flor salınımı yapan ortodontik kompozitlerin ... - 111.pdf · 16-18). flor salınımı yapan...
TRANSCRIPT
Yrd.Doç.Dr. Fırat ÖZTÜRK*Yrd.Doç.Dr. Ebubekir TOY*Yrd.Doç.Dr. Uğur ARSLAN**Dt. Erdem HATUNOĞLU*
Yaz›flma Adresi/Corresponding Author:
Dr. Fırat Öztürkİnönü Üniversitesi, Dişhekimliği
Fakültesi, Ortodonti A. D. Malatya Turkey
E-posta: [email protected]
* İnönü Üniv. Dişhek. Fak.Ortodonti A. D. Malatya, **
Selçuk Üniv. Selçuklu Tıp Fak.Mikrobiyoloji A. D. Konya /
*İnönü Univ. Faculty ofDentistry, Dept. of
Orthodontics, Malatya,**Selçuk Univ., Selçuklu
Faculty of Medicine, Dept. ofMicrobiology, Konya, Turkey
ÖZET
Amaç: Bu çalışmanın amacı DirektKontakt Testi (DKT) kullanılarak; üç farklıtipte flor salınımı yapan ortodontikkompozitin antibakteriyel özelliklerinindeğerlendirilmesidir. Gereçler ve Yöntem:Flor salınımı yapan ortodontik kom-pozitlerin antibakteriyel özellikleri DKTkullanılarak değerlendirildi. DKT içindoksan altı kuyucuklu kültür kabınınduvarları her grupta 8 örnek olacak şekildetest materyalleri ile [Transbond Plus (3MUnitek, Monrovia, ABD) Light Bond(Reliance Ortho Prod. Inc. Itasca, IL, ABD)Kurasper F (Kuraray Medical Inc., Okayama,Japonya)] kaplandı. Pozitif kontrol materyaliolarak Kalzinol (çinko oksit öjenol siman)(Dentsply, Konstanz, Almanya) kullanıldı.Streptococus mutans süspansiyonuörneklerin yüzey alanına uygulanarak37oC’de bir saat bekletildi. Bakteri üremesi,ısı kontrollü spektrofotometre ile 16 saatboyunca gözlemlendi. Herbir kuyucuktakiüremenin kinetiği her 30 dakikada bir 650nm düzeyinde sürekli olarak kaydedildi.Veriler tek yönlü ANOVA testinin yanı sıraTamhane’ın T2 çoklu karşılaştırma testi ileincelendi. İstatistiksel önem seviyesi P<0.05olarak belirlendi. Bulgular: DKT sonuç-larının değerlendirilmesi dört grup arasındaistatistiksel olarak anlamlı farklar olduğunuortaya koymuştur. (F= 156,951, P= 0.000).Kontrol materyali olan Kalzinol bakteriüremesini tamamen engellemiştir (ortalama0.01±0.05). Çoklu karşılaştırma testi,Kalzinol ve Transbond Plus (ortalama0.12±0.17) arasında anlamlı bir farkolmadığını göstermiştir (P= 0.509)Transbond Plus, Kalzinol ile hemen hemenbenzer etkinlik sergilemiştir (Şekil 1).Kurasper F (ortalama 0.73±0.06) ve LightBond (ortalama 0.85±0.02) ise Kalzinol’lekarşılaştırıldığında istatistiksel olarak anlamlıbir fark göstermiştir (P= 0.000) Sonuç:Transbond Plus belirgin antibakteriyeletkinlik göstermiştir. (Türk Or to don ti Der gi si2011;24:3-12)
Anah tar Ke li me ler: Flor, Antibakteriyelajanlar, Ortodontik adezivler
Gönderme: 21.04.2011Kabul: 17.05.2011
SUM MARY
Aim: The purpose of this study was toevaluate the antibacterial effects of 3different fluoride-releasing orthodonticcomposites using a direct contact test(DCT). Materials and Methods: Theantibacterial properties of fluoridereleasing orthodontic composites wereevaluated with the DCT. For the DCT,wells (n=8) of 96-microtitre plates werecoated with the tested bonding adhesives[Transbond Plus (3M Unitek, Monrovia,USA) Light Bond (Reliance Ortho Prod.Inc. Itasca, IL, USA) Kurasper F (KurarayMedical Inc. Okayama, Japan)]. Kalzinol(Zinc-Oxide Eugenol Cement) (Dentsply,Konstanz, Germany was used as apositive control material. A Streptococcusmutans suspension was placed on thesurface of each specimen for 1 hour at37°C. Bacterial growth was monitored for16 hours with a temperature-controlledmicroplate spectrophotometer. Thekinetics of the outgrowth in each well wasrecorded continuously at 650 nm every30 minutes. The data were analyzed byone-way ANOVA, as well as byTamhane’s T2 multiple comparison test.The level of significance was determinedas P < 0.05. Results: The evaluation of theresults of the DCT revealed that therewere statistically significant differencesbetween the four groups (F= 156,951, P=0.000). The control material (Kalzinol)showed complete inhibition of bacterialgrowth (mean 0.01±0.05). The multiplecomparison test indicated that there wereno significant difference in bacterialgrowth between Kalzinol and TransbondPlus (mean 0.12±0.17) (P= 0.509)..Kurasper F (mean 0.73±0.06) and LightBond (mean 0.85±0.02) showedstatistically significant differences (P=0.000) compared to Kalzinol.Conclusion: Transbond Plus showedmarked antibacterial effects. (Turkish JOrthod 2011;24:3-12)
Key Words: Fluorides, Antibacterialagents, Orthodontic adhesives.
Date Submitted: 21.04.2011Date Accepted: 17.05.2011
ARAfiTIRMA / ARAfiTIRMA / RESEARCHRESEARCH
Flor Salınımı Yapan Ortodontik Kompozit ler inFlor Salınımı Yapan Ortodont ik Kompozit ler in
Ant ibakter iyel Etkiler i: Pilot ÇalıAnt ibakteriyel Etkiler i: Pilot Çalışşmama
Ant ibacter ial Ef fects of Fluor ide-Releasing OrthodonticAntibacterial Effects of Fluoride-Releasing Orthodont icComposites: A Pilot StudyComposites: A Pilot Study
Turkish Journal of Orthodontics 2011;24:3-123
fırat:muammer 7/14/11 11:07 AM Page 3
Turkish Journal of Orthodontics 2011;24:3-125
Ortodontik kompozitlerin antibakteriyel etkileriAntibacterial effects of orthodontic composites
test materyali ile incelenen mikroorganizmaarasındaki direk ve yakın kontak etkisini nicelolarak ölçmeye yarar (14).Farklı rezin materyallerinin antibakteriyel
özellikleri birkaç araştırmada belirlenmiştir (15,16-18). Flor salınımı yapan ortodontik kompo-zitlerin antibakteriyel özelliklerini inceleyen biraraştırma yoktur. Bu çalışmanın amacı florsalınımı yapan üç farklı ortodontik kompozitinantibakteriyel etkilerini DKT ile incelemektir.
GEREÇLER ve YÖNTEMÇalışmada kullanılan flor salınımı yapan
kompozitler ve kontrol materyali Tablo 1’degösterilmiştir. Streptococcus mutans (RefikSaydam National Public Health, 676) deneytasarımına göre örneklere uygulanmadanönce, 37oC’de 48 saat süreyle 0,5%Bacitracin içeren “brain hearth infusion”(BHI) besi yerinde dondurulmuş kültürlerdenaerobik olarak üretilmiştir.DKT (14) 96 kuyucuklu kültür kabında
bakteri büyümesinin turbidometrik olarakbelirlenmesine dayanır (96-well, flat-bottomNunclon; Nunc, Kopenhag, Danimarka). Herbir kuyucuktaki büyüme kinetiği, ısı kontrollüspektrofotometre cihazı (µquant, Bio-TekInstruments Inc. Winooski VT, ABD)kullanılarak 650 nm dalga boyu düzeyindeher 30 dakikada bir devamlı olarakkaydedilir. Her bir kuyucukta, kültür kabı dikyönde tutularak (yani kültür kabının yüzeyiyere dik olacak şekilde) yan yüzeyler testmateryali ile kaplanır.Araştırmamızda, ışıkla sertleşen primer
(Transbond Plus Paste ile kullanılanTransbond Plus Self Edge Primer (3M Unitek,Monrovia, ABD) fırçayla kuyucukların yanduvarına sürüldü. İnce bir film tabakasıolmasına dikkat edildi. Sonra düzgün biryüzey alanı sağlamak için mikrobrush ileince bir adesiv katmanı uygulandı. Buçalışmada Kalzinol (çinko oksit ojenol siman)kontrol materyali olarak kullanıldı. Testörnekleri üretici firmanın önerilerine tama-men uygun olarak karıştırıldı, sertleşmeyebırakıldı veya ışıkla sertleştirildi. Kuyucuk-ların yan duvarları boyunca ışık geçişiniengelleyerek hatalı okumalara sebep olacağıiçin, materyalin kuyucukların altınaakmaması için son derece dikkatli davranıldı.10µL bakteri süspansiyonu her bir örneğeyerleştirildi ve dik konumda 37oC’de nemli
Türk Ortodonti Dergisi 2011;24:3-124
Öztürk, Toy, Arslan, Hatunoğlu
G‹ R‹fiOrtodontik tedavi gören hastalar tedavide
kullanılan apareylerden dolayı diştemizliklerini sağlamada güçlük çekerler.Braketlerin etrafında oluşan minedemineralizasyonları ortodonti hastalarındasık karşılaşılan komplikasyonlardandır (1).Artmış plak formasyonu ve eşlik edenbakteriyel asit üretimi braketlerin kenarındamine demineralizasyonuna neden olur (2).Bu demineralizasyonlar temel olarakStreptococus mutans’la ilişkili lezyonlardanoluşur (3). Ortodontik tedavi görenhastalarda bu bakterilerin tükrük ve plakseviyelerinde önemli bir artış vardır (4,5).Sabit apareyler kullanan hastalardaki yenidemineralizasyon prevalansı %15 den %70’ekadar değişen aralıklarda bildirilmiştir (6,7).Çürük başlangıç lezyonları braketlerin
etrafında in vivo olarak dördüncü haftadansonra gösterildiği için, ortodontik tedavisüresince demineralizasyonun azaltılmasıve/veya önlenmesi için gerekli yöntemlerinbulunması son derece önemlidir (8). Flor,bugüne kadar en çok bilinen antikaryojenikajandır (8). Florun antikaryojenik etkisindebirçok mekanizma rol oynar. Bunlar içindedemineralizasyonun inhibisyonu, reminera-lizasyonun artırılması, plak oluşumununengellenmesi ve mikrobiyal artışın vemetabolizmanın durdurulması sayılabilir (9).Florun bakteriyel metabolizma ve dental plakasiditesini engelleyebilme mekanizması,bakteriyel kolonizasyonun yanı sıra glikolitikenzim enolazın ve proton salınımı yapanATPaz’ın inhibisyonunu içerir. Plak oluşumuylailgili enzimler olan asit fosfataz, pirofosfataz,peroksidaz ve katalaz enzimleri floriyonlarından etkilenebilmektedir (10). Flor seviyesi bakteriyel büyümeyi, dental
plak kompozisyonunu ve asit üretiminiazaltabilir (9). Resin kompozitler, inorganiktuzlar, ince cam partikülleri veya organik florgibi birçok formda flor içerebilir. Bu yüzden,sadece flor miktarı değil, aynı zamanda florludoldurucuların parçacık boyutu ve tipi,rezinin tipi, silan uygulaması ve pörözite deflor salınımına katkıda bulunan önemlifaktörlerdir (11,12). Bundan başka, florsalınımı polimer matriksin hidrofilitesi ve asitkarekteri ile artar (9,13). Direkt Kontakt Testi (DKT) bileşenlerinin
çözünürlük ve dağılabilirliğine bakmaksızın
IN TRO DUC TI ONPatients generally have difficulties in
maintaining adequate oral hygiene withorthodontic appliances. Demineralization ofthe enamel surface adjacent to theorthodontic brackets is a common adverseeffect of orthodontic treatment (1). Increasedplaque formation and the concomitantbacterial acid production result in enameldemineralization adjacent to the brackets (2).This enamel demineralization consistsprincipally of Streptococcus mutans-associated lesions (3) There is a significantincrease in the salivary and plaque levels ofthese bacteria in patients undergoing fixedappliance treatment (4,5). The prevalence ofnew demineralizations among orthodonticpatients with fixed appliances is reported torange from 15% to 75% (6,7).Because caries lesions have been
demonstrated in vivo around the bracketsafter only 4 weeks, finding methods ofreducing and preventing demineralizationduring orthodontic treatment is important (8).Fluoride is the most anticariogenic agentknown to date (8). A variety of mechanismsare involved in the anticariogenic effects offluoride, including the inhibition ofdemineralization, the enhancement ofremineralization, the prevention of pellicleand plaque formation, and the inhibition ofmicrobial growth and metabolism (9). Themechanisms by which fluoride may interferewith bacterial metabolism and dental plaqueacidogenicity include the inhibition of theglycolytic enzyme enolase and the proton-extruding ATPase as well as bacterialcolonization and competition (10).Fluoride levels may reduce bacterial
growth, dental plaque composition and acidproduction (9). Resin composites maycontain fluoride in a variety of forms, such asinorganic salts, leachable glasses or organicfluoride. Thereby, not only the amount offluoride, but also the type and particle size ofthe fluoridated filler, the type of resin, silanetreatment and porosity might be importantfactors contributing to fluoride release(11,12). Moreover, fluoride release increaseswith the hydrophicility and the acidcharacter of the polymer matrix (9,13).The direct contact test (DCT)
quantitatively measures the effect of directand close contact between the testmicroorganism and the tested materials,
fırat:muammer 7/14/11 11:07 AM Page 4
Turkish Journal of Orthodontics 2011;24:3-125
Ortodontik kompozitlerin antibakteriyel etkileriAntibacterial effects of orthodontic composites
test materyali ile incelenen mikroorganizmaarasındaki direk ve yakın kontak etkisini nicelolarak ölçmeye yarar (14).Farklı rezin materyallerinin antibakteriyel
özellikleri birkaç araştırmada belirlenmiştir (15,16-18). Flor salınımı yapan ortodontik kompo-zitlerin antibakteriyel özelliklerini inceleyen biraraştırma yoktur. Bu çalışmanın amacı florsalınımı yapan üç farklı ortodontik kompozitinantibakteriyel etkilerini DKT ile incelemektir.
GEREÇLER ve YÖNTEMÇalışmada kullanılan flor salınımı yapan
kompozitler ve kontrol materyali Tablo 1’degösterilmiştir. Streptococcus mutans (RefikSaydam National Public Health, 676) deneytasarımına göre örneklere uygulanmadanönce, 37oC’de 48 saat süreyle 0,5%Bacitracin içeren “brain hearth infusion”(BHI) besi yerinde dondurulmuş kültürlerdenaerobik olarak üretilmiştir.DKT (14) 96 kuyucuklu kültür kabında
bakteri büyümesinin turbidometrik olarakbelirlenmesine dayanır (96-well, flat-bottomNunclon; Nunc, Kopenhag, Danimarka). Herbir kuyucuktaki büyüme kinetiği, ısı kontrollüspektrofotometre cihazı (µquant, Bio-TekInstruments Inc. Winooski VT, ABD)kullanılarak 650 nm dalga boyu düzeyindeher 30 dakikada bir devamlı olarakkaydedilir. Her bir kuyucukta, kültür kabı dikyönde tutularak (yani kültür kabının yüzeyiyere dik olacak şekilde) yan yüzeyler testmateryali ile kaplanır.Araştırmamızda, ışıkla sertleşen primer
(Transbond Plus Paste ile kullanılanTransbond Plus Self Edge Primer (3M Unitek,Monrovia, ABD) fırçayla kuyucukların yanduvarına sürüldü. İnce bir film tabakasıolmasına dikkat edildi. Sonra düzgün biryüzey alanı sağlamak için mikrobrush ileince bir adesiv katmanı uygulandı. Buçalışmada Kalzinol (çinko oksit ojenol siman)kontrol materyali olarak kullanıldı. Testörnekleri üretici firmanın önerilerine tama-men uygun olarak karıştırıldı, sertleşmeyebırakıldı veya ışıkla sertleştirildi. Kuyucuk-ların yan duvarları boyunca ışık geçişiniengelleyerek hatalı okumalara sebep olacağıiçin, materyalin kuyucukların altınaakmaması için son derece dikkatli davranıldı.10µL bakteri süspansiyonu her bir örneğeyerleştirildi ve dik konumda 37oC’de nemli
regardless of the solubility and diffusibility oftheir components (14).Antibacterial properties of different resin
materials have been identified in a severalinvestigations (15,16-18). There have beenno studies that investigated the antibacterialeffects of fluoride releasing orthodonticcomposites. The purpose of the present studywas to asses and compare the antibacterialeffects of 3 different fluoride-releasingorthodontic composites using the DCT.
MATERIALS and METHODSThe fluoride-releasing composites and
control material used in this study are shownin Table 1. Streptococcus mutans (RefikSaydam National Public Health, 676) wasgrown aerobically from frozen stock culturesin brain hearth infusion (BHI) brothcontaining 0.5% Bacitracin for 48 hours at37ºC before applying it to the specimensaccording to the experimental design. The DCT (14) is based on the
turbidometric determination of bacterialgrowth in 96-well microtitre plates (96-well,flat-bottom Nunclon; Nunc, Copenhagen,Denmark). The kinetics of the outgrowth ineach well was recorded continuously at 650nm every 30 minutes, using a temperature-controlled spectrophotometer (µquant, Bio-Tek Instruments Inc., Winooski VT, USA). Inall the wells, the sidewall was coated withthe tested material while the plate was heldvertically (i.e. the plate’s surface wasperpendicular to the floor). In our study, light-cured primers
(Transbond Plus Self Etch Primer used withTransbond Plus Paste) were brushed on andapplied to the sidewalls of the wells. Carewas taken to have a thin film thickness. A thincoat adhesive was applied with a microbrush to ensure a uniform surface area. In thisstudy Kalzinol (Zinc-oxide Eugenol cement)was used as a control material. The testsamples were mixed, and were allowed toset, or else were light polymerized in strictcompliance with the manufacturers’recommendations. Special care was taken toavoid the material’s flow to the bottom of thewell, which would interfere with the lightpath through the microplate well and wouldresult in a false reading. A 10µL bacterialsuspension was placed on each sample andincubated in a humid atmosphere at 37°C forone hour while the plate remained in a
Türk Ortodonti Dergisi 2011;24:3-124
Öztürk, Toy, Arslan, Hatunoğlu
IN TRO DUC TI ONPatients generally have difficulties in
maintaining adequate oral hygiene withorthodontic appliances. Demineralization ofthe enamel surface adjacent to theorthodontic brackets is a common adverseeffect of orthodontic treatment (1). Increasedplaque formation and the concomitantbacterial acid production result in enameldemineralization adjacent to the brackets (2).This enamel demineralization consistsprincipally of Streptococcus mutans-associated lesions (3) There is a significantincrease in the salivary and plaque levels ofthese bacteria in patients undergoing fixedappliance treatment (4,5). The prevalence ofnew demineralizations among orthodonticpatients with fixed appliances is reported torange from 15% to 75% (6,7).Because caries lesions have been
demonstrated in vivo around the bracketsafter only 4 weeks, finding methods ofreducing and preventing demineralizationduring orthodontic treatment is important (8).Fluoride is the most anticariogenic agentknown to date (8). A variety of mechanismsare involved in the anticariogenic effects offluoride, including the inhibition ofdemineralization, the enhancement ofremineralization, the prevention of pellicleand plaque formation, and the inhibition ofmicrobial growth and metabolism (9). Themechanisms by which fluoride may interferewith bacterial metabolism and dental plaqueacidogenicity include the inhibition of theglycolytic enzyme enolase and the proton-extruding ATPase as well as bacterialcolonization and competition (10).Fluoride levels may reduce bacterial
growth, dental plaque composition and acidproduction (9). Resin composites maycontain fluoride in a variety of forms, such asinorganic salts, leachable glasses or organicfluoride. Thereby, not only the amount offluoride, but also the type and particle size ofthe fluoridated filler, the type of resin, silanetreatment and porosity might be importantfactors contributing to fluoride release(11,12). Moreover, fluoride release increaseswith the hydrophicility and the acidcharacter of the polymer matrix (9,13).The direct contact test (DCT)
quantitatively measures the effect of directand close contact between the testmicroorganism and the tested materials,
fırat:muammer 7/14/11 11:07 AM Page 5
Turkish Journal of Orthodontics 2011;24:3-127
Ortodontik kompozitlerin antibakteriyel etkileriAntibacterial effects of orthodontic composites
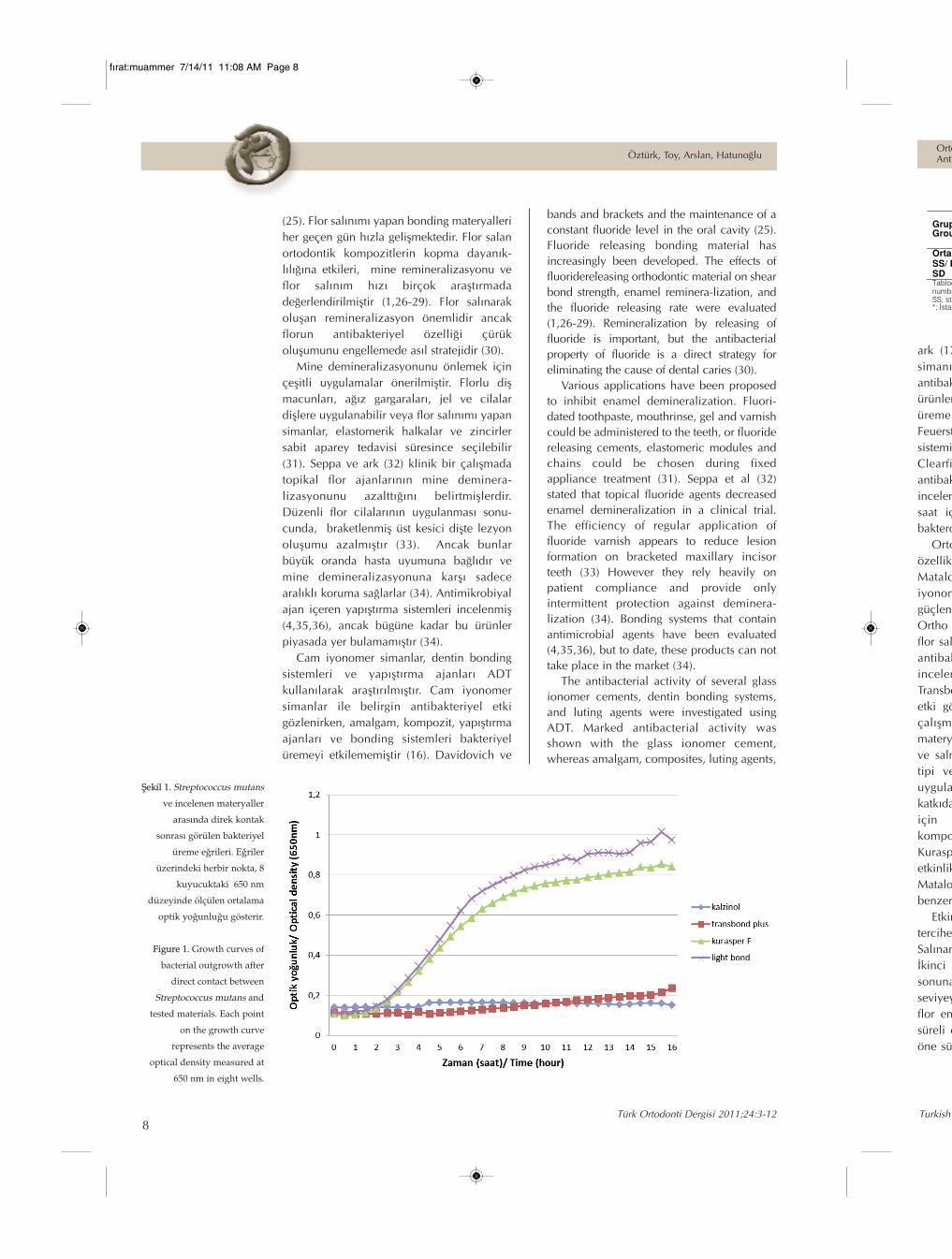
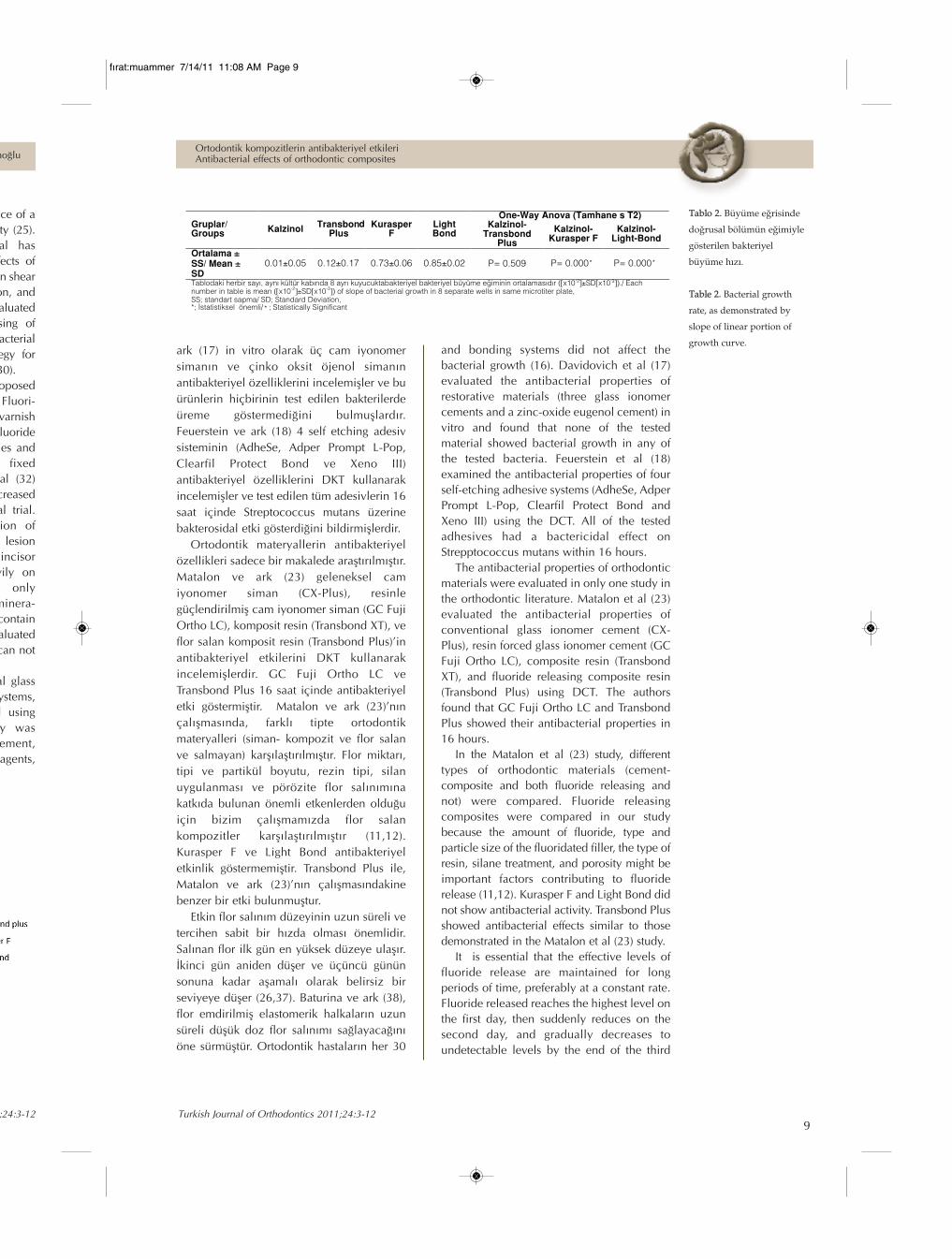
ve Tablo 2’de sunulmuştur. Büyümeeğrisindeki her bir nokta Şekil 1’dekiherhangi bir zamanda her bir gruptaki 8kuyucukta ölçülen ortalama optik yoğunluğuverir. Her bir eğri 16 saat içinde alınan 32ölçümü içerir. DKT sonuçlarının değer-lendirilmesi dört grup arasında istatistikselolarak anlamlı farklar olduğunu ortayakoymuştur (F= 156,951, P= 0,000). Kontrolmateryali olan Kalzinol bakteri üremesinitamamen engellemiştir (ortalama 0,01±0,05). Çoklu karşılaştırma testi, Kalzinol veTransbond Plus (ortalama 0,12±0,17)arasında anlamlı bir fark olmadığınıgöstermiştir (P= 0,509) Transbond Plus,Kalzinol ile hemen hemen benzer etkinliksergilemiştir (Şekil 1). Kurasper F (ortalama0,73±0,06) ve Light Bond (ortalama0,85±0,02) ise Kalzinol’le karşılaştırıldığındaistatistiksel olarak anlamlı bir farkgöstermiştir (P= 0,000).
TARTIŞMABeyaz nokta lezyonları sabit ortodontik
tedavi görmüş hastaların %50’ye yakınındarapor edilmiştir (6,19). Ortodontik tedavisonrası görülen demineralizasyonlarınyüksek prevalansına braketlere bitişikStreptococcus mutans sayısındaki artış sebepolmaktadır (20). Bu araştırma, TransbondPlus’ın Streptococcus mutans üremesiniinhibe ettiğini göstermiştir. Çalışmamızdaçürüğün birincil etiyolojik etkeni ve çürüklezyonlarından sıklıkla izole edilenStreptococcus mutans deney mikro-organizması olarak kullanıldı. Streptococcusmutans dişhekimliğinde restoratif mater-yallerin antimikrobiyal etkinliğinin sınan-masında yaygın olarak kullanılmıştır(14,21,22). Streptococcus mutans üremesi buaraştırmada DKT kullanılarak değerlendirildi.Yapılan çalışmalarda dental ürünlerinantibakteriyel etkinliği hem ayar difüzyontesti (ADT) hem de DKT ile incelenmiştir(15,22-24). DKT dental ürünlerin anti-bakteriyel etkisini belirlemede ADT’ye göredaha etkin bulunmuştur (15).Sabit apareylerle tedavi gören hastalarda
çürük başlangıç lezyonlarının gelişiminiengellemek için alınacak önlemler, bant vebraketlerin çevresinde oluşan bakteriyelplağın kontrolüne ve ağız boşluğunda sabitbir flor seviyesi sağlanmasına odaklanmıştır
Türk Ortodonti Dergisi 2011;24:3-126
Öztürk, Toy, Arslan, Hatunoğlu
bir ortamda bir saat inkube edildi. Bu sürezarfında süspansiyon likitinin çoğu buharlaş-tırılarak bütün bakteriler ve test materyalininyüzeyi arasında direk kontak sağlandı.Bundan sonra her bir kuyucuğa 220 µL
BHI besi yeri eklendi ve spektrofotometreyeyerleştirildi. Bakteri üremesi 16 saat boyuncaher 30 dakikada bir, 650 nm düzeyinde optikokuyucu ile otomatik olarak ölçülerekkaydedildi. Deney tasarımına paralel olarak,sayısal ve tekrarlanabilir tarzda, deneyşartları altında bakteriyel üremeyi saptamakiçin kalibrasyon deneyleri yapıldı (14).
İstatistiksel AnalizHer bir kuyucuk için bakteriyel büyüme
eğrileri analiz edildi ve lineer regresyonuy=ax+b denklemi kullanılarak hesaplandı. Budenklem ilgili büyüme hızıyla ilişkili eğimdeğerini sağladı.Tüm istatistiksel analizler SPSS 10.3
yazılım programı ile yapılmıştır (SPSS forWindows 13.0; SPSS, Chicago, Ilionis, ABD).Dört grubun herbiri için ortalama, standartsapma, minimum ve maksimum değerleriiçeren tanımlayıcı istatistikler hesaplandı.Shapiro-Wilks’in normalite ve Levene’invaryans homojenite testleri yapıldı. Verilernormal dağılım gösterdi ve gruplar arasındavaryansın homojen olduğu görüldü. Verilertek yönlü ANOVA testinin yanı sıraTamhane’ın T2 çoklu karşılaştırma testi ileincelendi. İstatistiksel önem seviyesi P<0.05olarak belirlendi.
BULGULARKalibrasyon deneyleri, sayısal ve
tekrarlanabilir tarzda, kültür kabındabakteriyel üremenin izlendiğini göstermiştir.Doksan altı kuyucuklu kültür kabındaStreptococcus mutans büyümesi Şekil 1’de
vertical position. During that time, most ofthe suspension liquid evaporated, ensuringdirect contact between all bacteria and thetested material surface. Then, 220 µL of BHIbroth was added to each of the wells and theplate was placed in the spectrophotometer.
The bacterial outgrowth was estimatedafter direct contact with the tested materialon the basis of the changes in the readings ofoptical density at 650 nm, which wererecorded automatically by the spectrop-hotometer every 30 minutes for 16 hours.Parallel to the experimental setup, calibrationexperiments were performed to establishbacterial outgrowth under experimentalconditions in a quantitative and reproduciblemanner (14).
Statistical Analyses Bacterial growth curves for each well were
analyzed and a regression line on theascending linear portion of the curve wascalculated, using the equation y = ax + b.This equation provided the value of the slopecorresponding to the growth rate. All statistical analyses were performed
using the Statistical Package for SocialSciences, version 13.0 for Windows (SPSS forWindows 13.0; SPSS, Chicago, Ilionis, USA).Descriptive statistics, including the mean,standard deviation, minimum and maximumvalues, were calculated for each of the fourgruops. Shapiro-Wilks normality and Levene’svariance homogeneity tests were applied tothe data. The data showed normal distrubitionand there were homogeneity of variancesamong the groups. The data were analyzed byone-way ANOVA, as well as by Tamhane’s T2multiple comparison test. The level ofsignificance was determined as P < 0.05.
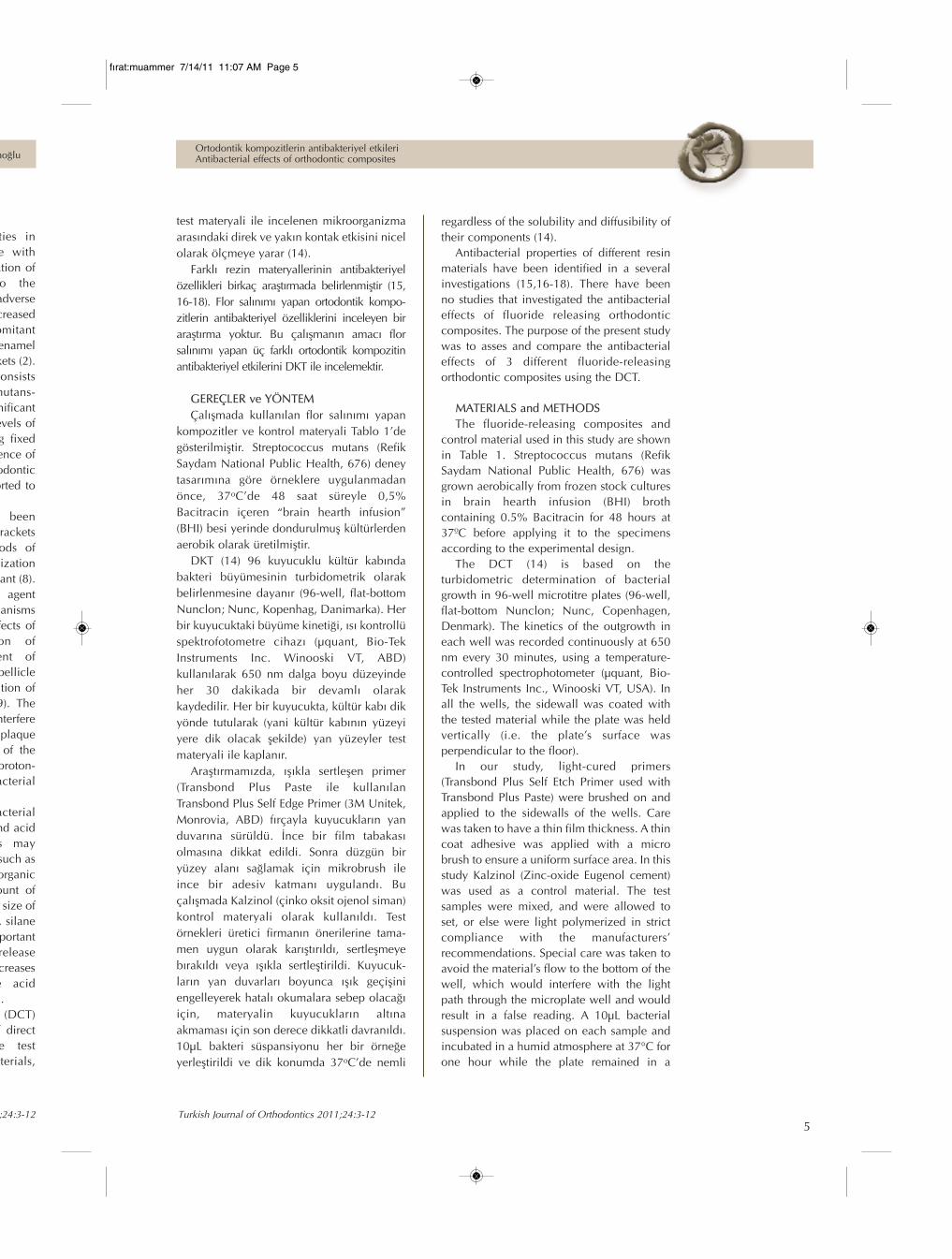
Tab�lo�1.�Çalışmada
kullanılan�ortodontik
materyaller.
Table�1. Orthodontic
materials�used�in�this�study.
fırat:muammer 7/14/11 11:08 AM Page 6

Turkish Journal of Orthodontics 2011;24:3-127
Ortodontik kompozitlerin antibakteriyel etkileriAntibacterial effects of orthodontic composites
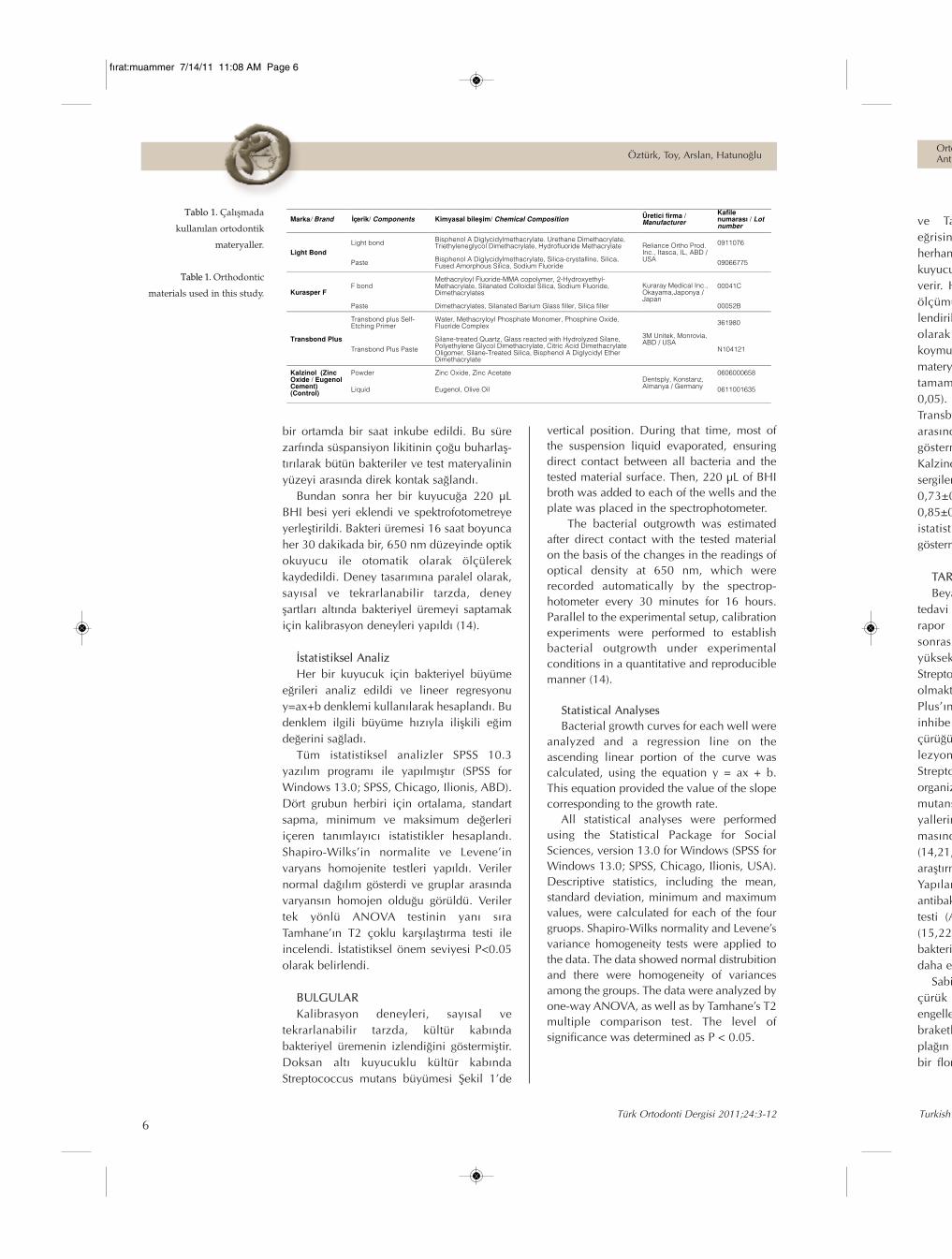
ve Tablo 2’de sunulmuştur. Büyümeeğrisindeki her bir nokta Şekil 1’dekiherhangi bir zamanda her bir gruptaki 8kuyucukta ölçülen ortalama optik yoğunluğuverir. Her bir eğri 16 saat içinde alınan 32ölçümü içerir. DKT sonuçlarının değer-lendirilmesi dört grup arasında istatistikselolarak anlamlı farklar olduğunu ortayakoymuştur (F= 156,951, P= 0,000). Kontrolmateryali olan Kalzinol bakteri üremesinitamamen engellemiştir (ortalama 0,01±0,05). Çoklu karşılaştırma testi, Kalzinol veTransbond Plus (ortalama 0,12±0,17)arasında anlamlı bir fark olmadığınıgöstermiştir (P= 0,509) Transbond Plus,Kalzinol ile hemen hemen benzer etkinliksergilemiştir (Şekil 1). Kurasper F (ortalama0,73±0,06) ve Light Bond (ortalama0,85±0,02) ise Kalzinol’le karşılaştırıldığındaistatistiksel olarak anlamlı bir farkgöstermiştir (P= 0,000).
TARTIŞMABeyaz nokta lezyonları sabit ortodontik
tedavi görmüş hastaların %50’ye yakınındarapor edilmiştir (6,19). Ortodontik tedavisonrası görülen demineralizasyonlarınyüksek prevalansına braketlere bitişikStreptococcus mutans sayısındaki artış sebepolmaktadır (20). Bu araştırma, TransbondPlus’ın Streptococcus mutans üremesiniinhibe ettiğini göstermiştir. Çalışmamızdaçürüğün birincil etiyolojik etkeni ve çürüklezyonlarından sıklıkla izole edilenStreptococcus mutans deney mikro-organizması olarak kullanıldı. Streptococcusmutans dişhekimliğinde restoratif mater-yallerin antimikrobiyal etkinliğinin sınan-masında yaygın olarak kullanılmıştır(14,21,22). Streptococcus mutans üremesi buaraştırmada DKT kullanılarak değerlendirildi.Yapılan çalışmalarda dental ürünlerinantibakteriyel etkinliği hem ayar difüzyontesti (ADT) hem de DKT ile incelenmiştir(15,22-24). DKT dental ürünlerin anti-bakteriyel etkisini belirlemede ADT’ye göredaha etkin bulunmuştur (15).Sabit apareylerle tedavi gören hastalarda
çürük başlangıç lezyonlarının gelişiminiengellemek için alınacak önlemler, bant vebraketlerin çevresinde oluşan bakteriyelplağın kontrolüne ve ağız boşluğunda sabitbir flor seviyesi sağlanmasına odaklanmıştır
RESULTSThe calibration experiments showed that
bacterial outgrowth in microtiter wells couldbe monitored in a quantitative andreproducible manner. The Streptococcusmutans growth in a 96-well microtitre plate ispresented in Figure 1 and Table 2. Each pointon the growth curve in Figure 1 is the averageof the optic density measured in eight wells atany given time. Each curve includes 32measurements taken within 16 hours.The evaluation of the results of the DCT
revealed that there were statisticallysignificant differences between the fourgroups (F= 156,951, P= 0.000). The controlmaterial (Kalzinol) showed completeinhibition of bacterial growth (mean0.01±0.05). The multiple comparison testindicated that there were no significantdifference in bacterial growth betweenKalzinol and Transbond Plus (mean0.12±0.17) (P= 0.509). Transbond Plusexhibited nearly similar effectiveness withKalzinol (Figure 1). Kurasper F (mean0.73±0.06) and Light Bond (mean0.85±0.02) showed statistically significantdifferences (P= 0.000 ) compared to Kalzinol.
DISCUSSIONWhite spot lesions have been reported in
50% of the teeth treated with fixedappliances and in up to 50% of theorthodontic patients (6,19). The highprevalence of post-orthodontic treatmentdemineralizations is caused by the increaseof Streptococcus mutans adjacent to brackets(20). This study demonstrated that TransbondPlus inhibit Streptococcus mutans growth.Streptococcus mutans, a primary etiologicagent of caries and a frequent caries-lesionisolate, was used as the test microorganism.Streptococcus mutans has been widely usedfor testing the antimicrobial activity ofrestorative materials in dentistry (14,21-22).Growth of the Streptococcus mutans wasevaluated in this study using the DCT. Theantibacterial activity of dental materials hasbeen intensively tested with both the agardiffusion test (ADT) and DCT (15,22-24). TheDCT was found to be more effective indetecting the antibacterial properties ofdental materials than ADT (15). The approaches to inhibiting the
development of white spot lesions in patientswith fixed appliances have focused oncontrolling the bacterial plaque around the
Türk Ortodonti Dergisi 2011;24:3-126
Öztürk, Toy, Arslan, Hatunoğlu
vertical position. During that time, most ofthe suspension liquid evaporated, ensuringdirect contact between all bacteria and thetested material surface. Then, 220 µL of BHIbroth was added to each of the wells and theplate was placed in the spectrophotometer.
The bacterial outgrowth was estimatedafter direct contact with the tested materialon the basis of the changes in the readings ofoptical density at 650 nm, which wererecorded automatically by the spectrop-hotometer every 30 minutes for 16 hours.Parallel to the experimental setup, calibrationexperiments were performed to establishbacterial outgrowth under experimentalconditions in a quantitative and reproduciblemanner (14).
Statistical Analyses Bacterial growth curves for each well were
analyzed and a regression line on theascending linear portion of the curve wascalculated, using the equation y = ax + b.This equation provided the value of the slopecorresponding to the growth rate. All statistical analyses were performed
using the Statistical Package for SocialSciences, version 13.0 for Windows (SPSS forWindows 13.0; SPSS, Chicago, Ilionis, USA).Descriptive statistics, including the mean,standard deviation, minimum and maximumvalues, were calculated for each of the fourgruops. Shapiro-Wilks normality and Levene’svariance homogeneity tests were applied tothe data. The data showed normal distrubitionand there were homogeneity of variancesamong the groups. The data were analyzed byone-way ANOVA, as well as by Tamhane’s T2multiple comparison test. The level ofsignificance was determined as P < 0.05.
fırat:muammer 7/14/11 11:08 AM Page 7
Turkish Journal of Orthodontics 2011;24:3-129
Ortodontik kompozitlerin antibakteriyel etkileriAntibacterial effects of orthodontic composites
ark (17) in vitro olarak üç cam iyonomersimanın ve çinko oksit öjenol simanınantibakteriyel özelliklerini incelemişler ve buürünlerin hiçbirinin test edilen bakterilerdeüreme göstermediğini bulmuşlardır.Feuerstein ve ark (18) 4 self etching adesivsisteminin (AdheSe, Adper Prompt L-Pop,Clearfil Protect Bond ve Xeno III)antibakteriyel özelliklerini DKT kullanarakincelemişler ve test edilen tüm adesivlerin 16saat içinde Streptococcus mutans üzerinebakterosidal etki gösterdiğini bildirmişlerdir.Ortodontik materyallerin antibakteriyel
özellikleri sadece bir makalede araştırılmıştır.Matalon ve ark (23) geleneksel camiyonomer siman (CX-Plus), resinlegüçlendirilmiş cam iyonomer siman (GC FujiOrtho LC), komposit resin (Transbond XT), veflor salan komposit resin (Transbond Plus)’inantibakteriyel etkilerini DKT kullanarakincelemişlerdir. GC Fuji Ortho LC veTransbond Plus 16 saat içinde antibakteriyeletki göstermiştir. Matalon ve ark (23)’nınçalışmasında, farklı tipte ortodontikmateryalleri (siman- kompozit ve flor salanve salmayan) karşılaştırılmıştır. Flor miktarı,tipi ve partikül boyutu, rezin tipi, silanuygulanması ve pörözite flor salınımınakatkıda bulunan önemli etkenlerden olduğuiçin bizim çalışmamızda flor salankompozitler karşılaştırılmıştır (11,12).Kurasper F ve Light Bond antibakteriyeletkinlik göstermemiştir. Transbond Plus ile,Matalon ve ark (23)’nın çalışmasındakinebenzer bir etki bulunmuştur.Etkin flor salınım düzeyinin uzun süreli ve
tercihen sabit bir hızda olması önemlidir.Salınan flor ilk gün en yüksek düzeye ulaşır.İkinci gün aniden düşer ve üçüncü gününsonuna kadar aşamalı olarak belirsiz birseviyeye düşer (26,37). Baturina ve ark (38),flor emdirilmiş elastomerik halkaların uzunsüreli düşük doz flor salınımı sağlayacağınıöne sürmüştür. Ortodontik hastaların her 30
Türk Ortodonti Dergisi 2011;24:3-128
Öztürk, Toy, Arslan, Hatunoğlu
(25). Flor salınımı yapan bonding materyalleriher geçen gün hızla gelişmektedir. Flor salanortodontik kompozitlerin kopma dayanık-lılığına etkileri, mine remineralizasyonu veflor salınım hızı birçok araştırmadadeğerlendirilmiştir (1,26-29). Flor salınarakoluşan remineralizasyon önemlidir ancakflorun antibakteriyel özelliği çürükoluşumunu engellemede asıl stratejidir (30).Mine demineralizasyonunu önlemek için
çeşitli uygulamalar önerilmiştir. Florlu dişmacunları, ağız gargaraları, jel ve cilalardişlere uygulanabilir veya flor salınımı yapansimanlar, elastomerik halkalar ve zincirlersabit aparey tedavisi süresince seçilebilir(31). Seppa ve ark (32) klinik bir çalışmadatopikal flor ajanlarının mine deminera-lizasyonunu azalttığını belirtmişlerdir.Düzenli flor cilalarının uygulanması sonu-cunda, braketlenmiş üst kesici dişte lezyonoluşumu azalmıştır (33). Ancak bunlarbüyük oranda hasta uyumuna bağlıdır vemine demineralizasyonuna karşı sadecearalıklı koruma sağlarlar (34). Antimikrobiyalajan içeren yapıştırma sistemleri incelenmiş(4,35,36), ancak bügüne kadar bu ürünlerpiyasada yer bulamamıştır (34). Cam iyonomer simanlar, dentin bonding
sistemleri ve yapıştırma ajanları ADTkullanılarak araştırılmıştır. Cam iyonomersimanlar ile belirgin antibakteriyel etkigözlenirken, amalgam, kompozit, yapıştırmaajanları ve bonding sistemleri bakteriyelüremeyi etkilememiştir (16). Davidovich ve
bands and brackets and the maintenance of aconstant fluoride level in the oral cavity (25).Fluoride releasing bonding material hasincreasingly been developed. The effects offluoridereleasing orthodontic material on shearbond strength, enamel reminera-lization, andthe fluoride releasing rate were evaluated(1,26-29). Remineralization by releasing offluoride is important, but the antibacterialproperty of fluoride is a direct strategy foreliminating the cause of dental caries (30).Various applications have been proposed
to inhibit enamel demineralization. Fluori-dated toothpaste, mouthrinse, gel and varnishcould be administered to the teeth, or fluoridereleasing cements, elastomeric modules andchains could be chosen during fixedappliance treatment (31). Seppa et al (32)stated that topical fluoride agents decreasedenamel demineralization in a clinical trial.The efficiency of regular application offluoride varnish appears to reduce lesionformation on bracketed maxillary incisorteeth (33) However they rely heavily onpatient compliance and provide onlyintermittent protection against deminera-lization (34). Bonding systems that containantimicrobial agents have been evaluated(4,35,36), but to date, these products can nottake place in the market (34). The antibacterial activity of several glass
ionomer cements, dentin bonding systems,and luting agents were investigated usingADT. Marked antibacterial activity wasshown with the glass ionomer cement,whereas amalgam, composites, luting agents,
fiekil�1.�Streptococcus�mutans
ve�incelenen�materyaller
arasında�direk�kontak
sonrası�görülen�bakteriyel
üreme�eğrileri.�Eğriler
üzerindeki�herbir�nokta,�8
kuyucuktaki��650�nm
düzeyinde�ölçülen�ortalama
optik�yoğunluğu�gösterir.
Figure�1.�Growth�curves�of
bacterial�outgrowth�after
direct�contact�between
Streptococcus�mutans and
tested�materials.�Each�point
on�the�growth�curve
represents�the�average
optical�density�measured�at
650�nm�in�eight�wells.
fırat:muammer 7/14/11 11:08 AM Page 8
Turkish Journal of Orthodontics 2011;24:3-129
Ortodontik kompozitlerin antibakteriyel etkileriAntibacterial effects of orthodontic composites
ark (17) in vitro olarak üç cam iyonomersimanın ve çinko oksit öjenol simanınantibakteriyel özelliklerini incelemişler ve buürünlerin hiçbirinin test edilen bakterilerdeüreme göstermediğini bulmuşlardır.Feuerstein ve ark (18) 4 self etching adesivsisteminin (AdheSe, Adper Prompt L-Pop,Clearfil Protect Bond ve Xeno III)antibakteriyel özelliklerini DKT kullanarakincelemişler ve test edilen tüm adesivlerin 16saat içinde Streptococcus mutans üzerinebakterosidal etki gösterdiğini bildirmişlerdir.Ortodontik materyallerin antibakteriyel
özellikleri sadece bir makalede araştırılmıştır.Matalon ve ark (23) geleneksel camiyonomer siman (CX-Plus), resinlegüçlendirilmiş cam iyonomer siman (GC FujiOrtho LC), komposit resin (Transbond XT), veflor salan komposit resin (Transbond Plus)’inantibakteriyel etkilerini DKT kullanarakincelemişlerdir. GC Fuji Ortho LC veTransbond Plus 16 saat içinde antibakteriyeletki göstermiştir. Matalon ve ark (23)’nınçalışmasında, farklı tipte ortodontikmateryalleri (siman- kompozit ve flor salanve salmayan) karşılaştırılmıştır. Flor miktarı,tipi ve partikül boyutu, rezin tipi, silanuygulanması ve pörözite flor salınımınakatkıda bulunan önemli etkenlerden olduğuiçin bizim çalışmamızda flor salankompozitler karşılaştırılmıştır (11,12).Kurasper F ve Light Bond antibakteriyeletkinlik göstermemiştir. Transbond Plus ile,Matalon ve ark (23)’nın çalışmasındakinebenzer bir etki bulunmuştur.Etkin flor salınım düzeyinin uzun süreli ve
tercihen sabit bir hızda olması önemlidir.Salınan flor ilk gün en yüksek düzeye ulaşır.İkinci gün aniden düşer ve üçüncü gününsonuna kadar aşamalı olarak belirsiz birseviyeye düşer (26,37). Baturina ve ark (38),flor emdirilmiş elastomerik halkaların uzunsüreli düşük doz flor salınımı sağlayacağınıöne sürmüştür. Ortodontik hastaların her 30
and bonding systems did not affect thebacterial growth (16). Davidovich et al (17)evaluated the antibacterial properties ofrestorative materials (three glass ionomercements and a zinc-oxide eugenol cement) invitro and found that none of the testedmaterial showed bacterial growth in any ofthe tested bacteria. Feuerstein et al (18)examined the antibacterial properties of fourself-etching adhesive systems (AdheSe, AdperPrompt L-Pop, Clearfil Protect Bond andXeno III) using the DCT. All of the testedadhesives had a bactericidal effect onStrepptococcus mutans within 16 hours.The antibacterial properties of orthodontic
materials were evaluated in only one study inthe orthodontic literature. Matalon et al (23)evaluated the antibacterial properties ofconventional glass ionomer cement (CX-Plus), resin forced glass ionomer cement (GCFuji Ortho LC), composite resin (TransbondXT), and fluoride releasing composite resin(Transbond Plus) using DCT. The authorsfound that GC Fuji Ortho LC and TransbondPlus showed their antibacterial properties in16 hours. In the Matalon et al (23) study, different
types of orthodontic materials (cement-composite and both fluoride releasing andnot) were compared. Fluoride releasingcomposites were compared in our studybecause the amount of fluoride, type andparticle size of the fluoridated filler, the type ofresin, silane treatment, and porosity might beimportant factors contributing to fluoriderelease (11,12). Kurasper F and Light Bond didnot show antibacterial activity. Transbond Plusshowed antibacterial effects similar to thosedemonstrated in the Matalon et al (23) study. It is essential that the effective levels of
fluoride release are maintained for longperiods of time, preferably at a constant rate.Fluoride released reaches the highest level onthe first day, then suddenly reduces on thesecond day, and gradually decreases toundetectable levels by the end of the third
Türk Ortodonti Dergisi 2011;24:3-128
Öztürk, Toy, Arslan, Hatunoğlu
bands and brackets and the maintenance of aconstant fluoride level in the oral cavity (25).Fluoride releasing bonding material hasincreasingly been developed. The effects offluoridereleasing orthodontic material on shearbond strength, enamel reminera-lization, andthe fluoride releasing rate were evaluated(1,26-29). Remineralization by releasing offluoride is important, but the antibacterialproperty of fluoride is a direct strategy foreliminating the cause of dental caries (30).Various applications have been proposed
to inhibit enamel demineralization. Fluori-dated toothpaste, mouthrinse, gel and varnishcould be administered to the teeth, or fluoridereleasing cements, elastomeric modules andchains could be chosen during fixedappliance treatment (31). Seppa et al (32)stated that topical fluoride agents decreasedenamel demineralization in a clinical trial.The efficiency of regular application offluoride varnish appears to reduce lesionformation on bracketed maxillary incisorteeth (33) However they rely heavily onpatient compliance and provide onlyintermittent protection against deminera-lization (34). Bonding systems that containantimicrobial agents have been evaluated(4,35,36), but to date, these products can nottake place in the market (34). The antibacterial activity of several glass
ionomer cements, dentin bonding systems,and luting agents were investigated usingADT. Marked antibacterial activity wasshown with the glass ionomer cement,whereas amalgam, composites, luting agents,
Tablo�2.�Büyüme�eğrisinde
doğrusal�bölümün�eğimiyle
gösterilen�bakteriyel�
büyüme�hızı.
Table�2.�Bacterial�growth
rate,�as�demonstrated�by
slope�of�linear�portion�of
growth�curve.
fırat:muammer 7/14/11 11:08 AM Page 9
Turkish Journal of Orthodontics 2011;24:3-1211
Ortodontik kompozitlerin antibakteriyel etkileriAntibacterial effects of orthodontic composites
Türk Ortodonti Dergisi 2011;24:3-1210
Öztürk, Toy, Arslan, Hatunoğlu
ile 45 günde bir kontrol randevuları olduğuiçin, ideal olarak bu flor uygulama yöntemihastalarda uyum gereksinimini yok edecekve her randevuda flor uygulamasıyenilenecektir.
SONUÇBu çalışmanın sınırları içinde, Transbond
Plus güçlü antibakteriyel etki göstermiş,ancak Light Bond ve Kurasper F bakteriüremesini engellememiştir. İncelenen mater-yallerin uzun süreli antibakteriyel özellik-lerini incelemek için ileri çalışmalargereklidir.
TEŞEKKÜR Araştırmacılar, 3M Unitek, Reliance ve
Kuraray firmalarına test edilen ürünlerisağladıkları için teşekkür eder.
day (26,37). Baturina et al (38) suggested thatelastomeric ligature ties (rings) impregnatedwith fluoride would provide a long-term low-dose fluoride release. Because orthodonticpatients have routine examining appoint-ments every 30 to 45 days, ideally, thismethod of fluoride delivery would eliminateany need for patient compliance and wouldreplace fluoride at each orthodontic visits.
CONCLUSIONWithin the limitations of this study,
Transbond Plus exhibited potent antibacterialactivity but Kurasper F and Light Bond didnot inhibit the bacterial growth. Furtherstudies are required to investigate the long-lasting antibacterial properties of the testedmaterials.
ACKNOWLEDGEMENTThe autors thank 3M Unitek, Reliance,
and Kuraray for providing the adhesivestested in this study.
KAYNAKLAR/REFERENCES
1. McNeill CJ, Wiltshire WA, Dawes C, Lavelle CL.Fluoride release from new light-cured orthodonticbonding agents. Am J Orthod Dentofacial Orthop2001;120:392-97.
2. Benson PE, Parkin N, Millett DT, Dyer FE, Vine S, ShahA. Fluorides for the prevention of white spots on teethduring fixed brace treatment. Cochrane Database SystRev 2004;3:CD003809.
3. Meiers JC, Wirthlin MR, Shklair IL. A microbiologicalanalysis of human early carious and non-cariousfissures. J Dent Res 1982;61:460-4.
4. Al-Musallam TA, Evans CA, Drummond JL, Matasa C,Wu CD. Antimicrobial properties of an orthodonticadhesive combined with cetylpyridinium chloride. AmJ Orthod Dentofacial Orthop 2006;129:245-51.
5. Kocak MM, Ozcan S, Kocak S, Topuz O, ErtenH. Comparison of the efficacy of three differentmouthrinse solutions in decreasing the level ofstreptococcus mutans in saliva. Eur J Dent2009;3:57-61.
6. Gorelick L, Geiger AM, Gwinnett AJ. Incidence ofwhite spot formation after bonding and banding. Am JOrthod Dentofacial Orthop 1982;81:93-98.
7. Uysal T, Amasyali M, Koyuturk AE, Sagdic D.Efficiency of amorphous calcium phosphate-containing orthodontic composite and resin modifiedglass ionomer on demineralization evaluated by a newlaser fluorescence device. Eur J Dent 2009;3:127-34.
8. O’Reilly MM, Featherstone JDB. Demineralization andremineralization around orthodontic appliances: an invivo study. Am J Orthod Dentofacial Orthop1987;92:33-40.
9. Wiegand A, Buchalla W, Attin T. Review on fluoride-releasing restorative materials-fluoride release and
uptake characteristics, antibacterial activity andinfluence on caries formation. Dent Mater2007;23:343-62.
10. Hamilton IR. Biochemical effects of fluoride on oralbacteria. J Dent Res 1990;69:660-67.
11. Dijkman GE, de Vries J, Lodding A, Arends J. Long-term fluoride release of visible light-activatedcomposites in vitro: a correlation with in situdemineralization data. Caries Res 1993;27:117-23.
12. Xu X, Burgess JO. Compressive strength, fluoriderelease and recharge of fluoride-releasing materials.Biomaterials 2003;24:2451-61.
13. Asmussen E, Peutzfeldt A. Long-term fluoride releasefrom a glass ionomer cement, a compomer, and fromexperimental resin composites. Acta Odontol Scand2002;60:93-97.
14. Weiss EI, Shlhav M, Fuss Z. Assessment of antibacterialactivity of endodontic sealers by a direct contact test.Endod Dent Traumatol 1996;12:179-84.
15. Lewinstein I, Matalon S, Slutzkey S, Weiss EI.Antibacterial properties of aged dental cementsevaluated by direct-contact and agar diffusion tests. JProsthet Dent 2005;93:364-71.
16. Prati C, Fava F, Di Gioia D, Selighini M, Pashley DH.Antibacterial effectiveness of dentin bonding systems.Dent Mater 1993;9:338-43.
17. Davidovich E, Weiss E, Fuks AB, Beyth N. Surfaceantibacterial properties of glass ionomer cements usedin atraumatic restorative treatment. J Am Dent Assoc2007;138:1347-52.
18. Feuerstein O, Matalon S, Slutzky H, Weiss EI.Antibacterial properties of self-etching dental adhesivesystems. J Am Dent Assoc 2007;138:349-54.
19. Øgaard B. Prevalence of white spot lesions in 19-year-olds: a study on untreated and orthodontically treatedpersons 5 years after treatment. Am J OrthodDentofacial Orthop 1989;96:423-27.
20. Zimmer BW, Rottwinkel Y. Assessing patient-specificdecalcification risk in fixed orthodontic treatment andits impact on prophylactic procedures. Am J OrthodDentofacial Orthop 2004;126:318-24.
21. Tobias RS. Antibacterial properties of dental restorativematerials: a review. Int Endod J 1988;21:155-60.
22. Herrera M, Carrion P, Baca P, Liebana J, Castillo A. Invitro antibacterial activity of glass-ionomer cements.Microbios 2001;104:141-48.
23. Matalon S, Slutzky H, Weiss EI. Antibacterial propertiesof 4 orthodontic cements. Am J Orthod DentofacialOrthop 2005;127:56-63.
24. Duran I, Sengun A, Hadimli HH, Ulker M. Evaluationof antibacterial effectiveness of desensitizers againstoral bacteria. Eur J Dent 2008;2:43-47.
25. Stephen M. The role of diet, fluoride and saliva incaries prevention. J Indian Soc Pedod Prev Dent1997;15:109-13.
26. Basdra EK, Huber H, Komposch G. Fluoride releasedfrom orthodontic bonding agents alters the enamelsurface and inhibits enamel demineralization in vitro.Am J Orthod Dentofacial Orthop 1996;109:466-72.
27. Cacciafesta V, Sfondrini MF, Tagliani P, Klersy C. In-vitro fluoride release rates from 9 orthodontic bondingadhesives. Am J Orthod Dentofacial Orthop2007;132:656-62.
28. Yildirim S, Tosun G, Koyutürk AE, Sener Y, Sengün A,Ozer F, Imazato S. Microtensile and microshear bondstrength of an antibacterial self-etching system toprimary tooth dentin. Eur J Dent 2008;2:11-17.
29. Chin MY, Sandham A, Rumachik EN, Ruben JL,Huysmans MC. Fluoride release and cariostatic
potential of orthodontic adhesives with and withoutdaily fluoride rinsing. Am J Orthod Dentofacial Orthop2009;136:547-53.
30. Eminkahyagil N, Korkmaz Y, Gokalp S, Baseren M.Shear bond strength of orthodontic brackets withnewly developed antibacterial self-etch adhesive.Angle Orthod 2005;75:843-48.
31. Uysal T, Amasyali M, Koyuturk AE, Ozcan S. Effects ofdifferent topical agents on enamel demineralizationaround orthodontic brackets: an in vivo and in vitrostudy. Aust Dent J. 2010;55:268-74.
32. Seppä L, Leppänen T, Hausen H. Fluoride varnishversus acidulated phosphate fluoride gel: a 3-yearclinical trial. Caries Res. 1995;29:327-30.
33. Øgaard B, Larsson E, Henriksson T, Birkhed D, BisharaSE. Effects of combined application of antimicrobialand flüoride varnishes in orthodontic patients. Am JOrthod Dentofacial Orthop 2001;120:28–35.
34. Spencer CG, Campbell PM, Buschang PH, Cai J,Honeyman AL. Antimicrobial effects of zinc oxide inan orthodontic bonding agent. Angle Orthod2009;79:317-22.
35. Imazato S, Torii M, Tsuchitani Y, McCabe JF, RussellRR. Incorporation of bacterial inhibitor into resincomposite. J Dent Res 1994;73:1437–43.
36. Fan C, Chu L, Rawls HR, Norling BK, Cardenas HL,Whang K. Development of an antimicrobial resin--apilot study. Dent Mater 2011;27:322-8.
37. Rix D, Foley TF, Banting D, Mamandras A. Acomparison of fluoride release by resin-modified GICand polyacid-modified composite resin. Am J OrthodDentofacial Orthop 2001;120:398–405.
38. Baturina O, Tufekci E, Guney-Altay O, Khan SM,Wnek GE, Lindauer SJ Development of asustained fluoride delivery system. Angle Orthod2010;80:1129-35.
fırat:muammer 7/14/11 11:08 AM Page 10
Turkish Journal of Orthodontics 2011;24:3-1211
Ortodontik kompozitlerin antibakteriyel etkileriAntibacterial effects of orthodontic composites
Türk Ortodonti Dergisi 2011;24:3-1210
Öztürk, Toy, Arslan, Hatunoğlu
day (26,37). Baturina et al (38) suggested thatelastomeric ligature ties (rings) impregnatedwith fluoride would provide a long-term low-dose fluoride release. Because orthodonticpatients have routine examining appoint-ments every 30 to 45 days, ideally, thismethod of fluoride delivery would eliminateany need for patient compliance and wouldreplace fluoride at each orthodontic visits.
CONCLUSIONWithin the limitations of this study,
Transbond Plus exhibited potent antibacterialactivity but Kurasper F and Light Bond didnot inhibit the bacterial growth. Furtherstudies are required to investigate the long-lasting antibacterial properties of the testedmaterials.
ACKNOWLEDGEMENTThe autors thank 3M Unitek, Reliance,
and Kuraray for providing the adhesivestested in this study.
KAYNAKLAR/REFERENCES
1. McNeill CJ, Wiltshire WA, Dawes C, Lavelle CL.Fluoride release from new light-cured orthodonticbonding agents. Am J Orthod Dentofacial Orthop2001;120:392-97.
2. Benson PE, Parkin N, Millett DT, Dyer FE, Vine S, ShahA. Fluorides for the prevention of white spots on teethduring fixed brace treatment. Cochrane Database SystRev 2004;3:CD003809.
3. Meiers JC, Wirthlin MR, Shklair IL. A microbiologicalanalysis of human early carious and non-cariousfissures. J Dent Res 1982;61:460-4.
4. Al-Musallam TA, Evans CA, Drummond JL, Matasa C,Wu CD. Antimicrobial properties of an orthodonticadhesive combined with cetylpyridinium chloride. AmJ Orthod Dentofacial Orthop 2006;129:245-51.
5. Kocak MM, Ozcan S, Kocak S, Topuz O, ErtenH. Comparison of the efficacy of three differentmouthrinse solutions in decreasing the level ofstreptococcus mutans in saliva. Eur J Dent2009;3:57-61.
6. Gorelick L, Geiger AM, Gwinnett AJ. Incidence ofwhite spot formation after bonding and banding. Am JOrthod Dentofacial Orthop 1982;81:93-98.
7. Uysal T, Amasyali M, Koyuturk AE, Sagdic D.Efficiency of amorphous calcium phosphate-containing orthodontic composite and resin modifiedglass ionomer on demineralization evaluated by a newlaser fluorescence device. Eur J Dent 2009;3:127-34.
8. O’Reilly MM, Featherstone JDB. Demineralization andremineralization around orthodontic appliances: an invivo study. Am J Orthod Dentofacial Orthop1987;92:33-40.
9. Wiegand A, Buchalla W, Attin T. Review on fluoride-releasing restorative materials-fluoride release and
uptake characteristics, antibacterial activity andinfluence on caries formation. Dent Mater2007;23:343-62.
10. Hamilton IR. Biochemical effects of fluoride on oralbacteria. J Dent Res 1990;69:660-67.
11. Dijkman GE, de Vries J, Lodding A, Arends J. Long-term fluoride release of visible light-activatedcomposites in vitro: a correlation with in situdemineralization data. Caries Res 1993;27:117-23.
12. Xu X, Burgess JO. Compressive strength, fluoriderelease and recharge of fluoride-releasing materials.Biomaterials 2003;24:2451-61.
13. Asmussen E, Peutzfeldt A. Long-term fluoride releasefrom a glass ionomer cement, a compomer, and fromexperimental resin composites. Acta Odontol Scand2002;60:93-97.
14. Weiss EI, Shlhav M, Fuss Z. Assessment of antibacterialactivity of endodontic sealers by a direct contact test.Endod Dent Traumatol 1996;12:179-84.
15. Lewinstein I, Matalon S, Slutzkey S, Weiss EI.Antibacterial properties of aged dental cementsevaluated by direct-contact and agar diffusion tests. JProsthet Dent 2005;93:364-71.
16. Prati C, Fava F, Di Gioia D, Selighini M, Pashley DH.Antibacterial effectiveness of dentin bonding systems.Dent Mater 1993;9:338-43.
17. Davidovich E, Weiss E, Fuks AB, Beyth N. Surfaceantibacterial properties of glass ionomer cements usedin atraumatic restorative treatment. J Am Dent Assoc2007;138:1347-52.
18. Feuerstein O, Matalon S, Slutzky H, Weiss EI.Antibacterial properties of self-etching dental adhesivesystems. J Am Dent Assoc 2007;138:349-54.
19. Øgaard B. Prevalence of white spot lesions in 19-year-olds: a study on untreated and orthodontically treatedpersons 5 years after treatment. Am J OrthodDentofacial Orthop 1989;96:423-27.
20. Zimmer BW, Rottwinkel Y. Assessing patient-specificdecalcification risk in fixed orthodontic treatment andits impact on prophylactic procedures. Am J OrthodDentofacial Orthop 2004;126:318-24.
21. Tobias RS. Antibacterial properties of dental restorativematerials: a review. Int Endod J 1988;21:155-60.
22. Herrera M, Carrion P, Baca P, Liebana J, Castillo A. Invitro antibacterial activity of glass-ionomer cements.Microbios 2001;104:141-48.
23. Matalon S, Slutzky H, Weiss EI. Antibacterial propertiesof 4 orthodontic cements. Am J Orthod DentofacialOrthop 2005;127:56-63.
24. Duran I, Sengun A, Hadimli HH, Ulker M. Evaluationof antibacterial effectiveness of desensitizers againstoral bacteria. Eur J Dent 2008;2:43-47.
25. Stephen M. The role of diet, fluoride and saliva incaries prevention. J Indian Soc Pedod Prev Dent1997;15:109-13.
26. Basdra EK, Huber H, Komposch G. Fluoride releasedfrom orthodontic bonding agents alters the enamelsurface and inhibits enamel demineralization in vitro.Am J Orthod Dentofacial Orthop 1996;109:466-72.
27. Cacciafesta V, Sfondrini MF, Tagliani P, Klersy C. In-vitro fluoride release rates from 9 orthodontic bondingadhesives. Am J Orthod Dentofacial Orthop2007;132:656-62.
28. Yildirim S, Tosun G, Koyutürk AE, Sener Y, Sengün A,Ozer F, Imazato S. Microtensile and microshear bondstrength of an antibacterial self-etching system toprimary tooth dentin. Eur J Dent 2008;2:11-17.
29. Chin MY, Sandham A, Rumachik EN, Ruben JL,Huysmans MC. Fluoride release and cariostatic
potential of orthodontic adhesives with and withoutdaily fluoride rinsing. Am J Orthod Dentofacial Orthop2009;136:547-53.
30. Eminkahyagil N, Korkmaz Y, Gokalp S, Baseren M.Shear bond strength of orthodontic brackets withnewly developed antibacterial self-etch adhesive.Angle Orthod 2005;75:843-48.
31. Uysal T, Amasyali M, Koyuturk AE, Ozcan S. Effects ofdifferent topical agents on enamel demineralizationaround orthodontic brackets: an in vivo and in vitrostudy. Aust Dent J. 2010;55:268-74.
32. Seppä L, Leppänen T, Hausen H. Fluoride varnishversus acidulated phosphate fluoride gel: a 3-yearclinical trial. Caries Res. 1995;29:327-30.
33. Øgaard B, Larsson E, Henriksson T, Birkhed D, BisharaSE. Effects of combined application of antimicrobialand flüoride varnishes in orthodontic patients. Am JOrthod Dentofacial Orthop 2001;120:28–35.
34. Spencer CG, Campbell PM, Buschang PH, Cai J,Honeyman AL. Antimicrobial effects of zinc oxide inan orthodontic bonding agent. Angle Orthod2009;79:317-22.
35. Imazato S, Torii M, Tsuchitani Y, McCabe JF, RussellRR. Incorporation of bacterial inhibitor into resincomposite. J Dent Res 1994;73:1437–43.
36. Fan C, Chu L, Rawls HR, Norling BK, Cardenas HL,Whang K. Development of an antimicrobial resin--apilot study. Dent Mater 2011;27:322-8.
37. Rix D, Foley TF, Banting D, Mamandras A. Acomparison of fluoride release by resin-modified GICand polyacid-modified composite resin. Am J OrthodDentofacial Orthop 2001;120:398–405.
38. Baturina O, Tufekci E, Guney-Altay O, Khan SM,Wnek GE, Lindauer SJ Development of asustained fluoride delivery system. Angle Orthod2010;80:1129-35.
fırat:muammer 7/14/11 11:08 AM Page 11