first aide - napa valley college
TRANSCRIPT
1
1Elsevier items and derived items © 2005 by Elsevier Inc. Slide 1Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 1
Chapter 24Emergency First Aid NursingChapter 24Emergency First Aid Nursing
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 2Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 2
Medical Emergency Aid• The nurse’s ability to recognize the need
for medical assistance and knowledge of how to obtain medical emergency aid can mean the difference between life and death to an injured or ill person.
• Health care providers must be prepared to provide cardiopulmonary resuscitation (CPR) if needed until emergency medical assistance arrives.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 3Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 3
Moral and Legal Responsibilities• Good Samaritan Laws
– Enacted in most state to protect health professionals from legal liability when providing emergency first aid.
– Follow a reasonable and prudent course of action.• Victim must give verbal permission• The law assumes that an unconscious person
would give consent if he or she were able.• Once first aid is initiated, the nurse has the moral
and legal obligation to continue the aid until the victim can be cared for by someone with comparable or better training.
2
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 4Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 4
Assessment of the Emergency• Primary Assessment
– Airway– Breathing– Circulation (pulse and severe bleeding)
• Life-threatening Situations– Arrested or abnormal breathing or pulse
• Observe for indications of skull injury and brain or spinal cord damage.
• Fractures, dislocations, and superficial ecchymoses or wounds require attention after the more serious conditions are treated.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 5Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 5
Ethical Implications
• Reasons Why Individuals Choose Not to Perform CPR– Lack of motivation– Fear of doing harm– Lack of knowledge– Fear of contracting communicable diseases
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 6Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 6
Events Requiring CPR• Clinical Death
– The heartbeat and respirations have ceased.• Biological Death
– This results from permanent cellular damage caused by lack of oxygen.
– The brain is the first organ to suffer from lack of oxygen.
– In many cases, CPR can reverse clinical death if initiated before 4 minutes of cardiopulmonary arrest.
– After 10 minutes without CPR, brain death is certain.
3
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 7Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 7
Events Requiring CPR
• Brain Death– This is an irreversible form of
unconsciousness characterized by a complete loss of brain function while the heart continues to beat.
– The usual clinical criteria for brain death include the absence of reflex activity, movements, and respiration; pupils that are fixed and dilated; and absent electric activity of the brain on two electroencephalograms (EEGs) performed 12 to 24 hours apart.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 8Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 8
Shock• Shock is an abnormal condition of inadequate
blood flow to the body’s peripheral tissues, with life-threatening cellular dysfunction, hypotension, and oliguria.
• It results from failure of the cardiovascular system to provide sufficient blood circulation to the body’s tissues and decreased metabolic waste removal.
• To maintain circulatory homeostasis, there must be a functioning heart to circulate blood and a sufficient volume of blood.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 9Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 9
Shock
• http://www.wonderhowto.com/how-to/video/how-to-diagnose-septic-shock-symptoms-254886/
4
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 10Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 10
Shock
• Classification of Shock– Classified according to cause
• Severe blood loss• Intense pain• Extensive trauma; burns• Poisons• Emotional stress or intense emotions• Extremes of heat and cold• Electrical shock• Allergic reactions• Sudden or severe illness
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 11Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 11
Shock
• Assessment– Level of consciousness– Skin changes– Blood pressure– Pulse– Respirations– Urinary output– Neuromuscular changes– Gastrointestinal effects
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 12Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 12
Shock• Nursing Interventions
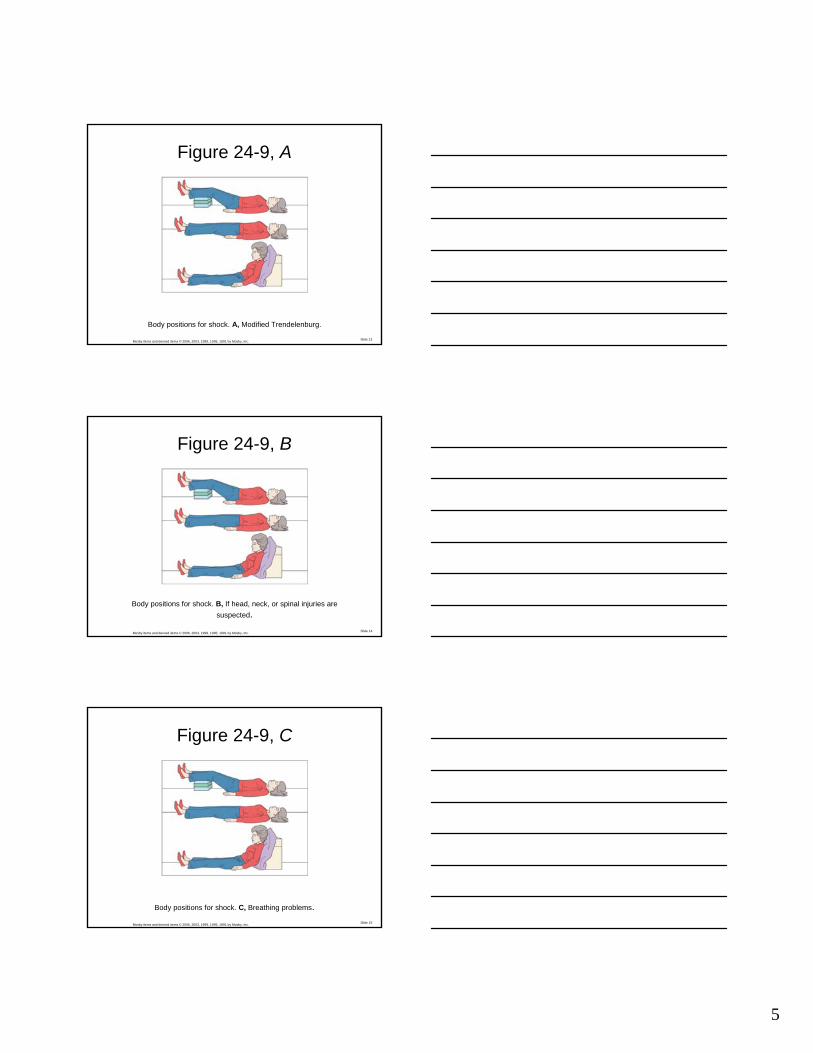
– Establish airway.– Control bleeding.– Reduce pain.– Position the victim flat with the head slightly
lower than the rest of the body (elevate the feet and legs).
– If victim is unconscious or is vomiting or bleeding around the nose or mouth, position on the side.
– If victim is having breathing problems, elevate head and shoulders.
5
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 13Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 13
Figure 24-9, A
Body positions for shock. A, Modified Trendelenburg.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 14Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 14
Figure 24-9, B
Body positions for shock. B, If head, neck, or spinal injuries are suspected.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 15Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 15
Figure 24-9, C
Body positions for shock. C, Breathing problems.

6
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 16Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 16
Shock
• Nursing Interventions (continued)– Cover victim with a blanket or other covering
to keep warm.– Do not give anything to eat or drink.– Relieve pain: support injury; avoid rough
handling; adjust tight or uncomfortable clothes.
– Do not give analgesics unless directed by a physician.
– Provide emotional support and reassurance.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 17Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 17
Bleeding/Hemorrhage• Effects of Blood Loss
– Blood loss from internal or external bleeding causes a decrease in oxygen supply to the body.
– Blood pressure drops.– Heart pumps faster to compensate for the
decreased volume and blood pressure.– The body will attempt to clot the blood to halt
bleeding; usually requiring 6 to 7 minutes.– Uncontrolled, bleeding can result in shock and
death.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 18Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 18
Bleeding/Hemorrhage
• Types of Bleeding– Capillary
• Most common; results from damaged or broken capillaries and causes oozing of minor cuts, scratches, and abrasions
– Venous• Occurs when the vein is severed or punctured • Results in a slow, even flow of dark red blood• Embolism may occur if air enters the severed vein.
7
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 19Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 19
Bleeding/Hemorrhage
• Types of Bleeding (continued)– Arterial
• Least common; usually protected by bones, fat, and other structures
• Heavy spurting of bright red blood in the rhythm of the heartbeat
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 20Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 20
Bleeding/Hemorrhage
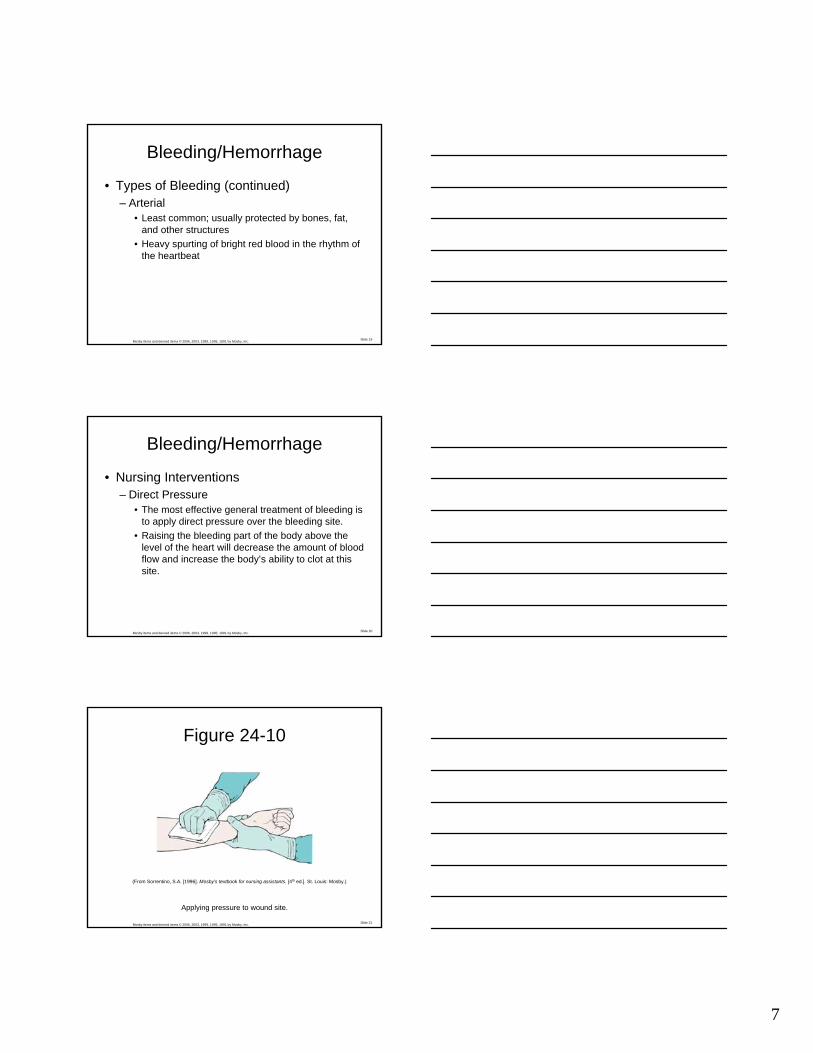
• Nursing Interventions– Direct Pressure
• The most effective general treatment of bleeding is to apply direct pressure over the bleeding site.
• Raising the bleeding part of the body above the level of the heart will decrease the amount of blood flow and increase the body’s ability to clot at this site.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 21Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 21
Figure 24-10
Applying pressure to wound site.
(From Sorrentino, S.A. [1996]. Mosby’s textbook for nursing assistants. [4th ed.]. St. Louis: Mosby.)

8
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 22Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 22
Bleeding/Hemorrhage• Nursing Interventions (continued)
– Indirect Pressure• If direct pressure and elevation do not control
bleeding, indirect pressure may be applied to any of the pressure points situated along main arteries.
– Application of a Tourniquet• A tourniquet must be used only when the other
methods have failed and the victim’s life is in danger.
• It can cause extensive damage to the body part.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 23Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 23
Figure 24-11
Applying pressure to wound site.
(From Kidd, P.S., Stuart, P.A. [1996]. Mosby’s emergency nursing reference. St. Louis: Mosby.)
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 24Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 24
Skill 24-1: Step 7
Applying a tourniquet.
9
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 25Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 25
Bleeding/Hemorrhage
• Epistaxis– Nosebleed– Common but seldom a serious emergency– Causes
• Trauma• Epistaxis digitorum (trauma from nasal picking)• Infections• Hypertension• Strenuous activity• Low humidity
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 26Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 26
Bleeding/Hemorrhage• Epistaxis
– Nursing Interventions• Keep the victim’s head tilted slightly forward.• Apply steady pressure to both nostrils for 10 to 15
minutes.• Remind the victim to breathe through the mouth
and to expectorate any accumulated blood.• Apply ice compresses over the nose at the same
time.• Look in the victim’s mouth at the back of the throat
to assess for bleeding from a posterior site.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 27Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 27
Bleeding/Hemorrhage• Internal Bleeding
– This is a potentially life-threatening situation.– Common causes are fractures, knife or bullet
wounds, crushing injuries, organ injuries, and medical conditions such as ruptured aneurysms.
– Assessment• Signs and symptoms of shock.• Vertigo• Hemoptysis or hematemesis• Melena• Hematuria

10
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 28Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 28
Bleeding/Hemorrhage
• Internal Bleeding– Nursing Interventions
• This is a priority medical emergency.• Place on a flat surface with legs elevated.• Establish an airway.• Cold compress or ice is placed on the area of
injury.• Maintain body temperature with blankets.• Assess vital signs.• Oxygen may be ordered by the physician.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 29Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 29
Wounds and Trauma• Closed Wounds
– The underlying tissue of the body is involved; the top layer of skin is not broken.
– Ecchymoses (bruises) and contusions occur.– Signs and symptoms
• Edema, discoloration, deformity, shock, pain and tenderness, and signs of internal bleeding
– Nursing interventions• Small wound: ice packs and elastic bandage• Large wound: treat for shock; cold compresses
and pressure bandage
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 30Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 30
Wounds and Trauma
• Open Wounds– Openings or breaks in the mucous membrane
or skin– Always danger of bleeding or infection– Types
• Abrasions• Puncture wounds• Incisions• Lacerations• Avulsions• Chest injuries

11
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 31Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 31
Wounds and Trauma• Dressings and Bandages
– General Principles of Bandaging• Bleeding should be controlled before bandage is
applied.• Use sterile material if possible; if not use, the
cleanest material possible.• Dressing should never cover the entire wound.• Wounds should be bandaged firmly but not too
tightly.• Bandage in alignment is desired.• Tips of fingers and toes should remain exposed if
possible.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 32Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 32
Wounds and Trauma• Application of Common Types of
Bandages– Bandage Compress
• Most common type of dressing; consists of several thicknesses of gauze, covered with tape or gauze.
– Triangular Bandage• Made of a piece of cloth that is folded diagonally
and cut along the fold; used as a sling to support injured bones.
– Roller Bandage• Used to support an injured part apply pressure to a
dressing, or secure a splint to immobilize a part.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 33Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 33
Figure 24-13
Use of roller bandage.
(From Henry, M.C., Stapleton, E.R. [1997]. EMT prehospital care. [2nd ed.]. Philadelphia: Saunders.)

12
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 34Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 34
Poisons• General Assessment of Poisonings
– Signs and symptoms may be delayed for hours.
– Indications may be respiratory distress; nausea, vomiting, or diarrhea; seizures; decreased level of consciousness; restlessness, delirium, agitation; color changes; signs of burns; pain on swallowing; unusual urine color; abnormal constriction or dilation of pupils; abnormal eye movement; skin irritation; and shock or cardiac arrest.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 35Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 35
Poisons
• Ingested Poisons– Poisoning by mouth is the most common type
of poisoning, especially in children.– Common substances include household
cleaning products, garden and garage supplies, drugs, medications, food, and plants.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 36Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 36
Poisons
• Ingested Poisons– Nursing Interventions
• Immediately call the poison control center.• Maintain airway.• Possible instructions by the poison control center
– Dilute the poison by giving one or two glasses of water.– Induce vomiting if gag reflex is present and poison is not
a corrosive.
• Treat for shock and administer CPR if needed.

13
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 37Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 37
Poisons
• Inhaled Poisons– Common Sources
• Carbon monoxide, carbon dioxide, and refrigeration gases; poisonous fumes from chlorine and other liquid chemical sprays
– Nursing Interventions• Remove victim from the dangerous area only if
there is no danger to the rescuer.• Maintain airway; perform CPR if needed.• Victim should remain quite and inactive while
being transported to the nearest medical facility.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 38Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 38
Poisons• Absorbed Poisons
– Poisons, caustic chemicals, and poisonous plants that come in contact with the skin
– Causes burning, skin irritation, allergic responses, or severe system reactions
– Signs and symptoms• Nausea, vomiting, diarrhea, flushed skin, dilated
pupils, cardiovascular abnormalities, and CNS reactions
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 39Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 39
Poisons
• Absorbed Poisons– Nursing Interventions
• Quickly remove the source of the irritation; wash with soap and water.
• Skin preparations include baking soda, Burow’ssolution, and oatmeal.
• Calamine lotion and hydrocortisone cream are effective to relieve pruritus.

14
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 40Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 40
Poisons• Injected Poisons
– Minor reactions to insect bites• Remove stinger, if present, by scraping.• Wash the bite with soap and water.• Apply cold packs; baking soda paste.
– Severe reactions to insect bites• Urticaria, wheezing, edema of the lips and tongue,
generalized pruritus, and respiratory arrest• Nursing interventions
– Apply a wide constricting band proximal to the wound; keep affected part in dependent position; transport to the hospital immediately.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 41Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 41
Drug and Alcohol Emergencies– Mild Intoxication Signs and Symptoms
• Nausea, vomiting, diarrhea, lack of coordination, and poor muscle control, flushing, erythema of the face and eyes, visual disturbances, rapid mood swings, slurred or inappropriate speech, inappropriate behavior and lethargy
– Serious Intoxication Signs and Symptoms• Drowsiness to coma, rapid weak pulse, depressed,
labored breathing or respiratory arrest, loss of control of urinary and bowel functions, disorientation, restlessness, and hallucinations
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 42Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 42
Drug and Alcohol Emergencies
• Drugs – Signs and Symptoms
• Loss of reality orientation, hallucinations, and varying degrees of consciousness; slurred speech; extremes in mood swings; inappropriate behavior; anxiety; flushed skin; diaphoresis; lack of coordination; impaired judgment; increased or decreased pulse; pupils constricted or dilated; needle marks on the arms, legs, and neck

15
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 43Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 43
Drug and Alcohol Emergencies• Nursing Interventions
– Obtain information about the substance ingested.– Life-threatening situations are handled first.– Establish airway.– If unconscious, turn on the side.– Loosen clothing.– If fever is present, apply cool, wet compresses.– Protect the victim from injury during a seizure of
hallucination.– Carefully assess mental status and vital signs
frequently.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 44Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 44
Thermal and Cold Emergencies
• Heat Injury– Heat Exhaustion
• The most common type of heat injury, this results from prolonged perspiration and the loss of large quantities of salt and water.
• Observe for signs and symptoms of headache, vertigo, nausea, weakness, and diaphoresis.
• Mental disorientation and brief loss of consciousness may occur.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 45Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 45
Thermal and Cold Emergencies
• Heat Injury (continued)– Heat Exhaustion (continued)
• Nursing interventions– Cool the victim as quickly as possible; use cold, wet
compresses and fan or air conditioner.– Have victim lie down with feet elevated.– If alert, give one-half glass of water every 15 minutes for
1 hour.– In the clinical setting, IV fluids are given.

16
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 46Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 46
Thermal and Cold Emergencies• Heat Injury (continued)
– Heatstroke• This is a more serious heat injury; death can result.• The most common cause is vigorous physical
activity in a hot, humid environment.• The body becomes overheated, but the cooling
mechanism of perspiration does not operate.• Assessment: rapidly rising body temperature; hot, dry,
erythemic skin; no visible perspiration; pulse rapid initially and then slow and blood pressure falls; breathing deep and rapid; victim complains of headache, dry mouth, nausea, and vomiting
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 47Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 47
Thermal and Cold Emergencies
• Heat Injury (continued)– Heatstroke (continued)
• Nursing interventions– Cool the victim as quickly as possible; use cold packs
around the victim’s neck, under the arms, and around the ankles to cool the blood in the main arteries.
– Establish and maintain an airway.– Monitor for chilling as the body temperature falls.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 48Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 48
Thermal and Cold Emergencies
• Exposure to Excessive Cold– Hypothermia
• Lowering of the body temperature below the normal level; 95° F or below
• Assessment– Uncontrollable shivering but ceases when body
temperature drops below 90° F– Slurred speech, memory lapses, disorientation and poor
judgment, uncoordinated gait, skin mottled and edematous, weak irregular pulse, decreased respiratory rate, loss of all reflexes

17
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 49Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 49
Thermal and Cold Emergencies
• Exposure to Excessive Cold (continued)– Hypothermia
• Nursing interventions– Initiate CPR if necessary; must continue until the body is
rewarmed.– Place victim in a supine position with the head lower than
the feet.– Rewarm slowly: move to a warm area, remove wet
clothing, and wrap with warm blankets.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 50Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 50
Thermal and Cold Emergencies• Exposure to Excessive Cold (continued)
– Frostbite• Freezing and damage of body cells• Commonly affected area are ears, nose, fingers,
and toes.• Assessment: initially, skin takes on a red flush with
numbness, tingling, and pain; progressively, the part becomes hard and loses all sensation; color turns to grayish white; if thawing occurs, may change to blue-purple or black; edema may develop, followed by blisters.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 51Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 51
Thermal and Cold Emergencies• Exposure to Excessive Cold (continued)
– Frostbite (continued)• Nursing interventions
– Treat the victim for shock and hypothermia; establish and maintain an airway.
– Warm part by immersion in warm water at 104 to 110° F for 20 to 45 minutes.
– If tub is not available, may use a hot moist towel. – Be very careful not to rub the part.– The thawed part is wrapped in clean towels or bulky
dressings and elevated.

18
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 52Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 52
Bone, Joint, and Muscle Injuries• Fractures
– A break in the continuity of a bone– Types of common fractures
• Open or compound fracture• Closed fracture• Comminuted fracture• Greenstick fracture• Spiral fracture• Impacted fracture• Compressed fracture• Depression fracture
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 53Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 53
Bone, Joint, and Muscle Injuries
• Fractures– Assessment
• Radiography can determine if a bone is fractured.• There is pain and tenderness in the area and pain
during movement.• Deformity of the limb may be obvious, with edema
and discoloration of the area.• Fragments of bone may be protruding through the
skin.• Crepitus: grating sound is heard when the affected
part is moved.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 54Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 54
Bone, Joint, and Muscle Injuries
• Fractures– Nursing Interventions
• Do not move unless he or she is in danger.• ABCs of first aid take priority.• Control bleeding if present.• Immobilize the fracture but do not attempt to
realign the bone.• Monitor circulation in the limb.• Apply ice or cold packs to the area.

19
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 55Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 55
Figure 24-14
Immobilization of fractured arm.
(From Henry, M.C., Stapleton, E.R. [1997]. EMT prehospital care. [2nd ed.]. Philadelphia: Saunders.)
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 56Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 56
Bone, Joint, and Muscle Injuries• Dislocations
– Occurs in joints; usually results from a blow or fall
– Assessment: complaints of pain and edema; deformity of the part; part may be rigid, and the victim is unable to move it.
– Nursing interventions: never attempt to reduce a dislocation; splint the joint; apply ice or cold packs.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 57Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 57
Skill 24-2: Step 4
Applying an arm splint using a triangular (sling and swathe) bandage.

20
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 58Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 58
Bone, Joint, and Muscle Injuries• Strains and Sprains
– Strains are injuries to muscle tissue from stretching and tearing due to overexertion.
– Sprains are injuries to joints resulting from stretched or torn ligaments due to twisting of the joint beyond the normal range of motion.
– Assessment– Sprains: pain or tenderness around a joint; immobility of the
joint; rapid and marked edema
– Strains: spasms of the muscle, acute pain, stiffness, and weakness on movement; back pain radiating down the leg; discoloration
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 59Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 59
Bone, Joint, and Muscle Injuries• Strains and Sprains
– Nursing Interventions• RICE
– Rest the affected extremity– Ice should be applied to the part– Compression with a compression bandage– Elevation above the level of the heart
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 60Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 60
Bone, Joint, and Muscle Injuries• Spinal Cord Injuries
– Assessment• Assess for paralysis.• Test for sensation.• Assess for abrasions and ecchymosis on the back.
– Nursing Interventions• Take spinal cord precautions.• Maintain airway; keep head in a neutral position.

21
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 61Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 61
Skill 24-3: Step 1
Moving the victim with a suspected spinal cord injury.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 62Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 62
Burn Injuries
• Shallow Partial-Thickness Burns– Involves the outer layer of the skin– Caused by simple sunburns or burns from
contact with hot objects– Nursing interventions
• The burn should be cooled immediately by soaking in cold water or applying cold compresses.
• A sterile dressing should be placed over the burn to prevent infection.
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 63Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 63
Burn Injuries
• Deep Partial-Thickness Burns– Involve the entire first layer of skin (epidermis)
as well as some of the underlying tissue.– Severe sunburn, scalding liquids, direct flame,
and chemical substances.– Assessment
• Deep erythema of the skin, or mottled skin with blister formation.
• Weeping of fluid through the skin surface and intense pain.
22
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 64Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 64
Burn Injuries• Full-Thickness Burns
– These burns involve destruction of the skin and underlying tissue, including fat, muscle, and bone.
– Skin may be thick and leathery, with black or dark brown, cherry red, or dry and milky white colors.
– The victim may not complain of pain, because nerve endings may be severed.
– Wounds weep a great deal of fluid and blood.– Causes: direct flame, explosions, and
gasoline or oil fires
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 65Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 65
• Deep Partial-Thickness Burns and Full-Thickness Burns– Nursing interventions
• Establish airway.• Assess respiratory and cardiac function.• Remove all of victim’s clothing, shoes, and jewelry.• Administer CPR if necessary.• Treat for shock.• Cool the burn with cool compresses for partial-
thickness burns.• Avoid touching the burn with anything but sterile
dressings.
Burn InjuriesBurn Injuries
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 66Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc. Slide 66
Nursing Process• Nursing Diagnoses
– Confusion, acute– Tissue perfusion, ineffective– Anxiety– Cardiac output, decreased– Hyperthermia or hypothermia– Skin integrity, impaired– Airway clearance, ineffective– Pain, acute and chronic– Posttrauma syndrome– Infection, risk for