fractional flow reserve clinical study commitment · pdf filefractional flow reserve clinical...
TRANSCRIPT
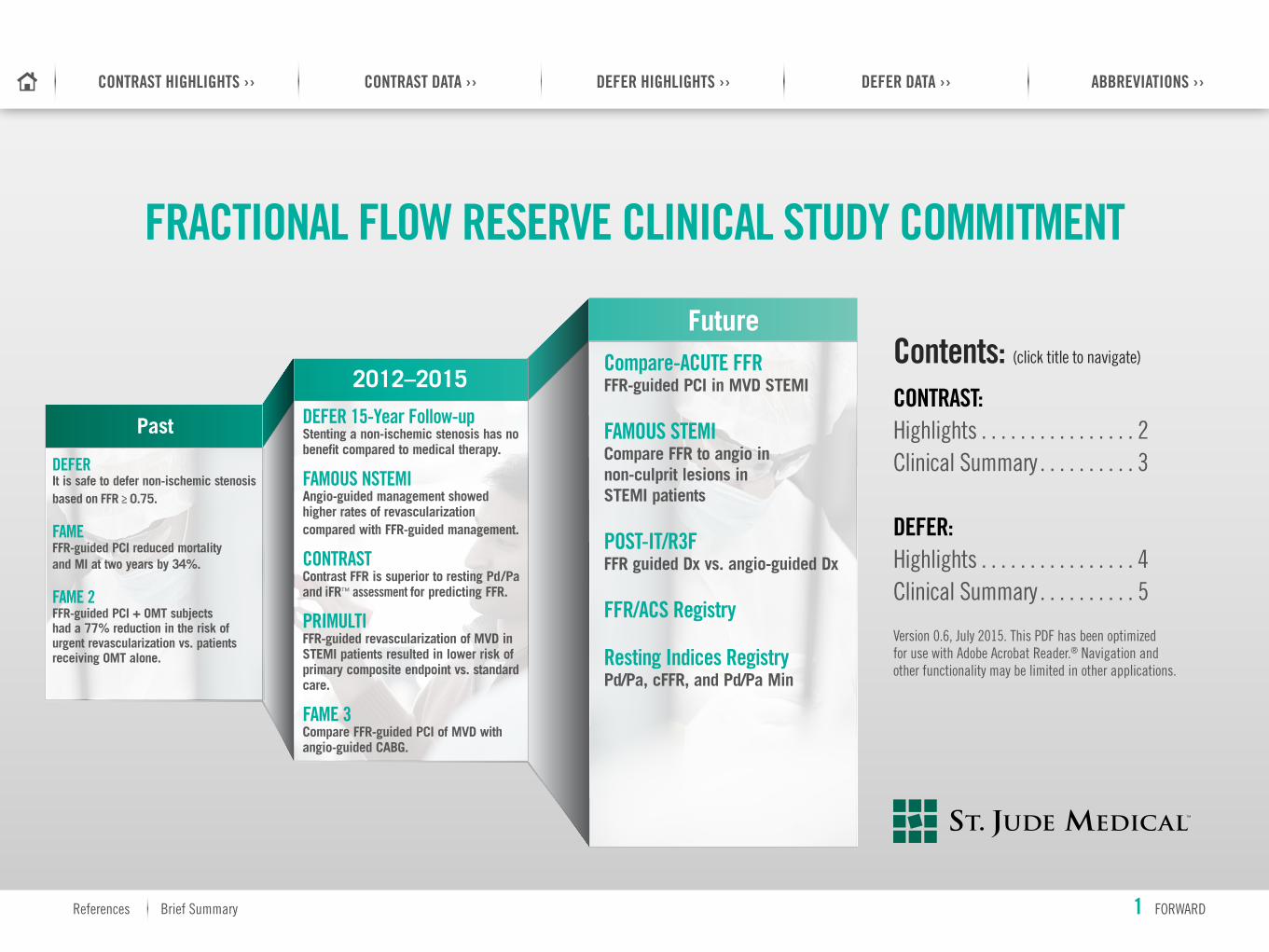
FRACTIONAL FLOW RESERVE CLINICAL STUDY COMMITMENT
Contents: (click title to navigate)
CONTRAST: Highlights . . . . . . . . . . . . . . . . 2 Clinical Summary . . . . . . . . . . 3 DEFER: Highlights . . . . . . . . . . . . . . . . 4 Clinical Summary . . . . . . . . . . 5
Version 0 .6, July 2015 . This PDF has been optimized for use with Adobe Acrobat Reader .® Navigation and other functionality may be limited in other applications .
2012–2015
Future
Past
DEFERIt is safe to defer non-ischemic stenosis based on FFR ≥ 0.75.
FAMEFFR-guided PCI reduced mortality and MI at two years by 34%.
FAME 2FFR-guided PCI + OMT subjects had a 77% reduction in the risk of urgent revascularization vs. patients receiving OMT alone.
DEFER 15-Year Follow-up Stenting a non-ischemic stenosis has no benefit compared to medical therapy.
FAMOUS NSTEMI Angio-guided management showed higher rates of revascularization compared with FFR-guided management.
CONTRAST Contrast FFR is superior to resting Pd/Pa and iFR™ assessment for predicting FFR.
PRIMULTI FFR-guided revascularization of MVD in STEMI patients resulted in lower risk of primary composite endpoint vs. standard care.
FAME 3 Compare FFR-guided PCI of MVD with angio-guided CABG.
Compare-ACUTE FFR FFR-guided PCI in MVD STEMI
FAMOUS STEMI Compare FFR to angio in non-culprit lesions in STEMI patients
POST-IT/R3F FFR guided Dx vs. angio-guided Dx
FFR/ACS Registry
Resting Indices Registry Pd/Pa, cFFR, and Pd/Pa Min
References Brief Summary
CONTRAST DATA ››CONTRAST HIGHLIGHTS ›› DEFER HIGHLIGHTS ›› DEFER DATA ›› ABBREVIATIONS ››
1 FORWARD

CLINICAL HIGHLIGHTS FROM THE CONTRAST STUDY1
Hyperemic FFR remains the reference standard for diagnostic accuracy.
Contrast FFR is superior to resting Pd/Pa and iFR™ assessment for predicting FFR.
Resting Pd/Pa and iFR™ assessment provide equivalent diagnostic accuracy.
#1 #2 #3
65%
80%
85%
85-95%
100%
Angio Alone6
Contrast FFR1
Hybrid Approach 2-5
FFR (IV/IC Adenosine†)
Pd/Pa and iFR™ Single Cutoff2,4
DIAG
NOST
IC AC
CURA
CY
0
20
40
60
80
100
RESOLVE2 ADVISE II3,4
Accu
racy
Com
pare
d to
FFR
(%)
VERIFY 27 CONTRAST 1
Pd/Pa iFR™ Assessment
100 90 10080 806040200
0 0
20 20
40 40
60 60
80 80
100 100
Binary Approach1 = No Adenosine Used
Hybrid Approach1 = Selective Adenosine Used
True
Pos
itive
s (%
)
False Positives (%)
Contrast FFR = 0.929
Contrast FFR
iFR™ Assessment
= 0.879iFR™
Assessment
Pd/Pa = 0.874 Pd/Pa
Accuracy (%)
Free
dom
from
Ade
nosin
e (%
)
†Prior to using hyperemic agents, please review the Instructions for Use for a complete listing of indications, contraindications, warnings, precautions, potential adverse events and directions.References Brief Summary
CONTRAST DATA ››CONTRAST HIGHLIGHTS ›› DEFER HIGHLIGHTS ›› DEFER DATA ›› ABBREVIATIONS ››
BACK 2 FORWARD
CONTRAST HIGHLIGHTS
Quality assessment, then: Pd/Pa, iFR™ assessment,
cFFR, FFR
Tracings blinded and sent to central
CRF core lab
Rest, IC contrast, IC adenosine, IV adenosine
(each repeated), plus drift check
750 patients undergoing clinical
FFR assessment
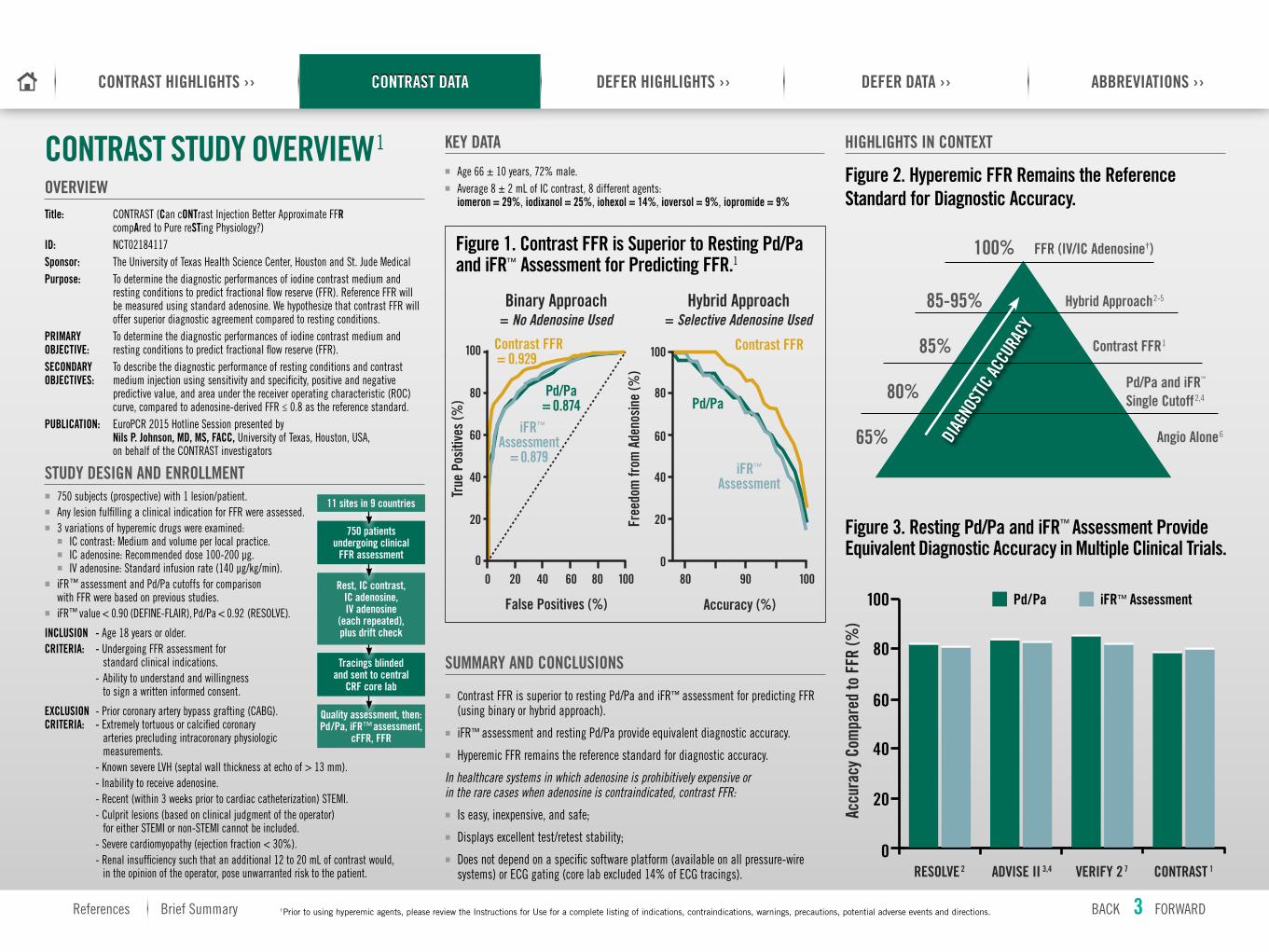
OVERVIEWTitle: CONTRAST (Can cONTrast Injection Better Approximate FFR compAred to Pure reSTing Physiology?)ID: NCT02184117Sponsor: The University of Texas Health Science Center, Houston and St . Jude MedicalPurpose: To determine the diagnostic performances of iodine contrast medium and resting conditions to predict fractional flow reserve (FFR) . Reference FFR will be measured using standard adenosine . We hypothesize that contrast FFR will offer superior diagnostic agreement compared to resting conditions .PRIMARY To determine the diagnostic performances of iodine contrast medium and OBJECTIVE: resting conditions to predict fractional flow reserve (FFR) .SECONDARY To describe the diagnostic performance of resting conditions and contrast OBJECTIVES: medium injection using sensitivity and specificity, positive and negative predictive value, and area under the receiver operating characteristic (ROC) curve, compared to adenosine-derived FFR ≤ 0 .8 as the reference standard .PUBLICATION: EuroPCR 2015 Hotline Session presented by Nils P. Johnson, MD, MS, FACC, University of Texas, Houston, USA, on behalf of the CONTRAST investigators
STUDY DESIGN AND ENROLLMENT�� 750 subjects (prospective) with 1 lesion/patient .�� Any lesion fulfilling a clinical indication for FFR were assessed .�� 3 variations of hyperemic drugs were examined:�� IC contrast: Medium and volume per local practice .�� IC adenosine: Recommended dose 100-200 μg .�� IV adenosine: Standard infusion rate (140 μg/kg/min) .
�� iFR™ assessment and Pd/Pa cutoffs for comparison with FFR were based on previous studies .
�� iFR™ value < 0 .90 (DEFINE-FLAIR), Pd/Pa < 0 .92 (RESOLVE) .
INCLUSION - Age 18 years or older .CRITERIA: - Undergoing FFR assessment for standard clinical indications . - Ability to understand and willingness to sign a written informed consent .
EXCLUSION - Prior coronary artery bypass grafting (CABG) .CRITERIA: - Extremely tortuous or calcified coronary arteries precluding intracoronary physiologic measurements . - Known severe LVH (septal wall thickness at echo of > 13 mm) . - Inability to receive adenosine . - Recent (within 3 weeks prior to cardiac catheterization) STEMI . - Culprit lesions (based on clinical judgment of the operator) for either STEMI or non-STEMI cannot be included . - Severe cardiomyopathy (ejection fraction < 30%) . - Renal insufficiency such that an additional 12 to 20 mL of contrast would, in the opinion of the operator, pose unwarranted risk to the patient .
CONTRAST STUDY OVERVIEW1 KEY DATA
�� Age 66 ± 10 years, 72% male .�� Average 8 ± 2 mL of IC contrast, 8 different agents:
iomeron = 29%, iodixanol = 25%, iohexol = 14%, ioversol = 9%, iopromide = 9%
HIGHLIGHTS IN CONTEXT
SUMMARY AND CONCLUSIONS
�� Contrast FFR is superior to resting Pd/Pa and iFR™ assessment for predicting FFR (using binary or hybrid approach) .
�� iFR™ assessment and resting Pd/Pa provide equivalent diagnostic accuracy .
�� Hyperemic FFR remains the reference standard for diagnostic accuracy .
In healthcare systems in which adenosine is prohibitively expensive or in the rare cases when adenosine is contraindicated, contrast FFR:
�� Is easy, inexpensive, and safe;
�� Displays excellent test/retest stability;
�� Does not depend on a specific software platform (available on all pressure-wire systems) or ECG gating (core lab excluded 14% of ECG tracings) .
11 sites in 9 countries
Figure 1. Contrast FFR is Superior to Resting Pd/Pa and iFR™ Assessment for Predicting FFR.1
Figure 3. Resting Pd/Pa and iFR™ Assessment Provide Equivalent Diagnostic Accuracy in Multiple Clinical Trials.
0
20
40
60
80
100
RESOLVE 2 ADVISE II 3,4
Accu
racy
Com
pare
d to
FFR
(%)
VERIFY 2 7 CONTRAST 1
Pd/Pa iFR™ Assessment
Figure 2. Hyperemic FFR Remains the Reference Standard for Diagnostic Accuracy.
65%
80%
85%
85-95%
100%
Angio Alone6
Contrast FFR1
Hybrid Approach2-5
FFR (IV/IC Adenosine†)
DIAG
NOST
IC AC
CURA
CY
Pd/Pa and iFR™ Single Cutoff2,4
†Prior to using hyperemic agents, please review the Instructions for Use for a complete listing of indications, contraindications, warnings, precautions, potential adverse events and directions.
100 90 10080 8060402000 0
20 20
40 40
60 60
80 80
100 100
Binary Approach = No Adenosine Used
Hybrid Approach = Selective Adenosine Used
True
Pos
itive
s (%
)
False Positives (%)
Contrast FFR = 0.929
Contrast FFR
iFR™ Assessment
= 0.879iFR™
Assessment
Pd/Pa = 0.874 Pd/Pa
Accuracy (%)
Free
dom
from
Ade
nosin
e (%
)
References Brief Summary
CONTRAST DATA ››CONTRAST HIGHLIGHTS ›› DEFER HIGHLIGHTS ›› DEFER DATA ›› ABBREVIATIONS ››
BACK 3 FORWARD
CONTRAST DATA
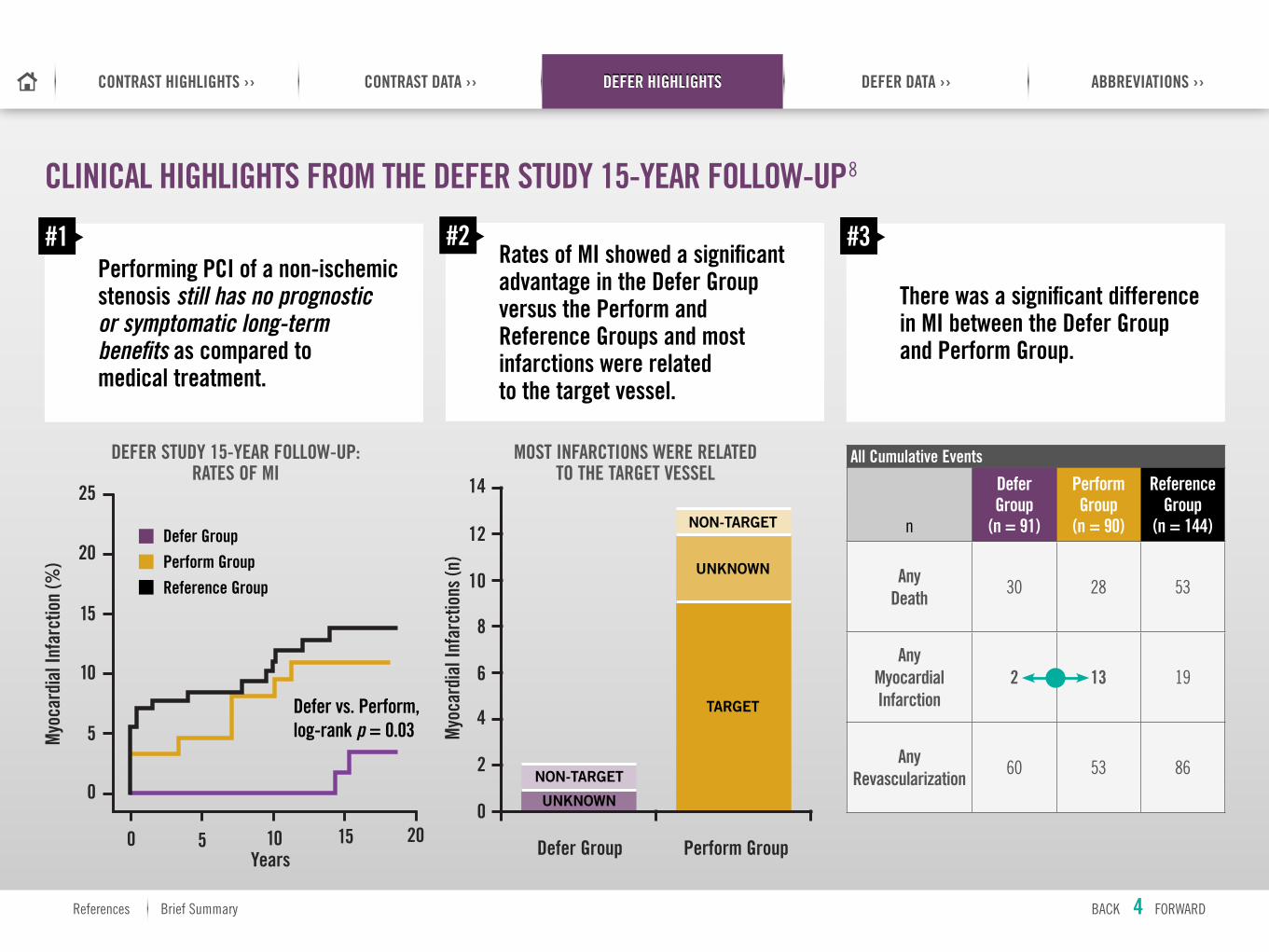
CLINICAL HIGHLIGHTS FROM THE DEFER STUDY 15-YEAR FOLLOW-UP8
Performing PCI of a non-ischemic stenosis still has no prognostic or symptomatic long-term benefits as compared to medical treatment.
#1Rates of MI showed a significant advantage in the Defer Group versus the Perform and Reference Groups and most infarctions were related to the target vessel.
#2
There was a significant difference in MI between the Defer Group and Perform Group.
#3
All Cumulative Events
n
Defer Group
(n = 91)
Perform Group
(n = 90)
Reference Group
(n = 144)
Any Death 30 28 53
Any Myocardial Infarction
2 13 19
Any Revascularization 60 53 86
14
12
10
8
6
4
2
0
Myo
card
ial I
nfar
ctio
ns (n
)
Defer Group Perform Group
TARGET
UNKNOWN
UNKNOWN
NON-TARGET
NON-TARGET
DEFER STUDY 15-YEAR FOLLOW-UP: RATES OF MI
MOST INFARCTIONS WERE RELATED TO THE TARGET VESSEL
Defer GroupPerform GroupReference Group
Defer vs. Perform, log-rank p = 0.03
0
25
20
15
10
5
0
5 10 15 20
Myo
card
ial I
nfar
ctio
n (%
)
Years
References Brief Summary
CONTRAST DATA ››CONTRAST HIGHLIGHTS ›› DEFER HIGHLIGHTS ›› DEFER DATA ›› ABBREVIATIONS ››
BACK 4 FORWARD
DEFER HIGHLIGHTS
OVERVIEW
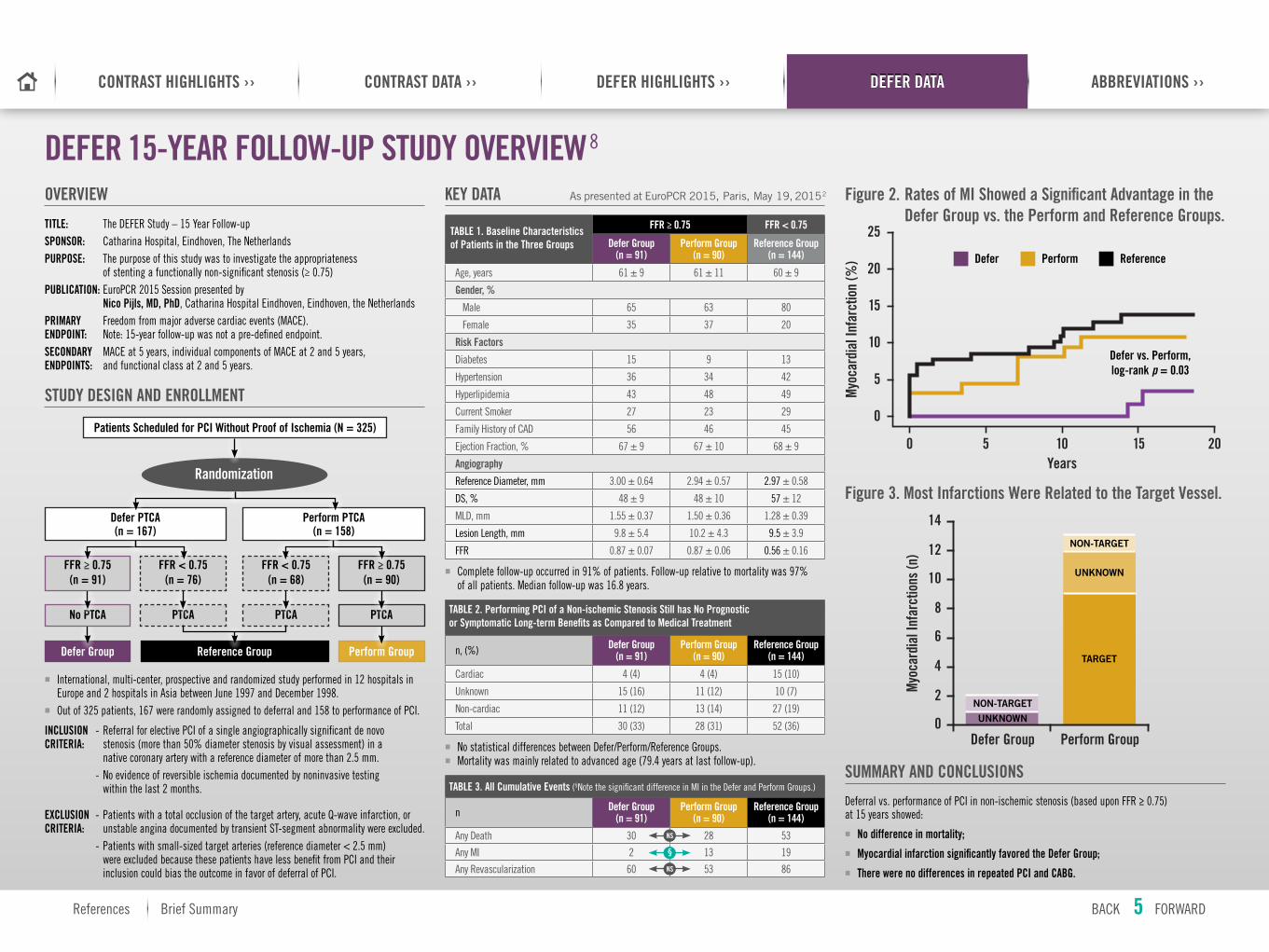
TITLE: The DEFER Study – 15 Year Follow-upSPONSOR: Catharina Hospital, Eindhoven, The Netherlands PURPOSE: The purpose of this study was to investigate the appropriateness of stenting a functionally non-significant stenosis (≥ 0 .75)PUBLICATION: EuroPCR 2015 Session presented by Nico Pijls, MD, PhD, Catharina Hospital Eindhoven, Eindhoven, the Netherlands PRIMARY Freedom from major adverse cardiac events (MACE) . ENDPOINT: Note: 15-year follow-up was not a pre-defined endpoint .SECONDARY MACE at 5 years, individual components of MACE at 2 and 5 years, ENDPOINTS: and functional class at 2 and 5 years .
STUDY DESIGN AND ENROLLMENT
�� International, multi-center, prospective and randomized study performed in 12 hospitals in Europe and 2 hospitals in Asia between June 1997 and December 1998 .
�� Out of 325 patients, 167 were randomly assigned to deferral and 158 to performance of PCI .
INCLUSION - Referral for elective PCI of a single angiographically significant de novo CRITERIA: stenosis (more than 50% diameter stenosis by visual assessment) in a native coronary artery with a reference diameter of more than 2 .5 mm . - No evidence of reversible ischemia documented by noninvasive testing within the last 2 months .
EXCLUSION - Patients with a total occlusion of the target artery, acute Q-wave infarction, or CRITERIA: unstable angina documented by transient ST-segment abnormality were excluded . - Patients with small-sized target arteries (reference diameter < 2 .5 mm) were excluded because these patients have less benefit from PCI and their inclusion could bias the outcome in favor of deferral of PCI .
DEFER 15-YEAR FOLLOW-UP STUDY OVERVIEW8
KEY DATA
SUMMARY AND CONCLUSIONS
Deferral vs . performance of PCI in non-ischemic stenosis (based upon FFR ≥ 0 .75) at 15 years showed:
�� No difference in mortality;�� Myocardial infarction significantly favored the Defer Group;�� There were no differences in repeated PCI and CABG.
As presented at EuroPCR 2015, Paris, May 19, 20152
TABLE 1. Baseline Characteristics of Patients in the Three Groups
FFR ≥ 0.75 FFR < 0.75
Defer Group (n = 91)
Perform Group (n = 90)
Reference Group (n = 144)
Age, years 61 ± 9 61 ± 11 60 ± 9
Gender, %
Male 65 63 80
Female 35 37 20
Risk Factors
Diabetes 15 9 13
Hypertension 36 34 42
Hyperlipidemia 43 48 49
Current Smoker 27 23 29
Family History of CAD 56 46 45
Ejection Fraction, % 67 ± 9 67 ± 10 68 ± 9
Angiography
Reference Diameter, mm 3 .00 ± 0 .64 2 .94 ± 0 .57 2 .97 ± 0 .58
DS, % 48 ± 9 48 ± 10 57 ± 12
MLD, mm 1 .55 ± 0 .37 1 .50 ± 0 .36 1 .28 ± 0 .39
Lesion Length, mm 9 .8 ± 5 .4 10 .2 ± 4 .3 9 .5 ± 3 .9
FFR 0 .87 ± 0 .07 0 .87 ± 0 .06 0 .56 ± 0 .16
�� Complete follow-up occurred in 91% of patients . Follow-up relative to mortality was 97% of all patients . Median follow-up was 16 .8 years .
TABLE 2. Performing PCI of a Non-ischemic Stenosis Still has No Prognostic or Symptomatic Long-term Benefits as Compared to Medical Treatment
n, (%) Defer Group (n = 91)
Perform Group (n = 90)
Reference Group (n = 144)
Cardiac 4 (4) 4 (4) 15 (10)
Unknown 15 (16) 11 (12) 10 (7)
Non-cardiac 11 (12) 13 (14) 27 (19)
Total 30 (33) 28 (31) 52 (36)
�� No statistical differences between Defer/Perform/Reference Groups .�� Mortality was mainly related to advanced age (79 .4 years at last follow-up) .
TABLE 3. All Cumulative Events (§Note the significant difference in MI in the Defer and Perform Groups .)
n Defer Group (n = 91)
Perform Group (n = 90)
Reference Group (n = 144)
Any Death 30 28 53
Any MI 2 13 19
Any Revascularization 60 53 86
Perform Group
PTCAPTCA
Reference Group
PTCA
Defer Group
No PTCA
FFR < 0.75 (n = 76)
FFR < 0.75 (n = 68)
FFR ≥ 0.75 (n = 90)
FFR ≥ 0.75 (n = 91)
Perform PTCA (n = 158)
Defer PTCA (n = 167)
Randomization
Patients Scheduled for PCI Without Proof of Ischemia (N = 325)
Figure 2. Rates of MI Showed a Significant Advantage in the Defer Group vs. the Perform and Reference Groups.
Defer Perform Reference
Defer vs. Perform, log-rank p = 0.03
0
25
20
15
10
5
0
5 10 15 20
Myo
card
ial I
nfar
ctio
n (%
)
Years
Figure 3. Most Infarctions Were Related to the Target Vessel.
14
12
10
8
6
4
2
0
Myo
card
ial I
nfar
ctio
ns (n
)
Defer Group Perform Group
TARGET
UNKNOWN
UNKNOWN
NON-TARGET
NON-TARGET
NS
NS
§
References Brief Summary
CONTRAST DATA ››CONTRAST HIGHLIGHTS ›› DEFER HIGHLIGHTS ›› DEFER DATA ›› ABBREVIATIONS ››
BACK 5 FORWARD
DEFER DATA
1. Johnson N, The CONTRAST Study. (Can contrast injection better approximate FFR compared to pure resting physiology?). EuroPCR. May 2015.
2. Jeremias, A., Maehara, A., Genereux, P., Asress, K. N., Berry, C., De Bruyne, B., Stone, G. W. (2014). Multicenter core laboratory comparison of the instantaneous wave-free ratio and resting Pd/Pa with fractional flow reserve: The Resolve Study. Journal of the American College of Cardiology, 63, 1253-1261.
3. Escaned, J., Echavarría-Pinto, M., Garcia-Garcia, H. M., van de Hoef, T. P., de Vries, T., Kaul, P., et al. Prospective Assessment of the Diagnostic Accuracy of Instantaneous Wave-Free Ratio to Assess Coronary Stenosis Relevance Results of ADVISE II International, Multicenter Study (ADenosine Vasodilator Independent Stenosis Evaluation II). JACC Cardiovascuar Intervention 2015;8;6:824-833. NCT01740895.
4. Echavarría-Pinto, M., van de Hoef, T. P., Garcia-Garcia, H. M., de Vries, T., Serruys, P. W., Samady, H., et al. Diagnostic Accuracy of Baseline Distal-to-Aortic Pressure Ratio to Assess Coronary Stenosis Severity A Post-Hoc Analysis of the ADVISE II Study. JACC Cardiovascuar Intervention 2015;8;6:834-6.
5. Johnson, N. P., Kirkeeide, R. L., Asrress, K. L., Fearon, W. F., Lockie T., Marques, K. M., Gould, K. L. (2013). Does the instantaneous wave-free ratio approximate the fractional flow reserve? Journal of the American College of Cardiology, 61, 1428-1435.
6. Park S.J., JACC Cardiovasc Interv. 2012 Oct;5(10):1029-36.
7. Watkins, S., Hennigan, B., Eteiba, H., Lindsay, M., McEntegart, M., Berry, C., & Oldroyd, K. (2014, May). VERIFY-2 presentation. SCAI presentation
8. Pijls N, et al. Deferral vs Performance of PCI in Functionally Non-Significant Coronary Artery Stenosis- 15 Year Follow-up of the DEFER Trial. EuroPCR. May 2015
AUC Area under ROC curve (Delong comparison)
CAD Coronary artery disease
CABG Coronary artery bypass grafting
cFFR Contrast FFR
DS Diameter stenosis
ECG Echocardiogram
FFR Fractional flow reserve
IC Interventional cardiology
IV Intravenous
LVH Left ventricular hypertrophy
MACE Major adverse cardiac event
MI Myocardial infarction
MLD Minimum lumen diameter
PCI Percutaneous coronary intervention
Pd/Pa Ratio of distal coronary pressure across a stenosis over the aortic pressure at rest (non-hyperemic) throughout the entire cardiac cycle
PTCA Percutaneous transluminal coronary angioplasty
STEMI ST-segment elevation myocardial infarction
ReferencesAbbreviations
References Brief Summary
CONTRAST DATA ››CONTRAST HIGHLIGHTS ›› DEFER HIGHLIGHTS ›› DEFER DATA ›› ABBREVIATIONS ››
BACK 6 FORWARDReferences
ABBREVIATIONS
St. Jude Medical Brasil Ltda. Rua Itapeva, 5385º ao 8º andares01332-000 – São Paulo – SPBrazilT +55 11 5080 5400 | F +55 11 5080 5423
St. Jude Medical (Hong Kong) Ltd. Suite 1608, 16/F Exchange Tower33 Wang Chiu RoadKowloon Bay, KowloonHong Kong SART +852 2996 7688 | F +852 2956 0622
St. Jude Medical Japan Co., Ltd. Shiodome City Center 15F1-5-2 Higashi Shinbashi, Minato-kuTokyo 105-7115JapanT +81 3 6255 6370 | F +81 3 6255 6371
St. Jude Medical Australia Pty, Ltd. 17 Orion RoadLane Cove, NSW 2066AustraliaT +61 2 9936 1200 | F +61 2 9936 1222
St. Jude Medical Inc. Global Headquarters One St. Jude Medical Drive St. Paul, MN 55117 USA T +1 651 756 2000 | F +1 651 756 3301
St. Jude Medical S.C., Inc. Americas Division6300 Bee Cave RoadBldg. Two, Suite 100Austin, TX 78746USAT +1 512 286 4000 | F +1 512 732 2418
SJM Coordination Center BVBA The Corporate VillageDa Vincilaan 11-Box F1B-1935 Zaventem, BelgiumT +32 2 774 68 11 | F +32 2 772 83 84
SJMprofessional.com
Rx Only Brief Summary: Prior to using these devices, please review the Instructions for Use for a complete listing of indications, contraindications, warnings, precautions, potential adverse events and directions for use.
iFR is a trademark of Volcano Corporation and Adobe Acrobat Reader is a trademark of Adobe Systems Incorporated. Unless otherwise noted, ™ indicates that the name is a trademark of, or licensed to, St. Jude Medical or one of its subsidiaries. ST. JUDE MEDICAL and the nine-squares symbol are trademarks and service marks of St. Jude Medical, Inc. and its related companies. © 2015 St. Jude Medical, Inc. All Rights Reserved.
SJM-OPS-0715-0061 | This document is for global use.
References Brief Summary
CONTRAST DATA ››CONTRAST HIGHLIGHTS ›› DEFER HIGHLIGHTS ›› DEFER DATA ›› ABBREVIATIONS ››
Brief Summary BACK 7