ftplectures musculoskeletal system lecture notes ... · ftplectures musculoskeletal system lecture...
TRANSCRIPT
Ftplectures Musculoskeletal system Lecture Notes
MUSCULOSKELETAL
Medicine made simple
This content is for the sole use of the intended recipient(s) and may contain information that is proprietary, confidential, and exempt from disclosure under applicable law. Any unauthorized review, use, disclosure, or distribution is prohibited. All content belongs to FTPLECTURES, LLC. Reproduction is strictly prohibited.
COPYRIGHT RESERVED

Ftplectures Clinical Medicine Copyright 2014 Adeleke Adesina, DO Clinical Medicine © 2012 ftplectures LLC 1133 Broadway Suite 706, New York, NY, 10010 The field of Medicine is an ever-changing profession and as new evidence based studies are conducted, new knowledge is discovered. Ftplectures has made tremendous effort to deliver accurate information as per standard teaching of medical information at the time of this publication. However, there are still possibilities of human error or changes in medical sciences contained herein. Therefore, ftplectures is not responsible for any inaccuracies or omissions noted in this publication. Readers are encouraged to confirm the information contained herein with other sources. ALL RIGHTS RESERVED. This book contains material protected under International and Federal Copyright Laws and Treaties. Any unauthorized reprint or use of this material is prohibited. No part of this book may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system without express written permission from ftplectures.
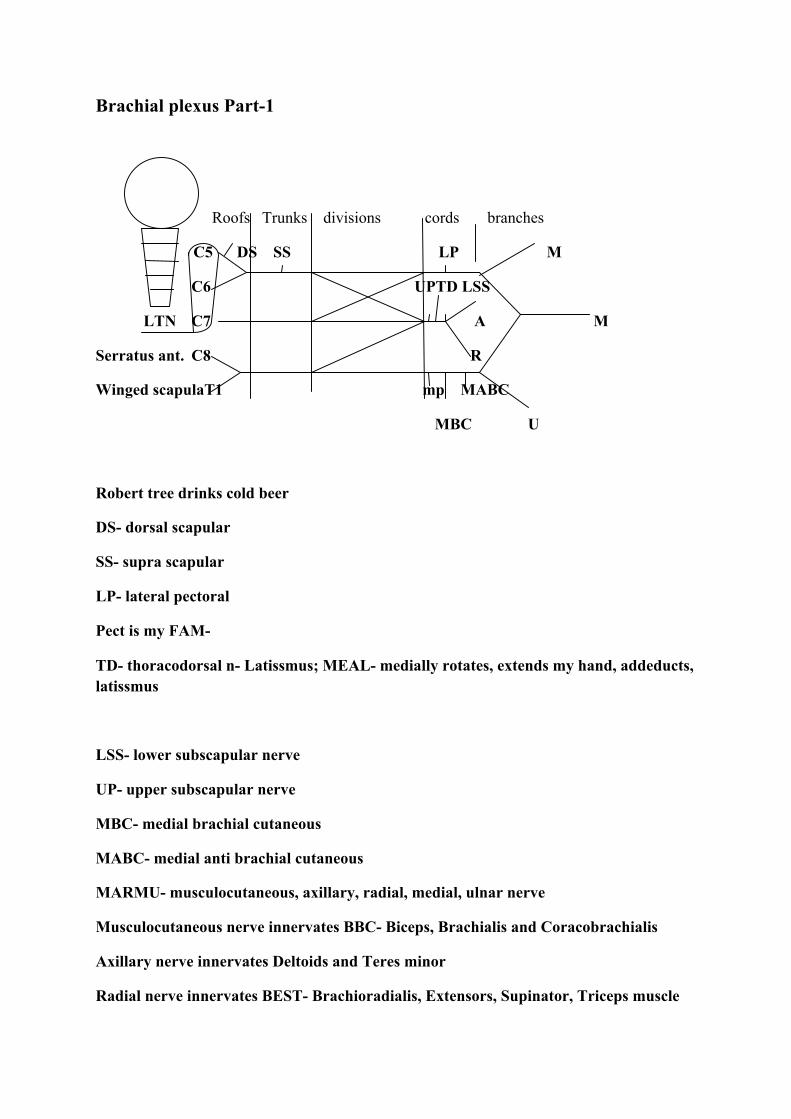
Brachial plexus Part-1
Roofs Trunks divisions cords branches
C5 DS SS LP M
C6 UPTD LSS
LTN C7 A M
Serratus ant. C8 R
Winged scapulaT1 mp MABC
MBC U
Robert tree drinks cold beer
DS- dorsal scapular
SS- supra scapular
LP- lateral pectoral
Pect is my FAM-
TD- thoracodorsal n- Latissmus; MEAL- medially rotates, extends my hand, addeducts, latissmus
LSS- lower subscapular nerve
UP- upper subscapular nerve
MBC- medial brachial cutaneous
MABC- medial anti brachial cutaneous
MARMU- musculocutaneous, axillary, radial, medial, ulnar nerve
Musculocutaneous nerve innervates BBC- Biceps, Brachialis and Coracobrachialis
Axillary nerve innervates Deltoids and Teres minor
Radial nerve innervates BEST- Brachioradialis, Extensors, Supinator, Triceps muscle
Median nerve innervates 2 LOAF- 2 lumbricals, oppones pollicis bravis, abductor pollicis bravis and flexor pollicis bravis
Compression of median nerve causes Carpal Tunnel syndrome- caused by excessive use, prednisone, hyperthyroidism.
Hand of benediction due to damage to median nerve- pope sign- ulnar nerve works but median nerve does not function
Ulnar nerve-75% of all muscles in your hand innervated.
Hypothenar nerve, 2 lumbricals, PAD [palmar interossi addeduct] and DAD dorsal interossi [abduct]
Ulnar nerve damage causes claw hand when asked to make a fist.
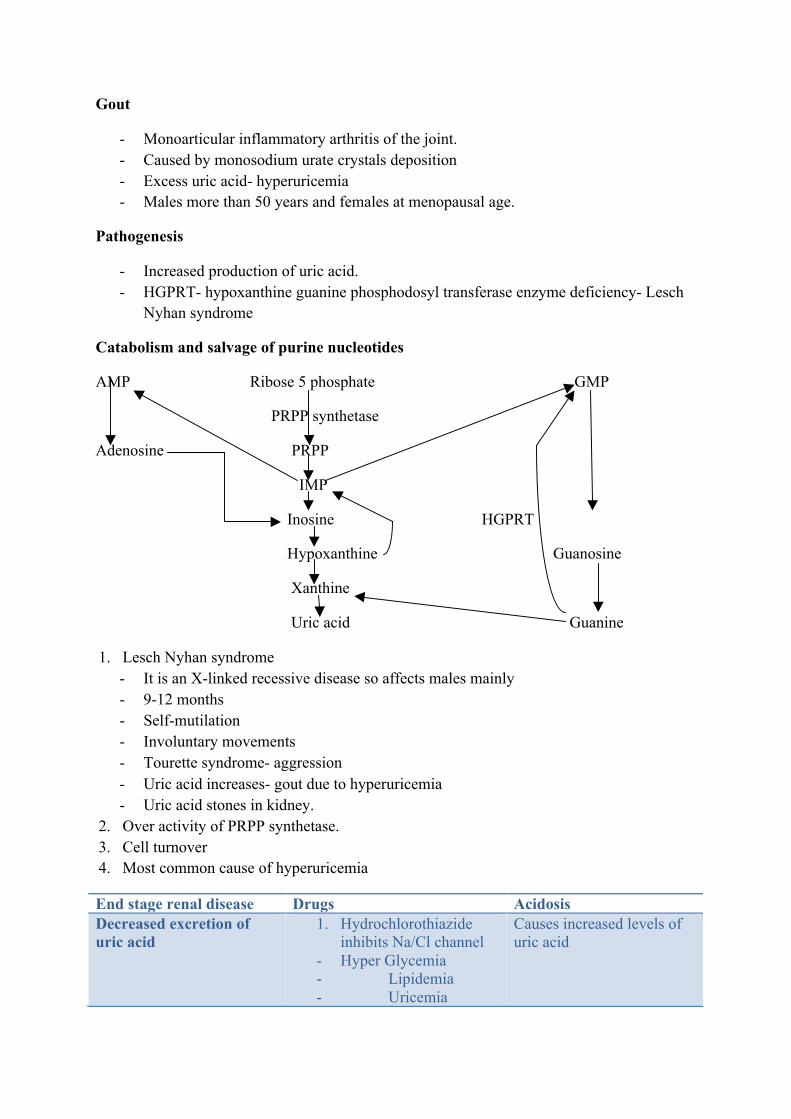
Gout
- Monoarticular inflammatory arthritis of the joint. - Caused by monosodium urate crystals deposition - Excess uric acid- hyperuricemia - Males more than 50 years and females at menopausal age.
Pathogenesis
- Increased production of uric acid. - HGPRT- hypoxanthine guanine phosphodosyl transferase enzyme deficiency- Lesch
Nyhan syndrome
Catabolism and salvage of purine nucleotides
AMP Ribose 5 phosphate GMP
PRPP synthetase
Adenosine PRPP
IMP
Inosine HGPRT
Hypoxanthine Guanosine
Xanthine
Uric acid Guanine
1. Lesch Nyhan syndrome - It is an X-linked recessive disease so affects males mainly - 9-12 months - Self-mutilation - Involuntary movements - Tourette syndrome- aggression - Uric acid increases- gout due to hyperuricemia - Uric acid stones in kidney.
2. Over activity of PRPP synthetase. 3. Cell turnover 4. Most common cause of hyperuricemia
End stage renal disease Drugs Acidosis Decreased excretion of uric acid
1. Hydrochlorothiazide inhibits Na/Cl channel
- Hyper Glycemia - Lipidemia - Uricemia
Causes increased levels of uric acid
- Calcemia 2. NSAIDS- Aspirin 3. Immunosuppressants
like TAcrolismus and cyclosporine
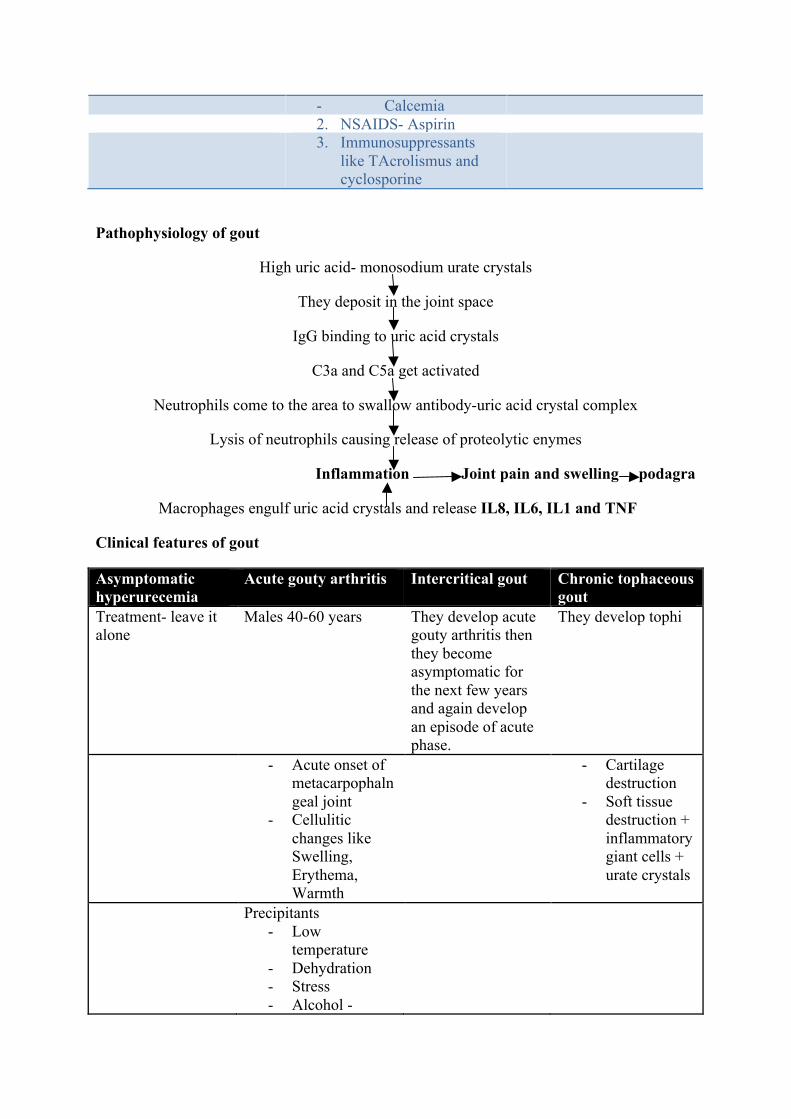
Pathophysiology of gout
High uric acid- monosodium urate crystals
They deposit in the joint space
IgG binding to uric acid crystals
C3a and C5a get activated
Neutrophils come to the area to swallow antibody-uric acid crystal complex
Lysis of neutrophils causing release of proteolytic enymes
Inflammation Joint pain and swelling podagra
Macrophages engulf uric acid crystals and release IL8, IL6, IL1 and TNF
Clinical features of gout
Asymptomatic hyperurecemia
Acute gouty arthritis Intercritical gout Chronic tophaceous gout
Treatment- leave it alone
Males 40-60 years They develop acute gouty arthritis then they become asymptomatic for the next few years and again develop an episode of acute phase.
They develop tophi
- Acute onset of metacarpophalngeal joint
- Cellulitic changes like Swelling, Erythema, Warmth
- Cartilage destruction
- Soft tissue destruction + inflammatory giant cells + urate crystals
Precipitants - Low
temperature - Dehydration - Stress - Alcohol -
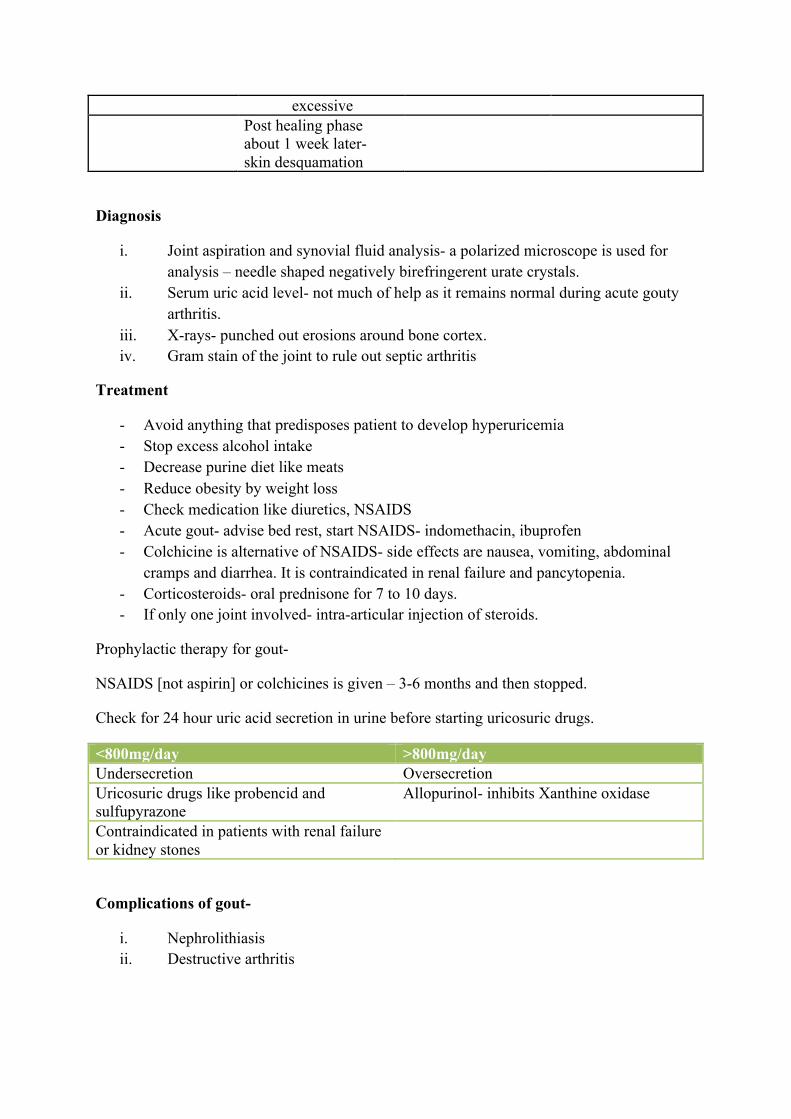
excessive Post healing phase
about 1 week later- skin desquamation
Diagnosis
i. Joint aspiration and synovial fluid analysis- a polarized microscope is used for analysis – needle shaped negatively birefringerent urate crystals.
ii. Serum uric acid level- not much of help as it remains normal during acute gouty arthritis.
iii. X-rays- punched out erosions around bone cortex. iv. Gram stain of the joint to rule out septic arthritis
Treatment
- Avoid anything that predisposes patient to develop hyperuricemia - Stop excess alcohol intake - Decrease purine diet like meats - Reduce obesity by weight loss - Check medication like diuretics, NSAIDS - Acute gout- advise bed rest, start NSAIDS- indomethacin, ibuprofen - Colchicine is alternative of NSAIDS- side effects are nausea, vomiting, abdominal
cramps and diarrhea. It is contraindicated in renal failure and pancytopenia. - Corticosteroids- oral prednisone for 7 to 10 days. - If only one joint involved- intra-articular injection of steroids.
Prophylactic therapy for gout-
NSAIDS [not aspirin] or colchicines is given – 3-6 months and then stopped.
Check for 24 hour uric acid secretion in urine before starting uricosuric drugs.
<800mg/day >800mg/day Undersecretion Oversecretion Uricosuric drugs like probencid and sulfupyrazone
Allopurinol- inhibits Xanthine oxidase
Contraindicated in patients with renal failure or kidney stones
Complications of gout-
i. Nephrolithiasis ii. Destructive arthritis
Pseudogout
- It is the deposition of calcium pyrophosphate crystals inside the joint causing inflammation.
- Seen in older patients with degenerative joint disease. - People at increased risk are those with hemachromatosis, hypothyroidism,
hyperparathyroidism - Diagnosis- joint aspiration. Positively birefringent rod shaped or rhomboid shaped
crystals. - X-rays- cartilage calcification- chondrocalcinosis- white colored rim on bone - Treatment- according to the underlying cause. For symptomatic relief give NSAIDS,
colechicine, intra-articular steroid injection. Joint replacement may be needed.
Shoulder pain evaluation
A patient comes with shoulder pain.
Checking of active and passive movements of cervical vertebrae-
- He is asked by the doctor to bend his head forwards, backwards and side to side. - He is asked to turn the head left and right.
Palpation of cervical vertebrae
- It hurts.
Check the back- active and passive movements
- Bringing both the hands in the front. - Asking to flex forward, backwards and turning on right and left side. - Palpation of the vertebrae from back.
Checking of first and second rib
- Asking to take a deep breath during palpation.
Checking of pectorals
- Pull the right hand back and then left
Check the range of motion of upper body and shoulder muscles
- Ask the patient to lift up both arms [flexion] and then bring them down [extension] - Then the arms should be lifted up from side- abduction and then brought back-
adduction - Then locking of hands at the back- joints undergo internal and external rotation. - Now the doctor will flex, extend, abduct and adduct the arms of the patient. Locking
the arms in the back also and exaggeration of it by the doctor. - Doctor asks the patient to put his fists together in the front. - He pushes the patient down and checks for resistance during abduction, pushes up to
check adduction - Similarly flexion and extension is also checked - Fists are asked to be put on sides to check external rotation by pressure inwards and
internal rotation by pressure outwards.
Empty can test for supra spinatus
- Pressure given downwards and the resistance is checked for supraspinatus
The arms are checked by
- Flexing the arms forward and then returning back by keeping them close to the chest. - Now supination and pronation of arms by the patient and then by the doctor himself.
Now for wrists
- Wrists are flexed, extended and internally rotated and externally rotated. It is called radial deviation and ulnar deviation.
- Now the doctor does the same to understand the strength of flexion and extension on the patient.
Sensory nerve and reflexes
- C5, C6, C7 and T1
Check for reflexes
- Biceps- C5, radialis- C6 and triceps- C7
Spencer test
- Shoulder examination - Make the person lie down. - Check the ribs and the clavicles - Check for internal rotation mainly - Make the person lie down on his side. - Check for flexion, extension, adduction and abduction.

Head and neck physical examination
Patient has sinus pain.
- Ask the patient to bend the head forward and then passively extend the head - As the patient is asked to rotate the head to the right and left and passively acted upon
by the doctor also. - Now the patient’ head is turned from one side to other and checked - He patient has a good range of motion. - Next, the cervical vertebrae are checked C2-C7, - Sinus- check- frontal sinus, maxillary sinus - Lymph nodes- posterior auricular- light to deep palpation, anterior lymph node,
preauricular , submaxillary, submental, sternocleidomastoid muscle- posterior to it are posterior cervical lymph nodes- light to deep palpation, then anterior cervical lymph nodes and supraclavicular lymph nodes.
Ear examination
- Pull the pinna superiorly and posteriorly - Next check nasal sinuses. - Ask the patient to say ‘ah’- check for anterior and posterior faucial pillars and tonsils
Check thorasics
- Ask the patient to put the arms forward and then bend and then backward. Rotate from one side to other. Now side-bend on both the sides.
Check thorasic vertebrae
- Palpate nicely.
Next listen to heart and lungs
- Place the stethoscope on the 2nd intercostal space- falls between the 2nd and 3rd rib to hear S2 sounds. On the other side for pulmonary sounds, then in midsternum for tricuspids, for mitral valve placement on 4th intercostal midclavicular.
- Triangular auscultation- a triangle formed by inferior angle of scapula, medial side of scapula, medial surface of trapezius and base of latissmus dorsi.
- While breathing lung moves from T8 to T10. - Check for rib 1 and rib2.
Check for patient rib function
- Ask the patient to breathe - Check the clavicles. - Flex the sternum.
Crohn’s disease
Another name is regional enteritis.
Definition
It is a chronic trans mural inflammatory disease that can affect any part of the GI tract from mouth to anus. Most commonly affects terminal ileum and cecum. Small intestine= 30%, terminal ileum=40%, colon=25%. More common in Caucasians
Pathology
- The lesions within the bowel are discontinuous skip lesions. - Fistula formation-enteroenteric fistula, enterovesicular fistula-bladder and bowel
connected (bubbles in urine- pneumaturia), fistula connecting bowel and vagina= enterovaginal fistula
- Luminal strictures due to the inflammation of the bowel wall. - Non-caseating granulomas - Creeping fat surrounds the inflamed bowel.
Extra-intestinal manifestation of Crohn’s disease
a. Eyes 1. Episcleritis 2. Anterior uveitis b. Skin
1. Erythema nodosum- painful nodules on their skin which are red in color 2. Pyoderma gangrenosum- huge skin ulcer which does not heal.
c. Arthritis- 1. monoarticular and migratory type 2. ankylosing spondylitis- bamboo spine 3. sacro-iliatis
d. Hypercoagulable state 1. deep venous thrombosis 2. pulmonary embolism 3. stroke
e. osteoporosis f. gall stones [esp. Crohn’s disease] g. primary sclerosing colengitis
Clinical features
1. Non-bloody diarrhea 2. Weight loss and malabsorption 3. Abdominal pain- right lower quadrant mostly 4. Fever, malaise 5. Aphthous oral ulcers
6. Cholelithiasis and nephrolithiasis
They have flare-ups and remissions so they are unpredictable.
Diagnosis
1. Endoscopy- sigmoidoscopy and colonoscopy - Aphthous ulcers – a cobblestone appearance of the bowel wall - Pseudo-polyps or patchy skip-lesions
2. Upper endoscopy
Complications
1. Fistula formation 2. Abscesses inside the GI tract 3. Small bowel obstruction- only reason for surgery 4. Malabsorption of Vit. B12 and bile acids 5. Gall stones- lack of bile acids absorption 6. Nephrolithiasis- Increased oxalate absorption in the colon- calcium bind to form
calcium oxalate stones inside the kidney. 7. Toxic megacolon
Treatment
1. Sulfasalazine- 5-ASA- mesalamine- Block prostaglandins 2. Metronidazole 3. Corticosteroids- systemic prednisone- given in acute exacerbations 4. Immunosuppressive agents like azathioprine or 6, mecaptopurine 5. Bile acid sequesterants- cholestyramine or colestipol 6. Surgical resection-segmental- disease can recur 7. They need a lot of nutritional supplements
Ulcerative colitis
Definition-
It is the Chronic inflammatory disease of the colon or the rectum.
Age-
adolescents, young adults
Site-
Mostly rectal area=10%, rectum+ left colon= 40%, left colon+ right colon, entire colon= 30% [pancolitis], backwash ileitis=10%
Not predictable
Pathology
- No skip lesions. The lesions are continuous. - Limited to mucosa and submucosa - PMNs accumulate in the crypts of the colon. They form crypt abscess.
Clinical presentation
1. Hematochezia/ bloody diarrhea 2. Abdominal pain 3. Frequent bowel movements- small amounts 4. Fever, anorexia, weight loss in severe cases. 5. Tenesmus – rectal dry heaves.
Extra-intestinal
- Pyoderma gangrenosum- skin lesions - Eyes- anterior uveitis - Arthritis- joints
Diagnosis
1. Stool culture- clostridium difficile, ova, parasite 2. Fecal leukocytes- crypt neutrophils are reflected. 3. Colonscopy
Complications
1. Iron deficiency anemia- low ferritin level and iron levels. MCV<70. Microcytic anemia
2. Hemorrhage 3. Dehydrated due to loss of electrolytes 4. Increased risk of developing colon cancer.
5. Primary sclerosing cholengitis- strictures and dilatation in biliary tree. 6. Cholangiocarcinoma- Klatskin tumor if the tumor is in the Y of the biliary tree. 7. Toxic megacolon 8. Depression, narcotic abuse.
Treatment
1. Systemic corticosteroids in case of acute exacerbation. 2. Main drug is sulphasalazine—5ASA, proptysis – 5 ASA enema. 3. Immunosuppressants- Azothiaprine / 6 Mecaptopurine 4. Only cure is total colectomy- then anastomosed to skin.
Polyarthralgia rheumatica
It is common in elderly female patients more than 70 years of age
Cause unknown
Autoimmune process
Genetic predisposition- HLA-DR4 allele
Clinical symptoms-
1. Shoulder and hip pain bilaterally. 2. Morning stiffness is there and worsens without movement. 3. Muscle strength is normal 4. Fever, fatigue, weight loss, malaise and depression 5. Synovitis in knee, wrist- joint swelling. 6. Tenosynovitis- shoulder muscles- SITS- supra spinatus, infraspinatus, teres minor and
subscapular 7. Adhesive capsulitis 8. 10% develop temporal arteritis.
Diagnosis
1. Clinical- bilateral 2. ESR>50
Treatment
1. Corticosteroids 2. Temporary arteritis may cause blindness if not treated.
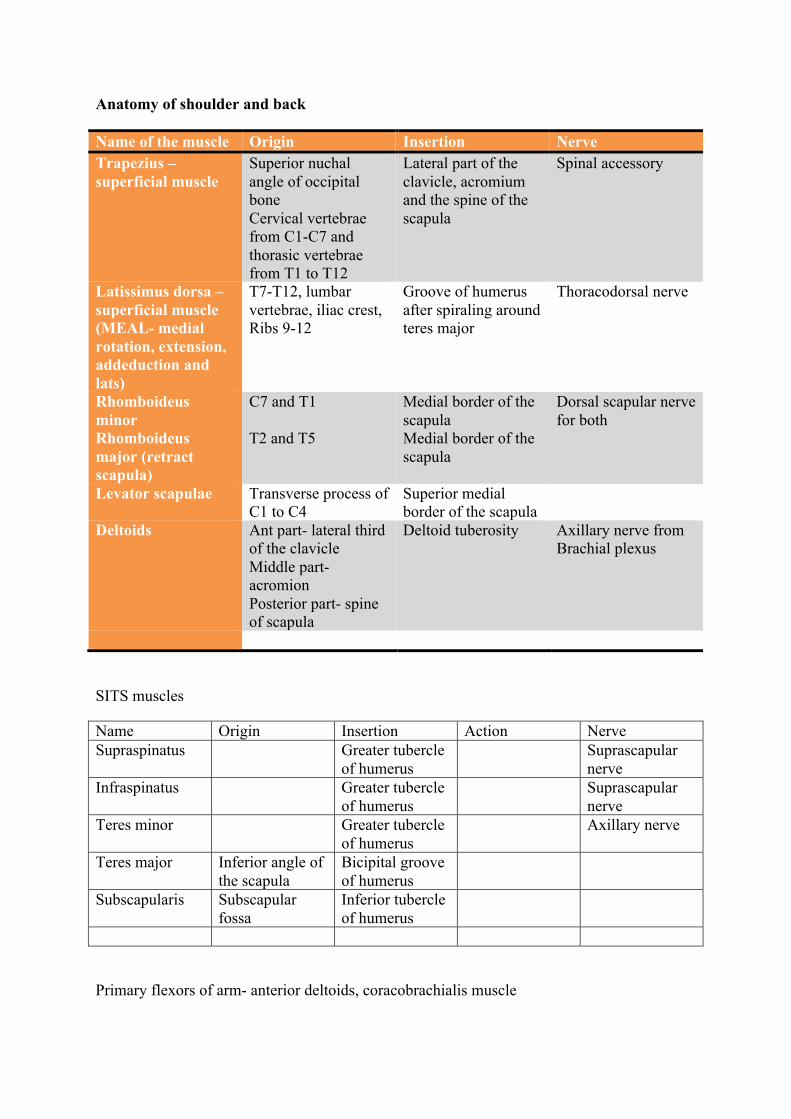
Anatomy of shoulder and back
Name of the muscle Origin Insertion Nerve Trapezius –superficial muscle
Superior nuchal angle of occipital bone Cervical vertebrae from C1-C7 and thorasic vertebrae from T1 to T12
Lateral part of the clavicle, acromium and the spine of the scapula
Spinal accessory
Latissimus dorsa –superficial muscle (MEAL- medial rotation, extension, addeduction and lats)
T7-T12, lumbar vertebrae, iliac crest, Ribs 9-12
Groove of humerus after spiraling around teres major
Thoracodorsal nerve
Rhomboideus minor Rhomboideus major (retract scapula)
C7 and T1 T2 and T5
Medial border of the scapula Medial border of the scapula
Dorsal scapular nerve for both
Levator scapulae Transverse process of C1 to C4
Superior medial border of the scapula
Deltoids Ant part- lateral third of the clavicle Middle part-acromion Posterior part- spine of scapula
Deltoid tuberosity Axillary nerve from Brachial plexus
SITS muscles
Name Origin Insertion Action Nerve Supraspinatus Greater tubercle
of humerus Suprascapular
nerve Infraspinatus Greater tubercle
of humerus Suprascapular
nerve Teres minor Greater tubercle
of humerus Axillary nerve
Teres major Inferior angle of the scapula
Bicipital groove of humerus
Subscapularis Subscapular fossa
Inferior tubercle of humerus
Primary flexors of arm- anterior deltoids, coracobrachialis muscle
Primary extensors of arm- posterior deltoid, latissmus dorsa
Abduction- middle deltoid till 90 degree, supraspinatus for the first 15 degree
Serratus anterior muscle- stabilizes scapula, laterally rotate- origin- medial aspect of scapula, insertion- ribs 5,6,7 & 8. Nerve – long thorasic nerve
Primary adductors- subscapularis muscle
Adduction- pectoral muscles- nerve- axillary nerve - FAM- flexion, adduction and medial rotation
Internal rotation- pectorals and latissmus
External rotation- infraspinatus and pect minor
Teres major- nerve- subscapular nerve
Rheumatoid arthritis
Definition
It is the chronic inflammatory autoimmune disease of the synovium.
Cause
Unknown
Age of onset-
Females of 20 to 40 years of age.
Pathogenesis
- Foreign body- genetic predisposition. - Fb activate CD4 helper Tcells- which in turn activate plasma cells- antibodies like
IgM- attach and attack to Fc part of IgG antibodies- this complex is called Rheumatoid factor(RF)
- It cause inflammation- chronic inflammatory synovitis - Pannus formation- destruction of cartilage, edgy bone - Increased synovial fluid in the joint space.
Clinical features
- Symmetrical inflammatory arthritis- DIP (distal interphalangeal joint) remains untouched.
- It affects PIP (proximal interphalangeal joint) and MCP (metacarpal phalangeal ) - Morning stiffness due to PM - PIP and MCP affected. - Fever, weight loss, fatigue - Hand deformities- ulnar deviation, Boutonniere’s deformity (PIP is flexed and DIP is
hyper-extended), swan-neck deformity also called the Z-arm (MCP is flexed, PIP is hyperextended and DIP is flexed)
- Cervical spine (C1-C2) is affected in case of rheumatoid arthritis.- ca develop subluxation. Before surgery make sure you do a cervical xray.
Different organs affected-
1. Skin - Subcutaneous nodules present on elbow, occiput, sacrum- classic rheumatoid nodules - Tend to bruise easily as it is thin and atrophic - Ulcers around their hands due to poor blood flow. 2. Heart - Pericardium affected- pericarditis- chest pain due to that especially during bending
front. - Pericardiac effusion. - Predisposed to develop bundle branch blocks
3. Lungs - Pleural effusion- low glucose - Pleuritis - Pulmonary fibrosis- interstitial lung disease - Honeycomb pattern on chest xray 4. Eyes - Scleritis - Scleromalacia- soft sclera- can get perforated and go blind - Dry eyes- Sjogren’s syndrome - Mononeuritis multiplex – infarction of the nerve trunks 5. Blood vessels - Microvascular vasculitis
Felty syndrome
1. Neutropenia 2. Rheumatoid arthritis 3. Splenomegaly
Blood cells
- Low platelets - Lymphadenopathy - Anemia
Diagnosis
1. Rheumatoid factor titre- 80% will have high RF level. It is a non specific test. 2. ESR and CRP- high 3. Anemia of chronic disease- normocytic and normochromic 4. Xrays- bone loss at the finger joints, cartilage eroded, narrowing of the joint space,
bone erosions, a lot of synovial fluid in joint space. 5. Synovial fluid analysis- non-specific- cloudy yellow fluid- WBC>5000 /mm3
Treatment
1. Slow down or prevent bone destruction 2. Watch out for toxicity 3. Exercise- for mobility 4. Pain control- NSAIDS 5. Low dose short term corticosteroids 6. DMARDS- disease modifying anti rheumatoid arthritis drugs- reduce the morbidity
and mortality of the patient.- 6 weeks to work a. Methotrexate- can cause GI ulcers/upset, bone marrow suppressant,
hepatotoxicity, pulmonary fibrosis.

Check renal function and LFT b. Hydroxychloroquine- ADR- vision loss due to retinopathy so carry out eye
examination once in every 6 months. c. Sulfasalazine
All of them require folate replacement.
Second line of drugs- C the GAP 1. Gold 2. Azathioprine 3. Pencillamine 4. Cyclosporine
Last resort- synovectomy or joint replacement therapy
Scleroderma (systemic sclerosis)
Definition-‐ It is a connective tissue disorder in which collagen is involved causing widespread fibrosis.
Pathogenesis
Fibroblasts stimulated by cytokines-‐ excess production of collagen fibers-‐ women of 35-‐50 years old.
Types
Diffuse Limited Skin-‐ Raynaud’s phenomenon Face, neck and distal extremities Cutaneous fibrosis-‐ claw hands-‐ sclerodactyly Facial contractions and claw hands GI tract-‐ develop vomiting from acid reflux, develop dysphagia, delayed gastric emptying, constipation, diarrhea, esophageal strictures( secondary to excess acid reflux)
Raynaud’s phenomenon-‐ digital ischemia
Lungs-‐ pulmonary hypertension. It can be the major cause of death
Pulmonary hypertension
Heart-‐ pericardial effusion, congestive heart failures, arrhythmias Kidneys-‐ rapid malignant hypertension-‐ today it is rare due to ACE inhibitors
Better prognosis than diffuse CREST syndrome Calcinosis Raynaud’s phenomenon Esophageal dysmotility Sclerodactyly Telangictasis
Diagnosis-‐ ANA-‐ elevated Increased anti-‐topomerase 1. Also called anti-‐scl 70 Check barium swallow and pulmonary function test-‐ restrictive pattern as it s ILD
ANA-‐elevated Anti centromere antibody-‐ specific to limited
A certain % of people with scleroderma can have Sjogren’s syndrome.
Treatment
-‐ No cure -‐ NSAIDS for joint pain -‐ H2 blockers or proton pump inhibitors for acid reflux-‐ drugs like omeprazole, cimetidine -‐ Raynaud’s phenomenon-‐ stop smoking, avoid cold, stay warm, calcium channel blockers in
severe cases -‐ Kidneys-‐ lisinopril-‐ ACE inhibitor – to prevent renal hypertension.
Idiopathic inflammatory myopathies
Polymyositis and dermatomyositis
Cause- viral infection or autoimmune. Actual cause is unknown. Genetic susceptibility is there. Immune system is activated which causes chronic inflammation.
Occurrence- mostly in females, rare form in males- inclusion body myositis- distal muscle weaknesses, no autoantibody, low creatinine levels.
Clinical features
-‐ Symmetrical proximal muscle involvement- weakness. – shoulder girdle, pelvic muscles, neck flexors
-‐ Myalgia- -‐ Dysphagia – esophageal muscles affected
Skin rash- dermatomyositis
1. Heliotrope rash- butterfly rash- Around the eyes, bridge of the nose, cheeks- redness and erythema
2. Gotrons papules- MCP, PIP, DIP- affected- red scaly rash. They show a V sign on the front or back of their neck. It is called as the Shawl sign
3. Periungal telangiectasias 4. Arthralgias- joint pain 5. They are at an increased risk of cancer- lung, breast, GI, ovarian, myeloproliferative disorder
Diagnosis
1. CPK- creatinine kinase level is elevated in muscle damage cases, LDH, Aldosterone, AST/ALT-elevated
2. ANA levels high in 50% of the patients. 3. Anti-synthetase antibody/ antiJo-1 antibody 4. Anti-signal recognition particle- worst prognosis if positive 5. Anti-MI2 antibody- good prognosis if positive 6. EMG- 7. Muscle biopsy- best by far. Inflammation around the muscle fibres, lymphocytes
Treatment
1. Corticosteroids 2. Methotrexate, cyclophosphamide, chloramloncil - immunosuppressive agent 3. Physical therapy
Ankylosing spondylitis
Seronegative spondyloarthropathies
- No rheumatoid factor ( anti IgG antibodies) - HLA-B27 (gene for HLA MCH1) - PAIR - Psoriasis arthritis - Ankylosing spondylosis - Inflammatory bowel disease - Reactive arthritis/ Reiter’s syndrome - Common factor for PAIR
i. Asymmetrical oligo-arthritis. ii. Enthesitis – inflammation in the area where tendon meets the bone iii. Inflammatory arthritis- sacro-iliac joint iv. Genetically linked
Ankylosing spondylitis
- Males (HLA-B27) - Bilateral sacroilitis - It starts at a very young age. - Gradually the spine starts fusing- from lumbar to cervical - There may be acute exacerbation
Clinical features
- Lower back pain - Neck pain - Morning stiffness which gets better by exercise. - Enthesitis- tendon of the supraspinatus muscle that goes and inserts into the head of
the humerus, cheilius tendon that attaches to the calcaneous. - Limited spinal movements due to fused spine so prone to fractures even by a small
trauma. - Chest pain due to limited mobility of spine. - Shoulder pain, hip pain - Fever- low grade and weight loss
Extra-articular events
- Anterior uveitis or iridocyclitis
Diagnosis
1. Imaging- X-ray plain film, MRI, CT scan of lumbar and pelvis, 2. Sacral-iliatis 3. Bamboo spine
4. ESR- just let you know about inflammation 5. HLA-B27- not required as such
Treatment
1. NSAIDS- indomethacin 2. Maintain good posture 3. Physical therapy
Warning
Immobilize the neck with C collar to prevent injury to spinal cord.
Complications
1. Restrictive lung disease – FEV1:FVC ratio is increased or normal 2. They may develop Cauda Equina syndrome. 3. More prone to spinal fracture + osteoporosis

Psoaritic arthritis
- 10% of psoarisis patients affected. Gradual onset of arthritis. - Joints affected-upper extremities - Asymmetrical and polyarticular - Treatment by NSAIDS for pain control.
Inflammatory bowel disease
- Ulcerative colitis - Crohn’s disease
Reactive arthritis
Definition
It is an asymmetric inflammatory arthritis of the upper and the lower extremities where the lower ones are affected more.
It is preceded by infection and starts after 4 or 6 weeks.
The infection can be genitourinary (2) of gastrointestinal infection (1,3,4,5) which are namely-
1. Salmonella 2. Chlamydia 3. Campylobacter 4. Yersinia 5. Shigella
Reiter’s syndrome- can’t see, can’t pee, can’t climb a tree
1. Conjunctivitis 2. Urethritis 3. Arthritis
Symptoms
1. Asymmetrical joint pain- Effusion and no mobility 2. Check for previous GI/GU infections 3. Fever, weight loss and fatigue
Diagnosis
1. Synovial fluid analysis- rule out crystals as in gouty arthritis and septic joint.
Treatment
NSAIDS- IST TIME
Immunosuppressive agents- sulfasalazine or azothioprine
Sjogren’s syndrome
- Autoimmune disease - Lacrimal gland, parotid gland affected- destruction of the glands due to lymphocytic
infiltration - Dry eyes, dry mouth- primary Sjogren’s syndrome - Secondary Sjogren’s syndrome- lupus, rheumatoid arthritis, systemic sclerosis,
polymyositis- other rheumatological disease. Dry eyes, dry mouth + any of the above mentioned disease.
- Increased risk of developing non-Hodgkin’s lymphoma- can cause death.
Symptoms-
- Redness, burning sensation in eyes - Blurring of vision - Dry eyes + dry mouth - Arthralgias - Fatigue - Intestinal nephritis, vasculitis and chronic arthritis.
Diagnosis
1. ANA=anti nuclear antibodies-it is not specific as such but 95% of patient show positive ANA
2. Rheumatoid factor is positive 3. Anti Ro (SS-A) or anti La (SS-B)- those with positive anti Ro have higher risk of
developing neonatal lupus. 4. Increased ESR 5. Leucopenia 6. Normocytic, normochromic anemia
Treatment
- Pilocarpine- increase secretions – saliva + tears - Artificial tears - Good oral hygiene - NSAIDS for arthralgia/arthritis
Systemic Lupus Erythematosus
Definition- It is an autoimmune disease
Cause- unknown. Sometimes genetic component, environmental factors
Pathophysiology- antibodies binds to the double stranded DNA- compliments attracted –C3 activation- neutrophils are attracted.
IgG+C3 complex causes inflammation= pain+redness
Race- African Americans are most common patients. Always women at 20’s to 30’s.
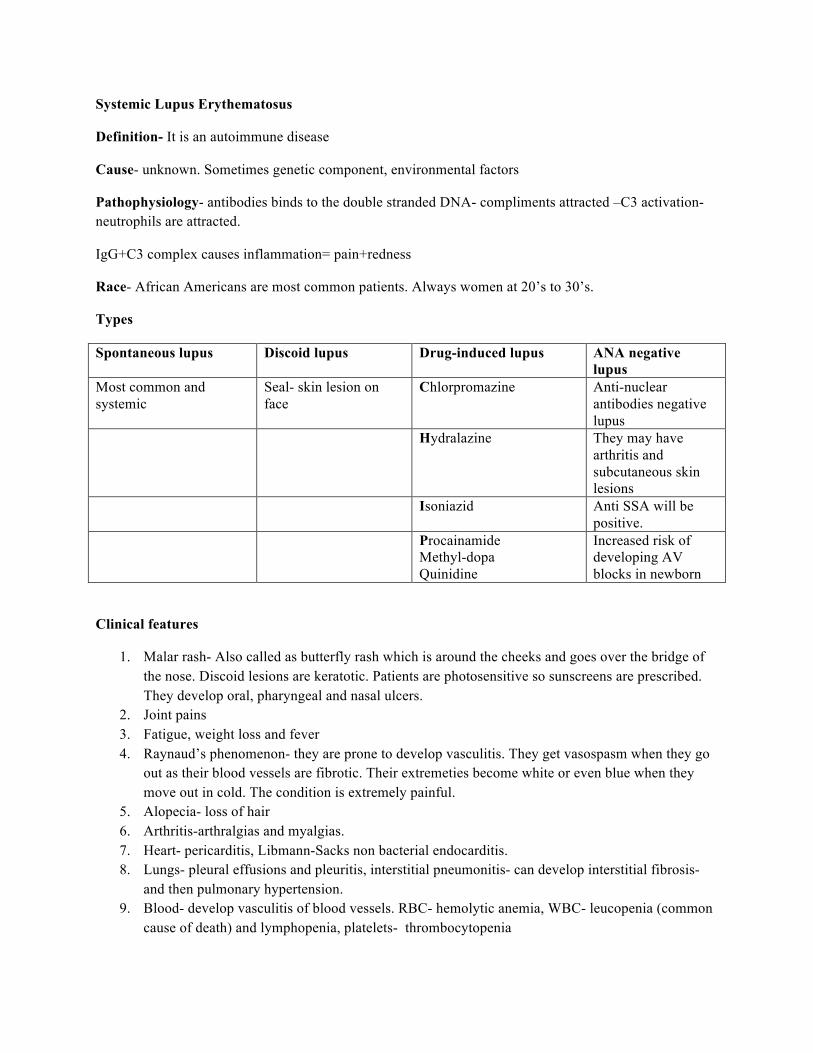
Types
Spontaneous lupus Discoid lupus Drug-induced lupus ANA negative lupus
Most common and systemic
Seal- skin lesion on face
Chlorpromazine Anti-nuclear antibodies negative lupus
Hydralazine They may have arthritis and subcutaneous skin lesions
Isoniazid Anti SSA will be positive.
Procainamide Methyl-dopa Quinidine
Increased risk of developing AV blocks in newborn
Clinical features
1. Malar rash- Also called as butterfly rash which is around the cheeks and goes over the bridge of the nose. Discoid lesions are keratotic. Patients are photosensitive so sunscreens are prescribed. They develop oral, pharyngeal and nasal ulcers.
2. Joint pains 3. Fatigue, weight loss and fever 4. Raynaud’s phenomenon- they are prone to develop vasculitis. They get vasospasm when they go
out as their blood vessels are fibrotic. Their extremeties become white or even blue when they move out in cold. The condition is extremely painful.
5. Alopecia- loss of hair 6. Arthritis-arthralgias and myalgias. 7. Heart- pericarditis, Libmann-Sacks non bacterial endocarditis. 8. Lungs- pleural effusions and pleuritis, interstitial pneumonitis- can develop interstitial fibrosis-
and then pulmonary hypertension. 9. Blood- develop vasculitis of blood vessels. RBC- hemolytic anemia, WBC- leucopenia (common
cause of death) and lymphopenia, platelets- thrombocytopenia
10. Kidney- glomerulonephritis, proteinuria (>0.5g/day), hematuria, azotenia (increased BUN/creatnine ratio), cellular casts in urine
11. CNS- develop seizures, headaches, psychosis, depression 12. Transient ischemic attack or stroke (CVA) 13. GI tract- nausea, vomiting, dysphagia, peptic ulcer disease. Can develop Sjogren’s syndrome.
Diagnosis
1. Antinuclear antibody of serum- sensitive but not specific- elevated levels then chances for lupus 2. False VDRL/ RPR test for syphilis- positive- it is due to the presence of anticardiolipin 3. Anti double-stranded DNA antibody test- specific to lupus- not sensitive. 4. Anti-Smith antibody posistive- definite diagnosis 5. Anti-SS DNA- 70% 6. Anti-histamine antibodies- drug induced lupus if positive 7. Anti-Ro (SS-A): La(SS-B)- sjogren’s syndrome, neonatal lupus (AV block/ transposition of great
vessels, ASDs or VSDs), low complement levels (C2/C4) 8. Check for CBC 9. Renal function test 10. Urinalysis – casts, hematuria
Diffuse proliferative glomerulonephritis is usually a type IV- almost developing renal failure
TYPE V- lupus- common cause of renal failure
11. Anticardiolipin+ lupus anticoagulant test – -‐ Antiphospholipid antibody syndrome -‐ hypercoagulable state-. It is associated with lupus, scleroderma, -‐ Deep venous thrombosis- increased risk of pulmonary embolism. Recurrent arterial
thrombosis- recurrent miscarriages. -‐ Thrombocytopenia, levidoreticularis
Labs
-‐ PTT prolonged -‐ Warfarin given
Treatment
-‐ Long term anticoagulation to keep INR within 2.5-3.5
Treatment modalities
1. Prevention- decrease sun exposure, by wearing sunscreen 2. Pain control –mild cases- NSAIDS 3. Local/systemic corticosteroids- prednisone in acute cases 4. Hydroxychloroquine- for skin, joint and constitutional symptoms. 5. Cyclophosphamide- lupus glomerulonephritis (mesna) 6. Monitor- kidney function and hypertension

7. Patients die due to renal failure, opportunistic infections
Vasculitis
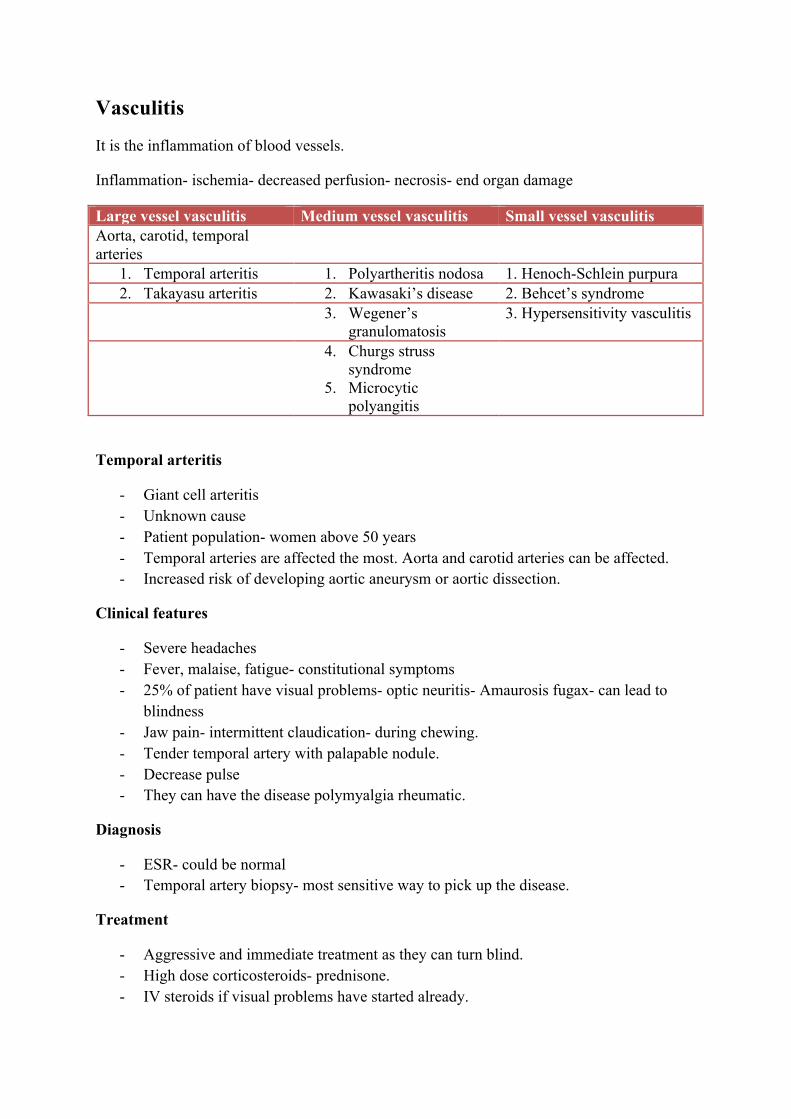
It is the inflammation of blood vessels.
Inflammation- ischemia- decreased perfusion- necrosis- end organ damage
Large vessel vasculitis Medium vessel vasculitis Small vessel vasculitis Aorta, carotid, temporal arteries
1. Temporal arteritis 1. Polyartheritis nodosa 1. Henoch-Schlein purpura 2. Takayasu arteritis 2. Kawasaki’s disease 2. Behcet’s syndrome
3. Wegener’s granulomatosis
3. Hypersensitivity vasculitis
4. Churgs struss syndrome
5. Microcytic polyangitis
Temporal arteritis
- Giant cell arteritis - Unknown cause - Patient population- women above 50 years - Temporal arteries are affected the most. Aorta and carotid arteries can be affected. - Increased risk of developing aortic aneurysm or aortic dissection.
Clinical features
- Severe headaches - Fever, malaise, fatigue- constitutional symptoms - 25% of patient have visual problems- optic neuritis- Amaurosis fugax- can lead to
blindness - Jaw pain- intermittent claudication- during chewing. - Tender temporal artery with palapable nodule. - Decrease pulse - They can have the disease polymyalgia rheumatic.
Diagnosis
- ESR- could be normal - Temporal artery biopsy- most sensitive way to pick up the disease.
Treatment
- Aggressive and immediate treatment as they can turn blind. - High dose corticosteroids- prednisone. - IV steroids if visual problems have started already.
- Check ESR during treatment to know if the corticosteroids are working or not.
Takayasu’s arteritis
- Found in Asian women, - Aortic arch, major branches- subclavian, carotid, - Stenosis of blood vessels - Diagnosis by arteriogram
Clinical features
- Fever, night sweats, malaise, arthralgia, fatigue - Tenderness on the area involved. - Los of radial, ulnar or carotid pulses. - Aortic regurgitation - Stroke, aortic aneurysm, limb ischemia
Treatment
- Steroids - Angioplasty- surgery- a stent placed to maintain patency of the blood vessel.
Churg-Struss syndrome
- Medium vessel vasculitis - Affects many organs- lungs, heart, GI, kidney and skin
Symptoms-
- Shortness of breath- dyspnoea-asthma - Fever, fatigue, weight loss - Skin nodules with palpable purpura
Diagnosis
- Biopsy-lung/skin- eosinophils - P-ANCA[ anti neutrophil cytoplasmic antibody] - Poor prognosis
Treatment
- Steroids
Wegener’s granulomatosus

- Kidney and upper and lower respiratory tract involvement
Symptoms-
- Sinusitis - Bloody or purulent nasal discharge. - Oral ulcers - Cough, hemoptysis, dyspnoea - Rapidly progressing glomerulonephritis - Conjunctivitis/scleritis - Tracheal stenosis
Diagnosis
1. Chest Xray- nodules/infiltrate 2. ESR- elevated 3. Positive C-ANCA 4. Open lung biopsy
Treatment
1. Corticosteroids +Cyclophosphamide 2. Kidney transplant in case of end stage renal failure.
Polyarteritis nodosa (PAN)
- Affects nervous system and GI - Associated with HepB, HIV, drug reactions
Pathophysiology
Decrease in the size of lumen- fibrinoid necrosis- ischemia due to decreased blood flow
Symptoms
- Fever, weakness, weight loss- constitutional symptoms - Abdominal pain - Myalgia - Bowel angina- due to ischemia - Hypertension - Levido reticularis, mononeuritis multiplex
Diagnosis
- Biopsy - ESR - P-ANCA positive - Test for fecal occult blood
Treatment
- Corticosteroids or cyclophosphamide
Behcet’s syndrome
- Recurrent mouth and genital ulcers - Very painful - Arthritis (knees and ankles) - Autoimmune disease - Vasculitic syndrome 1. Eye involvement- conjunctivitis, optic neuritis 2. CNS problems- meningoencephalitis, intracranial hypertension
Diagnosis
Biopsy
Treatment – steroids
Buerger’s disease
- Smokers – young men who smoke cigarettes - Decreased perfusion- necrosis of arm and legs - Limb ischemia and amputation
Symptoms
- painful digital extremities - Cold - Cyanotic - Tingling and numbness - Ulcerations of digits
Treatment
- Stop smoking- prevent the progression of the disease.