final paper.docx - web viewresults indicating common unhealthy dietary trends including sweet and...
TRANSCRIPT

Running Head: Nutrition in Lao Nadi
Nutrition in Lao Nadi
Lucy Aranda, Michael Marino, Mackenzie O’Brien, Veronica Thao, Elsa Weltzien
Khon Kaen University
Running head: Nutrition in Lao Nadi
Abstract
Thailand and other countries in Southeast Asia have recently undergone a nutritional
transition, resulting in changes in dietary trends to more similar to a Western diet.
Consequently, there have been increases in the rates of chronic degenerative diseases
including hypertension, diabetes mellitus and heart disease. Research in the form of semi-
structured interviews was performed in the Lao Nadi slum community of urban Khon Kaen,
Thailand to explore: What are the top five dietary trends among the Lao Nadi community;
(2) How do they affect villagers’ nutritional status; (3) What are some factors in diet that
contribute to hypertension, diabetes, and obesity? Results indicating common unhealthy
dietary trends including sweet and oily food consumption and lack of formal nutritional
education were used to create a culturally sensitive nutrition intervention for the community
that was attended by 24-26 participants. Topics covered were portion size, the Thai Nutrition
Flag, and balanced meal planning. Evaluation demonstrates a successful intervention with an
increase in participant knowledge but a need to research and address more specific
community nutritional needs.
2
Running head: Nutrition in Lao Nadi
1. Introduction
Over the past few decades, Asian countries including those in Southeast Asia have
experienced rapid socio-economic development resulting in increased urbanization and
Westernization and leading to changes in dietary patterns. There has been a shift from a
more traditional diet based on starches and low in fat to a diet “characterized by increased
consumption of animal products, fats and sugars and decreasing consumption of complex
carbohydrate foods” (Kosulwat, 2002). As an example, Malaysia has seen degenerative
diseases including coronary heart disease, hypertension, diabetes, and obesity become
prominent (Noor, 2002). It has been projected that by 2020, chronic diseases will account for
three-quarters of all deaths worldwide, in both developed and developing/middle-income
nations (WHO, 2002). In Thailand, when considering the overall causes of death, the leading
causes are diet-related chronic degenerative diseases (Kosulwat, 2002). This is comparable
to the highly developed United States. As of 2010, heart disease, stroke, and diabetes graced
the top 10 causes of death of both countries (CDC, 2010).
The location for this research project was Lao Nadi, a railroad slum community with
a population of 238 people located in Khon Kaen, Thailand, existing on one main road.
Research was guided by the goals of understanding community members’ nutritional status
and their knowledge on healthy eating. These goals were guided by three main research
questions (1)What are the top five dietary trends among the Lao Nadi community; (2) How
do they affect villagers’ nutritional status; (3) What are some factors in diet that contribute
to hypertension, diabetes, and obesity? Data collected in the form of semi-structured
interviews was then used to create and implement a nutrition intervention in Lao Nadi.
3

Running head: Nutrition in Lao Nadi
As illustrated by previous studies, health problems in Thailand are influenced by a variety
of factors including socioeconomic changes, cultural ties, and limited access to resources and
education. Research has found significant connections between nutrition and chronic illness in
Thailand. Previous campaigns and interventions have focused mainly on screening and
management of nutrition-related chronic diseases, lacking a focus on primary prevention and
basic nutritional behaviors. Therefore, the research and intervention initiatives made in Lao Nadi
have the purpose to use basic nutritional information to encourage community members to find
solutions to improve the nutritional health status of their community and to increase their access
to healthier food choices.
2. Literature Review
According to the World Health Organization (1990), “nutrition is coming to the fore as a
major modifiable determinant of chronic non-communicable disease (NCD), with scientific
evidence increasingly supporting the view that alterations in diet have strong effects, both
positive and negative, on health throughout life” (p. 1). The risk of developing a NCD is
compounded by “motorized transportation, labor-saving devices in the home, the phasing out of
physically demanding manual tasks in the workplace, and leisure time that is devoted to
physically undemanding pastimes” (WHO, 2003). These fairly recent changes in dietary and
lifestyle patterns have caused “chronic NCDs to become significant causes of disability and
premature death in both developing and newly developed countries” (WHO, 2003). Third,
(WHO, 2003) also says “one of the problems is that in many developing countries, food policies
remain focused only on undernutrition and are not addressing the prevention of chronic disease.”
Our research sought to address this gap in health policy by trying to identify the nutrition-related
causes of chronic disease in the Lao Nadi community. Our intervention also focused on the lack
4

Running head: Nutrition in Lao Nadi
of chronic disease prevention policy by educating the community about the three most prevalent
NCDs in Lao Nadi.
Taechangam et al. (2008) center the discussion of nutrition-related chronic illnesses
specifically on Thailand, explaining that: “Thai staples, which are rich in complex carbohydrates,
are being replaced by diets containing a higher proportion of fats and animal meat which can be
critically harmful for health” (p. 1). Thailand’s recent “dietary shift towards processed, calorie
dense foods” comes with the territory of being a “rapidly developing nation” and this
“contributes to Thailand’s double burden of disease” (Kelly et al., 2010, p. 1). When a country is
facing a double burden of disease, it simply means that there are health threats from both non-
communicable diseases as well as communicable infectious diseases.
Clearly, nutrition is a key factor in the discussion of diet-related chronic illnesses. To
provide guidelines for proper diets, Thai Food Based Dietary Guidelines (FBDG) and a Thai
Nutritional Flag were developed by the Food and Agricultural Organization and World Health
organization. These tools are intended to help address nutritional transition based health issues
regarding undernutrition and overnutrition. The FBDGs include the recommendations that an
individual should “eat a variety of foods from each of the five food groups and maintain proper
weight, eat adequate rice or alternate carbohydrates, eat plenty of vegetables and fruits regularly,
eat fish/lean meats/eggs/legumes/pulses regularly, drink a sufficient amount of milk every day,
eat moderate amounts of fat, avoid excessive intake of sweet and salty foods, eat clean and
uncontaminated foods, and avoid or reduce consumption of alcoholic beverages (Sirichakwal et
al., 2011, p. 477).” Sirichakwal et al. emphasize that, “FBDGs have been considered as one of
the most important tools for nutrition education, communication for promotion of desirable of
eating habits, and nutritional well being and good health” (p. 477). FBDGs can also be used for
5

Running head: Nutrition in Lao Nadi
“setting up food and nutritional policy and strategy in health, education, and agriculture because
they create demand for healthy diets which will lead to the supply of appropriate nutritious and
safe food in various settings (p. 477).” Overall, FBDGs have the potential to help guide
communities in making healthier food choices.
The article by Sirichakwal et al. (2011) helped us to shape our nutrition intervention in
Lao Nadi. For example, the intervention was designed so that each component included simple
health tips and guidelines. Each of the Thai FBDGs were addressed and additional tips were also
provided to the participants. Furthermore, a 3’x5’ Thai Nutritional Flag was hung in the center
of the community and each participant received a miniature Thai Nutritional Flag.
While limited nutritional health information affects many communities of Thailand,
culture also perpetuates food-induced health problems. More specifically, the cultural importance
of certain foods has an effect on nutritional health status. Leedom Lefferts (2005) discusses the
complicated relationship between poor food choices and the challenge of eliminating these foods
due to their cultural significance in Thailand. More specifically, in the Northeast region of
Thailand, “Isaan culture has a long-rooted history of consuming traditional foods high in
unhealthy salts, fats, and sugars” (p. 247). For example, “one staple food in the Isaan diet
includes sticky rice, which is typically consumed by people on a daily basis” (Lefferts, 2005, p.
247). Ultimately, “sticky rice is a symbol of unity and identity for Isaan people and it is difficult
to totally eliminate it from people’s diets because it is significant to Isaan culture and tradition”
(Lefferts, 2005, p. 247). The sticky rice example highlights the larger conflict that results from
the strong cultural attachment to certain Thai foods.
More importantly, Lefferts’ article highlights a serious issue of how the culture
complicates behavioral changes related to food choice and nutritional health status. Therefore,
6

Running head: Nutrition in Lao Nadi
“when addressing health problems that can arise from eating traditional Thai foods, it is
important to ensure that Thai culture and tradition are kept in consideration” (Lefferts, 2005, p.
258). Overall, Lefferts’ findings indicate a need for the “distribution of more comprehensive
nutritional information to communities in the Northeast region of Thailand while remaining
culturally sensitive” (p. 248). Related to his suggestions is the research of Gibson and Ferguson.
According to Gibson and Ferguson (1998), “to implement effective dietary strategies,
knowledge of the local dietary patterns, food beliefs, preferences and taboos is required, as well
as the ability to change attitudes and practices” (p. 123)
These two articles were particularly useful in helping researchers to develop an effective
and successful nutrition-related intervention in Thailand. It was not difficult for the researchers
to respect Thai culture and tradition because of our unique position as CIEE study abroad
students. To elaborate, over the course of the student group’s four months in Thailand, they had
multiple opportunities to live in the Lao Nadi community. We were able to glean a lot of
important information about Lao Nadi’s culture and traditions from these homestays through
observing ceremonies, helping to cook, and conducting research interviews, to name a few. Each
of the semi-structured interview questions were chosen specifically to obtain information about
Lao Nadi’s local dietary patterns, food beliefs, preferences, and taboos, as recommended by
Gibson and Ferguson (1998). In addition, building personal relationships with members of the
potential intervention audience allowed us to integrate into the Isaan culture.
According to Davis et al. (2012), “there is evidence that group programs can be more
effective than individual or self help approaches to weight management” (p. 176). Davis et al.
also cite a study by Heshka et al. (2003) stating that “one trial found that a multi-component
commercial group program (Weight Watchers) was more effective in terms of weight loss and
7

Running head: Nutrition in Lao Nadi
weight control over a 2-year period than individualized or self help programs.” Finally, Davis et
al. cite Waleekhachonloet et al., (2007) who compared group behavior therapy with individual
behavior therapy for promoting healthy dieting behavior and weight control in overweight and
obese women in a rural community in Thailand. The group behavior therapy was found to be
“practical, cost and time effective and not inferior to individual therapy in terms of
effectiveness” (p. 230). The added bonus of Waleekhachonloet et al.’s (2007) research is that it
is applicable to obese women in rural Thailand. “The most promising programs are those that
address the needs and concerns of the target communities using culturally appropriate methods
and messages” (Doak, 2002).
Colleen Doak’s (2002) journal article further validates the need for research and
subsequent nutrition interventions, stating that, “early prevention is a necessary, cost-effective
means of avoiding the high social, biological and economic costs of a treatment-based approach
to nutrition-related chronic diseases” (p. 275). According to Doak (2002), “assessment of the
extent of overweight, obesity and nutrition-related chronic diseases is critical to addressing the
problem” (p. 275). This assessment should be the responsibility of the Lao Nadi village health
volunteers (VHVs), however the responses gathered from our semi-structured interviews indicate
that VHVs in the Lao Nadi community are not as accessible as they should be.
Doak (2002) also relates to our survey question about nutrition education in school. “A
school-based program began in Thailand in September, 2001. This program, in regional primary
and secondary schools, focuses on physical activity and a healthy diet” (p. 275). This statement
validates the “yes” responses to the survey question “is nutrition education provided in schools?”
For adults, “the workplace is ideal for interventions reaching adults and the promotion of
physical activity in Thailand in the workplace is among the strategies of health promotion in the
8

Running head: Nutrition in Lao Nadi
National Plan, although implementation of this varies by region” (Doak, 2002, p. 276). This
statement supports the need for our nutrition intervention because even if health promotion exists
in workplaces, there is a lack of health promotion in the community. Finally, “national
campaigns in Thailand for nutrition-related chronic disease prevention focus on screening and
management of nutrition-related chronic diseases such as hypertension and diabetes” (Doak,
2002, p. 277). The presence of these chronic disease campaigns is promising; however, while
screening is a form of secondary prevention, there is a gap in primary prevention. Our
intervention addresses this gap in policy by focusing completely on prevention instead of
management.
Raiha et al., (2012) evaluated the effects of a nutritional health intervention on student’s
nutrition knowledge and eating habits from grade seven to grade nine. The researchers suggest
that “more attention should be paid to the importance of actively involving parents in the effort”
(Raiha et al., 2012, p. 280). More specifically, Raiha et al. cite Woolfe & Stockley (2005)
stating that “attention should be paid to committing parents to the intervention and promoting
nutritional health within the entire school community including political decision-makers in the
local community.” Our intervention mimicked this strategy by involving the parents of children
as well as the village headman.
As illustrated by scholars and organizations alike, health problems in Thailand are
influenced by a variety of factors including socioeconomic changes, cultural ties, and limited
access to resources and education. It is important that research efforts continue to explore these
topics to better understand and address these nutrition-related health problems in Thailand.
9

Running head: Nutrition in Lao Nadi
Taken as a whole, previous research has made it evident that there are significant
connections between nutrition and chronic illness in Thailand. Therefore, the nutritional status
of the railroad slum community, Lao Nadi, was of interest to researchers and community alike.
While communities may understand the basic connection between their food choices and the
potential increased risk of disease, many do not fully understand the extent to which their food
choices and poor eating habits can negatively impact their overall health status. Therefore, it is
important that research initiatives are made to better educate communities about nutrition and to
increase their access to healthier food choices.
3. Methods
3.1 Sample population
The target population of interest for the pre-intervention data collection period was adults
aged 30 and up, both males and females. The age of 30 was selected as a minimum age because
people within this age range are more likely to be the ones doing the majority of the food
preparation and purchasing for the family. No target gender was selected in consideration of the
small population size of Lao Nadi, to avoid difficulties in finding participants. The sample size
for data collection was 30 individuals, aged 30 or older, from the Lao Nadi community.
Convenience sampling was used because of the restricted size of Lao Nadi and available time
allotted for data collection. Participants were selected by random, by the researchers walking
down the single street of the community and asking whoever was available that met the age
criteria if they would be willing to partake in the survey. Data collection was conducted during a
weekend to allow a potentially wider selection of available participants, as opposed to
conducting research during a workday where it was likely that many people would not be home.
Although the target population for the pre-intervention period was restricted to 30 and older, the
10
Running head: Nutrition in Lao Nadi
target population for the intervention was open to any and all ages, along with all genders. The
reason for this was again based on Lao Nadi’s small community size, but also because the
students did not want to limit the pool of participants.
3.2 Measurements
In order to collect data about the dietary habits of community members and their
knowledge on proper nutrition, the students conducted semi-structured interviews with the
sample population in Lao Nadi community. A list of basic questions regarding individuals’
general eating behaviors, current health status, and their access to nutrition information was
asked to gain a sense what should be addressed during the intervention. Information gathered
was both qualitative and quantitative. A total of 10 questions were asked, covering a few
different topics. Students began each interview with an introduction of themselves as U.S.
international students studying public health at Khon Kaen University and presented their
research purpose as gathering information on nutrition with the Lao Nadi community. They then
asked for the individuals’ consent to partake in a questionnaire to contribute to their research.
The questionnaire included questions asking for the individuals age, gender, whether or not they
had any existing chronic diseases, what types of foods they typically ate and drinks they drank
for breakfast, lunch, dinner and snacks, how these meals were prepared and where the
ingredients were purchased from. In order to gain a better perspective on participants’ knowledge
on nutrition, the questionnaire also asked where the individual received their nutrition
information from along with if they believed their community was doing enough to fill this part.
3.3 Budget
The student group requested a total of 9,997 B for the nutrition intervention in Lao Nadi as
described above. The majority of funds went to the translator and translations, and materials for
11
Running head: Nutrition in Lao Nadi
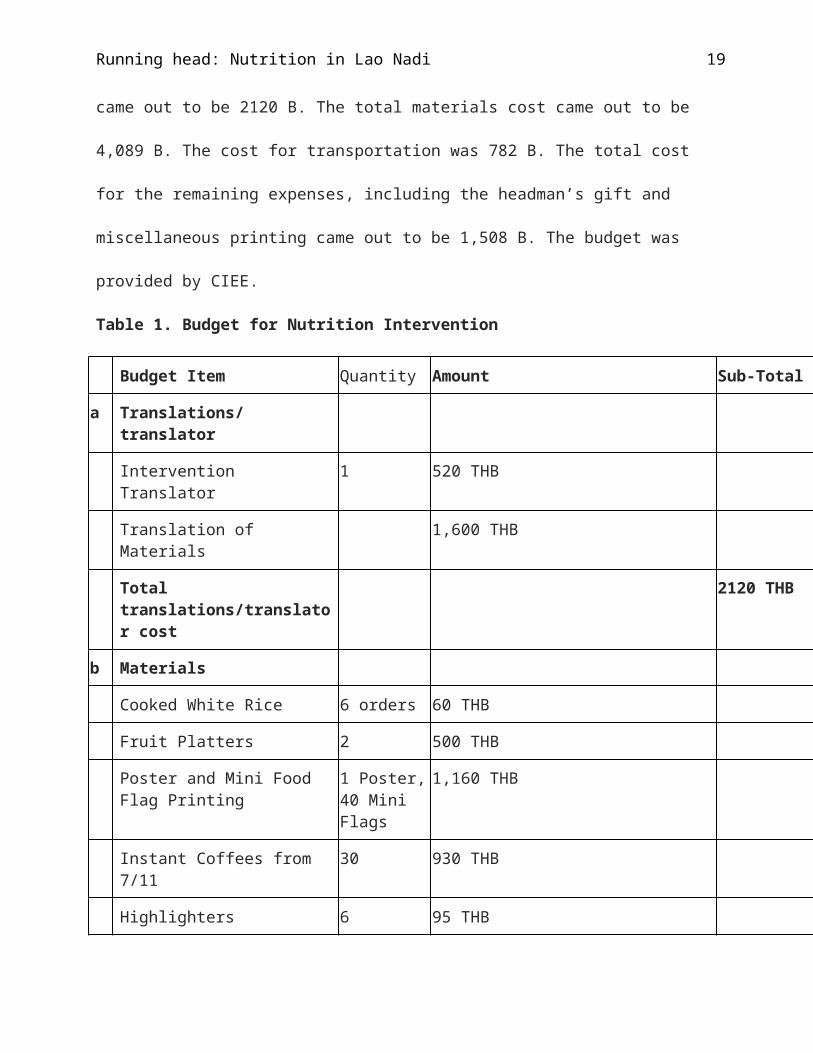
the actual intervention. The total translations/translator cost came out to be 2120 B. The total
materials cost came out to be 4,089 B. The cost for transportation was 782 B. The total cost for
the remaining expenses, including the headman’s gift and miscellaneous printing came out to be
1,508 B. The budget was provided by CIEE.
Table 1. Budget for Nutrition Intervention
Budget Item Quantity Amount Sub-Total
a Translations/translator
Intervention Translator 1 520 THB
Translation of Materials 1,600 THB
Total translations/translator cost
2120 THB
b Materials
Cooked White Rice 6 orders 60 THB
Fruit Platters 2 500 THB
Poster and Mini Food Flag Printing
1 Poster, 40 Mini Flags
1,160 THB
Instant Coffees from 7/11 30 930 THB
Highlighters 6 95 THB
Ink Pens 40 240 THB
Napkins for Intervention 1 pack of 50 5 THB
Hooks for hanging large poster 4 47 THB
Bags of seaweed crisps 4 120 THB
Water for intervention 4 packs of 12 104 THB
Coffee from Tesco Lotus 10 290 THB
Paper cups 5 115 THB
Coffee stirring spoons 1 pack of 50 25 THB
12

Running head: Nutrition in Lao Nadi
Plate 1 39 THB
Rice serving spoon 1 15 THB
Plastic gift bags 1 pack 29 THB
Sugar 1 pack 22 THB
Creamer 1 pack 39 THB
Bowls 2 packs 58 THB
Sunflower granola bars 2 bars 26 THB
Pumpkin chips 1 box 44 THB
Mixed Nut and pumpkin seed granola bars
4 72 THB
Uncooked White Rice 1 bag 34 THB
Roll of tape 1 20 THB
Total Material Cost 4089 THB
c Transportation Cost
Taxi to and from Tesco Lotus 132 THB
Songtaew rides 650 THB
Total Transportation Cost 782 THB
Miscellaneous printing 118 THB
Village Headman’s Gift: Gas Stove
1 1390 THB
Total Other Cost 1508 THB
Total Cost 8499 THB
Total Request: 10000 THB
13

Running head: Nutrition in Lao Nadi
3.4 Timeline
3.4.1 Research and Intervention: November 21-December 3, 2013
Length of task
Day 1 Nov 21
Day 2 Nov 23
Day 3 Nov 24
Day 4 Nov 25
Day 5 Nov 26
Day 6 Nov 29
Day 7 Dec 2
Day 8 Dec 3
Consultation with Aj. Pattara
2
X
X
Data Collection
2 X X
Consultation with Aj. Jen and P. Fac
1
X
Materials Translated and Printed
1
X
Materials Purchased
1 X
Intervention Run-Through
1
X
Intervention 1 X
Debriefing 1 X
14

Running head: Nutrition in Lao Nadi
3.4.2 Intervention Day Timeline: December 3, 2013
15:00 Meet at CIEE and brief translator
16:00 Leave for community
16:30 Arrive and set-up intervention space
17:00 Begin intervention
17:00-17:30 Disease, Portion Size, Nutrition Lecture
17:30-17:40 Snack Break
17:40-17:55 Daily Food Activity
17:55-18:00 Question and Answer Session and Discussion
18:00-18:30 Clean up and talk with community members
3.5 Outcome Measurements
In order to measure the success of the intervention and the knowledge that was learned by
the participants through this intervention, questions were asked directly post-intervention. These
questions related back to the information that was taught during the nutrition education section.
● What is the maximum servings of rice should one eat daily?
● What are healthy snack options?
● What did you learn throughout this presentation?
These questions correlate to the success because the participant’s correct answers show
that the information was well taught and knowledge was retained even after the intervention. If a
participant stated a false answer this would have meant that the information was not presented
clearly or correctly. Thankfully, all of the participants answered the questions correctly and even
provided valuable information when discussing what they had learned. One participant stated
15

Running head: Nutrition in Lao Nadi
that they learned breakfast was the most important meal of the day and should not be skipped.
This truly shows the intervention was successful as that was a point that was continuously
stressed throughout. Others learned the importance of portion control and nutrition balance. This
post-intervention discussion allowed participants to talk freely. Many even asked questions of
their own, further showing that they learned and desired to learn more from the student
presenters. Furthermore, participants talked amongst themselves as they were leaving the
meeting area, collecting extra daily nutrition guides and Thai nutrition flags for their family and
friends. In conclusion, the participation that was evident throughout the entire intervention shows
a successful intervention. Their continued desire for more information and the successful
discussion towards the end is a true measure of the participant’s gained knowledge.
3.6 Data Analysis
Prior to the intervention the data that was collected was qualitative for the most part. The
majority of the questions in the semi-structured interview relied on open-ended answers such as
varying food that was consumed. In contrast, the quantitative information that was collected was
age, gender, history of disease, and whether nutrition was learned in the community or in
schools. This information is quantitative because it is objective, but is helpful when separating
the backgrounds of each participant.
Due to the purpose of the research, the best data analyzing came from the qualitative
answers. This is because answers could remain subjective to each individual participant.
Nonetheless, each answer was collected and categorized into qualitative versus quantitative
sections. From this point the answers were broken up question by question to see if there was a
correlation between the data that was received. Correlations were noted and the quantitative data
was placed in charts and tables for better representation. Though they are useful in analyzing
16

Running head: Nutrition in Lao Nadi
separate styles of data, using both tools together is helpful in getting an overall understanding of
the answers the interviewee provided.
Post-intervention there was no data to be collected as there was no formal post-test or
questionnaire. The answers that were collected after the intervention were simply observations of
the intervention participants made by the students. Similarly, when asked what the participants
learned their answers are not necessary to be analyzed.
3.7 Ethics
As the intervention began, there was an introduction to explain who the students were, as
well as, the purpose of the intervention itself. It was set up as a voluntary meeting in the common
area, so individuals were invited but not forced to participate. No names, ages, or genders were
recorded at any point in the intervention to remain anonymity and encourage all to participate.
No personal information was asked of any participants. At the end of the intervention,
participants were thanked for their voluntary service towards our own personal education. There
has been no contact with the participants post-intervention day, maintaining the anonymity of all.
4. Results
Prior to our intervention, the results of our research include: demographic information
about the sample population, access to nutritional information in the community, top foods
consumed for breakfast, lunch, and dinner, and a total of thirty community members from Lao
Nadi were recruited in our study. The demographics of our sample population include gender
and age. 66.6% of the participants were female, while 33.3% of the participants were males
(Table 1). The lower number of male participants may be due in part to the fact that many males
were not available at the time of our interviews. Additionally, there is a larger female presence
among Lao Nadi community. This may be reflective of the actual gender distribution of Lao
17
Running head: Nutrition in Lao Nadi
Nadi community. All participants were required to be thirty years or older to participate in our
study, the average of all participants was 49 years of age (Table 2). The age distribution among
our sample population is reflective of Thailand’s growing elderly population. According to the
United Nation’s Population Fund’s study titled Population Ageing in Thailand: Prognosis and
Policy Response, “[Thailand] has now moved up to be the second most aged country in the
region (next to Singapore), with older persons constituting more than 10 per cent of the
population (UNFPA, p. 2).”
Table 1. Distribution of Participants by Gender
Male Female Total10 20 30
% Male % Female % Total33.33333333 66.66666667 100
Table 2. Distribution of Participants by Age
Youngest Oldest Average Age32 76 49.3809524
Our thirty semi-structured interviews with Lao Nadi community indicate that there was little
nutritional information available to Lao Nadi community. As displayed in Figure 1, of the thirty
participants, who responded to the question, “Do you learn about nutrition in Lao Nadi?” 53% of
all participants answered “no” (Figure 1).
18
Running head: Nutrition in Lao Nadi
Figure 1.
Community Members Learn about Nutrition in Lao Nadi
YesNoI Don't Know
While we assessed community members’ access to nutritional information in Lao Nadi, we
further discussed other options for accessing nutritional information. Many community members
received health information from their health care providers, such as nurses and doctors.
However, sixteen participants answered that “nobody” taught them about proper nutrition
(Figure 2).
Figure 2
19

Running head: Nutrition in Lao Nadi
Nobody
TV
VHV
School
Nurse
0 2 4 6 8 10 12 14 16 18
Resources for Learning about Nutri-tion in Lao Nadi Community
Number of VillagersIndi
vidu
als t
hat V
illag
ers L
earn
Fro
m
Additionally, we focused on learning about the different types of foods that are
commonly eaten by community members. In Figure 3, the top answers for ‘What do you
typically eat for breakfast?’ include: 1) white rice 2) nothing 3) stir-fried vegetables 4) omelets,
fish, stir-fried pork, sticky rice, bread, 5) boiled vegetables, boiled egg, steamed vegetables,
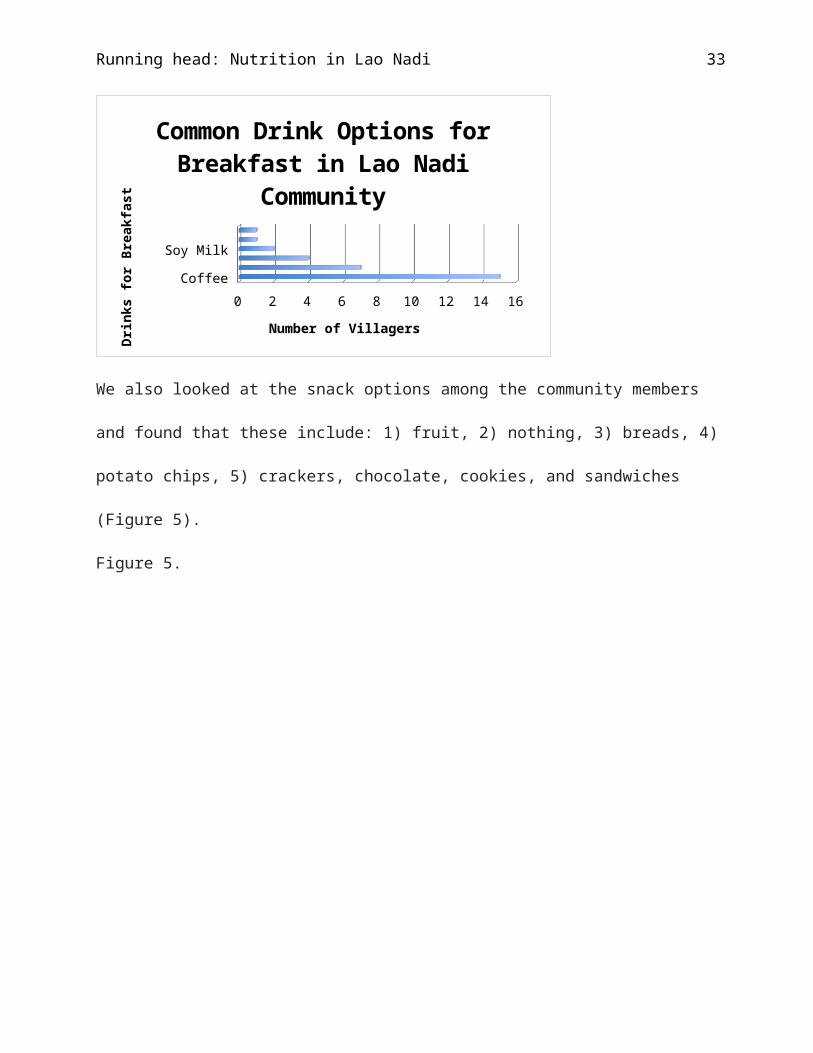
sweet bun, soups and noodles, fried rice, oatmeal. The most popular drink option for breakfast is
3 in 1 coffee, as displayed in Figure 4.
Figure 3.
20

Running head: Nutrition in Lao Nadi
Bread
Cereal
Grilled Pork
Soup/Noodle
Stir Fried Prk
Sweet Bun
Steamed Veg
Boiled Veg
White Rice
0 1 2 3 4 5 6 7 8 9
Common Foods Eaten for Breakfast in Lao Nadi Community
Number of Villagers
Food
s Eat
en fo
r B
reak
fast
Figure 4.
CoffeeWaterMilk
Soy MilkWhiskey
Beer
0 2 4 6 8 10 12 14 16
Common Drink Options for Breakfast in Lao Nadi Community
Number of Villagers
Dri
nks f
or B
reak
fast
We also looked at the snack options among the community members and found that these
include: 1) fruit, 2) nothing, 3) breads, 4) potato chips, 5) crackers, chocolate, cookies, and
sandwiches (Figure 5).
21

Running head: Nutrition in Lao Nadi
Figure 5.
VietnameseGrilled Pork
Cake Yogurt
SandwichCookie
ChocolateCrackers
Potato Chips
BreadsNothing
Fruit
0 1 2 3 4 5 6 7 8 9
Common Snacks for Lao Nadi Community
Number of Villagers
Food
s
We continued to look at the top foods for all meals: breakfast, lunch, and dinner, as well as
snacks. For lunch, som tam, sticky rice, white rice, and soups/noodles were popular dishes
among Lao Nadi community members. These options are reflective of the high consumption of
rice, that is staple to the Asian diet (Kiple, Ornelas).
Figure 6.
22

Running head: Nutrition in Lao Nadi
Sticky RiceWhite RiceFried Rice
Fresh VeggiesStirfried VeggiesSteamed veggies
ChickenBoiled Chicken
Stirfried ChickenGrilled Chicken
Fried ChickenPork
Boiled PorkStirfried PorkGrilled Pork
Fried PorkFish
Steamed FishBoiled FishGrilled Fish
Fried FishFried Egg
Noodles and SoupsGreen Salads
FruitsSom Tam
0 2 4 6 8 10 12 14 16 18
Common Foods for Lunch in Lao Nadi Community
For dinner, white rice, sticky rice, stirfried vegetables, stirfried pork, and soups and noodles were
some of the top foods that community members choose (Figure. Again, rice is consumed in high
numbers. Therefore, we concluded that it was important to limit rice intake and incorporate this
into our intervention nutritional information session.
Figure 7.
23

Running head: Nutrition in Lao Nadi
Sticky RiceWhite Rice
Boiled RiceStirfried VeggiesSteamed Veggies
Boiled ChickenFried Chicken
Grilled ChickenStirfried Chicken
Boiled PorkFried Pork
Grilled PorkStirfried Pork
FishSteamed Fish
Boiled FishFried Fish
Stirfried FishFried Egg
Soups/NoodlesGreen Salad
FruitsSom Tam
0 2 4 6 8 10 12 14 16 18 20
Common Foods for Dinner in Lao Nadi Comunity
Number of Villagers
Food
s for
Din
ner
In regard to meal trends, we found 53.8% declared dinner as their biggest meal of the
day. After collecting all of our data, we found that a significant number of participants did not
list foods for breakfast, and discovered that 30% of the participants did not eat breakfast
altogether (Figure 5).
Figure 9.
24
Running head: Nutrition in Lao Nadi
Breakfast
Lunch
Dinner
0 2 4 6 8 10 12 14 16
Biggest Meal of the Day among Lao Nadi Com-
munity Members
Number of Villagers
Mea
ls
In our research, we also explored issues of access and affordability of healthy food
options, as well access to processed foods. Therefore, we asked participants where they typically
shop for groceries. As displayed in Figure 10, we found that 73% shop at the downtown market,
13% shop at Tesco Lotus, 4% shop at 7-11 convenient store, and 3% shop at Tops Super Market,
3% shop at Ton Tann market, and 3% prefer to go fishing for their own fresh fish.
Figure 10.
Dwntwn Mkt71%
Seven-Eleven3%
Comm. Mkt3%
Tesco Lotus13%
Ton Tann3%
Fishing 3%
Topps3%
Places where Lao Nadi Community Members Buy Food
25

Running head: Nutrition in Lao Nadi
Furthermore, we asked participants “Do you have any health problems or illnesses?” Of the 30
participants, 14 mentioned that they were diagnosed with one, two, or three of the following
diseases: diabetes, hypertension, and heart disease. These three diseases are likely linked to poor
dietary habits ( Bumrungrad International Hospital).
Figure 11.
DiabetesHypertension
AsthmaMuscle/JointHeart Disease
HeadachesGout
HeartburnAllergies
0 1 2 3 4 5 6 7 8
Disease and Health Problems in Lao Nadi Community
Number of Villagers
Hea
lth P
robl
em
Post-intervention results were based on the events that occurred during our intervention.
More specifically, we base our post intervention results largely on responses from the attendees,
participation, perceived interest among the attendees, and perceived engagement from the
attendees. Our intervention focused on the research findings. At our intervention, approximately
24 community members attended the nutritional information session. We found that most
community members in attendance were adult females and children, while only one adult male
was present but not involved in the intervention session. Therefore, it is evident that there is a
gender gap regarding interest in health among Lao Nadi community. There needs to be more
emphasis on drawing in male community members to get involved with health-related
opportunities.
26

Running head: Nutrition in Lao Nadi
The community members were engaged in the nutritional information session, especially
during the rice portion control session and during the meal planning activity. In order to evaluate
the audience interests and assess the audience’s gained knowledge, we organized a discussion
session following the intervention. Some community members stated that they learned about
how many servings of rice to eat and how to navigate the nutrition flag. Additionally, during this
time, the audience asked the following questions: “How many eggs should I eat per day as I get
older? What is a good body weight? What is a good substitute for salt? What is a good substitute
for sugar?” These questions ultimately conveyed the community members’ further interest on the
topic of nutrition and their desire to learn more about nutrition for the benefit of their own health.
Overall, the results convey that the community members in attendance gained knowledge from
the basic information that student researchers provide during the intervention. More importantly,
the discussion confirmed that many community members were highly interested in the topics
covered during the intervention session and wanted to seek out more information in the future.
5. Discussion
Overall, our research results and intervention process indicate that there is a lack of
adequate nutritional information available to Lao Nadi community members. In Lao Nadi, the
only efforts to promote healthy eating habits come from the few available village health
volunteers that usually only tend to community elders. While there are intentions to improve Lao
Nadi’s access to health information and provide community members with healthy outlets, there
are little efforts being made to implement these opportunities. Therefore, the community could
greatly benefit from more nutrition-based information sessions and the increase of access to
education resources. .
27

Running head: Nutrition in Lao Nadi
The high consumption of white rice, sticky rice, stir-fried dishes, noodles/soups, som
tam, pork, omlettes, and 3-1 coffee are all are dishes that are core to the Thai diet (source). While
these foods cannot be completely eliminated, we discussed the idea to educate community
members on using portion control and meal planning methods to lesson their intake of these
foods. We also used the Thai nutritional guidelines and Thai food flag as a guide to help
community members understand what food groups were important to eat and in what quantities.
These food choices are not only rooted in Thai cultural attachment certain dishes , but also relate
to the nutritional transition that has occurred in Thailand. The consumption of animal proteins
and processed foods is quite common as more and more community members shop at super
markets and are consuming a lot of meat. While we did not discuss the different options of
protein outside of pork and red meats, our research findings indicate that chicken and fish are
common food choices within the Lao Nadi community. In our observational study at Thalad
Lampoon, we found that there is substantial access to fish, chicken, tofu and soy products—all
which are forms of protein. Perhaps the discussion of other protein options could have been
beneficial to our intervention session.
To address the issue of 3-1 coffee, we offered an instant coffee alternative sample, which
is higher in coffee and lower in sugar. However, community members were largely opposed to
the taste of the coffee because it wasn’t as sweet as they were used to. We also did not consider
the difference in preparation between 3-1 coffee and instant coffee. This posed a challenge to us
during the intervention when community members tasted plain black coffee. Shocked by the
bitterness, many immediately expressed their dislike. To address the mistake, we explained the
different steps associated with preparing the coffee and provided samples for families to further
experiment at home.
28

Running head: Nutrition in Lao Nadi
Additionally, we confirmed that access to healthy foods or affordability of it was not an
issue, but the issue lied in knowledge of nutrition and the methods in which food is typically
prepared. Stir-frying is a common form of cooking specific to Thai foods. This method is not the
healthiest way to cook, so we provided a solution to this issue with portion control as an option
in order to control the intake of foods high in unhealthy fats and excess oil.
Overall, the intervention brought in many interested community members, however, there
was an unequal gender distribution. Only one male community member was present, but he
unfortunately was not engaged in the information session. Therefore, it could be deduced that
there is a lack of interest in nutrition among men in the community. While we did not foresee the
issue of gender distribution as being a potential problem, it is important that future student
groups focus on the need to draw in more male community members. Ten male community
members were interviewed during the data collection process. The data indicates that men too
are affected by similar health problems that result from unhealthy diets and also consume the
common unhealthy foods typically consumed in the community. Perhaps male community
members perceive meal preparation and cooking as female responsibilities, and therefore, did not
understand the direct impact that food choice, meal preparation, and nutrition has on their health.
Therefore, these gendered norms may affect how men view health in relation to food and
nutrition.
Additionally, language barriers and cultural difference had an inevitable effect on our
research and intervention. Because we are foreign students, there is a possibility that many
community members attended the intervention for us, rather than for themselves. However, we
strongly feel that regardless of their intentions, community members actively engaged and
learned from the nutritional information session. Also, communication between the translator
29

Running head: Nutrition in Lao Nadi
and the student group was difficult, as we were unsure if our words were communicated clearly.
There was some miscommunication that occurred during data collection between the translator
and the student group. At times, we realized that the translator did not provide us with the
complete answers given by the community members, and we sometimes had to encourage the
translator to relay the details of the conversations with community members. Therefore there
were certain gaps in the information provided to us and to the community members. Language
barriers were also a reoccurring issue during the intervention, as community members were
reliant on the translator to help walk them through the meal planning session. This was a
constraint because there was only one available translator assisting several community members.
Additionally, the cultural difference between American students and Thai community members
is also an inevitable constraint that restricted us to fully understand the cultural ties that may
withhold community members and their understanding of nutrition the way they saw it.
Despite the challenges faced during the research and intervention session, community
members expressed interest in our intervention. Additionally, they were actively engaged
throughout the intervention. During the evaluation, some community members expressed further
interest in learning about nutrition and asked questions that we could not answer due to or
limited knowledge on n nutrition. Other participants also expressed interest in more
informational sessions to address body mass index and food consumption. We recommend that
future groups invite a nutrition expert to help answer questions that come up to avoid the
spreading of inaccurate information. Overall, attendants of our intervention enjoyed themselves
and were engaged in what we had to teach them about. Hopefully our efforts further motivated
them to take their health into their own hands and improve their dietary habits.
30

Running head: Nutrition in Lao Nadi
6. Conclusion
6.1 Summary of Findings
It was found that the Lao Nadi community members share many common dietary trends.
The top five foods and drinks consumed in the community are white rice, sticky rice, stir-fried
dishes, noodles/soups, and “3-in-1” instant coffee drink. Skipping breakfast was also common.
Additionally, diabetes, hypertension, and heart disease are the three most common NCDs that
affect adults within the community. An information based intervention session was created
based on the community research results. The intervention focused on the concepts of the
common NCDs, the top 5 consumed foods, portion control, alternative food options, the Thai
Nutritional Flag, and meal planning. The intervention was evaluated to be successful based upon
participation levels and audience comprehension.
6.2 Strengths and Limitations
There were several strengths and limitations to the research and intervention. A major
strength is that each member of the research group had developed a strong relationship with the
Lao Nadi community by returning several times over the course of the semester. As a result, the
community was highly receptive to being involved in the research and intervention process. The
intervention had a large number of participants in attendance considering that the intervention
took place on a weekday right before dinnertime. In addition to the strong relationship with the
community, a second strength contributing to the participation was the use of advertising. The
creation of a budget that aimed high was a strength because while many items ended up costing
less than anticipated, other basic items that had not been previously factored into the budget were
able to be purchased, such as tape and highlighters.
31

Running head: Nutrition in Lao Nadi
Strengths of the intervention itself include the structure and content. The information
presented was based off of the findings of the research and these findings were presented to the
community members so that they could understand the reasoning behind selecting the
information being taught to them. It was highly beneficial to incorporate a mixture of
information and interactive activities and discussion into the structure of the intervention because
it maintained participant interest and could address the differences in learning styles of the
audience.
While there were multiple strengths, this final project had limitations as well.
Other than the addition of a small amount of observational data collection, only one research tool
was utilized for conducting research within the Lao Nadi community. The use of semi-structured
interviews, while highly beneficial, may not have provided complete information on the topic.
The use of a focus group may have proved to be beneficial as well for gathering information
about nutritional knowledge and motivations of certain eating habits and patterns, however this
tool was not implemented due to poor attendance at previous focus groups in the Lao Nadi
community during research earlier in the semester. In relation to this, a small sample size limited
the conclusions that could be drawn from the data collected. While there was a decent number of
people in attendance for the intervention, the time allotted for it was a possible limitation. The
headman had indicated that weekends were the best time for the community and originally the
intervention was scheduled for a Sunday but it had to be changed to a Tuesday evening due to
scheduling logistics for all of the interventions. The lack of men in attendance could be related to
them not yet returning home from work.
The use of a translator is always a limitation because of the possibility of mistranslations
and some information being lost in translation. Additionally, it would have been beneficial to use
32
Running head: Nutrition in Lao Nadi
more than one translator during the meal planning activity because many participants required
assistance. The translator was the only person with the language capability to assist the
participants in need and she had to focus her attention on those who were illiterate, preventing
some other participants from receiving help and fully understanding the activity. Next, the
researchers were not experts on nutrition and therefore only had the knowledge to teach basic
concepts of nutrition. Some questions presented by the participants could not be answered.
The effectiveness of the intervention was limited due to the short amount of time allotted for the
project and because it is difficult to change long-term and culturally based habits, especially after
a single presentation of information. Finally, effectiveness of this intervention cannot be
evaluated in the long-term by the research group who ran the intervention. It is possible that
future CIEE students will conduct further research related to nutrition in Lao Nadi for a potential
intervention but there is not a way to follow-up with the specific participants of this particular
intervention.
6.3 Recommendations for Future Interventions
It is highly recommended that students perform interventions within communities that
they have built a strong rapport with. The community and the students will be able to best meet
each other’s needs if a strong relationship between the two parties is developed over the course
of the semester. A recommendation for future interventions would be to hire an expert on the
intervention topic to help with certain components of the intervention. For example, in this case,
a nutritionist would best able to address the specific needs of the community and answer specific
questions. Next, a structure that includes the use of interactive activities is beneficial because
active tools can be effective in teaching and engaging the participants. The Lao Nadi community
members enthusiastically participated and remained attentive during the rice serving portion
33

Running head: Nutrition in Lao Nadi
activity and meal planning activity, while appearing distracted during the lecture component.
Finally, remaining flexible to unforeseen circumstances and possible changes is a necessary
component of the intervention process. Planning research and a subsequent intervention involves
not only the considerations of the student group and CIEE, but also the outside parties. Changes
are inevitable and the research team will need to adapt. Even if change occurs, the intervention
can still be successful.
6.4 Future Considerations and Directions for Further Research
Future considerations and directions for further research can be based on aspects of this
intervention. More research could be conducted about actual levels of nutritional knowledge
since the research that has been conducted within the community was mainly focused on dietary
trends and habits. The attendance and participation of multiple children during the intervention
indicates that they could be a potential target group for future research since the research
conducted had previously been limited to those ages 30 and up. Interviewing individuals under
the age of 18 could possibly bring about ethical implications. Possible directions for research and
interventions involving a younger demographic could focus on investigating what is taught in
schools and the actual knowledge level of children. Men could be another population to further
target because the research results indicate that they have a need for nutrition education but were
absent in attendance from the intervention. Therefore, potential means for reaching out to them
could be explored. Lastly, it could be beneficial to interview a nutritionist at Khon Kaen
University to understand potential nutrition related issues that Thai people in the Isaan region
face and how they could be addressed.
34

Running head: Nutrition in Lao Nadi
7. Acknowledgements
The Lao Nadi nutrition research team would like to extend a big thank you to the
individuals who made our research and intervention possible and successful. First, we would
like to thank Ajaans Toon and Nai for being incredibly prompt in their responses to all of our
group’s needs. Next, we would like to thank Ajaan Pattara for his helpful suggestions during the
research and intervention planning process. Third, Ajaan Jen and KJ provided extra academic
and moral support. Finally, we would like to thank the Lao Nadi headman for graciously
welcoming us into his home on multiple occasions and for helping us to advertise our
intervention over the community loudspeaker system.
35

Running head: Nutrition in Lao Nadi
References
Bumrungrad Intenational Hospital. (2010, December, 3). Hypertension and Diabetes: Living with
serious chronic conditions. Better Health. Retrieved from
http://www.bumrungrad.com/en/betterhealth/2010/30th-anniversary/hypertension---diabetes--
living-with-serious-chron
Center for Disease Control and Prevention (17 October, 2013). Global Health Thailand. Retrieved from
http://www.cdc.gov/globalhealth/countries/thailand/
Center for Disease Control and Prevention (11 January, 2013). Fast Stats – Leading Causes of Death.
Retrieved from http://www.cdc.gov/nchs/fastats/lcod.htm
Davis, D.L, Raymond, J.E., Clements, V., Adams, C., Mollart, L.J., Teate, A.J., Foureur, M.J. (2012).
Addressing obesity in pregnancy: The design and feasibility of an innovative intervention in
NSW, Australia. Women and Birth, 25, 174-180.
Doak, C. (2002). Large-scale interventions and programmes addressing nutrition-related chronic
diseases and obesity: examples from 14 countries. Public Health Nutrition, 5, 275-277.
Gibson R. S., Ferguson E. L. (1998). Nutrition intervention strategies to combat zinc deficiency in
developing countries. Nutrition Research Reviews, 11, 115-131.
Heshka, S., Anderson, J., Atkinson, R., Greenway, F., Hill, J. (2003). Weight Loss With Self-help
Compared With a Structured Commercial Program: A Randomized Trial. JAMA, 289, 1792–
1798.
Kelly, M., Banwell, C., Dixon, J., Seubsman, S., Yiengprugsawan, V., Sleigh, A. (2010). Nutrition
transition, food retailing and health equity in Thailand. Australas Epidemiol. 17 (3), 1-11.
36

Running head: Nutrition in Lao Nadi
Kiple, K. Ornelas ,K. (2000). The Cambridge World History of Food. Retrieved from
http://www.cambridge.org/us/books/kiple/rice.htm
Kosulwat, V. (2002). The nutrition and health transition in Thailand. Public Health Nutrition, 5(1A),
183-189.
Lefferts, L. (2005). Sticky rice, fermented fish, and the course of a kingdom: The politics of food in
Northeast Thailand. Asian Studies Review, (29) 3, 247-258.
Noor, M.I. (2002). The nutrition and health transition in Malaysia. Public Health Nutrition, 5(1A), 191-
195.
Räihä, T., Tossavainen, K., Turunen, H., Enkenberg, J., Kiviniemi, V. (2012). Effects of Nutrition
Health Intervention on Pupils’ Nutrition Knowledge and Eating Habits. Scandinavian Journal of
Educational Research, 56, 277-294.
Sirichakwal, P. Sranacharoenpong, K. & Tontisirin K. (2011). Food based dietary guidelines
development and promotion in Thailand. Asia Pacific Journal of Clinical Nutrition 2011; 20 (3):
477-483.
Taechangam, S., Pinitchun, U., Pachotikarn, C. (2008). Development of nutrition education tool: healthy
eating index in Thailand. Asia Pacific Journal of Clinical Nutrition, (17) 1, 365-367.
UNFPA. (2006). Population Ageing in Thailand: Prognosis and Policy Response. Retrieved from
http://thailand.unfpa.org/documents/thai_ageing_englishversion.pdf
Waleekhachonloet, O.A., Limwattananon C., Limwattananon S., Gross, C.R. (2007). Group behavior
therapy versus individual behavior therapy for healthy dieting and weight control management in
overweight and obese women living in rural community. Obesity Research & Clinical Practice,
1, 223–232.
37

Running head: Nutrition in Lao Nadi
Woolfe, J., Stockley, L. (2005). Nutrition health promotion in schools in the UK: Learning from Food
Standards Agency funded schools research. Health Education Journal, 64, 229–246.
World Health Organization, (1990). Diet, nutrition and the prevention of chronic diseases. Report of a
WHO Study Group. Geneva. WHO Technical Report Series, No. 797
World Health Organization. (2003). Diet, nutrition, and the prevention of chronic diseases. Geneva,
Switzerland: WHO Technical Report Series.
38