CPB36)3ny. Whether or not the use of full flow
CPB affords more neurological protection remains to
be demonstrated and is currently under investigatient tmour own unlt.
'・
We are evaluating a cohort of 220 survivors of ASO
for TGA with intact ventricular septum. Five year
actuarial survival in this group is 99%. All of these
patients had operation according to a similar flow and
temperature stragtegy whicli consisited primarily of
full flow bypass at 150 ml!kgfmin. These patients
have been reviewed and compared to "best
friend"
controls, Using a battery of standard neurodevelop-
mental outcome tests, as well as clinical examination
and neurologic testing. our results to date suggest that
the switch patients cannot be 'distinguished from the
best friend controls, based on a total impairment seore
which takes into account a number of growth and
manual skill factors. Likewise vision, hearing,
neurological exam abnormalities, and learning
disabilities were similar in the two greups. '
Conclusion
The ASO has emerged as the treatment of choice
for most TGA variants. The results compare favor-abiy to what was achieved in the era of atrial level
repairs. The promise of an improved outlook has been
fulfi11ed at 15 year follow-up, Unresolved issues center
on the Iongterm fate of the coronaries and neoaortic
valve as survivors or neonatal ASO reach their adult
years.
Referenceg
1 > Taussig HB, Bing RJ : Complete transposition of
the aorta and a levoposition of the pulmonary
artery, Am Heart J, 37 I 551, 1949.
2)・ Karl TRITransposition of the great ・arteries.
in : Nichols DG, Cameren DE (eds) I Critical
Cardiac Disease in Infants and Childreni pp 825-
840, Mosby Year Book, St. Louis, 1994,
3) Gittenberger-de Greot AC, Sauer U, et al:
)
NII-Electronic

The Japanese Society of Pediatric Surgeons (JSPS)
NII-Electronic Library Service
The JapaneseSociety of Pediatric Surgeons {JSPS)
36
Corenary artery anatomy in transposition of the
great arteriesIa morphologic study. Pediatr
CardioL 4: 15, 1983.
4) Aseu T, Karot TR, Mee RBB I Arterial switch
operation : Translocation of intramural corollary
arteries, Ann Thorac Surg, 57 1 461'465, 1993.
5) Kirklin JW, Celvin EV, McConnell ME, et aL 1
Complete transposition of the great arteries 1
Treatment in the current era. Pediatr Clin North
Am, 37:l71-177, 1990.
6) Davis AM, Wilkinson JL, Karl TR, et al :
Transposition of the great arteries with intact
ventricular septum. Arterial switch repair in
patients 21 days of age or older. J Thorac
Cardiovasc Surg, 106 : 111'l15, 1993.
7) Karl TR, Sano S, Brawn W, et alIRepair of
hypoplastic or interrupted arch via Sternotomy. J
Thorac Cardiovasc Surg, 104 1 688'695, 1992.
8) Jatene AD, Fontes V'F, Paulista PP, et at:
Successful anatomic correction oi transposition of
the great vessels. A preliminary report. Arq Braz
Cardiol, 28 I 461-464, 1975.
9) Lecompte Y, Zannini L, Hazan E, et al1
Anatomic correetion of transposition of the great
arteries. J Thorac Cardiovasc Surg, 821629'631,
1981.10)
Quaegebeur JM 1 The arterial switch operation :
Rationale, results and perspect,ives. Thesis :
Leiden University, The Netherlands 1986.
11) Cemas JV, Mignosa C. Cochrane AD, et al:
Taussig-Bing anomaly and arterial switch : Aortic
arch obstruction does not influence out.come. Eur
J Cardiothor Surg, 10 1 1114-1119, 1996.
12) Horton SB, Mullary RJ, Butt WW, ez al 1 IL-6
and IL-8 levels following CPB are net affected by
surface coating. Ann Thorae Surg, 199, in press.
13) Duke T, Butt W, South M, et al 1 Early markers
of major adverse events in children after cardiac
operatiens, J Thorac Cardiovase Surg, 114:1042-
1052, 1997.
14) Kirklin JW, Blackstone EH, Tehervenkov CI, et
al : Clinical outcomes after thc arterial switch
operation for transposition, patient support, proce-
dural, and institutional risk factors. Circulation, 86
(56)
11,1iVFft1・S ac36ts1- ZOOOff2J]
C 5 ) : 1501-1515, 1992.
15) Yacoub MH, Radley-Smith R. Maclaurin R ]
Twostage operation for anatemical correction of
transposit{on of the great arteries with intact
ventricuLar scptum, Lancet, 1 1 1275-1278, 1977.
16) Kirklin JW, Barratt-Boyes BG : Complete
transposition of the great arteries. in Kirklin JW,
Barratt Boyes BG (eds) : Cardiac Surgery, pp.
1383-1467, Churchill-Livingstone, New York, l993.
17) Duke T, Butt W. South M, et al I Eary markers
ef major adverse events in children after carcliac
operation. J Thorac Cardiovasc Surg, ll4:1042'
1052, ]997.
17)' Cochrane AD, Karl TR, Mee RBB 1 Arteriat
switch for Eate failure of the systemic right
ventricle. Ann Thorac Surg, 56 1 854-861, 1993.
]8) Sohn Y, Brizard C, Cochrane A, et al : Arterial
switch in hearts with left ventricular outflow and
pulmonary valve abnormalities. iXnn Thorac Surg,
66 1 842-848, 1998,
19) Milanesi O, Thiene G, Bini RM, et aliComplete
transposition of great arteries with coarctation of
aorta. Br Heart J, 481 566-571, 1982.
20) Schneeweiss A, Motro M, Shem-Tov A, et al [
Subaortic stenosis I An unrecognised problem in
transposition of the great arteries. Am J Cardiol,
48 : 336-339, 1981.
21) Kart TR, Watterson K, Sano S, et aliOpera-
tions for subaortic stenosis in univentricular
hearts. Ann Thorac Surg, 52: 420-42T I991,
22) Karl TR. Weintraub RG, Cochrane AC, et alI
Senning and arterial switch:a good option for
children with discordant (corrected) t,ranspo-
sition. Ann Thorac Surg, 64 : 495-502, 1997.
23) Sano T. Riesenfeld T, Karl TR. et al]Inter-
mediate-term outcome after intracardiac repair of
associated cardiac defects in patients with atrioven-
tricular and ventriculoarterial diseordance.
Circulation, 92 1 II272-278, 1995.
24) Ilbawi MN, DeLeon SY, Backer CL, et al[An
alternative approaeh to the surgical management
for physiologically corrected transposition with
ventricular septal defect and pulmonary stenosis
or atresia. J Thorac Cardiovasc Surg, 100:410-
NII-Electronic
The Japanese Society of Pediatric Surgeons (JSPS)
NII-Electronic Library Service
The JapaneseSociety of Pediatric Surgeons {JSPS)
HtJheVISts ngB6-kl g- 2000f2n
415, 1990.
25) Senning A : Surgical correction of transposition
of the great arteries. Surgery, 45 [ 966-980, 1959,
26) Soto R, Brizard CP. Conchrane AD, et al : Intra-
mural coronaries in transposition of the great
arteries, results of arterial switch operation.
Proceedings of Second World Congress of
Pediatric Cardiology and Cardiac Surgery, 160,
1997.27)
Jatene AD, Fontes VF. Paulista PP, et al :
Anatomic correction of transposition of the great
yessels. J Thorac Cardiovasc Surg, 72:364'370,
1976.28)
Brawn WJ, Mee RBB 1 Early results for anatom-
ic correction of transposition of the great arteries
and fer double outlet right ventricle with
subpuimonary ventricular septal defect. J Thorac
Cardiovase Surg. 95 : 230-238, 1988.
29) Moat NE, Pawade A, Lamb RK[Complex
coronary arteriaL anatomy in transposition of the
great arteries, Arterial switch procedure without
coronary relocation. J Thorac Cardiovasc Surg,
103 : 872-876, 1992.
30) Veelken N, Gravinghoff L, Keck EW. et al]
Improved neurological outcome following early
anatemical corre'ction of transposition of the great
arteries. Clin Cardiol, 15 : 275-279, 1992.
31) Lupinetti FM, Bove EL, Mimich LL, et al:
Intermediate-term survival and functional results
after arterial repair for transposition of the great
(57)
37
arteries. J Thorac Cardiovasc Surg, 103:421J427,
1992.32)
Minet P, Vaksmann G, Rey C, et aL:Doppler
echocardiography after anatomical repair of
transposition of the great vessels. Arch Mal Coeur
Vaiss, 85 :515-520, 1992.
33) Serraf A, Bruniaux J, Lacour-Gayet F, et al:
Anatomic repair of Tassuig-Bing hearts.
Circulation, 84 I M 200-M 205, 1991.
34) Kramer HH, Rammos S, Krian A, et al1
Intermediate-term clinical and hemodynamic
results of the neonatal arterial switch operation
for complete transposition of the great arteries.
International J Cardiol, 36 : 13J22, 1992,
35> Vouhe PR, Tamisier D, Leca F, et al1Trans-
position of the great arteries. ventricular septal
defect and pulmonary outflow tract obstruction i
Rastelli or Lecompte procedure ? J Thorac
Cardiovas Surg, 103 I 428, 1992.
36) Bellinger DC, Jonas RA, Rappaport LA, et ali
Developmental and neurologic status of children
after heart surgery with hypotermic circulatory
arrest or low-flow cardiopulmonary bypass.
MEJM,・332 1 549-555, 1995,
37) Newburger JW, Jonas RA, Wernovsky G. et al:
A comparison of the perioperative neurologic
effect of hypothermic circulatory arrest versus
low-flow cardiopulmonary bypass in infant heart
surgery. MEJM, 329 1 1057'1064, 1993.