financing drug development
TRANSCRIPT

Whitty 2 nd lecture: Economic value added
Financing Drug Development

FINANCING DRUG DEVELOPMENT
Jeremy Whitty

Economic Value Added (EVA)
• EVA is a specific type of residual income calculation that gained popularity 10+ years ago
• Weighted-average cost of capital equals the after-tax average cost of all long-term funds in use
After-tax Weighted-Average Total Current
Operating Income Cost of Capital Assets Liabilities ) }EVA {= X (

Step 2: Choosing Time Horizon of Performance Measures
• Multiple periods of evaluation are sometimes appropriate
• ROI, RI, EVA, and ROS all basically evaluate one period of time
• but may all be adapted to evaluate multiple periods of time

Step 3: Choosing Alternative Definitions for Performance Measures
• Four possible alternative investment measurements
1. Total Assets Available
2. Total Assets Employed (available – unused)
3. Total Assets Employed minus Current Liabilities
4. Stockholders’ Equity (assets - assigned liabilities by sub-unit)

Step 4: Choosing Measurement Alternatives for Performance Measures
• Possible alternative definitions of cost:
1. Current Cost
2. Gross Value of Fixed Assets
3. Net Book Value of Fixed Assets

Step 5: Choosing Target Levels of Performance
• Historically driven targets used to set new goals
• Business Plan
• Goal should include a Continuous Improvement component

Step 6: Choosing the Timing of the Feedback
• Timing of feedback depends on:
• How critical the information is for the success of the organization
• The specific level of management receiving the feedback
• The sophistication of the organization’s information technology

Intensity of Incentives
• Intensity of Incentives – how large the incentive component of an employees compensation is relative to their salary component
1. Designing performance measures for activities that require multiple tasks (quantity vs. quality)
2. Designing performance measures for activities done in teams
Well-designed plans use a compensation mix that balances risk (the effect of uncontrollable factors on the performance measure, and hence compensation) with short-run and long-run incentives to achieve the firm’s goals
Remember, you have to budget performance and compensation

• Your approach to budgeting (design, development, execution and control) must be as rigorous as your specialisation.
• CRO
• EDC
• Proj Mgt Package
• PI / Mgr
• Site
Don’t Believe the Hype
All contribute to this!

Annual Budget V Clinical Trial Budget
Capital Budget
Annual Ops
Budget
Clinical Trial
Budgets







5. MONITOR & CONTROL6. PAYMENT

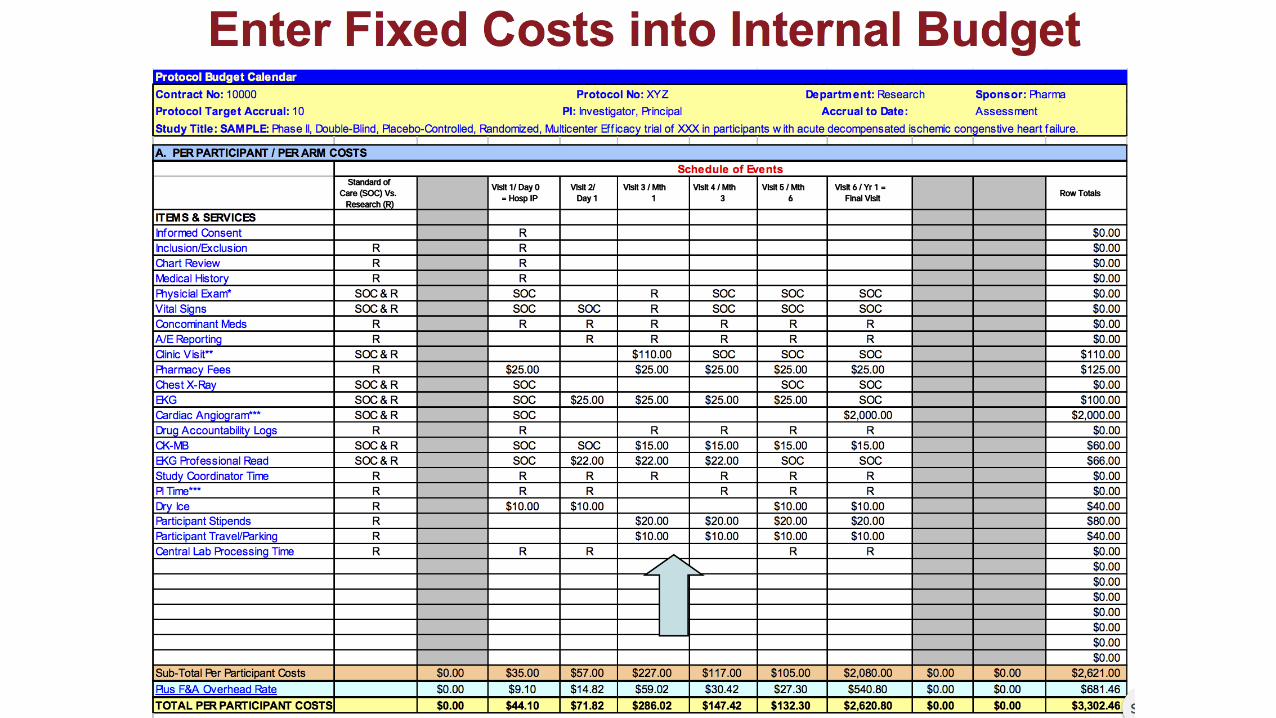
START WITH INTERNAL BUDGET

START WITH INTERNAL BUDGET

BUDGET!



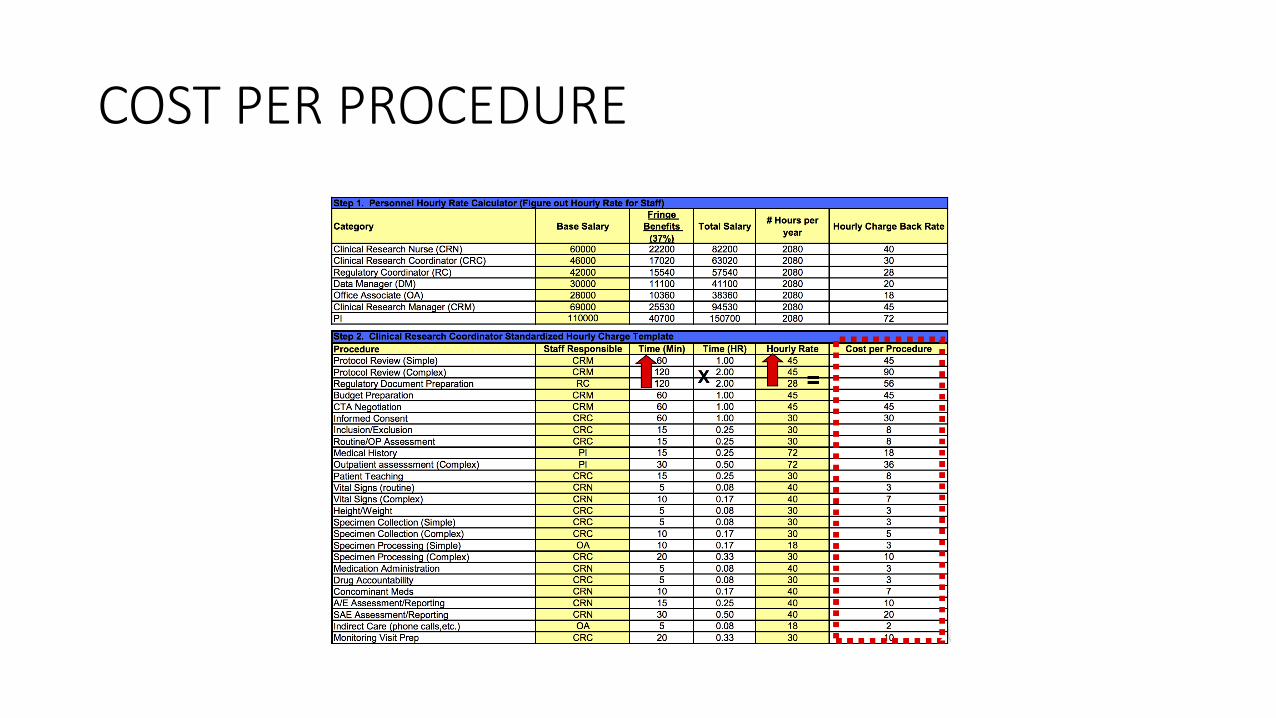
COST PER PROCEDURE

PERSONNEL COST PER PROCEDURE




REPEAT
Capital Budget
Annual Ops
Budget
Clinical Trial
Budgets

LAST TALK ....
Jeremy Whitty

it’s late ...
• You are all probably still like this ...

Nuritas
36
Founded by Dr Nora Khaldi in 2013 as a spin-out
of a university accelerator programme, Nuritas is
a fast growing start-up.
Combining life sciences and AI, they develop
advanced algorithms that mine DNA and protein
data from plant material.
Following Khaldi’s appearance at Inspirefest, the
company got U2’s Bono and The Edge to invest.
They raised a total of €5m in funding from
investors
.

Inflazome
37
Inflazome successfully raised €15m in a Series A fund
led by medtech giants Fountain Healthcare Partners
and Novartis Venture Fund,
Inflazome is a Dublin-based start-up tackling chronic
inflammatory diseases.
The name comes from inflammasome activation,
which occurs in many diseases such as Parkinson’s and
asthma.

Signum Surgical
38
Founded in 2014 Signum Surgical is a medtech start-up
striving to develop technology that could cure perianal
fistula.
The device they developed is implanted post-surgery to
prevent reinfection and to allow a faster healing process.
In November 2016, they closed out a €2.6m Series A
funding round. This funding will be used to further
develop the technology, and to submit it to the FDA to
seek regulatory approval.

Why do the case?
• Provide a context to discuss capacity expansion where capacity cannot be added in small increments.
• Expose you to the realities of the pharma industry where we must manage long lead times and lots of uncertainty
• Expose you to the details of operational planning based on estimates of future demand.
• A skill that is also useful in all financial management roles from R&D to Ops to Sales & Marketing
• Give you an appreciation of the trade offs required in making location decisions
• Introduction to some issues that are distinctive to biotech and the FDA

Intro
• While facilitating a complex clinical approval process over the next two to three years for a family of new cancer drugs, Genentech must develop a long-term capacity plan for a major class of new cancer products.
• Adding to the complexity and uncertainty is the fact that the lead time for planning, building, and certifying a new $600 million plus production-scale facility is five years.
• In addition, ensuring that the best process technology is incorporated into such a new plant makes the task facing David Ebersman, the senior vice-president of products operations, and his management team a daunting one.

Questions
• This case revolves around Genetech’s capacity planning for its newly approved and launched cancer drug, Avastin. The key issues in this case are as follows:
• Given the expected demand for Avastin and other G products ‘till 2015 and proper safety margin for production, will G encounter capacity shortage problems?
• What are the specific implications/recommendations for Ebersman’s group regarding CCP3 (location, capacity, technology) and contract manufacturing?
• What is the optimal process for Ebersman’s group in order to best plan for production capacity, both in this specific instance and on an ongoing basis?

Think about
• How to evaluate Genentechs production capacity requirements given expected demand in 2010 and 2015 for Avastin and Genentech’s other products as per Ex 3?
• Does your evaluation change if Genentech wants to cover the 85th percentile level of demand?

• Assuming they proceed with CCP3, what size production lines (tank sizes) would you recommend?
• Why?
• What criteria should Ebersman use in selecting a location?
• Why?

• What recommendations would you make to Ebersman regarding the process he and his team should use in deciding how best to meet the demands for Avastin?

Assume
• Each of the 2 contract manufacturers can devote two 10,000 L tank lines to Genentech production, and G hopes they will achieve yields similar to those at G’s own plants.
• These tanks will be fully utilised in the production of Rituxan and Herceptin

Assume We must deal with uncertainty!
• TBD dosages and treatment regimens,
• unexpected problems in the FDA’s approval process,
• unexpected success or failure of a rivals product and
• unexpectedly large or small consumer uptake.
• Therefore assume the future demand is distributed normally,
• centred on the experts’ forecasts, and with variation such that one standard deviation is about 25% of the expected demand.
• For example if expected demand is 100kg per year, then 85th
percentile demand (about one standard deviation above the expected demand) would be 125kg per annum.
Assumptions
• Adjusted demand figures in Ex 12 to include the 50% probability of success of clinical trials (as per footnote c)
• Prescribed avg patient dosage is 0.375 grams (page 8)
• CCP2 starts producing in 2009 at full capacity, while contract outsourcing of Rituxan & Herceptin stops in 2009 (i.e. those products are moved to CCP2)

Capacity V Expected Demand
• Total capacity per yr 1,872kgs in 2005 grows to 2,808 in 2009 as 200,000 L (1,170 kgs pa) new capacity becomes available from CCP2
• This compares favourably to the expected demand pa of 1,151kgs in 2005 to 2,124 in ‘10 and 2,714 in ‘15.
• Recommend postponing any investment in a new plant until expected market demand indicates much higher shortfall than current forecasts estimate.
• Can revisit plans for increasing capacity after 2010 when we have better views on the actual demand and FDA approval.

Capacity V 85%-ile Forecasted Demand
• The demand per year is 1,439kgs in 2005, increasing to 2,655kgs in 2010 in 3,426kgs in 2015.
• This leads to a capacity shortfall of 53kgs in 2007 and 297kgs in 2008, just prior to increase due to CCP2 & then another shortfall of 155kgs in 2012 growing to 618kgs by 2015.
• At $2000/dose, the cumulative revenues foregone more than $8 billion from 2012-2015
• Forget 2007-2008, it takes 5 yrs to build a plant.
• Therefore we should invest $600 million in CCP3.

Capacity V 85%-ile Forecasted Demand
• However, considering that the shortfall will start in 2012, we won’t need to make any investments until 2007.
• This gives 2 years to analyze the actual demand in 2005 and 2007 and as the FDA approval process progresses we will get better knowledge how many cancer patients could benefit from Avastin.

Capacity V 85%-ile Forecasted Demand
• Recommendation:
• Delay any investment undertakings until 2007, but keep updating capacity and demand forecasting to better plan for the investment should figures by 2007 show new capacity needed.
• In the meantime continue research on the plant size, design and location in order to have better formulation into the company needs by the time the plant investment needs to start. In addition, continue exploring new technologies for increasing protein yield, so that a new plant design could take advantage of these.

• Assuming they proceed with CCP3, what size production lines (tank sizes) would you recommend?
• Why?
• What criteria should Ebersman use in selecting a location?
• Why?

Plant Size
• Based on capacity shortfall figures, would need more than 106,000 litres
• (i.e. more than 8 tanks of 12,000 litres)
• Assuming demand will grow after 2015, I would install 8 tanks of 25,000 for a capacity of 200,000 ltrs.
• This is inline with their optimal facility size of 150,000-200,000 at a cost of $500-$600 million.
• Extra capacity will serve as a cushion for increasing demand post 2015 as no incremental production vessels could be feasibly added once the plant is built.
• In addition, there is not much additional cost of going for 8 tanks of 25,000 V 12,000

Risk?
• 25,000 ltr tanks would not have the flexibility to be used to manufacture other smaller products in lesser quantities.
• Free up Porrino in Spain which is currently dedicated to producing Avastin in 4 X 10,000 ltr tanks and consolidate all Avastin production at CCP2 and CCP3

Plant Location
• Build next to CCP2 in Vacaville?
• Buy good earthquake insurance!
• By being next to CCP2
• Leverage the highly specialised experience of scientists at CCP2.
• Smoother start up of the plant due to lessons learned
• Eliminate mgt distraction from having to operate two similar plants in two different locations & time zones

Plant Design
• Recommend using newer technologies into the plant design?
• Difficult call.
• Yes, could lead to increased protein yields, potentially doubling output.
• If we need to invest in the new plant in 2007 we have time to research new technologies and allow FDA to become familiar with these technologies to ensure plant approval.

Recommendations to Ebersman
• Even if clinical trial success was 100% the expected demand will only lead to capacity shortfall and need for CCP3 in 2011.
• This buys G time.
• 2 years before spending money to carefully review market performance of Avastins metastatic colon cancer drug & assess actual and expected demand for other drugs 2 years from now.
• FDA is very uncertain so 2 years will allow G make better decision at that time.

Contract Manufacturer• Yes there will be capacity shortfall in 2007-2008 prior to CCP2 plant coming on stream in 2009.
• Whilst the manufacturing processes for Rituxan and Herceptin are stable enough to outsource (as that have years of experience with both products), Avastin is different.
• New product, so they should not risk quality by outsourcing right away.
• Also they should be wary of opening secrets up to potential future competitors by releasing an extra product to contract manufacturers.
• The shortfall in 2007 is due mostly to demand for other drugs.
• Ask the contract manufacturer to take on these additional volumes with Rituxan and Herceptin to fill up their unused capacity instead of giving them Avastin.
• This is a win-win for G who do not forego revenue nor hand over secrets and contractor as they use their idle capacity.

YIELD @ CCP1 • Growth yield: 0.75gm/l
• Recovery yield: x65% = 0.49gm/l
• Contamination yield x80% = 0.39gm/l
• 0.39gm/l good protein *12,000 litres = 4,680gm
• = 4.68 kg/line/batch x 15 batches/yr = 70.2kg/line/yr
• CCP1 (with 12 lines) makes 70.2*12 = 842.4 kg/good protein /yr
• That’s less than 1 cubic meter.
• A desk is roughly 1 cubic meter, how much would my desk be worth if product?

YIELD @ CCP1
• $2,000 per 375 mg (0.000375 kg) dose, this desk sized quantity has a market value of $4.5 Billion!

The Importance of Attention to detail

What happened
• April 5: Request to replace thermo-probe on this Autoclave: • It has being giving problems since December.
• April 6. Begin batch D1192/C
• SOP:• Load autoclave
• Close door, tighten handles firmly
• Close condensate drain valve
• Check other valves closed
• Open vacuum valve
• Open main steam valve at 15 inches vacuum
• When pressure just above atmospheric open condensate valve
• Unwritten amendment: Steam shuts off at intervals, read pressure before continuing steaming ensure that there is a slight positive pressure in the chamber before opening the condensate drain valve

What happened
• SOP: Close condensate valve when condensate drain temperature reaches 240°F (115°C) on temperature chart
• SOP: Mark recorder chart when 240°F reached - external pressure gauge should read 10 pounds per square inch (processing time 40 minutes)
• Unwritten amendments: Close the valve when the temperature reached 220°F
• Processing time less than 30 minutes
• Problem with the temperature recorder on Autoclave No 4
• SOP Report the problem to Supervisor
• Supervisor and immediate superior absent
• Unwritten procedure: Check the steam drain and the steam trap are working
• Continue cycle based on correct pressure and temperature gauge readings (external instrumentation)

What happened
• What they did not realise was that the bottom 3rd of the autoclave was not reaching 100°C & external gauges were only measuring top of the chamber
• 25 April. Batch released
• 25 February. Gillian Myatt admitted to Plymouth General Hospital
• 33 years old mother of two
• Surgery for thrombosis in left leg
• Collapsed 34 hours post-operation
• died 6 hours later - 1 March
• Given dextrose IV infusion from batch D1192/C
• Klebsiella aerogenes var oxytoca isolated from lungs

What happened
Clothier Report: # of shortcomings in management ....Failure of:
the Autoclave operator to follow his instructionsHis supervisor who should have checked work was carried outMr Devonport, the manager of the transfusion unit did not check on his
staff and relied too much on supervisorSupervisor knew autoclave was faulty and thought bringing it to the
notice of Engineering was enoughLargest blame rested with Davonport's boss who failed to provide
Devonport with training nor did he monitor Devonport's performance or capability.
Senior Management were largely blameless.Really?

What Clothier did not tell us:
• Devonport, the QP had voiced his concerns that the autoclave was not working
• He was threatened with the sack by the “largely blameless” senior management if he did not release the product.
• As a result 5 patients died in total

Mix Ups
• Mix Up:• Confusion regarding an item’s identity or status
• Area clearances should ensure labels and documentation are removed.
• Labelling Mix Ups:• 93% of deaths
• 93% of recalls

Consequences
• The Star, January 27, 1999
• Brussels: German pharmaceuticals manufacturer B.Braun has accepted responsibility for the death of two Belgian babies who died after being injected with potassium chloride from vials that were supposed to contain harmless glucose solution. The company said that a “double human error” at one of its plants results in the wrong labelling of the vital vials.
• Aircraft Crash:
• Experienced pilots looking at instrument panel & saying “I don’t believe that” as they pump fuel from the plane.

Industry Today
• Cycle time from experimental drug to medicine chest can take anywhere from 7 to 12 years.
• Only 5 in 40,000 compounds screened in animal testing make it to human testing.
• Of the five tested in humans only one is approved.
• Development cost is close to $1.2 billion.
J. Kindler: “The company must change in ways that are fundamental and sustained. We
need to look at everything we do with fresh eyes ... to make sure we‘re
operating nimbly and decisively”.

Industry Today• “The golden age of medicine was traditionally looked at as the 1940’s, 1950’s, the development of
antibiotics. Based on what we now know about the human genome, more careful targeting of discovery efforts, you haven’t seen anything yet. The golden age of medicine clearly lies ahead of us.” Henry McKinnell, Chairman and CEO, Pfizer in 2006.
Historically
Price = Cost + Profit
Profit = Price – Cost
NOW
24

The New Economics of Innovation
Historical margins
Historicalrevenues
Revenues with greaterprice pressures andshorter cycles
Productintroduction
€/$
Years from product launch
Historical fixed development and manufacturing costs
6 12
New fixed development and manufacturing costs
Margins in new environment
19

How is the industry adapting?

Who is equipped to lead in this environment?

How is science adapting?
LoC captures single cells from a mix, isolate rare cells and
count cells based on cell types.
Cancer, Malaria, tuberculosis and HIV
Flow Cytometer sorts and count cells

How is the industry adapting?
€1 €100,000

Don’t judge the ostrich

until you see the view

Bethlehem Steel

I keep six honest serving-men
(They taught me all I knew);
Their names are What and Why and When
And How and Where and Who.
Rudyard Kipling
Always ask questions &

Ever tried.
Ever failed. No matter.
Try again.
Fail again.
Fail better
Samuel Beckett
be prepared to fail
