fluency plus program - asha
TRANSCRIPT
Fluency Plus ProgramA Comprehensive Treatment for School Aged
Children
Robert Kroll, Ph.D.Marni Grotell, M.H.Sc.
Lea Ayuyao, M.Sc.Rachelle Vekris, M.H.Sc.
The Speech and Stuttering InstituteToronto, Canada
www.speechandstuttering.com

Presentation Outline
The Nature of Stuttering– Definitions and Characteristics
Treatment for Stuttering– Models and Principles
Treatment Efficacy Studies
The Fluency Plus Program– Fluency Skills (Targets)
Presentation OutlineTransfer
– Definition and procedures– Mental rehearsal– Types of fluency
Cognitive Restructuring– Issues during transfer– The stuttering mentality– Self-talk
Maintenance– Definition and procedures– Forms of practice
Therapy Formats– Groups vs individual– Associated factors

Stuttering
A complex multidimensional condition in which the flow of
speech or fluency is disrupted by involuntary speech motor events

Stuttering
ProblemPsychological StateAttitudeFeelingsEmotionsSelf ConceptSelf EsteemPsychological FactorsEtc
BehaviorDisfluency Form TypesBlocksRepetitionsProlongationsDisrhythmic PhonationContingent BehavioursEtc.

Types of Disfluency
• audible/ silent sound and syllable repetitions
• sound prolongations
• dysrhythmic phonations
• blocks
• intra-syllabic fragmentation

Stuttering Contingent Behaviours
• disordered breathing• glottal fry• lip pursing• eye blinks• facial grimacing• head jerks• abnormal body movements
may be observed at the respiratory, phonatory or articulatory levels of the speech mechanisms

Avoidance Behaviour
• specific sounds and words are often reported to result in increased stuttering
• scanning behaviour in order to predict stuttering
• avoidance strategies include word substitution, phrase revision, circumlocution, stopping the communicative process
• situational avoidance

WHO International Classification of Functioning, Disability and
Health (ICF)
Disorder
Body Structure/Function (Impairment)
Activity and Participation (Disability)
Environmental Factors (Handicap)

Body Structure and Function
Any loss or abnormality of psychological, physiological, or anatomical structure or function.

Stuttering in terms of the WHO Classification
Body Structure and Function• Frequency of stuttering behaviour• Duration of instances of disruption• Severity• Secondary behaviour

Activity and Participation
• Any restriction or lack of ability (resulting from an impairment) to perform a normal human activity.
• A disability is the functional consequence of an impairment.

Stuttering in Terms of the WHO Classification
Activities and Participation• Inability to say specific words/sounds• Difficulty communicating in specific
situations» Telephone» Groups» Answering specific questions» Formal Presentations» Authority figure

Environmental Factors
The social consequence of an impairment or disability defined by the
attitude and responses of others. Thus, the state of being handicapped is
relative to other people.

Stuttering in terms of the WHO Classification
Environmental Factors• Classroom discrimination• Teasing and bullying• Social, leisure and recreational
limitations• Issues of self confidence, self esteem• Effect on overall quality of life

Treatment Approaches to Stuttering
• stuttering modification
• fluency shaping

Stuttering Modification
• deals more directly with psychological aspects
• attitudes, feelings and emotions are addressed in therapy
• techniques include self-acceptance, attitude change, avoidance and anxiety reduction
• techniques employed to modify the moment of stuttering
Fluency Shaping• establishment of fluency within clinic setting• fluency is reinforced and gradually shaped to
approximate normal sounding speech• therapy procedures reconstruct the respiratory,
phonatory and articulatory gestures used in speech production
• no direct emphasis on fear or avoidance reduction
• transfer or generalization of skills is addressed

Behavioural Criteria for Successful Treatment
Outcome• significant, positive change in speech output
• generalization across speaking situations
• maintenance over time

Communication Criteria for Successful Treatment
Outcome• To be able to talk any time, any place and to any
body
• To be able to communicate effectively and efficiently
• And to be able to do so with little more than a normal amount of negative emotion.

Summary of our clinical and research findings with adults and adolescents who stutter
(Kroll and Scott-Sulsky, 2010)
What did we learn?

The Two Year Follow-up Study
18
2
7
02468
101214161820
Pre Post Follow-up
Percent WordsStuttered
Kroll & De Nil, 1994
Mean percent words stuttered for 14 subjects pretreatment, post treatment and at two year follow-up

The Two Year Follow-up Study
Mean total scores on the Situation Checklist
0
20
40
60
80
100
120
140
160
Pre Post Follow-up
SituationChecklist Score
Kroll & De Nil, 1994
N=14

Current Maintenance DataMean percent disfluency, SSI, PSI and STAI scores for 13 subjects
7.071.61 3.46
15.38.15 10.3
48
18 21
34.829.5 31.7
0
10
20
30
40
50
60
Pretreatment Posttreatment Follow-up
Percent DisfluenciesStuttering SeverityMean PSIMean STAI
De Nil & Kroll, 2003
So ……
The Treatment ProgramMust:• be based on science• be comprehensive• focus on observable behaviours• also deal with attitudes, feelings and emotions• be intensive• stress over learning and exaggeration• limit response variability• allow for immediate feedback

The Client
• have age appropriate reading and learning ability
• have emotional stability• have a degree of objectivity• have adequate performance
on trial probes• have family support
• have valid reasons for seeking treatment
• have realistic expectations and goals
• have realistic perceptions of therapy
• have realistic perceptions of stuttering
• be self-reliant and work independently
Must:

The Fluency Plus Program
Based on our clinical work and research findings with older
individuals, we applied these principles and developed our treatment program
for school aged children.

Fluency Plus Program
1. Speech Presents Complex Behavior
2. Primary Focus on Observable Behavior
3. Intensification of Treatment
4. Over-learning5. Exaggeration of
Speech Responses
6. Small Response Units Taught Individually
7. Sequential Synthesis of Response Units
8. Reduction of Response Variability
9. Immediate Feedback• re: Response Accuracy
Principles

Fluency Plus Program
10. Clinician As Instructor11. Clinician As Therapist12. Client Self-Pacing and
Self-Reliance13. Fading14. Family Involvement
15. Transfer Component16. Follow-Up and
Maintenance Program17. Post-Treatment
Support Groups18. Refresher Programs
Principles

Fluency Plus Program
• Establishment• Transfer• Maintenance
Critical Phases of Therapy

Targets
Speech gestures employed in speech production which are characterized by one or more designated properties of position,
force, velocity or duration.
Definition

Fluency Plus Program
Fluency facilitating procedures- Targets -
• Full Breath• Stretched Syllable• Gentle Onset• Light Contact• Blending• Full Movement

Response ProgressionSpeech Responses
C-V CombinationsMonosyllabic WordsBi-syllabic Words
Polysyllabic Words
Short Self-Generated ChainsLong Self-Generated Chains
Syllable Durations
2 Seconds/Syllable1 Second/Syllable1 Second/Syllable-½ Second/Syllable½ Second Syllable-New NormalNew NormalNew Normal

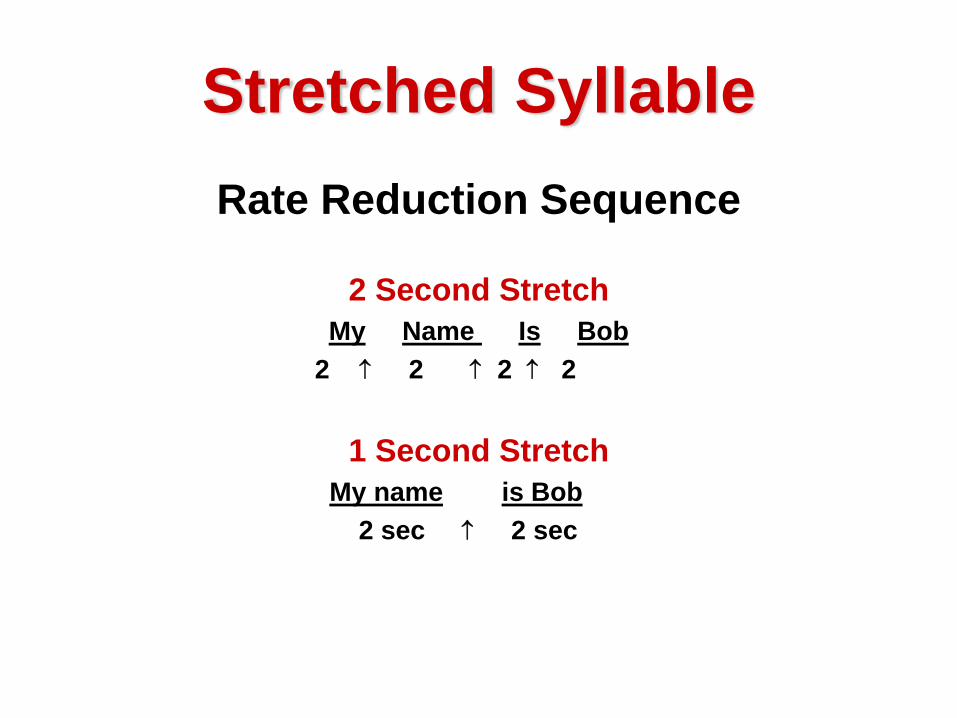
Stretched SyllableRate Reduction Sequence
2 Second StretchMy Name Is Bob
2 ↑ 2 ↑ 2 ↑ 2
1 Second StretchMy name is Bob
2 sec ↑ 2 sec

Stretched Syllable
Response Progression continued…..
½ Second StretchMy name is Bob
2 sec
New Normal – Syllable durations are not timed.Normal prosody and inflection restored

Full Breath Target
Definition: A full and controlled inhalation/ exhalation cycle with the diaphragm as the major muscle contributor
Purpose: To correct learned faulty breathing patternsTo facilitate the reconstruction of voicing characteristics

3 Steps of the Full Breath Target
1. Take a slow, comfortable breath by movingthe diaphragm out.
2. Don't pause between inhaling and exhaling.3. Exhale by relaxing the diaphragm - don't
push.

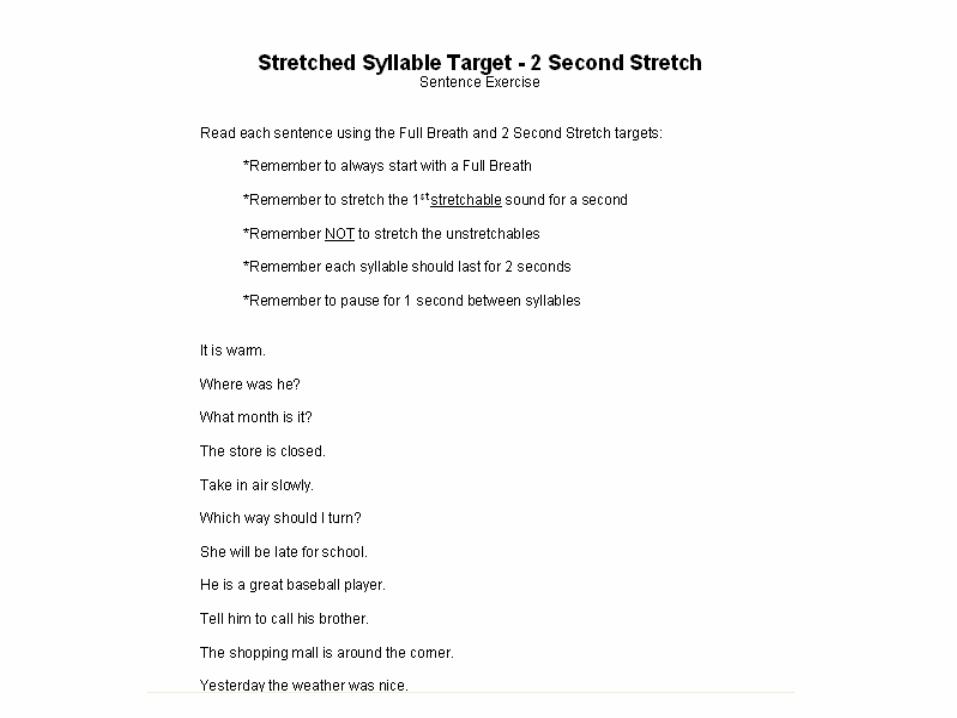
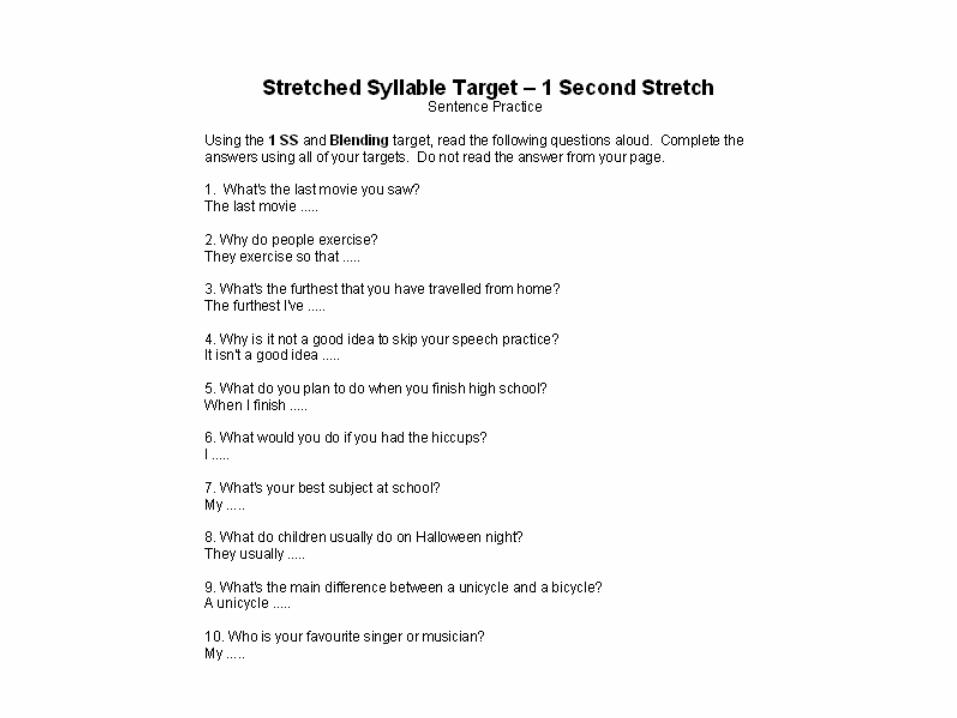
Stretched Syllable Target
Definition: The duration of each syllable, and each sound within the syllable is exaggerated well beyond normal limits
Purpose: To enhance the client’s awareness of the specific motor movements of speechTo provide a foundation of fluent speech which can then be systematically shaped towards normal patterns.

The 4 Rules of 2 Second Stretched Syllable Target:1. Each syllable is stretched for 2 seconds (example:
zzzziip = 2 seconds)2. The first sound in the syllable is held for 1 full
second. Your mouth should keep still while holding the sound for one second (example: zzzziip, the "zzzz" is held for 1 second).
3. The rest of the syllable gets the other 1 second: "zzzz(1 sec)iiip(1 sec).
4. If you have a word with more than one syllable, you must pause for 1 full second in between syllables and take a Full Breath (the Full Breath target).

Unstretchables
• Referred to as “hissing” and “popping” sounds
• Consist of the voiceless fricatives and plosives
• These sounds are not stretched to avoid excessive air loss or to avoid the build up of articulatory pressure



Gentle Onset TargetDefinition: An initial low amplitude vibration of the
vocal folds followed by a steady and gradual increase in the strength of these vibrations
Purpose: To facilitate proper phonatory onsets. To reduce the abrupt, excessive tensioning of the vocal folds and the forceful expulsion of air characteristic of laryngeal block.

5 Steps of the Gentle Onset Target
1. Take a slow, full breath.2. Start the voice very gently, that is, very
softly.3. Raise the loudness of your voice very
gradually.4. Raise the loudness to your normal
conversational loudness level, or slightly louder if you speak softly.
5. Decrease your loudness back down to where you began the onset





Light Contact Target
Definition: A reduction of air flow through the vocal tract.
Purpose: To prevent excessive air loss on voiceless fricative sounds
To ensure correct initiation of voicing on subsequent sounds
Voiceless Fricative Sounds


Light Contact Target
Definition: Light contacts of the peripheral articulators
Purpose: To prevent excessive lip and tongue pressure build-up on plosive sounds
To ensure correct initiation of voicing on subsequent sounds.
Plosive Sounds


Stretched SyllableRate Reduction Sequence
2 Second StretchMy Name Is Bob
2 ↑ 2 ↑ 2 ↑ 2
1 Second StretchMy name is Bob
2 sec ↑ 2 sec


Blending TargetDefinition: Variation of the amplitude and
blending of syllables within the speech chain
Purpose: To facilitate the initiation of syllables embedded within the words and phrases
To improve speech flow and prosody

Blending Target• Constant voicing between syllables• Gentle Onset on each syllable
oooovvvveeeennnn


Paragraph Reading
My fa/vourite/ drink is/ iced tea./ I rea/lly en/ joy a/ cold drink/ on a/ hot day./ Sometimes/ my bro/ther likes/ his iced/ tea fla/voured with/ lemon./
Full Movement Target
Definition: The full and deliberate movement of the articulators from sound to sound within syllables
Purpose: To decrease physical tensioning in jaw and neck areas
To facilitate kinesthetic perception of other target behaviors

Stretched Syllable
Response Progression continued…..
½ Second StretchMy name is Bob
2 sec
New Normal – Syllable durations are not timed.Normal prosody and inflection restored


Stretched Syllable
Response Progression continued…..
½ Second StretchMy name is Bob
2 sec
New Normal – Syllable durations are not timed.Normal prosody and inflection restored
New Normal Speech
Definition: New normal is defined as that rate of speech which is stretched enough to feel the targets being completed accurately but natural enough to be able to transfer to all outside speaking situations.






Transfer
The voluntary or conscious application of learned or acquired behaviors
outside of the clinic situation.
Definition:


Transfer Procedures
1. Mental Rehearsal
2. Talking While Applying Targets
3. Objective Evaluation
Cognitive and Speech Motor Processes


Mental Rehearsal• The mental or preparatory set with
which the individual enters a speaking situation
• The first step of transfer• Should be positive as opposed to
negative
Evaluation
• Should be objective and in reference to target behaviours
• Should be written down• Should be used in subsequent transfers

Fluency Types
1. Lucky (Unmonitored)
2. Monitored

When is Transfer Introduced?
• Not too early in the program– Exaggerated forms of speech do not transfer
easily to natural speech situations.• Not too late in the program
– Delaying transfer may feed the child’s fears of specific speech situations. Emphasis should be placed on the fact that some forms of transfer have been accomplished earlier in the program.


What is the Major Problem Encountered During
Transfer?• The link between the clinic and the outside
world is not made• The transfer experience is not viewed as
an opportunity to practice• The client is waiting for fluency skills to
happen (the medical model)• The client is overcome by negative
emotion
The Stuttering Mentality
“I hope the teacher doesn’t call on me because I’ll blow it!”
“Maybe I’ll just pretend I don’t know the answer.”
“I hope they don’t ask me to introduce myself.”
“Uh-oh! Here comes a word that starts with a “D”. Let me pick another one - fast!”
“I know they are going to laugh at me if I stutter.”
“I don’t want to answer the phone, I might stutter.”

Monitored Speech Output
Broca’s Area
Premotor Area
(Motor Speech Area and message formulation)
Motor : execution Act of talking
Motor Planning of:
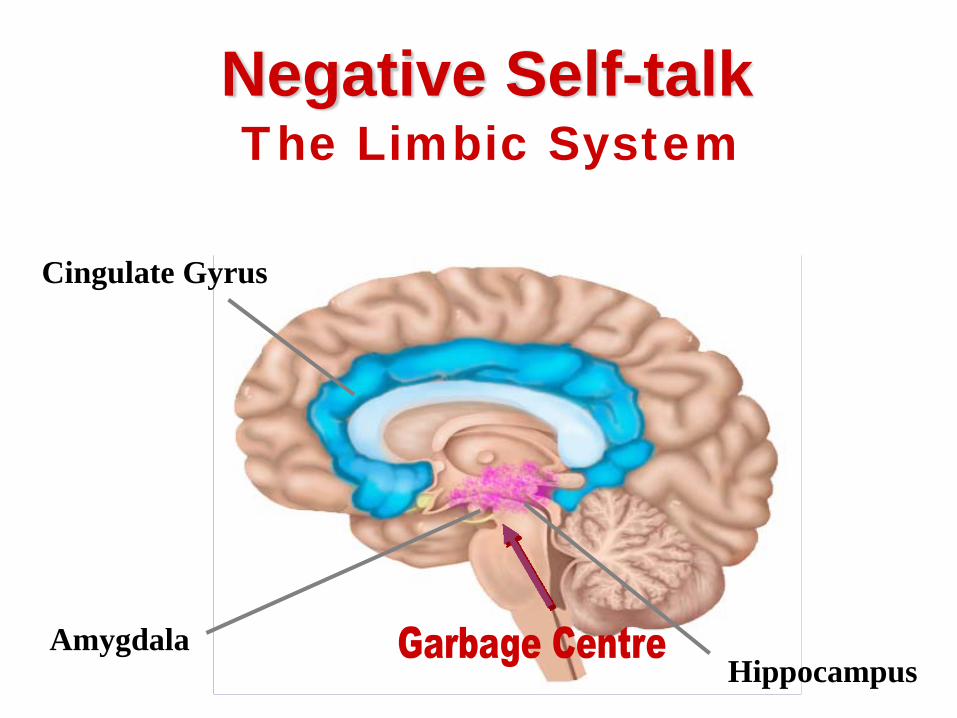
Negative Self-talkThe Limbic System
Cingulate Gyrus
AmygdalaHippocampus

Cognitive RestructuringDefinition- The alteration of attitudes, feelings, belief systems and emotions associated with the act of speech communication. This is accomplished by replacing faulty or irrational thought with more accurate and beneficial ones through supported self-realization and counseling.

Positive Self-talkSilent, internal messages regarding the
speaking situation or speaking performance.
Can be negative or positivePositive self-talk should serve as a mental
reminder to use target behaviours
“I will block for sure on my name”=>”Remember to use LC and GO”
“This person is in a rush, I better talk fast”=>”I will use SS and FM and I will be in control of how I speak”



Following Speech Hierarchies During Transfer• The danger here is encouraging the notion that
the situation is causing stuttering• The basic premise of fluency shaping therapy is
that violations of speech mechanics will ultimately lead to stuttering, not specific speech situations
• Thus, desensitization procedures are often not necessary, especially with children

What is the transfer process for younger children?
• In some cases transfer occurs spontaneously, depending on the age, sophistication and awareness level of the child
• The transfer process for older children exhibiting specific fears is very similar to that for adults

Maintenance
The continuation of the therapy program as the involvement of the clinician is gradually decreased.
Fluency maintenance is a long, gradual process of consolidation and stabilization of skills, and maturing of expectations by both the client and the therapist.
Definition:

What is the clinician’s role in maintenance?
• To provide on-going professional evaluative feedback during follow-up sessions
• To monitor practice schedules• To ensure that correct skills are being practiced
for appropriate lengths of time• To deal with psychological and behavioural
issues as they arise

When does the maintenance process begin?
• When the client can reliably transfer newly acquired speech skills in a variety of extra clinical situations
• When the stuttering mentality is replaced by a speech communication mentality

What are some of the challenges during maintenance?
1. Acceptance of modified speech pattern2. Constructive analysis of error patterns including
objective weighting of successes and failures3. Willingness to continually plus actively monitor speech4. Contingency plans to deal with anxiety and/or cognitive
demands of the dual speech process5. Acceptance of role and responsibility of fluent speech6. Acceptance of responsibility for the clinical process7. Possible alteration of perceived situational speech
difficulty8. Attitudinal and psychological changes

When is maintenance complete?
• When speech is no longer considered an issue
• Observed confidence and comfort level for communication
• Frequency and severity of disfluencies are minimal
Maintenance Practice Strategies
• Shaping• Structured transfer• Spontaneous transfer• Target review

Shaping• Daily practice of all targets and speech rates
to reinforce skill accuracy• Consists of reading aloud at each speech
rate, followed by a monitored conversation with a partner
1 minute full breath+ 3 minutes 2 second syllable stretch+ 4 minutes 1 second syllable stretch+ 6 minutes ½ second syllable stretch+ 6 minutes new normal= 20 minutes (reading) +10 minutes (conversation) = 30 minutes in total

Group vs. Individual Formats
• Group formats are ideal for children aged 7 and up
• Group activities encouraged• Reduces waiting time• Healthy competitive spirit ensures
program compliance• Children younger than 7 often not ready
for group

Group Therapy Formats
10 – 12 Year Olds:
• 26-28 weeks for establishment and transfers• “Speech partner” does not attend group
sessions• 5 children (maximum) per group

Group Therapy Formats7 – 9 Year Olds:
• 14-16 weeks for establishment and transfer• “speech partner” attends all group
sessions• 5 parent child pairs (maximum) per group• Rate reduction strategies replaced by
general instructions and modelling

The Role of the Parent/Caregiver
• To understand the nature of stuttering• To understand the goals of treatment• To serve as the child’s “speech partner”• To attend all parent meetings• To consult with SLP on a continual basis• To learn and model all speech targets• To carry out home practice with child• To create a home environment conducive to fluency• To educate family members• To liaise with the teacher

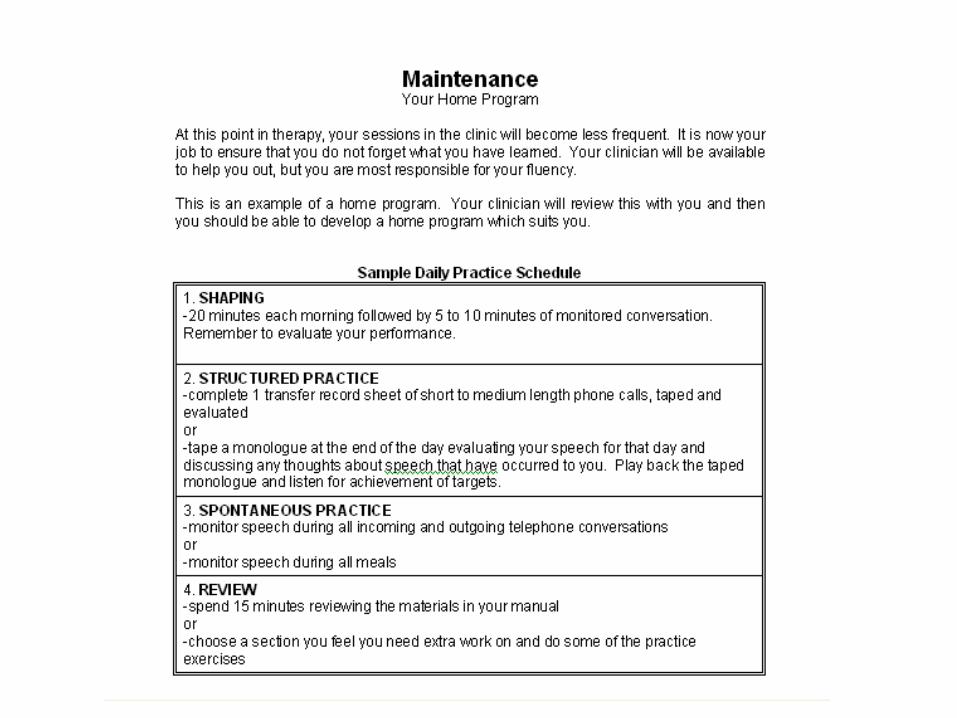
Home Practice• Instructions for practice should be clear
and formalized– Written down– Practice sheets provided– Recording devises used to:
• Provide samples of individual speech targets• Allow SLP to determine completeness and accuracy
of home assignments– Practice sessions conducted daily– Sessions should be 20-30 minutes in duration

Intensive Therapy• Can refer to in-clinic or extra-clinic
sessions• Eliminates spaced practice and retention
issues• Ensures experience of speech gain• Facilitates generalization of speech skills• Reduces client dependence on SLP• Challenges priorities and commitment• Builds in-home programming

Use of Video Recordings• Provides pre and post treatment fluency
count data • Visual record of stuttering and stuttering
contingent behaviours• Allows clients to examine their pretreatment
speech patterns • Allows for objective evaluation of target
behaviours during speech activities such as group presentations

The Younger Child• Children younger than 8 typically lack the
conceptual abilities for many of the details in Fluency Plus
e.g. Stretched syllables replaced by modeling “easy talking”
• Clinical materials and activities modified for this age group
• Parents attend all sessions• Parents assigned role of learning partner and
facilitator in clinic and at home

Pre/Post Data (Conversation)on 26 Children 9-12 years
02468
10121416
0-5% 6-10% 11-15%
16-20%
21-25%
26-30%
>30%
Pre-therapyPost-therapy
Percentage of dysfluency in conversation
Total Num
ber of Children

Pre/Post Data on 11 Children in the 7-9 Year Old Program
(
0
1
2
3
4
5
6
0-5% 6-10% 11-15%
16-20%
21-25%
26-30%
>30%
Pre-therapyPost-therapy
Percentage of dysfluency in conversation
Total Num
ber of Children

Pre/Post Data on 8 Children in the 5-6 Year Old Program
00.5
11.5
22.5
33.5
44.5
5
0-5% 6-10% 11-15%
16-20%
21-25%
26-30%
>30%
Pre-therapyPost-therapy
Percentage of dysfluency in conversation
Total Num
ber of Children

Questions, Discussion, etc.Robert Kroll, Ph.D.Executive DirectorThe Speech and Stuttering Institute2-150 Duncan Mill RoadToronto, Ontario M3B 3M4
Tel. 416 491 7771Email [email protected]