foot/ankle injuries in ice hockey - mosbrook design injuries in ice hockey john theodoropoulos, ......
TRANSCRIPT

Foot/Ankle Injuries in Ice Hockey
John Theodoropoulos, MD MSc FRCSC
Mount Sinai & Women’s College Hospital

Disclosure
Neither I, John Theodoropoulos, nor any family member(s), author(s), have any relevant financial relationships to be discussed, directly or indirectly, referred to or illustrated with or without recognition within the presentation.

Objectives
•! Epidemiology of foot/ankle injuries •! Ankle Syndesmosis Injury •! Foot Fractures •! Ankle Cartilage Injuries •! Peroneal Subluxation •! Dermatoses in hockey
3!

Epidemiology
Head 10%
Neck 3%
Face 19% Mouth
4%
Shoulder/upper arm
14%
Elbow/lower arm 8%
Wrist/hand/finger 14%
Hip/trunk 9%
Upper leg/knee 8%
Lower leg/ankle/foot
11%
Other/unkown 0%
4!
Contact with Puck 20%
Falls 12%
Contact with
Boards 10%
Contact with
Skate 6%
Player-to-Player contact
5%
Contact with Stick 4%
Other 43%
Lower Leg/ankle/foot
Hockey ER Visits 1990-2006
Deits et al (2010) Hockey ER Visits 1990-2006 (18,898/yr NATIONALLY US)

Epidemiology
5!

Epidemiology
6!6

Foot & Ankle Injuries (2006-2012) NHL DATA
7!

8!
Most Common Foot & Ankle Fractures/Year

9!
Season Breakdown - Top 5 Foot & Ankle Injuries
Ankle Sprains
•! Lateral ankle sprains most common: –! 1/10,000 people per day
–! 90% typical lateral inversion
•! Syndesmosis: only 10% –! often missed
–! MRI useful ! high interobserver agreement (Vogl et al. 1997; Muhle et al. 1998)
–! MRI sensitive (100%) and specific (93%) compared to arthroscopy in acute injury (Takao et al. 2003)

Syndesmosis Injuries in Hockey
11!

Syndesmosis Injuries in Hockey
•! External rotation (foot dorsiflexion/pronation) –! Ligamentous –! +/- fracture
•! Body internally rotates on planted foot, hyperdorsiflexion
•! NHL (Wright et al. 2004): –! 14 syndesmosis injuries = 45 avg days
lost –! 4 low sprains = 1.5 avg days lost
•! NCAA hockey: longest RTP of all injuries (Flik et al. 2005)
12!

Syndesmosis Injuries in Hockey
•! Incidence in general population: 10% •! NHL injury surveillance system: 50% •! Football: only 18.4% •! Why difference?
–!Mechanical stiffness of boot protects from inversion injuries (lateral ligament) but predisposes to external rotation injuries (syndesmosis)
13!

Anatomy


Clinical Exam 1. Squeeze test
2. External rotation test 3. Translation of malleolii
pain at syndesmosis

Imaging - Radiographs
17!
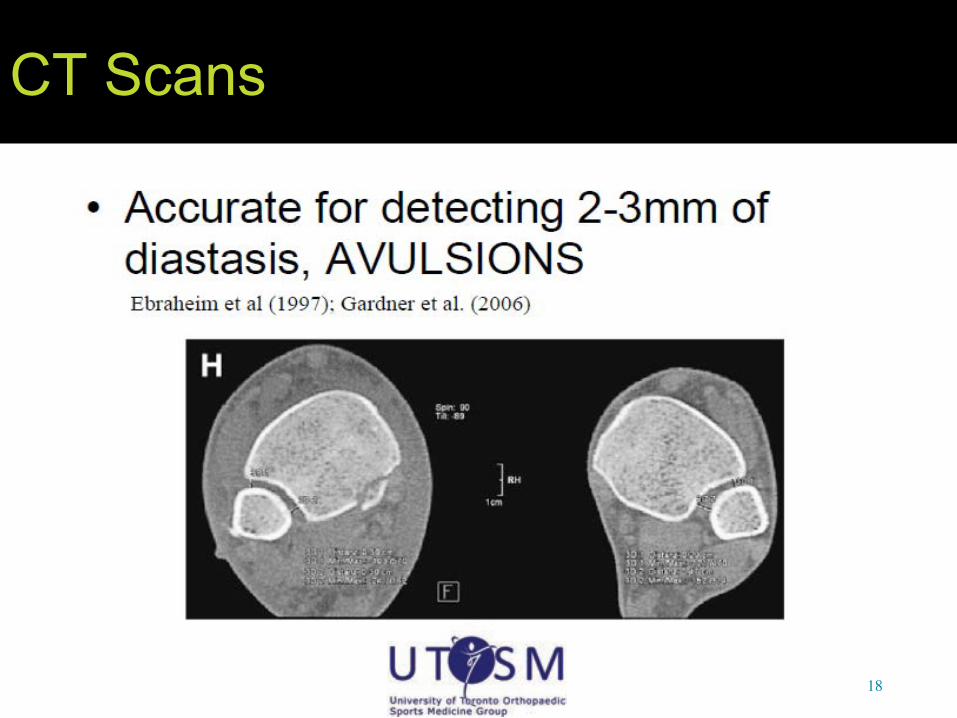
CT Scans
18!
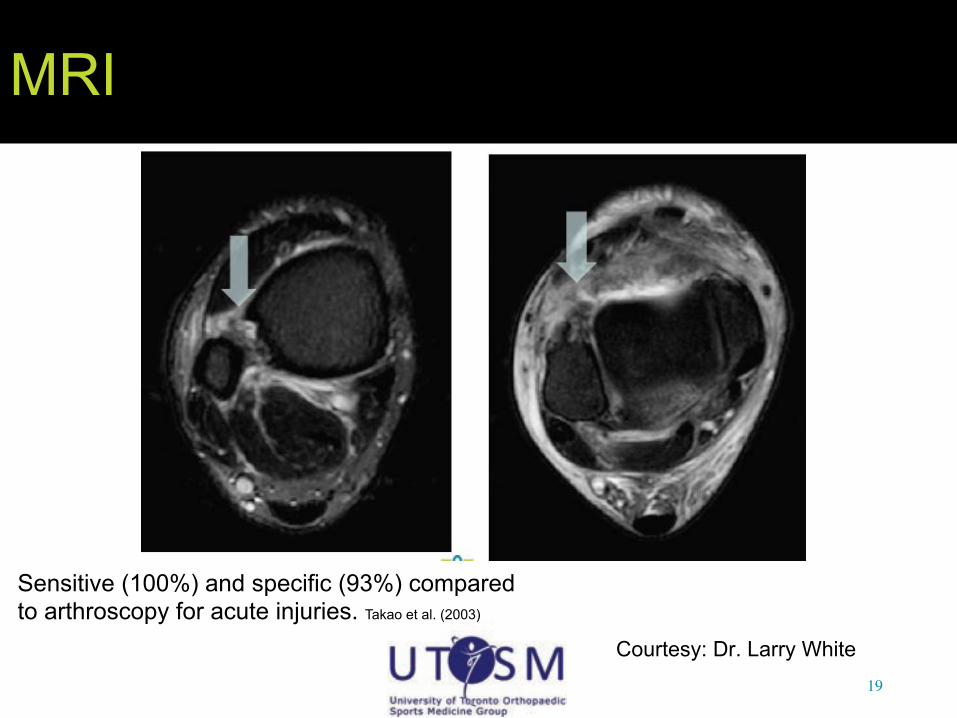
MRI
Courtesy: Dr. Larry White 19!
Sensitive (100%) and specific (93%) compared to arthroscopy for acute injuries. Takao et al. (2003)

NHL DATA 2006 - 2011
•! 66 INJURIES –! PRESEASON: 7 –! REGULAR SEASON: 53 –! POST SEASON: 4 –! OFFSEASON:2
•! 9 DURING PRACTICE •! 1 NON-HOCKEY
RELATED

NHL DATA 2006 - 2011
•! MECHANISM –!EVERSION: 13 –!NON CONTACT TWIST: 12 –! INTO BOARDS: 10 –!OPPOSING PLAYER FELL ON ANKLE: 10 –!CAUGHT ANKLE IN RUT OF ICE: 7 –! INVERSION: 2 –!HIT BY PUCK: 1

NHL DATA 2006 - 2011
•! 8.7 MAN GAMES MISSED •! 24.6 DAYS TO RETURN TO PLAY
•! 25 DEFENCEMEN •! 4 GOALIES •! 37 FORWARDS

Subset MRI Results
•! N=16 •! Age range 17-29 years (median 23) •! 9 right, 7 left •! Clinical symptoms:
•!Pain/ecchymosis above joint line •!Painful external rotation stress •!Pain to compression testing
•! Median 7 days to MRI (IQR 3, 14) •! All within 3 weeks except one patient

Results – recovery
GAMES LOST (Median, IQR):
18 (11, 25) DAYS LOST (Median, IQR):
43 (24, 56)*
*On par with Wright et al. (2004) – 45 games; one player was still off end of season

Syndesmotic Ligaments
COMPLETE PARTIAL NORMAL
AITFL 12 (75%) 4 (25%) 0
PITFL 0 9 (56%) 7 (44%)
IOM All edematous (hard to distinguish)

Ankle Ligaments
Intact Ant Talofibular ligament
COMPLETE PARTIAL NORMAL
ATFL 1 (6%) 7 (44%) 8 (50%)
PTFL 0 0 16
CFL 0 3 (19%) 13 (81%)
DELT 1 (6%) 4 (25%) 11 (69%)

Bone Contusions
•! 11/16 patients had bone contusions
•! Most common locations:
1.! posterior/posteromedial talus
2.! Posterior/posteromedial tibia (malleolus)
•! 1 patient with OCL Bone bruising - Posterior Med Malleolus

Bone bruising - Posterior Tibial Plafond

Days lost – no patterns
4 players had a complete AITFL + bone bruise + !2 other ligaments. These players lost a mean 47 days.
0
5
10
15
20
25
30
35
40
45
50
complete AITFL No bony contusion Bony contusion AITFL + 1 other lig AITFL + !2 other lig
Mean days lost

NHL Data MRI Findings
•! Reproducible! –!Tearing AITFL (75% complete, 25% partial) –!Partial injury distal interosseous membrane –!Other ligaments rarely completely torn –!High incidence bone bruising – especially
posteromedial talus and tibia –!Maybe bone bruising and multiple
ligaments increased man-games lost
30!

Elite athletes time lost for injury
31!


Foot Fractures/Contusions
•! Kazuhara et. Al –!MC injury = contusions (35.4/1000 player
game hours) –!MC contusion = foot contusion (5.1/1000
player game hours)
33!

Why foot injuries? •! Puck
–!Maximal impact force 1250 lbs Sim et al (1987)
•! Traumatic contact with stick, rigid boards Kuzuhara et al (2009) , Agel et al 2010, Deits et al 2010
•! Agel et al (2010): –!Marketing push for lighter equipment last 10
years •! less material over front, tongue, and sidewall of skate
–!No data yet to determine whether increased incidence of injury from these “lighter” skates
34!

Fractures
•! Navicular and base of fifth metatarsal (styloid) are more frequently fractured than other foot bones
•! Usually oblique type
35!
and fifth
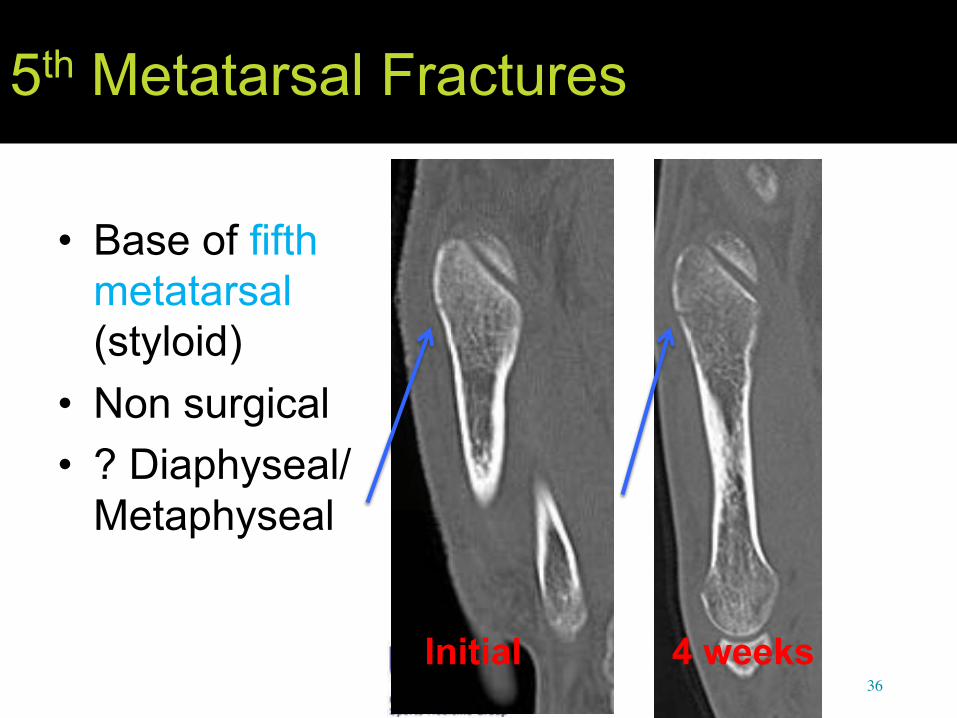
5th Metatarsal Fractures
•! Base of fifth metatarsal (styloid)
•! Non surgical •! ? Diaphyseal/
Metaphyseal
36!Initial 4 weeks

1st Metatarsal Fractures
•! Common •! Blocked shots •! Usually
minimally or non displaced
37!
Initial Initial

1st Metatarsal Fractures
•! Common •! Blocked shots •! Usually
minimally or non displaced
38!
2 months 2 months
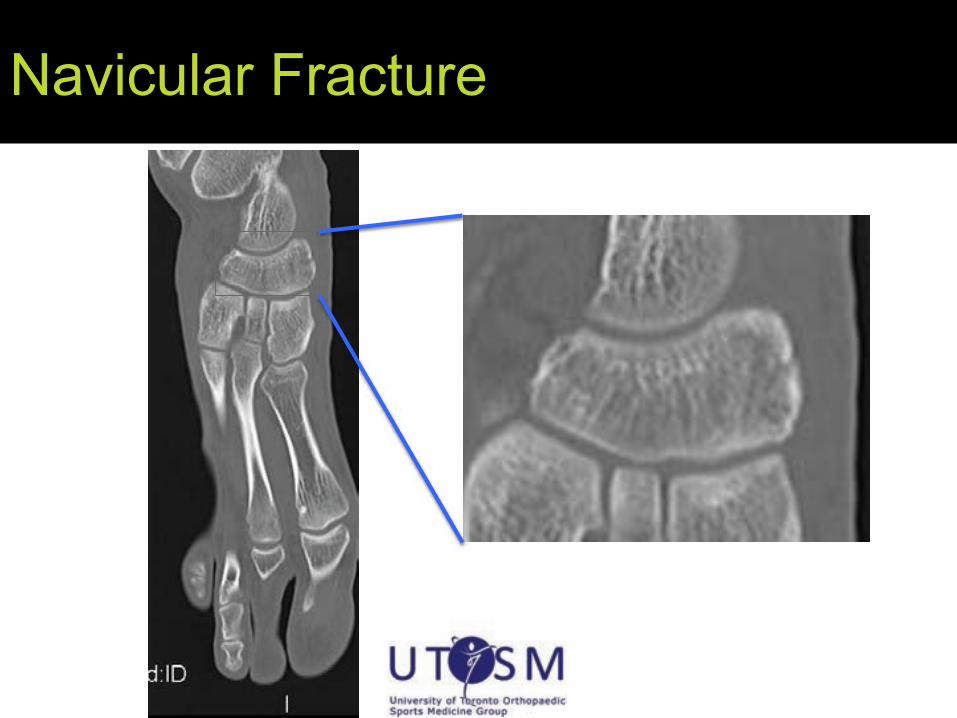
Navicular Fracture

Navicular Fracture
•! 17 yo M •! Painful foot after blocking shot •! PMHx:
–!Type I DM controlled with insulin •! O/E:
–!Tender midfoot


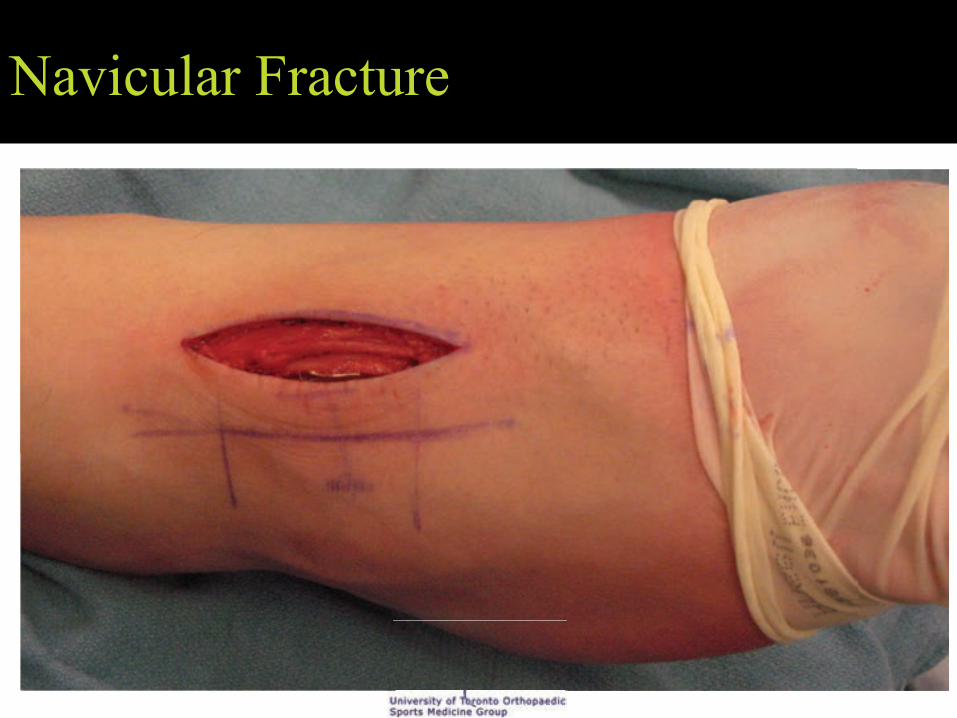
Treatment

Navicular Fracture
•! 8 months after injury. –!+++ pain with walking and weightbearing



Treatment?
Navicular Fracture

Navicular Fracture


Treatment of Navicular and MT #s
•! Non displaced –!Immobilization 4-8
weeks •! Displaced
–!Closed reduction; may require ORIF
50!
Caselli et al (2002)

Toe Fractures
•! Toe fractures less likely due to rigid skate toe, but can happen
•! Pain, edema, ecchymosis of affected toe in player
•! Subungual hematoma may be suggestive
51!
Caselli et al (2002)

Toe Fracture Treatment
•! Nondisplaced –! Immobilization splinting to
the neighboring toe with tape, felt, prefabricated splints
–!Return to play in few days! •! Displaced
–!Closed reduction or ORIF –!Return to play at least a few
weeks 52!
Caselli et al (2002)

OCD Injuries Talus
•! Talar OCD usually
due to trauma.
•! Rarely heal without intervention. Rarely heal without

Pathology
WHY DOES ANKLE OCD HURT? •! Cartilage has no nerve fibers •! Nerve fibers:
–!Synovium –! Joint Capsule –!Bone
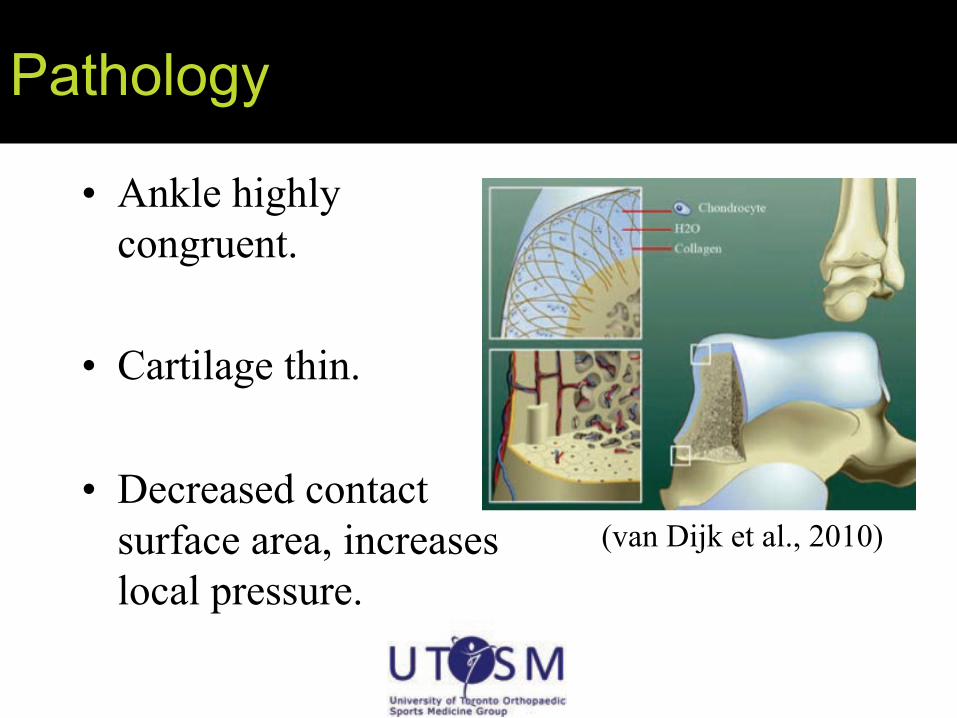
Pathology
•! Ankle highly congruent.
•! Cartilage thin.
•! Decreased contact surface area, increases local pressure.
(van Dijk et al., 2010)

Pathology
•! Cartilage withstands compression: –!Liquid (synovial fluid) –!Solid (collagen + PG)
•! When one part of jt loaded, unloaded jt is stretched and fluid flows to unloaded area.
•! Subchondral plate prevents fluid from going into bone.
(van Dijk et al., 2010)

Pathology
•! Damaged subchondral bone can’t support cartilage. –!Water flows from cartilage into microfractured
areas of subchondral bone. –!Continuous high fluid pressure causes osteolysis
and larger defects. –!+++PAIN
(van Dijk et al., 2010)

Surgical Treatment Options
•! Arthroscopic –! Excision –! Excision & Curettage –! Excision, Curettage & Microfracture
•! Drilling –! Transmalleolar –! Retrograde
•! Mosaicplasty/OATS •! Autogenous Chondrocyte Implantation •! Allograft

Peroneal Tendon Instability
•! Snapping Peroneal Tendon
•! Pain •! Tape/treat local
symptoms •! Surgery at end of
season
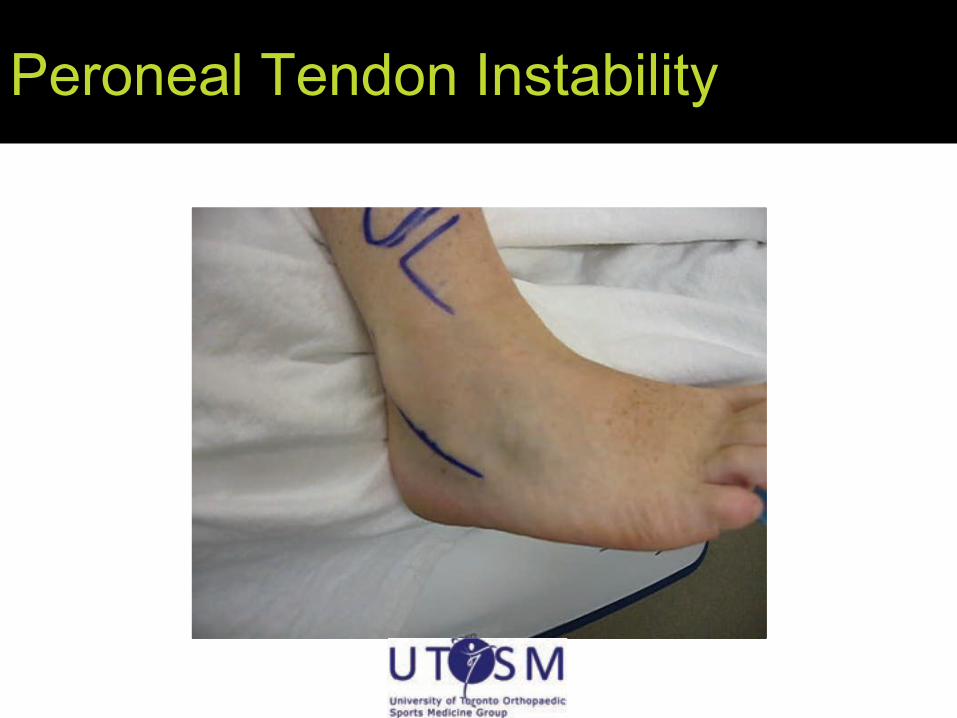
Peroneal Tendon Instability
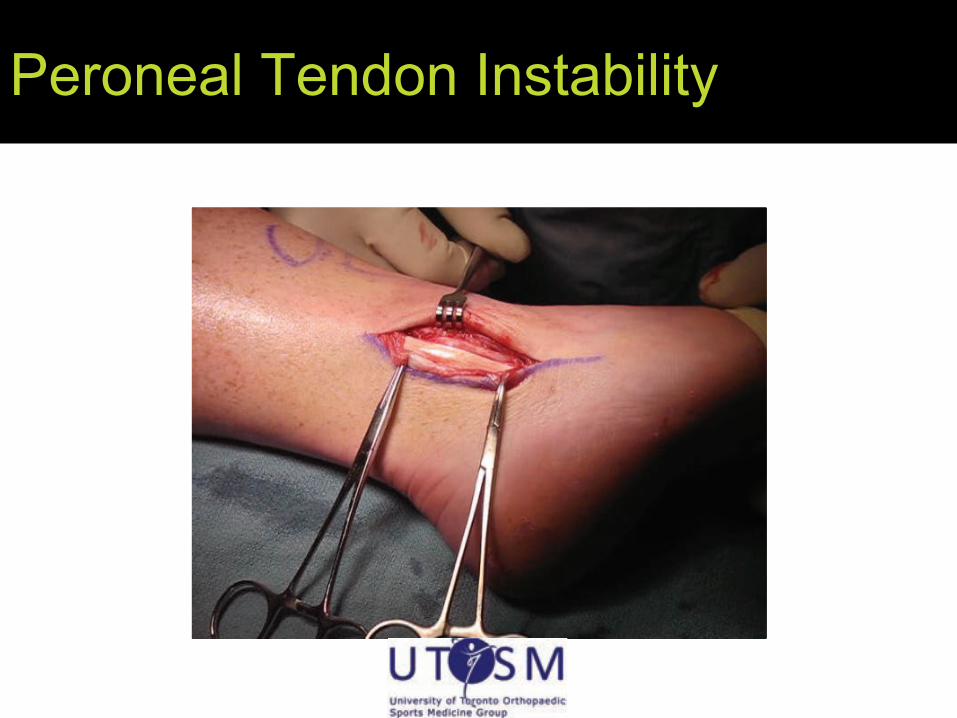
Peroneal Tendon Instability

Skater’s Nodules
•!Pathogenesis: repeated friction, pressure, and irritation during skating ! increased laying down of collagen
•!Location: Lateral malleoli, lateral sides, skin over Achilles’ tendon
•!Presentation: Pain during skating
Tlougan et al (2011)

Skater’s Nodules
•!Histology: Epidermal acanthosis, compact hyperkeratosis, and thickening of dermis with increase in collagen
•!Ddx: calluses, skater’s pads, hypertrophic scars, dermal neoplasms, granulomas, and warts
63!Tlougan et al (2011)

Skater’s Nodules Treatment
•! Reduction in chronic stimulation •! keratolytics and intralesional injections of tiamcinolone acetonide •! ultrapotent topical corticosteroids •! Must protect skin as well, otherwise above won’t work •! Surgical excision not recommended due to complications from scarring and high recurrence rate
64!Tlougan et al (2011)

Skater’s pads
•! Path same as skater’s nodules, except more callus-like
•! Respond to paring & same treatment as nodules
•! Prevention: protective padding, stretching of skate in areas of greatest pressure
Tlougan et al (2011)

Malleolar Bursitis - Presentation
Pressure/force by skates over the area of the malleoli ! adventitious bursa (malleoli don’t normally have bursae) Pain/swelling over medial malleolus, point tenderness and soft tissue mass – interferes with practice and games Clinical Dx

Malleolar Bursitis Non-op Mngmt
•! rest will eliminate, but usually not an option in NHL players
•! Stretching of skate over malleoli
•!Doughnut cushion over malleolus
•! Aspirate and betamethasone injections (1-2 ml 2x max)
67!
If these fail and pt cannot rest, or septic bursitis ! Resection Brown et al (2000)

Malleolar Bursa Resection
•! If septic, add IV Abx
•! Shaving of Malleolus not recommended •! Does not address underlying problem of rigid
skate •! Elastic ankle sleeve post-op – resume
activities once incisions healed and edema absent
68!

Pump Bump (a.k.a. Haglund’s deformity)
•!Repeated vertical movement of back of foot against rigid skate back
•!Calcaneal tuberosity enlarges ! painful bursitis

Pump Bumps
On exam, inflamed bump on back of heel and tenderness in Achilles insertion site
Essential Radiology in Sports Medicine Robinson P (2010)
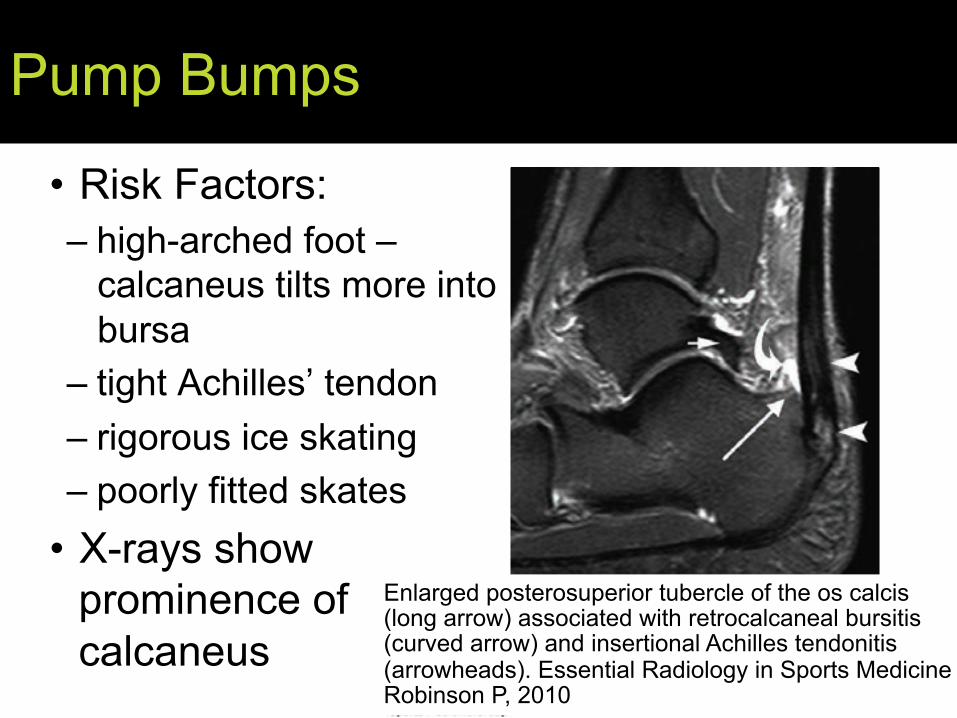
Pump Bumps
•!Risk Factors: –!high-arched foot –
calcaneus tilts more into bursa
–! tight Achilles’ tendon –! rigorous ice skating –!poorly fitted skates
•! X-rays show prominence of calcaneus
71!
Enlarged posterosuperior tubercle of the os calcis (long arrow) associated with retrocalcaneal bursitis (curved arrow) and insertional Achilles tendonitis (arrowheads). Essential Radiology in Sports Medicine Robinson P, 2010

Pump Bumps
•! Treatment: Reduce bursal inflammation! –!Oral anti-inflammatories, ice, and exercises
aimed at stretching heel cord –!Skate mods to lift heels in athletes with high
arches, heel pads, and custom orthotics –!Off-training: Avoid shoes with rigid heel back
as well as avoid running on hard surfaces and uphill during off-ice training
72!
Tlougan et al (2011)

Skate Bite
•! inflexible skate tongue ! " pressure on anterior ankle with repeated dorsiflexion
•! Happens early in season with new skates
•! Leads to Tibialis Anterior tendonitis
73!LaPrade et al (2009)

Skate Bite
•! Pain and swelling around dorsal aspect of foot near tongue of skate
•! May see callus or “pseudonodules” over tibialis anterior tendon
LaPrade et al (2009)
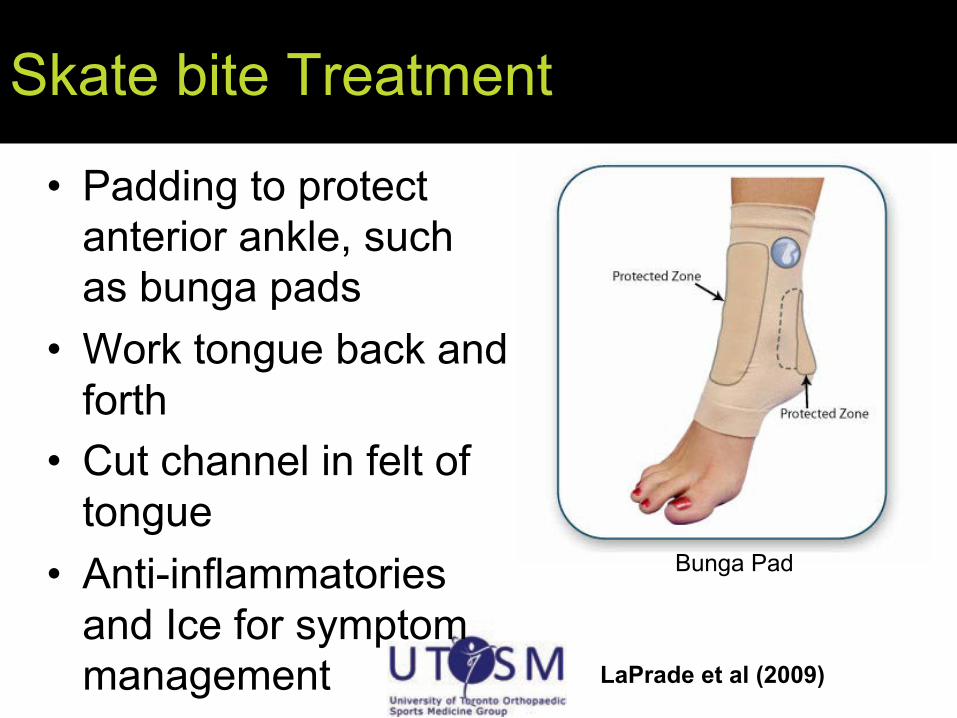
Skate bite Treatment
•! Padding to protect anterior ankle, such as bunga pads
•! Work tongue back and forth
•! Cut channel in felt of tongue
•! Anti-inflammatories and Ice for symptom management
Bunga Pad
LaPrade et al (2009)

Skate Bite Prevention
•! Educate players with new skates to work the tongue before engaging activities
•! Foam padding over anterior ankle in new skates
76!LaPrade et al (2009)

Friction bullae •! From acute friction in
areas of increased temperature, dryness, or moisture
• Shearing forces split stratum granulosum which fills with transudate
• Location: Tips of toes, lateral feet, balls of feet, posterior heels
Tlougan et al (2011)
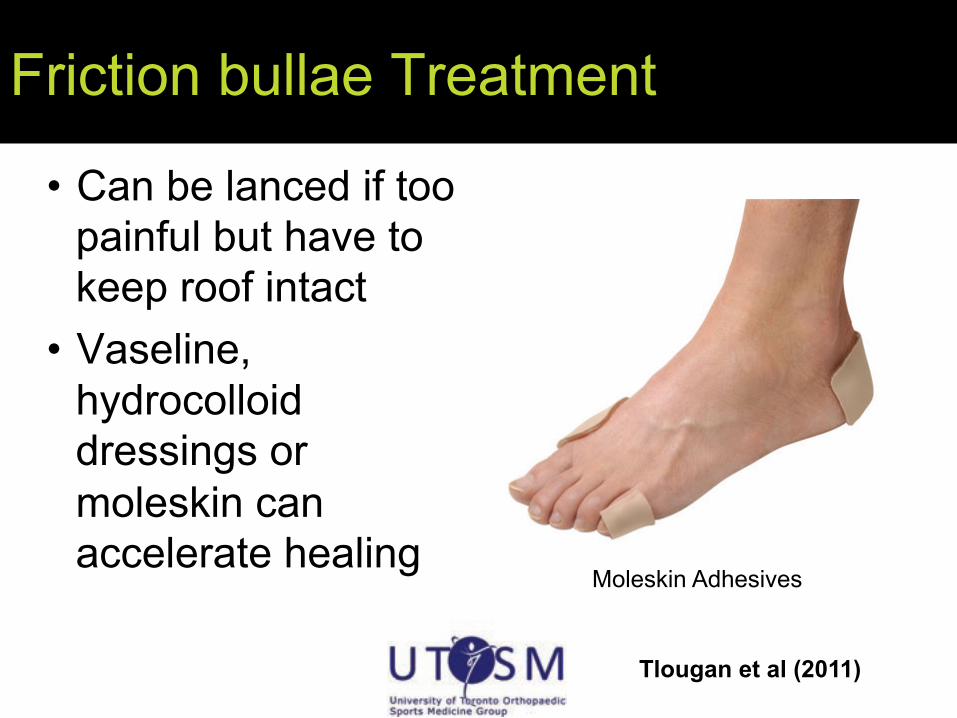
Friction bullae Treatment
•!Can be lanced if too painful but have to keep roof intact
•! Vaseline, hydrocolloid dressings or moleskin can accelerate healing
Moleskin Adhesives
Tlougan et al (2011)

Friction Bullae Prevention MINIMIZE FRICTION! • Well fitted skates with
space around toes • on slip in-soles • moisture-wicking
socks • pads or padded socks • topical agents:
Vaseline, drying powders, aluminum chloride.
Tlougan et al (2011)

Corns – Why?
•!mechanical stress ! Hyperkeratotic papule
•! In hockey ! ill-fitting skates, abnormal repetitive foot maneuvers, high levels of physical activity
80!Tlougan et al (2011)
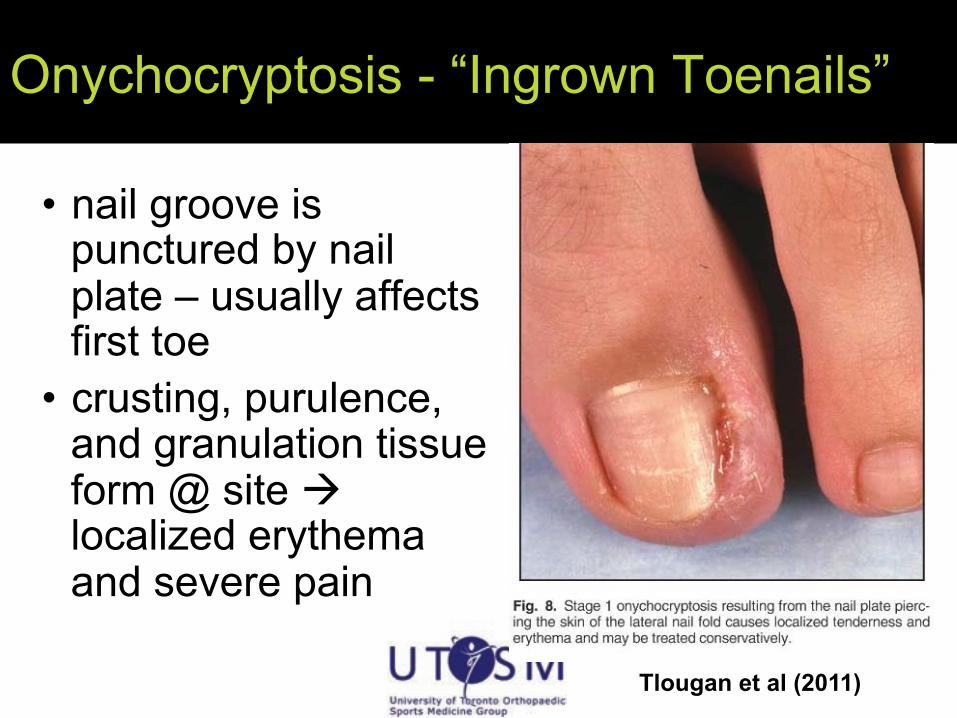
Onychocryptosis - “Ingrown Toenails”
•! nail groove is punctured by nail plate – usually affects first toe
•! crusting, purulence, and granulation tissue form @ site ! localized erythema and severe pain
Tlougan et al (2011)

Corns Prevention
•! Best Prevention: well fitting skates •!Orthotics with silicone orthodigital splints
may be beneficial •!Moleskins and toe separators reduce
friction (do not eradicate corn)
82!Tlougan et al (2011)

References 1.! Deits, Jeff. "Patients With Ice Hockey Injuries Presenting to US Emergency Departments,
1990-2006." Journal of Athletic Training. 45.5 (2010): 467-74. Print. 2.! Sim, Franklin H. "Ice Hockey Injuries." American Journal of Sports Medicine. 15.1 (1987): 30-40. Print. 3.! Caselli, Mark A. "Ice Hockey Injuries: How to Maximize Treatment Results." Podiatry Today. 15.8 (2002):
84-86. Web. 31 May. 2012. <http://www.podiatrytoday.com/article/666>. 4.! LaPrade, R F. "Division I intercollegiate ice hockey team coverage." British Journal of Sports Medicine.
43. (2009): 1000-005. Print. 5.! Moslener, Matthew D. "Ice Hockey: A Team Physician's Perspective." Current Sports Medicine Reports.
9.3 (2010): 134-38. Print. 6.! Tlougan, BE. "Skin conditions in figure skaters, ice-hockey players and speed skaters: part I -
mechanical dermatoses.." Sports Medicine (Auckland, N.Z.). 41.9 (2011): 709-19. Print. 7.! Kuzuhara, Kenji. "Ice hockey injuries in a Japanese elite team: a 3-year prospective study ." Journal of
Athletic Training. 44.2 (2009): 208-14. Print 8.! Agel, Julie. "A 7-year review of men's and women's ice hockey injuries in the NCAA." Canadian Journal
of Surgery. 53.5 (2010): 319-23. Print. 9.! Brown, Treg. "Malleolar Bursitis in Figure Skaters: Indications for Operative and Nonoperative
Treatment." American Journal of Sports Medicine. 28.1 (2000): 109-11. Print. 10.! Brown, Robert. "MRI of Medial Malleolar Bursa." American Journal of Roentgenology. 184.3 (2005):
979-83. Print. 11.! Martinez-Nova, Alfonso. "A New Onychocryptosis Classification and Treatment Plan." Journal of the
American Podiatric Medical Association. 97.5 (2007): 389-93. Print.
83!